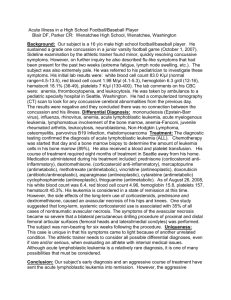
CLINICAL PATHOLOGY CASE 1 CASE SUMMARY HISTORY • Age: 5 years • Sex: male SIGNS AND SYMPTOMS • Nasal congestion • Cough • Constant headache • Osteodynia • Easy bruising PHYSICAL EXAMINATION • Swollen lymph nodes Region: axillary, cervical and submandibullar region • Splenomegaly • Hepatomegaly • Hematoma Region: trunks and limbs DIFFERENTIAL DIAGNOSIS • • • • • Hairy Cell Leukemia Acute Myeloid Leukemia Acute Lymphoblastic Leukemia Tuberculosis Malaria HAIRY CELL LEUKEMIA RULE IN RULE OUT Splenomegaly swollen lymph node bruising osteodynia hepatomegaly Other symptoms does not match Histology section depicts otherwise There is no detailed history of patient Age doesn’t meet the range ( 55 years) ACUTE MYELOID LEUKEMIA Rule in Rule Out Easy bruising Histology finding depicts otherwise Headache Hepatomegaly splenomegaly Does not fall under the average age (patient is 5 years of age) osteodynia ACUTE LYMPHOBLASTIC LEUKEMIA Rule in Common in young children Constant headache Osteodynia Easy bruising Splenomegaly Hepatomegaly Swollen lymph node Cough Nasal congestion Rule out No detailed history of patient. TUBERCULOSIS RULE IN Cough Hepatosplenomegaly Erythema nodosum Lymphadenopathy RULE OUT Not enough patient history is taken Other symptoms do not match Age MALARIA Rule In Rule Out Age group Malaria caused by mosquitoes Dry cough Mostly affects RBC Hepatosplenomegaly Doesn’t affect much in lymphocyte, monocyte increases. Other symptoms common MAIN DIAGNOSIS ACUTE LYMPHOBLASTIC LEUKEMIA • Acute Lymphoblastic Leukemia is a type of cancer whereby too many immature lymphocytes are made by the bone marrow. • It is a cancer affecting white blood cells and bone marrow. The affected cells at this case are lymphocytes thus giving the name lymphoblastic. • ALL has been rated as one of the most common cancer disease in children younger than 15 years. RISK FACTORS • • • • • Exposure to benzene and radiation Conditions caused by genetic factors Viruses Overweight or obesity Weakened immune system SIGNS AND SYMPTOMS • • • • • • • • • • • • • Fever Cough Easy bruising Headache Swollen lymph nodes Sweating Bone pain Weight loss Fatigue Petechiae Splenomegaly Hepatomegaly Hematoma CONFIRMATION OF DIAGNOSIS • • • • • • • • Physical and Abdominal Examination Complete blood count Peripheral blood smear Blood chemistry and coagulation test Bone marrow Tests: Aspiration and Biopsy Cytochemistry Flow cytometry immunohistochemistry • Cytogenetics • Fluorescent in situ hybridization (FISH) • Polymerase Chain Reaction (PCR) • Lumbar puncture • Lymph node biopsy Imaging Tests: • Computed Tomography Scan • Magnetic Resonance Imaging Scan • X Rays • Ultrasound • Bone Scan DISCUSSION WHY ACUTE LYMPHOBLASTIC LEUKEMIA ? • ALL has been chosen as the confirmed diagnosis of the case because mainly all the symptoms , and histological findings match those of Acute Lymphoblastic Leukemia. • Age is also one of the factors which rules in for the diagnosis Five year old boy • Acute lymphoblastic leukemia happens in the age group of people younger than 15 years, thus age has been chosen as a factor to rule in for the diagnosis. • Nasal congestion- membrane lining in the nose becomes swollen from inflamed blood vessels. • Cough- can be due to enlarged thymus. • Constant headache- shortages of normal blood cells, and can be due to if ALL is spread to the brain by lymph nodes. • Osteodynia- aka bone pain, caused by the spread of blasts cells to the surface of the bone or into the point from the marrow cavity. • Easy bruising- shortages of normal blood cells. Also by blood vessels under the skin being damaged. Platelet levels are low. • Swollen lymph nodes – Lymphoblasts build up in the bone marrow and may spread to other sites in body. Accumulation of leukemia cells • Splenomegaly/Hepatomegaly- accumulation of leukemia cells. Also by pressure on splenic veins. • Hematoma- can be presented as lumps which is caused by the limitation of the blood to a sac Region: trunks and limbs • Weight loss- Abdominal pain, so the patient doesn’t have desire to eat, therefore weight decreases. • Sweating- can be due to body trying to fight the disease. • Petechiae- are tiny red spots or lines in the skin due to low platelet levels. The histological slide shows lymphocytes that has scant agranular cytoplasm, small nucleoli and condensed nuclear chromatin which matches to be distinctive histologic