Supraventricular Tachycardia: Diagnosis and Management
advertisement

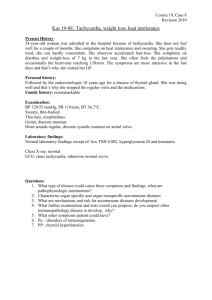
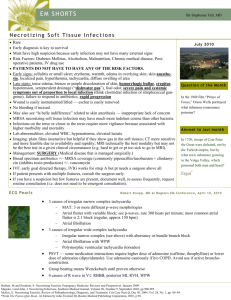
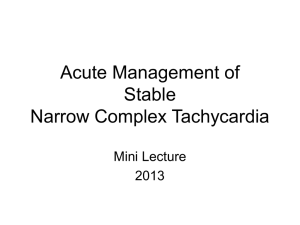
SYMPOSIUM CARDIOVASCULAR DISEASES SUPRAVENTRICULAR ON TACHYCARDIA: DIAGNOSIS AND MANAGEMENT Supraventricular Tachycardia: Diagnosis and Management DAVID J. FOX, BMSC, MBCHB, MRCP; ALEXANDER TISCHENKO, MD, FRCPC; ANDREW D. KRAHN, MD, FRCPC; ALLAN C. SKANES, MD, FRCPC; LORNE J. GULA, MSC, MD, FRCPC; RAYMOND K. YEE, MD, FRCPC; AND GEORGE J. KLEIN, MD, FRCPC Supraventricular tachycardia (SVT) includes all forms of tachycardia that either arise above the bifurcation of the bundle of His or that have mechanisms dependent on the bundle of His. We conducted a review of the techniques used to differentiate the mechanisms of SVT. We searched the PubMed and MEDLINE databases for English-language literature published from 1970 to 2008. Articles were selected for either their historical importance or up-todate clinical data. This review focuses on techniques for scrutinizing electrocardiograms of patients, analyzing in particular the onset of tachycardia, the mode of tachycardia termination, and the effects of premature ventricular contractions, premature atrial contractions, and aberrancy during tachycardia. Both short-term and long-term management of SVT are examined, including the urgent treatment of patients in the emergency department. This review also describes management of patients who have ongoing symptomatic SVT, outlining such available treatment options as atrioventricular node–blocking drugs, antiarrhythmic drugs, and catheter ablation. Mayo Clin Proc. 2008;83(12):1400-1411 AV = atrioventricular; AVNRT = AV nodal reentrant tachycardia; AVRT = AV reentrant tachycardia; BBB = bundle branch block; ECG = electrocardiography; JET = junctional ectopic tachycardia; PAC = premature atrial complex; PJRT = permanent junctional reciprocating tachycardia; PSVT = paroxysmal supraventricular tachycardia; SVT = supraventricular tachycardia S upraventricular tachycardia (SVT), by definition, includes all forms of tachycardia that either arise above the bifurcation of the bundle of His or that have mechanisms dependent on the bundle of His. In patients with SVT, the heart rate is at least 100 beats/min, but ventricular rates can be lower as a result of atrioventricular (AV) block. On electrocardiography (ECG), QRS morphology is usually normal or supraventricular; however, it may be widened or abnormal because of intrinsic conduction disturbance, myocardial disease, or rate-related bundle branch block (BBB). INCIDENCE OF SVT The incidence of SVT in the general population remains unclear. Published incidence data from studies vary widely depending on the characteristics of the enrolled patients, the diagnostic modality used to identify SVT, and specific definitions incorporated into the studies. In a short-term ambulatory monitoring study of 301 men with a mean age of 56 years, the documented occurrence of any form of SVT was 76%.1 The study’s population had an 1400 Mayo Clin Proc. • incidence of coronary artery disease of approximately 20%. By contrast, Clarke et al2 analyzed the SVT rate in a normal disease-free population with an age range of 16 to 65 years, reporting a rate of documented SVT of only 12%. Harrison et al3 also reported a low SVT incidence rate of only 18%. Research has shown that the incidence of SVT, in particular the most common forms (ie, atrial arrhythmias), increases with age and presence of cardiac disease.4,5 However, SVT incidence is difficult to quantify precisely because of the high rate of asymptomatic episodes in patients. Although SVT includes such arrhythmias as atrial fibrillation and atrial flutter, the current review focuses on diagnosis, patient treatment, and management for the 3 most commonly encountered forms of paroxysmal (ie, suddenonset) SVT (PSVT). These forms are AV nodal reentrant tachycardia (AVNRT), AV reentrant tachycardia (AVRT), and atrial tachycardia. METHODS We searched the PubMed and MEDLINE databases for English-language literature published from 1970 to 2008. Articles were selected for either their historical importance or up-to-date clinical data, particularly in regard to techniques for scrutinizing ECG results of patients with PSVT. CLINICAL PRESENTATION OF PSVT Most patients with PSVT present clinically with episodes of palpitations that are of sudden onset and, in some cases, also abrupt offset. The duration of palpitations is highly variable among individuals, with episodes that may last from a few seconds to several hours. Patients usually cannot identify a precipitating trigger that provokes their sudden tachycardia. From the University of Western Ontario, Division of Cardiology, Arrhythmia Section, University Hospital, London, Ontario, Canada. Dr Fox is now with the Wythenshawe Hospital, Manchester, United Kingdom. Address correspondence to David J. Fox, BMSc, MBChB, MRCP, North West Regional Cardiac Centre, Wythenshawe Hospital, Manchester M23 9LT, United Kingdom (david.j.fox@talk21.com). Individual reprints of this article and a bound reprint of the entire Symposium on Cardiovascular Diseases will be available for purchase from our Web site www.mayoclinicproceedings.com. © 2008 Mayo Foundation for Medical Education and Research December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT Patients with PSVT may present either to the emergency department or to the physician’s office. In patients who have symptoms of tachycardia but no diagnosis based on ECG results, appropriate steps need to be taken to ensure that the tachycardia is recorded and that a symptom-rhythm correlation exists. Hence, the use of ambulatory monitoring and event recorders may be required. At presentation, PSVT may be associated with presyncope, syncope, chest pain, and abnormal pulsations in the neck.6 Syncope may occur if an episode of PSVT is extremely rapid, resulting in compromise in cardiac output, or it may follow a prolonged pause immediately after spontaneous termination of tachycardia. Syncope may also be related to the triggering of a vasovagal response caused by the tachycardia itself.7 The mechanism of chest pain is unclear. Although chest pain in PSVT is usually unrelated to coronary artery disease, such pain in older patients raises the possibility of myocardial ischemia. By definition, PSVT is paroxysmal, both starting and stopping abruptly. However, it may be prolonged because of the cardiac adrenergic drive that builds up during PSVT as a result of hypotension or anxiety. The build-up of adrenergic drive results in a less perceptible transition to a sinus tachycardia after the PSVT has terminated. An atrial tachycardia or junctional tachycardia may accelerate more gradually and, thus, would be nonparoxysmal. Some patients with PSVT may describe an urge to urinate, possibly as a