CA 125, a New Prognostic Marker for Aggressive NHL
advertisement

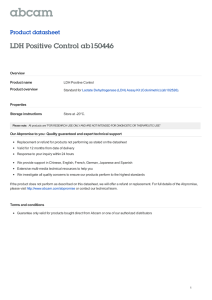
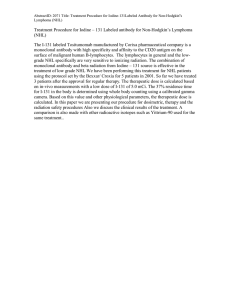
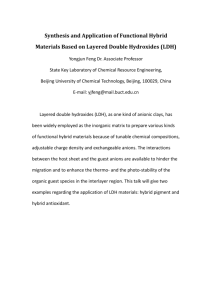
Journal of the Egyptian Nat. Cancer Inst., Vol. 21, No. 3, September: 209-217, 2009 CA 125, a New Prognostic Marker for Aggressive NHL IMAN A. ABD EL GAWAD, M.D.* and HANAN E. SHAFIK, M.D.** The Departments of Clinical & Chemical Pathology* and Medical Oncology**, NCI, Cairo University. A shorter disease-free survival was associated with increased CA 125 (p<0.001). ABSTRACT Purpose: CA 125 was evaluated in the sera of patients with aggressive NHL, together with LDH and ß2m, in a trial to assess its value in the diagnosis and follow-up, and to compare it to some prognostic factors. Conclusion: CA125 was found to correlate with stage, tumor bulk, involvement of more than 1 extranodal site, and presence of effusion. Elevated levels of CA 125 and LDH were found to predict decreased survival. Initial measurement of CA125 may, therefore, provide valuable prognostic information. Subjects and Methods: The study included 78 newly diagnosed patients with diffuse large B cell non-Hodgkin’s lymphoma (DLBCL), with age range 18-60 years, and a WHO performance status of 0, I or II, in addition to twenty apparently healthy controls. All patients received CHOP regimen for 6 cycles. Key Words: CA125 – LDH – ß2m, NHL – DLBCL. INTRODUCTION Results: The levels of CA 125 and LDH were significantly higher in DLBCL compared to the control group (p-value = 0.031 and = 0.009, respectively). Cutoff levels used were 20U/ml, 310 U/L, and 2µg/l for CA125, LDH and ß2m, respectively. CA125 serum level was high in 55%, LDH level in 72%, and ß2m level in 62% of patients. Cancer antigen 125 (CA 125) is a 220kDa glycoprotein expressed in normal tissues originally derived from coelomic epithelia such as peritoneum, pleura, pericardium [1], epithelium of the female genital tract, mucosal cells of the stomach and colon, and mesothelial cells of serous membranes [2,3]. As regards the stage, CA 125 was elevated in 17%, 52%, 80%, and 100% of patients in stage I, II, III, and IV, respectively. CA 125 was elevated in 81.3% of patients with bulky disease, in 83.3% presenting with involvement of more than 1 extranodal site, and in 90% presenting with effusion. CA125 serum levels are used to monitor response to therapy and for follow-up of patients with ovarian cancer [1]. They may also be elevated in other malignant and nonmalignant conditions [4,5]. Although elevated levels have been reported in patients with non-Hodgkin's lymphoma (NHL), its role as a prognostic factor remained uncertain [6]. The highest levels of CA125, LDH, and ß2m were observed in stage IV, and lowest in stage I (p-value <0.001, 0.005, and 0.154, respectively). There was also a significant positive correlation between CA 125 and LDH (p-value <0.001). CA 125 showed specificity of 80% with 95% CI (5694), and LDH showed sensitivity of 72% with 95% CI (60-81). Non-Hodgkin's lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignant diseases with differing patterns of behavior and response to treatment [7]. Complete response to treatment was achieved in 71.8% of our patients. Survival at 24 months was 78.2%. There was a statistically significant increase in survival in patients with CA125 <20U/ml, patients with LDH <310U/L, and patients with ß2m <2µg/l (p-value = 0.006, 0.025, and 0.042, respectively). Many prognostic factors have been described in aggressive NHL: B symptoms (fever, night sweats, and weight loss), performance status, age, serum lactate dehydrogenase (LDH) level, serum ß2 microglobulin, tumor