Burns: Clinical features and prognosis
advertisement

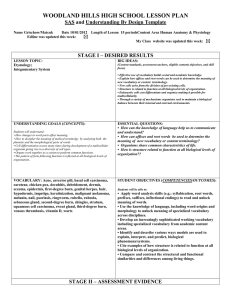
cp, jul_aug, p245-48, cf1.qxp_Layout 1 08/07/2010 11:13 Page 245 Vol 2 July/August 2010 Clinical Pharmacist CLINICAL FOCUS There are many causes of burns. Patients with complex burns should be referred to a specialist burns unit Nils Oskar Johansen | Dreamstime.com Burns clinical features and prognosis By Nicola Rudall, MSc, MRPharmS, and Andy Green, DipClinPharm, MRPharmS E ach year, around 175,000 cases of burns, of varying severity and cause, present for treatment at UK accident and emergency departments.1 Severe burns can be fatal, with 378 deaths from exposure to smoke, fire or contact with heat or hot substances reported in England and Wales in 2008.2 Patients who survive are likely to stay in hospital for lengthy periods. Types of burn There are several causes of burns, ranging from direct heat (including flames and hot liquids) to chemical or electrical injury.3 Presentations differ depending on the cause, and severity is dependent on both contact time and the temperature to which the skin has been exposed. Flame burns account for approximately 50% of adult cases, whereas in children scalding predominates, accounting for 70% of injuries.4 Flame burns can be associated with other injuries, including airway trauma. Electrical burns may present with an entry and exit point where the current has passed through the body. Internal damage, following the path of electricity, can occur along with the external burns. Cardiac involvement, particularly arrhythmias, may be present; damage is voltage-dependent. Chemical burns can be caused either by household products or, more usually, by an industrial accident; wet cement is a common cause. With the exception of hydrofluoric acid, alkaline substances generally cause more damage than acids, although pain is often minimal in the initial stages. Alkali damage is due to saponification of fat, creating further heat and damage. Other causes of burns or burn-like injuries include direct contact thermal burns (from radiators, motorbike ❝ SEVERE BURNS CAN BE FATAL, WITH 378 DEATHS FROM EXPOSURE TO SMOKE, FIRE OR CONTACT WITH HEAT OR HOT SUBSTANCES REPORTED IN ENGLAND AND WALES IN 2008 ❞ exhausts, etc) friction burns and prolonged exposure to ultraviolet radiation (eg, sunburn). Clinical features Burn injuries can be divided into primary and secondary injuries, with the former being the immediate damage caused by the burn and the latter the morbidity resulting from the initial injury.5 Large burns present with local as well as systemic symptoms.4–6 Locally, there may be redness, blistering, swelling and pain or altered sensation. Systemic effects such as hypovolaemic shock, hypothermia, deranged blood test results and metabolic changes may occur as discussed below. Compartment syndrome (see below) can be a problem depending on the burn site. Hypovolaemic shock may be seen in patients with burns greater than 25% of body surface area (BSA) and is caused by increased vascular permeability that continues for at least the first 36 hours following the burn. Proteins, including albumin, leak out into the interstitial space pulling fluid with them leading to oedema and dehydration. Additionally, the body loses fluid via the burn area, which compounds dehydration. To compensate, the peripheral and splanchnic vessels vasoconstrict and this can lead to hypoperfusion. In the initial phase, cardiac output also decreases because of reduced myocardial contractility, increased afterload and reduced plasma volume. Tumour necrosis factor-α, released as part of the inflammatory response, appears to play a role in the SUMMARY Burns are sustained by approximately 175,000 people in the UK each year and vary widely in severity and cause. The presentation depends of the cause of the burn (eg, from heat, chemicals, electricity or other miscellaneous causes such as friction) and the severity of the burn (which depends on percentage of body surface area burnt and thickness of the burn). Sequelae of large burns include hypovolaemic shock, hypothermia, deranged blood test results, metabolic abnormalities and compartment syndrome. 