Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April - iPath
advertisement
.April - iPath")
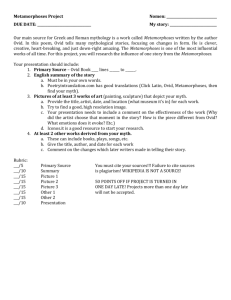
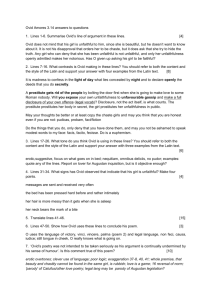
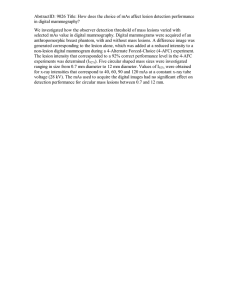
Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi © Lippincott-Raven Publishers Volume 20(4), April 1996, pp 483-491 Clear Cell Dermatofibroma: Case Report of an Unusual Fibrohistiocytic Lesion [Case Report] Zelger, Bernhard W. M.D.; Steiner, Hansjörg M.D.; Kutzner, Heinz M.D. From the Department of Dermatology (B.W.Z.) and Pathology (H.S.), University of Innsbruck, Innsbruck, Austria, and Dermatohistopathological Private Laboratory, Friedrichshafen, Germany (H.K.) Address correspondence and reprint requests to Dr. Bernhard Zelger, Department of Dermatology, University of Innsbruck, Anichstraße 35, A-6020 Innsbruck, Austria. Abstract A case of clear cell dermatofibroma is presented. Clinically, a 41-year-old woman exhibited a hard brown nodule on her instep that was assumed to be a dermatofibroma. Histologically, more than 90% of the lesion was composed of clear cells. Epidermal hyperplasia and a storiform arrangement of spindle cells and sclerotic collagen in some foci at the periphery of the lesion indicated the fibrohistocytic origin. Moreover, prominent vascularity and some bizarre giant cells in the lower part of the lesion were reminiscent of multinucleate cell angiohistiocytoma. Of a broad panel of antibodies, the lesion was positive only for Factor XIIIa (and vimentin). Ultrastructurally, clear-cell changes corresponded to a mostly translucent cytoplasm, focally with some endoplasmic reticulum and prominent lysosomal structures. A review of 1,496 dermatofibromas seen during the last 15 years at our institute revealed 12 cases (1%) with similar clear-cell changes in a minor part of the infiltrate (<10%). The differential diagnosis includes metastases of renal-cell carcinoma, which exhibit more atypia and mitoses and are positive for epithelial cell markers; clear-cell sarcoma, a lesion of tendons or aponeurosis with some moderate cytoplasmic melanin deposition and immunoreactivity with HMB-45; and various non-X histiocytic disorders, such as the predominantly vacuolated type of juvenile (or adult) xanthogranulomas or papular xanthoma, with a mixed infiltrate of various types of mononuclear and multinucleate histiocytes positive with a variety of macrophage markers. Dermatofibroma is a common benign fibrohistiocytic lesion that occurs most commonly on the legs of middle-aged women. Because of the wide array of histologic aspects, various other designations, such as (benign) fibrous histiocytoma, histiocytoma cutis, sclerosing hemangioma, nodular subepidermal fibrosis, or fibrous xanthoma, have been used synonymously. Over the last decade, numerous distinctive clinicopathologic variants have been described: deep penetrating dermatofibroma or dermatofibroma extending into subcutaneous tissue (7); atrophic dermatofibroma hemosiderotic cutaneous (1); (12), (14), dermatofibroma with monster cells epithelioid (16), (15); aneurysmal (“angiomatoid”) and multinucleate cell angiohistiocytoma atypical (“pseudosarcomatous”) (4,10), cellular benign fibrous histiocytoma associated with hyperlipoproteinemia (6). (2), (17); (13), palisading and cholesterotic The present case report describes another variant of fibrohistiocytic tissue response characterized by an abundance of clear cells, which may cause considerable (differential) diagnostic difficulties. 1 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi CASE REPORT A 41-year-old woman consulted her general practitioner for a dermal tumor on the instep of her right leg. The lesion had been present for more than 2 years without a tendency to grow or change. Clinically, it was described as a hard brown tumor of approximately 2-cm diameter assumed to be a dermatofibroma. There was no history of trauma or insect bite before the development of this lesion; her history was otherwise unremarkable. The patient was in good general health. Following excision (with the histologic differential diagnosis of a secondary renal-cell carcinoma), internal examination with routine