as a PDF
advertisement

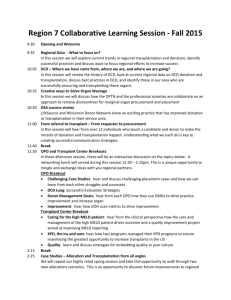
American Journal of Transplantation 2008; 8: 1282–1289 Blackwell Munksgaard C 2008 The Authors C 2008 The American Society of Journal compilation Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2008.02231.x Early Lung Transplantation Success Utilizing Controlled Donation After Cardiac Death Donors G. I. Snella, ∗ , B. J. Levveya , T. Otob , R. McEgana , D. Pilcherc , A. Daviesc , S. Marascod and F. Rosenfeldtd a Lung Transplant Service, Department of Allergy, Immunology and Respiratory Medicine, Alfred Hospital and Monash University, Melbourne, Australia b Department of Thoracic Surgery, Okayama University, Okayama, Japan c Intensive Care Unit, Alfred Hospital and Monash University, Melbourne, Australia d Department of Cardiothoracic Surgery, Alfred Hospital and Monash University, Melbourne, Australia ∗ Corresponding author: A/Prof G. Snell, g.snell@alfred.org.au Donation-after cardiac death (DCD) donor organs have potential to significantly alleviate the shortage of transplantable lungs. However, only limited data so far describes DCD lung transplantation (LTx) techniques and results. This study aims to describe the Alfred Hospital’s early and intermediate outcomes following DCD donor LTx. Following careful experimentation and consultation DCD guidelines were created to utilize Maastricht category III lung donors from either the ICU or operating room(OR), with a warm ischemic time(WIT) of <60 min. Between May 2006 and December 2007, 22 referred DCD donors led to 11 attempted retrievals after withdrawal, resulting in 8 actual bilateral LTx (2 donors did not arrest in prescribed period and 1 donor had nonacceptable lungs). ICU WIT = 38.4 min (range 20–54, OR WIT = 12.7 min (11–15), p < 0.05. Post-LTx, 1 pulmonary hypertensive patient required ECMO for PGD3. The mean group pO2/FiO2 ratio at 24 hours was 307.7 (240–507) with an ICU stay of 9.5 days (2–21) and ward stay of 21.5 days (11–76). All 8 survive at a mean of 311 days (10–573) with good performance status and lung function. In conclusion, the use of Maastricht category III lungs for human LTx is associated with acceptable early clinical outcomes. Key words: Donation referral, donor management, early graft function, lung transplantation, nonbeating heart donor Received 15 December 2007, revised 29 February 2008 and accepted for publication 2 March 2008 1282 Introduction Lung transplantation (LTx) is limited by the availability of transplantable donor lungs. Traditionally, donation-after brain death (DBD) donors have provided a vast majority of lungs for LTx, however donation-after cardiac death (DCD) donors are now being utilized for clinical transplantation (1–3). In theory this ‘new’ source of organs has great potential, but the description of outcomes is thus far limited to case reports and only small published series. In fact, even among the human DCD cases performed differing techniques of assessment, preservation and recovery have been used depending on the Maastricht category descriptor of the donor (Table 1) (4). Based on the local ethical and legal framework (5), an individual center will have commenced DCD LTx using a particular donor category. De Antonio and coworkers reported a series utilizing category I donors (6). They describe a 29% incidence of severe primary graft dysfunction (PGD) and a 69% 1-year survival. Steen reported the use of a single category II donor with good initial graft function, but death occurred from a nonrespiratory cause by 6 months (1). The successful use of category III donors has been reported in abstract form (7– 11) and anecdote (2,12), with our group recently publishing a case report detailing the technique and definitions (13). Category IV retrieval is limited to two positive case reports (14,15). On a world scale, the recent upsurge in DCD LTx activity in the area of category III donors is likely to continue. The organ transplant breakthrough collaborative has made DCD category III transplantation in general a US priority (16). Similar approaches by organ procurement organizations and individual LTx units in Australia, UK, the Netherlands and Canada are producing a similar result (17). Notwithstanding, detailed early and intermediate term outcome measures are yet to be published for category III donor lung transplants. This study aims to present the Alfred Hospital’s small series of early and intermediate term LTx results utilizing category III DCD donors. Based on this evolving experience, it becomes apparent that precise definitions, and the prospective recording of donor and recipient details and outcomes, are mandated to properly audit this ‘new’ advance. Early Lung Transplant Success from DCD Donors Table 1: Donation after cardiac death (DCD) donors: Maastricht workshop categories, as per (4) 1 2 3 4 Dead on arrival Unsuccessful resuscitation Awaiting cardiac arrest/cessation of futile treatment Cardiac arrest in brain dead donor absence of cardiac output and the start of cold flush preservation (13). In principle, the aim is to reduce the WIT as much as practical, but based on the existing literature (2) and our own experiments (18,19), we are prepared to accept lungs for transplant with a WIT less than 60 min. We note there is a second WIT that occurs at the time of lung implantation, but have deliberately excluded this from the definition (21). Donor assessment, recipient selection and donor/recipient matching Methods Creating an institutional guideline Prospectively, a large animal model was used to assess DCD donor LTx preservation and surgical techniques (18). The initial focus was on DCD lung-only recovery, but to optimize transplantation opportunities and efficiencies, DCD multiorgan recovery was also modeled (18,19). As detailed elsewhere (13), with the ultimate endorsement of numerous hospital and external agencies (specifically including the Alfred Hospital Ethics Committee), an Institutional DCD Guideline was created to cover in-house DCD lung-only recovery (20). A variation of this guideline was also formulated to facilitate lung recovery as part of a multiorgan DCD donor procedure from other institutions. Although the DCD donation process will be intrinsically directed by the general philosophical, practical and legal constraints of the donor hospital (5), it is notable that any LTx unit DCD guideline must consider specific lung requirements, parameters and management principles (Table 2). Unless specified, the warm ischemic time (WIT) was defined as the time between the Table 2: DCD lung donor management guidelines (1) General medical acceptance criteria and contraindications as per National Guidelines (42). The results of prior arterial blood gases and X rays must be known and interpreted. Calculation of the University of Wisconsin DCD Evaluation Tool score was sought where practical (12). (2) Specific lung DCD donor acceptance criteria a. Age <55 years b. PaO 2 > 300mmHg ( on FiO 2 1.0) c. Relatively normal chest x-ray d. Time for cardiothoracic recovery team to be on site before withdrawal (aim for >2 h to enable meeting with operating room, intensive care and other donor organ recovery surgical staff) (3) Specific lung DCD donor contraindications a. Prior thoracic surgery (4) Specific features of lung DCD donor pathway a. Protect airway via i. Aspiration of nasogastric (if present) prior to extubation ii. If possible withdraw treatment with endotracheal tube in situ, alternatively reintubate as soon as practical after death (may require skilled anesthetist if upper airway edema or trauma). Avoid pressure on abdominal organs until cuffed airway protection in place b. Administer heparin 50 000 IU as per local practice premortem, or if not possible, add to flush preservation solution post-mortem c. Ventilate donor 10 min after arrest (12) d. Donor bronchoscopy recommended e. In the event of late, unexpected operating room delay, consider topical cooling via pleural intercostal catheters to gain up to a further 6 h after death (1,18) American Journal of Transplantation 2008; 8: 1282–1289 We have described our Alfred approach to lung donor referral, assessment and general management elsewhere (22,23). DCD donor assessment attempted to incorporate the features of the University of Wisconsin DCD Evaluation Tool (12,13). Recipient selection is based on International Guidelines (24). Donor-recipient matching was