September 5, 2013
MORGAN STANLEY BLUE PAPER
MORGAN STANLEY RESEARCH
Global
1
Michael K Jungling
Michael.Jungling@morganstanley.com
+44 (0)20 7425 5975
1
Patrick A Wood, CFA
Patrick.Wood@morganstanley.com
+44 (0)20 7425 4107
Yukihiro Koike
2
Yukihiro.Koike@morganstanleymufg.com
+81 (0)3 5424 5316
See page 2 for all contributors to this report
1 Morgan Stanley & Co. International plc+
2 Morgan Stanley MUFG Securities Co., Ltd.+
MedTech: 3D Printing
A Solution for Innovation
Read Capital Goods: 3D Printing –
Don’t Believe (All) The Hype
MedTech is especially suited for 3D printing. 3D printing is not new, but improvements
in printers and a growing portfolio of materials are making the technology much more
relevant. In this Blue Paper, we explore how 3D printing is opening up an age of
‘personalised medical solutions’. Although the broader impact of 3D printing on traditional
manufacturing may be limited near term, the potential patient and manufacturing benefits
for MedTech are substantial. The sector accounts for almost 40% of patent applications
for 3D manufacturing over the past two years – more than any other space.
Orthopaedics and Prosthetics look most promising short term. These subsectors are
already using early-stage products and have real opportunities to boost revenues and cut
costs. Longer term, research into printing functional organs is well under way – although
most commentators agree that it will be at least 10 years before the technology is viable.
We look in detail at the implications of 3D printing by subsector – in particular, we
highlight Dentistry, where we think the impact will be increasingly significant with winners
determined by how rapidly companies can adapt to the changing technology.
Our illustrative example for Smith & Nephew shows scope for upside. Orthopaedics
could benefit from lower cost of sales and inventory, with ‘just-in-time’ manufacturing of
customised implants. Costing data from AM technology supplier Arcam suggests a hip
joint can be produced at ~65% of the cost of conventional methods. Conservatively, 25%
lower costs would increase 2016 free cash flow yield from 8.4% to 11.4%, we estimate. A
15% improvement in inventory turn would add another 0.3%, for 11.7% free cash flow
yield, and increase our DCF by up to 35%. Ultimately, the impact 3D printing has on
S&N’s financials depends largely on how fast it can implement the technology available.
by Ben Uglow, published
September 5, 2013
Morgan Stanley Blue Papers focus on critical
investment themes that require coordinated
perspectives across industry sectors, regions,
or asset classes.
Morgan Stanley does and seeks to do business with companies covered in Morgan Stanley Research. As a result, investors should be aware that the firm may
have a conflict of interest that could affect the objectivity of Morgan Stanley Research. Investors should consider Morgan Stanley Research as only a single factor
in making their investment decision.
For analyst certification and other important disclosures, refer to the Disclosure Section, located at the end of this report.
* = This Research Report has been partially prepared by analysts employed by non-U.S. affiliates of the member. Please see page 2 for the name of each non-U.S.
affiliate contributing to this Research Report and the names of the analysts employed by each contributing affiliate.
+= Analysts employed by non-U.S. affiliates are not registered with FINRA, may not be associated persons of the member and may not be subject to NASD/NYSE
restrictions on communications with a subject company, public appearances and trading securities held by a research analyst account.
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Global MedTech & Services
Europe
Michael Jungling1
Patrick Wood1
+44 20 7425-5975
+44 20 7425-4107
Michael.Jungling@morganstanley.com
Patrick.wood@morganstanley.com
+1 415 576-2324
+1 212 761-6672
+1 212 761-4847
+1 212 761-3222
David.R.Lewis@morganstanley.com
Steve.Beuchaw@morganstanley.com
Jonathan.Demchick@morganstanley.com
James.Francescone@morganStanley.com
+81 3 5424 5926
+81 3 5424-5316
Shinichiro.Muraoka@morganstanleymufg.com
Yukihiro.Koike@morganstanleymufg.com
+852 2239-7596
+852 2848-5649
Bin.Li@morganstanley.com
Yolanda.Hu@morganstanley.com
+91 22 6118-2214
+91 22 6118-2215
Sameer.Baisiwala@morganstanley.com
Saniel.Chandrawat@morganstanley.com
+55 11 3048-6039
Javier.Martinez.Olcoz@morganstanley.com
US
David Lewis 2
Steve Beuchaw 2
Jonathan Demchick2
James Francescone2
Japan
Shinichiro Muraoka3
Yukihiro Koike3
Asia/Pacific (China)
Bin Li4
Yolanda Hu4
Asia/Pacific (India)
Sameer Baisiwala5
Saniel Chandrawat5
Latin America
Javier Martinez de Olcoz Cerdan6
1 Morgan Stanley & Co. International plc+
2 Morgan Stanley & Co. LLC
See page 38 for recent Blue Paper reports.