245 Nicola Rudall is senior lead clinical pharmacist for perioperative and critical care and Andy Green is senior lead clinical pharmacist for surgical services, both at Newcastle upon Tyne Hospitals NHS Foundation Trust. E: nicola.rudall@nuth.nhs.uk cp, jul_aug, p245-48, cf1_Layout 1 08/07/2010 11:27 Page 246 Clinical Pharmacist July/August 2010 Vol 2 reduction of myocardial contractility. Early fluid resuscitation is essential to minimise the effects of shock. Initially, core body temperature is substantially reduced with large burns. This is a result of heat loss from the burn (caused by high skin temperatures around the area of the burn leading to evaporation of fluids) and hypovolaemic shock. Because of this, patients should be kept in a warm, humid room. Blood test results are often deranged, with high potassium (caused by damage to cells), low calcium (caused by hypoalbuminaemia), and abnormal clotting (resulting from disseminated intravascular coagulopathy). About 48 hours after the burn injury, a patient with large burns will become hypermetabolic (the metabolic rate can increase up to threefold). The patient’s cardiac output, and therefore organ perfusion, will increase. The baseline temperature will increase to 38.5C as part of the systemic inflammatory response associated with burns.6 Compartment syndrome is characterised by muscle and tissue damage and reduced blood flow, caused by the compression of nerves and blood vessels in an enclosed space (eg, as a result of swelling). For patients with burns, compartment syndrome, particularly in the abdomen, can lead to renal impairment, gut ischaemia and cardiac and pulmonary complications. In the extremities, compartment syndrome can cause pain, reduced capillary refill and paraesthesia. The patient’s immune response is reduced because of receptor downregulation, increasing the risk of infection (which may already be high due to damage to the body’s natural shield, the skin). Inhalational injuries may accompany flame burns, creating problems such as bronchoconstriction or adult respiratory distress syndrome. Patients with inhalational injuries may present with wheezing, hoarseness, increased respiratory secretions, tachypnoea, stridor and hypoxaemia. Carboxyhaemoglobin should be checked to assess the degree of carbon monoxide exposure and patients should receive 100% oxygen. Airway tissues may become inflamed leading to obstruction, so a secure airway is vital. Full-thickness burn Epidermis Dermis Subcutaneous tissue Nucleus Medical Art, Visuals Unlimited | SPL CLINICAL FOCUS 246 Muscle Figure 1: Illustration of a full-thickness burn endings growing back into healing tissue can cause altered sensations and neuropathic pain. It is estimated that 52% of burn survivors suffer from long-term or chronic pain.7 Assessment There are two common methods used to assess the extent of a patient’s burns: Wallace’s “rule of nines” and the Lund and Browder chart (see Figure 2).1,3,5 The rule of nines splits the body into 12 sections: 11 of the areas are each allocated 9% and the groin region is given 1%. The percentage of the BSA that has been burnt can then be estimated. The Lund and Browder chart is the more accurate of the two methods because it takes into account the change in body proportion relating to age (eg, children have relatively larger heads than adults). Erythematous regions should not be included in BSA estimations.5 Burn depths can be classified by degree. They can also be described as superficial, partial thickness or full Figure 2: Lund and Browder chart Percentage of total body surface area burnt PERCENTAGE Pain Burn-associated pain comes from a variety of Region sources including the burn itself, surrounding tissue, dressing changes and donor graft sites. Following a burn, the inflammatory response leads to the release of mediators, such as bradykinin and histamine, which trigger pain signals.7 A full-thickness burn (Figure 1) may damage the nerve to the extent where the pain signal cannot be felt. However, the surrounding tissue may not have been burnt to the same depth, meaning that pain is still present. Primary hyperalgesia is the heightened response to pain at the burn site. Secondary hyperalgesia develops minutes later and is caused by nerve transmission from the surrounding undamaged skin. Hyperalgesia may last for days. Pain alters during the treatment period but tends to be worst at donor sites or areas of upper- or mid-dermal skin loss. Once the burn site is covered with either a graft or appropriate dressing the pain usually reduces. Donor site pain may persist for 10–14 days after harvesting. Five to six weeks post-burn, nerve regeneration occurs, and nerve Head PT FT Neck Anterior trunk Posterior trunk Right arm Left arm Buttocks Genitalia Right leg Left leg PT = partial thickness FT = full thickness Relative percentage of areas dependent on growth Age (years) 0 1 5 10 15 Adult A = 1/2 of head 9 1/2 8 1/2 6 1/2 5 1/2 4 1/2 3 1/2 B = 1/2 of one thigh 2 3/4 3 1/4 4 4 1/4 4 1/2 4 3/4 C = 1/2 of one lower leg 2 1/2 2 1/2 2 3/4 3 3 1/4 3 1/2 cp, jul_aug, p245-48, cf1.qxp_Layout 1 08/07/2010 11:14 Page 248 CLINICAL FOCUS 248 Clinical Pharmacist July/August 2010 Vol 2 Box 1: Burn damage according to depth1,3,5 DEPTH DEGREE EXTENT OF DAMAGE APPEARANCE HEALING TIME Superficial First Epidermis Pink, moist, bleeding, painful Pink, blistering, moist, bleeding, painful Patchy red and white, dry, no bleeding, reduced sensation White/black, dry and leathery, no bleeding, lack of sensation