generally undertaken according to our standard protocol, which has been described previously (23,25). Recipients chosen to receive DCD organs were particularly ill individuals at high risk of death on the waiting list. They had been generally consented about the use of extended donor organs (including DCD lungs), but following discussion with the Ethics Committee, specific consent for DCD transplantation was not required. Prospective donor-recipient T- and B-cell lymphocytotoxic cross-matching was performed in all patients. Lung procurement, preservation and transplantation Following reintubation of the donor after the 2 or 5 min stand-off time (as per local legal or administrative requirements), a rapid sternotomy and pulmonary arterial cannulation was initiated (Table 2). Subsequent lung preservation with Perfadex (Vitrolife, Goteborg, Sweden), lung recovery and transplantation followed standard practice (13,22,23,25). In order to avoid inadvertent cardiac stimulation, ventilation starts at 10 min after cardiac standstill (12). When participating in a DCD multiorgan recovery procedure the thoracic team assists the liver team with clamping of the thoracic aorta (19). At the time of lung implantation, a retrograde pulmonary venous flush and antegrade pulmonary artery flush are performed to remove any pulmonary microemboli. Postoperative management A postoperative fluid management regimen was instituted encompassing both respiratory and cardiovascular management algorithms and targeting a central venous pressure <7 mmHg, where mean arterial pressure and cardiac index permitted (26). The protocol provided an algorithm for early extubation where the ratio PaO 2 /FiO 2 was >200. PGD was defined and managed as per recent International guidelines (26,27). Triple immunosuppression was achieved, and acute rejection and bronchiolitis obliterans syndrome (BOS) were diagnosed and treated, according to standard protocols and practice (22,23,25,28). All patients received prophylactic antibiotics on the basis of known or suspected donor and recipient microbiology results. Ganciclovir was used as prophylaxis against CMV where indicated. Surveillance bronchoscopy and transbronchial biopsies were performed strictly according to protocol at 2, 4, 8,12, 26, 52 and 78 weeks post-LTx (25). Statistics Data were expressed as means unless otherwise stated. Comparisons were made between groups using the Fisher exact test for categorical variables, the unpaired Student’s t-test for parametric continuous data and the Mann-Whitney test for nonparametric continuous data. Results Between May 2006 and December 2007 there were 22 referrals of lungs from DCD donors from six hospitals. Eleven were considered but not taken further because: lungs were 1283 1284 28 55 18 26 26 16 17 36 4 5 6 7 8 9 10 11 Female Female Male Male Female Male Male Male Male Male Male Gender Local Local Interstate Interstate In-house Local In-house In-house In-house Interstate Interstate Site Hypoxia CVA MVA Hypoxia MVA MVA MVA MVA MVA MVA MVA Medical diagnosis 584 543 463 337 465 308 422 289 353 549 166 Last PaO 2 / ratio FiO 2 MVA = motor vehicle accident; CVA = cerebrovascular accident. 25 24 22 Age (years) 1 2 3 Donor no. Table 3: The demographics and features of the 11 potential DCD donors Lower lobe consolidation Midzone change Normal Normal Basal changes Basal changes Perihilar haze Apical changes Perhilar haze Normal Left basal collapse Chest x-ray appearance Minor Nil Blood Nil Blood Minor Minor Moderate Nil Nil Minor Airway secretions Extubation Cease inotropes Extubation Extubation Extubation Extubation Extubation Extubation Extubation Extubation Extubation Extubation Withdrawal mode 327 1355 1052 720 690 413 990 420 138 735 734 Time from referral-withdrawal (minutes) Lungs Lungs, liver, kidneys No donation in 90 minutes Lungs Lungs, kidneys Lungs Visualized lungs Not suitable No donation in 90 min Lungs, liver, kidneys Lungs, liver, kidney, pancreas Lungs, kidney Organs recovered Snell et al. American Journal of Transplantation 2008; 8: 1282–1289 Early Lung Transplant Success from DCD Donors Systolic blood pressure after withdrawal (mmHg) Actual donor 1 Actual donor 2 No donation <90mins Actual donor 3 Actual donor 4 Actual donor 5 Nonacceptable donor No donation <90mins Actual donor 6 Actual donor 7 Actual donor 8 250 200 150 100 50 Figure 1: The systolic blood pressure response after donor extubation in 11 potential DCD lung donors: 8 actual and 3 not realized. 