Clinical Neurophysiology 115 (2004) 1697–1708
www.elsevier.com/locate/clinph
Electric field properties of two commercial figure-8 coils in TMS:
calculation of focality and efficiency
Axel Thielschera,*, Thomas Kammerb
b
a
Department of Psychiatry III, University of Ulm, Leimgrubenweg 12-14, D-89075 Ulm, BW, Germany
Cortical Physiology Research Group, Department of Neurology, Hertie Institute for Clinical Brain Research, University of Tuebingen, Tuebingen, Germany
Accepted 21 February 2004
Available online 2 April 2004
Abstract
Objective: To compare two commonly used TMS coils, namely the Medtronic MC-B70 double coil and the Magstim 70 mm double coil,
with respect to their electric field distributions induced on the cortex.
Methods: Electric field properties are calculated on a hemisphere representing the cortex using a spherical head model. The coil designs
are characterised using several parameters, such as focality, efficiency and stimulation depth.
Results: Medtronic and Magstim coils exhibit similar focality values and stimulation depths, despite very different coil designs. However,
the Medtronic coil is about 1.2 times more efficient compared to the Magstim coil. This difference corresponds to different motor and visual
phosphene thresholds obtained in previous physiological studies, thereby validating the chosen coil modelling approach. Focality of the
Medtronic coil changed less with varying coil –cortex distance compared to the Magstim coil, whereas both coils exhibited similar
dependencies on changes in cortex radius.
Conclusions: The similar values for focality and stimulation depth indicate that both coil types should evoke similar physiological effects
when adjusting for the different efficiencies. The different physiological thresholds of the two coils can be traced back to differences in coil
design. Ideally, focality should depend neither on coil– cortex distance nor on cortex radius in order to allow for an inter-subject
comparability. In particular, in motor mapping experiments the size of the resulting maps is affected by these two parameters. Consequently,
they are at least partially the cause of the variability across subjects seen in these experiments.
q 2004 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
Keywords: Transcranial magnetic stimulation; Coil design; Electric field properties; Focality; Efficiency
1. Introduction
An important question in transcranial magnetic stimulation is to determine the site and size of stimulated cortex.
For these purposes the geometries of the electric field
induced by different coil types have been characterised by
theoretical calculations (Jalinous, 1991; Ravazzani et al.,
1996; Roth et al., 1990; Ruohonen, 1998; Zimmermann
et al., 1996) or measurements of the electric currents
induced in saline tanks (Maccabee et al., 1993). For
example, using idealised coils consisting of one or two
wire loops, it has been demonstrated that figure-8 coils
allow for a more focused stimulation than simple round
* Corresponding author. Tel.: þ 49-731-5004-1253; fax: þ 49-731-50026751.
E-mail address: axel.thielscher@medizin.uni-ulm.de (A. Thielscher).
coils (Ravazzani et al., 1996). However, electric field
calculations for the standard commercial figure-8 coils are
still lacking. In the manuals of the manufactures only
calculations of the induced magnetic field are given.
In the present paper we will compare the electric field
properties of two commonly used figure-8 coils, namely the
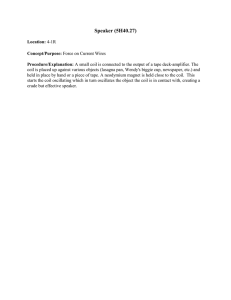
Magstim 70 mm (P/N 9790) and the Medtronic-Dantec MCB70 double coils (Fig. 1). The field strengths and the field
geometries induced on the cortex will be theoretically
estimated using a spherical head model (Ilmoniemi et al.,
1996; Sarvas, 1987) and compared with each other.
Furthermore, the differences between these fields and
that of an idealised figure-8 coil will be demonstrated. Our
results will be directly compared with measurements of
motor and visual phosphene thresholds using the same coil
types (Kammer et al., 2001a,b). This allows us to determine
those coil parameters causing the physiological differences
1388-2457/$30.00 q 2004 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.clinph.2004.02.019
1698
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
Fig. 1. Photos and X-ray pictures of (a) the Magstim figure-8 coil and (b) the Medtronic MC-B70 coil.
observed in the threshold measurements, in turn providing a
link between predicted fields and physiological data.
Two parameters of a TMS coil are of particular interest:
(i) the stimulation focality, and (ii) the efficiency, i.e.
the amount of stimulator energy required to elicit a
physiological response (e.g. a muscle action potential).
(i) The focality is normally defined as the cortical area in
which the electric field strength exceeds a certain value
relative to the maximum (e.g. the half maximum) (Roth
et al., 1990). The smaller this area, the steeper the spatial
decay of the field strength, in turn indicating a good focality.
For a given position over the skull, the focality of a coil can
be approximated using, e.g. a spherical head model and a
hemisphere approximating the cortex.
(ii) The energy needed to get a physiological response
when using a particular stimulator-coil-combination (i.e. the
‘efficiency’ of that combination) can be reliably measured
using activation thresholds (Kammer et al., 2001b), but up to
now it can hardly be determined by theoretical calculations.
