Detecting abnormal vital signs on six observation charts: An experimental comparison Report prepared for the Australian Commission on Safety and Quality in Health Care’s program for Recognising and Responding to Clinical Deterioration Mark S. Horswill, Megan H. W. Preece, Andrew Hill, and Marcus O. Watson May 2010 Detecting abnormal vital signs on six observation charts: An experimental comparison Preface Chief Investigator: Dr Mark Horswill School of Psychology The University of Queensland Project Manager: Ms Megan Preece School of Psychology The University of Queensland Principal Investigator: Associate Professor Marcus Watson Queensland Health Skills Development Centre Senior Consultant: Mr Andrew Hill School of Psychology The University of Queensland Corresponding author: Dr Mark Horswill m.horswill@psy.uq.edu.au (07) 3346 9520 School of Psychology, The University of Queensland, St Lucia, QLD 4072, Australia Acknowledgments We would like to thank all of the interested parties who provided us with observation charts from their hospital or area health service for inclusion the current study. We would also like to thank the following people for providing the de-identified patient data used in the experiment: Rozemary Karamatic from Royal Brisbane and Women’s Hospital; Lynette Adams from the Patient Safety Centre, Queensland Health; Kevin McCaffery from the Royal Children’s Hospital, Brisbane; Imogen Mitchell and Heather McKay from The Canberra Hospital, ACT Health; and Helen Ward and Aaron Armstrong from The Prince Charles Hospital, Brisbane. We thank David Collard (Information Division, Queensland Health) for adapting our draft versions of the Adult Deterioration Detection System (ADDS) charts into a desktop publishing format for use in the current experiment. We would also like to thank Nicola Dunbar and Alexandra Sonsie from the Commission and Jillann Farmer, Lynette Adams, and Kirsten Price from the Patient Safety Centre, Queensland Health, for their support throughout the project. We thank Mark Wetton for his assistance with the Media software. Thanks also to members of the Royal Brisbane and Women’s Hospital for their help in recruiting participants, and to staff at the Skills Development Centre, Queensland Health for their help in running the experiment. Finally we thank the research assistants who helped to prepare materials and collect the data for the current study: Melany Christofidis, Georgina Parker, Natasha Innes, Olivia Ng, John Manly, and Nonie Finlayson. 2 Detecting abnormal vital signs on six observation charts: An experimental comparison Contents Preface ....................................................................................................................................... 2 Acknowledgments...................................................................................................................... 2 Executive Summary.................................................................................................................... 4 1. Introduction ....................................................................................................................... 5 1.1 General background ................................................................................................... 5 1.2 Background to the project ......................................................................................... 6 1.3 The Adult Deterioration Detection System (ADDS) chart .......................................... 6 1.4 Rationale for the current study .................................................................................. 7 2. Method .............................................................................................................................. 9 2.1 Participants................................................................................................................. 9 2.2 Materials .................................................................................................................... 9 2.3 Design and procedure .............................................................................................. 13 2.4 Data analysis............................................................................................................. 14 3. Results .............................................................................................................................. 14 3.1 Participant characteristics ........................................................................................ 14 3.2 Error rates................................................................................................................. 14 3.3 Response times ........................................................................................................ 18 4. Discussion............................................................................................................................. 22 References ............................................................................................................................... 26 Appendix A: The ADDS chart with systolic blood pressure table ............................................ 27 Appendix B: The ADDS chart without systolic blood pressure table ....................................... 29 Appendix C: Single parameter track and trigger chart ............................................................ 31 Appendix D: Multiple parameter track and trigger chart ........................................................ 33 Appendix E: No track and trigger graphical chart .................................................................... 35 Appendix F: No track and trigger numerical chart .................................................................. 37 Appendix G: Questionnaire and Test For Novice Group ......................................................... 38 Appendix H: Questionnaire For Health Professional Group .................................................... 41 Appendix I: Summary sheet of background information ........................................................ 46 Appendix J: Participant Knowledge Test .................................................................................. 48 Appendix K: Participant Knowledge Test Answers .................................................................. 50 Appendix L: Testing manual for novice group ......................................................................... 51 Appendix M: Testing manual for health professional group ................................................... 57 3 Detecting abnormal vital signs on six observation charts: An experimental comparison Executive Summary Paper-based observation charts are the principal means of monitoring changes to patients’ vital signs. There is considerable variation in the design of observation charts and a lack of empirical research on the performance of different designs. This report describes the results of a study carried out as part of a project funded by the Australian Commission for Safety and Quality in Health Care and Queensland Health to investigate the design and use of observation charts in recognising and managing patient deterioration, including the design and evaluation of a new adult observation chart that incorporated human factors principles. The first phase of this project involved using a procedure known as heuristic analysis to review 25 observation charts from Australia and New Zealand. 1,189 usability problems, which could lead to errors in recording data and identifying patient deterioration, were identified in the charts. The results from the heuristic analysis were used to design a new chart (the Adult Deterioration Detection System [ADDS] chart) based on human factors principles and current best practice. The study described in this report involved an empirical comparison of six charts (two versions of the ADDS chart, two existing charts rated as “well designed” in the heuristic analysis, one existing chart rated as being of “average design”, and one existing chart rated as “poorly designed”). Novices (individuals who were unfamiliar with using patient charts) and health professionals (doctors and nurses) were recruited as participants. Each chart design was shown to each participant four times displaying different physiological data with one abnormal vital sign (e.g. a high systolic blood pressure), and four times displaying different normal physiological data. After memorising the normal ranges for each vital sign, participants had to classify the physiological data on the charts as “normal” or “abnormal”. Error rates (the proportion of trials where participants made an incorrect normal/abnormal judgement) and response time (the time to read the chart and make the judgement) were measured. Results indicated that chart design had a statistically significant effect on both error rates and response time, with the charts identified as having better design tending to yield fewer errors and shorter decision times. Specifically, the two versions of the ADDS chart outperformed all the existing charts on both metrics, where the other charts yielded between 2.5 and 3.3 times as many errors as the ADDS chart. There was no significant difference between novices and health professionals in error rates for any chart, but the health professionals were significantly faster than novices at making their decisions for the charts rated as “average” and “poor”. There was no significant difference between doctors and nurses on either of the two performance measures for any of the charts. These data indicate that differences in the design of observation charts have a profound impact on chart users’ decisions regarding patients’ vital signs as well as the time it takes to make such decisions. Based on the current data, it appears that the ADDS chart is significantly better at signalling patient deterioration than other currently available charts. 4 Detecting abnormal vital signs on six observation charts: An experimental comparison 1. Introduction 1.1 General background Improving the recognition and management of patients who deteriorate whilst in hospital is a priority both at the national and state level. The Australian Commission on Safety and Quality in Health Care (ACSQHC) has launched a national program for ‘Recognising and Responding to Clinical Deterioration’ (1). In parallel, Queensland Health’s Patient Safety Centre have released a strategy options paper discussing gaps in the recognition and management of the deteriorating patient (2). Changes in physiological observations or ‘vital signs’ commonly precede serious adverse events such as cardiac or respiratory arrest, unplanned Intensive Care Unit (ICU) admission, or unexpected death (3-8). Several studies report that derangements in vital signs are observable up to 48 hours before the adverse event (3, 5, 6, 9). This suggests that if deterioration is recognised early and appropropriately managed, then complications arising from delays could be reduced (e.g. morbidity, unexpected ICU admissions, extended length of stays in hospital), and some serious adverse events could potentially be avoided altogether (10-13). Paper-based observation charts are the principal means of recording and monitoring changes to patients’ vital signs. However, vital signs are not always correctly recorded or appropriately acted upon (3, 6, 9, 10, 14). The design of the observation charts themselves may contribute to failures in the ability of medical and nursing staff to record vital signs and recognise deterioration. There is considerable variation in the design of observation charts in current use in Australia. They vary in both the number and selection of vital signs monitored. Observation charts also exhibit diversity in the way in which they display information. For instance, respiration rate may be displayed on one chart as a row containing boxes in which to write the number of breaths taken by a patient per minute at each time-point, while on another chart it may be plotted as a graph over time. Finally, observation charts also vary in the degree to which they incorporate track and trigger systems based on clinical criteria to help users recognise a deteriorating patient and respond appropriately. There is presently a lack of empirical research on the design and use of observation charts. In Australia, observation charts tend to be designed at the local hospital or individual health service area level, resulting in a nationwide duplication of effort (10). Some observation charts appear to have been trialled in specific wards before full implementation or evaluated by means of a staff survey. Rigorous empirical evaluation is lacking in most cases. There are indicative findings that efforts to improve the design of observation charts can produce benefits for patients, staff, and the hospital. In the United Kingdom, Chatterjee et al. carried out an empirical evaluation of five observation charts in use at a district general hospital (15). They reported that the design of the charts had a significant effect on the ability of staff to recognise patient deterioration (with a detection rate as low as 0% for one vital sign), and that no single existing chart was best for all vital signs. As a result, they designed and implemented a new chart incorporating a track and trigger system. They found that there was a significant improvement in 5 Detecting abnormal vital signs on six observation charts: An experimental comparison staff’s ability to recognise deterioration (all detection rates over 90%), after the re-design and implementation of the new chart. Their new chart produced improvements in the detection of four forms of deterioration, hypoxia (45% increase in detection), tachypnoea (41% increase in detection), tachycardia (29% increase in detection), and fever (16% increase in detection). A recent Australian project to improve the early detection of patient deterioration, which included improvements to observation chart design (together with other interventions such as training), was found to produce statistically significant gains in the frequency of recording vital signs, as well as decreasing unplanned ICU admissions, decreasing the rate of cardiac arrests, and decreasing the rate of hospital deaths (16). 