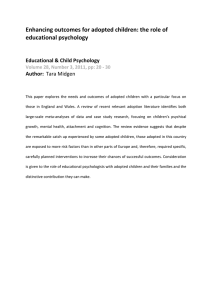
The Wiff Curve' The 'Kiff Curve': An integrative model for thinking about the provision of clinical psychology Joe Kiff This paper describes an integrative model that I have used for many years to understand what clinical psychologists do in adult mental health. unpublished in the academic literature, the integrative model I describe in this article is not new: I provided an early copy of this paper to Mowbray as part of my submission to the MAS review (Mowbray, 1989). Many of my colleagues and supervisees have found it a useful framework for thinking about clinical issues. It developed out of my work in adult mental health but colleagues from other specialties have also found it helpful. In the paper I hope to highlight some historical trends that I believe have taken place over the past couple of decades, the result of which has meant that, for many of us, the bulk of our work now lies with people with complex, moderate to severe problems that pose difficult clinical challenges for all practitioners. THOUGH PREVIOUSLY The Model In 1986, after I had been practising in adult mental health for five years, I sat down to try to clarify what I knew. I had originally trained on the (then) behaviourally oriented Birmingham course and subsequently completed the certificate in psychodynamic therapy at the Tavistock clinic. I had also been a supervisor for the Lichfield counselling service for three years. By then I had personally seen a broad spectrum of approximately 250 people and felt that I had developed a satisfactory grasp of behavioural, counselling and psychotherapy techniques. The question at the forefront of my mind was: what approach seemed relevant to which kind of client? 46 Now, with over 17,500 hours of direct clinical work and 3000 hours as a supervisor, I feel the model I came up with provides a useful framework for thinking about clinical issues and for helpfully thinking about this question. The model, which colleagues christened the 'Riff curve', is represented in Figure 1. On the y axis I wanted to get away from the notion that the main therapeutic approaches are mutually exclusive. I feel that I, and many of my colleagues, work in three main modes: • Prescriptive. With some people I primarily give advice about practical courses of action. Such people are often referred with a specific problem and the active ingredient of therapy has been to help them make cognitive and behavioural changes to resolve the presenting problem. CBT and psycho-educational models of working largely inform this work. • Supportive. Other people present with problems that seem to reflect current conflicts in their lives. They are depressed and anxious because of social and relationship conundrums that they cannot resolve. In these situations the active ingredient in the therapy appears to involve providing a safe environment from which people can clarify their options and values and come to necessary decisions to improve their lives. This encompasses various humanistic models (primarily Rogerian counselling). III Exploratory. Other people are referred with problems that appear to reflect long-term patterns based on their early life experiences. Current difficulties may not be resolved at the supportive or prescriptive level, and the active Clinical Psychology Forum 204— December 2009 ingredient in the therapy involves exploring the learning history and the links between this and the person's presenting problems. Primarily this involves psychodynamic models. I also attempted to place each client along a continuum of 'mental health' (x axis). For the majority of people seen, early life experiences mirror social and relationship functioning and the combination of these factors relates to both the severity and complexity of their problems. Taking account of these factors I found I could place people on a notional Mental Heath Index. At one end were people who seemed well integrated, who were able to relate to me as a therapist in a trusting and straightforward way. Generally speaking they appeared to come from relatively stable family backgrounds, to have rewarding social lives, usually living in a stable relationship with someone who provided some support, and were consulting with spe- cific difficulties. At the other end were people who seemed to have tremendous difficulties relating to me, because they were psychotic, extremely withdrawn or very emotionally labile. Generally, they had experienced very disturbed early lives, had disturbed (or nonexistent) current relationships and had a whole plethora of problems, many of which were severe, many of which had long histories. Placing people between these points I started to see what approach seemed to be effective for different clients. In making sense of this picture I identified six loose groupings that seemed to run into each other although each seemed to warrant different interventions. Group 1: Short-term directive therapy This has worked well with well-integrated people with specific problems. Such people are