Multifactorial Inheritance & Polygenic Disorders Presentation
advertisement

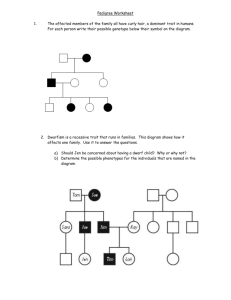
Chapter 12 Multifactorial Inheritance and Common Diseases ( Polygenic Disorders) (多基因病) Li Lingyun Department of developmental genetics Tel: 025-86869463 Email:lilingyun@njmu.edu.cn Huntington's disease Single gene Disorders Hemophilia 血友病 亨廷顿氏舞蹈症 Duchenne muscular dystrophy 杜氏肌营养不良 Albinism 白化病 Brachydactyly 短指症 Example: A woman/man who is a prolific writer has a daughter who becomes a successful novelist. Yan,Geling (严歌苓) and her father Example: An overweight man /woman have obese children. Example: A man whose father suffers from alcoholism has the same problem. Question Are these characteristics—writing talent, obesity, and alcoholism—inherited or learned? Are they a combination of nature (genetics) and nurture (the environment)? What are Polygenic Disorders ? Polygenic disorders are the diseases result from complex interaction between multiple gene and variety of environmental exposures that trigger, accelerate, exacerbate the disease process. Also called multifactorial disorders, complex disorders. NOTE: 1. Multi-gene involvement, with each gene exerting a small additive effect. 2. Often have environmental factors influences. Gene Gene Gene environment al factors Gene Polygenic trait polygenic disorder The difference of polygenic disorders and single-gene disorders Unclear transmittance patterns These disorders show a definite familial tendency, but the pattern of inheritance is different from single gene disorders. The incidence in close relatives of affected individuals is usually around 2~4%,lower than single-gene disorders. Both genetic factors and environmental factors are all involved in causing these disorders. Polygenic Traits:Height、skin color and weight Genes Height Improved diet Yao Ming Chinese basketball player (爸爸)姚志源 2.08m (妈妈)方凤娣 1.88m (儿子)姚明 2.26m Polygenic disorders Hypertension 高血压 Schizophrenia 精神分裂症 Asthma 哮喘 Section 1. Principles of Multifactorial Inheritance Single-gene disorders: qualitative trait Mendelian trait that is either present or absent. One has the trait or not. such as “normal” versus “affected.” Exhibit discontinuous variation among the phenotypes. Example – albinism ; green peas vs yellow peas Qualitative trait AA Aa AA Compete dominance Aa aa Incompete dominance Mendelian trait Single gene trait Present or absent With no overlap RR rr AA/Aa aa Rr Polygenic Disorders: quantitative trait A polygenic trait, the combined action of many genes often produces a “continuously varying” phenotype. which are measurable characteristic . Often fit normal distribution Examples - height, blood pressure, skin color, intelligence Quantitative trait Polygenic Trait Continuous variation: phenotypes distribute from one extreme to another in an continuous fashion Physiological or biochemical quantities Example: The distribution of height in a population 1920 The tallest people : 5′9′′ tall 1997 The tallest : 6′5′′ tall Height is influenced by genes and environment during growth Improved nutrition can impact height Polygenic traits show continuous distribution in the general population. Mean Number of men (thousands) 12 a symmetrical bellshaped curve 10 8 6 4 2 0 150 155 Height(cm) 160 165 170 175 180 185 190 Regression to the mean Shortest Tallest P Francis Galton Multifactorial inheritance was first studied by Galton, a close relative of Darwin. Galton established the principle of what he termed "regression to mediocrity." F1 F2 Polygenic trait In general, Galton noticed that extremely tall fathers tended to have sons shorter than themselves, and extremely short fathers tended to have sons taller than themselves. QUESTION: How do genes generate such a normal distribution? Use height as a model trait Assume that height is controlled by a single locus with genotypes AA, Aa, and aa. Allele A tends to make people tall, and allele a tends to make them short. intermediate Assume: two separate loci (Aa, and Bb) are involved in determining final adult height. P1 gametes AaBb x AaBb AB ab Ab AB AABB AaBb AABb AaBB ab AaBb aabb Aabb aaBb Ab AABb Aabb AAbb AaBb aB AaBB aaBb AaBb aaBB aB According to mendelian law, it is can be produced 16 fertilization recombination, 5 phenotypic classes. The distribution of height, assuming that height is controlled by two loci 2 1 0 3 4 Number of dominant allele There are now five distinct phenotypes instead of three, and the distribution begins to look more like the