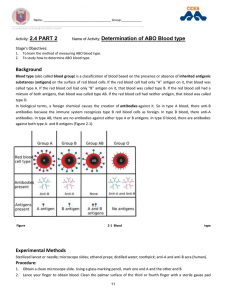
Practical physiology Blood types and cross matching By Dr. Sadat A. Aziz Blood Types: Blood types are the hereditary presence or absence of antigens on RBCs. The antigens are glycoproteins and glycolipids-membrane proteins and phospholipids with short carbohydrate chains bonded to them. The most common blood types are: 1. The ABO blood group 2. The Rh blood group Note/ The ABO blood type and the Rh blood type are usually expressed together. For example, a person designated as type A in ABO system and Rh positive, is said to be A-positive. • The ABO blood group: This system is used to categorise blood basis on the presence or absence of two antigens (A and B antigens) on RBCs. The letters A and B represent antigens • Basis on this, blood can be classified into A, B, AB, and O types. • Type A blood has the A antigen. • Type B blood has the B antigen. • Type AB means that both A and B antigens are present. • Type O means that neither the A nor the B antigen is present. • Normally, antibodies for those antigens not present on the surface of the circulating RBCs. • Instead, type A has anti-B antibodies in the plasma. • type B has anti-A antibodies. • type AB has neither anti-A nor anti-B antibodies. • and type O has both anti-A and anti-B antibodies. The Rh Group: • The Rh blood group is named for the rhesus monkey, in which the Rh antigens were discovered in 1940 • People are Rh-positive if they have certain Rh-antigens on the surface of their RBCs and they are Rh-negative if they don’t have these Rh-antigens. • In contrast to the ABO group, anti-D antibodies are not normally present in the blood. They form only in Rh- individuals who are exposed to Rh+ blood. • Type O blood (especially, O-negative) is a “universal donor” because type O RBCs have neither the A nor the B antigens to react with whatever antibodies the recipient may have. • Type AB is sometimes called the universal recipient because this blood type lacks both anti- A and anti-B antibodies. • Note/If possible, a person should receive blood of his or her own type; only if this type is not available should type O negative blood be given. • Type and crossmatch: To prevent transfusion reaction, blood must be typed. Blood typing determines the ABO and Rh blood groups of a blood sample. • Transfusion reaction: that can be seen in the blood of a recipient as a result of mismatching that may lead to 1. RBCs clump formation (agglutination) and hemolysis. 2. The released hemoglobin into the blood may clog the capillaries of the kidneys and lead to renal damage or renal failure. Blood typing and cross matching test: A blood type can be determined by mixing one drop of blood in a pool of anti-A or anti-B or anti-D serum a. Type A or B agglutinates only in the corresponding antiserum b. Blood type AB exhibits conspicuous agglutination in both anti-A and B sera c. Type O does not agglutinate in either one d. Rh-positive agglutinate after adding anti-D sera e. While Rh-negative does not agglutinate • Disorders associated with Rh blood group: • If Rh- person receives Rh+ transfusion, the recipient produces anti-D which presents little danger in the first mismatched transfusion. But in the second blood transfusion (Rh- positive), the already formed anti-bodies could agglutinate the donor’s RBCs. • Hemolytic disease of the newborn (HDN), or erythroblastosis fetalis: If Rh- woman carries Rh+ fetus, the first pregnancy is likely to be uneventful because the placenta normally prevents maternal and fetal blood from mixing. However, at the time of birth, or miscarriage, some of the fetal blood may leak through damaged placenta that exposes the mother to Rh+ fetal blood, and induces anti-D antibodies. At the next pregnancy with an Rh+ fetus, her anti-D antibodies may pass through the placenta and agglutinate the fetal erythrocytes which leads to a condition these conditions. Hemolytic disease of the newborn (HDN), or erythroblastosis fetalis: 1. like so many other disorders, is easier to be prevent than to treat. 2. If an Rh-negative woman gives birth to (or miscarries) an Rh-positive child, she can be given an Rh immune globulin (RhoGAM and Gamulin). The immune globulin binds fetal RBC antigens so they cannot stimulate her immune system to produce anti-D. Note/ It is now common to give immune globulin at 28 to 32 weeks’ gestation or at first 72 hours after birth in any pregnancy in which the mother is Rh-negative and the father is Rhpositive.