bulk, and number of nodal and extranodal sites of disease [8]. Correspondence: Dr Iman Attia Abdel Gawad Lecturer of Clinical Pathology, NCI, imanaga70@yahoo.com 209 210 CA 125, a New Prognostic Marker for Aggressive NHL Elevated serum CA125 levels have been reported in patients with NHL, especially those with advanced disease [9]. CA125 was reported by Lazzarino et al. [1], to be a reliable biologic marker for the staging and restaging of patients with NHL. The aim of this work is to study CA 125 in the sera of patients with diffuse large B cell lymphoma (DLBCL) in a trial to assess its value in the diagnosis and follow-up, and to compare it with some prognostic factors. CA125 will be compared to LDH, and ß2m. The relation between CA125 and patients’ survival will also be studied. PATIENTS AND METHODS Patients: Patients included in this study were subjected to careful history taking, clinical examination, histopathological typing, and routine laboratory investigations. Fresh blood samples were obtained from seventy-eight newly diagnosed patients with DLBCL who presented to the outpatient clinic of the medical oncology unit, NCI, Cairo University, over a period of eight consecutive months from January to May, 2006. They were 47 males and 31 females with ages ranging from 20 to 64 years. Blood samples were obtained from twenty apparently healthy volunteers as controls. Eligibility requirements included patients with histologically proven DLBCL, age from 18 to 60 years, a WHO performance status of 0, I or II. All patients received CHOP regimen for 6 cycles: • Cyclophosphamide: 750mg/m2 i.v. day 1. • Doxorubicin: 50mg/m2 i.v. day 1. • Vincristine: 1.4mg/m2 i.v. day 1 (maximum 2mg). • Predenisone: 100mg/m2 p.o. days 1-5 [10]. A written consent was taken from all patients according to the international ethics committee guidelines. Methods: Serum samples were prepared and aliquoted. All patients and control samples were subjected to the following: 1- Routine laboratory investigations: • Liver function tests (ALT, AST, ALP), kidney function tests (urea, creatinine, uric acid), and LDH using Beckman autoanalyzer CX9 (USA). • Complete blood picture (CBC) using Coulter Counter (USA). 2- CA125 using AxSYM enzyme immunoassay (Abbott Diagnostics, USA) [11]. 3- ß2m using AxSYM enzyme immunoassay (Abbott Diagnostics, USA) [11]. Statistical analysis: Data management and analysis were performed using the Statistical Analysis System (SPSS) software. Comparison of groups with respect to numerical variables was done using the Mann Whitney test. The Kruskal Wallis test was used to compare medians of 3 or more independent groups. Pearson’s correlation was used to measure the strength of association between 2 numerical variables [12] . Overall survival and progression-free survival were estimated in all patients using the Kaplan-Meier test. All p-values were two sided. p-values ≤0.05 were considered significant. Sensitivity, specificity and diagnostic accuracy were the validity measures used for testing the studied parameters as diagnostic tools for NHL. The different cutoffs were chosen using the receiver operating characteristic (ROC). The ROC curve was constructed by plotting sensitivity versus 1specificity. The curve was drawn through points that represent different decision cut-off levels [13]. RESULTS Table (1) shows the patients’ characteristics. Table (2) shows percentages of elevation of the studied markers according to some prognostic factors. Table (3) shows comparative analysis of CA 125, LDH, and ß2m serum levels in NHL and control group. The comparison was statistically significant for CA125 and LDH (p-value = 