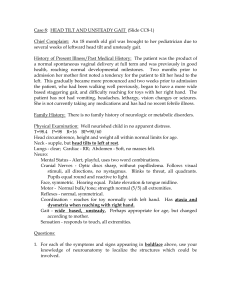
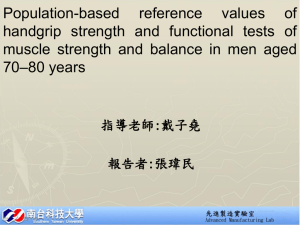
Geriatr Gerontol Int 2015; 15: 182–188 ORIGINAL ARTICLE: EPIDEMIOLOGY, CLINICAL PRACTICE AND HEALTH Effects of balance ability and handgrip height on kinematics of the gait, torso, and pelvis in elderly women using a four-wheeled walker Hyuk-Jae Choi,1 Chang-Yong Ko,1 Sungjae Kang,1 Jeicheong Ryu,1 Museong Mun1 and Hye-Seon Jeon2 1 Korea Orthopedics & Rehabilitation Engineering Center, Incheon, and 2Department of Physical Therapy, College of Health Science, Yonsei University, Wonju, Korea Aim: Numerous elderly individuals use the four-wheeled walker (FWW) as a gait-assistive device. The walker’s handgrip height is important for correct use. However, few clinical studies have investigated the biomechanical effects of the FWW’s handgrip height on balance. Therefore, the present study assessed kinematic features of the gait, torso and pelvis during use of the FWW at two levels of handgrip height (48% vs 55% of the subject’s height) while assessing balance in older adults. Methods: A total of 20 older adults were allocated into two groups according to the Berg Balance Scale (BBS): good balance (GB; BBS ≥46) versus poor balance (PB; BBS <45). Participants walked with the FWW at 48% or 55% handgrip height for 10 m. Results: Our study showed that the double-support period and stance phase significantly increased at 55% handgrip height, but the swing phase significantly decreased in the GB group. In the PB group, velocity and stride length significantly increased at 55% handgrip height. Tilt angle of the torso in the GB group was significantly lower at 55% than at 48% handgrip height, but no differences were observed in the PB group. In the pelvis, initial contact and toe-off angles of tilt were lower in the GB group at 55% handgrip height, but no differences were observed in the PB group. Conclusions: These results showed that kinematic features of the gait, torso, and pelvis in older adults using the FWW might be dependent on the handgrip height of the FWW and the patient’s balance. Additionally, greater than 48% of the body height might be appropriate for older adults with poor balance. Geriatr Gerontol Int 2015; 15: 182–188. Keywords: balance ability, Berg Balance Scale, four-wheeled walker, gait features, torso and pelvic kinematics. Introduction In the elderly, gait function and balance decline with age, leading to limited activities of daily living (ADL). Consequently, their quality of life is significantly reduced.1 Use of gait-assistive devices (GAD) extends the base of support and controls the range of motion around the center of mass.2 Furthermore, GAD can compensate for damaged motor control and weakness of the lower extremities in the elderly.3,4 Thus, gait stability, feeling of safety and confidence can be improved, leading to enhanced ADL, independence, gait and mobility-related tasks.4,5 Accepted for publication 21 December 2013. Correspondence: Dr Chang-Yong Ko PhD, Korea Orthopedics & Rehabilitation Engineering Center, Bupyeong, Incheon 403-712, Korea. Email: monamicyko@gmail.com 182 | doi: 10.1111/ggi.12246 Several studies have attempted to verify the biomechanical effects of GAD on gait. Cetin et al. compared two types of walkers, front-wheel versus fixed-frame, and showed less energy consumption with the use of front-wheel walkers.6 Probst et al. showed improvement in walking distance in patients with chronic obstructive pulmonary disease through enhanced ventilator capacity and/or walking efficiency.7 Protas et al. evaluated temporal and spatial parameters of gait and energy consumption in elderly participants using the WalkAbout, which was developed to prevent falls in the elderly and disabled.8 With the WalkAbout, the patient can sit down on a safety seat while walking. That study showed positive effects in oxygen demands while walking, but no effects on gait. Bryant et al. showed a decrease in stride length during WalkAbout walking, but no changes in walking distance and oxygen uptake.9 Evaluating kinematics of the torso and pelvis is important to assess postural stability and pathomechanics of © 2014 Japan Geriatrics Society Gait features using four-wheeled-walker the low back and hip.10–12 Therefore, it is required to