result of atrionatriuretic peptide release, which produces an intrinsic diuretic effect. In a less common scenario, some patients with SVT may present with chronic cardiac failure and cardiomyopathy. In such cases, patients generally do not experience palpitations during tachycardia and will have excessive heart rates until cardiac decompensation occurs. The tachycardia in these patients likely takes weeks or months to cause heart failure, depending on the patient’s heart rate and on the amount of time that the patient experiences tachycardia episodes. Ventricular dysfunction is usually reversible, even, to some degree, in patients who have not been treated for long-standing tachycardia. The mechanism of SVT is usually AV reentry involving a decremental accessory pathway, atypical AV nodal reentry, or atrial tachycardia.8 All these types of AV reentry are frequently referred to as permanent junctional reciprocating tachycardia (PJRT); strictly speaking, however, this term refers only to atypical AV nodal reentry.9,10 More recently, PJRT has become synonymous with AV reentry involving a slowly conducting decremental accessory pathway.11 The ECG appearance of PJRT is similar to that of SVT, but with the RP interval (the distance from the peak of the QRS to the onset of the next visible P wave during tachyMayo Clin Proc. • cardia) longer than the PR interval (the conduction time after the RP interval). During tachycardia, if the distance from the R wave to the next P wave is longer than the distance from that same P wave to the next R wave, the condition is termed long RP tachycardia. If the distance from the R wave to the next P wave is shorter than the distance from that same P wave to the next R wave, the condition is termed short RP tachycardia. CLASSIFICATION AND MECHANISMS OF PSVT Paroxysmal SVT can be classified in several ways. The classifications may be based on ECG appearance (ie, long RP tachycardia or short RP tachycardia) or on the underlying mechanism of tachycardia (ie, AV reentry, AV nodal reentry, or atrial tachycardia). It is also clinically useful to consider PSVT classifications in terms of whether the condition is dependent on AV nodal conduction. This type of consideration is useful because it generally allows the arrhythmia to be classified clinically without the need for specialized arrhythmia studies. Supraventricular tachycardia that persists even when AV block is achieved by carotid sinus massage or other interventions is clearly independent of AV nodal conduction. The use of adenosine may terminate some focal atrial tachycardias, but some degree of AV block usually precedes this termination, allowing the diagnosis of AV nodal independence. By contrast, if an intervention that causes AV block terminates the tachycardia, the SVT is clearly AV node–dependent. Atrioventricular nodal dependence is more commonly encountered in the clinical setting than is AV nodal independence. AV NODE–DEPENDENT ARRHYTHMIAS The two most common forms of PSVT (ie, AVNRT and AVRT) are both dependent on AV nodal conduction to maintain the tachycardia circuit. Any interruption of AV nodal conduction will normally terminate tachycardia. These 2 arrhythmias are, of course, reentrant. In the case of AVNRT, the reentrant circuit is small (ie, microreentrant) and is in or closely related to the AV node. In the case of AVRT, the reentrant circuit is large (ie, macroreentrant) and involves the atria, AV node, and ventricles. A much less common form of AV node–dependent arrhythmia is junctional ectopic tachycardia (JET).12,13 This arrhythmia is most common in childhood and may be associated with congenital heart disease. It may also be seen in the early phase after surgery for congenital heart disease.12,13 The mechanism of JET is abnormal automaticity in the AV nodal region. The ECG findings in JET show a tachycardia that, in some cases, has identical ventricular and atrial rates, and, in December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com 1401 For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT other cases, has a ventricular rate that is faster than the atrial rate, with ventriculoatrial block. Tachycardia myopathy has been observed in cases in which the AV rate or rhythm has not been adequately controlled.14,15 AV NODE–INDEPENDENT ARRHYTHMIAS Less commonly encountered forms of PSVT, including atrial tachycardia, are independent of AV nodal conduction. These arrhythmias may persist during AV block. The source of these arrhythmias is usually a small focus, and the mechanism is usually abnormal automaticity or triggered activity. The mechanism is usually microreentrant, especially in diseased atria. Atrial tachycardias (commonly called flutters, if sufficiently rapid) may also occur as a result of a macroreentrant mechanism. However, the reentrant circuit in these tachycardias lies within the atrium (eg, a surgical atriotomy scar) and is not dependent on the AV node. Although PSVT may be related to reentry in and around the sinus node region, this type of reentry is rarely observed as a clinically relevant SVT. Technically, multifocal atrial tachycardia, atrial flutter, and atrial fibrillation are all AV node–independent arrhythmias. However, these conditions are not discussed further in the current review. INTERPRETATION OF ECG FINDINGS IN PSVT Most PSVTs are represented on ECGs as narrow QRScomplex tachycardias, with the QRS duration being less than 90 ms (ie, normal QRS duration). Tachycardia-contingent BBB (ie, aberrancy) is relatively frequent in patients with PSVT. Many of these patients may have preexistent BBB, interventricular conduction delays, or some other QRS abnormality. These abnormalities carry over to the tachycardia. An initial analysis of ECG findings for a patient with PSVT is best followed by a methodical approach to ECG interpretation, in which the physician reviews the elements of the differential diagnosis, either mentally or in writing, and examines the evidence supporting each diagnostic possibility. A high-quality12-lead ECG is much more useful in the clinical setting than limited presentations or individual cardiac rhythm strips. The main ECG findings of interest are compelling atrial activity and zones of transition, such as ectopy, cycle length change, or intermittent aberrant conduction. Interventions may be helpful if the mechanism of the tachycardia is unclear from examination of the routine ECG or rhythm strips. Vagal stimulation maneuvers, such as carotid sinus massage or Valsalva maneuver, are classic 1402 Mayo Clin Proc. • procedures for assessing the role of the AV node in the tachycardia mechanism. Pharmacologic interventions are most useful for quickly determining the mechanism of an arrhythmia. Features to consider in ECG interpretation include the following: (1) tachycardia rate; (2) mode of onset and termination of the tachycardia; (3) relative position