0.031 and = 0.009, respectively). Iman A. Abd El Gawad & Hanan E. Shafik Table (4) shows comparison between CA125, LDH, and ß2m serum levels according to the different stages. All parameters showed the highest level in stage IV, followed by stage III, then stage II, and lowest in stage I. The comparison was statistically significant for only CA125 and LDH (p-value <0.001, 0.005, respectively). For CA125, there was a statistically significant difference between stage I & II, between stage I & III, between stage I & IV, between II & III, and between stage II & IV. For LDH, there was a statistically significant difference between stage I & III, between I & IV, between II & IV, and between II & IV. Table (5) shows comparison of CA125, LDH and ß2m with some prognostic factors. As regards the presence or absence of bulky disease, the results were statistically significant for the three markers (p-value <0.001, <0.001 and 0.009, respectively). As regards involvement of more than 1 extranodal site, the comparison was statistically significant for CA125 and LDH (p-value <0.001). On comparing the 3 markers according to presence or absence of effusion, the results were also statistically significant for only CA125 and LDH (p-value <0.001, 0.002, respectively). CA125, LDH and ß2m showed no significant results in relation to the presence or absence of B symptoms (p-value = 0.238, 0.187 and 0.527 respectively). On performing Pearson’s correlation between CA125 and the other two markers LDH and ß2m, and between CA125 and age, there was a statistically significantly positive correlation between CA125 and LDH (p-value <0.001, r=0.607) (Fig. 1), and weak correlation between CA125 and ß2m (p-value <0.001, r=0.398), but no statistically significant result was obtained between CA125 and age (p=0.381, r=0.101). Table (6) shows measurement of diagnostic performance of the different markers in NHL patients. LDH showed high sensitivity of 72% with 95% CI (60-81), and CA 125 showed high specificity of 80% with 95% CI (56-94). However, there was no significant difference between the 3 markers as regards sensitivity and specificity due to overlapping of their 95% CI. As regards sensitivity, the 95% CI for CA125, LDH, and ß2m was (43-66), (60-81), and (4972), respectively. As for specificity, 95% CI was (56-94), (19-63), and (15-59), respectively. 211 Table (1): Patients characteristics. n (%) Sex: Male Female 47 (60.3) 31 (39.7) Age (years): Median : 43 Range : 20-64 Stage: I II III IV 23 (29.0) 29 (37.0) 10 (12.0) 16 (20.0) Prognostic factors: Involvement of more than one extranodal site Bulky disease Effusion B symptoms 24 (30.8) 16 (20.0) 10 (12.8) 27 (35.0) CA125: High Low 43 (55.0) 35 (45.0) LDH: High Low 56 (72.0) 22 (28.0) ß2M: High Low 48 (62.0) 30 (38.0) Table (2): Percentages of elevation of the studied markers according to prognostic factors. Stage I II III IV Bulky diseaes (a) More than 1 extranodal site (b) Effusion (c) Total CA125 n (%) LDH n (%) ß2m n (%) 23 29 10 16 16 24 4 (17.0) 15 (52.0) 8 (80.0) 16 (100.0) 13 (81.3) 20 (83.3) 13 (56.0) 20 (69.0) 8 (80.0) 14 (87.0) 16 (100.0) 21 (87.5) 12 (52.0) 20 (69.0) 6 (60.0) 10 (62.0) 10 (62.5) 14 (58.3) 10 9 (90.0) 10 (100.0) 6 (60.0) a: Elevation of marker in relation to presence of bulky disease. b: Elevation of marker in relation to involvement of more than 1 extranodal site. c: Elevation of marker in relation to effusion. Table (3): Comparative analysis of CA125, LDH, and ß2m serum levels in DLBCL patients and control group using the Mann-Whitney test. Control group N=20 NHL group N=78 10.0 (9.0-11.0) 20.9 (7.6-49.0) 0.031* LDH (U/L) 318.0 (300.5-342.0) 408.0 (267.0-588.5) 0.009* ß2m (µg/l) 2.2 (1.6-2.7) 2.2 (1.8-2.7) 0.764 CA125 (U/ml) p-value * Significant. Values are medians with interquartile ranges in parenthesis. 