0 0 medically not suitable (n = 4, consolidation, poor gas exchange, excessive smoking history), progressed to become brain dead (n = 4, 3 of which were ultimately recovered as DBD lung donors), donor legal or logistic issues (n = 2) and no suitable recipient (n = 1). Eleven potential DCD donors from five hospitals were considered acceptable on all criteria and a retrieval team was put in place (Table 3). The blood pressure response after donor extubation in these 11 donors is shown in Figure 1. On eight occasions suitable lungs were recovered (= actual donor) while two donors failed to arrest in the prescribed 90 min window (= no donation <90 min) and 1 donor arrested but the excised specimen was rejected after careful inspection (= nonacceptable donor). The actual time lines of lung recovery are shown in Figures 2 and 3. It can be seen that the ICU withdrawals typically had a longer WIT when compared to Operating Room withdrawals [38.4 min (range 20–54), versus 12.7 min (range 11–15), p < 0.05]. 5 10 15 20 25 30 35 40 45 Time (minutes) shown in Tables 4 and 5. Notably, airway complications and clinically significant acute allograft rejection (A grade >2) were not seen, with all patients completing the planned biopsy schedule. The detailed first 72 h PaO 2 /FiO 2 ratios are shown in Figure 4. Recipient three was supported on an extracorporeal membrane oxygenator (ECMO) for 60 h and therefore only T0 and T72 figures are available, while recipients 6,7 and 8 were extubated within the first day and without arterial blood gases beyond T24. The mean PaO 2 /FiO 2 ratio at T24 was 307.7 (range 240–507, excluding 1 patient on ECMO). The associations between the WIT and the PaO 2 /FiO 2 ratios at 24 h and the duration of ICU stay (essentially trends only given the small numbers) are shown in Figures 5 and 6 (p = not significant). Discussion The demographics, early and intermediate clinically important outcomes of the eight actual LTx recipients are This case series demonstrates very acceptable early and intermediate results from LTx using category III DCD donor lungs, thereby confirming and extending the previous case report, anecdotes and abstracts (7–12). Figure 2: The time line of lung recovery following withdrawal for ICU DCD donors. Figure 3: The time line of lung recovery following withdrawal for operating room DCD donors. American Journal of Transplantation 2008; 8: 1282–1289 1285 Snell et al. Table 4: Recipient demographics and outcomes from DCD donor lung transplantation Recipient no. Age (years) Medical diagnosis Gender 1 34 Female 2 57 Female 3 19 Female 4 63 Male Primary pulmonary hypertension Emphysema 5 6 7 8 Mean 60 38 23 42 42 Female Male Female Female Emphysema Cystic fibrosis Re-LTx BOS LAM Primary pulmonary hypertension Emphysema Pretransplant therapies/ features NYHA class Overall cold ischemic time (min) ICU stay (days) Ward stay (days) Survival (days) I.V. prostacyclin IV 368 14 17 633 BiPAP pCO 2 110 mmHg I.V. prostacyclin NYHA class IV BiPAP pCO 2 86 mmHg BiPAP - IV 600 7 16 515 IV 420 7 11 386 IV 376 18 76 350 IV III IV IV 609 548 560 459 443 21 4 2 3 9.5 11 11 13 17 21.5 303 129 112 65 311 I.V. = intravenous; NYHA = New York Heart Association; BiPAP = bilevel positive airway pressure support; BOS = bronchiolitis obliterans syndrome; LAM = lymphangioleiomyomatosis. To start DCD donor lung transplantation in an organ donation system unfamiliar with DCD transplantation in general has taken a significant amount of effort and time formulating guidelines and educating staff. However, despite only a small number of Australian hospitals currently set up to contribute DCD donors, at present we have been referred one donor per month. Eight of 22 (36%) have converted to actual lung transplants, consistent with our institutions high overall acceptance rate for DBD donors (22,23). One additional donor (5%) was not matchable for size and a further 3 (15%) of these 22 potential