analyze not only temporal and spatial parameters of gait kinematics, but also joint motion to improve the understanding of the biomechanical effects of the FWW. However, most of the prior biomechanical studies have focused on temporal and spatial parameters of gait.9,13,14 Furthermore, elderly individuals show diverse balance abilities; however, previous studies have not addressed this issue. In addition, previous studies have shown that the handgrip height of GAD was one of the most important criteria to enable appropriate use. Incorrect use of GAD causes serious problems, such as falls1–3 and excessive muscle force.15 Van Hook et al. stated that the flexion angle of the patient’s elbow should be 15–30° while the GAD is in contact with the floor and the patient is wearing shoes.3 The flexion angle corresponds to the distance between the floor and the patient’s greater trochanter, or with the wrist crease of the arm relaxed at his/her side.3 Furthermore, Takanokura calculated that the critical height of the handgrips should be 48% of the patient’s body height through mathematical modeling.15 However, few clinical studies have investigated gait kinematics at varying handgrip heights. Therefore, the aim of the present study was to evaluate 3-D gait parameters in older adults using the FWW considering their balance ability and handgrip heights, and simultaneously to evaluate kinematics of the torso and pelvis during FWW use. Additionally, we suggested criteria for use of the FWW Methods Participants A total of 20 elderly women (age 77.9 ± 5.9 years, height 149.3 ± 4.3 cm, weight 56.0 ± 9.9 kg) were recruited in the present study. All participants had scores of more than 24 on the Mini-Mental State Examination. The participants had no history of serious surgery, including brain surgery, and orthopedics disease or musculoskeletal disorder, and had less than 4 points (<4) on the visual analog scale scores for back and limb pain, which corresponds to no pain or mild pain.16 Before the experiment, the Berg Balance Scale (BBS) was administered to the participants. Based on their scores, they were allocated into two groups: good balance (GB; scores ≥46; n = 10) and poor balance (PB; scores <46; n = 10).17 The height (150.8 ± 3.0 cm) and weight (54.4 ± 9.7 kg) in the GB group were not different from those (147.7 ± 5.1 cm, 57.7 ± 10.3 kg) in the PB group. We notified participants regarding the purpose and procedures of the present study. All procedures were carried out according to a protocol approved by the institutional review board in the Korea Orthopedics & Rehabilitation Engineering Center. © 2014 Japan Geriatrics Society Four-wheeled walker The FWW used in the present study was the V4208 (Jinsan Medical, Seoul, Korea), which is made of aluminium steel. This FWW featured adjustable heights from 69 to 98 cm (seat height, 47 cm; weight, 7 kg). In addition, the maximum load for the seat was 100 kg. 3-D temporal and spatial parameters of FWW walking A 3-D motion analysis system with eight infrared cameras (Eagle 4; Motion Analysis, Santa Rosa, CA, USA) was used to carry out 3-D gait analyses. To capture these data, we used 19 10-mm reflective Helen Hayes markers. A wand was used to place markers on the following anatomical landmarks of both limbs: sacrum, anterior superior iliac spine (bilaterally), lateral femoral epicondyle (bilaterally), calcaneus and malleo- lus (bilaterally), metatarsal head (bilaterally), and the lower lateral one-third surface of both shins and thighs (bilaterally). Kinematic data from all the markers were sampled at 120 Hz using real-time software (EvaRT 5.0.4; Motion Analysis). The data on each marker were smoothed by Butterworth filters at 6 Hz using gait analysis software (Orthotrak 6.5; Motion Analysis).18,19 Gait cycle ranging from heel-strike to toe-off was identified by frame analysis and normalized from 0% to 100%. The participants practiced FWW walking for approximately 10 min to familiarize themselves with the FWW. The participants were tested barefoot in a static position, and then walked with the FWW at a self-selected walking speed along a 10-m walkway.18 At that time, handgrip height was set as 48% or 55% of the participant’s body height. Before these tests, the participants walked without the