212 CA 125, a New Prognostic Marker for Aggressive NHL Table (4): Comparison of CA 125, LDH and ß2m serum levels according to stage using the Kruskal Wallis test. CA125 (U/ml) LDH (U/L) 7.3 c (3.3-9.8) 382.0 b 2.0 (230.3-428.0) (1.4-2.4) Stage II (n=29) 20.1 b (7.6-23.0) 406.0 b 2.2 (254.8-513.0) (1.8-2.7) Stage III (n=10) 47.0 a (21.0-61.6) 480.0 a 2.3 (350.0-605.0) (1.8-4.0) Stage IV (n=16) 57.5 a 650.0 a 2.3 (51.0-104.0) (468.5-842.3) (1.8-5.4) <0.001* 0.005* 0.154 * Significant. Values are medians with interquartile ranges in parenthesis. Group medians sharing same letter are statistically insignificant. Table (5): Comparison of CA 125, LDH and ß2m with some prognostic factors of NHL using the Mann Whitney test. CA125 (U/ml) LDH (U/L) ß2m (µg/l) Bulky disease (n=16) 53.0 (47.0-68.0) 647.0 (583.0-814.0) 3.0 (2.0-4.3) Non bulky disease (n=62) 13.9 (4.0-23.2) 389.0 (250.0-473.0) 2.1 (1.5-2.5) <0.001* <0.001* 0.009* Pos invol (n=24) (p) 49 (32.0-63.3) 614.0 (462.5-715.0) 2.3 (1.9-3.0) Neg involv (n=54) (n) 11.5 (4.0-22.7) 382.0 (247.5-439.0) 2.1 (1.5-2.6) p-value <0.001* <0.001* 0.132 Effusion (n=10) 63.3 (48.0-68.3) 650.0 (523.0-828.0) 2.8 (2.0-6.5) No effusion (n=68) 16.5 (7.0-35.0) 396.0 (255.0-486.0) 2.0 (1.6-2.6) <0.001* 0.002* 0.065 p-value p-value CA 125 LDH ß2m cutoff cutoff cutoff 20 (U/ml) 310 (U/L) 2 (µg/l) ß2m (µg/l) Stage I (n=23) p-value Table (6): Measurement of diagnostic performance of the different markers in NHL patients. *Significant. Values are medians with interquartile ranges in parenthesis. (p): Positive involvement of more than 1 extranodal site. (n): Negative involvement of more than 1 extranodal site. Sen % Sen (95% CI) Spe % Spe (95% CI) PPV PPV (95% CI) NPV NPV (95% CI) Diagnostic accuracy % 56 (43-66) 80 (56-94) 91 (79-97) 31 (19-45) 60 72 (60-81) 40 (19-63) 82 (71-90) 27 (12-45) 65 62 (49-72) 35 (15-59) 79 (66-88) 19 (7-35) 56 Sen: Sensitivity. Spe: Specificity. PPV: Positive predictive value. NPV: Negative predictive value. DA : Diagnostic accuracy. 95% CI: 95% confidence interval. Response: Complete response was achieved in 71.8% of patients (56/78), while 28.2% were resistant to chemotherapy. Survival: All patients were followed for 24 months, median time of follow-up was 18 months. Survival at 12 months was 83.3%, and at 18 months 75.9%. Median survival was not reached. Patients with CA125 <20U/ml, LDH <310U/L, and ß2m <2µg/l showed a statistically significant longer overall survival than those with higher levels (p-values = 0.006, 0.025, and 0.042, respectively) (Figs. 2,3,4). As regards disease-free survival (DFS), 22 patients were not eligible for analysis as they were resistant to treatment, so DFS analysis was done for 56 patients only. Median time to progression was not reached. At 12 months, 16.4% of patients relapsed, and at 18 months 23.2% of the patients relapsed (Fig. 5). There was a statistically significant difference in disease free survival between patients with CA125 <20U/ml compared to those ≥20U/ml, (p-value <0.001) (Fig. 6). As regards LDH and ß2m, there was no statistically significant difference in disease free survival between patients with LDH <310U/L compared with those with LDH ≥310U/L (p-value = 0.747) and with ß2m <2µg/l, and those with a value ≥20µg/l, (pvalue = 0.11). Iman A. Abd El Gawad & Hanan E. Shafik 213 Survival Functions 1.0 200 0.8 CA125 150 0.6 100 CA125 High Low High-censored Low-censored 0.4 50 0.2 0 0.0 0 500 1000 LDH 1500 Fig. (1): Correlation between LDH, and CA125. p<0.001 & r=0.607. 