T h e o f f i c i a l m a g a z i n e o f T h e a m e r i c a n S o c i e T y f o r h e a lT h c a r e e n g i n e e r i n g
• f a l l 2 0 15
insideASHE
www.ashe.org
EARN CEUs
WhilE READiNG
INSIDE ASHE
learn more
on page 8
1
Co Sp
mm ec
feat issi ial Se
ur o ct
Ins ed in t ning ion!
ide his i Ins
s
Pa AS sue o ider
ge HE f
4
of facility operations
We make data big™.
These days, everyone’s making a big deal of big data. But the fact is, Automated Logic has been putting
analytics to work in buildings for more than 30 years. We design and develop intuitive, intelligent,
complete controls that make it easy for building owners and managers to understand data, make
decisions and balance efficiency with occupant comfort. We are a world leader in energy solutions, and
in making data simpler, we make it big.
We make data big.
Next level building automation engineered
to help you make smart decisions.
automatedlogic.com
© Automated Logic Corporation, 2015. All rights reserved.
insideASHE
06 Letter from the President
08 What’s New
recognizes outstanding
10 ASHE
members, facilities with awards
By David A. Dagenais, BS, CHSP, CHFM, FASHE
ASHE at a glance
By Deanna Martin
if? Thinking through
15 What
emergency scenarios
By Dave Schonfelder, BS, CHFM, CHSP
FALL 2015
the future of health care:
36 Securing
A hospital’s approach to alternate
energy solutions
By Benjamin S. Blankenship, CHFM
39 Member Spotlight
41 Commissioning Insider
62 Advertisers’ index
matter: Understanding patient
18 Words
vicinity and patient space
By Krista McDonald Biason, PE
Joint Commission collaborate
21 ASHE,
on compliance resources
By Deanna Martin
delivery models,
22 Changing
changing needs: Energy
management in smaller facilities
Linda Dickey, RN, MPH, CIC
18
Commissioning
Insider
How ASHE’s commissioning process
can reduce costs and create more
efficient facilities
By Robin M. Laub
24
and acquisitions: Reducing
24 Mergers
the cost of facility operations in the
changing health care landscape
By Edmund Lydon, MS, CHFM, SASHE
value of complete and accurate
28 The
fire protection and life safety
documentation in health care
By Dale Wilson, RA, AIA
overtime costs: Different
32 Controlling
solutions for different facilities
By John R. Franks, CHSP, CHFM
operations cost reduction
34 Facility
through best practices
Beginning on page 41
36
By Nick Burke, PE
insideASHE
is the official quarterly publication of
the American Society for Healthcare
Engineering of the American
Hospital Association
155 N. Wacker Drive, Suite 400
Chicago, IL 60606
P: 312-422-3800, F: 312-422-4571
www.ashe.org, ashe@aha.org
ASHE PRESIDENT
David A. Dagenais, BS, CHSP, CHFM, FASHE
Director of Plant Operations/Security
Wentworth/Douglass Hospital
ASHE STAFF
Senior Executive Director
Dale Woodin, CHFM, FASHE
dwoodin@aha.org
Deputy Executive Director of Advocacy
Chad E. Beebe, AIA, SASHE
cbeebe@aha.org
Deputy Executive Director of Operations
Patrick J. Andrus, MBA, CAE
pandrus@aha.org
Director, Administration and Governance
Sharon Autrey, MPA, CAE
sautrey@aha.org
Director, Leadership Development
Tim Adams, FASHE, CHFM, CHC
tadams@aha.org
Communications Manager and
Inside ASHE Managing Editor
Deanna Martin
dmartin@aha.org
For a complete staff list, please go to
www.ashe.org/about/staff.html
PUBLISHED BY
5950 N.W. First Place
Gainesville, FL 32607
800-369-6220
www.naylor.com
Publisher: Jack Eller
Editor: Heather Williams
Project and Sales Manager:
David Freeman
Advertising Lead: Chris Zabel
Marketing: Cayla Degen
Design and Layout: Dan Proudley
Advertising Sales: Loren Burney,
Anook Commandeur, Krys D’Antonio,
Shaun Greyling, Debbi McClanahan,
Jacqueline McIllwain, Beth Palmer,
Marjorie Pedrick, Debbie Phillips,
Vicki Sherman, Matthew Yates
For advertising inquiries, please contact
Chris Zabel directly at 352-333-3420.
To submit editorial content for review,
please contact Deanna Martin directly
at 312-422-3819.
©2015 ASHE, all rights reserved.
The contents of this publication may not be
reproduced in whole or in part, without the
prior written consent of ASHE.
PUBLISHED SEPTEMBER 2015
ENV-Q0315 • 1202
An interactive
digital version of
insideASHE
is available at
www.ashe.org
www.ashe.org 5
Letter from the President
T
David A. Dagenais, BS,
CHSP, CHFM, FASHE
ASHE President
Director of Plant
Operations/Security
Wentworth/Douglass Hospital
Dover, New Hampshire
his summer, ASHE held its 52nd Annual Conference and Technical Exhibition
in Boston. As a native of the Northeast, I was proud to attend this event as
ASHE president, to see familiar faces, and to reconnect with our members.
Most importantly, I was proud that the event provided our members the
education and networking needed to thrive in a challenging health care climate.
Several sessions at this year’s Annual Conference were focused on operational
excellence. These sessions provided information on how to lower operating
costs and find more efficient ways to provide safe, healing environments for our
patients. This edition of Inside ASHE is also focused on reducing the cost of facility
operations. You’ll find articles on reducing energy costs, using health system
integration to create efficiency, reducing overtime staffing, and more.
In addition, this edition contains a special section on commissioning, a process
that can save resources and create efficiency. ASHE’s two books on the health
care commissioning process—both available at www.ashestore.com—can
provide further information and step-by-step instructions on how to use the
commissioning process to reduce costs.
To help hospitals reduce utility costs, which are one of the biggest expenditures
for most facility departments, ASHE created
the Energy to Care benchmarking and awards
program. We’ve seen tremendous growth in the
program this year, with more than 1,000 facilities
participating. Congratulations to the facilities that
won 2015 Energy to Care Awards by reducing
energy use. And for those of you who aren’t
familiar with the program or who haven’t used it
to help track and reduce utility costs, I encourage
you to visit
www.energytocare.com to learn more and
sign up.
Facility professionals are involved in
many aspects of health care, but reducing
operational costs is a critical part of our jobs. Our
organizations are counting on us to help in this
area, and I hope the ideas presented here spark your interest and spur you to find
your own solutions. When you do, consider sharing your ideas with fellow ASHE
members by submitting your own article (you can do that at www.ashe.org/
publish). By sharing information—whether it’s through articles and publications
or discussions at the Annual Conference—ASHE members can continue to help
each other as we work to meet the challenges of tomorrow.
“Facility professionals are involved
in many aspects of health care, but
reducing operational costs is a critical
part of our jobs. Our organizations are
counting on us to help in this area,
and I hope the ideas presented here
spark your interest and spur you to
find your own solutions.”
Sincerely,
6 inside ashe | Fall 2015
What’s New
ASHE at a glance
Scholarship supports continuing education for members
A
new scholarship is providing continuing education funding for
facility professionals and others involved in optimizing the health
care physical environment. ASHE recognized the first group of
recipients of the Ilse B. Almanza Scholarship at its 52nd Annual Conference
and Technical Exhibition in Boston. The scholarship paid the way for 12
ASHE members to attend the conference and benefit from education and
networking opportunities.
ASHE created the scholarship in memory of Ilse Almanza, ASHE’s
longtime education planner who for years helped develop, plan, and deliver
education to ASHE members.
“Ilse had a passion for lifelong learning that inspired all of us who knew
her,” said ASHE Senior Executive Director Dale Woodin, CHFM, FASHE. “We
created the scholarship to honor her memory and to provide continuing
education for others.”
ASHE is now accepting donations to help fund the Ilse B. Almanza
Scholarship and provide continuing education opportunities in the
future. Organizations looking for a way to demonstrate their commitment
to the field of health care facility management can learn more at
www.ashe.org/scholarship.
ASHE expands member resources with help
from thought leaders
A
SHE is working with several organizations with expertise in the health
care facility management field to help expand member benefits
and resources.
Many of the new resources will help ASHE members reduce operational
costs through energy efficiency. ASHE is working with power management
company Eaton, for example, to add more how-to guides to the Sustainability
Roadmap for Hospitals website (www.sustainabilityroadmap.org), which
provides free, practical, vendor-neutral tools to help health care facilities
reduce their environmental footprints and reduce costs. In addition, Eaton will
author two new management monographs on energy efficiency and power
reliability, which will be reviewed and published by ASHE. Each monograph will
be followed by a webinar, available to ASHE members at no charge, to provide
additional information and allow for questions and answers.
ASHE’s new relationship with Eaton follows a model that has previously
shown success. For years, Trane has sponsored a number of ASHE programs
including ASHE’s Leadership Institute, which helps develop new leaders
within the ASHE membership. Johnson Controls, meanwhile, is sponsoring
ASHE’s Energy to Care, an energy benchmarking and awards program.
Schneider Electric partnered with ASHE to develop a national internship
program that supports ASHE’s succession planning strategic imperative.
Grainger and Caterpillar recently sponsored live streaming from ASHE
conferences so members could, at no cost, watch certain sessions without
traveling to the conference.
8 inside ashe | Fall 2015
Earn continuing education
units through Inside ASHE
A
SHE members can earn free
continuing education units by
reading this fall 2015 edition of
Inside ASHE and passing a quiz based on
articles in this issue. Those wishing to
earn 0.1 CEU (1 contact hour) from the
American Hospital Association should
follow these instructions:
1. Read this edition of Inside ASHE and
understand the articles.
2. Go online to www.prolibraries.com/
ashe and create a ProLibraries account
if you have not already done so.
3. Click on “Continuing Education” in
the left column to access and take the
online quiz.
4. Members who pass the quiz will be
able to print a CEU certificate for 1
contact hour (0.1 CEU).
Step-by-step instructions for
registering with ProLibraries are available
at www.ashe.org/insideasheceus.
Eligibility information
• To earn CEUs through the fall 2015
edition of Inside ASHE, you must be
an ASHE member as of Sept. 1, 2015.
Members who joined after that
date will not be eligible for CEUs
through Inside ASHE until the winter
2015 edition.
• Quizzes for this edition must be
completed by Dec. 1, 2015. After that
date, the quiz will no longer
be available.
Tree Branch
SW7525
SoftTop® Seamless Resinous Flooring
Every one of our acute care solutions
has a unique name.
At Sherwin-Williams, our professionals like Chris understand that you need high performance coatings, an appealing environment and positive patient experiences. Our people can recommend a wide
range of solutions to help you meet performance, budget and deadline requirements and reduce
repaint cycles.
Take advantage of our expertise in the healthcare market and discover our wide range of products for
walls, floors, roofs and concrete surfaces. swhealthcaresolutions.com
©2015 The Sherwin-Williams Company
Feature
ASHE recognizes outstanding
members, facilities with awards
By Deanna Martin, ASHE communications manager
A
t its recent Annual
Conference and Technical
Exhibition, ASHE
recognized members
and facilities doing
outstanding
work to optimize the health care
physical environment.
Personal awards and accomplishments
The Crystal Eagle award, considered
ASHE’s “lifetime achievement” award, was
presented to Michael Kuechenmeister,
FASHE, CHFM, CHC, director of plant
operations at West Chester Hospital in
West Chester, Ohio. Kuechenmeister
has contributed to the field through his
work in health care safety, advocacy, and
energy efficiency. He became a nationally
recognized leader in helping several
southern hospitals stay open during
Hurricane Katrina.
The President’s Award, which is
presented at the discretion of the sitting
ASHE president to an individual who goes
above and beyond to optimize the health
care physical environment, was presented
to Walt Vernon, CEO of the national
consulting and engineering firm Mazzetti.
ASHE also recognized members
who attained senior (SASHE) and fellow
(FASHE) status within ASHE. The following
members are new SASHE recipients:
• Donna Craft, RN, MHA, SASHE,
Premier, Inc., Huntersville, NC
• David Dierking, MBA, CHFM, SASHE,
Edward Hospital, Naperville, IL
• Ralph Graham Jr., CHFM, SASHE,
University of Alabama, Birmingham, AL
• Gary Hamilton, PE, LEED-AP, SASHE,
SmithGroupJJR, Washington, DC
• Eric Herrera, CHFM, SASHE,
Memorial Hermann Hospital, Katy, TX
• John Holderman II, CHFM, CHC,
SASHE, St. John Health System,
Tulsa, OK
10 inside ashe | Fall 2015
ASHE President David A. Dagenais, BS, CHSP, CHFM, FASHE (at right), presents the Crystal Eagle
Award to Michael Kuechenmeister, FASHE, CHFM, CHC.
• Sean Mulholland, PE, CHFM, CHC,
SASHE, Penrose/St. Francis Health
Services, Colorado Springs, CO
• Hank Schuurman, CHC, SASHE,
Christian Health Care Center, Wyckoff, NJ
• Dana Swenson, PE, MBA, SASHE,
UMass Memorial Health Care System,
Worcester, MA
The following members are new
FASHE recipients:
• Steve Cutter, MBA, HFDP, CHFM,
FASHE, Dartmouth-Hitchcock Medical
Center, Lebanon, NH
• Bert Gumeringer, CHFM, FASHE,
Texas Children’s Hospital, Houston, TX
• Richard Parker, FACHE, CHSP, FASHE,
Tucson Medical Center, Tucson, AZ
• Walt Vernon, PE, FASHE, Mazzetti,
San Francisco, CA
ASHE leaders also announced
the following emerging regional
leaders from each of ASHE’s 10
regions. The Emerging Regional
Leader award recognizes people for
their contributions to the fields of
health care engineering and facilities
management; planning, design, and
construction; safety; clinical and
biomedical engineering; and technical
management.
• Region 1: Paul Cantrell, Jr., CHFM,
Concord Hospital, Concord, NH
• Region 2: James Walsh, CHFM,
Atlanticare Regional Medical Center,
Pomona, NJ
• Region 3: David Murray, CHFM, High
Point Regional/UNC Health Systems,
High Point, NC
• Region 4: Donald Stewart, CHFM,
Florida Hospital East, Orlando, FL
• Region 5: Jo Ellen McCarthy,
CHEP, Shriners Hospital for Children,
Cincinnati, OH
continued on page 12
IT’LL PROBABLY BE
TAKEN FOR GRANTED.
We’re okay with that.
One look at the new and innovative Meridian™ Series from Scotsman and
you’ll see why constantly monitoring your ice machine is a thing of the past.
Intuitive diagnostics. Quick front panel access. And an exclusive QR code. All
working together inside one of the industry’s smallest operational footprints.
So it’s easy to see how such a reliable ice machine might never be the center
of attention. But isn’t that the point? See more at scotsman-ice.com/meridian.
TM
ST
JU
D
SE
A
LE
RE
• Region 6: Phillip Nelson, CHFM,
Buena Vista Regional Medical
Center, Storm Lake, IA
• Region 7: Casey Miranda,
Jackson County Memorial
Hospital, Altus, OK
• Region 8: Carol McCormick,
CHFM, CHI Health, Omaha, NE
• Region 9: Michael Cooper,
CHFM, Kaiser Permanente,
Modesto, CA
• Region 10: J. Brett Dille, Weiser
Memorial Hospital, Weiser, ID
12 inside ashe | Fall 2015
690157_Dynalock.indd 1
Energy to Care Awards
ASHE also recognized more than 20
hospitals for earning Energy to Care
Awards for their work to slash energy
use, reduce operational costs, and free
up more resources for patient care.
The Energy to Care program,
sponsored by Johnson Controls,
encourages hospitals across the country
to reduce their energy consumption by
10 percent or more over their baseline
energy consumption. Since 2009,
hospitals participating in the Energy to
15/05/14 6:26 PM
Care program have tracked more than
$67 million in energy savings.