The efficiency not only depends on the maximum field
strength induced in the cortex, but also on the stimulus
waveform and duration. For a given coil position and a given
rate of change of the coil current, the maximum field strength
only depends on the coil geometry and can be approximated
just as the focality using a theoretical head model. However,
the effects of stimulus waveform and duration on the
excitation of cortical neurons are poorly understood. Due
to the complex neuronal dynamics and geometry as well as
the interaction within the neural network, no realistic
mathematical model exists up to now. For this reason, we
focus on the efficiencies of the different coil geometries, but
do not consider stimulus waveform and duration, which
slightly differ between the stimulators of Magstim and
Medtronic (Kammer et al., 2001b). We thereby characterise
the efficiency of a coil by the maximum field strength value
induced on the cortex, assuming the coil current to change by
a rate of dI=dt ¼ 1 A/s. The higher this value, the more
effective the coil.
2. Methods
2.1. Spherical head model and dipole coil models
The induced electric field was estimated using the
spherical head model described by Sarvas (1987). The
model was implemented in MATLAB 6.0 (The Mathworks
Inc., Natick, MA) using custom-made software. It allows to
calculate the electric field which is induced in the head by a
small magnetic dipole. In turn, the field of a coil can be
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
1699
them. For example, a dipole in the middle of a wing is
surrounded by all wire loops of the wing and was therefore
weighted by n times the coil current, whereby n represents
the number of loops of that wing. In contrast, a dipole at the
outer loop is surrounded by only one loop and consequently
weighted by only once the coil current. A detailed
specification of the model of the Medtronic coil can be
found in Appendix A, the specification of the Magstim coil
is given in Thielscher et al. (2002). Both coil dipole models
were validated by comparison of calculated and measured
electric fields induced in unbounded media (Appendix B).
2.2. Focality
Fig. 2. (a) Dipole model of the idealised double coil (r ¼ 5:0 cm). The dots
indicate the positions of the dipoles. (b) The current counterrotates in the
two wings. The z direction of the dipoles in one wing is therefore
antiparallel to that of the dipoles in the other wing (indicated by the big
arrows pointing up- and downwards).
described as a superposition of the fields of appropriately
placed dipoles. A method of approximating a coil using
dipoles is described in detail by Ravazzani et al. (1996).
Briefly, the coil area is divided into subregions and the
dipoles are placed perpendicular to the coil area in
the centres of the subsurfaces. The dipoles are weighted
by the coil current and the areas of the subregions. For
example, the idealised figure-8 coil used in this paper can be
modelled as two circular disks (radius r ¼ 5 cm), which are
divided into 10 rings each. Each ring is further divided into
elements and the dipoles are placed in the centres of the
elements, as shown in Fig. 2. The inner and outer radii of the
rings as well as the number of elements of each ring are
given in Table 1. The current counterrotates in the two
wings. The direction of the dipoles in one wing is therefore
antiparallel to that of the dipoles in the other wing.
The dipole models of the Magstim and Medtronic coils
were created using X-ray pictures (Fig. 1). In contrast to an
idealised coil, the coils of Magstim and Medtronic consist of
several wire loops of different radii in each wing. In order to
take this into account, the dipoles were weighted by the area
of the subregion and the amount of current circling around
Table 1
Dipole model of the idealised 50 mm double coil: inner and outer radii of
the rings representing one wing and number of elements per ring
Inner
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5
radius (cm)
Outer
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0
radius (cm)
No. of
3
9
16
22
28
35
41
47
53
60
elements
The focality of a coil was determined by calculating the
electric field on a hemisphere representing the cortex (radius
r ¼ 8 cm; change of coil current dI=dt ¼ 1 A/s; see right half
of Fig. 3). The coil centre was placed 1.5 cm above it and the
coil was oriented tangentially to it. The hemisphere was
divided into subareas of 0.24 mm2 and the electric field
strength was calculated in the centre of each subarea. The total
area of the hemisphere, in which the field strength exceeded,
e.g. 50% of the maximum value, could then be simply
determined by counting the number of subareas having a value
offield strength greater than the given threshold and weighting
the result with 0.24 mm2. Assume, for example, that one
stimulates a point-wise cortical area at motor threshold.
Assume further, that the cortical excitation threshold is
constant in the area under the coil and that the hemisphere is a
sufficient approximation for the cortex surface. Then the area
as determined above gives the approximate cortical area,
which is stimulated when the stimulation level is raised to
twice the motor threshold. Using the method described above,
we systematically calculated the approximate cortical areas,
which are stimulated at 110 –200% intensity in relation to the
threshold in steps of 10%.