of the P wave within the R-R interval; (4) morphology of the P wave; (5) change in QRS morphology, including variability in cycle length and relative movement of the atrial ECG and ventricular ECG during variability in tachycardia rate; and (6) effect of intermittent BBB on the tachycardia. TACHYCARDIA RATE Careful analysis of the R-R interval should be performed to determine the rate of the tachycardia. A rate of 150 beats/ min raises the suspicion of atrial flutter with 2:1 AV block because the usual atrial rate during flutter is 300 beats/ min. In general, a tachycardia with an atrial rate of less than 160 to 170 beats/min and without a visible P wave implies the presence of the slow-pathway component of the AV node. The most frequently encountered PSVT of this type is typical AV nodal reentry (ie, AVNRT), a schematic of which is shown in Figure 1. Atrial tachycardia or AVRT involving a slow AV nodal pathway for anterograde conduction are considerably less frequently observed than AVNRT. Faster rates of tachycardia are not generally helpful in narrowing the differential diagnosis. MODE OF ONSET AND TERMINATION OF TACHYCARDIA Onset. The physician should check if the onset of the patient’s tachycardia is captured on the ECG. Most PSVTs are triggered by a premature atrial complex (PAC). If the PAC conducts to the ventricle with a very long PR interval at initiation of tachycardia (ie, a “jump” in the PR interval), the physician can safely postulate that the tachycardia is dependent on anterograde slow-pathway conduction of the AV node to the ventricle. Atrioventricular nodal reentrant tachycardia is the typical tachycardia that begins with this mechanism. It is important to remember that a PAC, if coupled closely enough, generally results in a longer PR interval in the premature cycle because of normal decremental AV nodal physiologic factors. Supraventricular tachycardias that start with a ventricular premature complex are usually AV node–dependent tachycardias. Supraventricular tachycardias are almost never atrial tachycardias. Termination. Tachycardias in which the last event at termination is a P wave are highly unlikely to be atrial tachycardias. If such conditions were atrial tachycardias, it would be necessary to postulate that the last atrial beat caused the block in the AV node. It is more logical to December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT FIGURE 1. Schematic of typical atrioventricular nodal reentry. The panel on the left demonstrates anterograde conduction from the atrium (ATR) to the ventricle (VTR) over both slow and fast pathways. The ventricle is activated initially in sinus rhythm by the fast pathway. The panel in the center shows the effect of a premature atrial complex (PAC). Although the fast pathway conducts rapidly, it repolarizes slowly. In this hypothetical scenario, the fast pathway is refractory to the PAC, allowing the PAC to proceed via the slow pathway, which has a shorter refractory period. In the panel on the right, conditions are such that anterograde conduction of the PAC occurs via the slow pathway, with subsequent recovery of the fast pathway. These conditions allow retrograde conduction into the atrium via the fast pathway, thereby creating the first beat of typical slow-fast atrioventricular nodal reentrant tachycardia. postulate that the block in the AV node caused the tachycardia to terminate and, consequently, that the condition is an AV node–dependent tachycardia. Although an atrial tachycardia almost always terminates with a ventricular complex, this observation may not be helpful in diagnosis because some AV node–dependent tachycardias also terminate in this manner. Figure 2 shows a schematic of 2 terminations of tachycardias. RELATIVE POSITION OF THE P WAVE WITHIN THE R-R INTERVAL When analyzing ECGs of any PSVT, the physician should attempt to identify the presence of P waves. A widely used classification nomenclature of PSVT morphology, as previously mentioned, is the long RP tachycardia vs the short RP tachycardia. This nomenclature is purely descriptive and in most cases does not help the physician to narrow the differential diagnosis. Nevertheless, in cases in which simultaneous atrial and ventricular activation occurs, this classification system can be used to rule out AVRT, pointing to typical slow-fast AVNRT. This type of AVNRT is depicted in the center panel of Figure 3. With any extremely rapid PSVT, both the RP interval and PR interval become short, making it difficult to distinguish between the two. However, at slower PSVT rates, a shorter RP interval is usually indicative of AVRT, as shown in the top panel of Figure 3, and a long RP interval most commonly represents atrial tachycardia. Long RP morphologies, shown in the bottom panel of Figure 3, may also represent atypical AVNRT or AVRT. Finally, sinus tachycardia is technically a long RP tachycardia, but it can often be differentiated from atrial tachycardia through Mayo Clin Proc. • close comparison of P-wave morphology during sinus rhythm vs during the tachycardia. These guidelines for ECG interpretation have been validated with electrophysiologic data. Kalbfleisch et al16 reported that more than 90% of AVNRTs and 87% of AVRTs are short RP tachycardias. By contrast, only 11% of atrial tachycardias present as short RP tachycardias.16 MORPHOLOGY OF THE P WAVE P waves may be difficult to distinguish in ECGs, especially during more rapid tachycardia, because of overlap with the FIGURE 2. Schematic of 2 terminations of paroxysmal supraventricular tachycardia (PSVT) as recorded on electrocardiograms. The top panel demonstrates PSVT terminating with a ventricular complex. The bottom panel shows PSVT terminating with an atrial complex, indicating that this patient is highly unlikely to have atrial tachycardia. December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com 1403 For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT FIGURE 3. Schematic representing appearances of long RP tachycardia and short RP tachycardia morphologies. The electrocardiogram (ECG) in the top panel indicates a short RP tachycardia. The 3 examples of this condition shown to the right of the ECG are (left to right) atrioventricular reentrant tachycardia (AVRT), atrial tachycardia, and atrioventricular nodal reentrant tachycardia (AVNRT). The ECG in the panel in the center also indicates a short RP morphology, with a very short ventriculoatrial time. Examples shown for this condition are (left to right) typical AVNRT and atrial tachycardia with anterograde slow-pathway conduction. The ECG in the bottom panel indicates a long RP morphology. Examples shown for this condition are (left to right) atypical AVNRT, atrial tachycardia, and AVRT. Theoretically, junctional ectopic tachycardia can present as any of the morphologies shown in this figure. QRS and T waves. If P waves are visible during