laboratory parameters including urine analysis, chest radiograph, and abdominal sonography, were normal. The patient remained well with no recurrence during a follow-up of 2 years. MATERIALS AND METHODS Slides and paraffin material were sent to one of us (B.W.Z.) for a second opinion. In addition to hematoxylin and eosin, Perl's prussian blue stain for iron, melanin, van Gieson, periodic acid Schiff's, and trichrome stains were performed on semiadjacent sections (4 µm) of two blocks. Moreover, immunolabelling with a wide variety of markers was done using a standard three-step streptavidin biotin complex technique. Markers included Factor XIIIa, Q BEnd10 (CD34); S100 protein, HMB-45, NK1/C3 (CD57); pankeratin, CAM 5.2, carcinoembryonic antigen, epithelial membrane antigen; HAM56, KP1 (CD68), Ki-M1p (another CD68 epitope), MAC387 (L1-antigen), lysozyme, [alpha]1-antitrypsin; labelling for the adherence of peanut and Ulex europeus agglutinin, Factor VIII-related antigen; vimentin, desmin, myoglobin, smooth muscle actin, HHF-35 (for details of markers, see 19,21). The enzyme product was developed with 3amino-9ethyl carbazole. The sections were finally counterstained with Harris hematoxylin. Well-suited negative and positive controls were included in each staining procedure. Moreover, positive internal controls were present in most specimens. Ultrastructural studies were performed using two blocks of formalin-fixed, paraffin-embedded tissue. Selected tumor parts were punched out of the paraffin block, reembedded in Epon 812, and stained with uranyl acetate/lead citrate in the usual way. Specimens were scanned with a goniometer-equipped Philips EM 400 electron microscope operating at 80 KV. A total of 1,496 dermatofibromas sent to the Dermatohistopathological Laboratory of the Department of Dermatology, University of Innsbruck, Innsbruck, Austria, during the last 15 years (23) were reviewed for clear-cell change. This laboratory is a primary health care laboratory with approximately 10,000 to 15,000 specimens per year. RESULTS Histology Specimens of both blocks (with serial sections) revealed identical findings: At scanning magnification (Fig. 1), the dermis was completely replaced by a faintly stained tumor with a regular, roundish silhouette, which elevated the hyperplastic epidermis above and abutted on the subcutis below the lesion. The demarcation was smooth with a small grenz zone toward the epidermis and a smooth nodular border toward the subcutis with some superficial, scalloped extensions along preexisting septs. No hemorrhage or necrosis was present. Higher magnification (Fig. 2) revealed a moderately dense infiltrate of markedly vacuolated to optically clear cells (>90% of the infiltrate), similar in size to keratinocytes. These oval to polygonal 2 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi cells had well-defined cell borders and round to oval, large (20-25 µm) hypochromatic nuclei with single prominent, eosinophilic nucleolei. Cells were surrounded by fine to sclerotic collagen and reticulin fibers, resulting in a lace-like pattern in particular outlined by special stains such as van Gieson, trichrome (Fig. 3a), and Gomori. No mitoses were seen. Occasional lymphocytes were interspersed between the clear cells. Sclerosis and lymphocytic infiltration or demarcation (Fig. 4) were more prominent at the periphery of the lesion, where many of the vacuolated cells also had a more oval to spindly shape, resulting in a storiform-like pattern. Occasional bizarre giant cells (Fig. 4b and c), similar to those observed in multinucleate cell angiohistiocytoma (17) or dermatofibroma with monster cells (15), were interspersed in the deep parts of the lesion. Epidermal hyperplasia with a moderate increase in basal pigmentation, but no sebaceous, hair follicle, or basal cell carcinoma-like features, was present. The lesion was richly vascularized with numerous partially ectatic capillaries, but showed no pigment deposition. FIG. 1. Silhouette of clear-cell dermatofibroma (composite microphotograph). Note the faint staining of most of the lesion, in contrast to epidermis, adnexal structures, and lower margin. 