1.2 Background to the project The study described in this report was part of a research project carried out at The University of Queensland and funded by the Australian Commission for Quality and Safety in Health Care and Queensland Health. The aim of the project was to investigate the design and use of observation charts in recognising and managing patient deterioration, including the design and evaluation of a new adult observation chart that incorporated human factors principles. The initial phase of the project was a systematic usability evaluation of the quality and extent of design problems in 25 existing observation charts (17). A total of 1,189 usability problems were identified in the observation charts. Usability problems were identified as affecting the observation charts’ page layout, information layout, recording of vital signs, integration of track and trigger systems, language and labelling, cognitive and memory load, use of fonts, use of colour, photocopying legibility, and night-time legibility. In compiling lists of the various usability problems present in the observation charts, principles for producing a better designed observation chart were developed. 1.3 The Adult Deterioration Detection System (ADDS) chart Using the information obtained from the heuristic analysis, a new chart was designed by combining what were considered to be the best design features of existing charts (see reference 18 for details). The chart was largely based on: (a) The Prince Charles Hospital chart (Brisbane, Queensland), which in turn was based on the Compass chart developed at The Canberra Hospital, ACT Health, and (b) the Children’s Early Warning Tool (CEWT) paedriatric chart developed at Royal Children’s Hospital (Brisbane, Queensland). The new chart was named the Adult Deterioration Detection System (ADDS) chart and incorporated the following features designed to minimize the design problems that might lead to human error in both recording and interpreting patient data (see Appendices A and B to view the two versions of the ADDS chart). Note that the key function of the ADDS chart was to detect patient deterioration, rather than to act as a general observation chart. The ADDS chart featured both a single parameter and a multiple parameter colour-coded track and trigger system to facilitate the detection of deterioration. The single parameter system (in which a medical emergency response was required when any single patient vital sign was outside a given range) had the advantage of simplicity of use. The multiple parameter system (in which vital signs were scored using a colour-coded key and scores 6 Detecting abnormal vital signs on six observation charts: An experimental comparison were summed to give an overall indication of the patient’s condition) was potentially more sensitive to deterioration and could lead to earlier detection of deterioration or fewer false alarms (see reference 18 for further details and discussion of this issue). Chart colours were chosen such that colour density correlated with the extent to which the patient’s vital signs were outside the normal range (apart from being an intuitive progression, this strategy would aid colour-blind users). All information required for use (for example, the colour key, the medical emergency criteria, and the actions to be taken when different levels of deterioration were detected) was provided on the same page as the vital signs data. This was in order to reduce cognitive load (for example, to avoid the user having to retain vital sign data in memory while turning the page to access more information). Terms and abbreviations used on the chart were selected in part based on the preferences expressed among a large sample of health professionals. Only vital signs considered to be the most important for detecting deterioration were included on the chart. If additional information had been included, this less important information would potentially compete with the more important information for the user’s attention. Each vital sign was presented as a separate graph. Many existing charts either displayed data numerically (making it difficult to see data trends and hence making deterioration harder to detect) or included graphs with multiple vital signs plotted on the same graph area (increasing visual clutter, and potentially making deterioration harder to detect). The most critical vital signs were placed towards the top of the page, as this is where users would look first. Most existing charts did not follow this practice. Scales were labelled on both the left and right of each graph and bold vertical lines were placed every 3 columns. These features were designed to minimize the chance of users reading from the wrong column or row. There was space to record modifications to vital sign thresholds. This information was placed so that it would be in view when a user first picked up the chart. 1.4 Rationale for the current study The evidence from the heuristic analysis used to develop the ADDS chart was opinion-based and therefore required empirical verification. Given that a key aim of the new chart was to minimise errors in recognising patient deterioration, the present study was designed to investigate whether the ADDS chart was successful in this regard, relative to a range of existing charts. Six charts were 7 Detecting abnormal vital signs on six observation charts: An experimental comparison selected for empirical comparison: two versions of the ADDS chart and four charts in current use in hospitals in Australia. The four existing charts were chosen on the basis of ratings from the heuristic analysis: two of these charts were rated as “well designed”, one chart was rated as “average”, and one chart was rated as “poorly designed”. The objective of the experiment was to present actual patient data on each of the charts and ask both novices (individuals unfamiliar with using patient charts) and health professionals whether any of the vital signs were outside of pre-defined normal ranges for any timepoint. Their judgements were then coded as correct or incorrect. It was hypothesized that the charts that were rated as being better designed would yield fewer incorrect responses. It was also hypothesized that participants would be faster to reach their decision for the better-designed charts. Finally, we hypothesized that the new ADDS chart would perform at least on the same level as the charts rated as “well designed”, if not better. We also planned to compare the performance of the novices with the health professionals (for example, it could be that different chart designs favoured different groups) and, within the health professional group, compare doctors and nurses. The six charts involved in the comparison are described below. Two versions of the ADDS chart Two versions of the ADDS chart were included (see Appendices A and B). The first version included a systolic blood pressure table to allow the patient’s usual systolic blood pressure to be taken into account when deciding the normal range for this vital sign. The second version did not have this table; instead, the normal range was based on the assumption that the patient’s usual systolic blood pressure was 120 mmHg. The second version was potentially simpler to read than the first version, but the first version was likely to yield a more accurate decision as to whether a patient’s blood pressure was abnormal or not. Two existing charts rated as “well designed” in the heuristic analysis Two charts were chosen because they were rated as “well designed” and were currently being widely used in Australia. Both of these charts used colour as part of a track and trigger system and displayed nearly all of the vital signs as graphs. The first chart used a single parameter track and trigger system, with two bandings of colour (yellow and red) to denote different levels of patient deterioration outside the normal range (the chart can be viewed in Appendix C). With a single parameter track and trigger system, if any vital sign was outside its normal range, this would be signalled by the data point being recorded against a coloured background, indicating that action should be taken. The second chart used a multiple parameter track and trigger system (the chart can be viewed in Appendix D). With this system, different bandings of colour (based on the severity of deterioration) were used to score each vital sign, and scores for key vital signs were summed to provide a single number summarising the patient’s overall condition. This score was used to determine the action that should be taken. The second chart (unlike the first) also used a systolic blood pressure table to allow a patient’s usual systolic blood pressure to be taken into account. 8 Detecting abnormal vital signs on six observation charts: An experimental comparison One chart rated as “average” in the heuristic analysis One chart was chosen to represent a chart of “average” quality according to the heuristic analysis (the chart can be viewed in Appendix E). The chart was monochrome and did not have a track and trigger system. Three of the key vital signs were graphed (the rest were represented numerically). One chart rated as “poor” in the heuristic analysis One chart was chosen to represent a chart of “poor” quality according to the heuristic analysis (the chart can be viewed in Appendix F). The chart was navy and light blue and did not have a track and trigger system. All of the key vital signs were presented as numbers rather than as graphs. 2. Method 2.1 Participants A novice group (n = 44) and a professional group (n = 45) were recruited for the experiment. Novices were recruited from members of The University of Queensland and were paid $20 for participating in the study. Health professionals were recruited from staff of the Royal Brisbane and Women’s Hospital and were paid $100 for participating in the study. 