3 Morgan Stanley MUFG Securities Co., Ltd.+
4 Morgan Stanley Asia Limited+
5 Morgan Stanley India Company Private Limited+
6 Morgan Stanley C.T.V.M. S.A.+
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Table of Contents
MORGAN STANLEY BLUE PAPER
Executive Summary
What is 3D Printing?
Why is MedTEch Suited to 3D Printing?
Where Does The Opportunity Lie?
Limitations to Opportunities
4
4
4
5
5
Medical Devices – AM Could Drive Innovation and Cost Savings
What is 3D Printing?
Market Size
Why is MedTech Suited?
Printing Technologies
Materials Available
Drawbacks
Patent Development – Medical Right Up There
7
7
7
7
8
9
9
9
Where Do Opportunities Lie?
Evaluation Framework
Size of Opportunity – Relative Analysis
Making the Selection
Example of AM Benefits
Opportunity or Risk?
AM Disruptive Example – Hearing Aids
11
11
12
13
15
17
18
AM Opportunities and Limitations by Sub-sector
Cardiovascular
Corrective Lenses
Dentistry
Dialysis
Diagnostic Imaging
Hearing & Hearing Devices
Hospital Supplies
Incontinence & Ostomy
In-vitro Diagnostics
Orthopaedics
Radiation Therapy
Wound Care
Other Areas
Japan - Implications for MedTech Space
Pharma Companies
20
20
21
22
23
24
25
26
27
27
27
29
30
31
32
33
Limitations to Opportunities
Regulatory Issues
State of Technology
Design and Training
34
34
34
35
Companies Currently Involved
3D Systems Corporation
Arcam
ExOne
Organovo
Stratasys
36
36
36
36
36
37
3
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Executive Summary
Over the past five years falling R&D productivity and government
austerity measures have had a negative impact on organic growth
and margins for the sector. In this Blue Paper, we explore whether 3D
printing can increase R&D productivity through innovation and drive cost
efficiencies going forward.
While 3D printing is not new, improvements in printers and a
growing portfolio of materials is likely to make the technology
much more relevant. We believe the MedTech sector could be one of
the greatest beneficiaries of the technology, with clear patient and
manufacturing benefits.
While we acknowledge that 3D printing is unlikely to have a
material near-term growth or valuation impact on the MedTech
sector, we aim to provide a detailed guide as to which device
sub-segments are naturally more suited to the opportunity. We
conclude that early-stage segments with high revenue or cost-savings
opportunities are best placed. These include Dentistry (focus on
restorative), Orthopaedic Reconstructive (hips, knees and small joints),
Orthopaedic Trauma (cranio maxillofacial, nails) and Prosthetics. For
investors willing to consider a two- to five-year view, we would also
include categories such as Corrective Lenses, Advanced Wound Care
and Stents. We look at the companies under our coverage, and highlight
which, from a fundamental perspective, we think are more likely to
benefit.
implementing whatever features are needed to optimise the
functionality of the device.
Patient Benefits
For patients, we see the following potential advantages (some
of which are already in place):
Diagnosis & Therapy Choice – by using digital
diagnostic imaging in conjunction with 3D printing, models
can be used to help physicians diagnose disease.
Customised Medical Devices – the ability to custom
make patient-specific medical devices is likely to broaden.
This may include more customised solutions in dentistry,
corrective lenses and orthopaedics.
Entirely New Solutions – AM may provide entirely new
options for patients, such as organ replacement.
Manufacture Benefits
We see the following potential advantages for manufacturers,
with some, again, already in practice:
Low Volume, High Value – most medical devices
produced are relatively low volume, but sale value is high.
Furthermore, most devices are small, with design
complexities, for which small-scale AM manufacturing
systems are especially suited.
Reduce Inventory – AM offers the opportunity to reduce
working capital by moving towards a ‘just-in-time’
production system.
Reduce Waste – in some MedTech areas, materials used
in production are expensive, with high levels of scrap. To
make devices with precision could provide cost savings.
Other Savings – AM can manufacture an entire product in
a single step by eliminating assembly stages. This
eliminates tooling costs and should reduce labour costs.
Design Complexity – AM allows for design flexibility, and
thus products can have a higher level of complexity. AM
also opens up a multi-material possibility for improved
microstructure.
New Growth Opportunities – AM should open up entirely
new growth opportunities over the medium to long term,
potentially including organ replacement using cell printing.