FWW at a self-selected walking speed along a 10-m walkway to evaluate whether there were differences in gait parameters between the GB and PB groups. The mean values of the following spatiotemporal kinematic parameters were calculated: cadence, velocity, stride length, step width, double support (% of gait cycle), stand phase (% of gait cycle) and swing phase (% of gait cycle). In addition, to assess the torso and pelvic motion, their respective angular parameters were calculated according to previous studies.10,20 The following angular parameters were used: initial contact and toe-off angles at tilt and rotation, initial downward, toe-off, and maximum upward at obliquity. Statistical analysis A one-way t-test was carried out to compare the participants’ anthropometry. To compare spatial and temporal gait parameters, and angular parameters of the torso and | 183 H-J Choi et al. Table 1 Spatial and temporal gait parameters by balance ability during a gait without the four-wheeled walker Parameters GB PB Cadence (steps/min) Velocity (cm/s) Stride length (cm) Step width (cm) Double support (%) Stance phase (%) Swing phase (%) 106.3 ± 18.9 84.2 ± 26.1 93.4 ± 3.6 12.0 ± 3.6 20.9 ± 3.6 60.5 ± 1.8 39.5 ± 1.8 101.7 ± 7.3 43.8 ± 11.4 87.5 ± 11.7 10.7 ± 2.9 21.9 ± 2.7 61.0 ± 1.3 39.0 ± 1.3 Data on handgrip height group presented as mean ± SE. FWW, four-wheeled walker; GB, good balance group; PB, poor balance group. pelvis at 48% and 55% handgrip heights, paired t-tests were carried out in each group using SPSS 20.0 (Statistical Package for the Social Sciences, Chicago, IL, USA). The significance level was set at 0.05. Results Comparisons of spatiotemporal gait parameters There were no significant differences in any spatiotemporal gait parameters between the GB and PB groups during normal gait without the FWW (Table 1; P > 0.05). Changes in spatiotemporal gait parameters are shown in Table 2. In the GB group, double-support period and stance phase significantly increased at 55% handgrip heights (P < 0.05 and P < 0.05, respectively), but swing phase significantly decreased (P < 0.05). However, there were no changes in cadence, velocity, stride length and step width between the two groups (all P > 0.05, respectively). In the PB group, velocity and stride length significantly increased at 55% handgrip height (P < 0.05 and P < 0.05, respectively). However, there were no changes in cadence, step width, double-support period, and stance and swing phases between heights (all P > 0.05, respectively). For the anterior–posterior tilt angle of the torso, the gait-cycle pattern is shown in Figure 1. The tilt-angle parameters of the torso are shown in Table 3. All of the tilt-angle parameters in the GB group were significantly lower with handgrip heights of 55% than handgrip heights of 48% (all P < 0.05, respectively). However, there were no differences between 48% and 55% handgrip heights in the PB group. Nevertheless, the gaitcycle patterns were similar in both the GB and PB groups regardless of handgrip heights (Fig. 1). The pat- terns shifted to a lower degree in 55% handgrip heights when compared with 48% height. 184 | For pelvic motion, the gait-cycle pattern is shown in Figure 2. The angle-kinematic parameters of pelvic motion are shown in Table 4. The gait-cycle patterns were similar in both the GB and PB groups regardless of the handgrip heights. The patterns for tilt shifted to a lower degree in the 55% handgrip height when compared with the 48% height. In contrast, the patterns for obliquity and rotation shifted to a higher degree in the 55% height when compared with the 48% height. For tilt, initial contact and toe-off angles in the GB group were significantly lower for the 55% handgrip height than for the 48% height (all P < 0.05). However, there were no changes in the PB group (all P > 0.05). For obliquity, most of the angles in the GB and PB groups were not significantly different between the 48% and 55% handgrip heights (all P > 0.05), except for an increase in the toe-off angle in the GB group at 55% handgrip height (P < 0.05). Discussion In the GB group, the double-support period and stand phase increased, and swing phase decreased at 55% handgrip height compared with 48% height. Fear of falling affects gait parameters in