Flexor Tendon Injuries: Diagnosis, Repair & Post-Op Care
advertisement

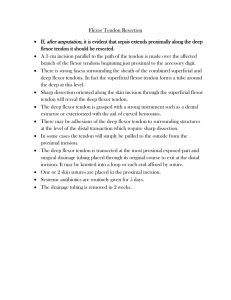
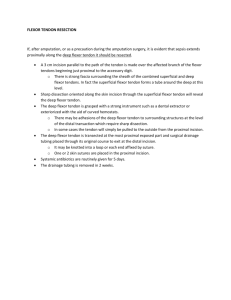
Flexor tendon injuries DR.M.M.Basumbuko (Medical intern) Department of Surgery and Orthopaedics Outline Definition Anatomy Classification Examination Examination of flexor tendons and identifying injuries Tendon repair Post operative care Conclusion Tendon-a flexible but inelastic cord of strong fibrous collagen tissue attaching a muscle to a bone.(70% collagen) used for movement. Anatomy FDP: Origin; antero-medial ulna, IOmembrane FDS: Origin; 2 heads. radius and ulnar heads Divided into muscle belly in mid forearm Insertion FDS divided into two slips, wrapping around FDP,reunite at Camper’s chiasma Continues to insert along the proximal half of the middle phalynx FDP passes through chiasma to insert at proximal base of distal phalynx Zones of flexor tendons in hand Sheaths Visceral and parietal synovial layers encloses the tendons Pulleys; A2 and A4 arise from periosteum of proximal and middle phalynx Examination of injured flexors Careful examination of the neurovascular status of the hand precedes the evaluation of tendon function. Even when gross deformity is absent, the posture of the hand often provides clues as to which flexor tendons are severed. When both flexor tendons of a finger are severed, the finger lies in an unnatural position of hyperextension,especially compared with uninjured fingers. Examination Flexor tendon injuries can be tentatively confirmed by several passive manoeuvres; Passive extension of the wrist does not produce the normal flexion of the fingers. If the wrist is flexed, even greater unopposed extension of the affected finger is produced. Gentle compression of the forearm muscle mass at times shows concomitant flexion of the joints of the uninvolved fingers. With the proximal interphalangeal joint stabilized, the flexor digitorum profundus is presumed severed if the distal interphalangeal joint cannot be actively flexed. • If neither the proximal nor the distal interphalangeal joint can be actively flexed with the metacarpophalangeal joint stabilized, both flexor tendons probably are severed. The method used to show the transection of FDS with an intact FDP involves maintaining the adjacent fingers in complete extension, anchoring the profundus tendon in the extended position, and removing its influence from the proximal interphalangeal joint. When a flexor superfcialis tendon has been severed, and the two adjacent fingers are held in maximal extension,flexion of the interphalangeal joint usually is impossible Exception is the result of the independent function of the index finger FD-Polices a technique advocated by Lister is helpful. The patient is requested to pinch and pull a sheet of paper with each hand, using the index fingers and thumbs. In the intact finger, this function is accomplished by the FDP . If a wound is located at the level of the wrist, the joints of a finger can be actively flexed even though the tendons to that finger are severed. This is the result of intercommunication of the flexor profundus tendons at the wrist, particularly in the Little and ring fingers. Classification Leddy and Packer ; Profundus avulsion classification • Type I: FDP tendon is avulsed from its insertion and retracts into the palm • Type II: The profundus tendon is avulsed from its insertion, but the stump remains within the digital sheath Type III: A bony fragment is attached to the tendon stump, which remains within the flexor sheath. Zone 1 injuries Leddy type I injuries require early (within 3 weeks)diagnosis and treatment. Although all flexor tendon avulsion injuries are best treated early, Leddy type II and III injuries may be amenable to later repair. Direct tendon repair is preferable if there is at least 1 cm of distal tendon stump. Tendon repair to bone is done if there is less than 1 cm of distal tendon stump. Either suture anchors or pull out suture and button constructs may be used. Bone site should be observed directly before final knot tying to ensure the tendon is well seated on the repair footprint (distal phalanx). Zone 2 Primary repair in the fibroosseous sheath (Bunnell’s “no man’s land”), which was controversial