3 6 Survival Functions 0.8 0.8 0.6 0.6 LDH High Low High-censored Low-censored 0.0 3 6 9 0.2 0.0 21 24 Fig. (3): Overall survival (OS) according to LDH. p=0.025. 3 6 9 0.8 0.8 0.6 0.4 0.2 12.00 CA125 High Low High-censored Low-censored 0.4 0.0 18.00 24 0.6 0.2 Survival function Censored 6.00 21 Survival Functions 1.0 Cum Survival Cum Survival Survival Functions 0.00 12 15 18 OS (Months) Fig. (4): Overall survival (OS) according to ß2m. p=0.042. 1.0 0.0 24 ß2m High Low High-censored Low-censored 0.4 12 15 18 OS (Months) 21 Survival Functions 1.0 0.2 12 15 18 OS (Months) Fig. (2): Overall survival (OS) according to CA125. p=0.006. 1.0 0.4 9 24.00 DFS (Months) Fig. (5): Disease-free survival (DFS) for the 56 analysed patients. Median DFS not reached. 0.00 6.00 12.00 18.00 24.00 DFS (Months) Fig. (6): Disease-free survival (DFS) in relation to CA125. p<0.001. 214 CA 125, a New Prognostic Marker for Aggressive NHL DISCUSSION Although it is clear that CA125 is not a product of lymphoma cells, elevated serum levels in approximately 40% of NHL patients at diagnosis, and the fact that in most series levels directly correlate with certain features of the disease, such as stage, response to therapy, and survival, suggests that initial and serial measurements of the antigen may provide prognostic information of value [14]. In this study, CA 125 and LDH were found to be higher in the NHL group than in the control group, both markers showed statistically significant elevation. Consistent with our results, Dileki et al. [15] found that the average CA125 level in NHL patients was significantly higher than the controls (p<0.05) in their study done on 149 patients and 26 healthy control subjects. The study group included 69 non-Hodgkin lymphomas (NHL), 25 Hodgkin disease (HD), 20 acute myelocytic leukemia (AML), 14 chronic lymphocytic leukemia (CLL), 12 chronic myelocytic leukemia (CML), and nine multiple myeloma (MM) patients. CA125 was elevated in 37 of the NHL patients and in none of the control subjects. High serum CA125 levels were found to correlate with mediastinal and/or abdominal involvement, high tumor mass, and effusions, reflecting the reaction of mesothelial cells to the tumor [1]. Contrary to other serum markers of established prognostic value in NHL related to tumor load and proliferative activity, such as ß2m and LDH activity, CA125 apparently is not released by lymphoma cells. The mechanism by which lymphoma stimulates CA125 production might be explained by mesothelial cell stimulation via lymphokines derived from NHL [1]. In the present study, CA125 serum level was elevated in 55%, LDH in 72%, and ß2m in 62% of patients. The highest elevation in the advanced stages of the disease was shown by CA125, followed by LDH, then ß2m. CA125 was elevated in 81.3% of patients with bulky disease, in 83.3% of patients presenting with involvement of more than 1 extranodal site and in 90% of patients presenting with effusion. LDH was elevated in 100% of patients with bulky disease, in 87.2% of patients presenting with involvement of more than 1 extranodal site and 100% of patients presenting with effusion. ß2m was elevated in 62.5% of patients with bulky disease, in 58.3% of patients presenting with involvement of more than 1 extranodal site and in 60% of patients presenting with effusion. In a study by Jamal et al. [16], done on thirtyeight patients (24 with aggressive and 14 with low-grade NHL), CA125 levels were elevated in 46% of patients with aggressive NHL and 43% of patients with low-grade NHL. Abdolmonem et al. [17], reported that serum CA125 was elevated above the cut-off value (30.1ng/ml) in 63.3% of patients in their