2.2 Materials The following materials were developed for use in this study. Questionnaire for novice participants Before the experiment, novice participants completed a questionnaire asking for their age and sex, as well as whether they had ever worked as a health professional and whether they had ever used a hospital observation chart before. Note that there were other questions not analysed in this report. After the experiment, participants were asked whether they had previously used a chart similar to any used in the experiment. See Appendix G for the full questionnaire. Questionnaire for health professionals Before the experiment, the health professionals group were asked to complete a questionnaire that recorded their occupation (nurse/doctor/other) and further details about their nursing or medical role. They were asked the number of years that they had been registered, the postcode of their institution, and where they spent the greatest proportion of time working (ward/emergency/ICU/theatre/outpatient clinic/management etc). They were also asked to record their age and sex. They were asked whether they used observation charts as part of their current role and how frequently. They were also asked whether they recorded information into observation charts and how frequently. Finally they were asked what training they had received in the use of observation charts (none/read the instructions/informal/formal/other). Note that there were other questions not analysed in this report. After the experiment, the health professionals completed the 9 Detecting abnormal vital signs on six observation charts: An experimental comparison same post-experiment questionnaire as the novices (including asking whether they had previously used a chart similar to the ones used in the experiment). See Appendix H for the full questionnaire. Training videos All participants viewed a number of training videos before commencing the experiment. Note that all videos are available for viewing online (please contact m.horswill@psy.uq.edu.au for further information). Background video: The first video covered background information essential to understanding the different vital signs and why they are monitored, as well as explaining the normal ranges for each vital sign that were applicable to the experiment. Also explained were cut-off scores and early warning scores. The novice and professional groups received different versions of the video. The novice version (13 minutes 6 seconds) assumed no previous knowledge of vital signs and so included basic introductory information (e.g. an explanation of patient deterioration and definitions and explanations of different vital signs). The health professionals’ version (4 minutes 55 seconds) was a truncated version of the novice video, where basic knowledge about vital signs was assumed (the focus was on the normal ranges to be used in the experiment as well as explanations of cut-off scores and early warning scores). The normal ranges used in this study were taken from the track and trigger systems used by three of the charts used in the study. The ranges are shown in Table 1. Table 1: Normal ranges of vital signs used in this study. Vital Sign Normal Range Respiratory rate Between 9 – 20 breaths per minute Oxygen Delivery Patient is receiving oxygen at equal to or less than 1 L/min Oxygen Saturation Between 93 – 100% Systolic Blood Pressure Between 100 – 160 mmHg Pulse Between 50 – 100 beats per minute Temperature Between 36.1 – 37.9 Celsius Consciousness Patient is classified as “Alert” Pain Patient is in no pain Chart videos: Training videos were created for each of the six charts used in the experiment. The videos described how to read each chart, including interpreting cut-off scores or early warning scores as appropriate. Experiment instruction video: This short video described the procedure to be followed in the experiment (see section 2.3 below). Participant Knowledge Test All participants completed a 10-item four-option multiple-choice examination testing key elements of the information that they were required to have learned while watching the training videos. Questions 1 to 8 asked about the normal ranges for the eight vital signs described in the videos. The 10 Detecting abnormal vital signs on six observation charts: An experimental comparison final two questions asked for definitions of cut-off scores and early warning scores. The full examination can be viewed in Appendix J, with answers given in Appendix K. Patient data De-identified patient data was collected from a number of locations (Royal Brisbane and Women’s Hospital, Royal Children’s Hospital, The Canberra Hospital, The Prince Charles Hospital). For each patient whose observations were used in the experiment, the data spanned at least 13 consecutive time points (out of the six charts included in the experiment, the minimum number of given time points that could be recorded was 13). The cut-offs for normal ranges were taken from those provided as part of the track and trigger systems on three of the charts in the study (the two ADDS charts and the multiple parameter track and trigger chart, which were consistent with one another). Note that two of the other three charts used did not provide cut-offs and the only other chart to have a track and trigger system (the single parameter track and trigger system chart) was modified to bring the cut-offs in line with the other charts. Any vital sign outside of these cut-offs was designated “abnormal”. Forty-eight cases were obtained (cut-offs are consistent with the normal ranges presented in the background training video and tested in the knowledge test): 3 cases of hypothermia (temperature below 36.1 C) 3 cases of fever (temperature above 37.9 C) 3 cases of hypotension (systolic blood pressure below 110 mmHg) 3 cases of hypertension (systolic blood pressure above 160 mmHg) 3 cases of bradycardia (heart rate fewer than 50 beats per minute) 3 cases of tachycardia (heart rate greater than 100 beats per minute) 6 cases of hypoxia (oxygen saturation less than 93%) 24 cases of normal data For the abnormal cases, only one observation (across the 13 time points recorded for each case) was abnormal for each patient. These abnormalities were restricted to one vital sign per patient to standardise the amount of deterioration present in each case. That is, there was no patient for whom more than one data point was outside the normal ranges (across all vital signs and across all time points). The patient data was modified in the following circumstances: (1) If a data point was missing for a particular vital sign, the average of the data points from the closest available time points before and after the missing value was inserted. (2) For cases showing deterioration, if a particular vital sign became abnormal at more than one time point, the data were adjusted so as to be outside the normal range at only one time point (to ensure homogeneity across the abnormal cases). (3) For six cases (five stable, one hypotension), we only had data for 12 out of the 13 time points. In these cases, an extra time point was inserted between two existing values. Data for this extra time point was generated by calculating the mean of the data from 11 Detecting abnormal vital signs on six observation charts: An experimental comparison the time points before and after. For a seventh case (hypoxia), two extra sets of observations were inserted in this way. Preparation of charts Six charts were evaluated in this study and are detailed in Table 2 (also described earlier). Table 2: Descriptions of the six charts used in the experiment. Chart Description 1.ADDS chart with A new chart (the ADDS chart) developed in an earlier phase of the systolic blood pressure current project, including both single parameter and multiple parameter table track and trigger systems. The format was A3 double-sided and the cutoffs for systolic blood pressure could take account of a patient’s usual blood pressure (in this study, usual blood pressure was taken as 120 mmHg). The chart can be viewed in Appendix A. 2. ADDS chart without A second version of the ADDS chart, which did not have systolic blood systolic blood pressure pressure cut-offs tailored to a participant’s usual blood pressure (it table assumed that usual blood pressure was 120 mmHg for all patients). The chart can be viewed in Appendix B. 3. Multiple parameter A double-sided A4 chart with a multiple parameter track and trigger track and trigger chart system. The cut-offs for blood pressure could take account of a patient’s usual blood pressure (in this study, usual blood pressure was taken as 120 mmHg). The chart can be viewed in Appendix D. 4. Single parameter track A double-sided A3 chart with a single parameter track and trigger and trigger chart system, without systolic blood pressure cut-offs tailored to usual blood pressure. The chart can be viewed in Appendix C. 5. No track and trigger A double-sided monochrome A3 chart with no track and trigger system, graphical chart where some of the vital signs were plotted as graphs but others were not. The chart can be viewed in Appendix E. 6. No track and trigger A single-sided A4 chart with no track and trigger system and all vital sign numerical chart data written as numbers. The chart can be viewed in Appendix F. The single parameter track and trigger chart was modified using Jasc Paint Shop Pro 8 where necessary to bring its cut-offs in line with those shown on other charts (the modification resulted in lower cut-offs than were originally used on this chart, so that any given vital sign would be more likely to be classified as outside the normal ranges). This was crucial to the experiment to ensure that the charts were being compared on the basis of their design and not their chosen cut-offs (that is, without the modification, we would be unable to tell if resulting differences between charts were due to differences in design or differences in cut-offs). The other five charts were not modified. The 48 patient cases were plotted onto the six charts (6 x 48 = 288 charts in total). Data was plotted by hand by a team of trained research assistants, with the Project Manager double-checking all entries for errors. 12 Detecting abnormal vital signs on six observation charts: An experimental comparison 2.3 Design and procedure The study was granted ethics approval by the Royal Brisbane and Women’s Hospital’s Human Research Ethics Committee and by The University of Queensland’s School of Psychology Ethics Review Officer. The novice group were tested at the University of Queensland and the health professional group were tested at the Skills Development Centre, Royal Brisbane and Women’s Hospital, Queensland, Australia. Participants were tested one at a time in quiet room under good lighting by two researchers. First, participants were asked to complete a consent form and the initial questionnaire. All participants were shown the background video explaining the different vital signs and their normal ranges (the explanation was truncated for health professionals). They were then given a laminated handout summarising the cut-offs which they were required to memorise (see Appendix I). Participants’ knowledge of the normal ranges for each vital sign was tested using the Participant Knowledge Test. If they obtained less than 10 out of 10 answers correct for the test, then they were asked to review the information again and retake the test until they were able to answer all of the questions correctly. Following the test, participants were shown the training videos explaining each of the six charts. To minimise the chances of one chart receiving an advantage over another (e.g., due to primacy or recency effects), the chart training videos were shown in a different random order for each participant using custom-made software. Finally, all participants were shown the video explaining the experimental protocol. Each participant completed 48 trials in which they viewed each of the 48 sets of patient data plotted on one of the six charts. Each chart design was therefore viewed eight times, four times with normal data and four times with abnormal data (for each chart design, these four cases contained derangements in temperature, systolic blood pressure, pulse, and oxygen saturation). Each session was recorded using a digital voice recorder to allow checking of responses at a later date. The protocol for each trial was as follows. First, a chart with 13 sets of observations completed was placed in front of the participant. A timer was started when the participant starting viewing the chart. The participant had to indicate whether any of the vital signs were abnormal, or whether all of the observations were normal (based on the normal ranges given in the instructions). If they responded “abnormal”, then they had to say which vital sign was abnormal. Subsequently, the remaining 47 charts were presented to the participant, one-at-a-time, and the same procedures were followed. Note that, to prevent order effects, the 48 charts were presented in an order that was individually randomised for each participant. The testing session took approximately one and a half hours per participant. The full experiment protocol and instructions can be viewed in Appendices L (novice group) and M (health professional group). 13 Detecting abnormal vital signs on six observation charts: An experimental comparison 2.4 Data analysis Participant responses (normal vs. abnormal) and response times for each chart were entered into Microsoft Excel 2007. Data was then exported into SPSS for Windows version 17 for statistical analysis. 3. Results 3.1 Participant characteristics The novice group (n = 44) consisted of both medical students (n = 6) and other members of The University of Queensland recruited from a research participant pool (n = 38). The health professionals (n = 45) consisted of both doctors and nurses recruited from the Royal Brisbane and Women’s Hospital. Characteristics of the two groups are listed in Table 3. Two participants were excluded (both novices) for having overall error rates greater than chance (50%), given that they were unlikely to be following instructions. Note that these exclusions had no effect on the pattern of results reported. Table 3: Participant characteristics of the two groups. Novices (n = 44) Age in years 23.7 (4.4)a Gender Female: 70.5% Male: 29.5% Health profession Years registered - Health professionals (n = 45) 32.6 (8.2)a Female: 64.4% Male: 35.6% Doctor: 53.3% Nurse: 46.6% Doctor: 2.8 (2.3)a Nurse: 9.8 (10.8)a Note. aValues are mean (standard deviation). 