3 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi FIG. 2. (a-c) Series of close-ups (indicated by arrow in Fig. 1) outlining the marked clear cell change. Cells are surrounded by fine to sclerotic collagen fibers. 4 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi FIG. 3. (a) Trichrome stain outlines a delicate to prominent, lace-like collagen network around clear cells. (b) Immunoreactivity for Factor XIIIa (50% of cells) with sparing in cells of prominent clear cell change. (c) Labeling for CD34 outlining prominent vascularity of the lesion. 5 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi FIG. 4. (a-c) Series of closeups from the lower margin (indicated by arrowhead in Fig. 1) outlining more typical dermatofibroma features such as storiform spindle-cell changes, prominent (peripheral) collagen, and lymphohistiocytic response. Note the bizarre giant cells in higher magnifications. Immunohistochemistry Up to 50% of the infiltrate was positive for Factor XIIIa (Fig. 4b), with more prominent labelling in vacuolated than in clear cells and at the periphery of the lesion. Except for vimentin, the lesion was negative for all other markers, in particular HMB-45 and epithelial and 6 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi macrophage markers, but it revealed prominent vascularity with endothelial cell markers (Fig. 3c). Electron microscopy Clear-cell changes corresponded to a mostly translucent cytoplasm, focally with some endoplasmatic reticulum and prominent lysosomes, giving these cells a granular appearance. The cells had large round to oval euchromatic nuclei with prominent nucleoli and were densely surrounded by collagen fibers. Review of all 1,496 dermatofibromas sent to our Dermatohistopathologic Unit during the last 15 years revealed 12 cases (1%) with similar clear-cell changes (Fig. 5 and 6) in a minor part (10%) of the infiltrate. For clinicopathologic details see 7 of 13 Table 1. 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi FIG. 5. (a) Silhouette of lower parts from a deep penetrating dermatofibroma. Note more faintly stained parts, in particular in upper left corner. (b, c) Higher magnifications (corresponding structures indicated by arrowhead and arrow) reveal focal clear cell change (case 5). 8 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi FIG. 6. (a) Typical example of dermatofibroma. Note more faintly stained areas in lower dermis (indicated by arrows). (b, c) Higher magnifications from right lower margin (corresponding structures indicated by arrowheads) reveal prominent clear cell features (case 8). 9 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi TABLE 1. Clinicopathological data of dermatofibromas with focal clear cell changes (cases 1-12) DISCUSSION Numerous clinicopathologic variants of dermatofibroma are known for their problems in delineation from various other (soft tissue) tumors: (a) deep penetrating dermatofibroma (7,22), which usually occurs on the lower legs of adult women, may mimic dermatofibrosarcoma protuberans; (b) epitheliod histiocytoma (16), which has a clinically similar profile, Spitz nevi; (c) cellular benign fibrous histiocytoma (2), which prefers the upper extremities of men and has a high rate of local recurrence, is often confused with dermatofibrosarcoma protuberans or leiomyosarcoma; (d) atypical (“pseudosarcomatous”) fibrous histiocytoma (4,10) as atypical fibroxanthoma; (e) aneurysmal (angiomatoid) histiocytoma (13), which often presents as a rapidly growing, tender lesion suspected to be of vascular origin; other examples include: (f) hemosiderotic histiocytoma (12), which is clinically often assumed to be a (malignant) melanocytic lesion, or (g) multinucleate cell angiohistiocytoma (17), whose grouped violaceous erythematous papules may mimic Kaposi's sarcoma. The present case expands the spectrum of difficulties in correctly interpreting the variable findings of fibrohistiocytic tissue response: Clear-cell features as described in this case might be confused with metastases of renal-cell carcinoma, clear-cell sarcoma, or various members of the non-X histiocytic family, in particular, early, predominantly vacuolated types of xanthogranuloma and