tachycardia, comparison with P waves in sinus rhythm is useful. Although all available ECG leads require inspection, evaluation of the inferior ECG leads (particularly lead II), as well as lead V1, is likely to be the most productive. A normal P wave has a positive QRS morphology in the inferior leads because normal atrial activation begins at the sinus node during sinus rhythm, with a wave of electrical propagation moving toward the AV node (ie, high to low sequence). As this impulse moves toward the inferior leads, it produces an upright P wave in leads II, III, and aVF. By contrast, junctional-dependent rhythms, such as AVNRT and AVRT, and atrial tachycardias with origins in the lower atrium result in negative P waves in the inferior leads. The negative P waves occur because these tachycardias activate the atrium in the opposite direction (ie, low to high sequence). Careful analyses of other ECG leads can help physicians to determine if the atria are being activated from left to right or vice versa. This conclusion can be achieved by examining the morphology of the P wave in leads I and aVL. In right atrial tachycardia foci, the P wave is positive or biphasic (ie, first negative, then positive) in lead aVL. That is because the right atrium is activated first, with the wave of depolarization moving toward the left atrium and, thus, to lead aVL. In left atrial tachycardia foci, the P wave 1404 Mayo Clin Proc. • is negative or isoelectric (ie, electrically neutral) in lead aVL. In addition, a positive P wave (ie, from the back to the front) is observed in lead V1 in left atrial foci. This contrasts with the negative or biphasic P wave observed in lead V1 when the atrial tachycardia is of right atrial origin. In the long RP tachycardias caused by atrial tachycardias, the P-wave morphology provides the first approximation of the site of the abnormal focus.17-19 These algorithms may be useful if the physician attempts to ablate the tachycardia. CHANGE IN QRS MORPHOLOGY A ventricular rate that is irregularly irregular (ie, a rate that is variable in unpredictable ways), including having an irregular baseline, suggests a diagnosis of atrial fibrillation. The cycle length in most cases of PSVT is reasonably regular; however, it may oscillate in a patient who has dual or multiple anterograde AV nodal pathways. In fact, most oscillation in cycle length occurs in the anterograde part of the circuit. Patients with atrial tachycardias may present with a notably irregular ventricular rate if there is variable block in the AV node. A more subtle oscillation in cycle length can be diagnostically useful. If the ECG shows that the QRS change initiates the P-wave change during SVT (ie, if the VV change precedes the AA change), the patient’s condition December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT FIGURE 4. Electrocardiograms indicative of paroxysmal supraventricular tachycardia, with no visible P wave. Left, normal QRS morphology; right, sudden development of right-sided bundle branch block (without any change in cycle length). The tachycardia shown in this electrocardiogram was verified as atrioventricular nodal reentrant tachycardia during electrophysiologic testing. cannot be an atrial tachycardia and must be a junctional reentrant tachycardia instead. The converse (ie, if the AA change precedes the VV change) is less useful for diagnostic purposes, although such an observation usually suggests an atrial tachycardia. QRS alternans is a phasic alteration of the amplitude of the QRS complex, of unclear mechanism, that is observed in 1 or more ECG leads. It is a nonspecific finding in faster tachycardias regardless of mechanism. Thus, it most commonly occurs in conjunction with AVRT (25%-38% of orthodromic AVRT, in which the usual direction of traffic is to the AV node). QRS alternans also occurs with AVNRT (13%-23% of AVNRT), but it is virtually never seen with atrial tachycardia.16,20-22 EFFECT OF INTERMITTENT BBB ON TACHYCARDIA A change in AV rate with the development of BBB aberration can mean only that a bundle branch is part of the tachycardia circuit. This characteristic excludes every SVT mechanism except AV reentry. Bundle branch block that occurs ipsilateral to an accessory pathway results in prolongation of the ventriculoatrial conduction time, which is generally reflected in the tachycardia cycle length.23 This association exists because those bundle branches are active (if not obligatory) components of the tachycardia circuit. The converse is also true. If leftsided BBB resolves during tachycardia and the cycle length decreases, an ipsilateral accessory pathway is suggested. By contrast, the development of right-sided BBB with a left-sided accessory pathway, or vice versa, will have no effect on the tachycardia cycle length because that bundle is not an integral part of the tachycardia circuit. Figure 4 shows an ECG indicative of the sudden development of right-sided BBB in a case of AVNRT. Mayo Clin Proc. • Furthermore, BBB that occurs in either AVNRT or atrial tachycardia has no effect on the tachycardia cycle length because the bundle branches are not integral parts of these tachycardia mechanisms. BROAD COMPLEX TACHYCARDIA SECONDARY TO PSVT A PSVT may present as a broad complex tachycardia for 3 main reasons. First, a preexisting BBB, intraventricular conduction disturbance, or other QRS abnormality in sinus rhythm will usually be manifested during tachycardia. Second, tachycardia-contingent BBB may occur if either the right- or left-sided bundle branch reaches its effective refractory period and cannot conduct impulses to match the rapid rate of the tachycardia. This condition is also called functional BBB or rate-related BBB. Subtle features of the bundle branch may point to PSVT-related broad complex tachycardia rather than ventricular tachycardia. For example, in a patient with PSVT and a structurally normal heart, the bundle branch pattern will usually have a typical appearance, virtually identical to conventional bundle branch morphology.24 Statistically, this is by far the most common cause of wide QRS morphology on ECG in patients with SVT. Third, the QRS morphology will be wide during SVT if the tachycardia is related to preexcitation or conduction over an accessory pathway. The most common preexcited tachycardia, other than atrial fibrillation, is antidromic tachycardia, in which the tachycardia proceeds in an anterograde manner over an accessory pathway and returns via the normal AV conduction system. The accessory pathway may also serve as a route for some other tachycardia mechanism (eg, an atrial tachycardia conducted over an accessory pathway). In such a case, the accessory pathway is December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com 1405 For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT FIGURE 5. Cardiac rhythm strips demonstrating (top) sinus rhythm and (bottom) paroxysmal supraventricular tachycardia. The P wave is seen as a pseudo-R wave (circled in bottom strip) in lead V1 during tachycardia. By contrast, the pseudo-R wave is not seen during sinus rhythm (it is absent from circled area in top strip). This very short ventriculoatrial time is frequently seen in typical atrioventricular nodal reentrant tachycardia. not part of the mechanism that causes the atrium to beat rapidly. Patients with accessory pathways may present on different occasions with either antidromic or orthodromic tachycardia because many pathways are capable of bidirectional conduction. Ventricular tachycardia needs to be considered in the differential diagnosis of any tachycardia, but especially a tachycardia represented by a wide QRS morphology. The hallmarks of ventricular tachycardia (eg, AV dissociation, capture and fusion beats, extreme axis deviation, atypical bundle branch morphology) should be investigated in the diagnosis. A useful rule of thumb is that, for patients who present with a broad complex tachycardia and a history of coronary artery disease/myocardial infarction, the arrhythmia should be considered to be a ventricular tachycardia until proven otherwise. PSVT SECONDARY TO AVNRT Patients with PSVT secondary to AVNRT are typically young (20-35 years) and generally healthy, with no history of structural heart disease. However, PSVT secondary to AVNRT also occurs in older individuals. Slightly more women than men have this type of PSVT. Typical AVNRT is seldom incessant and, hence, does not generally present as tachycardia myopathy or portend an adverse prognosis for patients. Unless either preexistent or rate-related BBB is present, the QRS morphology of AVNRT typically appears narrow and without clearly discernible P waves on ECG. In some cases, P waves can be seen as pseudo-R waves, particularly in lead V1 and in the inferior leads II, III and aVF (Figure 5). Rarely, P waves can also manifest as pseudo-Q waves, when retrograde atrial depolarization precedes ventricular depolarization. In such cases, a direct com1406 Mayo Clin Proc. • parison with QRS morphology in sinus rhythm is required to establish the presence of pseudo-Q waves. The ventricular rate during AVNRT is usually between 160 and 180 beats/ min. The most common form of AVNRT (ie, slow-fast AVNRT) is also the most frequent cause of any PSVT. The mechanism of tachycardia is related to the presence of dual AV nodal pathways (ie, functionally or anatomically separate routes of AV node conduction). Typical AV nodal reentry is thought to be related to a fast pathway (anteriorly near the AV node’s junction with the bundle of His) and to a slow pathway (at the entrance to the AV node between the coronary sinus orifice and the tricuspid annulus). Atrioventricular nodal reentry begins if these 2 pathways become dissociated (Figure 1). Normal AV nodal conduction occurs in an anterograde manner over both the fast and slow pathway. However, a PAC may reach the fast pathway early when it is refractory. The PAC will then act to block conduction in this pathway. Subsequent conduction occurs more slowly over the slow pathway, resulting in PR prolongation. The impulse may then find the distal end of the fast pathway recovered enough for retrograde conduction (ie, reentry) to the atrium, resulting in the first beat of tachycardia. Hence, the anterograde limb of the tachycardia occurs via the slow AV nodal pathway, whereas the retrograde limb occurs via the fast AV nodal pathway. Because the atria and ventricles are generally activated simultaneously as a result of this small circuit in the middle of the heart, the P wave is often obscured by, buried within, or very close to the QRS complex on the ECG. PSVT SECONDARY TO AVRT Patients who present with PSVT secondary to AVRT are generally similar demographically to those with AVNRT. However, individuals with AVRT are less likely to present in middle age or later than those with AVNRT. A narrow complex tachycardia is seen in the ECGs of patients with AVRT, because anterograde conduction usually proceeds via the AV node and His-Purkinje system to the ventricle. Retrograde conduction then occurs via the accessory pathway, which may be located on the right, left, or septal AV areas. This type of tachycardia is an orthodromic tachycardia and is the most common type of SVT observed in accessory pathways. In contrast to AVNRT, in which the atria and ventricles are typically activated nearly simultaneously, in AVRT, first the ventricles and then the atria are activated in sequence. Subsequently, the P wave is usually in the ST segment or T wave of an ECG and is often visible between successive R waves. Patients with accessory pathways may also present with broad complex tachycardia resulting from aberrancy or December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT preexcited tachycardia (ie, antidromic AVRT) or from ventricular tachycardia. However, the most common wide QRS tachycardia observed in patients with accessory pathways is orthodromic SVT with aberrant ventricular conduction. Preexcited tachycardia, in which the pathway conducts in an anterograde manner, occurs less frequently. The most common form of preexcited tachycardia uses the accessory pathway as the anterograde limb and the AV node as the retrograde limb of the circuit (Figure 6). Because the ventricle is activated via myocardium rather than specialized conduction tissue of the His-Purkinje system, ventricular depolarization happens slowly, resulting in the broad complex preexcited rhythm. Electrocardiograms of patients with accessory pathway arrhythmias may or may not show delta waves (ie, initial slurring of the QRS) in sinus rhythm. The presence of a delta wave in sinus rhythm usually suggests that the SVT is related to the accessory pathway. AP AVN QRS MORPHOLOGY IN TACHYCARDIA VENTRICULAR PREEXCITATION Preexcitation of the ventricles is indicated by the presence in the ECG of a shortened PR interval in association with slurring of the upstroke of the QRS complex.25 Preexcitation occurs as the sinus impulse travels to the ventricle via both the AV node and the accessory pathway, resulting in a fusion of ventricular activation via both the conventional His-Purkinje system and the accessory pathway. Because AV nodal conduction is decremental and, hence, relatively slow, the first part of the QRS is slurred—that is, the anterograde accessory pathway conduction reaches the ventricle first, forming a delta wave on the ECG. This slurring persists until AV nodal conduction propagates into the ventricle, activating the ventricles rapidly and resulting in a terminal QRS complex that is closer to normal in morphology. The greater the ventricular activation over an accessory pathway, the more preexcitation occurs (thus, the broader the QRS) and vice versa. Many algorithms used in diagnosis allow approximate localization of