DCD donors became DBD donors. These results are consistent with those published by Olson et al. on the impact of DCD donation on DBD numbers, and indicate a DCD program contributes additively to the overall organ donor pool, with a minimal impact on potential thoracic organ recovery. The current series describes scenarios where the withdrawal of donor support occurs in ICU and in the OR. We note advantages and disadvantages of both approaches but, as has been found previously (12,13,29,30), either approach is feasible and should simply reflect local sensitivities and practicalities. In our opinion, multiorgan DCD recovery is somewhat complex, requiring rapid vascular access for abdominal organ perfusion, and is best managed with an OR withdrawal. On the other hand, the more relaxed time frames of lung-only recovery allow an ICU withdrawal, a situation that caters better to the sensitivities of family and staff, particularly if there is a distinct possibility cardiac arrest might not occur in the requisite 90-min window. There are minor technical issues specifically related to multiorgan DCD transplantation that are described elsewhere (12,19), but clinical results appear satisfactory either way. Table 5: Early and intermediate outcomes from DCD donor lung transplantation Recipient no. Early clinical issues 1 2 PGD 2 No 3 PGD 3 ECMO Basal collapse Deconditioned Basal collapse Deconditioned No No No 4 5 6 7 8 Intermediate clinical Airway issues complication Any cause readmission Highest rejection grade# 3 month %Predicted FEV 1 Best %Predicted FEV 1 Current BOS status Current overall status A1,B0 A1,B0 59 117 100 127 0 1 Alive, NYHA I Alive, NYHA I A1,B0 76 84 0 Alive, NYHA I No 15% late fall in FEV 1 No No No No No Yes FEV 1 fall No No No CMV colitis A0,B2 60 78 0 Alive, NYHA I No No No A0,B0 95 104 0 Alive, NYHA I No No No No No No No No Nausea A0,B0 A1,B0 A0,B0 103 62 N/A 113 62 66 0 0 0 Alive, NYHA I Alive, NYHA I Alive, NYHA I PGD = Primary Graft Dysfunction; ECMO = extracorporeal membrane oxygenator; FEV 1 = forced expiratory volume in 1 second; NYHA = New York Heart Association; N/A = patient not yet reached this point, # see (23, 30). 1286 American Journal of Transplantation 2008; 8: 1282–1289 Early Lung Transplant Success from DCD Donors PaO 2/FiO2 ratio Warm ischemic time (minutes) 700 60 Recipient 1 600 Recipient 2 500 Recipient 3 400 Recipient 4 300 Recipient 5 50 40 30 R2 = 0.39 Recipient 6 200 Recipient 7 100 Recipient 8 20 10 0 T0 T6 T12 T18 T24 T48 T72 Time (hrs) post LTx 0 0 100 200 300 400 500 600 Recipient PaO2 /FiO2 ratio at 24 hours post-LTx Figure 4: Recipient PaO 2 /FiO 2 ratios for the first 72 h postLTx. The assessment of DCD donors remains challenging. Firstly, the predictability of a cardiac arrest within the protocol defined 90 min is important for DCD lung recovery in general, with real concerns about family and staff perception, and the tying up of precious Operating Room time and surgical staff if the process does not proceed to donation. We experienced two such events at interstate hospitals from the 11 realistic donors we have considered. The University of Wisconsin DCD Evaluation Tool (12) is considered to aid this process, but we have found calculations of a specific value to be impractical. The DCD Evaluation Tool suggests the single greatest predictor of subsequent early postextubation arrest is the absence of spontaneous ventilation, but not all ICU staff are willing to test for this, with concerns about family sensitivities and the potential to provoke donor distress or hemodynamic instability. The DCD Tool also suggests that the cessation of inotropic support in a patient requiring it will lead to a shorter agonal period (12). The data in Figure 1 support this: a lower withdrawal systolic blood pressure predicts earlier arrest. Figure 5: The association between the PaO 2 /FiO 2 ratios at 24 h and WIT. significantly beyond 60 min) may require reconsideration of this strategy. The definitions of WIT become very important as DCD LTx enters routine clinical practice and LTx units attempt to compare the outcomes of varying techniques and ischemic injury therapies (13). Indeed, there are a number of theoretical but