Fig. 3. Stimulated areas on a hemisphere for relative stimulation intensities
ranging from 110 to 200% with three different figure-8 coils: Medtronic,
Magstim and an idealized 50 mm coil. The Medtronic coil was calculated
with two orientations: (1) ‘normal’ orientation with the wings angled along
the convexity of the head, (2) ‘flipped’ with the wings pointing away from
the convexity. The idealised coil consists of two single loops with a
diameter of 50 mm each. Calculations are based on a sphere with
rCortex ¼ 8 cm, coil–cortex distance is d ¼ 1:5 cm (inset on the right).
1700
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
Subsequently, the influence of cortex radius on coil
focality was tested by keeping the coil –cortex distance
constant at 1.5 cm and systematically calculating focality
values for cortex radii between 6 and 8.5 cm (step size
0.5 cm) using 120 and 200% relative stimulation intensities.
Finally, the impact of coil – cortex distance on focality
was determined by keeping the cortex radius constant at
8 cm and varying the coil –cortex distance between 0.5 and
3 cm (step size 0.5 cm). Again, focality values for 120 and
200% relative stimulation intensities were calculated.
2.3. Decay of field strength with increasing
stimulation depth
For figure-8 coils it is known that the maximum field
strength is always located under the midpoint of the coil
for all stimulation depth (Cohen et al., 1990). In order to
determine the rate of decay of field strength with
increasing stimulation depth, we thus calculated the
electric field strength on a line perpendicular to the coil
surface and starting in the midpoint of the coil (inset of
Fig. 7a; change of coil current dI=dt ¼ 1 A/s). We
determined the field strength induced on that line for
both the Medtronic and Magstim coils, respectively.
Subsequently, we compared the efficiencies of their
designs by taking the ratio of the obtained field strength
values.
Finally, the steepness of field strength decay with
increasing stimulation depth was characterised by determining the distances at which the field strength was 66 and 33%,
respectively, of the maximum field strength value at the
cortex with r ¼ 8:0 cm.
Fig. 4. Field geometries induced on the cortical hemisphere (rCortex ¼ 8 cm, distance d ¼ 1:5 cm). The view from above on the head model is shown. Coil
configurations are the same as in Fig. 3. The field of the Medtronic coil is slightly asymmetric. Compared to the two commercial coils, the idealised double coil
has a more oval field geometry.
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
3. Results
3.1. Focality and geometry of the induced electric fields
The estimated cortical areas which are stimulated at
110 – 200% relative intensities are depicted in Fig. 3.
Unexpectedly, no large difference was found comparing
the size of the areas stimulated by the Magstim coil and the
Medtronic coil, although coil geometry largely differs. The
two wings of the Magstim coil are side-by-side in one plane
and they do not overlap. In contrast, the outer wings of the
Medtronic coil are bend by angles of 168 (right
wing) and 18.58 (left wing) towards the skull (Figs. 1b
and A1). Furthermore, the wire loops overlap in
the central part. Nevertheless, the Magstim coil
was slightly less focal compared to the Medtronic coil
1701
(e.g. Magstim/Medtronic ¼ 35/29.6 cm2 at 200% relative
intensity; Fig. 3). In order to determine the effect of the
bends of the Medtronic coil on focality, we additionally
flipped it and placed it up-side-down on the skull, with the
bends pointing away from the skull and then repeated the
calculation for that arrangement. The focality was slightly
increased by that arrangement (e.g. about 0.9 cm2 at 200%
relative intensity with respect to the standard position).
The rather equal geometries of the fields induced on the
hemisphere by the different coils was visualised by contour
plots, with the contours depicting isolevel values of the field
strength (Fig. 4). The greatest difference can be observed
when comparing the geometries of commercial coils with
the idealised coil, with wider and shorter field distributions
of the commercial coils (due to the wire loops having a
range of different radii) and a more oval shaped distribution
Fig. 5. Geometries of the vector potential induced on the cortical hemisphere (rCortex ¼ 8 cm, distance d ¼ 1:5 cm). The view from above on the head model is
shown. Coil configurations are the same as in Fig. 3. The distributions of the vector potential are markedly less focal than the electric fields calculated using the
spherical head model (compare Fig. 4).
1702
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
of the idealised coil. The wire loops of the Medtronic coil
overlap in the central part, resulting in unequal distances of
the two wings to the cortex (Appendix A). However, these
unequal distances do not remarkably shift the point of
maximum field strength away from a position directly under
the midpoint of the coil.
In order to visually demonstrate the substantial impact of
the spherical boundary on the electric field distribution, we
calculated the vector potential (i.e. the electric field in an
unbounded medium) on the ‘cortex’ hemisphere (Fig. 5;
compare with Fig. 4). In consequence, we concentrate on the
spherical model in the current paper to ensure more realistic
values of focality and efficiency (see Ravazzani et al. (1996)
for a systematic investigation of the impact of different
boundaries on the induced electric field).