older adults, particularly resulting in a prolonged double-support period, slowgait velocity and short stride length.21 Therefore, we suggest that elderly women with good balance might fear falling, which is not reflected in fall risk,22 when walking with a FWW at excessive handgrip heights.21 However, velocity and stride length in the PB group decreased with FWW handgrip height at 48%, suggesting that older adults with PB have a greater fear of falling with a 48% handgrip height than with a 55% handgrip height.4,22 Therefore, the present results suggest that handgrip heights greater than 48% (the recommended handgrip height) are appropriate in patients with poor balance. However, the changes in velocity and stride length seemed small. A future study might be required to evaluate whether these changes are clinically meaningful. The findings of the present study are inconsistent with those of previous studies. However, this inconsistency might be due to our study sample, which consisted of participants who were not true users of the FWW. Liu showed differences in gait parameters between those who used a walker (true user) and those who did not (potential user).4 Nevertheless, the present study suggested that adequate handgrip height might be dependent on the patient’s balance abilities, despite requirement of further studies to confirm this postulation. The present study also found that the tilt angle of the torso increased by 48% in the GB group. Furthermore, the gait-cycle patterns shifted to a lower degree at 55% handgrip height compared with 48% height. These results suggest that compared with the 55% handgrip © 2014 Japan Geriatrics Society Gait features using four-wheeled-walker Table 2 Spatial and temporal gait parameters by balance ability and four-wheeled walker handgrip height in elderly women Parameters Groupc 48% 55% P-value Cadence (steps/min) GB PB GB PB GB PB GB PB GB PB GB PB GB PB 93.20 ± 5.52 90.04 ± 2.26 75.85 ± 6.38 70.94 ± 2.83 96.74 ± 3.82 94.69 ± 2.83 8.51 ± 1.39 8.89 ± 1.50 21.29 ± 1.46 21.00 ± 0.84 60.64 ± 0.73 60.50 ± 0.42 39.36 ± 0.73 39.50 ± 0.42 93.78 ± 4.73 91.60 ± 2.59 74.51 ± 5.70 74.65 ± 3.17 94.32 ± 3.65 97.68 ± 3.20 8.89 ± 1.50 8.29 ± 0.91 22.82 ± 1.67 20.78 ± 0.91 61.41 ± 0.83 60.39 ± 0.46 38.59 ± 0.83 39.61 ± 0.46 0.362 0.095 0.255 0.020* 0.088 0.030* 0.264 0.456 0.046* 0.348 0.046* 0.348 0.046* 0.348 Velocity (cm/s) Stride length (cm) Step width (cm) Double support (%) Stance phase (%) Swing phase (%) *P < 0.05. Data on handgrip height group presented as mean ± SE. FWW, four-wheeled walker; GB, good balance group; PB, poor balance group. Figure 1 Gait-cycle pattern for anterior–posterior tilting angle of the torso in (a) the good balance (GB) group and (b) poor balance (PB) group. height, the 48% handgrip height causes a stooped posture in older adults with good balance. A stooped posture can lead to incorrect user position behind the handgrips but not between the handholds.12 Addition© 2014 Japan Geriatrics Society ally, the user might excessively lean on the FWW, and then the front wheels might be raised, resulting in slipping of the FWW during FWW gait. Therefore, gait with the FWW at the 48% handgrip height in older adults with good balance might increase the risk for falls. Although there were no differences between 48% and 55% handgrip heights in the PB group, the gait-cycle patterns shifted to a lower degree in the 55% handgrip height when compared with the 48% height. Hence, elderly participants, regardless of balance ability, attempted to maintain an upright position. In addition, the tilt in the PB group tended to be higher than that in the GB group, suggesting that older adults with poor balance carried their upper body more forward and walked in a stooped posture. Furthermore, the older adults in the PB group had poorer visibility while using the FWW, causing excessive loads to be transferred onto the FWW.15 Furthermore, tilt of the torso might be dependent on not only handgrip height of the FWW, but also balance. In both the GB and PB groups, the patterns of pelvic motion were similar regardless of handgrip heights. The patterns of pelvic tilt shifted to a lower degree with the higher handgrip height. Furthermore, the initial contact and toe-off angles in the GB group