study done on 13 paediatric patients with NHL, and 9 with HD. Also Bairey et al. [7] measured serum CA125 levels prospectively in 108 consecutive patients with NHL: 106 patients were measured at diagnosis, 39 in remission and 7 in relapse. Levels were elevated in 43% at diagnosis. Wei et al. [18] reported that the rate of elevated serum CA125 for all patients was 59.1% in their study done on 355 Chinese NHL patients. Aggressive lymphoma was diagnosed in 216 patients, indolent lymphoma in 87, and undetermined histology in 32. A B-cell immunophenotype was demonstrated in 220 patients. Also, Batlle et al. [19] studied serum levels of CA125, LDH and ß2m in 200 NHL patients with the following histologies: diffuse large Bcell lymphoma (DLBCL; n=95), low-grade (n=66), and other (n=39). CA125 was elevated in 43% of patients at diagnosis, LDH in 27% and ß2m in 24%. CA125 was the only elevated marker in 21% of patients. Bonnet et al. [20], in a similar study carried out on 99 newly diagnosed patients with NHL and HD, found that CA125 serum levels were elevated in 34% of patients, including 19% with aggressive NHL, 45% with indolent NHL. In a study carried by Benboubker et al. [21] on 137 newly diagnosed NHL patients, serum levels of CA125, LDH and ß2m were reported to be elevated in 43%, 44%, and 22% of patients, respectively, using cut-offs 25 IU/1, 300IU/1 and 3µg/1, respectively. LDH levels were higher in intermediate or high-grade NHL, (61%) than sCA125 (43%) or ß2m (23%), while in low- Iman A. Abd El Gawad & Hanan E. Shafik 215 grade NHL 44% had increased sCA125, 23% had increased LDH and 21% had increased ß2m levels. therapy and, in particular, of alternative therapy for patients likely to die either from treatment failure or treatment-related toxicity [21]. In this study, CA125, LDH, and ß2m all showed the highest level in stage IV, followed by stage III, then stage II, and lowest in stage I. Significant results were only obtained for CA125 and LDH (p-value <0.001 and 0.005, respectively). When comparing the 3 markers with bulky disease, all comparisons showed significant results, while when comparing them for the involvement of more than 1 extranodal site and effusion, only CA125 and LDH showed statistically significant results, and when comparing them with the presence or absence of B symptoms, no significant results were found for the three markers. In the present study, complete response was achieved in 56 patients (71.8%). Consistent with these results, Abdolmonem et al. [17] found a statistically significant higher mean level of CA125 in advanced stage (III and IV) paediatric NHL patients compared to stage II, yet LDH levels did not reach statistical significance. Also, in a study done by Bonnet et al. [20] , univariate analyses showed that CA125 levels correlated with poor performance status, the presence of B symptoms, and advanced clinical stage. Several other similar studies also reported that high CA125 in NHL patients were associated with advanced clinical stage of disease, bulky disease, B symptoms, a greater number of extranodal sites, marrow involvement, pleural or peritoneal effusions, poor performance status and high LDH. They suggested that CA125 might be used as a marker to predict prognosis, and to detect advanced disease in NHL [7,1518,21]. In the present study, a positive correlation was found between CA125 and both LDH and ß2m. In agreement with these results, Bairey et al. [7] and Bonnet et al. [20] both reported that elevated serum levels of CA125 were found to correlate with high serum LDH levels and high serum ß2m levels. However, the majority of NHL patients die from disease progression, regardless