3.2. Dependence of focality on coil –cortex distance
The focality of the idealised coil crucially depends on the
coil –cortex distance, as can be seen in Fig. 6a (left). For a
relative intensity of, e.g. 120%, the stimulated cortex
area varies between 3.28 and 9.68 cm2 for dcoil – cortex of
0.5 and 3.0 cm, respectively. This is an increase of 295%. In
contrast, the Medtronic coil has the most docile behaviour,
with an increase from 6.5 to 7.5 cm2 (< 115%). The increase
of the Magstim coil from 6.24 to 8.89 cm2 (< 142%) is
markedly higher than that of the Medtronic coil. In general,
the same differences between the coils can be observed for
200% relative stimulation intensity (Fig. 6a, right),
indicating that they are maintained over the full range of
relative intensities.
3.3. Dependence of focality on cortex radius
All coils show a moderate increase of stimulated area
(i.e. a decrease of focality) with increasing cortex radius
(Fig. 6b, left). At a relative stimulation intensity of 120%,
the idealised coil has the highest increase from 5.6 to
6.8 cm2 for cortex radii of 6 and 8.5 cm, respectively
(< 122%). The Medtronic and Magstim coils both have an
increase of 119%. The focality values for 200% relative
intensity (Fig. 6b, right) indicate that the observed increase
of stimulated area with increasing cortex radius remains
Fig. 6. (a) Dependence of coil focality on coil–cortex distance. For coil– cortex distances varying between 0.5 and 3 cm (see inset on the right,
rCortex ¼ const. ¼ 8 cm), the cortex areas stimulated at 120% (left) and 200% (right) relative intensity are depicted. (b) Dependence of coil focality on cortex
radius. For cortex radii varying between 6 and 8.5 cm, the cortex areas stimulated at 120% (left) and 200% (right) relative intensity are shown
(dCoil – Cortex ¼ const. ¼ 1.5 cm). Coil configurations are the same as in Fig. 3.
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
1703
Fig. 7. Dependence of maximum induced field strength on stimulation depth. (a) The maximum field strength induced at coil–cortex distances between 0.5 and
3 cm (rate of change of coil current dI=dt ¼ 1 A/s). The Medtronic coil achieves higher field strength values, i.e. a higher efficiency, compared to the Magstim
coil. (b) Ratio between the maximum field strength induced by the Medtronic and Magstim coils in dependence of stimulation depth.
more or less constant over the full range of relative
intensities.
3.4. Steepness of field strength decay and coil efficiency
The dependence of maximum field strength on stimulation depth is depicted in Fig. 7a (dI=dt ¼ 1 A/s). The
distances, at which the field strength is 66 and 33%,
respectively, of the maximum at the cortex hemisphere with
rCortex ¼ 8 cm, are given in Table 2. As can be seen, all coils
exhibit more or less the same decrease of field strength with
increasing stimulation depth.
It applies in first approximation that the higher the
number of wire loops of a coil, the higher its value of
maximum field strength. Consequently, it makes no sense to
compare the efficiency of an idealised coil consisting of only
two wire loops with commercial coils, as it has clearly to be
much lower. For that reason, we will focus on the two
commercial coils in the following. Although the two coil
designs result in quite equal focality values, their efficiencies differ from each other. For typical coil – cortex
distances of 1.5 cm (Kozel et al., 2000; McConnell et al.,
2001), the Medtronic coil is approximately 1.19 times more
efficient than the Magstim coil (Fig. 7b). This is mainly a
result of the bent wings, which can be seen when flipping the
coil (line with circles in Fig. 7a).
4. Discussion
The main results of the present study are: (i) focality, i.e.
the size of the electric field distribution does not largely
differ between the two commonly used commercial coils
Medtronic and Magstim, (ii) efficiency, i.e. the amount of
the induced field for a given stimulator intensity is slighly
higher for Medtronic compared to Magstim. This advantage
diminishes with an increased coil – cortex distance.
4.1. Focality
Both the Medtronic and Magstim coils have focality
values comparable to that of an idealised coil consisting of
two wire loops each with a diameter of 10.0 cm. So their
names (Medtronic MC-B70 and Magstim 70 mm double
coil) referring to the mean loop diameters are rather
misleading, as they do not allow any conclusions about
their focality. However, coil focality defined as the cortical
area stimulated at a certain above-threshold intensity is in
first instance only a technical index (Roth et al., 1990).
Several assumptions have to be made in order to allow for
conclusions to be drawn about the size of the stimulated
cortical area in reality:
† A sphere is an appropriate approximation of the cortex.
In TMS, superficial brain structures are particularly
stimulated rather than cortical tissue lying in deep sulci
(Epstein et al., 1990; Rudiak and Marg, 1994). Consequently, this assumptions holds in first approximation at
least for low relative stimulation intensities (e.g. 120%
motor threshold).
† The size of the cortical area stimulated at threshold
intensity (e.g. at motor threshold) is small and can be
neglected. While this seems to hold for, e.g. muscle
representations in M1 (Thielscher and Kammer, 2002), it
Table 2
Steepness of field strength decay with increasing stimulation depth
Field strength
Distance to cortex
relative to the
hemisphere (cm)
maximum at
rCortex ¼ 8 cm (%)
Medtronic Medtronic Magstim Idealised 50 mm
flipped
66
33
0.79
2.15
0.79
2.17
0.86
2.34
0.82
2.34
1704
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
is unclear for other cortical areas. The areas given in Fig.