but is now widely accepted Primary repairs at this level frequently fail because of adhesions in the area of the pulleys. If the timing of tendon repair is in doubt, the wound should be cleaned and the repair made later by an experienced surgeon. Routine tendon repairs are preferably done no later than 7 days after injury. After 6 weeks, primary repair is unlikely to be possible Zone III At zone III, the muscle bellies of the lumbricals and the tendons frequently are interrupted. If conditions permit, primary repair of sharply severed nerves is crucial because delaying the repair even a few weeks results in significant gaps between the nerve ends. If wound conditions preclude tendon and nerve repair,the ends of the tendons and nerves are sutured to adjacent fascia to prevent undue retraction. Lumbrical muscle bellies usually are not sutured because this can increase the tension of these muscles and result in a “lumbrical plus finger” (paradoxical proximal interphalangeal extension on attempted active finger flexion). Zone IV, V All tendons and nerves in zone IV can be repaired primarily when wound conditions are satisfactory Because zone V is proximal to the transverse carpal ligament, tendon gliding after repair usually is better here than in more distal zones Partial tendon lacerations; After partial tendon lacerations, complications reported by many authors include rupture, triggering, and tendon entrapment. • A tendon with 60% laceration can retain 50% or more of strength, 90% laceration can retain only slightly more than 25% of its strength. If a tendon is lacerated 60% or more,treated the same as a complete transection. If the laceration is less than 60%,evaluated for the risk of triggering. If triggering is seen, the flap of tendon is smoothly débrided, and the flexor sheath is repaired to help avoid entrapment or triggering of the flap in the defect in the flexor sheath. Tendon Repair Six characteristics of an ideal tendon repair: (1) easy placement of sutures in the tendon, (2) secure suture knots, (3) smooth juncture of tendon ends, (4) minimal gapping at the repair site, (5) minimal interference with tendon vascularity, and (6) sufficient strength throughout healing to permit application of early motion stress to the tendon. Timing 1.Primary repair Golden period With in 24hrs in a clean wound Best results 2.Delayed primary repair 24-10 days Done: suspicion of infection , viability questionable or came late 3.Secondary repair: 10-14days up to 4wks 4.Late secondary After 4 wks Delayed equal or better than emergent repair Tendon deterioration/shortening after several wks Delay several days if wound infected Types of repairs Stages of tendon healing Stage 1; 0-4 weeks • Encourage active extension of fingers hold for 10 counts and use rubber bands to passively flex the fingers. 10 repetitions every hour. Make sure PIP joint contracture does not develop StageII; 4-6 weeks Supervised active flexion Encourage to do active flexion and extension Stage III; 6-8 weeks; Bivalve cast, suture removal, dorsal POP slab Active flexion and extension within the slab Each day increase 10 degrees of extension by breaking the slab at MCP joint Isolation of FDS and FDP exercises using Bunnell’s block. Stage IV; 8-10 weeks; Volar cock up splint, wrist in neutral Encourage active flexion and extension of all fingers within the splint Light activities Home self care Post op care; The wrist usually is positioned in neutral position with the metacarpophalangeal joints in 90 degrees of flexion and interphalangeal joints left in 180 degrees extension. Beginning on the 2nd or 3rd day after surgery, flexion outrigger traction device is applied and active extension exercises within the limitations of the splint are encouraged. Conclusion Careful examination of the neurovascular status of the hand precedes the evaluation of tendon function. Even when gross deformity is absent, the posture of the hand often provides clues as to which flexor tendons are severed. Golden period is usually with in 24hrs in a clean wound. When adequate tendon repair is done patients can gain full function of the affected hand again. References Footer Text Greens operative hand surgery 6th edition Merk Manual Medscape Apley and Solomon 9th edition.