ASHE congratulates the following
hospitals for their leadership in
reducing energy consumption:
• Carolinas HealthCare System
Behavioral Health-Charlotte,
Charlotte, NC
• Carolinas HealthCare System Blue
Ridge Morganton, Morganton, NC
• Carolinas HealthCare System
Lincoln, Lincolnton, NC
• Carolinas HealthCare System
Pineville, Charlotte, NC
• Caromont Regional Medical
Center, Gastonia, NC
• Indiana Regional Medical Center,
Indiana, PA
• Excela Health Latrobe Hospital,
Latrobe, PA
• Excela Health Westmoreland
Hospital, Greensburg, PA
• Hardin Memorial Hospital,
Elizabethtown, KY
• Memorial Hermann Memorial City
Medical Plaza 3, Houston, TX
• Memorial Hermann Northeast
Medical Plaza 1, Humble, TX
• Memorial Hermann Prevention
and Recovery Center, Houston, TX
• Memorial Hermann Southeast
Hospital, Houston, TX
• Memorial Hermann Southwest
Heart and Vascular Institute,
Houston, TX
• Memorial Hermann Sugar Land
Medical Plaza 1, Sugar Land, TX
• Memorial Hermann The
Woodlands Medical Plaza 2, The
Woodlands, TX
• Memorial Hermann TIRR,
Houston, TX
• Mercy Hospital Lebanon,
Lebanon, MO
• Midland Memorial Hospital,
Midland, TX
• Swedish Covenant Hospital,
Chicago, IL
• UF Health Shands Cancer Hospital,
Gainesville, FL
• UF Health Shands Psychiatric/
Rehab Hospital, Gainesville, FL
• UW Hospitals and Clinics,
Madison, WI
To learn more about ASHE’s award
programs or to apply, visit
www.ashe.org/about/awards.
All the capabilities you want...
and some you may not have considered!
Custom Designed and Built
Power Control Systems
With mission-critical data and life safety at stake, why would you try to
make do with a standard catalog power control system? Why would
you settle for a less than optimal solution?
Don’t compromise. Insist on a powerful, flexible, fully-integrated
Russelectric Power Control System... custom-designed and built
with your specific needs and wants in mind. Russelectric will custom
tailor a power control system that not only provides all the operating,
monitoring, and reporting capabilities you want, but one that is intuitive
and easy to use because it is based on your way of doing things. And
because Russelectric specializes in custom systems, we can often
suggest features and capabilities you never even considered.
1-800-225-5250
russelectric.com
An Employee-Owned Company / An Equal Opportunity Employer
ME
EGApleat M8
®
Just what
the doctor
ordered.
MEGApleat M8
®
SAVE TIME AND MONEY WITH FEWER FILTER CHANGES
Longest Service Life
Strongest Construction
Reduced Energy Costs
Guaranteed
KVJ\TLU[LKOPNOLZ[K\Z[
OLH]`K\[`NHS]HUPaLK
SV^VWLYH[PUNYLZPZ[HUJL
JVUZPZ[LU[WLYMVYTHUJL
OVSKPUNJHWHJP[`VMHU`
L_WHUKLKTL[HSNYPKHUK
TLHUZSLZZLULYN`YLX\PYLK
JLY[PÄLKI`PUKLWLUKLU[
MERV 8^PYLIHJRLK
TVPZ[\YLYLZPZ[HU[HKOLZP]L
[VTHPU[HPUHPYÅV^
[OPYKWHY[`[LZ[SHIVYH[VY`
WSLH[LKÄS[LY
^^^HHÄU[SJVT
LUZ\YLK\YHIPSP[`
BETTER AIR IS OUR BUSINESS®
?
Member to Member
What if?
Thinking through
emergency scenarios
By Dave Schonfelder, BS, CHFM, CHSP, director of engineering,
Children’s Health System, Dallas, Texas
I
f there is one certainty today, it is that we live in a changing world full of
uncertainty. In health care we often focus on emergency preparedness drills
that anticipate an influx of patients and utility outages. To further stretch
my staff, I encourage my engineering leadership staff to think through other
“what if” scenarios on a weekly basis. The exercises help think through various
crisis scenarios and their possible outcomes. Consider asking the following
questions at your next meeting.
How easily will your team be able to manage solutions to the possible scenarios?
Q. What if U.S. satellites or Internet
access were knocked out?
Without satellite or Internet
connections, the methods in which
health care is provided would have to
be significantly altered. Think about all
the ways your facility uses a wireless
connection to the outside world. The
workplace is increasingly “paperless,”
and we rely heavily on computers,
phone systems, atomic clock systems,
biomedical equipment, out-patient
record keeping systems, personnel
actions and files, training systems,
and many more processes that require
remote access to digital information. If
the computers were rendered useless,
could preventative and corrective
maintenance processes continue to
operate in your facility? Could the
buildings be managed without the
building automation systems and the
facilities be operated or managed
without Internet service?
Q. What if the building lost power?
Consider the effects of buildingwide power loss. Discuss whether
the hospital has more than one
independent electrical feed, or how
long the facility can run on generator
power before the generator needs
to be refueled. What services should
be curtailed during prolonged power
outages? What equipment is connected
to the critical and life safety branches?
Should personnel be rotated using
12-hour shifts? Consider where the
facility generators are located; are
they on the lowest floor level of
the hospital? Will the generators be
affected by flooding water? Consider
the more mundane but very important
functions that require power: Has the
construction design team installed
sinks with sensors that rely on power
to operate? How many sinks become
useless when power is lost?
Q. What if we lose natural gas?
Will the boilers automatically transfer
to fuel oil? What departments are
affected? If dietary’s cooking equipment
burns gas, what back-up systems and
plans do they have? Will building steam
pressure be lost and affect sterilization?
How is natural gas used for dishwashers
in the dietary department, building
humidification systems, and hot water
heating systems?
Q. What if the hospital lost
incoming water?
Another scenario to talk through
would be loss of incoming water. Does
the facility have two independent water
feeds? Many hospitals use vendors
to supply back-up bottled water. Fire
departments often offer tankers to
back feed the hospital; if such is the
plan, are the correct connections in
place? Would backflow of water disturb
the sediment in the pipes and cause
brown water conditions? Does the
staff know where the exterior water
shutoff valves are in the event of a
broken main caused by a frost break
or by contractor digging operations?
Q. What if an event occurs on an
upper floor and wing?
Consider the implications of an event
occurring in an upper floor or wing of
the facility. How would the location
affect the contingency plan? Are there
isolation valves in place to prevent the
shutoff of the entire hospital or building?
Can a floor or wing’s power or water be
continued on page 16
www.ashe.org 15
isolated from the system? If spring rains
come so fast that the rivers fill and the
creeks back up, and the city storm drains
back up and the hospital sump pump
system eventually falls behind, how
will this water build up affect the boiler
room—boilers, chillers, generators,
chilled water circulation pumps, hot
water heaters, soft water tanks, and
more? At what point should boiler rooms
be shut down: when the breakers are
tripping or when combustion air intakes
cut off because of rising water?
Q. What if staff in the military
reserves are called up for active duty
or key staff are lost to retirement or
natural attrition?
The question regarding military
reserves will affect some facilities more
than others. If the facility employs
a significant number of staff in the
reserves, how would the loss of the
reserve staff affect facility operations?
What functions are particularly
vulnerable? Are skilled replacements
easy to find?
AcornVac
Makes it Possible.
Our Vacuum Plumbing Systems offer a versatile
engineered plumbing and waste solution.
Gravity Plumbing
Vacuum Plumbing
A Cleaner Flush
Tests conducted by NSF International comparing two
common types of gravity toilets to AcornVac’s vacuum toilets
showed that:
r)TCXKV[VQKNGVURTQFWEGFdetectable levels of
overspray and bacteria on the toilet seat and in
the area surrounding the toilets
r#EQTP8CEoUXCEWWOVQKNGVUUJQYGFno detectable
overspray or bacteria on the toilet seat or in the
area surrounding the toilet.
www.acornvac.com
Member of Morris Group International
13818 Oaks Avenue, Chino, CA 91710
Tel. 800-591-9920
16 inside ashe | Fall 2015
684027_AcornVac.indd 1
Leadership should also think through
how the loss of staff for any reason
could impact the facility. Functions such
as water chemical treatment, monthly
generator runs, managing building
automation systems or computerized
maintenance management systems,
managing and running the physical
plant, and other essential systems
require knowledgeable back up. Within
leadership, a strong second in command
is essential; is there a trustworthy
replacement if the head of the hospital,
department, or function is absent for
any reason?
Q. What if an earthquake rattles
the hospital?
In the event of an earthquake, at what
point does the facility require inspection
for structure damage? (With a 3, 4, or 5
on the Richter scale?) The facility should
have a thorough earthquake inspection
checklist. Does the checklist include
inspection of the incoming natural gas
meter area, any sky bridges, or expansion
joints in the facility? Does the inspection
need to check for particular damage on
the upper floors of the facility?
An event such as an earthquake can
present additional challenges. Who
on the team is designated to handle
communication of the event? What form
of communication would be available? Is
an incident command center necessary?
Who is to be notified and kept informed
during the event: departments affected,
infection control, senior leadership, the
safety officer? What kind of contractor
support would be necessary? Would
additional security be required?
It is a good exercise to ask staff these
challenging questions. While emergency
preparedness drills are conducted
twice annually, you can review “what
if” scenarios any time, such as at your
monthly departmental meetings.
By reviewing these scenarios at our
weekly meetings, my team and I are not
interfering with emergency preparedness
coordinators’ plans; rather we are making
our response to disasters stronger,
strengthening our team, and spurring
cooperation and teamwork. These benefits
not only help an organization during a
disaster, but they can help improve staff
morale and retention.
03/03/14 3:47 PM
ENTERTAIN
EDUCATE
&ENGAGE
Customized video
distribution solutions
for your healthcare
environment
www.z-band.com/healthcare
Learn More: 866-902-2606
758915_ZBand.indd 1
28/07/15 4:48 pm
759408_UVResources.indd 1
www.ashe.org 17
8/8/15 3:35 PM
Feature
Words matter:
Understanding patient
vicinity and patient space
By Krista McDonald Biason, PE, associate vice president, HGA Architects and Engineers
I
f there is one thing I have learned
while dealing with codes, it is that
words do matter. A simple word
like “shall” means something
very different than the phrase
“shall be permitted,” a distinction
that if missed often leads to confusion
regarding implementation of a code.
One of the more prevalent
misunderstandings I see is the
interpretation of patient vicinity versus
patient care space. Both include the word
18 inside ashe | Fall 2015
“patient,” so they mean the same thing—
right? Wrong. “Patient vicinity” is defined
in NFPA 99: Health Care Facilities Code
and reiterated by Article 517. 2 in NFPA
70: National Electric Code® (NEC) as “a
space, within a location intended for the
examination and treatment of patients,
extending 1.8 m (6 ft) beyond the normal
location of the patient bed, chair, table,
treadmill, or other device that supports
the patient during examination and
treatment and extending vertically to
2.3 m (7 ft, 6 in) above the floor.” So,
in simple terms, the patient vicinity is
the area within the wingspan of the
patient. This definition is intended not
only for inpatient functions but also
for outpatient services, and is not just
limited to a hospital bed location.
In contrast, the patient care space has
a much broader range of coverage. The
NEC definitions for spaces are derived
from the NFPA 99 definitions of “patient
care rooms.” NFPA 99 defines the general
“Why does a clear understanding of patient vicinity and patient care
space matter? Like everything else in the code, these terms are used in
other sections to inform and implement additional criteria.”
description of “patient care room” with
the same words that 517.2 uses for
“patient care space” as “space within a
health care facility wherein patients are
intended to be examined or treated.”
The patient care space encompasses
the patient vicinity—but is not limited to
the wingspan parameters of the vicinity
definition. The article provides further
information to clarify basic care spaces,
general care spaces, critical care spaces,
and support spaces. The categories
of spaces define the range of risk to
patients or caregivers from “not likely
to cause injury” to “likely to cause major
injury or death.” NFPA 99 also provides
Annex material, which is additional
explanatory material regarding the space
(room) criteria. (As a side note, I always
pause when I read these definitions.
Not every profession can say they make
decisions based on a potential outcome
of “major injury or death.”)
Why does a clear understanding of
patient vicinity and patient care space
matter? Like everything else in the code,
these terms are used in other sections
to inform and implement additional
criteria. Where the definition of patient
care space and vicinity really affect the
electrical design and construction of
a facility is in the wiring requirements.
Article 517.20 of the NEC indicates that
the wiring and protection requirements
of 517 apply to patient care spaces of
all health care facilities. Article 517.13
further indicates that wiring in patient
care areas shall comply with 517.13(A)
and (B). Section (A) indicates the branch
circuits serving the area “shall be provided
with an effective ground-fault current
path by installation in a metal raceway
system, or a cable having a metallic
armor or sheath assembly.” Section
(B) requires an insulated equipment
grounding conductor. This means that
the entire defined patient care space
(not just the vicinity) is required to have
a redundant ground path. The intent
of this requirement is to eliminate the
opportunity for the patient to be the
“ground path.” (Another side note: NFPA is
working on alignment between codes to
eliminate the word “area” and instead use
the word “space.” Again, words matter.)
Even though the patient care space is
defined in 517.2, the code throws in grey
area by adding informational note number
1 to the definition (which is not enforceable
but is provided for additional clarity): “The
governing body of the facility designates
patient care space in accordance with the
type of patient care anticipated and with
the definitions of the area classification.”
NFPA 99 also includes similar verbiage
requiring the governing body of the facility
or their designee to designate specific
patient care rooms, but the NFPA 99
requirement is within the main code text so
this criterion is enforceable.
The informational note in NFPA 70
(and the Annex article in NFPA 99) does
exclude business offices, corridors,
lounges, day rooms, dining rooms, or
similar areas as not being required to
be classified as patient care spaces. Be
mindful that some jurisdictions do require
critical branch receptacles in corridors
(which is above and beyond NFPA code
requirements and the FGI Guidelines) with
the concept that in the case of a major
catastrophe, patients might be brought
into the corridor for care. A hospital is
a defend-in-place facility, and during a
tornado patients and staff should move to
an interior space and away from windows.
With this particular interpretation, the
corridor would become a patient care
space and the determination would be in
direct contrast to the informational note
that a corridor is not a patient care space.
After all of the code verbiage has been
evaluated and regurgitated, the owner’s
preferences and the engineer’s opinions
are what define the installation criteria
for a particular project. When working
with a facility to define or enhance the
requirements for health care wiring in
and around a “patient care space,” as the
engineer I consider the type of facility
that is being designed or remodeled. Any
amount of experience in a health facility
or with health care design or installation
will demonstrate that the areas of a
health care facility are often fluid and
subject to remodeling.
Using both health care and non-health
care wiring as strictly defined by the
code verbiage concurrently in the same
space limits the ease of remolding and
repurposing existing infrastructure. If the
project scope is a complete renovation
and replacement of existing conditions,
then wiring isn’t as significant an issue
because everything will be demolished
and removed. If the scope is to add a
patient toilet or an exam room within an
existing space previously not identified
as “patient care,” then wiring will need to
be replaced or the facility will risk ending
up with a non-compliant installation. This
error often occurs when a small project
is implemented by an entity that does
not have health care expertise. For large
projects with a significant scope of work,
the upcharge for the health care wiring
isn’t usually significant compared to the
time required to map out what is and
is not defined by the governing body
of the facility as a health care space. By
maintaining consistent health care wiring
standards within a designated space,
confusion can be avoided during the
original installation, and there will be
additional flexibility for future changes.
Wiring methodology should be a
discussion point among team members
to ensure compliance with the code,
maintenance of the facility, and sensitivity
to the project budget.
One last thing to remember is
that the items in the code book
are minimum requirements to
protect health and life safety. They
do not necessarily include the
requirements from the engineer
in his/her specifications or any
additional requirements from the
authority having jurisdiction that
may be more stringent.
www.ashe.org 19
TM
FlexCart Facility Engineering Cart
Increased productivity • Tools and parts inventory control • Compact, light, maneuverable
• Impressively professional
Special, low pricing for ASHE members is being made available through Grainger.
Refer to Part#: 35XR82 and Cost Support Contract #: 2438ASHE1 to receive these savings.
www.flexcartllc.com • 614-348-2517 • Go to grainger.com or search “FlexCart”
Feature
ASHE, Joint Commission collaborate
on compliance resources
By Deanna Martin, ASHE communications manager
A
SHE is collaborating with
the Joint Commission on an
exciting new project that
will provide resources and
tools to help hospitals
comply with life safety
and Environment of Care requirements.
“The facility and building systems
play a vital role in creating the healing
environment,” said ASHE Senior
Executive Director Dale Woodin, CHFM,
FASHE. “Consistent compliance with
the Environment of Care and life safety
standards is an excellent indicator high
reliability in building systems. ASHE
is proud to collaborate with the Joint
Commission to provide focused tools
and resources to assist organizations in
achieving compliance and high reliability.”
The Joint Commission has identified
its top eight physical environment
standards that are frequently cited
during surveys of hospitals and
other health care facilities. The Joint
Commission has created an online
physical environment portal to house
its resources related to these top issues.