papular xanthoma. This problem may be even greater when the clinical situation is not quite so straightforward, as in our case of a middle-aged woman who presented with a lesion on the lower leg clinically diagnosed as a 10 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi dermatofibroma. In such cases, histology has a decisive input on the benefit and management of the patient. Metastases of renal-cell carcinoma (5) show a less regular growth pattern with necrosis, hemorrhages, cellular atypia, and mitoses; moreover, lesions are usually positive with epithelial markers. Clinically, skin metastases of renal-cell carcinoma before detection of the primary tumor are rare and occur mostly on the head, in particular, the scalp. Clear-cell sarcoma (3), or malignant melanoma of soft parts, is a deeply located tumor of tendon sheath or aponeurosis; an irregular growth of tumor nests and columns is surrounded by a delicate framework of collagen and reticulin bundles. Cytologically, cells are rather monomorphous, polygonal to fusiform with focal eosinophilic granulation. In addition, melanin deposition is frequently seen by Fontana stain, and, interestingly, the lesion is HMB-45 but not S100 protein positive. Clinically, this tumor prefers the lower legs of adult women (20-40 years). Various non-X histiocytic disorders, such as the predominantly vacuolated type of juvenile (or adult) xanthogranulomas (20) or papular xanthoma (18), show a more complex infiltrate of various types of mononuclear (xanthomatized, spindle-shaped, scalloped, oncocytic) and multinucleated (Touton) histiocytes that are positive with a variety of macrophage markers. Clinically, these lesions occur in decreasing frequency on the head, neck, trunk, and extremities. When multiple and within the first 2 years of life, they are easily recognized; yet solitary lesions in adults may cause greater diagnostic difficulties. Various other xanthomas (eruptive, tuberous, or xanthelasma) (9) are characterized by a predominance of xanthomatized cells as well as (occasional) Touton cells; xanthomas are clinically distinctive lesions, mostly multiple disseminated with a yellowish color and associated increase of plasma lipid levels. Finally, balloon cell nevi (11) are rarely intradermal only or without remnants of more typical nevus cells; moreover, this lesion is always S100 protein positive. The clear cells in clear-cell dermatofibroma should not be confused with foamy histiocytes (“fibrous xanthoma”). The latter show no optically clear cells but do show prominent xanthomatization, which is not present in clear-cell dermatofibroma. A review of the literature and our own experience suggest that clear-cell dermatofibromas must be quite rare. To the best of our knowledge, no comparable case has been reported. Only recently, a similar case occurring on the shoulder of a 42-year-old man was presented in a poster at the American Society of Dermatology in New Orleans, February 1-3, 1995 (8). Our own studies revealed no similar case in nearly 1,500 dermatofibromas seen during the last 15 years. Yet clear-cell change was found in 12 cases (1%) in a minor part of the infiltrate (<10%), documenting that such a feature represents a possible reaction pattern of dermatofibromas. In summary, we describe a case of clear-cell dermatofibroma, an unusual and rare manifestation of fibrohistiocytic tissue response, which might be confused with other clear-cell entities. We hope our observation will (a) make (dermato)pathologists aware of this lesion, which may then lead to a better characterization of this phenomenon, and (b) help to avoid this pitfall of differential diagnoses in clear-cell neoplasms whose misinterpretation, in particular as metastases of renal-cell carcinoma or clear-cell sarcoma, may lead to marked mismanagement of and discomfort for patients. Acknowledgment: We thank Prof. Parwaresch, Department of Pathology, University of Kiel, Germany, for kindly providing us with the macrophage marker Ki-M1p. REFERENCES 1. Beer M, Eckert F, Schmöckel C. The atrophic dermatofibroma. J Am Acad Dermatol 1991;25:1081-2. 