often trusting and once a course of action is explained to them they are able to DEPTH OF INTERVENTION Prescriptive Supportive Exploratory Good MENTAL HEALTH INDEX Poor Figure 1: The Kiff curve Clinical Psychology Forum 204 — December 2009 47 TJoe Kiff cooperate and generally benefit quickly from a symptomatic approach. At assessment there seems to be little justification for looking more deeply into their current relationships or further exploring their early life. An example of such a person might be a young man involved in a road crash who has spent six months recovering in hospital. Left with residual anxiety about driving and a loss of social confidence, having been out of circulation for so long, but with supportive friends and family, he benefited from 6 sessions of anxiety management and social tasksetting, spread over 12 weeks at once a fortnight intervals. Group 2: Short-term supportive therapy For people in this group counselling support is the main intervention. For example, a woman who nursed her ageing mother for two years presented as depressed shortly after her mother's death. With no evidence that the relationship between mother and daughter was particularly troubled, grief counselling was appropriate. There was no justification for exploring her early life and it would be insensitive to treat the depression as an isolated symptom. What was required was to provide the space in which grief could be explored, 'symptoms' understood, and plans formulated for the future, on the basis of her own values. In this case the woman felt she had learnt a great deal about nursing elderly people and wanted a job in a care home. This helped resolve her existential crisis, gave her satisfaction and purpose and a basis on which to build a fresh life. We met for eight sessions spread over five months, meeting at fortnightly intervals. Group 3: Short-term exploratory therapy As clients come from more disturbed backgrounds they are less able to resolve their current emotional difficulties without addressing the historical antecedents of these problems. For example, a woman who was having difficulties in her second marriage, because she could not trust her husband not to abandon her, in my opinion needed to examine the idea that this was the issue behind her first divorce, and appeared to be related to 48 The Wiff Curve' the fact that her father left home unexpectedly when she was a child. In addition, it was beneficial and important to address this dynamic in the transference with her (male) therapist, whom she had difficulty trusting. Assuming a reasonably integrated client, a short-term exploratory therapy (see Holmes, 1994), perhaps following Malan's model (see Malan, 1979) seemed appropriate, and this person benefited from 12 sessions of fortnightly psychotherapy spread over six months. Group 4: Long-term exploratory therapy With more damaged clients, longer-term exploratory therapy might be indicated. For example, if the client has been the victim of physical violence when young and had a history of involvement with a sequence of men who are violent to her, then one might anticipate that therapy might be more difficult and time consuming. One sees the benefits of longer-term work because the therapeutic issues are more complex, the problems are more pervasive and resistant to change, and the technical challenge of maintaining the therapeutic relationship is more taxing (but ultimately rewarding for the client). The woman described above eventually benefited from meeting me 25 times spread over 18 months (initially weekly, then on a fortnightly basis, with two follow-up meetings at three-monthly intervals). Group 5: Long-term supportive therapy For some clients the pain of working through the past is too much to bear, at least in the confines of NHS practice where the pressure of referrals and waiting lists rarely permits more than once a week therapy. For this group longer-term, episodic, supportive therapy is indicated to allow these people to re-establish the status quo in their current lives and to come to terms with the persuasiveness of their ingrained difficulties. For example, one client told of an extremely difficult childhood with his prostitute mother. Having six siblings, all by different fathers, it seemed the only reason he was not more disturbed was because his aunt had taken him away and provided a stable home when he was seven. When he came to therapy, with Clinical Psychology Forum 204— December 2009 crippling social anxiety, his aunt was dying. I did not feel he was integrated enough to withstand an exploratory approach, but he related to me enough to benefit from a supportive relationship that took him through the crisis. People in this group do not generally find a 'cure' for their condition, but can be helped to manage their difficulties and find less damaging ways of coping with their problems. They are often re-referred at other times of crisis in their lives. I have come to see the value of offering intermittent time-limited treatment contracts to such clients to provide