ASHE will be providing resources—
including tools, best practices, and
technical documents—on its new
Focus on Compliance webpage at
www.ashe.org/compliance.
“The Joint Commission is very
pleased to join with ASHE to offer
the Physical Environment Portal,”
said Mark R. Chassin, MD, FACP, MPP,
MPH, president and CEO of the Joint
Commission. “We created this portal
in response to customer needs,
identified through 10 focus groups
with customers and surveyors. As the
national leader in patient safety and
health care improvement, we felt it
was very important that each module
be readily available at no charge to
anyone seeking this information.”
Every two months, ASHE and
the Joint Commission will focus on
a new standard, with the previous
information archived on this page
to create a library of compliance
resources. The schedule (at left)
outlines when resources will be
available for each of the eight
standards.
PHySICAL ENVIRONMENT PORTAL SCHEDULE
July 2015
Introduction and announcement of collaboration
August/September 2015
Utility systems (EC.02.05.01)
October/November 2015
Means of egress (LS.02.01.20)
December 2015/
January 2016
February/March 2016
Built environment (EC.02.06.01)
Fire protection (EC.02.03.05)
April/May 2016
General requirements (LS.02.01.10)
June/July 2016
Life safety protection (LS.02.01.30)
August/September 2016
Automated suppression systems (LS.02.01.35)
October/November 2016
Hazardous materials and waste management (EC.02.02.01)
Quality
Healthcare
Lighting
Solutions
Bringing Buildings to Life
Services:
• Transition Planning
• Buildings Commissioning
• FreightTrain® Software
hew.com/healthcare
751052_HEWilliams.indd 1
www.consultHTS.com
8/5/15 4:59
678304_HTS.indd
AM
1
www.ashe.org 21
28/01/14 6:13 PM
Feature
Changing delivery models, changing needs:
Energy
management
in smaller facilities
By Robin M. Laub, healthcare strategic account manager, Northeast, Schneider Electric
A
wave of technological
changes in the health
care industry has driven
rapid change across the
continuum of care. From
diagnosis to treatment
to insurance, technology has enabled a
new level of personalized care.
Health care delivery models are also
changing—in recent years, health care
providers have been expanding their
network of services by opening remote
satellite clinics and offices, often by
renovating commercial office spaces
into health care facilities. The trend
toward retail health care, combined with
mergers and acquisitions, has resulted in
health care enterprises having to operate
dozens and sometimes hundreds of small
remote facilities equipped with little or
no energy control capabilities, except
for simple thermostats. For health care
providers who are striving to meet the
demand from consumers for lower-cost
and more accessible health care, these
types of facilities make good business
sense. But this rapid growth means that
health care enterprises are forced to
accept whatever environmental controls
come with the building.
These smaller, off-site outpatient
clinics, which include ambulatory care
centers and diagnostics and medical retail
sites, often operate in pre-existing spaces
22 inside ashe | Fall 2015
and storefronts that were not purposebuilt for health care. For example, a
hospital may open an urgent care center
in a space that was previously used
for retail. This scenario creates hurdles
because of the environmental regulations
and requirements that must be in place
in health care facilities to ensure patient
comfort and health. Room temperature,
air quality, humidity levels, and lighting
can all directly affect patients. For
laboratories that store bacteria cultures
or blood and urine samples, these
environmental factors are equally critical
to ensure accurate test results.
Further compounding the issue
is the Affordable Care Act’s (ACA)
system of reimbursement, whereby
reimbursement rates are adjusted
based on patient satisfaction levels.
Meant to add incentive for health care
facilities to ensure patient satisfaction
and comfort, the ACA reimbursement
system presents an additional hurdle
for retail health care facilities to deliver
quality care and operate effectively.
While building controls may seem
like a small factor in the broader
satisfaction equation, they present a
significant opportunity for satisfaction.
According to a 2011 report from the U.S.
General Services Administration, green
buildings—buildings that use structures
and processes that are environmentally
friendly and energy efficient—have
a 27 percent higher rate of occupant
satisfaction. Installing intelligent building
controls and upgrading building systems
can directly affect health care outcomes.
Energy management at smaller
facilities provides a considerable
opportunity to reduce operating costs
and improve financial health. The U.S.
Department of Energy stated in its 2011
Advanced Energy Retrofit Guide that
health care facilities’ energy spending is
three times that of typical commercial
buildings, totaling approximately $8.8
billion a year on energy expenditures.
This spending can be reined in with the
help of a holistic system through which
to monitor and control the facility. For
example, heating, ventilation, and air
conditioning (HVAC) can be set back, or,
as in the case of lighting, turned off in
unoccupied rooms or when the whole
facility is closed after business hours.
To address the energy management
and patient satisfaction challenges
in smaller facilities, health care
organizations should consider
implementing a series of applicationspecific room controllers. Room
controllers introduce a new level of
control to a building and provide
myriad options to reduce spending and
ensure comfort. Their features include
occupancy sensors, door and window
IMAGE COURTESY OF SCHNEIDER ELECTRIC.
sensors, lighting control, carbon dioxide
ventilation control, and advanced
programming. A single device can
automatically adjust HVAC and lighting
settings according to a preset schedule
based on a facility’s business hours. The
device can also adjust settings based
on room occupancy, further reducing
wasteful energy consumption. Similarly,
the room controllers ensure all settings
remain within an established range,
so that room temperature is never
extremely hot or cold, and air quality is
constantly monitored.
For added insight into building
operations, facility operators can
network room controllers into a building
management system (BMS). Traditionally
engineered for large commercial
buildings and large enterprises, BMSs
now come in many shapes and sizes.
By selecting a BMS right-sized for its
facility, a retail health care facility can
further use the features provided by the
room controllers. A BMS can generate a
real-time dashboard that compiles data
from all room controllers simultaneously,
painting a holistic picture of the building’s
energy use and occupancy rates. The
BMS can also provide alerts when faults
or abnormalities are detected in the
system, highlighting potential problem
areas that need to be maintained
or repaired. These small-scale BMS
systems can operate locally at a fantastic
value or they can be incorporated
into a larger enterprise system.
Incorporating a facility’s BMS into
a broader enterprise BMS is a perfect
solution for health care providers that
operate in multiple sites or branches.
This enterprise BMS can give a full
eagle-eyed view of all sites, ensuring
patient environments are consistently
comfortable across all locations. For
example, one nonprofit health care
provider installed application-specific
room controllers across three sites
and then installed an enterprise BMS,
resulting in a 35-percent energy savings
after just three months.
For health care facilities seeking to
add room controllers and a BMS, a typical
first step is identifying an area—for
example, one site, or even one room
within a site— to use as a test case.
Organizations should develop a shortterm plan for first benchmarking the
pilot area, then testing a room controller
and evaluating BMS integration.
Organizations should also consider
a long-term plan for measuring ROI
and mapping out energy savings
management and improvements as
other facilities are brought online.
Following the planning stage, facility
managers can hire a local electrician
to install room controllers in their test
area, which helps keep upfront costs
low. Facility managers can then evaluate
the room controller’s performance in
maintaining a comfortable environment
for health care delivery and patient
satisfaction and driving energy efficiency.
Patient satisfaction and comfort is at
the heart of health care delivery—it has
remained a constant as the health care
industry has shifted and expanded. As
health care increasingly occupies offsite
facilities not purpose-built for health
care, facility operators and managers
should consider room controllers and
a BMS to help ensure patients and
staff alike are provided a comfortable
environment. For networks operating
multiple clinics or facilities, an enterprise
BMS can provide a number of monitoring
and measuring capabilities to ensure the
network is running optimally, from both
a patient and energy standpoint.
www.ashe.org 23
Feature
Mergers and
acquisitions:
Reducing the cost of facility operations in
the changing health care landscape
By Edmund Lydon, MS, CHFM, SASHE, director of support services/facilities, Northeast Hospital Corporation
(Beverly Hospital, Adison Gilbert Hospital, and Bayridge Hospital) – a member of Lahey Health
T
he health care landscape
continues to change
as more and more
integrated health
systems emerge through
mergers, acquisitions, and
partnerships. Facility managers need to
understand the new business strategies
and to manage and provide services
with an open mind. Integrated systems
have produced positive changes that are
drastically improving the financial bottom
line. In following the national trend,
Northeast Health System, Winchester
Hospital, and Lahey Hospital and
Medical Center, formerly Lahey Clinic, in
Massachusetts, affiliated to form a new
integrated health care system called
Lahey Health. The system was formed
after years of extensive planning, due
diligence exploration, regulatory review,
and employee and physician discussions
and buy-in. I had the advantage of being
a part of the process and wrote this
article based on my experience to explain
some of the methods we used to help
successfully navigate becoming a health
system, and to offer suggestions for
facility professionals in similar situations.
The journey to create this health
system began some time ago with a
24 inside ashe | Fall 2015
vision to have a community-based health
care delivery system that would allow
growth and fulfill the mission to provide
quality community care locally at the
lowest cost possible to patients. The
affiliation between the three facilities
was spurred, in large part, to meet the
changes in the health care landscape,
including those caused by the Affordable
Care Act. As we anticipated the changes
to come, we quickly became aware of the
opportunities to leverage human capital,
purchasing power, and technology to
gain efficiencies that would change the
delivery of health facility services.
The creation of the Lahey Health
System required pulling together three
very different patient care delivery
models. Such a move can have its
challenges, and if not executed correctly
these challenges could impede the
performance of the newly formed
health care organization. Lahey Hospital
& Medical Center is a physician-led,
nonprofit group practice; Northeast
Health System is an integrated
community nonprofit health care system
comprised of a network of community
hospitals and behavioral health services,
long-term care, and human social service
providers; and Winchester Hospital is a
community hospital with ambulatory
centers and clinics. The good news was
that all three shared a focus on clinical
excellence, quality and safety, and
operational efficiency.
One of the most important factors
for a successful affiliation is recognition
that each organization has its own
cultures. We recognized this early
on and tried to keep the process as
transparent as possible with employees.
Treating transformation as an event
is the best approach, rather than
wandering into a mental, physical, and
emotional process; this is critical for
success when combining organizations.
According to an article by C.K. Goman
in 2000 titled, “The Biggest Mistakes
in Managing Change,” a large-scale
organizational change usually triggers
emotional reactions—denial, negativity,
tentative acceptance, commitment.
Leadership must understand these
reactions so they can facilitate the
emotional process; ignoring this
process could be at the peril of the
organizational transformation effort.
Another important aspect of
organizational change experienced
by Lahey Health was the change in
governance, hierarchy, processes,
and, most importantly, autonomy. The
leadership teams in each organization
have been and continue to be affected,
most often in a positive manner. The
newly formed organization understood
the importance of naming the new
hierarchy early in the process to ensure
that organizational direction stayed
intact. Newly formed system positions
were filled with leaders from each of
the organizations. Strategic hiring can
provide a level of relief to employees
who recognize the merger of multiple
organizations as a collegial process
rather than an “us-versus-them” scenario.
Experience has shown that it is best
for the newly formed organization to
announce the change in governance
quickly so leaders and staff are successful
in moving change forward. Such was
true with our facility management teams.
One organization came to the process
already with a vice president of facilities
and multiple facility leaders with varying
degrees of facility responsibilities and
titles. Recognizing the available human
capital, the vice president of facilities
moved into a system role to establish
leadership and structure by bringing
facility directors and managers together
from the various organizations within
the newly formed system. This surely
expedited the ability to leverage the
market in a unified front—one face,
one name now presenting as a large
integrated health system. Maintaining
three areas of focus can help create an
integrated facility team that reduces cost
and increases efficiencies for the newly
formed system.
continued on page 26
www.ashe.org 25
These areas are:
1. Value-based purchasing: Establish
a value-based purchasing process for
facilities materials and services across
the system to gain big results.
2. Human capital: Restructure work
within the facilities departments to
gain efficiencies.
3. Common identity: Develop a
common identity among the facility
managers to help secure and gain
market share. This is especially
important if one site or campus is
much larger than another.
Value-based purchasing
In our experience, facility managers
from various sites have recognized
that the new organization has created
leverage and increased buying power
with vendors, utilities, and contractors.
When suppliers and service providers
want your business, they will become
highly competitive. Securing business
“Health care has
always relied
heavily on strong
facility managers to
develop and support
physical spaces that
meet the needs of
service delivery.”
from a newly formed health care
system is highly desirable to vendors.
This “collaborative-based purchasing”
hinges on facility mangers breaking
down barriers to capture quick wins in
savings by creating new arrangements
and/or combining existing arrangements
for purchasing materials and services
with the creation of common product
and service lines. Such action can
include improving the purchasing
tier by identifying a common market
basket with a national supplier of facility
materials or competitively bidding
and contracting out the services of
large utility systems, such as vertical
transportation for the entire system.
Facility managers have become
a key part of the integrated health
care system by showing quick wins in
reducing cost to the new organization.
A facility manager’s ability to be flexible
and nimble in this new health care
environment is vital. If facility managers
cannot work together, the affiliation or
merger will flounder, and cost-effective,
quality patient care will not come to
fruition. Facility managers need to be
flexible and, in many cases, humble
directional change leaders for these
new organizations.
Human capital
Another important organizational
strategy is to ensure that the right
people—facility managers in this
case—are in the right locations to create
opportunities to capture and implement
change quickly and successfully. With
the appropriate steps, you can get
the right alignment and objectives.
26 inside ashe | Fall 2015
729279_PVI.indd 1
30/01/15 7:33 PM
People learn how to work across
geographic functional boundaries.
The insightful facility manger will
recognize where assets (property,
facilities, technology, etc.) should be
developed or changed in the various
geographic areas to meet the new
mission and vision of the organization.
A common value to purchasing
products and services among the facility
team(s) can lead to a strategic human
resource approach that shifts from
people-centered purchasing values to
the harder business-value approach
that is necessary to deliver efficiencies
and cost controls. Linking human
capital, in this case facility department
talent and skills, with organizational
strategic goals and objectives will
improve business performance and
develop an organizational culture within
system facility departments that will
foster innovation, flexibility, and even
competitiveness within the organization.
Facility managers who embrace and
become partners in the journey will
be successful in adjusting the delivery
of services and ensure that strategies
are in place to recruit, select, train, and
align personnel appropriately across the
system to meet new service demands.
Common identity
Lastly, facility managers need
to be seen as positive and effective
change managers within the ranks
of the transforming organization.
Health care is changing rapidly with
the move from fee for service to global
payment systems, accountable care
organizations; value-based purchasing,
pay for performance, at-risk contracts
with payers, and the need to cut waste
from the day-to-day delivery process.
These changes demand the need for
an efficient, culturally bonded, and
talented facility workforce.
Health care has always relied heavily
on strong facility managers to develop
and support physical spaces that meet
the needs of service delivery. Today’s
environments must support a wide
continuum of care that delivers safe,
efficient, and high-quality services at the
lowest cost to consumers. The facility
manager does all this while conforming
to the most stringent of regulations and
guidelines in any industry. Ours is no
small challenge!
As large integrated health systems
form to meet the needs of the new
health care delivery mandates, that
complexity will need to be met with a
workforce that is agile, embraces change,
can develop new competencies, and
is creative. Facility managers need to
prepare themselves for this paradigm
shift. We live, work, and compete in a
growing competitive health care market
that demands we be lean, efficient, and
flexible. The new health care market
will deliver more care locally in homes,
clinics, and outpatient facilities, and
hospitals, rather than the traditional
sense as we have known, which means
facility managers to be successful
need to adapt and be part of the new
delivery model. With this in mind, facility
managers need to move quickly to be a
part of the change ahead. If not, we risk
being left behind.
DO A FEW
MILS REALLY
MAKE A
DIFFERENCE?
MEMBRANE
THICKNESS
GUARANTEE
You bet they do. They can mean the difference between
going home a Superbowl champ and never wearing the
ring. Or the difference between a long lasting roof and one
that is less durable. So if you’re looking for superior, reliable
performance, you want the new Sarnafil Thickness Guarantee.
The roofing industry standard allows membranes to be
manufactured up to 10% below the advertised thickness,
which means your 60 Mil membrane could really be 54 mils
thick! But with our Thickness Guarantee, you get every mil
you pay for, guaranteed.
So don’t take a chance on your next roof.
Visit www.thicknessguarantee.com or call 800-576-2358
for Sarnafil Thickness Guarantee program details and to
see the difference a Sarnafil membrane can make. Because
a few mils can mean the difference between failure and a
performance that people will talk about for decades to come.