accessory pathways along the AV rings on the basis of preexcited ECG morphology. These algorithms are more reliable when the preexcitation is predominant. A minimally preexcited ECG makes precise localization difficult; however, such ECG results generally suggest a left lateral pathway that is much farther away from the source of normal atrial activation than the AV node.26,27 Accessory pathways are most commonly located in the left lateral position (Figure 7), where the ECG shows a delta wave that is positive in lead V1 and negative in lead I. In right-sided pathways, the delta wave is usually negative in lead V1 (with a QS pattern) and positive in lead I. Mayo Clin Proc. • FIGURE 6. Schematic of orthodromic and antidromic tachycardia, showing the relationship between the atrioventricular node (AVN) and the accessory pathway (AP) and the associated QRS morphology. The top panel demonstrates anterograde conduction through the AV node and retrograde conduction to the atria via the accessory pathway. This condition is an orthodromic tachycardia, which usually has a narrow complex QRS morphology. The bottom panel demonstrates anterograde conduction via an accessory pathway and retrograde conduction via the AV node. This condition is an antidromic tachycardia, presenting with a wide complex QRS morphology. Accessory pathways may conduct only intermittently or be so far lateral as to ensure that the bulk of anterograde ventricular activation during sinus rhythm occurs via the sinus node, resulting in an ECG that does not show preexcitation. Although most accessory pathways are capable of bidirectional conduction, some are concealed, meaning that they are capable only of retrograde conduction. These accessory pathways never produce preexcitation on ECGs, and they can result only in orthodromic tachycardia. PREEXCITED ATRIAL FIBRILLATION An association exists between accessory pathways and an increased risk of atrial fibrillation. A classic feature of preexcited atrial fibrillation is an irregularly irregular cycle length in conjunction with an irregularly irregular QRS duration. This feature develops because the atrial fibrillation wave fronts conduct to the ventricle via both the AV node and the accessory pathway, causing a fusion of ventricular activation over both structures. Unlike the conduction properties of the AV node, the conduction properties December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com 1407 For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT FIGURE 7. Electrocardiogram showing a positive dominant R wave in lead V1, with slurring of the initial deflection of the QRS complex (ie, the delta wave indicated by the arrow), and ventricular preexcitation resulting from a left lateral accessory pathway. of accessory pathways are usually nondecremental. If the pathway has a short refractory period, conduction to the ventricles at extremely rapid rates (>250 beats/min) is possible and may lead to ventricular fibrillation.28 Accessory pathways are also capable of anterograde conduction in cases of atrial tachycardia, AVNRT, and atrial flutter. In such cases, the pathway acts like a bystander, not participating in the mechanism driving the tachycardia. PSVT SECONDARY TO ATRIAL TACHYCARDIA Patients may present with atrial tachycardia at any age. Younger patients, especially those in the pediatric age group, are most likely to have a focal atrial tachycardia suggestive of abnormal automaticity or triggered activity. Older patients, especially those with cardiac disease and such comorbidities as cardiorespiratory problems, are more likely to have an atrial tachycardia substrate related to such conditions as atrial stretch or scarring. Atrial tachycardia is usually revealed on an ECG as a long RP tachycardia, as in the bottom panel in Figure 3. The mechanism of atrial tachycardia usually includes enhanced automaticity, triggered activity, or reentry. If conduction happens conventionally to the ventricle via the AV node, variable AV block may result. Atrial tachycardias may also conduct in an anterograde manner over an accessory pathway, resulting in a preexcited broad complex tachycardia. Once again, the accessory pathway acts like a bystander, not participating in the driving mechanism of the tachycardia. Atrial tachycardias can be incessant. In such cases, patients may present with chronic cardiac failure caused by 1408 Mayo Clin Proc. • tachycardia-induced myopathy. Figure 8 shows an ECG indicative of incessant postpartum atrial tachycardia. EMERGENCY MANAGEMENT OF PSVT As with any emergency cardiac situation, the “golden rule of ABC” (airway, breathing, circulation) should be followed in emergency management of PSVT. A rapid assessment of the patient’s airway, breathing, and circulation should be conducted, and all vital signs should be documented. If the patient is hemodynamically compromised or in cardiovascular collapse (both of which are unusual conditions in PSVT), urgent direct-current cardioversion should be performed without delay.29 Most patients who present with PSVT are hemodynamically stable, allowing enough time for physicians to perform a thorough history, physical examination, and 12-lead ECG examination. Patients should also ideally undergo noninvasive blood pressure assessment, measurement of oxygen saturation levels, and continuous ECG monitoring. Oxygen supplementation should be used when necessary. The initial strategy for terminating a PSVT is generally a vagotonic maneuver, such as carotid sinus massage. However, the physician should evaluate the patient for the presence of a carotid bruit (ie, abnormal sound) before attempting this maneuver, especially in elderly patients. The Valsalva maneuver or possibly facial immersion in cold water may also be attempted. These methods serve to increase vagal tone, which may prolong AV nodal refractoriness to the point of AV block, thereby terminating the tachycardia. It should be noted that vagotonic maneuvers will not terminate atrial tachycardia, but they may create December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT transient AV block, clarifying the underlying mechanism by allowing visualization of the P wave. If these efforts are unsuccessful in terminating PSVT, the next step in treatment is pharmacologic intervention. Previous strategies of using infusions of sympathomimetic medications (eg, methoxamine hydrochloride, phenylephrine), parasympathomimetic medications (eg, neostigmine, edrophonium), or digoxin are now rarely, if ever, used. The use of intravenous verapamil and adenosine has become standard treatment. Adenosine has a rapid half-life of only a few seconds, and it produces intense but transient AV block. Adenosine is safe to use in patients who have structural heart disease because it does not produce a negatively inotropic effect. The standard starting dose of adenosine is a 6-mg bolus, which should be administered rapidly through a free-flowing intravenous line. Doses of 12 mg or even 18 mg may also be used. The physician needs to ensure that the patient does not have asthma or reversible obstructive pulmonary disease before administering adenosine because this drug can cause acute bronchospasm. Adenosine can be potentiated by dipyridamole. Hence, much smaller doses of adenosine should be used if the patient is taking dipyridamole to avoid prolonged AV block. Patients should be warned that administration of adenosine may cause transient sensations of chest tightness, nausea, and flushing. Despite these minor adverse effects, adenosine is a safe drug for patients in all age groups.30,31 Adenosine will usually terminate AV node– dependent rhythms, such as AVNRT and AVRT, and it may also terminate some types of atrial tachycardias.32 In some cases of PSVT, calcium channel blockers and !