3.2 Error rates Overall error rates (the proportion of incorrect responses) are given in Figure 1. 14 Detecting abnormal vital signs on six observation charts: An experimental comparison 45 40 Percentage Errors 35 30 25 20 Novices 15 Professionals 10 5 0 ADDS with ADDS Single Multiple No track andNo track and SBP table without SBP parameter parameter trigger trigger table track and track and graphical numerical trigger chart trigger chart chart chart Figure 1: Percentage of errors in detecting abnormal vital signs for the six charts. Error bars are standard errors of the mean. A mixed-design analysis of variance was conducted with chart type as a repeated-measures independent variable and participant group as a between-subjects independent variable. Mauchly’s test of sphericity indicated no significant sphericity in the data (Mauchly’s W = 0.771, p = 0.076). There was a significant main effect of chart type on error rates, F(5,435) = 42.08, p < 0.001. However, there was no significant effect of participant group on error rates; that is, health professionals made the same number of errors as novices overall, F(1,87) = 0.06, p = 0.807. However, there was a significant interaction between chart type and participant group, F(5,435) = 2.33, p = 0.042, potentially indicating that the health professionals made proportionally fewer errors on the monochrome charts (though see later for simple effects analyses of this interaction). Pairwise comparisons between charts were carried out separately for novices and health professionals using the Bonferroni-Holm method of correcting for multiple comparisons. Table 4 gives comparisons for the novices and Table 5 for the health professionals. 15 Detecting abnormal vital signs on six observation charts: An experimental comparison Table 4: Pairwise comparisons between charts for error rates for the novice group, arranged in order of effect size. Comparison Observed p Numerical chart vs. ADDS without SBP table No track and trigger numerical chart vs. ADDS with SBP table No track and trigger graphical chart vs. ADDS without SBP table No track and trigger graphical chart vs. ADDS with SBP table Single parameter track and trigger chart vs. ADDS without SBP table Multiple parameter track and trigger chart vs. ADDS without SBP table Single parameter track and trigger chart vs. ADDS with SBP table Multiple parameter track and trigger chart vs. ADDS with SBP table No track and trigger graphical chart vs. Single parameter track and trigger chart No track and trigger numerical chart vs. Single parameter track and trigger chart No track and trigger numerical chart vs. Multiple parameter track and trigger chart No track and trigger graphical chart vs. Multiple parameter track and trigger chart No track and trigger numerical chart vs. No track and trigger graphical chart Single parameter track and trigger chart vs. Multiple parameter track and trigger chart ADDS without SBP table vs. ADDS with SBP table Note. SBP = systolic blood pressure. 16 Comparison significant at 5% level? < 0.001 < 0.001 Critical p for significance at 5% level 0.003 0.004 < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.005 Significant < 0.001 0.005 Significant < 0.001 0.006 Significant < 0.001 0.006 Significant < 0.001 0.007 Significant < 0.001 0.008 Significant < 0.001 0.010 Significant < 0.001 0.013 Significant 0.57 0.017 Not significant 0.79 0.025 Not significant 0.92 0.050 Not significant Significant Significant Detecting abnormal vital signs on six observation charts: An experimental comparison Table 5: Pairwise comparisons between charts for error rates for the health professionals group, arranged in order of effect size. Comparison Observed p Comparison significant at 5% level? < 0.001 Critical p for significance at 5% level 0.003 No track and trigger graphical chart vs. ADDS with SBP table No track and trigger numerical chart vs. ADDS with SBP table Multiple parameter track and trigger chart vs. ADDS with SBP table Single parameter track and trigger chart vs. ADDS with SBP table No track and trigger graphical chart vs. ADDS without SBP table No track and trigger numerical chart vs. ADDS without SBP table Multiple parameter track and trigger chart vs. ADDS without SBP table Single parameter track and trigger chart vs. ADDS without SBP table ADDS without SBP table vs. ADDS with SBP table < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.005 Significant < 0.001 0.005 Significant < 0.001 0.006 Significant < 0.001 0.006 Significant 0.135 0.007 0.148 0.008 0.157 0.010 0.190 0.013 0.212 0.017 0.694 0.025 1.000 0.050 Not significant Not significant Not significant Not significant Not significant Not significant Not significant No track and trigger numerical chart vs. Single parameter track and trigger chart No track and trigger numerical chart vs. Multiple parameter track and trigger chart No track and trigger graphical chart vs. Multiple parameter track and trigger chart No track and trigger graphical chart vs. Single parameter track and trigger chart No track and trigger numerical chart vs. No track and trigger graphical chart Single parameter track and trigger chart vs. Multiple parameter track and trigger chart Note. SBP = systolic blood pressure. Significant Despite the significant interaction between chart type and novice/professional group differences (examining Figure 1 there appears to be a trend indicating that professionals produced fewer errors for the no track and trigger charts), there was no statistically reliable difference between novices and professional participants for any one chart. This means that we cannot be confident in this interpretation of the interaction. See Table 6 for pairwise comparisons with a Bonferroni-Holm correction for multiple comparisons. 17 Detecting abnormal vital signs on six observation charts: An experimental comparison Table 6: Comparisons between novice and health professionals’ error rates for the six charts, arranged in order of effect size. Chart (novice vs. professional comparison) Observed p Critical p for Comparison significance significant at at 5% level 5% level? No track and trigger numerical chart 0.078 0.008 Not significant No track and trigger graphical chart 0.099 0.010 Not significant ADDS chart with SBP table 0.153 0.013 Not significant ADDS chart without SBP table 0.465 0.017 Not significant Multiple parameter track and trigger chart 0.795 0.025 Not significant Single parameter track and trigger chart 0.942 0.050 Not significant Note. SBP = systolic blood pressure. There was no overall significant difference between the accuracy rates of doctors and nurses across all charts, F(1,43) = 1.00, p = 0.324, nor for any chart individually (see Table 7). Table 7: Comparisons between doctors and nurses’ error rates for the six charts, arranged in order of effect size. Chart (doctor vs. nurse comparison) Observed p Critical p for Comparison significance significant at at 5% level 5% level? No track and trigger graphical chart 0.017 0.008 Not significant ADDS chart with SBP table 0.187 0.010 Not significant No track and trigger numerical chart 0.586 0.013 Not significant Single parameter track and trigger chart 0.626 0.017 Not significant Multiple parameter track and trigger chart 0.635 0.025 Not significant ADDS chart without SBP table 0.663 0.050 Not significant Note. SBP = systolic blood pressure. 3.3 Response times Overall response times (regardless of whether responses were correct or incorrect) are given in Figure 2. 18 Detecting abnormal vital signs on six observation charts: An experimental comparison 25 Response time in seconds 20 15 Novices 10 Professionals 5 0 ADDS with ADDS Single Multiple No track andNo track and SBP table without SBP parameter parameter trigger trigger table track and track and graphical numerical trigger chart trigger chart chart chart Figure 2: Response times in for the six charts. Error bars are standard errors of the mean. A mixed-design analysis of variance was run with chart type as a repeated-measures independent variable and participant group as a between-subjects independent variable. Mauchly’s test of sphericity indicated a significant departure from sphericity in the data (Mauchly’s W = 0.068, p < 0.001) and so Greenhouse-Geisser estimates are reported for the degrees of freedom for all repeated-measures effects. There was a significant main effect of chart type on response times, F(2.056, 178.875) = 48.96, p < 0.001. Also, there was a significant effect of participant group on response times: Health professionals were faster to reach a decision than novices, F(1,87) = 8.69, p = 0.004. There was also a significant interaction between chart type and participant group: health professionals appeared to be proportionally faster than novices with the no track and trigger charts compared with the coloured charts, F(2.056, 178.875) = 3.86, p = 0.002. Pairwise comparisons between charts were carried out separately for novices and health professionals using the Bonferroni-Holm method of correcting for multiple comparisons. Table 8 gives comparisons for the novices and Table 9 is for the health professionals. 19 Detecting abnormal vital signs on six observation charts: An experimental comparison Table 8: Pairwise comparisons between charts for response times for the novice group, arranged in order of effect size. Comparison Observed p No track and trigger numerical chart vs. ADDS without SBP table No track and trigger graphical chart vs. ADDS without SBP table Multiple parameter track and trigger chart vs. ADDS without SBP table No track and trigger graphical chart vs. ADDS with SBP table No track and trigger numerical chart vs. ADDS with SBP table Single parameter track and trigger chart vs. ADDS without SBP table No track and trigger numerical chart vs. Single parameter track and trigger chart Multiple parameter track and trigger chart vs. ADDS with SBP table No track and trigger graphical chart vs. Single parameter track and trigger chart No track and trigger numerical chart vs. No track and trigger graphical chart No track and trigger numerical chart vs. Multiple parameter track and trigger chart ADDS without SBP table vs. ADDS with SBP table No track and trigger graphical chart vs. Multiple parameter track and trigger chart Single parameter track and trigger chart vs. ADDS with SBP table Single parameter track and trigger chart vs. Multiple parameter track and trigger chart Note. SBP = systolic blood pressure. 20 < 0.001 Critical p for significance at 5% level 0.003 Comparison significant at 5% level? Significant < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.005 Significant < 0.001 0.005 Significant < 0.001 0.006 Significant < 0.001 0.006 Significant < 0.001 0.007 Significant 0.001 0.008 Significant 0.001 0.010 Significant 0.007 0.010 0.013 0.017 Significant Significant 0.010 0.025 Significant 0.199 0.050 Not significant Detecting abnormal vital signs on six observation charts: An experimental comparison Table 9: Pairwise comparisons between charts for response times for the health professionals group, arranged in order of effect size. Comparison Observed p < 0.001 Critical p for significance at 5% level 0.003 Comparison significant at 5% level? Significant No track and trigger numerical chart vs. ADDS without SBP table No track and trigger numerical chart vs. ADDS with SBP table Multiple parameter track and trigger chart vs. ADDS with SBP table No track and trigger graphical chart vs. ADDS without SBP table Multiple parameter track and trigger chart vs. ADDS without SBP table No track and trigger graphical chart vs. ADDS with SBP table No track and trigger numerical chart vs. Single parameter track and trigger chart Single parameter track and trigger chart vs. ADDS without SBP table No track and trigger numerical chart vs. Multiple parameter track and trigger chart No track and trigger numerical chart vs. No track and trigger graphical chart Single parameter track and trigger chart vs. ADDS with SBP table No track and trigger graphical chart vs. Single parameter track and trigger chart Single parameter track and trigger chart vs. Multiple parameter track and trigger chart No track and trigger graphical chart vs. Multiple parameter track and trigger chart ADDS without SBP table vs. ADDS with SBP table < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.004 Significant < 0.001 0.005 Significant < 0.001 0.005 Significant < 0.001 0.006 Significant < 0.001 0.006 Significant < 0.001 0.007 Significant < 0.001 0.008 Significant 0.001 0.010 Significant 0.003 0.013 Significant 0.034 0.017 0.244 0.025 0.477 0.050 Not significant Not significant Not significant Note. SBP = systolic blood pressure. Overall, health professionals were significantly faster than novices at reaching a decision, F(1,87) = 8.69, p = 0.004. This difference was significant for the two no track and trigger charts but not the coloured charts when a Bonferroni-Holm correction for multiple comparisons was applied (see Table 10). 