What is 3D Printing?
3D printing is often referred to as additive manufacturing (AM),
which has been defined by the American Society for Testing
and Materials (ASTM) in F42 as the process of joining
materials to make objects from 3D model data, usually layer
upon layer. Wohlers Report 2013 estimates that the worldwide
AM industry for all primary products and services grew by 29%
to $2.2 billion in 2012. It also estimates that revenues from AM
systems and materials were ~$1bn last year, up 20%. AM
services seem to be the larger segment at $1.2bn, up 37%. It is
unclear, what the size of medical device segment is of the
aforementioned $2.2bn market; although Wohlers Report 2013
estimates ~16%.
Why is MedTech Suited to 3D Printing?
We believe AM may play a significantly more important role in
MedTech in future, thanks to the ability to provide personalised
medicine and improved healthcare. Historically, methods were
adopted to push “design to suit manufacturing” barriers. With
AM, the focus is on “manufacturing for designs” and
4
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
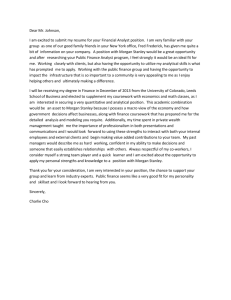
Patent Filings – Suggests Strong Future
The second highest number of patent filings involving 3D
printing has been in the medical field, at 29% (after
manufacturing at 38%). Based on patent applications, medical
has ranked first over the past two years. The patent activity, in
our view, is indicative of the suitability of AM technology for the
MedTech industry, and we believe it could be a strong
beneficiary over the medium term.
Exhibit 1
3D Patent Applications – Medical Dominates
Sector
2011
Medical
34%
38%
Manufacturing
33%
38%
Technology
18%
15%
Materials
10%
6%
Tooling
2%
2%
Business methods
1%
1%
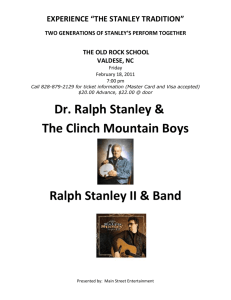
Where Does The Opportunity Lie?
We have developed an evaluation framework to help indentify
MedTech areas that could benefit most from the AM opportunity.
The framework is relatively simple, and looks at ‘Early vs. Late
Stage’ and ‘Size of Opportunity’. The sweet spot, in our view, is
‘Early Stage’ medical technology, which relates to devices that
should benefit from AM over the short term.
Exhibit 2
Faster Access to AM Opportunity in Early-Stage
MedTech – Early, Mid & Late Cycle Comparison
Mid Stage (2-5 Years)
Which Companies Could Benefit the Most?
From a European perspective, we believe Smith & Nephew
could be one of the main beneficiaries of advances in AM
technology, with material exposure to Orthopaedic Recon and
Trauma. We use S&N in an illustrative example below.
2012
Source: Castle Island Co, Morgan Stanley Research
Early Stage (Now)
Exoskeleton, Orthopaedic Spine and General Capital
Equipment. The most significant longer-term opportunity
relates to the potential printing of spare body parts, such as
kidneys or hearts, which according to many commentators is
over 10 years away.
Late Stage (+10 years)
3D Models
Corrective Lenses
Advanced Wound Care
Bench-top Testing
Cochlear Implants
Blood Vessels
Crowns & Bridges
General Capital Equipment Bone replacement
Dental Implants
Incontinence
Dialysis (kidney replacement)
Dentures
Ostomy
Aesthetics
Diagnostic Imaging
Stents
Heart Valves
Exoskeleton
Heart Replacement
Hearing Aids
Diabetes (pancreas replacement)
Orthodontics
Orthopaedic Recon
Orthopaedic Spine
Orthopaedic Trauma
Prosthetics
Source: Morgan Stanley Research
An equally important investment consideration is the size of the
opportunity. Given that AM can offer both revenue and cost
savings, we include both in our assessment. Sub-segments
that we think are most attractive for AM include Dentistry,
Orthopaedic Recon, Orthopaedic Trauma and Prosthetics.
Least attractive areas include Cochlear Implants, Hearing Aids,
Limitations to Opportunities
We see three major limitations to broad and rapid uptake of AM
in MedTech. 1) The existing regulatory framework will need to
evolve with emerging technology, which adds a layer of
uncertainty. 2) While there have been strong gains in AM in
recent years, meaningful technology shortcomings remain. 3)
AM is driven by software, which is typically complex and
provides a barrier for broader adoption of the technology.