SIKA CORPORATION — ROOFING
Phone: 800-576-2358
usa.sarnafil.sika.com
759746_Sika.indd 1
www.ashe.org 27
7/31/15 3:57 AM
Feature
The value of complete and
accurate fire protection and
life safety
documentation in
health care
By Dale Wilson, RA, AIA, project manager, national
healthcare practice leader, Aon Fire Protection
Engineering Corporation
28 inside ashe | Fall 2015
T
he health care facility is one of the most regulated building
types in the United States, and with regulatory oversight
comes a great burden of proof to demonstrate that facilities
are in compliance with all applicable requirements. There
are also costs associated with compliance. How can a facility
use fire protection and life safety documentation to reduce
expenses, improve efficiency, increase awareness, and minimize deficiencies?
Fire protection and life safety management emphasize protecting
patients and occupants from the risks associated with fire by focusing
on the physical environment and facility operations. Responsibility
for the life safety environment is typically in the hands of the facility
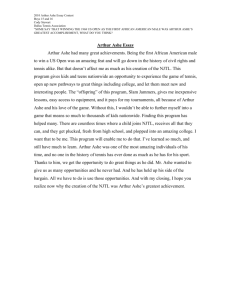
Equivalencies
and waivers
Fire safety
evaluation
system
Plans for
improvement
Interim life
safety
measures
Contracted
services
Fire Protection
and Life Safety
Documentation
Statement of
conditions
Age of
building
records
Construction
documents
Life safety
drawings
System
testing and
maintenance
records
These 10 items tend to be the primary fire protection and life safety-related records found within most
health care facilities. All of these records are important and have a specific purpose, along with a relative cost if not appropriately maintained.
management group. This team is
accountable for maintaining the
commercial property and equipment
through engineering services,
managing contractors and vendors,
and building upkeep. In addition,
they must oversee the associated
operational costs to provide a safe,
pleasing, and productive environment.
Whether a facility uses one person or
a team to manage life safety, there is
plenty of compliance documentation
to maintain. What information is
maintained, how it’s maintained,
and how long it is maintained can
have an effect on the overall success
of the facility’s performance.
The record keeping required in
health care is too extensive to list,
and the breadth of paperwork for the
facility management team is no less of
a challenge. To organize the content,
fire protection, and life safety record
keeping is divided into 10 primary
categories listed in the diagram above
in no particular order.
Fire protection and life safety
document overview
Contracted services include
items such as maintenance contracts,
engineering contracts, service
contracts, and employee contracts.
They provide contact information;
provider information; contract terms and
conditions; and a historical context for
parts, service, and warranty information.
Documents of this type should be
maintained for the duration of the
equipment or service.
Construction documents provide
a great deal of knowledge regarding
a building’s evolution, which is
important, since health care facilities
tend to undergo more changes
to the physical structure than any
other building type. Maintaining all
construction documents (paper or
electronic) offers a valuable historical
picture of a building’s transformation.
Important information that can be
found in these documents include
the name of the architect/designer,
materials and methods of construction,
relative code decisions, systems
diagrams, and spatial arrangements.
Life safety drawings provide a
visual snapshot of the facility’s fire
protection and life safety features. These
documents are essential for maintaining
accreditation. The life safety drawings
typically include important egress
information; locations of various fire
resistive barriers; vertical openings such
as shafts, stairs, or atria; non-sprinklered
areas of the building; and designated
hazardous rooms, smoke compartments,
and suites. More detailed plans may
include the locations of fire alarm and
fire sprinkler system devices, firefighting
equipment, fire extinguishers, fire door
ratings, exit capacities, or keyed notes
related to equivalencies and waivers.
System testing and maintenance
records provide requirements for the
continued performance of systems
and equipment as well as warranties,
operating procedures, installation
details, and product information. The
National Fire Protection Association
(NFPA) requires that these records
be kept until the next test and one
continued on page 30
www.ashe.org 29
Three New Healthcare
Lavatories to Meet Your Needs
Engineered with a 1,000-lb.
ZHLJKWUDWLQJDQGVSHFLÀF
features for bariatric
patients in healthcare
environments.
BHS-3123
Bariatric Healthcare Lavatory
Conceived to minimize
ligature points
for behavioral
healthcare
environments.
WBL-2320
Behavioral Healthcare Lavatory
2XUVWDLQOHVVVWHHOÁRRUPRXQWHG
WRLOHWLVVSHFLÀFDOO\GHVLJQHG
to reduce ligature points
and the use of the bowl
as a suicide device.
Shown with optional white
anti-bacterial gloss powder
FRDWHGHQDPHOÀQLVK
AS-ETWS-1490-FM-BS
Ligature Resistant Toilet
'HVLJQHGVSHFLÀFDOO\WR
minimize splashing and
reduce the spread
of infectious disease.
CSA Z8000 compliant!
WICS-2222
Infection Control Lavatory
Now we're even
easier to specify!
1.800.428.4065 TOLL FREE | www.willoughby-ind.com
30 inside ashe | Fall 2015
738537_Willoughby.indd 1
© 2015 Willoughby Industries Inc.
» ,QIRUPDWLRQVKHHWVDQG5(9,7ÀOHVDUHDYDLODEOHDWZLOORXJKE\LQGFRP
23/06/15 12:59 AM
year thereafter; however, best practice would suggest
maintaining these records for two accreditation (Centers for
Medicare & Medicaid Services/Joint Commission) cycles.
Age of building records is a simple document that
provides a map of the phases of the overall complex. It
condenses the numerous construction plans into a single
resource document. This document is an asset to confirm
compliance of existing buildings or systems with applicable
codes at the time of installation. Historical information found
in this document can possibly help avoid upgrading or
replacing building components through “grandfathering”—
confirming compliance of existing items with the applicable
codes at the time of construction.
Statement of conditions (SOC) is an assessment tool
used to help health care facilities identify deficiencies. The
SOC provides a current sketch of a facility’s state of Life
Safety Code® compliance to help the management team
develop a plan for improvement (PFI). The identification of
deficiencies helps manage corrective actions that can be
performed in-house, by outside services, or by determining
items that may require alternative approaches to
compliance. The SOC can also be of assistance in scheduling
tasks and allocating funds.
Plan for improvement is essentially the action plan to
correct any identified Life Safety Code deficiencies found
during the SOC survey. They are typically used for items
that are anticipated to take longer than 30 to 45 days to
correct because of the nature or complexity of the problem
or items that may require special funding. The PFI may
also include items that may not be resolved through an
equivalency or through a fire safety evaluation system
(FSES) analyses. A PFI typically includes a description of
corrective action for each deficiency with the anticipated
completion date, and should include the person(s)
responsible for the corrective action.
Equivalencies and waivers are accepted alternative
solutions recognizing that the intent of the code is met in a
manner different from what is prescribed by the applicable
code. These are usually substantiated or certified by a fire
protection engineer, architect, or the authority having
jurisdiction (AHJ). Equivalencies and waivers usually remain
with the facility until changes are made and can be affected
by additions or renovations. CMS offers categorical waivers
for certain code requirements often supported by new
editions of NFPA 101 that have yet to be adopted. Existing
equivalencies or waivers may be unknown to an AHJ during
the permit or inspection process, so they are important to
catalogue. Acceptance by one authority does not ensure
acceptance by another enforcement agency.
Fire safety evaluation system (FSES) is the more
formal type of equivalency. The FSES can be a practical,
economical, qualitative, and a quantitative solution for
compliance that might provide greater flexibility and lower
cost options in determining how to achieve Life Safety Code
compliance. This document should be updated regularly as
required by the AHJ, and following any major renovations
or improvements. The FSES helps demonstrate that a facility
provides a level of life safety protection
against fire that is equal to, or better
than, strict compliance with the
applicable NFPA 101 edition. The FSES is
particularly useful where conditions are
difficult or impossible to correct (e.g.,
widening existing stairways in existing
buildings, excessively long dead-end
corridors, or unrated shafts).
Interim life safety measures (ILSM)
outlines activities a facility will perform
to protect patients, staff, and visitors
during periods when the Life Safety
Code cannot be met and ILSM should
be implemented during temporary
situations (e.g., an exit is temporarily
unavailable because of renovations or
a fire protection system is temporarily
impaired). ILSM policies and procedures
must be in writing, should be updated
regularly, and staff should be made
aware of these procedures particularly
when implemented. Other aspects
of the ILSM include notifying the fire
department, posting signs, and/or
conducting a fire watch. Failure to do
these things can affect the facility’s
accreditation status.
Conclusion
As described, fire protection and life
safety in health care facilities require a
great deal of documentation. If given
the choice, presumably health care
management would rather spend
money on patient care, services,
or new equipment before building
maintenance or upgrades. Each of
the documents described herein
provides pertinent and valuable
information. If properly maintained,
made readily available, and kept
current, these documents will help
improve compliance, minimize
business disruption, and prevent
unnecessary spending. Current and
accurate fire protection and life safety
documentation can assist facilities
to achieve:
• Proper maintenance of relevant life
safety elements
• Only necessary work is performed
• The responsible party performs
the work
• Continued accreditation
• A better historical understanding of
the facility
• Proper mapping of the facility
• More accountability of staff, contractors,
and consultants
• More accurate and quantifiable data for
budgets and funding
• A staff that is better prepared for
inspections (particularly
unannounced visits)
• Improved communication between all
concerned parties
• Deficiencies are minimized and
corrected in a timely manner
• Most importantly, a safe environment
for patients, staff, and visitors
No single solution for maintaining all
of these records exists. Responsibility can
be assigned to various persons or a single
individual. A facility might even hire a
document controller. Other methods should
include keeping a maintenance calendar,
using third-party resources, maintaining
electronic forms, scanning paper
documents at regular intervals, creating and
managing checklists, conducting regularly
scheduled life safety meetings, updating
documents on a regular basis, and including
life safety plans as an attachment to every
construction or service contract.
Twice the Firestop Performance Half the Labor
L Rating<1 CFM
STC of 68
t Single Side Installation
t 100% Joint Movement
t UL 2079 Tested
t Lifetime Warranty
t1 & 2 Hour F Rating
for Gypsum Walls
TM
HEAD OF WALL FIRESTOP SYSTEMS
759303_RectorSeal.indd 1
www.ashe.org 31
29/07/15 6:03 pm
Feature
Controlling overtime costs:
Different
solutions for
different
facilities
By John R. Franks, CHSP, CHFM, director, facilities/safety,
CHI St. Luke’s Health—The Woodlands Hospital
F
acility managers continue to look
for ways to reduce facility budgets
as hospital budgets remain under
financial pressure from shrinking
reimbursements, increased medical
supply and equipment costs, and
increased costs for labor. Most facilities have
focused on energy conservation, and rightly
so, as these are direct costs and savings to
the bottom line. Another facet of controlling
facility expense budgets is managing staffing
levels and overtime. Finding capable and
trained FTEs (full-time equivalencies) is
increasingly difficult. Proper use of staff to
avoid overtime will help managers become
better stewards of limited resources. At the
same time they are asked to reduce costs,
managers are asked to ensure employee
32 inside ashe | Fall 2015
“By keeping departmental overtime ratios around 3 percent, the
facility manager shows his or her commitment to cost curtailment.”
engagement. There are ways to reduce
staffing and overtime costs and keep the
facility staff satisfied and engaged.
At CHI St. Luke’s Health—The
Woodlands Hospital, we have found
ways to significantly reduce our overtime
budget without sacrificing coverage.
When I arrived in 2008, we were not a
24/7 operation, and had an engineering
staff of seven working from 6 a.m. until
6 p.m. We had an engineer come in on
Saturday and Sunday for eight hours
each day to run the plant and perform
any necessary house calls. An additional
engineer was on-call for the hours the
weekend engineer was not present at
the hospital. An engineer worked the
weekend on overtime, which meant
an additional 16 hours of overtime was
being incurred every week in addition
to any call-ins that occurred during
that week. Of course, that was not a
sustainable model. After meeting with
the staff, we determined the best option
was to have the on-call engineer work
the weekend. The on-call engineer for
that period would take off work on a
Monday and then work 10 days straight
(Tuesday through the weekend and
finish on the following Thursday). He
or she would take that Friday off. The
engineering coming on call for the
following weekend would begin his
or her week on Tuesday, repeating the
process, with a total of five engineers
rotating according to this schedule.
This accomplished several things: We
avoided weekend overtime, gave the
engineer two three-day weekends, and
gave him or her the chance to take time
off if they had been called in during the
week. Each call-in would result in three
hours of overtime, even if the engineer
just came in to adjust a temperature. The
engineers were much more likely to take
the time off on a Saturday than go home
early during the week. We still required
the appearance of the engineer on the
weekend, to verify plant operations,
but if everything was under control,
they could leave early. This strategy has
worked very well for us, and the staff has
embraced the change. We also hired an
engineer to work second shift, from 2
p.m. until 10:30 p.m. This has eliminated
60 percent of the call-ins and provides
better coverage for the central plant.
Hospital staff also like having a facility
staff member available to resolve house
calls in a more timely manner.
Scott Reeves, CHFM, CHSP, CHEP,
manager for facilities, safety, and
emergency management at CHI St.
Luke’s Lakeside Hospital, manages his
staff a little differently for overtime.
Reeves has a smaller hospital (30 beds)
and a staff of two engineers. He allows
his staff members to set their own
schedules, as long as all of the work
gets done and he is kept aware of who
will be onsite. The two engineers work
together to take time off as required,
take calls, and provide coverage. At least
one engineer and/or Reeves is there
from 7 a.m. to 5 p.m. Staff are required to
coordinate time off so that all preventive
maintenance work is completed. They
plan surgery air handler and other critical
equipment shutdowns for weekends,
taking alternate days off so they can both
work on regular time. This system has
worked well for that location.
Larger facilities have additional
challenges that make self-scheduling
much more difficult. Richard Martinez
is director of facilities at CHI Baylor St.
Luke’s Medical Center campus. His facility
covers more than 1.2 million square feet
with 30 operating rooms and about 900
patient beds. The original hospital was
built in 1954, and a number of major
additions were added through the
years. Martinez has been focusing on
staffing and overtime reductions since
his promotion to director in 2013. He is
responsible for about 63 facility staff. In
2012 and 2013, the department logged
more than 2,581 overtime hours. In 2014,
that number was reduced to about 769
hours, and through June of 2015, that
number stands at only 42 hours. That is
a direct savings to the hospital of more
than $100,000 per year.
This reduction was accomplished
by the following process and program
changes:
• The number of staff on duty for
second and third shifts was increased
from two to five. This helps prevent
call-ins for assistance during
significant events.
• During holidays, the three eight-hour
shifts were reduced to two 12-hour
shifts. Now, fewer staff are used for
holiday coverage.
• All overtime must now be approved by
section managers.
• Employees that smoke must now
do so on their own time. They can
smoke before shift or at lunch but
must go off property. This has
improved productivity. Smokers were
offered smoking cessation program
information.
Facility managers today are being
asked to cut staffing levels to control costs.
By keeping departmental overtime ratios
around 3 percent, the facility manager
shows his or her commitment to cost
curtailment. Controlling overtime allows
you to reduce costs without reducing
staffing levels. Being proactive in adjusting
schedules and staffing levels to avoid
overtime allows the facility manager
a position of power when the C-suite
comes looking for the department to
cut costs. Take credit for the work you
do. Communicate any savings that your
department is able to accomplish, and
show those savings as dollars saved
against the bottom line.
www.ashe.org 33
Feature
Facility operations cost
reduction through
best practices
By Nick Burke, PE, capital project manager, The University of Kansas Hospital
H
ealth care facilities
have some of the
most stringent HVAC
requirements compared
with other commercial
and institutional spaces.
These requirements range from high
ventilation rates to tight humidity
controls, all of which enhance the patient
experience and help manage infection
control. The systems also result in
relatively high heating and cooling loads
per square foot, making the central HVAC
equipment a very important cost center
for a hospital to manage.
Central plants typically include
large equipment, so full system
replacement when new technology
becomes available is usually not possible.
34 inside ashe | Fall 2015
Significant efficiency improvements can
be made, however, by understanding
the operation of the systems, making
upgrades to key equipment, and
targeting these improvements to
leverage the investment.
One example of this targeted
improvement is the installation of water
treatment systems to improve the
operational costs of cooling towers. For
an investment of about 5 to 10 percent
of the cost of the cooling towers, water
softeners or a reverse osmosis system
can be installed to provide treated
water with significantly less dissolved
solids than the input city water. Cooling
towers reject heat by evaporating water
as the final stage of the cooling process
for the hospital HVAC system. While
the water evaporates, any dissolved
solids, most commonly calcium, remain
behind, building up like the ring around
a bathtub. For a 1,000 ton cooling load,
over 20 pounds of calcium is left inside
the tower every day. This calcium is
removed by blowing down a portion
of the water in the tower—a necessary
loss to avoid degradation of the
equipment. Without any pretreatment,
this blowdown may be one gallon (or
more) for every two gallons that are
evaporated. Treating the water can
reduce this ratio by typically two to six
times, depending on the local water
quality, saving 5,000 to 10,000 gallons
per day for the same 1,000 tons above.
