SKINmed: Dermatology for the Clinician (ISSN 1540-9740) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652.
Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including
photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors
and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at showell@lejacq.com or 203.656.1711 x106.
New Variant of Endemic Pemphigus
O r i g i n a l
C o n t r i b u t i o n
Rare Clinical Form in Two Patients
Affected by a New Variant of Endemic
Pemphigus in Northern Colombia
Ana María Abrèu Velez, MD, PhD;1 Isabel Cristina Avila, BS;2,3 Jaime Segovia, BS;1 Maria Mercedes Yepes, MD;4
Wendy B. Bollag, PhD1
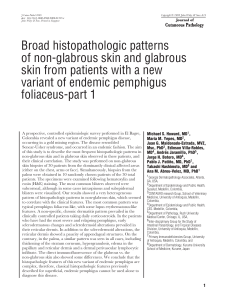
Background. Recently, the authors described a
new variant of endemic pemphigus foliaceus in
rural areas surrounding El Bagre, Colombia, but
without association with malignant tumors.
Methods. The authors’ 10-year fieldwork provided the opportunity to observe various manifestations of El Bagre endemic pemphigus foliaceus, including the presence of bilateral plaques
in pretibial areas.
Results. Based on personal experience and literature reviews, the authors have correlated the
auto-antibody profile with the appearance of
pretibial plaques.
Conclusion. Since pretibial plaques occur in
patients with both fogo selvagem and El Bagre
variants of endemic pemphigus foliaceus, as well
as in other forms of pemphigoid, these diseases
must be considered in the differential diagnosis of
patients with clinical, immunologic, and/or epidemiologic risk factors. (SKINmed. 2004;3:317–
321) ®2004 LeJacq Communications, Inc.
E
ndemic pemphigus foliaceus (EPF)
represents an exceptional group of
autoimmune diseases that occurs in
well-defined regions of South America1,2 and
has been recently described in Tunisia, Africa,
although no field epidemiological studies
have been reported for this possible focus.3
Recently, the authors have characterized a new
variant of EPF in a rural mining municipality
in El Bagre, situated in the northeastern part
of the state of Antioquia in Colombia, South
America.4–6 Ten years of fieldwork experience
November • December 2004
working with patients affected by EPF allows
the authors to have an idea of the natural
course of the disease, as well as the common
clinical manifestations. The clinical manifestations of El Bagre EPF resembled most strongly those of pemphigus erythematosus, also
known as Senear-Usher syndrome. El Bagre
EPF primarily affects 40–60-year-old males, as
well as postmenopausal females; patients are
primarily miners who also engage in farming.6–8 This incidence is quite dissimilar from
Brazilian EPF, or fogo selvagem, which mainly
affects children and young adults, with the
highest incidence at 10–30 years of age, and
with both sexes uniformly affected.1,2 Also, in
contrast to the El Bagre form, the EPF reported
in Tunisia most frequently affects females
of child-bearing age.3 The authors recently
reported the more common clinical manifestations of the El Bagre EPF.6–8
Case Reports
From the Institute of Molecular
Medicine and Genetics, Medical
College of Georgia, Augusta,
GA;1 Reproduction Group,
School of Medicine, University
of Antioquia, Medellin,
Colombia;2 Biotechnology
Group, School of Sciences,
National University, Medellin,
Colombia;3 Department of
Epidemiology and Public Health,
School of Medicine, University of
Antoquia, Medellin, Colombia4
Address for correspondence:
Ana María Abrèu Velez, MD,
PhD, Institute of Molecular
Medicine and Genetics, Medical
College of Georgia, 1120 15th
Street, Augusta, GA 30912
E-mail: aavelez@mail.mcg.edu
www.lejacq.com
ID: 3514
Case 1. A 43-year-old man who has had EPF
for 7 years and whose clinical control has
been difficult. This disease has been relapsing, despite a dosage of 30 mg per day of
oral steroids. The authors have attended this
patient in their health missions to the El Bagre
municipality and, during the physical examination, observed the presence of extended
pretibial plaques in both lower extremities.
The patient reported having them for the previous 3 weeks. He denies a history of trauma
or an insect bite episode associated with the
317
SKINmed: Dermatology for the Clinician (ISSN 1540-9740) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652.
Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including
photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors
and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at showell@lejacq.com or 203.656.1711 x106.
New Variant of Endemic Pemphigus
Figure 1. Case 1: Upper panels (A, B) show two different
pictures from the same patient
on the same day, demonstrating 3×5 cm indurated plaques
located on the lower aspect of
the legs with the presence of
superficial dry scales. At palpation, the plaques were firm and
located bilaterally. The ankle
was mildly distorted with the
plaque. In the lower panels (C,
D) the presence of fine crusts
and plaques with mild scaling
in the malar areas and round
flat plaques with a pinkish tone
are shown on the forehead.
appearance of the lesions. The patient was
not taking any other medication at the time,
usually wore open-toe shoes, and was in continuous contact with forest and agricultural
vegetation and water from creeks or rivers
in the endemic area. At the physical exam,
no regional or other lymphadenopathy was
observed. Figure 1 (A–D) illustrates the clinical
318
findings on the face and legs of this patient.