of histological sub-type. The identification of pretreatment variables that correlate with response to therapy, duration of remission and survival should lead to the rational selection of initial Survival at 24 months was 78.2%. Patients with CA125 <20U/ml, LDH <310U/L, and ß2m <2µg/l all showed a statistically significant longer overall survival than those with higher levels (p-values = 0.006, 0.025, and 0.042, respectively). A shorter disease-free survival was associated with increased CA125 (p<0.001). Consistent with the results of this study, Batlle et al. [19] reported that a CR was achieved in 61% of patients with normal CA125 and in 45% of patients with elevated levels (p=0.033). Further-more, elevated serum CA125 at diagnosis was associated with shorter OS (p=0.025). Also, Abdolmonem et al. [17] , in their study reported that none of patients who had normal serum CA125 at diagnosis died of their disease during a mean follow-up duration of 9±4.1 months compared to 21.4% mortality (3/14) in those who had high levels (p=0.002). Wei et al. [18], as well, reported that the esti-mated 5.5year OS was 65% for patients with a normal CA125 level and 25% for those with an elevated serum level, a result which was statistically significant. Also, Bairey et al. [7] reported that normal serum CA125 levels at diagnosis had strong association with event-free and overall survival (p=0.01 and 0.003, respectively), while patients with increased levels had worse survival. Patients with high CA125 levels at diagnosis who achieved remission showed a significant decrease in CA125 levels in remission. Similarly, Jamal et al. [16] found in their study that complete response occurred in 86% of patients with normal CA125 levels and in 59% of patients with elevated CA125 levels. In both aggressive and low-grade NHL, the estimated 5-year overall survival rate was higher in patients with normal CA125 levels than in patients with elevated CA125 levels (88% versus 50% and 70% versus 27%, respectively). Bonnet et al. [20], as well, performed a univariate analysis; they found that high CA125 levels corre- 216 CA 125, a New Prognostic Marker for Aggressive NHL lated with poor performance status (PS). In his univariate analyses, OS and DFS were affected by poor PS, B symptoms, advanced clinical stage, bone marrow involvement, low Hb, high CRP or ß2-microglobulin levels. Age and abdominal involvement affected only DFS. CA125 level did not affect OS and DFS. On the other hand, Benboubker et al. [21] reported that with a median follow-up of 35 months, the significant univariate biological prognostic parameters for five-year overall survival of all patients in their study were found to be s-LDH level (p<0.0001), ß2m level (p=0.005) and sCA125 level (p=0.021). When they separated intermediate, high-grade NHL and low-grade NHL, sCA125 was not of prognostic value in the high-grade NHL group (p=0.63), but was predictive of five-year survival of patients with low-grade NHL (94% Vs. 53%; p=0.0012). Conclusion: CA125 was found to correlate with stage, tumor bulk, and involvement of more than 1 extranodal site, presence of effusion, response to therapy, and survival, which suggests that initial measurements of the antigen may provide prognostic information of value. CA125 showed high specificity, and LDH showed high sensitivity. Elevated levels of CA125, LDH, ß2m were found to predict decreased survival. These results indicate that serum CA125 level is frequently increased in a subgroup of patients with NHL and correlates with a poor outcome in patients with aggressive NHL. It appears more predictive for this subgroup of patients and we propose a new serologic prognostic index combining sCA125 and LDH levels in patients with aggressive NHL. More studies are recommended with a larger number of patients and with serial measurements of CA125 in addition to LDH. REFERENCES 1- Lazzarino M, Orlandi E, Klersy C, Astori C, Brusamolino E, Corso A, et al. Serum CA125 is of clinical value in the staging and follow-up of patients with non-Hodgkin’s lymphoma: Correlation with tumor parameters and disease activity. Cancer. 