support at particularly difficult times. The man described above met me for three episodes of care, where I provided a containing, counselling relationship, over a five year period, receiving eight then two then five sessions each time he got in contact. He did not wait on the waiting list and sessions were offered as 'whenever necessary to contain crises'. Group 6: Long-term prescriptive therapy There are clients whose capacity to relate is so impaired that they cannot easily profit from a supportive or exploratory relationship alone, and their self-care difficulties require the concrete structure of directive approaches. The very socially isolated son of a mother diagnosed as schizophrenic exemplifies this group. For much of our contact he hardly seemed to engage meaningfully at all and we seemed to inhabit different worlds. It was only when we embarked on a programme of basic social skills training that he seemed to make significant progress. People with ingrained and severe problems in relating to others and few supportive relationships that they find meaningful seem to benefit more from a fixed number of sessions while supported by other members of a team. Our 16 sessions were spread out over 18 months, with an initial weekly focus to establish the model then monthly and subsequently six-weekly monitoring meetings focusing on a specific aspects of his difficulties. Some strengths of the model • The model underlines the importance of psychologists equipping themselves Clinical Psychology Forum 204 — December 2009 with a broad range of skills and perspectives to be able to mix and match their theoretical and practical skills to the needs of the person. This has implications for clinical training and the need to develop the capacity of learners to thoughtfully apply different approaches. • It helps us clarify the limitations of therapy with group 5 and 6 people. Coming out of a training that uses a mastery model, newly qualified psychologists spend years trying to find a realistic level of therapeutic hope. Avoiding interminable therapy with these clients is key to maintaining throughput and an important focus in terms of minimising waiting lists. Many psychologists struggle to apply the evidence base on What Works for Whom (e.g. Roth and Fonagy, 2004) and seem to intuitively relate to the Kiff Curve in a way that has greater impact on the interventions they provide. • For trainees faced with having to make sense of a number of approaches and therapy models the framework helps them see how different models might be related and effective in different circumstances. • When supervising trainees I endeavour to ensure that they mostly start with group 1 and 2 work, in order for them to gain confidence. Then, should the complexity of the work emerge with a particular client, or there be opportunities for trainees to see people from other categories, I look to help them develop their thinking from this base. • The model integrates a number of theories into a coherent whole and illustrates integrationist working that I think reflects the way in which many of us work on a day-to-day basis. III The model helps us understand the compatible roles of different professional groups within community mental health teams. Nurse Behaviour Therapists (and now Low Intensity IAPT workers) might have the skills and be the most appropriate people to do 49 Joe Kiff • • • mainly group 1 work; Counsellors and High Intensity IAPT workers group 2; Clinical Psychologists group 3 and 4; Social Workers and CPNs group 5 and 6. The model underlines the position that the bread and butter work for psychologists in these contexts is with the moderate severity, moderate complexity patients whose problems reflect their social contexts and certain patterns from their past, and whom frequently challenge members of other professions who can struggle to understand the underlying basis of their difficulties. The model illustrates level three working (Mowbray, 1989) and managers have found this useful in conceptualising how psychologists contribute therapeutically across the whole spectrum of care, clarifying our central role in assessment, allocation, supervision and consultation. The model is a useful framework from which to consider the workload of an individual, service or department; to develop ideas for training; and to consider skills mix and experience levels regarding recruitment. Conclusions Following a plethora of changes in the NHS two important trends have emerged. Many people with more straightforward problems and histories are no longer being referred into psychology departments or CMHTs but are instead being seen in primary care (e.g. by IAPT workers). From the pool of difficult cases remaining, many of the most complex of these are allocated to clinical psychologists, perhaps as CMHT staff do not feel they have the training or skills to help them effectively. Such referrals are consistently challenging and there is a feeling amongst many experienced colleagues and newly qualified psychologists that our clinical