All told, this strategy adds a relatively
small component to the cooling system,
which allows the entire system to operate at a lower utility cost,
using fewer resources to provide the same conditioning to
the hospital.
Many more examples of this type of improvement can be cited
that leverage a key component to make a large system operate
more effectively. Variable speed drives allow the same equipment
to be operated more efficiently at part load. High turn-down
burners allow the entire boiler, and consequently the entire boiler
system, to operate more efficiently at part load. Similar to the
water treatment changes improving the entire cooling tower
system with a small capital investment, a burner replacement may
improve boiler efficiency by 1 to 3 percent, at a cost of only 10
percent of the capital investment of the boiler. Because so much
of the central systems in hospitals are HVAC-related, the loading
of equipment varies widely with seasonal weather conditions.
High efficiency at low operating points is even more important in
health care than it may be in facilities with relatively fixed loads,
like industrial facilities, although many industrial facilities benefit
from these strategies as well.
As with any managed project in the health care environment,
Airflow
operations cost reduction opportunities need to be managed.
Many of these projects may be difficult to identify, because the
existing equipment works, just not as well as it can with best
practices. Having an active champion on the team who identifies
these types of projects and promotes their value is key to
achieving success.
Just as the goal of a hospital is to provide the best care to the
patient with the available resources, the goal of every facility
operations team is to provide the best central plant utilities to the
hospital at the lowest operating cost. Commodities prices move 635529_Airflow.indd 1
with market forces, which are largely out of the control of an
individual facility. Loads (heating, cooling, etc.) needed to provide
the conditions required for care can be managed, and are dictated
by climate, end use equipment type, and quality of maintenance.
One of the most powerful tools, then, of the central plant operator,
is to manage the efficiency of the central plant equipment.
Identifying best operating practices, proven across the field, and
targeting strategic capital investments can provide significant
benefits, reducing the operating cost of a health care facility while
maintaining high quality systems.
BALL-IN-THE-WALL®
ROOM PRESSURE
MONITOR
Case study
The University of Kansas Hospital, in Kansas City, Kan.,
brought a new energy center director on board who pursued
water savings by installing softeners on the hospital’s central
plant cooling towers. The hospital cooling system operates at
about 2,500 tons seasonal average load, and the water usage
was over 50 million gallons per year. The new director identified
this as a major utility expense with significant opportunity for
improvement. Because the original water quality was slightly
worse than typical, the baseline use included about 40 percent
blowdown. Installing the new soft water supply to the cooling
towers has reduced the water use by about 16 million gallons a
year, saving nearly $150,000 in annual operating expense.
Direction Incorporated
Toll Free: 888-334-4545
www.airflowdirection.com
ashe@airflowdirection.com
PATENT PENDING
®
Airflow Direction Inc.
4/3/13 5:51 PM
The patient’s life
was saved. But not
by a doctor.
When a patient at a large regional
medical center in Florida suddenly
began choking, two nurses rushed
to her aid. But they were unable
to perform the Heimlich maneuver
successfully on someone larger than
themselves. Fortunately, G4S officer
Michael Ward stepped in and was able
to save her life. Knowing our officers
have been trained for almost anything helps everyone breathe easier.
RISK NEVER SLEEPS.
Be ready for anything with customized G4S Custom Protection Officers
equipped with the latest technology. To read more about how G4S goes
above and beyond, please visit Risk-Never-Sleeps.com/bestofficers
and click the Respect The Uniform tab or call 855-622-5544.
746356_G4S.indd 1
Securing Your World.
www.ashe.org 35
5/11/15 5:57 PM
Feature
Securing the future of health
care: A hospital’s approach to
alternate energy
solutions
By Benjamin S. Blankenship, CHFM, director of facility
support services, Carilion Clinic
36 inside ashe | Fall 2015
“The solar array will produce 17 percent
of the annual electricity for the complex and
32 percent of the power demand.”
commitment to a common purpose of
better patient care, better community
health, and lower health care cost.
As director of facility support services
for Carilion’s Western Region Hospitals,
I have the responsibility for overseeing
non-clinical support operations at three
of the health system’s seven hospitals.
Throughout the last several years, the
facility teams at each of the three sites
have worked to implement energy
management projects and operational
strategies that have netted roughly
$400,000 worth of realized savings.
One of those sites is Carillion’s New
River Valley Medical Center (CNRV). The
engineering and facility management
teams, in addition to senior leadership,
have been committed to not only
reducing the cost of facility operations,
but to finding environmentally
responsible ways to do so.
A
s more and more hospitals
and health care systems
turn an educated eye
to sustainability and
green practices,
facility engineers are
identifying ways to reduce carbon
footprints and, in turn, improve the
bottom line on their energy spending.
Reducing carbon footprint and lowering
energy cost align with Carilion Clinic’s
organizational mission and vision.
Headquartered in Roanoke, Va., Carilion
Clinic serves approximately one million
residents in western Virginia. Energy
sustainability and cost reduction in
health care is a civic commitment
that coalesces with Carilion’s vision of
About CNRV
CNRV is located in Christiansburg,
Va. The site boasts 500,000 square feet
of interior space and sits on a 112-acre
campus that is surrounded by the natural
beauty of southwest Virginia. The CNRV
campus comprises two medical office
buildings, a standalone ambulatory
surgical center, two heliports, and is
home to a number of excellent medical
programs, including:
• Level III trauma emergency
department
• The Birthplace, a top-rated, awardwinning maternity facility
• Heart and vascular center
• Carillion Clinic Saint Albans Hospital, a
25-bed behavioral health hospital
Altogether the CNRV campus
employs approximately 1,000 full-time
equivalencies (FTEs), possesses 146
licensed beds, and serves a community
of approximately 250,000 patients.
CNRV was constructed in 1998 and
has undergone three major expansions.
It is the second-largest facility in Carilion
Clinic’s hospital portfolio. The medical
complex is powered through a detached
central plant. The plant contains three
650-ton chillers of varying ages and
rated efficiencies. Three cooling towers
are located on the roof of the plant.
The facility’s three gas-powered boilers
generate medium pressure steam for the
campus. Numerous pumps and motors
consisting of a multitude of horsepower
and sizes supply domestic and gray
water through the infrastructure
distribution systems.
Over the last several years, CNRV
has experienced the financial benefit of
energy reduction through the execution
of targeted energy management
projects. These projects were designed
to go after “low-hanging fruit” and
generate quick wins to establish
momentum and program credibility.
The first steps toward an energy
overhaul began with a benchmarking
project to assess the hospital’s existing
energy expenditure and usage. The
utilities management team, along with
an energy consultant, benchmarked
and entered energy data for the last
three years into Energy Star’s Portfolio
Manager. This important step allowed
us to identify where we were at the time
and which energy-saving projects were
measurable, scalable, and executable. We
installed metering systems to allow realtime tracking of utilities consumption
and developed dashboards to use this
data to provide management tools
for the plant’s facility operators to
implement demand/response strategies.
Energy efficient initiatives can
positively affect a hospital’s operating
margin. Up to 30 percent of a hospital’s
consumed energy can be saved
at little or no cost through energy
efficient technologies and improved
management practices without
continued on page 38
www.ashe.org 37
sacrificing the quality of care. This benchmarking activity and its
related projects resulted in substantial energy and cost savings.
We reported the following returns on our investments.
HVAC adjustments
Investment: A series of HVAC improvements, including
both equipment and controls optimization, required a total
investment of $34,434.
Return: These improvements resulted in $305,720 of annual
savings.
Steam valve insulation
Investment: A cost of $43,579 was required to insulate all
steam valves in the hospital and medical office buildings.
Return: The annual savings resulting from improved
insulation are $24,299, achieving a payback in less than two
years with continued savings.
Gas supplier switch
Investment: To change the way we purchased natural gas
we needed to switch to a different supplier. This required the
installation of digital meters on the gas distribution system. The
cost for the metering change was $8,500.
Return: The change in the way we purchased energy saved
$55,000 annually.
Parking lighting upgrade
Investment: Lighting upgrades in the parking area were
installed as a result of an Environment of Care safety audit. New
LED lighting replaced an aging and inefficient metal halide
system. The LED replacement resulted in a decrease of more
than 300 watts per fixture.
Return: The upgrade saved $6,291 per year, and reduces the
required maintenance and replacement of parking lighting.
The CNRV engineering team has larger plans on the horizon
that will take advantage of the campus’s geography and
substantial acreage. In an environment of tight funding, we
have found many ways to finance improvements. Investments
in energy efficiency are among the soundest investments today.
Most energy projects yield a one-to-five-year payback, which
GSA# - 07F0053W
Small Business# 412286-2013-09-SB
Protect door openings
against hot/cold air
and insects
AIR CURTAIN OFF
0
F
65
60
56
410 Air ows inside
52
48
44
40
888-359-2562
38 inside ashe | Fall 2015
756644_Powered.indd 1
AIR CURTAIN ON
Air Curtains
are up to
80% efcient
at stopping
inltration
www.poweredaire.com
23/07/15 1:38 PM
“The solar installment would not
only offset any escalation in energy
costs, but would decrease the
hospital’s actual energy demand,
resulting in tremendous savings in
terms of cost and energy usage.”
translates to a yield of 20 to 100 percent with little or no risk.
Currently, plans are under way to develop a seven-acre solar
array on the 112-acre campus.
To assist with the initial capital funding, CNRV has partnered
with a solar development company and is entering into a
customer self-generation agreement with the local utilities
supplier. The solar development company will design, develop,
finance, own, and operate the distributed solar photovoltaic
solution with purchase options available to CNRV. This business
model was designed for tax-exempt entities to enhance their
sustainability goals and to reduce their electricity costs to below
grid parity.
Carilion Clinic is a nonprofit health care organization, so
the partnership makes sense. The solar installment would not
only offset any escalation in energy costs, but would decrease
the hospital’s actual energy demand, resulting in tremendous
savings in terms of cost and energy usage.
Understanding the utility bill and surrounding tariff structure
was a key first step in the project analysis process.
A 1,300 kw ground mount tracker array system with a
35-system-year life cycle was designed to manage peak demand
loads and to provide insurance for the future against increasing
cost of electricity.
The solar array will produce 17 percent of the annual
electricity for the complex and 32 percent of the power demand.
A conservative analysis of a 4.5 percent power cost escalation
rate was presented to the executive suite for project approval
and reflects a 20-year net benefit of $850,000 for the facility.
However, a more realistic escalation rate of 6 percent denotes
the 20-year net benefit to be $1.2 million. Factoring in the actual
life cycle of the system reflects an even greater return. With no
capital required to get this project under way, the customer
self-generation agreement and solar development partnership
represents an attractive solution to offset escalation rates,
reduce dependency on fossil fuels, and better manage peak
demand. Regardless of which investment return scenario is
presented, this project’s success ensures a bright future for the
medical complex.
Not only did these control measures and projects save money
and energy at CNRV, they established momentum that has helped
further the green initiative. These projects and many others like
them have allowed the organization to be better positioned for
environmental stewardship in addition to contributing to reducing
health care cost for the community.
Member Spotlight
Linda Dickey
ASHE’s member spotlight
highlights ASHE members
making significant
contributions to the field of
health care engineering and
contributing to our mission
of optimizing the health care
environment. If you would
like to nominate someone to
be featured in the member
spotlight, contact Inside
ASHE managing editor
Deanna Martin at
dmartin@aha.org.
A
SHE member Linda Dickey, RN, MPH, CIC, is
the director of epidemiology and infection
prevention at University of California Irvine
(UCI) Medical Center and is a renowned expert in
infection control and prevention. Dickey is an ASHE
faculty member who teaches ASHE’s infection
prevention course as well as ASHE’s water system and
management of waterborne pathogens course. She
is a graduate of the ASHE Leadership Institute, has
presented sessions at many ASHE conferences, and
has written numerous articles and book chapters on
infection prevention. In addition to her work with
ASHE, Dickey volunteers with the Facility Guidelines
Institute, ASHRAE, APIC, and other organizations on
infection control issues.
Fire Door Solutions has developed products and services to assist hospitals and medical
facilities with adhering to the new 2012 Life Safety Codes as it applies to inspecting,
repairing and maintaining fire rated doors. We are committed to providing products and
services that ensure your fire rated doors are compliant with the new Life Safety Codes.
Fire Door Products
|
|
|
|
|
Fire Door Caulk
Fire Door Thru-Bolt
Fire Door Shims
Door Gap Gauge
NFPA 80 Inspection Kit
750899_Fire.indd 1
Fire Door Services
Fire Door Inspections
Fire Door Repairs
| Fire Door Field Labeling
| Inspection Training
|
|
www.ashe.org 39
7/25/15 3:06 AM
Slee
wel p
l
Alex ,
.
Some environments are more critical than others. When
proper air management can mean the difference between
a good night’s sleep and contamination, hospitals choose
the leader in the field. A partner they know stands for
comfort, innovation and safety.
Visit titus-hvac.com/critical today to learn more.
Commissioning
INSIDER
2015
How asHe’s
commissioning
process can reduce
costs and create
more efficient
facilities
CONTENTS
42
43
Letter to readers
By Dale Woodin, CHFM, FASHE
Commissioning resources and
training opportunities
By Deanna Martin
44
Why ASHE health facility
commissioning?
By Steven R. “Rusty” Ross, PE, LEED AP
BD+C, EMP, CxA
47
ASHE’s health facilities
commissioning:
An economic engine
By Mark Kenneday, MBA, CHFM, FASHE
50
52
Measurement and verification
By Jessica Jeffries, LEED AP BD+C, EMIT
Operations and maintenance
training programs in
facility management
By Lindsey Brackett, EI
55
Water commissioning:
Keeping the flow smooth
By John M. Dombrowski, PE, HFDP,
CPMP, CCP, LEED, and Heather L. Platt, PE
58
Rx for healthy hospitals:
Monitor-based commissioning
By Joe D’Arrigo
60
Proper witness testing: Five
best practices for success
By Justin Carron
www.ashe.org | Commissioning insider 41
LEttER tO REAdERS
Dear Readers,
Dale Woodin, CHFM, FASHE
Senior Executive Director
American Society for
Healthcare Engineering
“
Hospitals can
save millions of
dollars through
commissioning. And
by commissioning
your facility, you as a
facility professional
can demonstrate
your own personal
value to your
hospital leaders.
”
42 www.ashe.org | Commissioning insider
You’ve no doubt heard a lot in recent years about the need for reducing operational
costs in light of shifting hospital payment models and other changes in the health care
field. Maybe you’re being pressured to reduce your staff. Maybe your organization
is partnering with another in an effort to expand reach and gain efficiencies. Maybe
you’re simply on the lookout for every possible way to save resources.
The process of commissioning is one way to reduce operating expenses while
improving efficiency. Commissioning, which can be performed during new
construction as well as on existing facilities, examines the complex systems within
health care facilities to make sure they are performing as designed.
Hospitals can save millions of dollars through commissioning. And by
commissioning your facility, you as a facility professional can demonstrate your own
personal value to your hospital leaders. Although the current health care climate is
challenging, it presents opportunities for facility managers who can present valuable
solutions like commissioning.
This special section explains the commissioning process and gives you the
information you need to help your organization save resources and become more
efficient through commissioning. It’s important to note that the ASHE commissioning
process outlined here is tailored specifically for health care facilities. Traditional
commissioning processes don’t always work in hospitals, which are unique
environments in that they operate around the clock, house vulnerable patients, and are
heavily regulated.
While these articles provide an overview of commissioning, additional resources
are available to walk you step-by-step through the process. The Health Facility
Commissioning Guidelines describes a collaborative commissioning process that saves
hospital resources. The Health Facility Commissioning Handbook provides detailed
instructions on how to perform the health care commissioning. Both are available at
www.ashestore.com.
Facility professionals are facing a variety of challenges in today’s rapidly changing
health care environment. ASHE is committed to helping its members find new ways
to help hospitals reduce expenses. We are committed to showcasing our members’
ability to provide solutions to their organizations. And because of these reasons, we are
committed to commissioning. I hope after reading this special section that you too will
understand commissioning, recognize the savings it can provide, and commit to using
the commissioning process on your next project.