3 are thus minimal values.
† The spherical head model describes the real electric field
induced by a coil with sufficient accuracy. The limitations
of the model and putative future developments are
discussed in a separate section (see Section 4.4).
† The effect of current direction on the cortical activation
threshold can be neglected (Kammer et al., 2001a,b;
Mills et al., 1992; Pascual-Leone et al., 1994). The
current direction in the focus of a figure-8 coil differs
only slightly over different cortical positions (Fig. 1b of
Thielscher and Kammer, 2002). So this assumptions
seem to be uncritical for stimulation intensities slightly
above threshold, but is clearly violated for higher
intensities.
† The activation threshold is constant at different
cortical positions when keeping the current direction
constant. When comparing motor and visual thresholds
no significant correlation could be observed (Kammer
et al., 2003; Stewart et al., 2001), indicating that this
assumption may be difficult to hold. However, for the
calculation of the stimulated cortical area at low
relative stimulation intensities, the activation threshold
of only a few square centimeter of cortical tissue in
the neighbourhood of the position of maximum field
strength has to be constant. To our knowledge, no
systematic investigation has been performed up to
now addressing this question and consequently no
reliable data is available.
Taken together, the areas depicted in Fig. 3 give a good
idea about the size of stimulated cortical area at least for low
relative stimulation intensities, provided that the last
assumption holds to some degree. However, the discussion
above is only a qualitative, but not a quantitative description
of the sources of error.
4.2. Efficiency
For superficial cortical areas, the electric field induced by
the Medtronic coil is approximately 1.19 times stronger than
the field of the Magstim coil (Fig. 7b). In motor and visual
phosphene threshold measurements (Kammer et al., 2001a,
b) using the same figure-8 coils as in this paper, it was
demonstrated that the Medtronic stimulator-coil-combination is 1.3 times (motor) and 1.24 times (phosphene)
more effective than the Magstim stimulator-coil-combination. This indicates that the main part of the differences in
efficiency observed in the physiological experiments can be
traced back to the different coil designs. Several reasons are
possible for the remaining part, namely the slightly different
stimulus durations (Kammer et al., 2001b), noise in
the physiological experiments as well as deviations
between real and calculated electric field due to the
simplified sphere model and slightly inaccurate coil dipole
models (see below).
4.3. Dependence of focality on coil – cortex distance
and cortex radius
Taken together, the Medtronic double coil exhibits the
most moderate dependence of focality on variations of coil –
cortex distance and/or cortex radius. This is, e.g. important
for motor mapping experiments (Classen et al., 1998), in
which the coil focality should differ as little as possible
between subjects. However, our results clearly demonstrate
that the differences in map size observed between subjects
can at least partially be traced back to different coil – cortex
distances and cortex radii.
4.4. Limitations of the sphere model
The problem of estimating how much our calculations
using the sphere dipole model deviate from the electric
fields induced in reality can be divided into two subquestions: (i) How well do the coil dipole models (which were
created using X-ray pictures) describe the geometries of the
wire loops of the real coils? (ii) How well does the spherical
head model describe the real conductivity distribution in the
human head?
(i) We systematically measured the voltages induced in a
wire probe at several positions above the coil plane.
Subsequently, we compared the results with theoretical
values calculated using the coil dipole models and the
equation describing the vector potential (i.e. the electric
field in an unbounded medium) of a magnetic dipole
(Appendix B). The mean deviations between measured and
theoretical values were 3.5% (Medtronic) and 2.4%
(Magstim), indicating that the dipole models describe the
geometries of the real coils sufficiently good.
(ii) The limitations of spherical head models in
magnetoencephalography (MEG) and TMS have been
investigated in several theoretical as well as experimental
studies. In such models, the radial electric field component
is completely suppressed. It has been demonstrated by
Sarvas (1987) that, in consequence, the conductivity of the
sphere is not limited to a single value, but can have any
spherically symmetric profile. The induced electric field in
TMS and the external magnetic field in MEG, respectively,
are not affected by radially symmetric changes in conductivity. In first approximation, such profiles resemble the
changing conductivity levels of bone, liquor, grey and white
matter. Furthermore, Ilmoniemi (1995) showed that the
conductivity in radial direction can by an arbitrary function
of location, i.e. can be radially anisotropic. He argues that
radial anisotropies resemble conductivity changes due to
fibre bundles in the white matter. In simulation studies,
sphere models have been compared with more complex
finite element models (FEM) of the head used in MEG. It
was demonstrated that sphere models accurately describe
the magnetic field distribution of a given dipole, with
the exception of deep frontal and fronto-parietal areas
(Hämäläinen and Sarvas, 1989; Ilmoniemi et al., 1999).