normal distribution. Genome-wide association studies have identified more than 200 loci associated with human height. We now extend our example so that many genes and environmental factors influence height, each having a small effect. Then there are many possible phenotypes, each differing slightly, and the height distribution approaches the bell-shaped curve . Distribution of height, assuming that multiple factors, each with a small effect, contribute to the trait (the multifactorial model). Another example: Human Eye Color Light blue, deep blue, light brown, medium brown ,and black Example: Human skin Color Another example: Blood pressure There is a correlation between parents’ blood pressures and those of their children. But blood pressure is also influenced by environmental factors, such as diet and stress. Summary of Section 1 : The Multifactorial Model Many traits are thought to be influenced by multiple genes as well as by environmental factors. The genes underlying continuous traits are following Mendelian principles of segregation and independent assortment. Genes can generate a continuous trait when they act together. As the number of loci involved in a trait increase, the number of resulting phenotype classes increase, the distribution looks increasingly like a Normal distribution, also called the Bell Curve. Question If polygenic traits are quantitative traits with continuous distribution, how can account for discontinuous polygenic disorders (either present or absent in individuals)? These are best explained by the liability/threshold model. Spina bifida Section 2 The Liability/Threshold Model Liability The genetic determination of an individual’s predisposition to the disease is called susceptibility, while the genetic and environmental determination of the predisposition is defined their liability. Threshold To account for a discontinuous phenotype (i.e. affected or not affected) with an underlying continuous distribution, it is proposed that a threshold exists above which the abnormal phenotype is expressed. Distribution of liability in the population Threshold •Below the threshold, normal development is observed. •Beyond the threshold, disease results; unaffected affected population incidence low liability average liability high liability The liabilities of all individuals in a population form a continuous variable, which has a normal distribution both in the general population and in relatives of affected individuals. A liability distribution for a multifactorial disease in a population. Example: cleft lip/palate Threshold 阈值 Liability Low Few of the alleles or environmental factors High More of the disease causing alleles and environmental factors Threshold model for polygenic disorders 1. The threshold model assumes that there is a liability toward development of a disorder that is normally distributed in the general population. 2. This liability is composed of contributions from both genetic and environmental factors that can lead to expression of the trait. 3. Individuals will have more or less liability toward the trait, depending on how many of the predisposing genes they have inherited and the degree to which they are exposed to the relevant environmental factors. 4. The trait is expressed only in individuals whose liability exceeds a threshold. NOTE: This is a hypothesis rather than proven fact, is that it provides a simple explanation for the observed patterns of familial risks in conditions, such as cleft lip/palate and spina bifida. Liability cannot be measured, but the mean liability of a group can be determined from the incidence of the disease in that group using statistics of the normal distribution. Section 3 Estimating Recurrence Risk of polygenic Disorders • Risk estimation is more complex for multifactorial diseases • Geneticists use empiric risks, which are based on incidence in a specific population. Empiric risks Empiric risk is not a calculation, but a population statistic based on observation. Empirical recurrence risks for multifactorial diseases are based on studies of large collections of families. These risks are specific to a given population. Section 3 Estimating Recurrence Risk of polygenic Disorders 1. The recurrence risk is related to heritability. Condition: the frequency in population is 0.1%~1% and the heritability is 70%~80%。 