21 Detecting abnormal vital signs on six observation charts: An experimental comparison Table 10: Comparisons between novices and health professionals in response times for the six charts, arranged in order of effect size. Chart (novice vs. professional comparison) Observed p Critical p for Comparison significance significant at at 5% level 5% level? No track and trigger graphical chart 0.001 0.008 Significant No track and trigger numerical chart 0.007 0.01 Significant Single parameter track and trigger chart 0.030 0.0125 Not significant Multiple parameter track and trigger chart 0.032 0.017 Not significant ADDS chart with SBP table 0.037 0.025 Not significant ADDS chart without SBP table 0.229 0.050 Not significant Note. SBP = systolic blood pressure. There was no overall significant difference between the response times of doctors and nurses across all charts, F(1,43) = 0.05, p = 0.824, nor for any chart individually (see Table 11). Table 11: Comparisons between doctors and nurses for response times across the six charts, arranged in order of effect size. Chart (doctor vs. nurse comparison) Observed p Critical p for Comparison significance significant at at 5% level 5% level? ADDS chart with SBP table 0.951 0.008 Not significant ADDS chart without SBP table 0.516 0.010 Not significant Single parameter track and trigger chart 0.556 0.013 Not significant Multiple parameter track and trigger chart 0.688 0.017 Not significant No track and trigger graphical chart 0.272 0.025 Not significant No track and trigger numerical chart 0.488 0.050 Not significant Note. SBP = systolic blood pressure. 4. Discussion Improving the recognition and management of patients who deteriorate whilst in hospital is a frequently cited priority for improving patient safety (1, 2). One way to improve the recognition and management of deteriorating patients is to improve the design of paper-based adult observation charts (where patient management can be potentially influenced if action plans are included on a chart). The aim of the current study was to compare the ability of six observation charts to signal patient deterioration. De-identified patient data was presented on two versions of the new ADDS chart (designed to conform to human factors principles), two existing charts rated as “well designed”, one existing chart rated as being of “average design”, and one existing chart rated as “poorly designed”. Chart novices and health professionals were recruited as participants. Participants had to classify the 22 Detecting abnormal vital signs on six observation charts: An experimental comparison physiological data on the charts as “normal” or “abnormal”. Error rates and response times were the main outcomes of interest. It was hypothesized that the charts that were rated as being better designed would yield fewer incorrect responses. It was also hypothesized that participants would be faster to reach their decision for the better designed charts. Finally, we hypothesized that the new ADDS chart would perform at least on the same level as the charts rated as “well designed”, if not better. The results can be summarized as follows: 1. There were significant differences in both error rate and response time between the charts, indicating that chart design influences both of these performance measures. This is the first study to investigate both of these effects in novices and health professionals (a previous study by Chatterjee and colleagues (14) only investigated the effect of chart design on error rates among non-novice health professionals). 2. Error rates for both the novice and health professional groups were substantial, reaching 32.6% for one chart (the no track and trigger numerical chart, both groups combined), where 50% errors indicates chance performance. This is despite participants making their judgements under test conditions without distractions, when they were aware that they were under scrutiny. Even the best performing chart (the ADDS chart with systolic blood pressure table) yielded an error rate of 9.8%. It is possible that under real world conditions (where individuals are faced with external pressures, distractions, and a lack of scrutiny) error rates for some or all of the charts could be higher. 3. For the novice group, the error rates on the charts were grouped as follows: both versions of the ADDS chart had similar error rates to one another but yielded fewer errors than both existing coloured charts (the single parameter track and trigger chart and the multiple parameter track and trigger chart), which did not differ from one another. All of the coloured charts with track and trigger systems were superior to the no track and trigger charts, which did not differ from one another. This ordering is largely consistent with the conclusions of the heuristic analysis from Phase 1 of this project, which predicted that charts considered to be better designed would yield fewer errors (16). For the health professional group, the error rates on the charts indicated that the ADDS charts were superior to all four existing charts, which did not differ from one another. 4. The response time data yielded more pronounced differences between the charts, with approximately the same rank ordering of best to worse. For novices, there were significant differences in response time between all the charts except the two existing coloured charts (the single parameter track and trigger chart and the multiple parameter track and trigger chart). The ADDS chart without the systolic blood pressure table yielded the fastest decisions, followed by the ADDS chart with the systolic blood pressure table, and the existing coloured charts. The no track and trigger charts took the longest to interpret, with the no track and trigger numerical chart being the slowest, consistent with predictions from the heuristic analysis. For the health professionals, the rank ordering of charts by response time was the same as for novices, although there was no significant difference between the two versions of the ADDS chart, between the two existing 23 Detecting abnormal vital signs on six observation charts: An experimental comparison coloured charts, or between the no track and trigger graphical chart and the multiple parameter track and trigger chart. 5. There was no evidence for any difference between the novices and the health professionals in their ability to detect unstable vital signs, with both groups yielding the same, high error rates. However, the health professionals were significantly faster at reaching their decisions when confronted with the no track and trigger charts than were the novices. This suggests that the health professionals had a speed advantage when the charts did not incorporate any track and trigger systems (and participants were instead relying on the memorised cut-offs). It also potentially indicates the presence of a speed-accuracy trade-off, where it is possible that the health professionals might have been able to obtain lower error rates than the novices for the no track and trigger charts if they had taken the same amount of time over their decisions. However a further experiment (where viewing times are standardised) would be required to test this hypothesis. 6. There was no difference between doctors and nurses in either their ability to detect unstable vital signs or their speed of reaching a decision. Overall, the outcomes of this study indicate that the design of patient observation charts has dramatic effects on both the ability of individuals to detect abnormal vital signs as well as the time taken to make those judgements. Given that the detection of abnormal vital signs is critical to patient safety, we are in the position of being able to make the strong assertion that the way that observation charts are designed is likely to have a substantial impact on patient safety. For example, the error rate for the worst performing chart was 3.31 times the error rate of the best performing chart. The results are broadly consistent with the results of the heuristic analysis in that the four existing charts in the study emerged in more or less the rank order predicted. While it is not possible to provide definitive statements about each of the design principles highlighted in the heuristic analysis because the charts vary on more than one dimension, there are a number of indicative findings that could be followed up in future studies. First, the coloured charts tended to outperform the no track and trigger charts (where the coloured charts all had track and trigger systems incorporated into the vital signs’ graphs while the no track and trigger charts did not). This supports the idea that coloured track and trigger systems are beneficial. Second, the finding that the no track and trigger graphical chart that outperformed the no track and trigger numerical chart in terms of decision time (if not error rate) is consistent with the idea that graphed data is superior to numerical. However, a series of additional experiments, involving charts that differ on one design feature only, would be required to provide more convincing evidence about the utility of each of these design principles. The results also indicated that the ADDS chart outperformed all the existing charts, even those that were considered to be well designed in the heuristic analysis (namely the single parameter track and trigger chart and the multiple parameter track and trigger chart). The single parameter track and trigger chart yielded 2.50 times the error rate of the ADDS chart with the systolic blood pressure table and the multiple parameter track and trigger chart had 2.46 times the error rate of the ADDS chart with the systolic blood pressure table (both groups together). This indicates that, based on the metrics used in the present study, the ADDS chart should be recommended as current best practice 24 Detecting abnormal vital signs on six observation charts: An experimental comparison (bearing in mind that this recommendation may change depending on the results from studies investigating other issues). 25 Detecting abnormal vital signs on six observation charts: An experimental comparison References 1. Australian Commission on Safety and Quality in Health Care. Recognising and responding to clinical deterioration: Background paper: Australian Commission on Safety and Quality in Health Care, Department of Health and Ageing, Commonwealth of Australia2009 Jun. 2. Patient Safety Centre. Recognition and management of the deteriorating patient: Core strategy options paper. Brisbane, Queensland, Australia: Patient Safety Centre, Queensland Health2010. 3. Franklin C, Mathew J. Developing strategies to prevent inhospital cardiac arrest: Analyzing responses of physicians and nurses in the hours before the event. Critical care medicine 1994;22(2):189-91. 4. Buist M, Bernard S, Nguyen TV, Moore G, Anderson J. Association between clinically abnormal observations and subsequent in-hospital mortality: A prospective study. Resuscitation. 2004;62(2):137-41. 5. Hillman KM, Bristow PJ, Chey T, Daffurn K, Jacques T, Norman SL, et al. Antecedents to hospital deaths. Internal Medicine Journal. 2001;31(6):343-8. 6. Goldhill DR, White SA, Sumner A. Physiological values and procedures in the 24 h before ICU admission from the ward. Anaesthesia. 1999;54:529-34. 7. McQuillan P, Pilkington S, Allan A, Taylor B, Short A, Morgan G, et al. Confidential inquiry into quality of care before admission to intensive care. British Medical Journal. 1998;316:1853-8. 8. Kause J, Smith G, Prytherch D, Parr M, Flabouris A, Hillman K. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom-the ACADEMIA study. Resuscitation. 2004;62:275-82. 9. Endacott R, Kidd T, Chaboyer W, Edington J. Recognition and communication of patient deterioration in a regional hospital: A multi-methods study. Australian Critical Care. 2007;20(3):1005. 10. Lim P. Recognition and management of the deteriorating patient. Technical discussion paper: Patient Safety Centre, Queensland Health, 2009. 11. Bristow PJ, Hillman KM, Chey T, Daffurn K, Jacques TC, Norman SL, et al. Rates of in-hospital deaths and intensive care admissions: the effect of a medical emergency team. Medical Journal of Australia. 2000;173:236-40. 12. Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart GK, Opdam H, et al. A prospective before-and-after trial of a medical emergency team. Medical Journal of Australia. 