significantly decreased at 55% handgrip height compared with the 48% height; however, there were no changes in the PB group. These results corresponded to the tilt of the torso in both the GB and PB groups. Compared with a 55% handgrip height, a 48% handgrip height might cause a stooped posture in older adults with good balance, whereas there are no alterations in the posture in older adults with poor balance. In addition, patterns of pelvic obliquity and rotation shifted to a higher | 185 H-J Choi et al. Table 3 tilting Angle kinematic parameters of the torso’s anterior-posterior Cycle Group 48% 55% P-value Initial contact (°) GB PB GB PB 10.26 ± 1.50 13.49 ± 1.89 12.73 ± 1.64 16.17 ± 1.95 7.17 ± 1.18 11.92 ± 2.28 9.10 ± 1.65 14.40 ± 2.40 0.000* 0.096 0.000* 0.103 Maximum upward (°) *P < 0.05, 48% versus 55%. Handgrip height data presented as mean ± SE. GB, good balance group; PB, poor balance group. Figure 2 Gait-cycle pattern for pelvic motion, (a,b) anterior-posterior tilt, (c,d) obliquity and (e,f) rotation. (a,c,e) Good balance group. (b,d,f) Poor balance group. degree in higher handgrip heights. Most of the angles in the GB and PB groups were not changed, except for an increase in toe-off angle in the GB group at a 55% height. Crosbie showed that gait and joint kinematics features might be determined by the walking frame, rather than the user’s physiological status.23 Therefore, the results of pelvic kinematics in the present study (changes in pelvic tilt, but minimal changes in obliquity and rotation of the pelvis) might be attributable to the FWW used with variations only in the handgrip height, but not in the other dimensions. Hence, only pelvic tilt might be affected by the user’s balance. Furthermore, no differences were found in the anthropometry 186 | between the PB and GB groups. These results suggest that gait, torso and pelvic kinematics were dependent on the patients balance while using the FWW. The present study had some limitations. All participants of this study were potential FWW users. Therefore, future studies should include true FWW users to determine optimal FWW handgrip height. Additionally, only two levels of the handgrip height were investigated. Future studies should investigate additional handgrip heights, greater and lesser than the recommended 48% handgrip height level. In the present study, we did not directly evaluate fear of falling during FWW gait. Therefore, future studies should assess this fear by using, for © 2014 Japan Geriatrics Society Gait features using four-wheeled-walker Table 4 Angle kinematic parameters of pelvic motion Motion Cycle Group 48% 55% P-value Tilt Initial contact (°) GB PB GB PB GB PB GB PB GB PB GB PB GB PB GB PB 10.76 ± 1.72 10.64 ± 2.48 10.80 ± 1.52 10.40 ± 2.73 −1.70 ± 0.47 −2.30 ± 1.45 −3.51 ± 0.41 −3.91 ± 1.37 0.89 ± 0.59 −0.39 ± 1.27 1.59 ± 0.60 0.12 ± 1.29 0.59 ± 1.10 0.94 ± 1.04 −5.36 ± 1.42 −5.14 ± 1.20 9.47 ± 1.88 10.07 ± 2.99 9.67 ± 1.77 9.56 ± 3.19 −1.63 ± 0.61 −1.88 ± 1.05 −3.39 ± 0.52 −3.85 ± 0.94 1.30 ± 0.59 −0.02 ± 0.81 1.96 ± 0.63 0.56 ± 0.81 0.97 ± 1.06 1.86 ± 0.73 −4.44 ± 1.40 −4.68 ± 1.05 0.006* 0.272 0.031* 0.210 0.407 0.271 0.299 0.465 0.011* 0.311 0.111 0.272 0.184 0.048* 0.071 0.348 Toe-off (°) Obliquity Initial contact (°) Maximum downward (°) Toe-off (°) Maximum upward (°) Rotation Initial contact (°) Toe-off (°) *P < 0.05, 48% versus 55% (P < 0.05). Handgrip height data presented as mean ± SE. GB, good balance group; PB, poor balance group. example, the Modified Falls Efficacy Scale, if our result regarding fear of falling is true.21 In summary, gait, torso, and pelvic kinematics with use of the FWW might be dependent on handgrip height and the older adult’s balance. Therefore, the older adult’s balance should be considered when design- ing and developing criteria for use of the FWW. Specifically, a handgrip height greater than 48% of the older adult’s height with poor balance. In addition, the optimal height of the handgrip might depend on the older adult’s balance ability. Acknowledgment This research was financially supported by Chungcheonbuk-do Provincial Government through the Research and Development for Regional-based Promotion (no. 12167361) Disclosure statement The authors declare no conflict of interest. References 1 O’Hare MP, Pryde SJ, Gracey JH. A systematic review of the evidence for the provision of walking frames for older people. Phys Ther Rev 2013; 18: 11–23. 