11 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi Bibliographic Links [Context Link] 2. Calonje E, Mentzel T, Fletcher CDM. Cellular benign fibrous histiocytoma. Clinicopathologic analysis of 74 cases of a distinctive variant of cutaneous fibrous histiocytoma with frequent recurrence. Am J Surg Pathol 1994;18:668-76. [Context Link] 3. Enzinger FM, Weiss SW. Clear cell sarcoma. In: Enzinger FM, Weiss SW, eds. Soft tissue tumours. St. Louis: CV Mosby, 1994:913-9. [Context Link] 4. Fukamizu H, Oku T, Inoue K, Matsumoto K, Okayama H, Tagami H. Atypical (“pseudosarcomatous”) cutaneous histiocytoma. J Cutan Pathol 1983;10:327-33. Bibliographic Links [Context Link] 5. Healey PM, Malott K, Chalet MD. Cancers metastatic to the skin. In: Friedman RJ, Rigel DS, Kopf AW, et al., eds. Cancer of the skin. Philadelphia: WB Saunders, 1991;347-63. [Context Link] 6. Hunt SJ, Santa Cruz DJ, Miller CW. Cholesterotic fibrous histiocytoma: its association with hyperlipoproteinemia. Arch Dermatol 1990;126:506-8. [Context Link] 7. Kamino H, Jacobson M. Dermatofibroma extending into the subcutaneous tissue. Am J Surg Pathol 1990;14:1156-64. [Context Link] 8. Lee M, Ma CK, ohorodnik JM. Clear cell histiocytoma (dendrocytoma [Abstract]. J Cutan Pathol 1995;22:70. [Context Link] 9. Lever WF, Schaumburg Lever G. Lipidoses, histiocytoses. In: Lever WF, Schaumburg Lever G, eds. Histopathology of the skin. Philadelphia: JB Lippincott, 1990:426-31. [Context Link] 10. Leyva WH, Santa Cruz DJ. Atypical cutaneous fibrous histiocytoma. Am J Dermatopathol 1986;8:467-71. Bibliographic Links [Context Link] 11. Maize J, Ackerman AB. Balloon-cell nevus. In: Maize J, Ackerman AB, eds. Pigmented lesions of the skin. Philadelphia: Lea & Febinger, 1987:114-5. [Context Link] 12. Sanchez RL. The elusive dermatofibromas. Arch Dermatol 1990;126:522-3. Bibliographic Links [Context Link] 13. Santa Cruz DJ, Kyriakos M. Aneurysmal (“angiomatoid”) fibrous histiocytoma of the skin. Cancer 1981;47:2053-61. Bibliographic Links [Context Link] 14. Schwob VS, Santa Cruz DJ. Palisading cutaneous fibrous histiocytoma. J Cutan Pathol 1986;13:403-7. Bibliographic Links [Context Link] 15. Tamada S, Ackerman B. Dermatofibroma with monster cells. Am J Dermatopathol 1987;9:380-7. Bibliographic Links [Context Link] 16. Wilson Jones E, Cerio R, Smith NP. Epithelioid cell histiocytoma: a new entity. Br J Dermatol 1989;120:185-95. Bibliographic Links [Context Link] 17. Wilson Jones E, Cerio R, Smith NP. Multinucleate cell angiohistiocytoma: an acquired vascular anomaly to be distinguished from Kaposi's sarcoma. Br J Dermatol 1990;122:651-63. Bibliographic Links [Context Link] 18. Winkelmann RK. Cutaneous syndromes of non-X histiocytosis—a review of the macrophage-histiocyte diseases of the skin. Arch Dermatol 1981;117:667-72. [Context Link] 19. Zelger B, Calonje E, Sepp N, Fink FM, Zelger BG, Schmid KW. Monophasic cellular variant of infantile myofibromatosis (an unusual histopathologic pattern in two siblings.). Am J Dermatopathol 1995;17:131-8. Bibliographic Links [Context Link] 20. Zelger B, Cerio R, Orchard G, Wilson Jones E. Clinicopathological and immunohistochemical study comparing juvenile and adult xanthogranuloma. Am J Surg Pathol 1994;18:126-35. [Context Link] 21. Zelger B, Cerio R, Soyer HP, Misch KJ, Orchard G, Wilson-Jones E. Reticulohistiocytoma and multicentric reticulohistiocytosis (pathological and immunophenotypic distinct entities). Am J Dermatopathol 1994;16:577-84. Bibliographic Links [Context Link] 22. Zelger B, Sidoroff A, Stanzl U, et al. Deep penetrating dermatofibroma versus dermatofibrosarcoma protuberans—a clinicopathologic comparison. Am J Surg Pathol 1994;18:677-86. [Context Link] 23. Zelger BW, Öfner D, Zelger BG. Atrophic variants of dermatofibroma and dermatofibrosarcoma protuberans. Histopathology 1995;26:519-27. Bibliographic Links [Context Link] 12 of 13 3.6.2006 14:00 Uhr Ovid: Zelger: Am J Surg Pathol, Volume 20(4).April 1996.483-491 http://gateway.ut.ovid.com/gw2/ovidweb.cgi Key Words: Dermatopathology; Immunohistochemistry, clear cell; Dermatofibroma; Clear cell neoplasms Accession Number: 00000478-199604000-00013 Copyright (c) 2000-2006 Ovid Technologies, Inc. Version: rel10.2.2, SourceID 1.11354.1.251 13 of 13 3.6.2006 14:00 Uhr