-blockers may be useful. However, the dihydropyridine class of calcium channel blockers should not be used because they have no effect on AV nodal conduction. Typical intravenous calcium channel blockers that may be effective include verapamil and diltiazem. Among !-blockers, metoprolol and atenolol may be effective. If the physician is concerned about the patient’s ability to tolerate a !blocker, intravenous esmolol, which has a very short halflife, may be used. Verapamil is the medication most commonly used as an alternative to adenosine. Verapamil is especially useful if adenosine is contraindicated or if the PSVT terminates rapidly but is immediately recurrent. The use of vagal maneuvers, adenosine, or verapamil will convert most AV node–dependent SVTs and some atrial tachycardias. If atrial tachycardia persists, however, such intravenous medications as procainamide may be needed. If control of atrial tachycardia is not achieved with any of these interventions, the physician should consider using elective cardioversion, particularly if conversion is expediently desired. Mayo Clin Proc. • FIGURE 8. Electrocardiogram showing incessant atrial tachycardia in a young woman who presented with postpartum tachycardia-induced myopathy. Arrows indicate evidence of atrial activity. Management strategies for PSVT should not change for patients who are known to have accessory pathways, but physicians should be aware that atrial fibrillation with rapid ventricular response can develop during the treatment process. If this response occurs, intravenous procainamide or ibutilide may be useful. However, if their use is not feasible or successful, the threshold for using elective cardioversion should be low. LONG-TERM TREATMENT If sufficiently symptomatic, the patient with PSVT should be offered pharmacologic therapy or catheter ablation for long-term treatment. Catheter ablation should be considered early in the management of PSVT because of its proven efficacy and low procedural risk, particularly if the patient has not responded to medication or is reluctant to take medication. Catheter ablation is generally performed on an outpatient basis with a combination of local anesthesia and conscious sedation. Catheters are introduced into the heart via femoral and subclavian venous access, and an December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com 1409 For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT electrophysiologic study is performed to fully elucidate the nature of the SVT. Catheter ablation has a high procedural success rate of approximately 95% for patients with clinical tachycardia, particularly AVNRT and AVRT. As many as 5% of patients may experience a recurrence of tachycardia and require a second procedure. In the case of AVNRT, the patient can be treated by performing careful ECG mapping and delivering radiofrequency energy to the slow-pathway area of the heart (ie, the posteromedial tricuspid annulus, near the coronary sinus ostium). In patients with AVNRT and in some patients with accessory pathways, the site of ablation is extremely close to the compact AV node. Therefore, these patients should be informed of a small risk (0.1%-1%) of potential damage to the AV node. Such damage would require implantation of a permanent pacemaker. Catheter ablation is highly effective in most cases of PSVT, regardless of the mechanism. Research indicates that ablation may be more effective for AVRT and AVNRT (>95% success rate) than for the atrial tachycardias (>80% success rate). Nevertheless, certain considerations, such as a patient’s very advanced age or comorbidities, may lead a physician to reject the use of catheter ablation. Cryoablation (ie, using extreme cold to produce a “lesion”) is another procedure that can be used to ablate either AVNRT or AVRT. Cryoablation may have a lower risk of inadvertent AV block than catheter ablation.33-36 Some patients with PSVT may prefer using medications instead of undergoing ablation. Traditionally, AV nodal blocking agents, such as verapamil and diltiazem, or !blockers are used first. Class I antiarrhythmic agents, such as flecainide and propafenone, may also be effective. Such drugs are preferable for patients with known WolffParkinson-White syndrome because they generally prolong the effective refractory period of the accessory pathway. Class I antiarrhythmic agents may also have some efficacy in the prophylaxis of atrial fibrillation. Patients with atrial tachycardia generally require the use of an AV nodal blocking drug for atrial rate control. A membrane-active drug can be used for prevention of atrial tachycardia. Sotalol is a !-blocker with antiarrhythmic properties that may be useful in any case of PSVT. Amiodarone is effective in the management of PSVT, but it is rarely indicated because of its potential toxicity over the long term and because of the availability of effective alternatives. CONCLUSION Paroxysmal SVT is a common presenting diagnosis among patients with cardiac conditions, both in the emergency 1410 Mayo Clin Proc. • department and in the physician’s office. In the emergency department setting, the physician should conduct a thorough assessment of the patient, followed by close inspection of all available ECGs or cardiac rhythm strips. Comorbid conditions and current drug therapies should be considered before any decision is made regarding treatment for patients with arrhythmia. When sinus rhythm is restored, the physician should consider the long-term management options for the patient, including conservative pharmacologic and ablative strategies. REFERENCES 1. Hinkle LE Jr, Carver ST, Stevens M. The frequency of asymptomatic disturbances of cardiac rhythm and conduction in middle-aged men. Am J Cardiol. 1969;24(5):629-650. 2. Clarke JM, Hamer J, Shelton JR, Taylor S, Venning GR. The rhythm of the normal human heart. Lancet. 1976;1(7984):508-512. 3. Harrison DC, Fitzgerald JW, Winkle RA. Contribution of ambulatory electrocardiographic monitoring to antiarrhythmic management. Am J Cardiol. 