practical therapies, aimed at preventing PGD, which should be considered in clinical DCD LTx practice today. Potential novel strategies include DCD donor premortem treatment with N-acetyl cysteine (32) or surfactant (33) or preimplantation treatment with nitroglycerin (34), nitric oxide (35) or surfactant (36). The definitions of DCD transplantation and WIT are also relevant when attempting to cross compare different types of DCD donor, for example: category III versus category I. Our numbers are too small, and the patient group too heterogeneous to draw any solid conclusions, but Figures 5 and 6 at least raise Warm ischemic time (minutes) The second challenge for DCD donor assessment relates to the detail of local clinical DCD guidelines. Indeed, with theoretical concerns about ‘interventions’ on a patient who is yet to die, the initial lung assessment may be limited to historical data without bronchoscopic evaluation or even arterial blood gases on standard settings (5,20,23). Moreover, as distinct from the DBD circumstance, the DCD donor can aspirate stomach contents in the agonal phase or even post mortem (related to simultaneous abdominal organ recovery) (17–19), and there is the added but poorly characterized deleterious effect of variable warm ischemia prior to cold flush preservation (2,18). Although immediate pre-LTx graft performance could potentially be assessed by ex vivo lung perfusion (1,18,31) or the measurement of IL-1beta in donor bronchial lavage fluid (32), our DCD team have elected to use our standard DBD medical and surgical clinical assessments. Extended WIT DCD lung donors (i.e. American Journal of Transplantation 2008; 8: 1282–1289 60 50 40 30 R2 = 0.29 20 10 0 0 5 10 15 20 25 ICU stay (days) Figure 6: The association between the duration of ICU stay and WIT. 1287 Snell et al. the possibility that WIT may influence clinical outcomes. The exact point of onset of a relevant ischemic allograft injury, and the tolerable duration of WIT, is yet to be determined, but for lungs appears beyond 60 minutes. Although there have been significant numbers of DCD donor renal transplants performed over the years, clear WIT definitions have not been reached (21,38). Therefore, we encourage individual LTx units to record critical time-points, including the timing of systolic hypotension, cardiac arrest, ventilation reinstitution and the onset of cold flush perfusion (13). With careful database management, hopefully at an international level, the clinical correlations of warm ischemia can eventually be explored. These DCD donors have contributed 16% extra transplants beyond the cadaveric LTx performed over the same period, translating to at least equal results at this point for these 8 individuals at high risk of waiting list mortality. Unquestionably, the next test for DCD donor lungs relates to their potential to develop premature chronic allograft rejection or BOS. On the one hand the ischemic allograft may create an inflammatory milieu that leads to fibrosis and graft loss (2). Alternatively, the absence of the ‘brain storm’ inflammatory injury associated with DBD donors (2), the low rate of acute rejection so far noted, and the very reasonable absolute values of lung function already seen at 3 months in this small cohort, may even prove protective given these are known associations of chronic lung rejection (39). Furthermore, the solid and comparable long-term (10 year) outcomes from renal DCD transplantation bode well (40). The only other series of extended results of DCD donor LTx describes outcomes using 17 category I donors (6). There are differences in the nature of the ischemic injury, with donors in their series having up to 15 min without a circulation and thereafter external cardiopulmonary resuscitation (mean WIT 118 min, 95%CI 44–192) until conversion to hypothermic ECMO and topical cooling (mean preservation time 181 min, 95%CI 88–274). The results of this approach include PGD grade 3 in 29% [compared with our 13% in our DCD series and 18% in our overall DBD cohort (41)], 82% 1 month survival (our series 100%), 23% Grade >A2 rejection (our series 0%), 12% bronchial stenoses (our series 0%) and 7% BOS at 1 year (our series has