Smith & Nephew: Illustrative Example
We believe the orthopaedics sector could benefit from AM via lower
inventory (manufacturing a customised implant ‘just in time’) and reduced
cost of sales. Costing data from AM technology supplier Arcam suggests
a hip can be made for 35% less than conventional methods. In our Smith
& Nephew example, we assume the company can cut its Orthopaedics
COGS by 20% and improve inventory turn by 15%.
COGS – we estimate that a 25% reduction in COGS would expand the
free cash flow yield from 8.4% to 11.4% in FY16. The 3.1% improvement
equates to a ~35% increase in free cash flow yield. We assume that
incremental capex on AM technology can be offset by a fall in capex on
the traditional manufacturing process.
Inventory Turn – a 15% improvement in inventory turn boosts Smith &
Nephew’s free cash flow yield (including the COGS benefit) by a further
0.3 percentage points to 11.7% in FY16e. The 3.4% improvement is a
41% increase in the cash yield.
Based on a simplistic DCF model, the increase in free cash flow
generation adds up to 35% to Smith & Nephew’s valuation. Our
discussions with the company suggests that it is exploring the
opportunities AM has to offer over the medium to long term. Ultimately,
the impact 3D printing has on S&N’s financials depends largely on how
fast it can implement the technology available.
5
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 3
MedTech – Sector and Company Overview
Segment
Companies
Cardiovascular Sorin
Formal Strategy
Opportunity or Threat
Aware of technology Accelerates design
and using it where process
appropriate
Aware of technology May be more of a threat
Current Usage
Pros and Cons
Lack of accuracy, absence of
implantable polymers limits
opportunity
Lack of accuracy limits the
manufacture of customised
corrective lenses
Not relevant
Corrective
Lenses
Essilor
Dialysis
Fresenius Medical
Care
Nobel Biocare,
Straumann
Aware of technology Not relevant
GN, Sonova, William
Demant
Strong user of
technology
Good for custom shell
manufacturing
Hospital
Fresenius SE
Supplies
Incontinence & Coloplast
Ostomy
Not relevant
Not relevant
Aware of technology Not relevant
Small amount of
prototyping
Too slow
In-vitro
Diagnostics
Orthopaedics
bioMerieux, Diasorin
Aware of technology Not particularly relevant
Not particularly relevant
Smith & Nephew
More of an opportunity
than threat
Prosthetics
Ossur
More of an opportunity
than threat
Prototyping and
design
Radiation
Therapy
Elekta
Aware of technology
and exploring
opportunities
Aware of technology
and using it where
appropriate
Aware of technology
Small amount of
prototyping
Customised
cutting blocks
Wound Care
Smith & Nephew
Dentistry
Hearing Aids
Aware of technology More of an opportunity
than threat
Not particularly relevant
Aware of technology More of an opportunity
than threat
Eventual Significance
May eventually print artificial
heart valves, hearts and
blood vessels
May eventually be able to
print corrective lenses and
frame in one go
Small amount of
May eventually print artificial
prototyping
kidneys
Lack of accuracy and speed May eventually become the
Prosthetic
standard of care for
prototyping and for ceramic crowns and
‘chairside’ systems
bridges
temporaries
In-the-ear hearing Good accuracy, simple, cost May be able to print a large
aids
effective
amount of a hearing aids,
including electrics, in one go.
Smaller batteries.
Not relevant
Not relevant
Not relevant
Prototyping for
heart valves and
CRM housing
Little
Customisation, just-in-time
production, lower inventory
and COGS reduction
Increased speed to market
May eventually be able to
print body parts to get around
the medical condition
Not that relevant
Custom implants may
become standard
May be able to move into full
production use as the
technology develops
Stereotactic
Not particularly relevant
May eventually be able to
masks and shells
remove cancerous tissue and
replace with artificial tissue
Little
Printing skin could help with For complex wounds such as
complex wounds
diabetic foot ulcers or burn
victims, printing tissue could
provide additional solutions
Source: Company Data, Morgan Stanley Research
6
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Medical Devices – AM Could Drive Innovation and Cost Savings
Where we are today:
– What is 3D printing
– Market size
– Why is MedTech suited
– Printing technologies
– Materials available
– Drawbacks
– Patent development
What is 3D Printing?
3D printing is often referred to as additive manufacturing (AM),
which has been defined by the American Society for Testing
and Materials (ASTMN) in F42 as the process of joining
materials to make objects from 3D model data, usually layer
upon layer. Exhibit 4 provides an illustrative example of a 3D
printer creating a human heart.
Exhibit 4
3D Printer – Illustrative Example
ASTM is a globally recognised leader in the development and
delivery of international voluntary consensus standards, and
today some 12,000 ASTM standards are used around the
world.