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
These results can be adopted for TMS using the reciprocity
theorem describing the relation between MEG and TMS
(Ilmoniemi et al., 1996). In a previous study (Thielscher and
Kammer, 2002), we measured muscle action potentials and
used them together with theoretically determined electric
field distributions at several coil positions to determine the
most likely cortical representation of a given target muscle.
It could be demonstrated that the field strength values in the
cortical muscle representation obtained by this method
jittered with a variance of about 4% over the different coil
positions. These results indicate that the spherical head
model allows for a good approximation of the electric field
of a TMS coil at least for superficial neural structures, e.g. at
the top of a gyrus.
Future simulation studies might use more realistic
conductivity distributions derived from, e.g. diffusion tensor
measurements to bridge the remaining gap between
theoretical and physiological studies. For example, Miranda
et al. (2003) performed FEM simulations to determine the
impact of a high conductivity inclusion (resulting, e.g. from
a stroke) on the induced electric field in TMS. Furthermore,
they calculated the electric field induced in a sphere with a
constant anisotropic conductivity profile. Based on their
results, they discussed the putative influence of varying
conductivity levels in sulci due to the borders between grey
and white matter and cerebro-spinal fluid being approximately perpendicular to the outer surface of the brain. Most
interestingly, they argued that the resulting effects might be
the cause of changing stimulation thresholds with changing
coil orientations, as seen in physiological experiments
(Kammer et al., 2001a,b, 2003).
4.5. The electric field induced by TMS coils: previous
investigations
Several studies have been conducted to characterise the
electric field induced by various types of TMS coils
(Jalinous, 1991; Ravazzani et al., 1996; Roth et al., 1990;
Ruohonen, 1998; Zimmermann and Simpson, 1996).
Ravazzani et al. (1996) systematically investigated the
influence of different head models (unbounded, semiinfinite and spherical volume conductors) on the induced
field. They demonstrated the importance of using spherical
models in order to get a realistic approximation of a coil’s
field. However, they concentrated on idealised double and
round coils and did not use models of commercial coils.
Roth et al. (1990) calculated the field distributions induced
by several commercial round coils (of Cadwell and
Novametrix) and one double coil (Cadwell) using a
spherical head model and the same definition of focality
as utilised in this paper. Our study serves as a completion of
these previous approaches in that it helps to characterise the
fields of two of the most frequently used commercial figure8 coils. Furthermore, it gives a more complete characterisation of coil focality and tries to characterise the efficiency
1705
of their designs, in turn allowing for a direct comparison
with data obtained by physiological measurements.
In conclusion our modelling approach allows a meaningful approximation of the induced electric field of the two
common figure-8 coils investigated and accounts for
differences in efficiency found in previous physiological
studies. Since focality as well as stimulation depth of the
two coils hardly differ, both coil types should evoke similar
physiological effects when adjusting for the different
efficiencies. As a consequence, results from studies
performed with one of the two coils should be directly
comparable to those using the other one. Future coil
developments might consider the Medtronic design in
order to increase efficiency resulting in reduced thermal
load.
Acknowledgements
T.K. was supported by the DFG grant SFB 550/C5. The
critical comments and helpful suggestions of the anonymous reviewers helped to improve the manuscript.
Appendix A
A.1. Dipole model of the medtronic MC-B70 double coil
The MC-B70 double coil consists of two wings with 10
wire loops each (Fig. 1b). The inner and outer radii of the
loops are 1.2 and 5.4 cm, respectively. The wire is 3.5 mm
thick. In the coil centre the windings of the two wings
overlap. Next to the overlap, the windings of the left and
right wings are bent by an angle of 18.5 and 168,
respectively. The thickness of the plastic chassis is 2 mm
on the side attached to the head. Accordingly, two circular
disks with radii of 5.4 cm were used to model the wings of
the coil (Fig. A1). The disks were shifted by 3.2 cm in
positive and negative x direction, respectively, to create the
overlap. The distance between the wire loops and the
outside of plastic chassis was taken into account by shifting
the disks by 4.5 mm in negative z direction. Subsequently, a
distance of 5 mm between the two disks in negative z
direction was introduced. Each disk was divided into 12
rings and each ring was further divided into elements. The
inner and outer radii of the rings, the number of elements of
each ring, and the number of surrounding loops are given in
Table A1. To account for the height of the wire, the circular
disks were then divided into two planes each, which were
shifted by 1.0 mm in positive and negative z direction,
respectively. Consequently, a plane carries one-half of the
current and all dipoles were weighted by a factor of onehalf. The current counterrotates in the two wings. The
direction of the dipoles in one wing is therefore antiparallel
to that of the dipoles in the other wing. Finally, all dipoles in
1706
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
Fig. A1. Frontal view of the Medtronic dipole model as derived from the X-ray picture (radiological convention). The direction of the dipoles depends on the
wing (bottom left).
the right disk (as shown in Fig. A1) with an X coordinate
greater than 2.5 cm were bent up by 168 and all dipoles in
the left disk with an X coordinate smaller than 2 2.0 cm
were bent up by 18.58.