Sincerely,
Commissioning resources
and training opportunities
By Deanna Martin, ASHE communications manager
T
he articles in this publication
explain the basics of
commissioning and why it is
such an important process for
providing operational value.
ASHE also has other resources
available to help you dig deeper into
the process and to help you develop the
business case for using commissioning in
your next project.
Commissioning guidelines: To tailor
the commissioning process specifically to
complex hospitals and other health care
facilities, ASHE created the Health Facility
Commissioning Guidelines. This resource
establishes a standard process for
commissioning health care facilities and
stresses a collaborative approach among
project participants. This document is
available as a print or e-book edition at
www.ashestore.com.
Commissioning handbook: The
Health Facility Commissioning Handbook
provides step-by-step instructions
for implementing the health facility
commissioning process outlined in
the Health Facility Commissioning
Guidelines. The handbook also includes
information to help facility managers
and others communicate the importance
of commissioning and show the return
on investment the process can bring.
This resource is available in as a print or
e-book edition at www.ashestore.com.
Commissioning course: ASHE’s
commissioning course teaches attendees
how to develop a business plan that
presents the value of health facility
commissioning to your executive
leaders and demonstrate the return on
investment that comes from embracing
the health facility commissioning
process. The class also explores critical
aspects of the process, with emphasis
placed on a collaborative effort
that brings together the health care
organization, design team, constructors,
and commissioning agent. The course
also shows how the process can be
scaled to projects of various sizes. Visit
www.ashe.org/learn and click on health
facility commissioning to learn more
and see the schedule of courses. To
learn more about hosting this program
for your ASHE chapter or other group,
contact ASHE at ashe@aha.org.
Use these resources to incorporate
the commissioning process into
your project, no matter the scope.
For additional questions regarding
commissioning—or to share your success
stories with ASHE members—contact
ASHE at ashe@aha.org.
n
ONLY “UL Approved”
Air Flow Indicator on the market
•
•
•
•
•
•
•
•
•
Know at a glance, every minute, every shift your airflow is correct
Simple, yet accurate Negative or Positive Air Flow Monitors
Never any calibration or maintenance, ever!
2 Hour Fire Wall Rated by UL
Smoke Damper (California)
Lifetime Warranty against any mfg defects
Fire Protection installed in every unit
Highly Durable for Construction Barriers during renovations
Electronic unit available for use with alarm systems
725104_LAMIFLOW.indd 1
Call Us at
(800) 554-6221
www.Lamiflowtech.com
www.ashe.org | Commissioning insider 43
15/12/14 8:22 pm
commissioning insider
RESOuRCES
tHE ASHE WAy
Why ASHE health faci
construction firm to serve as the
commissioning agent (CxA). The
USGBC also allows the CxA to be
a consultant to the design team
and, on smaller projects, permits
the CxA to be a member of the
design or construction team.
By Steven R. “Rusty” Ross, PE, LEED AP BD+C, EMP, CxA, principal,
director of commissioning services, SSRCx
C
ommissioning is an important
part of the construction process,
and many organizations
have created commissioning
standards. Each standard has
its place, but the ASHE health
facility commissioning (HFCx) process
best meets the needs of those involved
in health care construction. This article
explains why that is by comparing the
ASHE HFCx process to five other leading
commissioning methods.
Selecting the agent
The ASHE HFCx process defines
the role of the commissioning agent
(HFCxA) or commissioning authority
as an individual or firm that works
directly for the owner, rather than
being an employee or subcontractor
44 www.ashe.org | Commissioning insider
of any other project team member.
The HFCxA is a consultant and
represents the owner’s interest and
as such should not be contractually
obligated or connected in any financial
way to any other team member.
The Associated Air Balance Council
Commissioning Group (ACG) and the
Building Commissioning Association
(BCA) advocate that the commissioning
authority should be an independent
third party. The U.S. Green Building
Council (USGBC, which promulgates the
Leadership in Energy & Environmental
Design [LEED] standards), the American
Society of Heating, Refrigerating, and
Air-Conditioning Engineers (ASHRAE),
and the National Environmental
Balancing Bureau (NEBB), on the other
hand, permit a member of the design or
Systems to be commissioned
The ASHE HFCx process involves
every system critical to operation
of the health care facility and
maintenance of the health care
physical environment, from the
building envelope to medical gas
systems. In addition to the criticality
of each individual system, the full
functionality of many systems depends
on integration with multiple other
systems. Consequently, in a health
care facility the full recommended list
of systems must be commissioned and
integration must be verified.
Design phase
The ASHE HFCx process and the
BCA process are the only standards that
require a design phase kickoff meeting.
The HFCx process specifically addresses
the need to define the project’s energy
efficiency goals early in the project.
Medical facilities both use a great deal
more energy than many other facility
types and offer fewer opportunities to
“set back” energy-consuming systems
in unoccupied modes. All the standards
except ACG require energy expectations
to be defined in the owner’s project
requirements (OPR), but ASHE takes
it further by requiring quantitative
definition of the energy efficiency goals
in the OPR.
The ASHE HFCx process is the only
standard that requires development of
a utility management plan (UMP). This
UMP is required by the Joint Commission
and historically has been created by the
operations and maintenance (O&M) staff
at some point prior to occupancy.
All standards require some level
of design review of the construction
documents, but the required frequency
and review criteria vary greatly:
• Although ASHRAE Guideline 0-2005:
The Commissioning Process defines a
review process for schematic design
(SD) documents, design development
(DD) documents, and construction
documents (CD), ASHRAE Standard 2022013 states that the number of reviews
should be defined by the owner.
• ASHRAE and BCA allow sampling
of portions of the design as an
acceptable method of plan review.
ASHE does not allow sampling.
• ACG requires only one review.
• NEBB states that a review of the SD
may be conducted, a review of the
DD documents should be conducted,
and a review of the final CD must
be conducted.
Construction phase
Many construction phase tasks
have similar requirements in the
various commissioning standards,
including those listed in the left
column of the table below. Some
requirements specific only to some
standards appear in the right column.
Only the ASHE HFCx process
requires the review of the HVAC
controls system programming prior
to functional testing. ASHE states that
much of the expected performance
of systems can be lost between the
creation of sequences of operations in
the contract documents and the actual
programming language developed for
the building automation system.
Requirements for documentation
of equipment and system installation
vary greatly among the commissioning
standards, but generally all of them
require development of installation
checklists. ASHE requires that the
installation checklists be completed
as the installation work progresses
and does not permit preparation of all
the documentation at one time after
installation is complete.
The ASHE HFCx process requires the
HFCxA to facilitate inclusion of the O&M
staff in construction phase activities, from
various required reviews to site tours.
Acceptance phase
The acceptance phase of construction
falls after start-up and initial checkout.
The ASHE HFCx process requires several
activities during this phase that are not
required by other standards.
All standards require the CxA to
create and maintain an issues log and
ensure items on it are addressed in a
timely manner. All require the CxA to
complete a final commissioning report.
All except for LEED require the CxA to
verify the O&M training process and
to either compile, create, or review the
systems manual. (LEED
offers “extra credit” to
>>
Construction Phase Activities
Activities common across the standards
Requirements specific to some standards
All standards require commissioning kickoff meetings and
other planning meetings.
The ASHE HFCx process requires milestone meetings to be held
to plan the various construction phase activities.
The CxA conducts periodic site visits to observe the work.
LEED defines the review of start-up forms and/or construction
checklists as a form of “pre-functional inspection.”
The CxA reviews the following:
•
•
•
•
•
•
•
•
Shop drawings and submittals for commissioned systems
Operations and maintenance manuals
Training plan
Systems manual
Start-up documentation
Test and balance reports
Updates to the OPR and basis of design
Changes to the contract documents affecting
commissioned systems
LEED does not require review of shop drawings and submittals
for commissioned systems, the O&M manual, the training plan,
or the systems manual.
www.ashe.org | Commissioning insider 45
commissioning insider
ility commissioning?
complete these activities, and ACG does
not address the systems manual.) LEED is
the only standard that requires a current
facility requirements and O&M plan;
the requirements for this document are
similar to those for a systems manual.
The requirements for functional
testing have notable differences
between the standards. Again, all
organizations require these test
procedures to be created and, again,
“
ASHRAE is not specific as to who creates
the testing documents. The ASHE
HFCx, ACG, NEBB, and BCA processes
require the CxA to create these test
procedures. The creation of the testing
documents, which identify all operating
modes, safeties and alarming, system
interoperability, and interdependence
between systems, and so forth, is critical.
During the acceptance phase, the
ASHE HFCx process requires provision
”
SICK OF
THIS?
Blueprint room a mess?
Prints decaying?
Take too long to find?
AccuScan will sort your Hospitals’ blueprints removing the
duplicates and bid sets. We will then scan them into a database
that will enable you to:
Retrieve the
exact print
or set
of blueprints
Scanned blueprints can be
viewed, edited,
emailed & printed
Cloud based
storage available
.info
ACCU SCAN
Blueprints can be
imported into
AutoCAD &
converted to AutoCAD
digital archival solutions
Experts in Blueprints and Document Management
Art@GetAccuScan.com
Call 609-386-6795 or visit us at www.GetAccuScan.com
46 www.ashe.org | Commissioning insider
698122_AccuScan.indd 1
The ASHE HFCx process
requires benchmarking
energy performance and
measuring and verifying
actual energy performance
for at least the first year of
occupancy. ASHE also requires
the HFCxA to review the
trends established in the
acceptance phase with the
O&M staff post-occupancy.
6/14/14 1:59 AM
of the several services that are unique
to its standard, including facilitating
the development of operations and
maintenance dashboards and facilitating
development of the maintenance budget.
Post-occupancy phase
All the commissioning standards
discussed in this article require opposite
season testing on systems that could
not be tested adequately during preoccupancy functional testing.
The ASHE HFCx process requires
benchmarking energy performance and
measuring and verifying actual energy
performance for at least the first year
of occupancy. ASHE also requires the
HFCxA to review the trends established
in the acceptance phase with the O&M
staff post-occupancy. The NEBB and
BCA processes define requirements for
benchmarking, measuring, and verifying
energy performance as well. The ACG
and ASHRAE processes do not specifically
address these tasks, and LEED offers “extra
credit” to complete a similar monitoringbased commissioning program.
The need for health
care-specific commissioning
Although the various commissioning
standards discussed include similarities,
development and use of the ASHE HFCx
process has made clear the importance
of using a health care-specific
commissioning process. The health care
field is unique, and health care facility
managers face challenges significantly
different than those faced by facility
managers in other industries.
n
ASHE’s health facilities
commissioning:
An economic engine
By Mark Kenneday, MBA, CHFM, FASHE, vice chancellor, campus operations, University of
Arkansas for Medical Sciences
T
he movement in health facilities
management to fully integrate
commissioning into the delivery
process has been met with slow
adoption. Almost all cultural
change requires time and the
tenacity of the visionaries to achieve
the intended goal. Every change
will be questioned, and the reasons
for embracing a change like health
facilities commissioning (HFCx) must
be substantial enough to move the
industry to a second curve; adopters
must be won over to the new way to
deliver health facilities projects, and
own and operate facilities.
Commissioning began to emerge
as a necessity to achieve the “owner’s
project requirement” (OPR) in just the
last decade. However, commissioning
has been a standard for the safe and
effective delivery of many projects for
other industries for more than half a
century. Although late to the market,
HFCx has the unique serendipitous
outcome of creating an economic
engine that can generate significant
positive cash flow in excess of what is
required to fund the process, along with
an excellent prescription for monitoring
various work activities.
For many years, commissioning
has been required by the military
for new equipment that will be used
to transport personnel or provide
surveillance. The U.S. Navy does not
accept a new ship without
proper commissioning to
ensure the vessel and all
>>
www.ashe.org | Commissioning insider 47
commissioning insider
FinAnCing
“The ASHE HFCx process provides specific strategies to
optimize energy expenses and significantly reduce the
institution’s cost.”
of the technology and hardware work
as expected. Sending warriors across
or under the sea in a ship that has not
been properly commissioned would be
putting their lives at risk unnecessarily.
The U.S. Army does not accept
transport, weaponry, or tanks without
commissioning them to ensure they
can transport and protect personnel as
well as deliver the required munitions
to their designated targets. Each branch
of the military has commissioning
specifications for designated equipment
that assures the safe and effective use
and optimal performance during battle.
The commissioning process, coupled
with a dynamic strategic plan, makes the
difference in the success of a battle, and
whether the warriors return home to
their loved ones.
Numerous industries have
commissioning as standard operating
procedure prior to taking productive
use of their equipment and structures.
The process is specialized for equipment
and facility use, and in many cases
commissioning is required to achieve
acceptance of their manufacturing
process. Commissioning goes by many
names. Toyota integrated commissioning
ARLINGTON
ATLANTA
AUSTIN
BOSTON
DALLAS
DENVER
HOUSTON
KANSAS CITY
NASHVILLE
NEW YORK
MIAMI
PHOENIX
RICHMOND
SEATTLE
SAN FRANCISCO
SHARPSBURG
WASHINGTON DC
48 www.ashe.org | Commissioning insider
758080_ccrd.indd 1
into their poka-yoke process, as error
proofing; Ford integrated it into their
production lines as part of Job 1—
every time the line is changed it must
be tested to validate that production
meets expectation. Many manufacturing
processes for line setup and teardown
require commissioning each cycle to
ensure production meets expectation.
Interestingly enough, health care
has been commissioning equipment,
especially medical equipment, for
decades. X-ray equipment, CTs, and
MRI equipment have not been installed
without proper commissioning. Specialty
equipment, such as robotic surgical
machines, is not accepted without
proper commissioning, and certainly
radiation-emitting equipment has
been commissioned since its use began
for cancer and tumor treatment. The
reasoning behind commissioning is not
hard to understand when considering
the significance of the desired outcome,
which for many processes is life or death.
Only one reasonable argument has
been made for not commissioning,
and that is cost. However, most
professionals in health care agree that a
commissioning process and a dedicated
health facility commissioning authority
(HFCxA) would bring tremendous value
to every project. As an independent
facilitator, the HFCxA has the capacity to
facilitate the OPR while optimizing the
financial resources so value engineering
(VE) exercises are no longer necessary.
ASHE has developed multiple case
studies that readily document savings
from health facility commissioning
in excess of cost. HFCx, when done
properly, creates a positive cash flow,
above its costs, that can be used to fund
other mission activities. Health care
has a history of planning, designing,
constructing, and owning and operating
facilities and uses standard processes
developed over the past 100 years.
The majority of buildings represent an
economic engine for resources that
can be used to support the growth and
expansion of the missions served. The
opportunities are there not because
buildings were poorly planned,
designed, and constructed, but rather
because at the time of their construction,
efficient design was not the focus. The
methodology used to own and operate
these facilities was defined as best
practice decades ago.
The ASHE HFCx process is a
fundamental shift—a disruption—in
how health facilities projects are
delivered. When properly executed
and coupled with collaborative teams
working in harmony to deliver the
OPR, the ASHE HFCx process virtually
PROVIDING LOCAL KNOWLEDGE
WITH GLOBAL COVERAGE
WSP has more than 1,450 personnel in 40 offices across the U.S.
Our commissioning team is staffed by professionals who understand
the latest technological advancements in building systems, as well as
optimizing existing building systems, ensuring proper integration and
long-term operational efficiency.
Paul M. Meyer
Senior Vice President
Paul.Meyer@wspgroup.com
512 Seventh Avenue
New York, NY 10018
wspgroup.com/usa
06/08/15 3:21 pm
758624_AKF.indd 1
to achieve the OPR ensures that it is
achieved and optimizes the value of the
project at the lowest delivery cost.
After the owner takes first
productive use, the HFCxA and the team
can follow the project through its first
year of use and resolve problems with
performance shortfalls before the end
of the warranty period. An additional
benefit is that the ASHE HFCx process
keeps the team engaged through the
first 12 months of operation to ensure
the systems are commissioned for
seasonal changes that traditionally are
not achieved in the standard delivery
model. The HFCxA works with the team
to verify that the measurement and
verification plan meets and exceeds the
OPR to achieve the energy efficiencies
defined and the customer utilization to
optimize their outcomes.
The greatest value of the ASHE
HFCx process comes after the customer
takes first productive use. This value
results from significant savings that
can be captured using newly defined
measurement and verification
techniques and improved competencies
from the operations and management
staff in daily operations. Energy
efficiency is a primary focus of the
ASHE HFCx process, and energy savings
strategies are the most significant
expectation of the commissioning
authority. To achieve these savings
the HFCxA can leverage their input
from the first OPR charrette to the
end-of-warranty walk though. ASHE
knows that on average, more than half
of the expense for a normal facilities
department is energy cost. The ASHE
HFCx process provides specific strategies
to optimize energy expenses and
significantly reduce the institution’s cost.