2003;179(6):283-7. 13. Bellomo R, Goldsmith D, Uchino S, Buckmaster J, Hart G, Opdam H, et al. Prospective controlled trial of medical emergency team on postoperative morbidity and mortality rates. Critical Care Medicine. 2004;32(4):916-21. 14. Van Leuvan CH, Mitchell I. Missed opportunities? An observational study of vital sign measurements. Critical Care & Resuscitation. 2008;10(2):111-5. 15. Chatterjee MT, Moon JC, Murphy R, McCrea D. The "OBS" chart: An evidence based approach to re-design of the patient observation chart in a district general hospital setting. Postgraduate Medical Journal. 2005;81:663-6. 16. Mitchell IA, McKay H, Van Leuvan C, Berry R, McCutcheon C, Avard B, et al. A prospective controlled trial of the effect of a multi-faceted intervention on early recognition and intervention in deteriorating hospital patients. Resuscitation. 2010. 17. Preece M, Horswill M, Hill A, Karamatic R, Hewett D, Watson M. Heuristic Analysis of 25 Australian and New Zealand Adult General Observation Charts. Sydney, New South Wales, Australia: Australian Commission on Safety and Quality in Health Care2009. 18. Preece MHW, Horswill MS, Hill A, Watson MO. The development of the Adult Deterioration Detection System (ADDS) chart. Sydney, New South Wales, Australia: Australian Commission on Safety and Quality in Health Care, 2010. 26 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix A: The ADDS chart with systolic blood pressure table Note: Chart is printed at A3 size double-sided. 27 Detecting abnormal vital signs on six observation charts: An experimental comparison 28 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix B: The ADDS chart without systolic blood pressure table Note: Chart is printed at A3 size double-sided 29 Detecting abnormal vital signs on six observation charts: An experimental comparison 30 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix C: Single parameter track and trigger chart Note: Chart is printed at A3 size double-sided and has been de-identified 31 Detecting abnormal vital signs on six observation charts: An experimental comparison 32 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix D: Multiple parameter track and trigger chart Note: Chart is printed at A4 size double-sided and has been de-identified 33 Detecting abnormal vital signs on six observation charts: An experimental comparison 34 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix E: No track and trigger graphical chart Note: Chart is printed at A3 size double-sided and has been de-identified 35 Detecting abnormal vital signs on six observation charts: An experimental comparison 36 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix F: No track and trigger numerical chart Note: Chart is printed at A4 single sided -sided and has been de-identified. 37 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix G: Questionnaire and Test For Novice Group Questions About Your Background All responses are completely anonymous. Please answer the following questions as honestly and accurately as possible. There are no right or wrong answers. 1. Your sex: Female Male 2. Your age: _____ years 3. Are you colour-blind? Yes No If you answered „Yes‟: 4. What type of colour-blindness do you have? (E.g. “red-green”) _____________________________ 5. Does your colour-blindness impact on your work or studies? Yes No 6. Do you wear glasses or contact lenses in order to read? Yes No 7. Was English your first language? Yes No 8. Did you complete the majority your professional training or schooling in English? Yes No 38 Detecting abnormal vital signs on six observation charts: An experimental comparison 9. Please indicate the description-step that better reflects the psycho-physical state you have experienced in the last ten minutes: = extremely alert = very alert = alert = rather alert = neither alert nor sleepy = some signs of sleepiness = sleepy, no effort to stay awake = sleepy, some effort to stay awake = very sleepy, great effort to keep awake, fighting sleep 10. Have you ever worked as a health professional (e.g. nurse)? Yes No If you answered „Yes‟, please describe your work as a health professional: ________________________________________________________ ________________________________________________________ ________________________________________________________ 11. Have you ever used a Hospital Observation Chart before? Yes No If you answered „Yes‟, please describe your experience with Charts: ________________________________________________________ ________________________________________________________ ________________________________________________________ 39 Detecting abnormal vital signs on six observation charts: An experimental comparison Post-Experiment Questions 1. Have you previously used a chart that was very similar to any of the Observation Charts that were presented in the study? Yes No If you answered „Yes‟, please tell the researcher so that they can show you copies of the Charts, then you can indicate which ones you have previously used. 2. Please indicate the description-step that better reflects the psycho-physical state you have experienced in the last ten minutes: = extremely alert = very alert = alert = rather alert = neither alert nor sleepy = some signs of sleepiness = sleepy, no effort to stay awake = sleepy, some effort to stay awake = very sleepy, great effort to keep awake, fighting sleep 40 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix H: Questionnaire For Health Professional Group Questions About Your Background All responses are completely anonymous. Please answer the following questions as honestly and accurately as possible. There are no right or wrong answers. 1. What is your occupation? Nurse Doctor Other health professional (please specify: _____________________________________ ) 2. Which of the following best describes your nursing role? Enrolled Nurse Nursing Assistant Registered Nurse Clinical Nurse Nurse Unit Manager Clinical Nurse Consultant Nurse Educator Nursing Director Nurse Practitioner Other (please specify: ____________________________________________________ ) 3. Which of the following best describes your medical role? Post-graduate year 1 (Intern) Post-graduate year 2 and not in an accredited training program Post-graduate year 3 and not in an accredited training program Post-graduate year 4+ and not in an accredited training program Post-graduate and in an accredited training program Hospitalist Career Medical Officer Senior Medical Officer Visiting Medical Officer Staff Specialist Senior Staff Specialist Other (please specify: ____________________________________________________ ) 41 Detecting abnormal vital signs on six observation charts: An experimental comparison 4. How many years have you been registered? ______ years 5. What is the postcode of your institution or place of work? _______ 6. At your institution, where do you spend the greatest proportion of your time working? Ward Emergency ICU Theatre Outpatient Clinic Management/administration Other (please specify: ____________________________________________________ ) 7. Your sex: Female Male 8. Your age: ______ years 9. Are you colour-blind? Yes No If you answered „Yes‟: a. What type of colour-blindness do you have? (E.g. “red-green”) _____________________________ b. Does your colour-blindness impact on your work? Yes No 42 Detecting abnormal vital signs on six observation charts: An experimental comparison 10. Do you wear glasses or contact lenses in order to read? Yes No 11. Was English your first language? Yes No 12. Did you complete the majority your professional training (e.g. BNurs, MB BS) in English? Yes No 13. Please indicate the description-step that better reflects the psycho-physical state you have experienced in the last ten minutes: = extremely alert = very alert = alert = rather alert = neither alert nor sleepy = some signs of sleepiness = sleepy, no effort to stay awake = sleepy, some effort to stay awake = very sleepy, great effort to keep awake, fighting sleep 43 Detecting abnormal vital signs on six observation charts: An experimental comparison The next few questions are about your current use of Observation Charts. 14. Do you use Observation Charts as part of your current role? Yes No 15. How frequently do you use Observation Charts? More than once a day Once a day More than once a week, but less than once a day Once a week More than once a month, but less than once a week Once a month Less than once a month 16. Do you record information in Observation Charts as part of your current role? Yes No 17. How frequently do you record information in Observation Charts? More than once a day Once a day More than once a week, but less than once a day Once a week More than once a month, but less than once a week Once a month Less than once a month 18. What training have you received in the use of Observation Charts? (tick all that apply) None Read the instructions Informal (e.g. by co-worker) Formal (e.g. in-service or workshop) Other (please specify: ____________________________________________________ ) 44 Detecting abnormal vital signs on six observation charts: An experimental comparison Post-Experiment Questions 3. Have you previously used a chart that was very similar to any of the Observation Charts that were presented in the study? Yes No If you answered „Yes‟, please tell the researcher so that they can show you copies of the Charts, then you can indicate which ones you have previously used. For researcher: __________________________________________________________ __________________________________________________________ __________________________ 4. Please indicate the description-step that better reflects the psycho-physical state you have experienced in the last ten minutes: = extremely alert = very alert = alert = rather alert = neither alert nor sleepy = some signs of sleepiness = sleepy, no effort to stay awake = sleepy, some effort to stay awake = very sleepy, great effort to keep awake, fighting sleep 45 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix I: Summary sheet of background information Vital Signs Summary Vital sign Normal physiological range Respiratory rate 9 to 20 breaths per minute Oxygen saturation 93% to 100% Oxygen delivery rate 0 to 1 litre of oxygen per minute Systolic blood pressure 110 to 159 mmHg Heart rate 50 to 99 beats per minute Temperature 36.1 to 37.9 °C Consciousness Alert Pain No pain 46 Detecting abnormal vital signs on six observation charts: An experimental comparison Scoring Summary System Definition Cut-off scores Cut-off scores compare a patient’s current observations with a simple set of criteria for the vital signs (the “cutoffs”) Early warning scores Early warning scores allow a patient’s current observations to be weighted and combined into a single total score 47 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix J: Participant Knowledge Test Multiple Choice Questions Please circle the most correct answer for the following questions: 1. For a healthy adult at rest, what is the normal range for their respiratory rate? a. 1 to 8 breaths per minute b. 9 to 20 breaths per minute c. 21 to 32 breaths per minute d. 33 to 40 breaths per minute 2. What is the normal range for oxygen saturation? a. 69 – 76% b. 77 – 84% c. 85 – 92% d. 93 – 100% 3. What is the normal range for oxygen delivery? a. 0 to 1 litre of oxygen per minute b. 1 to 2 litres of oxygen per minute c. 2 to 3 litres of oxygen per minute d. 3 to 4 litres of oxygen per minute 4. For a healthy adult at rest, what is the normal range for their systolic blood pressure? a. 10 to 59 mmHg b. 60 to 109 mmHg c. 110 to 159 mmHg d. 160 to 209 mmHg 5. For a healthy adult at rest, what the normal range for their pulse? a. 50 to 99 beats per minute b. 100 to 149 beats per minute c. 150 to 199 beats per minute d. 200 to 249 beats per minute 48 Detecting abnormal vital signs on six observation charts: An experimental comparison 6. For a healthy adult sitting in a room with a normal temperature, what is the normal range for their body temperature? a. 32.3 to 34.1 °C b. 34.2 to 36.0 °C c. 36.1 to 37.9 °C d. 38.0 to 39.8 °C 7. A healthy adult who is fully conscious is described as being what? a. Alert b. Responsive to voice only c. Responsive to pain only d. Unresponsive 8. A healthy adult at rest should be what amount of pain? a. No pain b. None to some amount of pain c. None to a moderate amount of pain d. None to a considerable amount of pain 9. Which of the following is a definition of Cut-Off Scores? a. Cut-off scores are indicators of a physiological processes that are essential for life b. Cut-off scores compare a patient‟s current observations with a simple set of criteria for the vital signs c. Cut-off scores are a set of criteria for when to stop monitoring a patient‟s vital signs d. Cut-off scores allow a patient‟s current