2 Liu HH. Assessment of rolling walkers used by older adults in senior living communities. Geriatr Gerontol Int 2009; 9: 124–130. 3 Van Hook FW, Demonbreun D, Weiss BD. Ambulatory devices for chronic gait disorders in the elderly. Am Fam Physician 2003; 67: 1717–1724. © 2014 Japan Geriatrics Society 4 Liu HH, McGee M, Wang W, Persson M. Comparison of gait characteristics between older rolling walker users and older potential walker users. Arch Gerontol Geriatr 2009; 48: 276–280. 5 Mann WC, Hurren D, Tomita M, Charvat B. An analysis of problems with walkers encountered by elderly persons. Phys Occup Ther Geriatr 1995; 13: 1–23. 6 Cetin E, Muzembo J, Pardessus V, Puisieux F, Thevenon A. Impact of different types of walking aids on the physiological energy cost during gait for elderly individuals with several pathologies and dependent on a technical aid for walking. Ann Phys Rehabil Med 2010; 53: 399– 405. 7 Probst VS, Troosters T, Coosemans I et al. Mechanisms of improvement in exercise capacity using a rollator in patients with COPD. CHEST J 2004; 126: 1102–1107. 8 Wolfe RR, Jordan D, Wolfe ML. The WalkAbout: a new solution for preventing falls in the elderly and disabled. Arch Phys Med Rehabil 2004; 85: 2067–2069. 9 Bryant MS, Rintala DH, Lai EC, Raines ML, Protas EJ. Evaluation of a new device to prevent falls in persons with Parkinson’s disease. Disabil Rehabil Assist Technol 2009; 4: 357–363. 10 Chockalingam N, Chatterley F, Healy AC, Greenhalgh A, Branthwaite HR. Comparison of pelvic complex kinematics during treadmill and overground walking. Arch Phys Med Rehabil 2012; 93: 2302–2308. 11 Vogt L, Pfeifer K, Portscher M, Banzer W. Lumbar corsets: their effect on three-dimensional kinematics of the pelvis. J Rehabil Res Dev 2000; 37: 495–500. 12 van Riel KMM, Hartholt KA, Panneman MJM, Patka P, van Beeck EF, van der Cammen TJM. Four-wheeled walker related injuries in older adults in the Netherlands. Inj Prev 2007. doi: 10.1136/injuryprev-2012-040593 13 Protas EJ, Raines ML, Tissier S. Comparison of spatiotemporal and energy cost of the use of 3 different walkers and unassisted walking in older adults. Arch Phys Med Rehabil 2007; 88: 768–773. 14 Choi H. Erector Spinae Muscle Activity and Characteristics of Gait With Different Grip Height of Four-Wheeled | 187 H-J Choi et al. 15 16 17 18 19 Walker. MS Thesis, Ergonomic Therapy, Yonsei University, Seoul, 2012. Takanokura M. Optimal handgrip height of four-wheeled walker on various road conditions to reduce muscular load for elderly users with steady walking. J Biomech 2010; 43: 843–848. Jensen MP, Smith DG, Ehde DM, Robinsin LR. Pain site and the effects of amputation pain: further clarification of the meaning of mild, moderate, and severe pain. Pain 2001; 91: 317–322. Berg K, Wood-Dauphinee S, Williams J, Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health 1992; 83: S7–11. Chang YH, Bae TS, Kim SK, Mun MS, Lee W-H. Intact hip and knee joint moment in coronal plane with unilateral transfemoral amputee. Int J Precision Eng Manuf 2011; 12: 129–134. Chang YH, Bae TS, Kim SK, Kim SB, Mun MS, Lee WH. Relationship between ankle inversion angle and 188 | 20 21 22 23 knee adduction moment on the intact limb in unilateral transfemoral amputees during walking. Int J Precision Eng Manuf 2012; 13: 609–615. Schache AG, Blanch PD, Rath DA, Wrigley TV, Starr R, Bennell KL. A comparison of overground and treadmill running for measuring the three-dimensional kinematics of the lumbo-pelvic-hip complex. Clin Biomech 2001; 16: 667–680. Chamberlin ME, Fulwider BD, Sanders SL, Medeiros JM. Does fear of falling influence spatial and temporal gait parameters in elderly persons beyond changes associated with normal aging? J Gerontol A Biol Sci Med Sci 2005; 60: 1163– 1167. Maki BE. Gait changes in older adults: predictors of falls or indicators of fear. J Am Geriatr Soc 1997; 45: 313– 320. Crosbie J. Comparative kinematics of two walking frame gaits. J Orthop Sports Phys Ther 1994; 20: 186–192. © 2014 Japan Geriatrics Society Copyright of Geriatrics & Gerontology International is the property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.