This is the economic engine that health
facilities and infrastructure represent. By
redirecting utility payments in support of
the mission, the health facility manager
no longer competes with mission-related
projects, and in many cases, provides for
them through utility savings. This is the
second curve: facilities as an economic
engine in support of the mission of
the institution.
n
www.ashe.org | Commissioning insider 49
01/08/15 2:08 am
commissioning insider
eliminates waste. VE is usually an
afterthought to right-size a project
that is no longer in budget. This is
“value eradication,” the real outcome
of VE activities as the value of specific
activities and elements are removed
from the project to fit into the project
budget. Such work should never have
been part of the project, as the owner
could not afford it, and when removed,
the work leaves behind a “tax” because
it is not removed at the same cost as
when first included. During the design
phase, the HFCxA can help the team
achieve the OPR without undue cost
overruns or VE exercises.
During construction, the HFCxA
works with the contractor and design
team to ensure the work is properly
installed and working correctly, reducing
rework and the construction timeline.
The savings are estimated by ASHE to
be approximately 2 percent of the total
project cost, which usually covers the
cost of commissioning as a first-cost
contributor. Having an independent
set of eyes that works within all parties
M&V PROgRAMS
Measurement and
VERIFICATION
By Jessica Jeffries, LEED AP BD+C, EMIT, principal/project manager, TME, LLC
M
easurements help define and
quantify progress. Verification
confirms the accuracy of the
measurements. Measurement
and verification are critical
to the ASHE health facility
commissioning process. Without
measuring and verifying progress,
participants, stakeholders, and facility
managers can be left in the dark to make
decisions based on incomplete data
and gut feelings. As hospitals embark
on the path to reduce energy and invest
in energy efficient buildings, they must
be confident that their program, new
building, or technology is worth the
cost. Accurate measurements can serve
as a report card to judge the success
of a project and, when combined with
50 www.ashe.org | Commissioning insider
ongoing monthly or daily measurement
and verification (M&V) programs,
can sustain or enhance an energy
conservation program.
When budgets are tight and
decisions must be made to fund
only part of the desired energy
conservation program, removing M&V
from the project might seem an easy
choice. However, eliminating M&V
is a detriment to the integrity of the
entire project. The well-designed M&V
program gives feedback during the
implementation of energy conservation
measures, verifies measures preform
as estimated, helps sustain savings
long after the project is complete, and
engages facility operators to make
energy-wise decisions.
The well-planned, high quality M&V
program must be executed by experts
that understand the fundamental
concepts and best practices and must
contain the following key components:
a documented plan, a methodology,
measurement of post-installation energy,
and documentation.
Documented plan
M&V programs start with the first
component, the documented plan,
designed by the M&V professional
in agreement with the facility and
key stakeholders. Plans should
be transparent, verifiable by an
independent third party, and based on
documented data and sound guidelines
like the International Performance
Methodology
The second key component of any
M&V plan, the methodology, should be
based on sound practices. Methodology
can vary greatly based on the type of
energy conservation measure (ECM),
goals of the project, and availability of
data, but methodologies can all be boiled
down to this basic equation: Savings
= (Baseline Energy – Post-Installation
Energy) +- Adjustments. Defining
baseline energy includes recording
actual physical conditions, weather,
operational strategies, and utility data.
Once the project has started, baseline
information can be difficult to obtain.
Record the methods used to establish
the baseline. Whole building metering
and measurements are a good way to
approach M&V, since it shows the energy
performance of the entire facility. Also
record all baseline end uses. Changes to
a facility’s operation, installation of new
medical equipment, and completion
of shell-space finish-outs can lead to
miscalculations. Changes during the
baseline can also complicate establishing
the baseline energy. All construction
activity and operational changes during
the baseline period should be discussed
with the M&V professional so adjustments
can be made to reflect the changes in the
baseline period.
Measurement of
post-installation energy
The next component of the M&V
plan is measuring post-installation
energy. Post-installation energy should
be measured at regular intervals,
and verification activities should be
conducted to ensure proper installation,
operation, and execution of the energy
conservation measures. At a minimum,
annual reports should be generated
to document savings and ensure
continued performance of the ECM.
Monthly and daily M&V reports, while
more costly, can increase the value of
the M&V program by avoiding savings
degradation, allowing fine-tuning of
measures through operational feedback,
and engaging the operations and
maintenance (O&M) staff in the energy
conservation program with quick
feedback of day-to-day operations.
As metering technology and data
computing capabilities become more
prevalent and less costly, hourly and realtime monitoring become additional tools
to enhance measuring activities.
Documentation
The success of any M&V
program comes down to planning,
communication, and documentation.
Documentation is the final and
most important component in the
M&V process. All changes must be
well documented. Not only should
changes be documented, but they
should not override previous versions.
Documenting changes will allow
others in the future to see important
transitions in the project. The M&V
professional should be able to present
the M&V plan and all reports to a third
party for review. The third party should
be able to explain and recreate each
calculation and adjustment.
M&V can be a complicated process
with many variables and moving parts. A
quality M&V plan can be invaluable to a
facility and provide immediate feedback,
both good and bad, to daily operations. n
commissioning insider
“Accurate measurements can serve as a report card
to judge the success of a project, and when combined
with ongoing monthly or daily measurement and
verification programs, can sustain or enhance an energy
conservation program.”
Measurement and Verification Protocol
and ASHRAE Guideline 14: Measurement
of Energy and Demand Savings. At
a minimum, the M&V plan should
contain background information
about the facility, a description of the
energy conservation measure(s), the
methodology and general approach to
M&V, and the agreed-on calculations
used to quantify the monetary value of
the energy saved.
Medically Minded Maintenance
Maintaining a regulatory compliant healthcare facility is vital to your
success. Let FacilityDude help you treat maintenance the way you
treat your patients, visitors, and staff — by putting health and safety
first. Our online tools will allow you to save money, increase efficiency,
and improve overall service quality in your healthcare facility.
Learn about FacilityDude’s maintenance
solutions for healthcare:
facilitydude.com
759483_FacilityDude.indd 1
www.ashe.org | Commissioning insider 51
30/07/15 4:23 pm
tRAining
Operations and maintenance
training programs
in facility management
Insightful solutions that deliver powerful results
By Lindsey Brackett, EI, principal/director of facility management services, TME, LLC
P
ower comes with knowing
what you don’t know. Once
you become aware of what you
actually know and what you
do not, you are able to decide
whether you want to change
your circumstances. Do you invest in a
strategy to fill in the gaps, or do you rely
on others to fill them in for you? Either
way, you acknowledge your personal
boundaries and can leverage your
knowledge in a meaningful way. This
insight is what makes operations and
maintenance training programs
so valuable.
Training provides operations and
maintenance (O&M) staff with the
opportunity to be purpose-driven
and to take ownership of their work.
Objective feedback, continuous training,
and succession planning help staff buy
into the big picture and work toward
the same goal—reducing energy
consumption and overall net costs.
Operations and maintenance training
programs can be implemented in five
simple steps:
52 www.ashe.org | Commissioning insider
Pre-training assessment
Curriculum development
E-learning instruction
Classroom and field instruction
Retention testing
Each of these steps builds on the
previous one and is necessary for the
program to remain effective long term.
1.
2.
3.
4.
5.
Pre-training assessment
Operator training programs must
begin with a pre-training assessment to
establish a benchmark for each training
participant. The assessment is a common
metric that quantifies each individual’s
proficiency level. This step is critical for
several reasons:
• Although we may believe we know
how our peers and direct reports
perform at their jobs, we need an
objective method to rationalize this
information.
• The assessment targets each
individual’s areas of strength and
opportunity. By determining areas
of strength, leadership can assess
whether each participant is correctly
allocated to a position that capitalizes
on his or her skill set. On the other
hand, targeting areas of opportunity
allows the training to be as
streamlined and effective as possible.
No time is wasted on training in areas
that have already been mastered.
• Finally, the assessment sets the
benchmark of current performance
that can be measured against an
exit exam after training is complete.
Improvement in performance is
quantified, and retention is verified.
In addition, in any areas where
performance or understanding does
not increase, additional training can
be administered.
Curriculum development
Once pre-training testing has
occurred, a data analysis is performed
to determine the areas of strengths and
opportunities. This step is necessary to
develop a tailored curriculum for the
training group. Many facility personnel
operate under a “fire-fighting” model
with little time allotted for training
terms on their own time, at their own
pace, and in their own environment. New
topics can be revisited as many times as
necessary until an essential knowledge
foundation is built. This step is important
to accomplish prior to classroom and
field instruction so that all training
participants walk into training sessions
with the same knowledge base. Time
in the classroom is not spent on basics
such as equipment recognition, essential
functions, and terminology. Even further,
no one is impeded by technical jargon
because these terms have already been
introduced through e-learning.
opportunities. In addition, formal
training and classroom learning is
not the preferred method of training;
therefore, time should not be wasted on
areas that are already mastered. Rather,
training sessions should be devoted to
areas that are not as well understood
and yield a high level of payback, either
in improving patient care or energy
efficiency. Another consideration when
determining the training curriculum is
the facility’s systems and equipment,
both current and planned future
installations. All personnel that control
the operations of the energy systems
should be trained on that specific
equipment. Again, time should not
be wasted on irrelevant systems or
equipment. Isolated sessions should be
administered if a facility has specialty
equipment including heat pump chiller
heaters, interruptible rate structures,
and district loops. Input from the
leadership staff is important to identify
any key areas of focus and to verify that
the coursework is appropriate for the
targeted personnel.
Each facility is different, but it is
typically best to organize curriculum to
focus on specific trades. For instance, an
HVAC technician should be trained on
air-side systems and instrumentation,
controls, and electronics. Similarly, a
plant operator should be trained on
central energy systems and controls.
Facilities that use a zone technician
model may prefer to cover general
equipment and layout, specialty
equipment, energy systems, basic
control theory, retro-commissioning,
energy economics, and fundamentals
all under one curriculum. The content
covered in this broad model will not
be as detailed as the trade-specific
approach, but it will be effective at
training zone technicians on the basics
they need to know for multiple systems.
E-learning instruction
After the curriculum is established
and vetted, training can begin. Although
e-learning programs are not ideal for
applications training, they do allow
facility staff to explore new concepts and
Classroom and field instruction
Once participants are prepared
for classroom and field training,
the curriculum’s focus shifts from
fundamental lessons to O&M
applications. On-site training is
sectioned into classroom and field
sessions that build off of each other.
In general, classroom sessions should
be limited to no more than two hours
and ideally closer to one hour. When
learning technical concepts, having an
opportunity to practice at workstations
and equipment is critical to success.
Although general theory can be taught
in a classroom environment, the
connection will not be solidified until it
is demonstrated and rehearsed in the
final form. Since all participants will be
given practice time during each field
lesson, groups should be limited to five
individuals per instructor, and lessons
may last up to four hours.
Retention testing
The final phase in the O&M training
process is to verify retention with an
exit exam. To ensure that the training
effort was effective to all
participants, a follow-up
exam is administered as a
>>
www.ashe.org | Commissioning insider 53
commissioning insider
“When individuals feel
as though they are an
investment and not
a commodity, their
commitment to excellence
exceeds all expectations.”
final common metric to establish and
quantify progress. If minimal progress
is measured, then the training process
starts over, this time beginning with step
two, curriculum development. In most
cases where gaps still exist, especially
with multiple participants, the training
delivery method was not effective and
should be reconsidered. A new approach
Effectively manage your ROUNDS:
must be delivered to effectively reach
the target audience. This new approach
· Eliminate hours of data entry
could include anything from switching to
· Automatically produce and send
a different trainer or spending more time
out work requests
reviewing concepts in the field rather
· Track deficiencies: origin to completion
than in the classroom. In any case, the
· Generate regulatory reports
original delivery method should not
· Accountability like never before
be repeated.
· Customized for you
A carefully crafted and executed O&M
training process will reap many benefits
on its completion. The greatest of these
benefits is that facility personnel will
gain the tools and knowledge they need
to perform their jobs more efficiently,
Rounds Tracker
thus improving patient care, customer
To schedule a demonstration contact us at
satisfaction, and energy performance.
1-800-925-7460 or information@walshintegrated.com
Gained efficiencies in operations will
www.walshintegrated.com
yield energy consumption and cost
savings that can be quantified with a
measurement and verification model.
HR_745557_Walsh.indd 1
5/5/15 8:41 PM A baseline period could be established
prior to executing the training program,
therefore allowing leadership to track
savings with progress in the program.
A vested staff will always take more
pride in their facility compared to
service contract providers. When
properly taught how to diagnose and
troubleshoot, facility personnel will be
more likely to take the extra time and
care in resolving everyday issues without
EOC Solutions is a comprehensive service provider for
shortcuts or quick fixes. Over time, this
professional inspection, installation, repair and maintenance of
sense of responsibility is passed on to
smoke and fire containment barriers for healthcare facilities.
new personnel, fostering an environment
of teamwork and ownership. For this
reason, a mentorship program and
a clear succession plan should be
developed, published, and executed as a
compliment to the training program.
Again, the insight from knowing
what you don’t know can ultimately
deliver powerful results, especially
Firestopping
Smoke & Fire
Fire Door Inspection Life Safety Surveys/
when a strategy to improve is carefully
Services
Dampers
and Labeling
Statements of Care
crafted and deliberately executed. When
individuals feel as though they are an
www.EOCSolutions.com
investment and not a commodity, their
Contact Chris: CLittrell@EOCSolutions.com or 215-258-3910
commitment to excellence exceeds
Contact Aaron: AWeiskittle@EOCSolutions.com or 419-309-7424
all expectations.
n
Automate Your
Environment of Care Rounds
Walsh Rounds Tracker
SERVICES
54 www.ashe.org | Commissioning insider
760288_EOC.indd 1
04/08/15 11:36 PM
Water commissioning:
Keeping the
flow smooth
By John M. Dombrowski, PE, HFDP, CPMP, CCP, LEED,
associate principal, Mazzetti, and
Heather L. Platt, PE, senior associate, Mazzetti
W
ater systems are the lifeblood of health
care facilities. Power outages get a lot
of attention, but a disruption in water
service can cause just as much trouble.
Commissioning your water system
after construction is complete, or recommissioning at some point after the facility is occupied,
is an essential step toward reliability.
As with commissioning other elements of your
hospital, commissioning your water system is a multistep process. It begins with a plan, which leads to an
investigation. After the investigation, improvements
are made, and the system is formally handed off to the
operations and maintenance team. To make sure the
improvements last, an on-going commissioning process
may also be developed.
Making the plan
To examine your facility’s water system, a team of
responsible, knowledgeable personnel need to be
assembled and dedicated to water safety. This team
should include members from administration, facilities,
infection prevention control, and other departments
such as nursing as needed. The purpose of this team is
to develop, implement, and manage an appropriate risk
management program for the water system(s).
A good place to start a program is with a detailed
diagram of how water flows through a facility. This
diagram provides facility personnel with an overview
of the system and identifies the system’s intended
operational goals.
Start with your original construction documents. Many
will already include a flow diagram of the system, or at
least the main components. These documents
>>
www.ashe.org | Commissioning insider 55
commissioning insider
WAtER SyStEMS
likely will not include areas that were added subsequent to
construction, nor any new or replacement equipment.
Identify the source of water and service entrances. Create a
comprehensive system diagram that indicates all equipment
and maintenance shut-off valves; this will be important to the
long-term operation of the system. This comprehensive diagram
helps the commissioning agent and a facility operator identify
potential areas of concern and inspection and testing locations
for water quality testing.
Once they understand what the water system should be
doing, the commissioning team can develop an inspection plan.
This involves examining every element, from intake to reservoirs
to discharge. Proper commissioning will reveal vulnerabilities in
the mechanical elements of the water system, and may reveal
leaks and other inefficiencies. The most important issue that may
be revealed by commissioning is the risk of pathogen growth.
The mechanical elements section lists some of the areas
that need to be examined during commissioning. This is not
a comprehensive list, but it gives you an idea of what the
inspection entails.
Pathogen growth
A consultant we know received a call from a newly
built major academic cancer center that reported a case of
Legionellosis. Investigation revealed that the facility had been
built with plastic pipe, had major dead ends, and had stored
the pipe outside before installing it. Also, the pipe had been
filled almost one year before occupancy of the building,
which meant water stood dormant in those pipes for nearly a
year. The facility did not commission the plumbing systems,
so the appearance of Legionella within weeks of occupancy
was no surprise.