Days Partial thickness: Second superficial Epidermis to papillary dermis Partial thickness: Second deep dermal Epidermis to reticular dermis Full thickness Third Whole thickness of skin Fourth Skin plus tendons, tissue, muscle and bone Figure 3: Jackson’s burn model Zone of hyperaemia Zone of stasis Epidermis One to two weeks Zone of coagulation Dermis > Four weeks Subcutaneous tissue > Four weeks disadvantage of LDI is that it is expensive and requires a high level of expertise to interpret the results (so is not routinely available in many centres that treat burns). Admission criteria thickness (see Box 1).1,3,5 First-degree burns are classed as superficial. Second-degree, partial-thickness burns are subdivided into superficial and deep dermal. Thirddegree burns are full-thickness. Fourth-degree burns, also full-thickness, can occur and these affect the tendons, subcutaneous tissue or bones as well as the skin. It is possible for there to be a mixture of burn depths in one patient, although reassessment should be made in the first few days after the burn since depth may increase depending on the treatment received. Patients with first-degree or second-degree superficial burns usually respond well to treatment and heal within two weeks; these types of burns are typically pink or red, painful and have a good blood supply. Patients with deep dermal or full-thickness burns can take months to recover and have significant scarring without surgical treatment and skin grafting. These types of burns tend to have a poor blood supply so will appear less red. Jackson’s burn model splits the burn into three distinct zones: the zone of coagulation, the zone of stasis and the zone of hyperaemia (see Figure 3).4,5 The zone of coagulation is at the centre of the burn and is an area of severe damage resulting in irreversible tissue loss. Although the zone of stasis contains less damaged tissue, perfusion is affected and the correct treatment must be provided to prevent progression to necrosis and allow full recovery. The zone of hyperaemia contains tissue that is well perfused and this usually recovers well. Assessment techniques In the first few days after injury it is often difficult to determine the depth of a burn and, thus, the prognosis and need for surgery to aid recovery. Various methods have been employed to supplement visual inspection of the burn.1,8,9 Techniques that assess tissue perfusion in the injured area give a more objective assessment of prognosis. Increasingly, a technique called laser Doppler imaging (LDI) is being used and appears to give the most accurate measurement of burn depth among the available techniques. Depth is assessed by taking a thermal image of the burn area which correlates with skin blood flow. The To ensure that treatment is appropriate, the British Burn Association has published criteria for complex burn injury. (see Box 2).1 Patients meeting these criteria should be referred to a specialist unit within six hours of injury since swift assessment and treatment of burns is crucial to optimise patient outcomes. The very young and the elderly are particularly at risk of complex burn injuries. References 1 Enoch S, Roshan A, Shah M. Emergency and early management of burns and scalds. BMJ 2009;338:937–41. 2 Mortality Statistics: Deaths registered in 2008. Office of National Statistics.www.statistics.gov.uk/downloads/theme_health/DR2008/ DR_08.pdf (accessed 18 June 2010). 3 Benson A, Dickson WA, Boyce DE. ABC of wound healing: Burns. BMJ 2006;332:649–52. 4 Hettiaratchy S, Dziewulski P. ABC of burns: Pathophysiology and types of burns. BMJ 2004;328:1427–9. 5 Duncan RT, Dunn KW. Immediate management of burns. Surgery 2006;24:9–14. 6 Latenser BA. Critical care of the burn patient: The first 48 hours. Critical Care Medicine 2009;37:2819–26. 7 Richardson P, Mustard L. The management of pain in the burns unit. Burns 2009;35:921–36. 8 Shelley OP, Dziewulski P. Late management of burns. Surgery 2006;24:15–7. 9 Orgill DP. Excision and skin grafting of thermal burns. New England Journal of Medicine 2009;360:893. Box 2: Specialist burns unit admission criteria All patients with complex burns should be referred to a specialist burns unit. A burn injury is more likely to be complex if associated with the following: ● Inhalational injury ● Deep burn ● High tension electrical ● ● ● ● ● Circumferential burns High pressure steam burn Chemical burn >5% BSA burn Suspicion of non-accidental burn ● Hydrofluoric acid burn Dermal or full-thickness burns >10% >1% BSA of BSA (>5% if over 16 years old) ● Existing medical conditions ● Dermal or full-thickness burns to (eg, pregnancy, cirrhosis or face, hands, perineum, feet or immunosuppression) flexures ● Other injury or major ● Age under five or over 60 years old trauma (eg, crush injuries) ● Exposure to ionising radiation BSA = body surface area