insufficient data to comment). Overall, it is apparent that category I DCD transplantation is clearly very challenging to initiate and resource, and our work suggests category III DCD transplantation appears a simpler option, and at least as successful. In conclusion, the use of Maastricht category III lungs for human LTx is associated with very acceptable early clinical outcomes. Lungs can be recovered from scenarios where the withdrawal of treatment in the donor takes place in either the ICU or Operating Room, and irrespective of the recovery of other organs for transplantation. The absolute clinical limit of useable lung WIT is unknown, but is at least 60 min. Graft WIT definitions and documentation are impor1288 tant in auditing and cross-comparing results. Although longterm LTx outcomes (particularly BOS) using DCD lungs are yet to be characterized, it is now justifiable to use these organs to facilitate LTx opportunities for our waiting list patients. Acknowledgments The authors acknowledge the support of Australian Rotary Health Research Fund, Margaret Pratt Foundation, Rotary Club of Williamstown and Alfred Foundation. References 1. Steen S, Sjoberg T, Pierre L, Liao Q, Eriksson L, Algotsson L. Transplantation of lungs from a non-heart-beating donor. Lancet 2001; 357: 825–829. 2. Van Raemdonck DE, Rega FR, Neyrinck AP, Jannis N, Verleden GM, Lerut TE. Non-heart-beating donors. Semin Thorac Cardiovasc Surg 2004; Winter 16: 309–321. 3. Egan TM. Non-heart beating donors in thoracic transplantation. J Heart Lung Transplant 2004; 23: 3–10. 4. Kootstra G. Statement on non-heart-beating donor programs. Transplant Proc 1995; 27: 2965.E 5. Snell GI, Levvey BJ, Williams TJ. Non-heart beating organ donation. Intern Med J 2004; 34: 501–503. 6. de Antonio DG, Marcos R, Laporta R et al. Results of clinical lung transplant from uncontrolled non-heart-beating donors. J Heart Lung Transplant 2007; 26: 529–534. 7. Erasmus MS, Van Der Bij W, Verschuuren EAM. Non-heart-beating lung donation in The Netherlands: The first experience. J Heart Lung Transplant 2006; 25(Suppl): S63. 8. Love RB, D’Alessandro AM, Cornwell RA, Meyer KM. Ten year experience with human lung transplantation from non-heart beating donors. J Heart Lung Transplant 2003; 22(Suppl): S87. 9. Butt TA, Aitchison JD, Corris PA, Wardle J, Clark S, Dark JH. Lung transplantation from deceased donors without pre treatment. J Heart Lung Transplant 2007; 26: S110. 10. Van Raemdonck DV, Verleden GM, Dupont L et al. Initial experience with lung transplantation from non-heart-beating donors. J Heart Lung Transplant 2008; 27: 198–199. 11. Mason DP, Murthy SC, Budev MM, Mehta AC, McNeil AM, Pettersson GB. Early experience with lung transplantation using donors after cardiac death. J Heart Lung Transplant 2008; 27: 199. 12. Edwards J, Mulvania P, Robertson V et al. Maximizing organ donation opportunities through donation after cardiac death. Crit Care Nurse 2006; 26: 101–115. 13. Oto T, Levvey B, McEgan R et al. A practical approach to clinical lung transplantation from a Maastricht Category III donor with cardiac death. J Heart Lung Transplant 2007; 26: 196–199. 14. Oto T, Rowland M, Griffiths AP et al. Third-time lung transplant using extended criteria lungs. Ann Thorac Surg 2007; 84: 642–644. 15. Shennib H. Discussion on Egan TM et al. A strategy to increase the donor pool: Use of cadaver lungs for transplantation. Ann Thorac Surg 1991; 52: 1120–1121. 16. Punch JD, Hayes DH, LaPorte FB, McBride V, Seely MS. Organ donation and utilization in the United States, 1996–2005. Am J Transplant 2007; 7(5 Pt 2): 1327–1338. 17. Dark J. Personal communication. 2007. 18. Snell GI, Oto T, Levvey B et al. Evaluation of techniques for lung transplantation following donation after cardiac death. Ann Thorac Surg 2006; 81: 2014–2019. American Journal of Transplantation 2008; 8: 1282–1289 Early Lung Transplant Success from DCD Donors 19. Snell G, Levvey B, Oto T et al. Effect of multiorgan donation after cardiac death retrieval on lung performance. Aust New Zealand J Surg 2008; 78: 262–265. 20. Ryan G. Bayside Health Clinical Guideline: Donation after cardiac death. Available from http://intranet.baysidehealth.org.au/ assets/contactfile/1/DonationaftercardiacdeathGlineRev2.pdf Accessed 26/2/8. 