On the other hand, we interviewed a colleague who holds
a leadership role within a facility group at a large health
system that very carefully monitors its water safety. The
facility samples water every quarter from random faucets,
shower heads, cooling towers, and other places where waterborne pathogens could grow. Nevertheless, occasionally
something potentially dangerous, such as a strain of the
bacteria that causes Legionnaire’s, shows up in minuscule
quantities. Pathogens can find a home even in presumably
well-maintained systems.
So what should you consider during commissioning
regarding pathogen growth? Keep in mind that many
pathogens prefer to grow in still water, so look for and control
spots where water pools and is not regularly circulated. Some
possible examples include storage tanks, dead ends of pipes,
and cooling towers.
Another area of concern is medical equipment that uses
water or has a potential for generating condensation. This
equipment should be routinely inspected to make sure it is
properly cleaned, drained, and stored per the manufacturers’
recommendations.
Mechanical elements
The mechanical elements of a hospital’s water system are
complex. The commissioning inspection will evaluate the entire
system, but some focus points will include the following:
• Inflow: The water entering the hospital needs to be clean and
secure. Among the issues to consider about inflow is how it
is being disinfected before it enters the hospital and whether
the disinfection system is operating properly.
Another issue to consider when examining the water
inflow is backflow prevention. Backflow is dangerous,
because it could allow pathogens from the facility to enter
the community’s general water system. Thus, codes require
a backflow prevention system. Additionally, and just as
important, routine inspections and annual testing should be
conducted to ensure the backflow system remains functional.
• Water piping systems: Among the many elements in
the piping system that need to be examined during
commissioning are the hand-held showerheads and faucets,
aerators, and hot water tanks.
• Cooling towers: Cooling towers in hospitals require regular
attention. Issues to consider during commissioning include
shutdown, start-up, and standby modes of operation; water
treatment; and maintenance procedures.
• Whirlpools/spas: Whirlpools and spas cause water to
aerosolize, which increases the transmission of some
pathogens. Similar to cooling towers, issues to consider
during commissioning include shutdown, start-up,
and standby modes of operation; water treatment; and
maintenance procedures.
56 www.ashe.org | Commissioning insider
759086_KLG.indd 1
30/07/15 4:41 pm
Similarly, a plan should be in place
to deal with internal failures of the
water system, such as a critical pump
breaking down or a major leak occurring.
What steps are identified within the
management plan to deal with these
potential problems?
After the inspection
The water commissioning process
is considered a singular event, but it
should lead to a chain of other events. For
example, an improvement plan should
Efficiency issues
An important role of water
commissioning is ensuring that the system
is running efficiently. Hospitals use a lot of
water, so conserving should be a priority.
Checking for leaks in the system is one
obvious aspect of this task, but in addition,
ensure that all valves are closing properly.
Another conservation issue involves
credit for water that does not flow into the
sewer. Health care facilities are typically
charged by water utilities for the amount
of water that goes in and the amount that
enters the sewer after being used. The
water entering the sewer is not metered:
the utility assumes as much water is
going out as went in. Many times this is
not the case, such as when water is used
for landscaping or to make up water that
has evaporated in a cooling tower. The
commissioning examination should verify
that meters exist to measure this water so
the facility can report it to the water utility
for a credit.
DESIGN WITH
CONFIDENCE.
Introducing the Next-Generation
PresSura™ Hospital Room
Pressure Products
With thousands installed, TSI PresSura™
Room Pressure Monitors and Controllers are
the industry standard for monitoring safety in
isolation rooms, operating rooms and rooms for
pandemic preparedness. Backed by our unique
pressure sensor, PresSura Products provide
precision measurements with high stability.
The next-generation PresSura Products offer
best-in-class features for confident isolation
room designs:
+ Expanded multiple room monitoring
+ Customizable on-screen notifications
+ Temperature and humidity measurements
+ BACnet® integration
Designed to comply with ASHRAE/ASHE 170,
CDC, and AIA Guidelines, you can be confident
that PresSura Room Pressure Products will
be created based on the inspection.
This plan should be developed by the
commissioning team in conjunction with
the water management team, and it should
be part of the documents for the system.
A final important step in the
post-commissioning process is the
establishment of, or confirmation of,
on-going procedures to maintain the
water system. This helps maintain the
improvements made after commissioning
and keeps the system healthy for the
long term.
n
commissioning insider
• Water treatment/filtration systems:
Water treatment and filtration are
common in hospitals, as these
ensure that the water is clean. The
operations personnel must have
a complete understanding of the
system to ensure effectiveness. Issues
to consider during commissioning
include modes of operation,
chemical treatment monitoring, and
maintenance procedures.
• Water heating/cooling: Properly
position water heating or cooling in
relation to the water treatment system
because some heating or cooling
applications may have a negative
effect on water treatment.
meet your standards.
Plan for failure
The commissioning process should
also ensure that the facility has a plan
in place to deal with a failure. For
example, if a water main breaks, is there
an alternate way for water to enter the
facility? Some facilities can get their
incoming water from different water
mains, allowing for isolation when a
break occurs. In other cases, a facility
makes an agreement with a local
company to supply water from a tanker
truck through an external connection to
the system.
Learn more at
www.tsi.com/pressura
UNDERSTANDING,
ACCELERATED
679456_TSI.indd 1
www.ashe.org | Commissioning insider 57
01/03/14 8:58 AM
monitoring
the operating budget. Commissioning
is all about fine-tuning systems and
equipment to meet a hospital’s goals.
Rx for healthy hospitals:
Monitor-based
commissioning
By Joe D’Arrigo, regional service manager, Schneider Electric
B
uildings, systems, and
equipment change over time.
Performance may decline.
Components may break or fail.
Other needs may arise. To deliver
the desired results, everything
needs maintenance—whether proactive,
reactive, or scheduled. At the same time,
technology continues to evolve and
facility staff and building owners often
struggle to stay current, leverage existing
systems, and do more with less.
Hospitals are no exception. Their
reason for being is to deliver high-quality
care, and their facilities play an important
role in achieving that goal. Hospitals face
the task of managing existing systems and
infrastructure while juggling challenges
ranging from budget constraints, staff
productivity, and regulatory standards
58 www.ashe.org | Commissioning Insider
to patient satisfaction, safety, and energy
mandates. As a result, hospital personnel
are always making choices that involve
trade-offs.
One way to resolve dilemmas that
may arise involves getting the right
information to the right person at the
right time to enable more informed
decision-making. Monitor-based
commissioning does just that. Monitorbased commissioning tools provide
intelligent control, management
flexibility, and meaningful analytics.
Designed to improve infrastructure
efficiency, these tools enable facility
staff to schedule maintenance and
minimize system downtime. In addition,
energy procurement and sustainability
planning software can help set a facility’s
energy strategy and add money back to
Focus on fine-tuning
A hospital’s facility staff must be
ready to respond to both expected
and unexpected changes ranging from
increased regulatory demands and rising
energy costs to environmental mandates
and innovations in technology. Moreover,
they need to understand why specific
issues arise and which remedies will drive
operational efficiency, mitigate risk, and
improve the value of existing assets.
Commissioning is a valuable tool to
help hospitals look at individual pieces
of equipment and whole systems to
identify faults and opportunities for
improvement. Different commissioning
strategies are used to fine-tune a
hospital’s equipment and systems:
•Initial commissioning ensures that
a new hospital operates as intended
and that facility staff is prepared
to operate and maintain systems
and equipment.
•Retrocommissioning seeks to
improve how existing equipment
and systems function together, with
a goal of improving operations and
maintenance (O&M) procedures to
enhance overall performance.
•Recommissioning occurs when a
previously commissioned hospital
undergoes another commissioning
process triggered by a change in
building use or ownership, the onset
of operational problems, or some
other need.
•Monitor-based commissioning
leverages manual remote
monitoring services or advanced
analytics engines to continuously
diagnose facility performance and
to identify equipment and system
faults, sequence of operations
improvements, and trends in system
and energy use.
Monitor-based commissioning
consistently maintains a hospital’s
performance at the desired level
over time. Systems and equipment
Verification of connections
Checking connections of electrical
equipment is essential to maintaining the
project schedule and controlling costs.
For example, cable entry requirements
are project specific; it is much easier
and less costly to make changes at the
manufacturer. Further, the sequence of
relays and mechanical connections—
including breaker cradles, busbar
connections, current transformers,
protective relays, instrument contactors,
switches, fuses, meters, mimic bus, and
any indicator lights and labels—should
be verified during testing. Making
changes in the field can take weeks and
throw the entire project off schedule.
An example: Automatic transfer switch
testing yields powerful advantages
Health care electrical systems
need to ensure always-on power for
essential systems to support patient
care. Automatic transfer switches (ATS)
are a crucial component of the backup
power protection, safeguarding the
availability of critical systems. Rigorous
witness testing provides a crucial
opportunity to verify how long it will
take to switch between utility and backup power systems, so facility managers
know exactly how much time it takes to
achieve a transfer.
During a recent witness test of an
ATS for a hospital expansion project in
the United States, the commissioning
agent and project team saw that the
combined sequential delay of the
generator, paralleling system, and
ATS exceeded code requirements for
completing a transfer to the backup
power source within 10 seconds.
The issue was caught before the ATS
equipment was shipped, and the project
team and manufacturer were able to
make adjustments to the programmed
time delays without adversely affecting
project schedules.
In this case, a capacitor bank and
timer were used to support Joint
Commission accreditation. The capacitor
bank helped support ride-through power
for the programmable logic controller
(PLC), which had been powering down;
this reduced the overall time to connect
to generator power and added a layer
of redundancy.
Despite the changes and added
equipment, making modifications
before equipment delivery was much
simpler; making such changes onsite
would be more difficult, costly, and timeconsuming. Engineering drawings would
need to be reworked, experts would
have to be brought in, and a service team
would be needed to make the fix. All in
all, the modifications could have added
weeks to the overall project schedule
and increased costs would be dramatic.
Conclusion
Rigorous and properly planned
witness testing can help avoid delays
and budget issues and reduce the risk
of adversely affecting patient care and
schedules. As an added bonus, with
witness testing facility managers become
familiar with system operation before the
equipment is onsite, necessary system
changes can be better planned and
less costly, and documentation can be
completed faster.
n
Repairing & refinishing tubs, tile, showers & vanities since 1979
Is your TILE making
patients sick?
Before
Grout lines hide infectious germs and bacteria!
After!
Don’t give germs a place to hide!
commissioning insider
5
Our process creates an easy-to-maintain barrier against bacteria
Surface Solutions without replacement for:
Tile Showers
Tile Floors
Tile Walls
Tile Shower Pans
See our work and case studies at:
MiracleMethod.com/hospitals
Email: sales@miraclemethod.com
Call 800-444-8827 for an estimate or referral
760878_Miracle.indd 1
Each franchise is independently owned and operated.
www.ashe.org | Commissioning insider 61
8/7/15 6:15 AM
Advertisers’ index
AIR CURTAINS/AIR DOORS
Powered Aire ..................................................38
www.poweredaire.com
AIR FILTERS
American Air Filters International ................... 14
www.aafintl.com
AIR FLOW INDICATORS
Airflow Direction, Inc. .....................................35
www.airflowdirection.com
LAMIFLOW technologies, LLC ........................43
www.Lamiflowtech.com
AIR FLOW MONITORS
Airflow Direction, Inc. .....................................35
www.airflowdirection.com
BATH FIXTURES
AcornVac......................................................... 16
www.acornvac.com
BLUEPRINT SCANNING
AccuScan........................................................46
www.GetAccuScan.com
BUILDING MANAGEMENT SYSTEMS
AKF Group ......................................................49
www.akfgroup.com
Automated Logic Corp. ...........Inside Front Cover
www.automatedlogic.com
FACILITIES MAINTENANCE
EQUIPMENT & CARTS
FlexCart, LLC ..................................................20
www.flexcartllc.com
FIRE DOOR INSPECTIONS
Fire Door Solutions ......................................... 39
www.firedoorsolutions.com
FIRE PROTECTION SYSTEMS
3M Industrial Adhesives
& Tapes.............................Outside Back Cover
www.3M.com/firestopfoam
EOC Solutions, LLC .........................................54
www.eocsolutions.com
ROOFING
Sika Sarnafil Inc.............................................. 27
www.thicknessguarantee.com
GERM & BACTERIA ABATEMENT
Miracle Method Surface Refinishing............... 61
www.MiracleMethod.com/hospitals
SAFETY/SECURITY
Dynalock Corporation ..................................... 12
www.dynalock.com
G4S .................................................................35
www.Risk-Never-Sleeps.com
Graybar Electric ................................................ 3
www.graybar.com/get-cured
HEALTHCARE LIGHTING
H.E. Williams, Inc. ........................................... 21
www.hew.com/healthcare
HVAC ENGINEERING
AKF Group ......................................................49
www.akfgroup.com
62 inside ashe | Fall 2015
PLUMBING ENGINEERING
AKF Group ......................................................49
www.akfgroup.com
FOOD WASTE DISPOSAL
EnviroPure Systems, Inc .........Inside Back Cover
www.enviropuresystems.com
CONSTRUCTION
AccuScan........................................................46
www.GetAccuScan.com
RectorSeal ..................................................... 31
www.rectorseal.com
EMERGENCY/BACKUP POWER
Russelectric .................................................... 13
www.russelectric.com
PAINT
The Sherwin-Williams Company....................... 9
www.swhealthcaresolutions.com
PLUMBING FIXTURES
Willoughby Industries, Inc. ..............................30
www.willoughby-ind.com
HVAC
Titus................................................................40
www.titus-hvac.com/critical
TSI Inc............................................................. 57
www.tsi.com/pressura
UV Resources* ................................................ 17
www.uvresources.com
ELECTRICAL ENGINEERING
AKF Group ......................................................49
www.akfgroup.com
MECHANICAL INSULATION
Isave Team........................................................ 7
www.isaveteam.com
FIRESTOP CONTRACTORS
Isave Team........................................................ 7
www.isaveteam.com
COMMISSIONING
AKF Group ......................................................49
www.akfgroup.com
ccrd.................................................................48
www.ccrd.com
KLG Jones, LLC ..............................................56
www.klgjones.com
CONSULTANTS/CONTRACTORS
AccuScan........................................................46
www.GetAccuScan.com
HTS, Inc. ......................................................... 21
www.consultHTS.com
MAINTENANCE MANAGEMENT SOFTWARE
FacilityDude .................................................... 51
www.facilitydude.com
ICE MACHINE MANUFACTURER
Scotsman........................................................ 11
www.scotsman-ice.com
INDOOR AIR QUALITY SERVICES
Oberon Wireless ............................................... 4
www.oberonwireless.com
LIGHTING
H.E. Williams, Inc. ........................................... 21
www.hew.com/healthcare
LIGHTING DESIGN
AKF Group ......................................................49
www.akfgroup.com
H.E. Williams, Inc. ........................................... 21
www.hew.com/healthcare
SOFTWARE
Walsh Integrated.............................................54
www.walshintegrated.com
TECHNOLOGY
AccuScan........................................................46
www.GetAccuScan.com
Z-Band Video, Inc. .......................................... 17
www.z-band.com/healthcare
TELEVISION DISTRIBUTION SYSTEMS
Z-Band Video, Inc. .......................................... 17
www.z-band.com/healthcare
WATER HEATERS
PVI Industries..................................................26
www.pvi.com
Please support the
advertisers that make
this publication
possible.
GET USED TO
SEEING YOUR
FAVORITE
TRASH
HAULER
A LOT LESS
FREQUENTLY.
With the EnviroPure food waste decomposition system, you can completely
eliminate the cost of hauling food waste, increase your diversion rate and
reduce your carbon footprint. By a simple and safe organic process, the
EnviroPure system turns food waste into nutrient-depleted greywater in less
than 24 hours. There’s no odor, sludge or bacteria unlike other disposal
systems, and you can save tens of thousands of dollars annually in hauling fees.
Save money and get closer to your zero waste goal, even if it means ignoring
the trash man. Visit www.enviropuresystems.com to learn more.
–\HDUDYHUDJH52,
–SRXQGVRIIRRGZDVWHGDLO\
6DIHIRUPXQLFLSDOZDWHUV\VWHPV
+DQGOHVEXONRUFRQWLQXRXVIHHG
&XVWRPPDGHWRLPSURYHZRUNÁRZDW\RXUIDFLOLW\
)LQDQFLQJDQGOHDVHRSWLRQVDYDLODEOH