training does not equip us for this work, particularly if it has been too limited in terms of training in a particular model. Formulating people's presenting problems and developing therapy plans can be quite a challenge, as can managing feelings in the sessions and maintaining an ability to think clearly in the face of the confusing and contradictory impacts associated with therapy in this client group. Clinical trainers and CPD managers will need to address these issues as they help us prepare for this new emphasis in our work. Acknowledgment Thanks to Guy Holmes for his endless encouragement and for reading and commenting on various drafts Affiliations Joe Kiff: Dudley & Walsall Mental Health Partnership NHS Trust Address Dr Joe Kiff, c/o Psychology Dept, Cross Street Health Centre, Cross Street, Dudley DY1 1RN; joe.kiff@dudley.nhs.uk References Holmes, J. (1994). Brief dynamic psychotherapy. Advances in Psychiatric Treatment, 1, 9-15. Malan, D. (1979). Individual psychotherapy and the science of psychodynamics. Oxford: Butterworth. Mowbray, D. (1989). Review of clinical psychology services. Cheltenham: 1\4AS. . Roth, A. & Fonagy, P. (2004). What works for whom? London: Guilford Press. Visit the Division's website www.bps.org.uk/dcp 50 Clinical Psychology Forum 204— December 2009 DCP Update Obituary: Catherine Caulfield 1969-2008 Catherine died suddenly and unexpectedly in November 2008, leaving behind a close and loving family and a wide circle of friends and colleagues, all of whom mourn her death. I first met Catherine when she joined Lewisham & Guy's Trust psychology services in 1997. I was immediately impressed by her intelligence, her humour and commitment to her work with children and families. She was an incredibly warm and friendly person, whom everyone liked. I was always pleased to meet up with her, or to hear from her. Cath was brought up in Whitley Bay in North East England and studied psychology at Leicester University. She trained in clinical psychology at the Institute of Psychiatry, graduating in 1997. Before her training as a clinical psychologist, she was employed as a research assistant with older adults at the Maudsley Hospital. But after training, Cath specialised in work with young people with complex difficulties, doing so with great skill, commitment and humanity. She worked in four different teams and services within the South London & Maudsley NHS Trust and Guys & St Thomas's Hospitals before moving to work at Great Ormond Street Hospital in 2008 to join their paediatric psychology team. Cath specialised in paediatric neuropsychology and completed a postgraduate diploma in clinical neuropsychology at IoP in 2000. With other remarkable psychologists at the Newcomen Centre, she combined her technical knowledge of brain and behaviour with a careful attention to, and respect for, the wider needs of the child and the family as a whole. She worked with children with neurodevelopmental disorders at the Newcomen Centre at Guy's Hospital in 1997, the brain and behaviour team at the Maudsley Hospital until 2000, and from 2000 to 2003, the OCD team in the Children's department with Isobel Heyman and psycholClinical Psychology Forum 204 — December 2009 ogy colleagues. She then moved back to Guy's Hospital in 2003, to set up a psychology service within the cleft palate service for South Thames region. By this time she was taking a lead clinical role in the team, conducting research and developing new services at a local level and nationally for children with cleft palate and their families. In 2008 she took up a senior psychology post in immunology and ENT at Great Ormond Street Hospital where, despite being there only a short time before her death, she was very highly regarded. Right from the start of her career, her senior psychology colleagues recognised her abilities. A former research supervisor described Cath as balanced, grounded, constructive, and 'emotionally intelligent'. Her clinical child supervisor described her as showing early signs as a trainee of becoming the outstanding clinician she became, always prepared to support others, and always prepared to go the extra mile with young people that were difficult to engage. She was a highly valued team colleague, described as caring, supportive and 'lovely' to work with, and generous with her time. She trained and nurtured junior psychologists too. The course tutor at IoP remembers her as an excellent and popular supervisor and teacher, and that all the trainees left their placement with Cath singing her praises. He recalls that mid-placement reviews always ended with their having a laugh together. And that smiling, sociable aspect of Catherine is part of our memories of her as a psychologist. One of her managers described her as having a wonderful creative ability to engage with children and make therapy fun. Children whom she saw really enjoyed her sessions. She was immensely likeable, with a great sense of humour. She was always friendly, and responsive to people around her. From the start of her career she made 51