For both the Magstim and Medtronic coils, monophasic
pulses were used and the maximum voltage induced at
the beginning of each pulse was determined. At each
position, the measurement was repeated two times in
order to detect putative outliers.
The probe was put on a panel of acrylic glass having a
specific distance to the coil plane and systematically moved
along the y- and x-axes of the coils in steps of 1 cm,
resulting in a cross of measurement positions (Fig. B1b).
The distance of the acrylic glass panel to the coil was
systematically increased until the measured voltages
became too weak. The position of the probe in relation to
the coil was controlled using an optical tracking system
(Flashpoint, Image Guided Technologies, USA).
Altogether, measurements at 91 probe positions were
performed per coil (Fig. B1c).
Along the crosses of measurement positions, the vector
potential should be directed approximately parallel to the
yz-plane of the coil. Consequently, the probe should
measure zero voltage when it is rotated by 908 and its
short side points in the direction of the coil’s x-axis. In
order to determine an upper limit of voltage induced in
the twisted wire pair, we rotated the probe by 908 and
repeated the measurements for the minimal coil-probe
distance for each coil. The mean ratios between the
voltages induced in the rotated and non rotated probe was
8.4% in case of the Medtronic coil and 4.3% in case of
the Magstim coil.
Appendix B
B.1. Verification of the coil dipole models by measurement
of the vector potential field
In order to verify the coil dipole models, we measured
the voltage induced in a wire loop at several positions above
the coil plane. We compared the obtained values with the
vector potential fields of the TMS coils (see e.g. Ilmoniemi
et al., 1999) which was theoretically determined using the
dipole models.
A rectangular wire loop (5 mm £ 11 mm) embedded
in a block of acrylic glass was used as probe (Fig. B1a).
It was attached to an oscilloscope which measured the
induced voltage using a twisted wire pair. In order to
minimize putative measurement errors due to voltage
induced in the twisted wire pair (and not in the probe),
the ending of the wire pair connected to the probe was
arranged perpendicular to the coil plane. The short side
of the probe was arranged parallel to the main (y-) axis
of the coil, and the long side was parallel to the z-axis.
Table A1
Dipole model of the medtronic MC-B70 double coil
Inner radius (cm)
Outer radius (cm)
No. of elements
No. of surrounding loops
0.0
0.6
3
10
0.6
1.2
9
10
1.2
1.7
12
10
1.7
2.1
16
9
2.1
2.5
20
8
2.5
2.9
24
7
2.9
3.3
28
6
3.3
3.7
32
5
3.7
4.1
36
4
Inner and outer radii of the rings representing one wing, number of elements per ring and number of surrounding loops.
4.1
4.6
40
3
4.6
5.0
44
2
5.0
5.4
48
1
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
1707
Fig. B1. (a) Dimensions and orientation of the rectangular wire probe. (b) Measurement setup. The wire probe was embedded in an acrylic glass block and put
on an acrylic glass panel to control the distance to the coil plane. Positions were recorded using an optical tracking system. (c) Magstim coil: Distribution of the
induced voltage in dependence on the probe position. The plots are normalized to the maximally induced voltage (at x ¼ 0; y ¼ 0; d ¼ 20:3 in z-direction) and
depict the distributions of the induced voltages in the xy-planes at the five measured coil-probe distances d. The normalised field strength are coded as line
length in z-dimension. (d) Deviation between the measured and the theoretically calculated induced voltages in dependence on the probe position, collapsed
across all coil-probe distances. The deviations are coded as line length (in y-direction), normalized to the maximum value across all positions. The deviation is
approximately equally distributed across all probe-coil distances in case of the Medtronic coil. In case of the Magstim coil, the values are slightly enhanced for
the probe-coil distance d ¼ 31:6:
1708
A. Thielscher, T. Kammer / Clinical Neurophysiology 115 (2004) 1697–1708
For each probe position, we calculated the theoretically
induced voltage using the coil dipole models to
numerically integrate the vector potential along the probe
wire. Subsequently, the measured voltages and the theoretically induced voltages were normalized relative to their
maximum values. The absolute difference between the
normalized voltages was determined at each probe position to finally calculate the mean deviation between the
measured and theoretical values over all positions
(Fig. B1d). The mean deviation was 3.5% in case of the
Medtronic coil and 2.4% for the Magstim coil, indicating
that the dipole models describe the geometries of the real
coils sufficiently good.
References
Classen J, Knorr U, Werhahn KJ, Schlaug G, Kunesch E, Cohen LG, Seitz
RJ, Benecke R. Multimodal output mapping of human central motor
representation on different spatial scales. J Physiol 1998;512(1):
163– 79.
Cohen LG, Roth BJ, Nilsson J, Dang N, Panizza M, Bandinelli S, Friauf W,
Hallett M. Effects of coil design on delivery of focal magnetic
stimulation. Technical considerations. Electroencephalogr Clin Neurophysiol 1990;75:350–7.