features of lymphocyte in acute lymphoblastic leukemia MANAGEMENT • Stem Cell Transplant • Chemotherapy: 3 phases -Induction -Consolidation -Maintenance PROGNOSIS • Mean survival rate: 5 year –90% REFERENCES • De Kouchkovsky, I. and Abdul-Hay, M. (2016). ‘Acute myeloid leukemia: a comprehensive review and 2016 update’. Blood Cancer Journal, 6(7), pp.e441-e441. • Kotepui, M., Phunphuech, B., Phiwklam, N., Chupeerach, C. and Duangmano, S. (2014). Effect of malarial infection on haematological parameters in population near Thailand-Myanmar border. Malaria Journal, 13(1), p.218. • Kumar.V;Abbas. A; Aster.J: RobbinandCotrans: Pathologic Basis of Disease, 9th edition, Elsevier Saunders, (2015), pg 592– 604 • Lowenberg, B. and Rowe, J. (2015). Introduction to the review series on advances in acute myeloid leukemia (AML). Blood, 127(1), pp.1-1. • Marais, B. (2014). Tuberculosis in children. Journal of Paediatrics and Child Health, 50(10), pp.759-767. • Ramesh, V., Venkata, N. and Sankar, J. (2017). Mixed malarial infection with pancytopenia in a child with acute lymphoblastic leukemia: An unusual presentation. Indian Journal of Medical and Paediatric Oncology, 38(1), p.92. • Saultz, J. and Garzon, R. (2016). Acute Myeloid Leukemia: A Concise Review. Journal of Clinical Medicine, 5(3), p.33. • Terwilliger, T. and Abdul-Hay, M. (2017). Acute lymphoblastic leukemia: a comprehensive review and 2017 update. Blood Cancer Journal, 7(6), p.e577. • Torpy, J. (2014). Acute Lymphoblastic Leukemia. JAMA, 301(4), p.452. • Troussard, X. and Cornet, E. (2017). Hairy cell leukemia 2018: Update on diagnosis, risk-stratification, and treatment. American Journal of Hematology, 92(12), pp.1382-1390. • • MANAGEMENT -STEM CELL TRANSPLANT • • • • • -CHEMOTHERAPY usually in 3 phases: Induction Consolidation Maintenance Induction treatment • SR/IR induction: Prednisolone tablets • HR induction : dexamethasone • Vincristine: IV weekly • doxorubicin: 2 doses IV on the 1st and 22nd day. • PEG-asparaginase: 1 dose of IM towards the finishing of induction treatment. • • • • • • • • • • • • • • • • • • • • • High risk Block A Day 1: triple intrathecal Day 1-5 : cyclophosphamide 440 mg/m2 etoposide 100 mg/m2 Day 6: PEG asparaginase Block B dexamethasone + mercaptopurine: orally, day 3 and 8: vincristine day 3: 5 g-MTX day 7 and 8:2 doses of cytarabine 2 g/m2 day 4: triple intrathecal day 8: PEG asparaginase Block C Day 1: triple intrathecal Day 2 and 6:fludarabine 30 mg/m² cytarabine 2g/m² days Day 2 and 4 :idarubicin 8 mg/m² Day 7: PEG-asparaginase • • • • • • Consolidation Standard and intermediate risk Mercaptopurine tablets: oral vincristine: 2 doses IV PEG asparaginase: 4 doses at a fortnightly interval With all high-dose methotrexate courses, Intrathecal methotrexate is given Delayed intensity Standard and intermediate risk • Dexamethasone tablets orally during 1st and 3rd week with a break during the 2nd week and a taper during the 4th week. • methotrexate: 2 doses intrathecal • vincristine: 4 injections weekly • PEG asparaginase injection: IM every second week ( 4 times) • Daunorubicin: infusion weekly (4 times) • Cyclophosphamide 1 g/m2 starting on 4th week. 6 thioguanine tablets given by oral administration. • Low dose cytarabine injections daily x 4 days during 4th and 5th week • Thioguanine : for 2 weeks from week 4 given orally on a daily basis. Maintenance • If leukemia remains in remission after induction and consolidation phase, maintenance therapy can begin. • Most treatment plans use daily 6- mercaptopurine and weekly methotrexate, given as pills, along with vincristine which is given intravenously and a steroid, usually prednisone or dexamethasone. Other drugs may be added depending on the type of ALL and risk of reoccurring. Treatment plans during the first few months of maintenance phase include one or two repeat intensified treatments which is similar to the initial induction. These four weeks of intensifications are often called re- induction or delayed intensification. • The total length of therapy (induction, consolidation and maintenance) for Acute Lymphoblastic Leukemia treatment plans is two to three years. • Treatment plans may change if leukemia does not go into remission during induction and consolidation phase. Child’s bone marrow may be checked properly soon after the treatment starts to observe if the leukemia is going away. If not, treatment may be intense and prolonged.