The risk of recurrence for first-degree relatives, i.e. siblings and offspring, approximates to the square root of the general population incidence. Edward Formula qr = f qr :The risk for offspring and sibling of probands f :Prevalence in population For example, cleft lip/palate The population incidence : 0.17%, Heritability: 76% The first-degree relative risk : 4% 2. The recurrence risk for the disease usually decreases rapidly in more remotely related relatives. Familial aggregation of quantitative traits. The risk is greatest among close relatives of the affected individual and decreases rapidly in more distant relatives. For example: In spina bifida the risks to first, second and thirddegree relatives of the affected individual are approximately 4%, 1% and less than 0.5%, respectively. Empiric risk of cleft palate Relationship Recurrence Risk General population 0.1% First cousin 0.3% Niece or nephew 0.8% Child 3.5% Sibling 4.1% Identical twin 40.0% As the degree of relatedness increases, the number of gene in common increases. 3. The recurrence risk is increasing with the number of affected members in a family. For example: spina bifida If one siblings are affected, the risk to a subsequent sibling is approximately 4%. If two siblings are affected, the risk to a subsequent sibling is approximately 10%. Note This increase does not mean that the family’s risk has actually changed. Rather, it means that we now have more information about the family’s true risk: because they have had two affected children, they are probably located higher on the liability distribution than a family with only one affected child. In other words, they have more risk factors (genetic and/or environmental) and are more likely to produce an affected child. Threshold 阈值 Liability Low One couple have one affected child High Another couple have two affected child 4. The recurrence risk is increasing with the severity of affected members within a family For example, in cleft lip/palate If the proband has a unilateral cleft lip ,the risk of first-degree relatives is only 2%. If the proband has bilateral cleft lip and palate , the risk of first-degree relatives is 6%, The more severely affected the individual, the more genes he/she has to transmit, and the higher the recurrence risk. Example: cleft lip/palate Liability Low Threshold 阈值 High unilateral cleft lip (one side) bilateral cleft lip and palate (both sides) 5. The recurrence risk is higher if the proband is of the less commonly affected sex A lower male threshold implies that fewer disease-causing factors are required to generate the disorder in males. The recurrence risk is higher when the proband is female than when the proband is male. For example: Pyloric stenosis • An overgrowth of muscle at the juncture between the stomach and the small intestine. • The condition must be corrected surgically shortly after birth, or the newborn will be unable to digest foods. It occurs in about 0.05% newborn males but only in about 0.01% newborn females. The risk of recurrence to the offspring of male probands are 5.5% for sons and 2.4% for daughters, whereas the risks to the offspring of female probands are 19.4% for sons and 7.3% for daughters. The recurrence risk is higher for families in which the proband is female than where the proband is male. Two threshold diseases Example : Pyloric stenosis mean 0.05% 0.01 % low high The reason A female, being more rarely affected, is presumed to require a greater liability in order to cross the threshold. A couple having a daughter with pyloric stenosis, is likely to transmit a greater number of genes predisposing to the disorder and therefore has a higher recurrence risk than those who have a son with the disorder. Question How much of a given phenotype is genetic (inherited) and how much is environment? Heritability: H The proportion of the phenotypic variation for a particular trait that is due to genetic difference . If H is high --- phenotypic variation is largely genetic H= 1 (100%) - genes only If H is low --- phenotypic variation is largely environmental H= 0 (0%) - environment only Heritability of various disorders Disorder Schizophrenia Asthma Hypertension (essential) Type II diabetes (NIDDM) Cleft lip ± cleft palate Heritability (%) 85 80 62 26 76 Note: 1. Heritability measures the genetic contribution to a polygenic trait. 2. It is specific to a particular population at a particular time. (e.g. the heritability of skin color ) 3. Remember that heritability is a population phenomenon and applied to groups, not to individuals. 