1978;41(6):996-1004. 4. Manolio TA, Furberg CD, Rautaharju PM, et al. Cardiac arrhythmias on 24-h ambulatory electrocardiography in older women and men: the Cardiovascular Health Study. J Am Coll Cardiol. 1994;23(4):916-925. 5. Roche F, Gaspoz JM, Da Costa A, et al. Frequent and prolonged asymptomatic episodes of paroxysmal atrial fibrillation revealed by automatic longterm event recorders in patients with a negative 24-hour Holter. Pacing Clin Electrophysiol. 2002;25(11):1587-1593. 6. Brembilla-Perrot B, Marçon F, Bosser G, et al. Paroxysmal tachycardia in children and teenagers with normal sinus rhythm and without heart disease. Pacing Clin Electrophysiol. 2001;24(1):41-45. 7. Leitch J, Klein G, Tee R, Murdock C, Teo WS. Neurally mediated syncope and atrial fibrillation [letter]. N Engl J Med. 1991;324(7):495496. 8. Nerheim P, Birger-Botkin S, Piracha L, Olshansky B. Heart failure and sudden death in patients with tachycardia-induced cardiomyopathy and recurrent tachycardia. Circulation. 2004 Jul 20;110(3):247-252. Epub 2004 Jun 28. 9. Coumel P, Flammang D, Attuel P, Leclercq JF. Sustained intra-atrial reentrant tachycardia: electrophysiologic study of 20 cases. Clin Cardiol. 1979;2(3):167-178. 10. Coumel P. Junctional reciprocating tachycardias: the permanent and paroxysmal forms of A-V nodal reciprocating tachycardias. J Electrocardiol. 1975;8(1):79-90. 11. Huang SKS, Wood MA. Catheter Ablation of Cardiac Arrhythmias. Philadelphia, PA: Saunders/Elsevier; 2006. 12. Garson A Jr, Gillette PC. Junctional ectopic tachycardia in children: electrocardiography, electrophysiology and pharmacologic response. Am J Cardiol. 1979;44(2):298-302. 13. Case CL, Gillette PC. Automatic atrial and junctional tachycardias in the pediatric patient: strategies for diagnosis and management. Pacing Clin Electrophysiol. 1993;16(6):1323-1335. 14. Villain E, Vetter VL, Garcia JM, Herre J, Cifarelli A, Garson A Jr. Evolving concepts in the management of congenital junctional ectopic tachycardia: a multicenter study. Circulation. 1990;81(5):1544-1549. 15. Walsh EP, Saul JP, Sholler GF, et al. Evaluation of a staged treatment protocol for rapid automatic junctional tachycardia after operation for congenital heart disease. J Am Coll Cardiol. 1997;29(5):1046-1053. 16. Kalbfleisch SJ, el-Atassi R, Calkins H, Langberg JJ, Morady F. Differentiation of paroxysmal narrow QRS complex tachycardias using the 12-lead electrocardiogram. J Am Coll Cardiol. 1993;21(1):85-89. 17. Morton JB, Sanders P, Das A, Vohra JK, Sparks PB, Kalman JM. Focal atrial tachycardia arising from the tricuspid annulus: electrophysiologic and electrocardiographic characteristics. J Cardiovasc Electrophysiol. 2001;12(6): 653-659. December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings. SUPRAVENTRICULAR TACHYCARDIA: DIAGNOSIS AND MANAGEMENT 18. Tang CW, Scheinman MM, Van Hare GF, et al. Use of P wave configuration during atrial tachycardia to predict site of origin. J Am Coll Cardiol. 1995;26(5):1315-1324. 19. Tada H, Nogami A, Naito S, et al. Simple electrocardiographic criteria for identifying the site of origin of focal right atrial tachycardia. Pacing Clin Electrophysiol. 1998;21(11, pt 2):2431-2439. 20. Green M, Heddle B, Dassen W, et al. Value of QRS alteration in determining the site of origin of narrow QRS supraventricular tachycardia. Circulation. 1983;68(2):368-373. 21. Morady F. Significance of QRS alternans during narrow QRS tachycardias. Pacing Clin Electrophysiol. 1991;14(12):2193-2198. 22. Kay GN, Pressley JC, Packer DL, Pritchett EL, German LD, Gilbert MR. Value of the 12-lead electrocardiogram in discriminating atrioventricular nodal reciprocating tachycardia from circus movement atrioventricular tachycardia utilizing a retrograde accessory pathway. Am J Cardiol. 1987;59(4):296300. 23. Coumel P, Attuel P. Reciprocating tachycardia in overt and latent preexcitation: influence of functional bundle branch block on the rate of the tachycardia. Eur J Cardiol. 1974;1(4):423-436. 24. Josephson ME. Clinical Cardiac Electrophysiology: Techniques and Interpretations. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002. 25. Wolff L, Parkinson J, White PD. Bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia: 1930. Ann Noninvasive Electrocardiol. 2006;11(4):340-353. 26. Szabo TS, Klein GJ, Guiraudon GM, Yee R, Sharma AD. Localization of accessory pathways in the Wolff-Parkinson-White syndrome. Pacing Clin Electrophysiol.1989;12(10):1691-1705. 27. Fitzpatrick AP, Gonzales RP, Lesh MD, Modin GW, Lee RJ, Scheinman MM. New algorithm for the localization of accessory atrioventricular connec- tions using a baseline electrocardiogram [published correction appears in J Am Coll Cardiol. 1994;23(5):1272]. J Am Coll Cardiol. 1994;23(1):107-116. 28. Klein GJ, Bashore TM, Sellers TD, Pritchett EL, Smith WM, Gallagher JJ. Ventricular fibrillation in the Wolff-Parkinson-White syndrome. N Engl J Med. 1979;301(20):1080-1085. 29. Zimetbaum P, Josephson ME. Evaluation of patients with palpitations. N Engl J Med. 1998;338(19):1369-1373. 30. Till J, Shinebourne EA, Rigby ML, Clarke B, Ward DE, Rowland E. Efficacy and safety of adenosine in the treatment of supraventricular tachycardia in infants and children. Br Heart J. 1989;62(3):204-211. 31. Camaiti A, Del Rosso A, Morettini A, Nozzoli C, Grifoni S, Berni G. Efficacy and safety of adenosine in diagnosis and treatment of regular tachycardia in the elderly. Coron Artery Dis. 1998;9(9):591-596. 32. Markowitz SM, Nemirovksy D, Stein KM, et al. Adenosine-insensitive focal atrial tachycardia: evidence for de novo micro-re-entry in the human atrium. J Am Coll Cardiol. 2007 Mar 27;49(12):1324-1333. Epub 2007 Mar 9. 33. Kriebel T, Broistedt C, Kroll M, Sigler M, Paul T. Efficacy and safety of cryoenergy in the ablation of atrioventricular reentrant tachycardia substrates in children and adolescents. J Cardiovasc Electrophysiol. 2005;16(9):960-966. 34. Collins KK, Dubin AM, Chiesa NA, McDaniel GM, Van Hare GF. Cryoablation in pediatric atrioventricular nodal reentry: electrophysiologic effects on atrioventricular nodal conduction. Heart Rhythm. 2006 May; 3(5):557-563. Epub 2006 Feb 28. 35. Collins KK, Dubin AM, Chiesa NA, Avasarala K, Van Hare GF. Cryoablation versus radiofrequency ablation for treatment of pediatric atrioventricular nodal reentrant tachycardia: initial experience with 4-mm cryocatheter. Heart Rhythm. 2006 May;3(5):564-570. Epub 2006 Feb 28. 36. Rostock T, Risius T, Ventura R, et al. Efficacy and safety of radiofrequency catheter ablation of atrioventricular nodal reentrant tachycardia in the elderly. J Cardiovasc Electrophysiol. 2005;16(6):608-610. The Symposium on Cardiovascular Diseases will continue in the January issue. Mayo Clin Proc. • December 2008;83(12):1400-1411 • www.mayoclinicproceedings.com 1411 For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.