vital signs to be weighted and combined into a single total score 10. Which of the following are features of Early Warning Scores? a. They are calculated to signal early signs that a patient is deteriorating b. They allow a patient‟s current vital signs to be weighted and combined into a single total score c. Early warning scores look at all the vital signs together, not just a single vital sign in isolation d. All of the above 49 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix K: Participant Knowledge Test Answers MCQ Scoring Key 1b 2d 3a 4c 5a 6c 7a 8a 9b 10d 50 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix L: Testing manual for novice group Recognition Study Testing Manual – Students Very Important We only have 1 copy of each of the charts. Make sure the charts are kept in a high, safe place and that water bottles are always placed on the floor. Also, apart from when having to fill in various sheets, make sure the participant does not have a pen when doing the experiment. Preparation Make sure that you are: Ready and able to explain any part of testing to the participant Clear and articulate when giving instructions Aware of building rapport with the participant and setting them at ease, whilst maintaining consistency in test administration and minimising your influence on their responses o It’s fine to chat to the participant before & after testing, but no talking during testing please Before testing, check that you have: The participant number The correct chart scoring sheet Observation charts in the correct order for that participant A Participant Information and Consent Form A questionnaire (with the participant number filled in) Laminated participant cut-off summary MCQ scoring key A Participant Debrief Sheet Payments to Research Participants Form for paid participants $20 for paid participants Computer set up with the Instructions presentation in Media (with correct parameter file for that participant) o Megan will log in each morning o Click Media on the desktop o Click Deterioration Study 3.4 shortcut (looks like filmstrip) on the Desktop o Click Run Experiment 51 Detecting abnormal vital signs on six observation charts: An experimental comparison o The ‘Loading…’ window appears, click ‘Browse’. Under ‘Data’, select the correct participant number and click ‘Open’ o Click ‘Load’ in the ‘Loading…’ window o The ‘Subject identifier’ window appears, enter the participant’s number e.g. “01” o The first screen of the Background Information presentation will appear Pens Stopwatch Voice recorder/mike Turned off your mobile phone (even receiving messages on Silent can distract the participant) Be ready and waiting for the participant at least 10 minutes before the session is scheduled to begin. There will be 2 Research Assistants (RAs) running the sessions, one should be in charge of interacting with the participant (i.e., explaining all instructions, handing them materials) and the other should be in charge of preparing materials and collecting data (i.e., getting forms ready for the other RA, setting up the voice recorder, timing & transcribing the participant’s responses in the experiment). To avoid fatigue, you can alternate between these roles across sessions. Start of the Session When the participant arrives, welcome them (thank them for taking the time to participate) and invite them to come in and sit down at the computer. Introduce yourself and explain the procedure. “My name is ___________ and I am a research assistant for the School of Psychology, thanks for coming today. We are conducting a study to identify which patient observation chart design best assists health professionals in recognising patient deterioration. First, you will fill in a background questionnaire. Second, you will be shown patients’ vital signs displayed on 6 different observation chart designs. This session will take up to 2 hours of your time – give or take. There are no trick questions; you can take every task at face value. All we ask is that you try your best on the tasks.” Give the participant the Participant Information and Consent Form. “The Participant Information and Consent Form explains what the study is about. Your participation is completely voluntary and confidential, and you are free to withdraw at any time. If you are happy with the information on the sheet, sign the bottom of the second page. Please feel free to ask me any questions before we begin.” 52 Detecting abnormal vital signs on six observation charts: An experimental comparison Give the participant the Questions About Your Background sheet. “First, can you fill in this questionnaire?” When they finish the questionnaire, introduce the Background Information presentation on the computer and show them the Participant Cut-off Summary briefly. “Next, I would like you watch a presentation on the computer. It explains important background information for the experiment. It’s about 35 minutes long. You will have to answer 10 multiple choice questions at the end to check that you understand the information. But you will be given this summary sheet at the end to help you remember the important points. Feel free to adjust the volume of the headphones” Get the participant to wear the headphones and let them adjust the volume if they want to. They will tell you when the presentation ends. While they are watching the presentation, one RA should stay in the room (the other RA can take a break if they want, but must be back before the instructions end). After the participant has watched the presentation, prepare them for the Multiple Choice Questions and give them the Participant Cut-off Summary to study, plus a pen and paper. “Soon, I’ll be giving you 10 multiple choice questions to check that you understand the background information. But first, here’s a summary of the information from the videos that you will need to know to pass the test. You can take as long as you like now to study this information, and here’s a pen and paper in case writing will help you memorise it all. When you’re confident that you know everything on this summary sheet, let me know and I’ll give you the test to complete. After you finish the test, I’ll compare your answers with the correct answers. If you get any of the questions wrong, you will have to study the summary sheet again and re-attempt all of the questions, because we can’t start the experiment until you can get 10 out of 10.” When the participant says that they are ready, give them the Multiple Choice Questions. Leave the computer as it is. Once the participant is finished, check how many they answered correctly with the MCQ scoring key, without showing the participant the scoring key. If the participant gets any questions wrong, get them to look at the Cut-off Summary again (and then re-attempt all questions on a blank form). Let the participant know how many they got wrong, but not which questions. Next, introduce the Experiment Instructions presentation on the computer. “Next, I would like you watch a very short presentation on the computer. It explains the instructions for the experiment”. 53 Detecting abnormal vital signs on six observation charts: An experimental comparison Play the video. You re-activate the video by clicking in the top-left of the screen (there’s a “secret button” here). Make sure the participant puts the headphones on again. If something goes wrong in Media, you can play the back-up WMV file on the desktop. Afterwards, ask the participant whether they understood the test instructions. If not, play the test instructions again. The Experiment Make sure the desk is free of water bottles and pens. Explain that we will be recording the experiment in case the scribe RA writes down the wrong answers, the participant won’t be able to be identified and the data is only used for preventing our errors. “Now, I’m going to turn on this mike, this is just to record your responses during the experiment in case the scribe misses something. We’re not using the recording for any other reason”. Make sure the mike is plugged in to the mains, and press the record button twice to activate recording. The red light under the Play/Rec label should be red and not flashing. Explain that for the experiment, 1 RA will give the participant the instructions and the charts, whereas the other RA will be in the room to read out the correct chart number and write down the participant’s answers. Tell the participant that it’s important that they speak in a loud, clear voice throughout the experiment. Tell the participant not to damage the charts as we only have 1 copy of each set of data. Make sure that the participant has a clear tabletop in front of them. When the participant is ready, begin the experiment. The “scribe” RA should read out the trial number then the chart number for the trial and the “instructor” RA should confirm that they have the correct chart before placing it in front of the participant (so that we can hear it on the recording). Place the 1st chart face-down in front of the participant. Instructor RA: “This is the first trial. Ready, set, go!” Begin timing as you say, “Go!” Scribe RA: When the participant says “Normal” or “Abnormal”, stop timing. Write down their answer in correct column of the Chart Scoring Sheet, then write down the time in the next cell MM:SS. If a participant answers “Abnormal” Instructor RA should ask them which vital sign they think is abnormal and the Scribe RA should write down their answer. If they answer this question by pointing, the Instructor RA should say which vital sign the participant is pointing to (like paraphrasing) so that the participant confirms it out loud. Take the finished chart away from the participant as soon as possible. 54 Detecting abnormal vital signs on six observation charts: An experimental comparison Throughout the experiment, always ask the participant to repeat anything that you did not hear properly, whether you are the instructor or the scribe. When you are ready, repeat the cycle. After trials 16 and 32, offer the participant a break. If a participant wants to stop during a trial (even though we’ve asked them not to do this), stop timing them and take back or flip over the observation chart (so that they can’t keep looking at the observations). When the problem is resolved, resume the trial by flipping the chart over again on “Go!” and resume timing. Make a note on the sheet of which trial this happened on and what the problem was. Note what the time (on the stopwatch) was when the interruption occurred. Post-experiment After completing all 48 trials, give the participant the Post-Experiment Questions sheet. If a participant has had previous experience with a chart, note which one(s) and how they are familiar with them. End of the Session Thank the participant for participating and give them a copy of the Participant Debrief Sheet. “Thank you for participating in our study. The research question was whether observation chart design can affect rates of recognising patient deterioration. The research is explained in more detail on the Debrief Sheet. Do you have any questions?” Answer any questions that the participant might have. If the participant is interested in the results, make a note of their email address and Megan will get back to them. Paid participants: Give them $20, and get them to complete and sign the Payments to Research Participants Form. It is very important that paid participants sign this form, or else we cannot be reimbursed for the participant payment. Afterwards After testing, you must: Check that there are enough consent forms, questionnaires, scoring sheets, debrief sheets, and money for the next testing session Enter the data from the questionnaire & experiment into the Excel spreadsheet Back-up the voice recording (Megan’s computer & markhgrp) Back-up the Excel spreadsheet (Megan’s computer & markhgrp) 55 Detecting abnormal vital signs on six observation charts: An experimental comparison Store the consent form & questionnaire Order of testing summary 1. Participant Information and Consent Form 2. Questions About Your Background sheet – pt to fill in 3. Background Information presentation on the computer (need correct pt ID) – pt to watch wearing headphones 4. Participant Cut-off Summary (plus pen & paper) – pt to study 5. Multiple Choice Questions – pt to fill in & get all correct (MCQ scoring key) 6. Experiment Instructions presentation – pt to watch wearing headphones 7. The Experiment a. Make sure the desk is free of water bottles and pens. b. Turn on voice recorder c. Scribe RA needs Chart Scoring sheet with correct pt ID, stopwatch, & pen d. Instructor needs charts in the correct order for that participant 8. Post-Experiment Questions (pt to fill in) 9. Participant Debrief Sheet 10. Pay participant & get pt to sign Payments to Research Participants Form 56 Detecting abnormal