4. The greater the value for the heritability the greater the role of genetic factors!!! Winter Summer Two research strategies that are often used to estimate the relative influence of genes and environment 1.Twin studies 2. Adoption studies 1. Twins Studies Monozygotic twins (MZ twins, or identical ): are derived from a single zygote and therefore are genetically identical. Monozygotic twins, showing a striking similarity in physical appearance. Both twins developed myopia as teenagers. Dizygotic twins (DZ twins, or fraternal twins ): develop from 2 fertilized sperm. They share half their genes in common, as do any pair of siblings. If both members of a twin pair share a trait, they are said to be concordant. If they do not share the trait, they are discordant. For a trait determined completely by genes, MZ twins should always be concordant, and DZ twins should be concordant less often. •Concordance measures the frequency of expression of a trait in both members of MZ or DZ twin pairs. •For a trait largely determined by genes, concordance is higher for MZ than DZ twins. •A trait molded mostly by the environment exhibits similar concordance values for both types of twins. For example If one MZ twin has sickle cell disease, the other twin will also have sickle cell disease. (100%) GAG GTG hemoglobin-beta gene For example In contrast, when one MZ twin has type 1 diabetes mellitus, only about 40% of the other twins will also have type 1 diabeties. Greater concordance in MZ versus DZ twins is strong evidence of a genetic component to the disease. Formula for heritability (H) in twin studies H = (Monozygotic Concordance % - Dizygotic Concordance %) /(100 - Dizygotic Concordance %) For example: Schizophrenia 25 Monozygotic twins , 20 have the disease. concordance is 20/25. 20 Dizygotic twins , 2 have the disease, concordance is 2/20. Please calculated the heritability. H = CMZ – CDZ 80 – 10 =0.78=78% = 100 – CDZ 100 – 10 2. Adoption Studies Studies of adopted children are also used to estimate the genetic contribution to a multifactorial trait. They consist of comparing disease rates among the adopted offspring of affected parents with the rates among adopted offspring of unaffected parents. For example, schizophrenia is seen in 8% to 10% of adopted children whose natural parent had schizophrenia, whereas it is seen in only 1% of adopted children of unaffected parents. Some examples of polygenic disorders 1. Congenital malformations • Example: Cleft lip/palate, Neural tube defects 2. Acquired diseases of childhood and adult life • Example: Diabetes mellitus, Hypertension 1. Congenital Malformations Club foot Congenital heart defects Cleft lip/palate Clubfoot can range from mild to severe, but typically has the same general appearance. The foot is turned inward and there is often a deep crease on the bottom of the foot. Neural tube defect llustration of a child with spina bifida the most common NTD The normal structure of the heart (left) in comparison to two common locations for a ventricular septal defect (right), the most common form of congenital heart defect.[1] 2. Multifactorial Disorders in the Adult Population • Cardiovascular Disorders • Hypertension • Diabetes mellitus • Obesity • Alzheimer Disease • Alcoholism • Psychiatric Disorders Summary 1. The concept of polygenic inheritance has been proposed to account for the common congenital malformations and acquired disorders that show nonMendelian familial aggregation. These disorders are thought to result from the interaction of genetic and environmental factors. 2. Human characteristics such as height and intelligence, which show a normally distributed continuous distribution in the general population, are probably caused by the additive effects of many genes. Summary 3. According to the liability/threshold model for polygenic inheritance the population’s genetic and environmental susceptibility, which is known as liability, is normally distributed. Individuals are affected if their liability exceeds a threshold. 4. Risks for multifactorial diseases usually increase if more family members are affected, if the disease has more severe expression, and if the affected proband is a member of the less commonly affected sex. Summary 5. Recurrence risks decrease rapidly with more remote degrees of relationship. 6. In general, the sibling recurrence risk is approximately equal to the square root of the prevalence of the disease in the population. 7. Heritability is a measure of the proportion of the total variance of a character or disease that is due to the genetic variance.