Epstein CM, Schwartzberg DG, Davey KR, Sudderth DB. Localizing the
site of magnetic brain stimulation in humans. Neurology 1990;40:
666– 70.
Hämäläinen M, Sarvas J. Realistic conductivity geometry model of the
human head for interpretation of neuromagnetic data. IEEE Trans
Biomed Engng 1989;36(2):165 –71.
Ilmoniemi RJ. Radial anisotropy added to a spherically symmetric
conductor does not affect the external magnetic field due to internal
sources. Europhys Lett 1995;30:313–6.
Ilmoniemi RJ, Ruohonen J, Virtanen J. Relationships between magnetic
stimulation and MEG/EEG. In: translator, editor, editors. Advances in
occupational medicine and rehabilitation, vol. 2(2). Pavia: Fondazione
Salvatore Maugeri Edizioni; 1996.
Ilmoniemi RJ, Ruohonen J, Karhu J. Transcranial magnetic stimulation—a
new tool for functional imaging of the brain. Crit Rev Biomed Engng
1999;27(3–5):241–84.
Jalinous R. Technical and practical aspects of magnetic nerve stimulation.
J Clin Neurophysiol 1991;8(1):10 –25.
Kammer T, Beck S, Erb M, Grodd W. The influence of current direction on
phosphene thresholds evoked by transcranial magnetic stimulation. Clin
Neurophysiol 2001a;112:2015–21.
Kammer T, Beck S, Thielscher A, Laubis-Herrmann U, Topka H. Motor
thresholds in humans. A transcranial magnetic stimulation study
comparing different pulseforms, current directions and stimulator
types. Clin Neurophysiol 2001b;112:250–8.
Kammer T, Beck S, Puls K, Roether C, Thielscher A. Motor and phosphene
thresholds: consequences of anisotropy. Suppl Clin Neurophysiol 2003;
56:198–203.
Kozel FA, Nahas Z, deBrux C, Molloy M, Lorberbaum JP, Bohning D,
Risch SC, George MS. How coil–cortex distance relates to age, motor
threshold, and antidepressant response to repetitive transcranial
magnetic stimulation. J Neuropsychiatry Clin Neurosci 2000;12(3):
376 –84.
Maccabee PJ, Amassian VE, Eberle LP, Cracco RQ. Magnetic coil
stimulation of straight and bent amphibian and mammalian peripheral
nerve in vitro: locus of excitation. J Physiol 1993;460:201–19.
McConnell KA, Nahas Z, Shastri A, Lorberbaum JP, Kozel FA, Bohning
DE, George MS. The transcranial magnetic stimulation motor threshold
depends on the distance from coil to underlying cortex: a replication in
healthy adults comparing two methods of assessing the distance to
cortex. Biol Psychiatry 2001;49:454–9.
Mills KR, Boniface SJ, Schubert M. Magnetic brain stimulation with a
double coil: the importance of coil orientation. Electroencephalogr Clin
Neurophysiol 1992;85:17–21.
Miranda PC, Hallett M, Basser PJ. The electric field induced in the brain by
magnetic stimulation: a 3-D finite element analysis of the effect of
tissue heterogeneity and anisotropy. IEEE Trans Biomed Engng 2003;
50(9):1074–85.
Pascual-Leone A, Cohen LG, Brasil-Neto JP, Valls-Solé J, Hallett M.
Differentiation of sensorimotor neuronal structures responsible for
induction of motor evoked potentials, attenuation in detection of
somatosensory stimuli, and induction of sensation of movement by
mapping of optimal current directions. Electroencephalogr Clin
Neurophysiol 1994;93:230–6.
Ravazzani P, Ruohonen J, Grandori F, Tognola G. Magnetic stimulation of
the nervous system: induced electric field in unbounded, semi-infinite,
spherical and cylindrical media. Ann Biomed Engng 1996;24:606 –16.
Roth BJ, Saypol JM, Hallett M, Cohen LG. A theoretical calculation of the
electric field induced in the cortex during magnetic stimulation. Muscle
Nerve 1990;13:734– 41.
Rudiak D, Marg E. Finding the depth of magnetic brain stimulation: a reevaluation. Electroencephalogr Clin Neurophysiol 1994;93:358–71.
Ruohonen J. Transcranial magnetic stimulation: modelling and new
techniques. Helsinki: Helsinki University of Technology; 1998.
Sarvas J. Basic mathematical and electromagnetic concepts of the
biomagnetic inverse problem. Phys Med Biol 1987;32(1):11–22.
Stewart LM, Walsh V, Rothwell JC. Motor and phosphene thresholds: a
transcranial magnetic stimulation correlation study. Neuropsychologia
2001;39(4):415 –9.
Thielscher A, Kammer T. Linking physics with physiology in TMS: a
sphere field model to determine the cortical stimulation site in TMS.
Neuroimage 2002;17:1117– 30.
Zimmermann KP, Simpson RK. Slinky coils for neuromagnetic stimulation. Electroencephalogr Clin Neurophysiol 1996;101:145– 52.