21. Halazun KJ, Al-Mukhtar A, Aldouri A, Willis S, Ahmad N. Warm ischemia in transplantation: Search for a consensus definition. Transplant Proc 2007; 39: 1329–1331. 22. Gabbay E, Williams TJ, Griffiths AP et al. Maximizing the utilization of donor organs offered for lung transplantation. Am J Respir Crit Care Med 1999; 160: 265–271. 23. Snell GI, Griffiths A, Macfarlane L et al. Maximizing thoracic organ transplant opportunities: The importance of efficient coordination. J Heart Lung Transplant 2000; 19: 401–407. 24. Orens JB, Boehler A, de Perrot M et al. A review of lung transplant donor acceptability criteria. J Heart Lung Transplant 2003; 22: 1183–1200. 25. Esmore DS, Brown R, Buckland M et al. Techniques and results in bilateral sequential single lung transplantation. The National Heart & Lung Replacement Service. J Card Surg 1994; 9: 1–14. 26. Pilcher DV, Scheinkestel CD, Snell GI, Davey-Quinn A, Bailey MJ, Williams TJ. High central venous pressure is associated with prolonged mechanical ventilation and increased mortality after lung transplantation. J Thorac Cardiovasc Surg 2005; 129: 912–918. 27. Christie JD, Carby M, Bag R, Corris P, Hertz M, Weill D. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part II: definition. A consensus statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant 2005; 24: 1454–1459. 28. Snell GI, Westall GP. Immunosuppression for lung transplantation: Evidence to date. Drugs 2007; 67: 1531–1539. 29. Olson L, Kisthard J, Cravero L et al. Livers transplanted from donors after cardiac death occurring in the ICU or the operating room have excellent outcomes. Transplant Proc 2005; 37: 1188–1193. 30. Johnson SR, Pavlakis M, Khwaja K et al. Intensive care unit extubation does not preclude extrarenal organ recovery from donors after cardiac death. Transplantation 2005; 80: 1244–1250. American Journal of Transplantation 2008; 8: 1282–1289 31. Aitchison JD, Orr HE, Flecknell PA, Kirby JA, Dark JH. Functional assessment of non-heart-beating donor lungs: Prediction of posttransplant function. Eur J Cardiothorac Surg 2001; 20: 187–194. 32. Rega FR, Vanaudenaerde BM, Wuyts WA et al. IL-1beta in bronchial lavage fluid is a non-invasive marker that predicts the viability of the pulmonary graft from the non-heart-beating donor. J Heart Lung Transplant 2005; 24: 20–28. 33. Rega FR, Wuyts WA, Vanaudenaerde BM et al. Nebulized N-acetyl cysteine protects the pulmonary graft inside the non-heart-beating donor. J Haert Lung Tarnsplant 2005; 24: 1369–1377. 34. Boglione M, Morandini M, Barrenechea M, Rubio R, Aguilar D. Surfactant treatment in a non-heart-beating donor rat lung transplantation model. Transplant Proc 2001; 33: 2554–2556. 35. Egan TM, Hoffmann SC, Sevala M, Sadoff JD, Schlidt SA. Nitroglycerin reperfusion reduces ischemia-reperfusion injury in nonheart-beating donor lungs. J Heart Lung Transplant 2006; 25: 110– 119. 36. Takashima S, Koukoulis G, Inokawa H, Sevala M, Egan TM. Inhaled nitric oxide reduces ischemia-reperfusion injury in rat lungs from non-heart-beating donors. J Thorac Cardiovasc Surg 2006; 132: 132–139. 37. Nonaka M, Kadokura M, Takaba T. Effects of initial low flow reperfusion and surfactant administration on the viability of perfused cadaveric rat lungs. Lung 1999; 177: 37–43. 38. Sohrabi S, Navarro A, Asher J et al. Agonal period in potential nonheart-beating donors. Transplant Proc 2006; 38: 2629–2630. 39. Estenne M, Maurer JR, Boehler A et al. Bronchiolitis obliterans syndrome 2001: An update of the diagnostic criteria. J Heart Lung Transplant 2002; 21: 297–310. 40. Bernat JL, D’Alessandro AM, Port FK et al. Report of a National Conference on Donation after cardiac death. Am J Transplant 2006; 6: 281–291. 41. Oto T, Griffiths AP, Levvey BJ, Pilcher DV, Williams TJ, Snell GI. Definitions of primary graft dysfunction after lung transplantation: Differences between bilateral and single lung transplantation. J Thorac Cardiovasc Surg 2006; 132: 140–147. 42. Australasian Transplant Coordinators Association. National Guidelines for Organ and Tissue Donation. 2006; Available from http://www.atca.org.au/files/ATCAguidelines Accessed 15/9/07. 1289