vital signs on six observation charts: An experimental comparison Appendix M: Testing manual for health professional group Recognition Study Testing Manual – RBWH Staff Very Important We only have 1 copy of each of the charts. Make sure the charts are kept in a high, safe place and that water bottles are always placed on the floor. Also, apart from when having to fill in various sheets, make sure the participant does not have a pen when doing the experiment. Preparation Make sure that you are: Ready and able to explain any part of testing to the participant Clear and articulate when giving instructions Aware of building rapport with the participant and setting them at ease, whilst maintaining consistency in test administration and minimising your influence on their responses o It’s fine to chat to the participant before & after testing, but no talking during testing please Before testing, check that you have: The participant number The correct chart scoring sheet Observation charts in the correct order for that participant A Participant Information and Consent Form A questionnaire (with the participant number filled in) Laminated participant Cut-off Summary MCQ scoring key A Participant Debrief Sheet Computer set up with the Instructions presentation in Media (with correct parameter file for that participant) o [reference to computer username and login removed] o Click Deterioration Study on the desktop o Click Deterioration Study 3.4 shortcut (looks like filmstrip) in that folder o Click Run Experiment o The ‘Loading…’ window appears, click ‘Browse’. Under ‘Data’, select the correct participant number and click ‘Open’ 57 Detecting abnormal vital signs on six observation charts: An experimental comparison o Click ‘Load’ in the ‘Loading…’ window o The ‘Subject identifier’ window appears, enter the participant’s number e.g. “01” o The first screen of the Background Information presentation will appear Pens Stopwatch Voice recorder/mike Turned off your mobile phone (even receiving messages on Silent can distract the participant) Be ready and waiting for the participant at least 10 minutes before the session is scheduled to begin. There will be 2 Research Assistants (RAs) running the sessions, one should be in charge of interacting with the participant (i.e., explaining all instructions, handing them materials) and the other should be in charge of preparing materials and collecting data (i.e., getting forms ready for the other RA, setting up the voice recorder, timing & transcribing the participant’s responses in the experiment). To avoid fatigue, you can alternate between these roles across sessions. Start of the Session When the participant arrives, welcome them (thank them for taking the time to participate) and invite them to come in and sit down at the computer. Introduce yourself and explain the procedure. “My name is ___________ and I am a research assistant for the School of Psychology, thanks for coming today. We are conducting a study to identify which patient observation chart design best assists health professionals in recognising patient deterioration. First, you will fill in a background questionnaire. Second, you will be shown patients’ vital signs displayed on 6 different observation chart designs. This session will take up to 1 and a half hours of your time – give or take. There are no trick questions; you can take every task at face value. All we ask is that you try your best on the tasks.” Give the participant the Participant Information and Consent Form. “The Participant Information and Consent Form explains what the study is about. Your participation is completely voluntary and confidential, and you are free to withdraw at any time. If you are happy with the information on the sheet, sign the bottom of the second page. Please feel free to ask me any questions before we begin.” Give the participant the Questions About Your Background sheet. “First, can you fill in this questionnaire?” 58 Detecting abnormal vital signs on six observation charts: An experimental comparison When they finish the questionnaire, introduce the Background Information presentation on the computer and show them the Participant Cut-off Summary briefly. “Next, I would like you watch a presentation on the computer. It explains important background information for the experiment. It’s about 25 minutes long. You will have to answer 10 multiple choice questions at the end to check that you understand the information. But you will be given this summary sheet at the end to help you remember the important points. Feel free to adjust the volume of the headphones” Get the participant to wear the headphones and let them adjust the volume if they want to. They will tell you when the presentation ends. While they are watching the presentation, one RA should stay in the room (the other RA can take a break if they want, but must be back before the instructions end). After the participant has watched the presentation, prepare them for the Multiple Choice Questions and give them the Participant Cut-off Summary to study, plus a pen and paper. “Soon, I’ll be giving you 10 multiple choice questions to check that you understand the background information. But first, here’s a summary of the information from the videos that you will need to know to pass the test. You can take as long as you like now to study this information, and here’s a pen and paper in case writing will help you memorise it all. When you’re confident that you know everything on this summary sheet, let me know and I’ll give you the test to complete. After you finish the test, I’ll compare your answers with the correct answers. If you get any of the questions wrong, you will have to study the summary sheet again and re-attempt all of the questions, because we can’t start the experiment until you can get 10 out of 10.” When the participant says that they are ready, give them the Multiple Choice Questions. Leave the computer as it is. Once the participant is finished, check how many they answered correctly with the MCQ scoring key, without showing the participant the scoring key. If the participant gets any questions wrong, get them to look at the Cut-off Summary again (and then re-attempt all questions on a blank form). You can let the participant know how many they got wrong, but not which questions. Next, introduce the Experiment Instructions presentation on the computer. “Next, I would like you watch a very short presentation on the computer. It explains the instructions for the experiment”. Play the video. You re-activate the video by clicking in the top-left of the screen (there’s a “secret button” here). Make sure the participant puts the headphones on again. If something goes wrong in Media, you can play the back-up WMV file on the desktop. 59 Detecting abnormal vital signs on six observation charts: An experimental comparison Afterwards, ask the participant whether they understood the test instructions. If not, play the test instructions again. The Experiment Make sure the desk is free of water bottles and pens. Explain that we will be recording the experiment in case the scribe RA writes down the wrong answers, the participant won’t be able to be identified and the data is only used for preventing our errors. “Now, I’m going to turn on this mike, this is just to record your responses during the experiment in case the scribe misses something. We’re not using the recording for any other reason”. Make sure the mike is plugged in to the mains and there’s a red light for the 2CH recording option, and press the record button twice to activate recording. The red light under the Play/Rec label should be red and not flashing. Explain that for the experiment, 1 RA will give the participant the instructions and the charts, whereas the other RA will be in the room to read out the correct chart number and write down the participant’s answers. Tell the participant that it’s important that they speak in a loud, clear voice throughout the experiment. Tell the participant not to damage the charts as we only have 1 copy of each set of data. Make sure that the participant has a clear tabletop in front of them. When the participant is ready, begin the experiment. The “scribe” RA should read out the trial number then the chart number for the trial and the “instructor” RA should confirm that they have the correct chart before placing it in front of the participant (so that we can hear it on the recording). Place the 1st chart face-down in front of the participant. Instructor RA: “This is the first trial. Ready, set, go!” Begin timing as you say, “Go!” Scribe RA: When the participant says “Normal” or “Abnormal”, stop timing. Write down their answer in correct column of the Chart Scoring Sheet, then write down the time in the next cell SS:MsMs. If a participant answers “Abnormal” Instructor RA should ask them which vital sign they think is abnormal and the Scribe RA should write down their answer. If they answer this question by pointing, the Instructor RA should say which vital sign the participant is pointing to (like paraphrasing) so that the participant confirms it out loud. Take the finished chart away from the participant as soon as possible. 60 Detecting abnormal vital signs on six observation charts: An experimental comparison Throughout the experiment, always ask the participant to repeat anything that you did not hear properly, whether you are the instructor or the scribe. When you are ready, repeat the cycle. After trials 16 and 32, offer the participant a break. If a participant wants to stop during a trial (even though we’ve asked them not to do this), stop timing them and take back or flip over the observation chart (so that they can’t keep looking at the observations). When the problem is resolved, resume the trial by flipping the chart over again on “Go!” and resume timing. Make a note on the sheet of which trial this happened on and what the problem was. Note what the time (on the stopwatch) was when the interruption occurred. Post-experiment After completing all 48 trials, give the participant the Post-Experiment Questions sheet. If a participant has had previous experience with a chart, note which one(s) and how they are familiar with them. Then, give the participant another copy of the Multiple Choice Questions to do 1 more time. They don’t need to repeat it if they get any wrong (checks that they remembered all/most of the ranges for the duration of the experiment). End of the Session Thank the participant for participating and give them a copy of the Participant Debrief Sheet. “Thank you for participating in our study. The research question was whether observation chart design can affect rates of recognising patient deterioration. The research is explained in more detail on the Debrief Sheet. Do you have any questions?” Answer any questions that the participant might have. If the participant is interested in the results, make a note of their email address and Megan will get back to them. Afterwards After testing, you must: Check that there are enough consent forms, questionnaires, scoring sheets, and sheets for the next testing session Enter the data from the questionnaire & experiment into the Excel spreadsheets Back-up the voice recording (testing computer/the external hard drive) 61 Detecting abnormal vital signs on six observation charts: An experimental comparison o Plug mike into USB on computer, on mike: Menu, scroll down to USB, “enter” USB, then Storage, and it should go to USB –PC mode & will be recognised on the computer. o Find FOLDER01 and copy the files across (then rename according to participant no.), note that these files are big and can take awhile if you have several to back up Back-up the Excel spreadsheet (testing computer/Melany’s laptop/external hard drive) Store the consent form & questionnaire Order of testing summary 11. Participant Information and Consent Form 12. Questions About Your Background sheet – pt to fill in 13. Background Information presentation on the computer (need correct pt ID) – pt to watch wearing headphones 14. Participant Cut-off Summary (plus pen & paper) – pt to study 15. Multiple Choice Questions – pt to fill in & get all correct (MCQ scoring key) 16. Experiment Instructions presentation – pt to watch wearing headphones 17. The Experiment a. Make sure the desk is free of water bottles and pens. b. Turn on voice recorder c. Scribe RA needs Chart Scoring sheet with correct pt ID, stopwatch, & pen d. Instructor needs charts in the correct order for that participant 18. Post-Experiment Questions & MCQ again (pt to fill in) 19. Participant Debrief Sheet 20. Pay participant & get pt to sign Payments to Research Participants Form 62
 0
0
advertisement

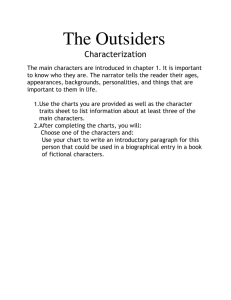
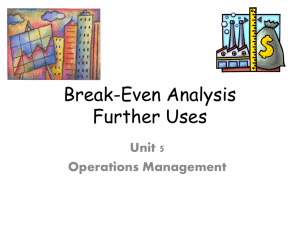
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users