Thiazide Diuretics
advertisement

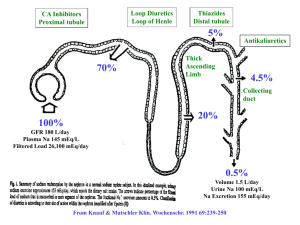
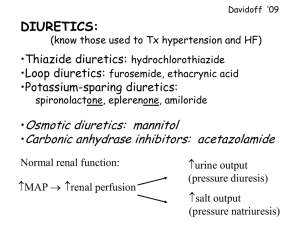
Prepared by Hindi Salem Alharbi Supervised by Dr. Vasudevan Mani Kumara DEFINTIONS Diuretics are chemicals that increase the volume of the urine excreted by the kidney through increase the rate of urine formation. Reduce the extracellular fluid volume by promoting the excretion of Na+or Cl-or HCO3-ions which constitute the main electrolytes of the extracellular fluid. • Natriuresis- increased sodium excretion • Kaliuresis- Increased Potassium excretion CLASSIFICATION • – • – • – • – • Carbonic Anhydrase Inhibitors Acetazolamide,Dorzolamide Osmotic Diuretic Glycerine,Mannitol Loop Diuretics Frusemide,Bumetanide,Torasemide,Ethacrynic acid Thiazide and thiazide related Diuretics Hydrochlorothiazide,polythiazide,Metolazone,Indapamide Potassium Sparing Diuretics – Aldosterone Antagonist • Spironolactone,Canrenone, Eplerone – Direct Acting • Triamterene, Amiloride (more potent) SITE OF ACTIONS Carbonic An-hydrase Inhibitors Thiazide diuretics SITE OF ACTION Osmotic Diuretics Potassium Sparing Diuretics Loop Diuretics (High Ceiling) THIAZIDE AND THIAZIDE-RELATED DIURETICS Thiazide and related Diuretics -Chlorothiazide (the only thiazide for parenteral use) -Chlorthalidone -Hydrochlorothiazide,Bendroflumethiazide -Indapamide (non-thiazide Sulfonamide) -Metolazone -Polythiazide, Benzthiazide -Quinethazone THIAZIDE AND THIAZIDE-RELATED DIURETICS Thiazide diuretics are sulfonamide compounds. Orally efficacious, have a moderate natriuretic effect, and have few adverse effects in most patients. All thiazide diuretics are secreted in the proximal tubule but their site of action is the distal tubule. They compete with uric acid for secretion (the same system secretory mechanism) hyperuricemia THIAZIDES MECHANISMS OF ACTION Thiazide diuretics inhibit re-absorption of Na+and consequently Cl-in the distal convoluted tubule by inhibition of Na+/ Clco transport system present in the luminal membrane (saluretic). They lead to loss of 5-8% of the load of sodium. THIAZIDES MECHANISMS OF ACTION NaCl-rich tubular fluid reaching late distal tubule and collecting duct stimulates exchange of Na+ and K+. Increased Na+ delivery leads to increased secretion of K+ and H+ by duct. By this process, thiazides produce a kaliuretic effect, causing hypokalemic metabolic alkalosis. THIAZIDES MECHANISMS OF ACTION Unlike other diuretics, Thiazides ↑ Mg+ excretion and Ca2+ reabsorption in distal convoluted tubule and thus ↓ Ca2+ excretion in urine.** **This is the basis for thiazides use in kidney stones caused by excessive calcium in the urine. Action of thiazides depends in part on renal PGs synthesis; therefore, actions of thiazides can be inhibited by NSAIDs under certain conditions. THIAZIDES MECHANISMS OF ACTION Thiazides ADVERSE EFFECTS AND DRUG-INTERACTIONS Hypokalemia. hypokalemic metabolic alkalosis. Hyperglycemia Hyprelipedemia. Hyperuricemia (may precipitate gout). Cross-reactivity with sulfonamides may result in hemolytic anemia, thrombocytopenia & acute necrotizing pancreatitis. Weakness, fatigability and paresthesias may occur. CLINICAL INDICATIONS -Hypertension -Congestive Heart Failure -Cirrhosis -Nephrolithiasis (kidney stones) due to idiopathic hypercalciuria -Nephrogenic Diabetes Insipidus (insufficient level of ADH) -Nephrotic Syndrome -Pulmonary Edema Hydrochlorothiazide is the most commonly used diuretic and Polythiazide has a much longer half life and duration of action (DOA) than HCTZ. THIAZIDE-LIKE DIURETICS Indapamide and Metolazone are slightly different in structures from thiazide diuretics, but similar in actions. Indapamide is generally used in the treatment of CHF and hypertension. Metolazone may be more effective than Thiazides in patients with impaired renal function. Metolazone is sometimes combined with loop diuretic to treat patients with diuretic resistance.