1998, 82: 576-82. 2- Kenemans P, Bast R, Yedima C, Price M, Hilgers J. CA125 and polymorphic epithelial mucin as serum tumor markers. Cancer Rev. 1988, 11: 119-44. 3- Bischof P. What do we know about the origin of CA125? Eur J Obstet Gynecol Reprod Biol. 1993, 49: 93-8. 4- Imai A, Itoh T, Niwa K, Tamaya T. Elevated CA125 serum levels in a patient with tuberculosis peritonitis. Arch Gynecol Obstet. 1991, 248: 157-9. 5- Halila H, Stenman UH, Seppala M. Ovarian cancer antigen CA125 levels in pelvic inflammatory disease and pregnancy. Cancer. 1986, 57: 1327-9. 6- Armitage JO. Treatment of non-Hodgkin’s lymphoma. N Engl J Med. 1993, 328: 1023-30. 7- Bairey O, Blickstein D, Stark P, Prokocimer M, Nativ HM, Kirgner I, Shaklai M. Serum CA125 as a prognostic factor in non-Hodgkin's lymphoma. Leuk Lymphoma. 2003, 44 (10): 1733-8. 8- The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N Engl J Med. 1993, 329: 987-94. 9- Zacharos ID, Efstathiou SP, Petreli E, Georgiou G, Tsioulos D, Mastorantonakis S, et al. The prognostic significance of CA 125 in patients with non-Hodgkin’s lymphoma. Eur J Haematol. 2002, 69: 221-6. 10- Mckelvey EM, Gottlieb JA, Wilson HE, Haut A, Talley RW, Stephens R, et al. Hydroxydaunomycin combination chemotherapy in malignant lymphoma. Cancer 1976; 38 (4): 1484-93. 11- Tempero MA, Uchida E, Takasaki H. Relationship of carbohydrate antigen 19-9 and Lewis antigen in pancreatic cancer. Cancer Res. 1987, 47: 5501-3. 12- Dawson-Saunders B, Trapp GT (editors). Basic and Clinical Biostatistics. Norwalk, Connecticut, Lange Medical Books, Appleton & Lange, 1994, p. 123. 13- Metz CE. Basic principles of ROC analysis. Semin Nucl Med. 1978, 8: 283. 14- Wiernik PH. Serum CA125 and PSA Concentrations in Patients with Lymphoma. Clin Adv Hematol Oucol. 2008, 6 (7): 527-31. 15- Dileki I, Ayakta H, Demir C, Meral C, Ozturk M. CA 125 levels in patients with non-Hodgkin lymphoma and other hematologic malignancies. (Clinical and Laboratory Haematology. 2005, Vol. 27, No. 1, pp. 51-55). 16- Jamal Zidan, Osamah Hussein, Walid Basher, Shmuel Zohar. Serum CA125: A Tumor Marker for Monitoring Response to Treatment and Follow-up in Patients with Non-Hodgkin’s Lymphoma. The Oncologist. 2004, 9 (4): 417-21. 17- Abdolmonem AM, Amany S, Maysa T, Saleh I, Saadia I. Serum CA 125; as a diagnostic and prognostic in paediatric lymphoma. J Med Sci. 2007, 7 (7): 11926. 18- Wei G, Yuping Z, Jun W, Bing Y, Qiaohua Z. CA125 expression in patients with non-Hodgkin’s lymphoma. Leuk Lymphoma. 2006, 47: 1322-6. Iman A. Abd El Gawad & Hanan E. Shafik 19- Batlle M, Ribera J-M, Oriol A. Usefulness of tumor markers CA125 and CA 15.3 at diagnosis and during follow-up in non-Hodgkin’s lymphoma: A study of 200 patients. Leuk Lymphoma. 2005, 46: 1471-6. 20- Bonnet C, Beguin Y, Fassotte M-F, Seidel L, Luyckx F, Fillet G. Limited usefulness of CA125 measurement in the management of Hodgkin's and non- 217 Hodgkin's lymphoma. Eur J Haematol. 2007, 78 (5): 399-404. 21- Benboubker L, Valat C, Linassier C, Cartron G, Delain M, Bout M, Fetissof F, et al. A new serologic index for low-grade non-Hodgkin's lymphoma based on initial CA125 and LDH serum levels. Ann Oncol. 2000, 11: 1485-91.