The presence of clinical tinea pedis and interdigital candidiasis was seen; however, diagnoses of subcutaneous mycosis, tuberculosis, or
atypical leishmaniosis were discarded because
of the absence of the causative agents as determined by potassium hydroxide and fungal,
bacterial, and parasitic diseases cultures. As a
November • December 2004
SKINmed: Dermatology for the Clinician (ISSN 1540-9740) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652.
Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including
photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors
and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at showell@lejacq.com or 203.656.1711 x106.
New Variant of Endemic Pemphigus
differential diagnosis, the authors also considered a pretibial myxedema, a chronic eczematous dermatitis, an elephantiasis secondary to
a lymphatic filariasis, a lupus profundus, and
an elephantiasis nostra verrucosa; however, all
these diagnoses could be excluded. Therefore,
two 6-mm deep-skin biopsies were taken and
deep cultured for fungi, bacteria (aerobic and
anaerobic), atypical and typical mycobacteria,
and atypical leishmaniosis according to the
World Health Organization (WHO) recommendations. Seven sections of the biopsies
were embedded in optimal cutting temperature, cryostat sectioning tissue freezing medium for direct immunofluorescence (using perilesional skin) and 10% formol for hematoxylin and eosin staining. In addition, peripheral
blood was taken for serological tests.7,8
Case 2. A 53-year-old man who has had EPF
for 3 years also showed the presence of plaques
in the lower extremities. As in Case 1, the
patient denied a history of previous trauma or
mosquito bites and also walked with open-toe
shoes. The patient had been taking 80 mg/d
of oral steroids for 5 weeks. No modification of the plaques was reported in association with the steroid medication. His physical
appearance is illustrated in Figure 2 (A, B). No
regional lymphadenopathy was observed, and
no arterial or venous insufficiency was noticed.
The physical exam revealed a plethoric face
and redistribution of fat with moon facies,
“buffalo” hump, truncal obesity, and thin
arms, resulting in a concomitant diagnosis of
Cushing’s syndrome, probably secondary to the
exogenous steroid. In addition, the skin of the
chest and face showed multiple annular lesions
with a peripheral scaling in an erythematous
base, which is commonly observed in patients
affected by the El Bagre variant of EPF. Because
of the unusual presentation of the lesions, the
authors thought of complications or secondary
infections that prevail in the tropical area of
El Bagre and followed similar synergies as for
those in the patient described in Case 1.
Results
Microbiological studies. Diagnoses of chromoblastomycosis, blastomycosis, bacterial
pyoderma, foreign-body granuloma, inflammatory dermatophytoses, tuberculosis, tertiary syphilis, leishmaniosis, and pyoderma
were excluded using standard procedures
and proper culture media following WHO
November • December 2004
Figure 2. The general
“cushingoid” appearance
of the patient, including the
pretibial plaques, is shown in
Figure 2A. Figure 2B shows
the presence of pretibial
lichenoid plaques on the
lower extremity, with features
similar to those described in
Case 1. The plaques were
indurated, bilateral, and
about 3×6 cm.
recomendations.7 To perform a differential
diagnosis to determine the cause of the pretibial plaques and subcutaneous inflammatory masses, the authors focused their studies on chromoblastomycosis, blastomycosis,
bacterial pyoderma, foreign-body granuloma,
inflammatory dermatophytoses, tuberculosis,
tertiary syphilis, leishmaniosis, and pyoderma
following standard procedures as described
elsewhere.7 Multiple serological tests and
cultures were performed to rule out associated pathologies, mostly related to bacterial or
fungi infections. No hyphal or pseudohyphal
forms or black dots were visualized. Gram
stains using the skin biopsy smears were also
negative. For microbiological analysis, the
lesional biopsies were ground in saline solution and tested using culture media for fungi
(Sabouraud’s glucose agar and in Mycocel),
bacillary forms, bacterias and Novy-MacNealNicolle medium. All these tests were negative.
Cultures for gram-positive, gram-negative, and
anaerobic microorganisms taken from both
the sera and skin lesions were negative. An
immunodiffusion and complement fixation
test was negative for histoplasma. Leishmania
(Montenegro) skin test and serology for leishmania were negative, as well as VDRL, FATS,
and a dark-field examination test. Serial gram
stains for bacterial and bacilli forms were
performed. An antigen detection test using
an enzyme-linked immunosorbent assay for
319
SKINmed: Dermatology for the Clinician (ISSN 1540-9740) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652.
Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including
photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors
and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at showell@lejacq.com or 203.656.1711 x106.
New Variant of Endemic Pemphigus
Figure 3. The hematoxylin
and eosin staining shows
a pseudoepitheliomatosus
hyperplasia of the epidermis.
Mixed inflammatory cell infiltration was seen on both the
superficial and the deep skin
vessels. Eosinophilic granules
in the horny layer and downward proliferation of epithelial
strands were pronounced.
Extensive hyperkeratosis,
hypergranulosis, acanthosis,
and papillomatosis were
clearly seen.
Figure 4. Results of
immunoblotting
Wuchereria bancrofti or Brugia malayi (trop ag
bancrofti), (JCU Tropical Biotechnology Pty
Ltd., Townsville, North Queensland, Australia)
were performed. In addition, assays for the
presence of antifilarial antibodies against
Brugia and W. malayi were performed and
were negative. X-rays of the legs showed an
increase in the amount of subcutaneous tissue. Chest x-rays showed no distinguishable
abnormalities in the interstitial or subcutaneous tissue. Bronchial wash secretions were
also negative for fungi, bacilli, bacterial, and
mycobacterium. A thyroid hormonal screen
was normal in both cases.
Immunohistopathological studies. The two
cases share some common histopathological
and immunofluorescence findings. In both
Case 1 and Case 2, the histopathology demonstrated a hyperparakeratosis with the pres-
320
ence of colloidal bodies in the corneal layer,
considerable acanthosis, hyperkeratosis with
a few cleft formations, and rare spot areas of
acantholysis in the granular layer. The granular
cells appeared shrunken and hyperchromatic.
In another field, atypical keratinocytes were
seen. In both case studies, a mixed inflammatory infiltrate was observed (Figure 3). Direct
and indirect immunofluorescent tests were
conducted, as described elsewhere, using sections of normal human skin in the case of the
indirect immunofluorescent test and patient
skin in the case of direct immunofluorescence.8
Both tests showed a concomitant basement
membrane zone deposition of granular immunoglobulin C3 and IgG4 in lesional skin, in
addition to intercellular staining in the epidermis, but only in spot areas. The patients’ sera
also contained autoantibodies that resulted in
intercellular staining as visualized with monoclonal antibodies that resulted in intercellular
staining and visualized with monoclonal antibodies to IgG4, with titers of 1:320 in Case 1
and 1:60 in Case 2; however, additional intracytoplasmic staining in both membrane zone
areas and throughout the epidermis could also
be visualized. Figure 4 illustrates the results
of immunoblotting. Using extracts of fullthickness epidermis as an antigen source and
enhanced chemiluminescence for detection,
immunoblotting analysis demonstrated that
the sera from the patient described in Case 1
(A) recognized a 160 kDa protein band. This
band comigrated with desmoglein 1, as determined using an anti-desmoglein 1 antibody
from Progen Biotech (Heidelberg, Germany);
however, other protein bands with molecular
weights of approximately 208, 190, 187, 145,
and 130 KDa (non-desmoglein 3 antigen were
also recognized by the endemic perphigus foliaceus (EPF) sera. An anti-periplakin antibody
November • December 2004
SKINmed: Dermatology for the Clinician (ISSN 1540-9740) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652.
Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including
photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors
and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at showell@lejacq.com or 203.656.1711 x106.
New Variant of Endemic Pemphigus
from a patient with paraneoplastic pemphigus
(PNP) comigrated with the 190 kDa band.
Serum from the other patient (Case 2) recognized 300 and 250 kDa bands that comigrated
with bands recognized by an anti-desmoplakin
monoclonal antibody (which detect desmoplakin I). A doublet of bands of about 210 kDa
that might represent envoplakin, and a band
of ≈190 kDa that might represent periplakin,
were also observed. Normal human epidermis
(full thickness) was prepared as previously
described.9 Serum from a patient with paraneoplastic pemphigus, which recognizes envoplakin and periplakin, was used as a control.
Conclusions
This paper reports two case studies of patients
affected by a new variant of EPF in El Bagre,
Colombia who have frequent, relapsing episodes, poor response to steroid therapy, and
bilateral pretibial plaques associated with the
presence of autoantibodies recognizing a heterogeneous autoantigen population, including
desmogleins and possibly desmoplakin molecules. In agreement with the authors’ findings,
in 1937, Dr. Joao Paulo Viera also reported the
presence of pretibial plaques in patients with
fogo selvagem as a part of a rare modality of
this disease.10 In addition to this manifestation, he also described other rare manifestations of fogo selvagem in the hair and scalp,
such as temporal patchy alopecia, tinea favus,
pseudopelade of Brocq, and a papillomatous
appearance of the scalp, predominantly seen
in chronic cases.10 Pretibial lichenoid plaques
were also described as a rare manifestation of
fogo selvagem, but have also been reported in
patients with bullous pemphigoid.11–18
It is important to consider as a differential
diagnosis a generalized atrophic benign epidermolysis bullosa17—a form of nonlethal
junctional epidermolysis bullosa characterized
by universal alopecia, atrophy of the skin, and
clinical pretibial presentation. Also, hypothyroidism (pretibial myxedema) or pretibial
epidermolysis bullosa should be considered as
possible diagnoses.18 Since no other concomitant diseases were seen in either case study, in
agreement with Viera,10 the authors suggest
that the presence of bilateral pretibial plaques
represents a rare form of El Bagre EPF.
REFERENCES
1 Castro RM, Proenca NG. Similarities and differences between South American pemphigus
foliaceus and Cazanave’s pemphigus foliaceus.
An Bras Dermatol. 1983;53:137–139.
2 Chiossi MP, Roselino AM. Pemphigus foliaceus (“Fogo selvagem”): a series from the
Northeastern region of the State of Sao Paulo,
Brazil, 1973–1998. Rev Inst Med Trop Sao Paulo.
2001;43:59–62.
3 Morini JP, Jomaa B, Gorgi Y, et al. Pemphigus
foliaceus in young women. An endemic focus
in the Sousse area of Tunisia. Arch Dermatol.
1993;129:69–73.
4 Hisamatsu Y, Abreu Velez AM, Amagai M, et
al. Comparative study of autoantigen profile
between Colombian and Brazilian types of
endemic pemphigus foliaceus by various biochemical and molecular biological techniques.
J Dermatol Sci. 2003;32:33–41.
5 Abréu-Vélez, AM, Beutner, E, Montoya F, et
al. Analyses of autoantigens in a new form of
endemic pemphigus foliaceus in Colombia.
J Am Acad Dermatol. 2003;49:599–608.
6 Abréu-Vélez AM, Hashimoto T, Tobón S, et al. A
unique form of endemic pemphigus in northern
Colombia. J Am Acad Dermatol. 2003;49:609–614.
7 Mabey D, Peelin RW, Ustianowsk A, et al.
Tropical infectious diseases: Diagnostics for
the developing world. Nat Rev Microbiol.
2004;2:231–240.
8 Beutner EH, Prigenzi LS, Hale W, et al.
Immunofluorescence studies of autoantibodies
to intercellular areas of epithelia in Brazilian
pemphigus foliaceus. Proc Soc Exp Biol Med.
1968;127:81–86.
9 Ogawa MM, Hashimoto T, Konohana A,
Castro RM, et al. Immunoblot analyses of
Brazilian Pemphigus foliaceus antigen using
November • December 2004
10
11
12
13
14
15
16
17
18
different antigen sources. Arch Dermatol Res.
1990;282:84–88.
Viera JP. Algumas modalidades raras do penfigo foliaceo entre nos. (Some rare modalities
of pemphigus foliaceus among our patients.)
(Archives of dermatol and syfilol of Sao Paulo).
Archivos de Dermatologia e Syphilographia de Sao
Paulo. 1937;1:22–26.
Nakatani C, Muramatsu T, Shirai T. Localized
pretibial pemphigoid associated with trichilemmal carcinoma. J Dermatol. 1998;25:448–452.
Muramatsu T, Iida T, Shirai T. Pemphigoid
and pemphigus foliaceus successfully treated with topical corticosteroids. J Dermatol.
1996;23:683–688.
Chang YT, Liu HN, Wong CK. Bullous pemphigoid-a report of 86 cases from Taiwan. Clin Exp
Dermatol. 1996;21:20–22.
Kitajima Y, Suzuki M, Johkura Y, et al. Localized
bullous pemphigoid: report of a case with
an immunofluorescence and electron microscopical studies on the lesional distribution
of 180-KD bullous pemphigoid antigen, beta
4 integrin, and type VII collagen. J Dermatol.
1993;20:406–412.
Muramatsu T, Iida T, Shirai T. Antibasement
membrane zone antibodies in localized pretibial
pemphigoid. Int J Dermatol. 1991;30:422–424.
Person JR. Hydrostatic bullae and pretibial pemphigoid. Int J Dermatol. 1983;22:237–238.
Jonkman MF, de Jong MC, Heeres K, et al. 180kD bullous pemphigoid antigen (BP180) is deficient in generalized atrophic benign epidermolysis bullosa: J Clin Invest. 1995;95:1345–1352.
Le Brun V, Boulinguez S, Bouyssou-Gauthier
ML, et al. [Pretibial epidermolysis bullosa
and hypothyroidism.] Ann Dermatol Venereol.
2000;127:184–187.
321

![Rare two cases of EPF.1540-9740.2004.03514.x[1]](http://s3.studylib.net/store/data/025569805_1-7ee21d121b52dd50fe47580027ac57dc-300x300.png)