Market Size
Wohlers Report 2013 estimates that the worldwide AM industry
for all primary products and services grew by 29% to $2.2bn in
2012. It also estimates that revenues from AM systems and
materials were ~$1bn in 2012, up 20% year on year. AM
services seem to be the larger segment at $1.2bn, up 37%.
There is also a secondary market, which includes tools
produced directly from AM technology. Over a longer period,
Wohlers Report 2013 estimates that the AM industry was
around $500mn in value in 2000, which equates to a CAGR of
14% for the period ended 2012. At present, AM is being widely
used to build physical models, whether prototype or final,
patterns, tooling components and production parts in a wide
variety of materials. It is unclear, what the size of medical
device segment is of the aforementioned $2.2bn market;
although Wohlers Report 2013 estimates it at ~16%.
Why is MedTech Suited?
We believe AM could become very relevant for Medical
Technology as it can provide better healthcare through
personalised medicine and improved patient outcomes.
Historically, methods were adopted to push “design to suit
manufacturing” barriers, while with AM it is more about
“manufacturing for designs”, implementing whatever feature is
needed to functionally optimise the device.
Patient Benefits
For the patients, we see the following potential advantages
(and in some instances, this is already happening):
Diagnosis & Therapy Choice – by using digital
diagnostic imaging technology in conjunction with 3D
printing, models can be used that will help physicians to
diagnose disease. This can be especially relevant with
more complex structural problems, such as those found in
heart disease or orthopaedic spine.
Customised Medical Devices – the ability to
custom-make patient-specific medical devices is likely to
broaden going forward. This may include more customised
solutions in areas such as dentistry, corrective lenses and
orthopaedics.
Source: Christopher Barnatt, explainingthefuture.com
7
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Entirely New Solutions – 3D printing may someday
provide entirely new options for patients such as organ
replacement, and could open up entirely new markets in
areas such as cardiology, diabetes and dialysis.
Manufacturer Benefits
While 3D printing in MedTech is still in its infancy, we feel the
ability to offer more patient-specific solutions could prove a
disruptive technology for some companies and an opportunity
for others. Later in the report, we provide more detail on how
relevant 3D printing is today among various sub-sectors and
where the technology may be heading going forward.
For medical device manufacturers, we see a number of
opportunities (and in some instances this has already started):
Low Volume, High Value – most medical devices
produced are relatively low volume/small scale, but the
value generated from the sale is relatively high.
Furthermore, most medical devices are small, with design
complexities, for which small-scale AM manufacturing
systems are especially suited. While we believe this to be
true for most areas of MedTech, we observe two
exceptions: custom-fit hearing aids and dental copings for
crowns and bridges, where many million units are
produced annually.
Reduce Inventory – medical device companies typically
carry high levels of stock, among other things to cater for
the different sizes needed. The opportunity to move more
towards a ‘just-in-time’ system and reduce working capital
is interesting, especially in areas such as orthopaedics.
We would argue that working capital can be reduced
materially with AM over time.
Reduce Waste – in some areas of medical devices,
materials used in the production process are expensive,
with high levels of scrap. The ability to make medical
devices precisely could provide cost savings opportunities,
especially with faster and more efficient AM technology.
Other Savings – AM can manufacture an entire product in
one single step by eliminating assembly stages. This
eliminates tooling costs and should reduce labour costs.
Design Complexity – AM allows for great design flexibility
and thus products can be designed with a higher level of
complexity. This, for instance, could include the production
of more porous surfaces, which are preferred in
orthopaedic implants and that may not be possible with
current manufacturing techniques. Furthermore, AM could
offer multi-material possibilities when using powdered
material; this functionality takes advantage of different
materials’ properties to improve the microstructure.
New Growth Opportunities – AM could open up entirely
new growth opportunities over the medium to long term,
including organ replacement using cell printing.
Example of Cost Effective Production
Our review of the literature shows that more and more medical
technology companies are recognising the benefits of AM. As an
example, we cite Andreas Hettich GmbH, a manufacturer of centrifuges,
where the process is used for product development and production. As a
result, the company was able to increase the value of its products and
lower production costs. The typical production volume of the company’s
centrifuges is between 10 and 1,000 units per year. Hettich invented and
patented a new type of centrifuge that enables the sedimentation and
separation of blood components in one device. The ROTOMAT consists
of a drum motor with six containers and drip trays. The containers have a
complex geometry and are subject to high rotational speeds with
acceleration forces up to 1,200g. Manufacturing the container
components using conventional methods required complex tools and
time-consuming assembly procedures. After a comprehensive technical
evaluation, Hettich decided to change its method for producing centrifuge
housings, using AM. While the cost of producing the modified component
was slightly higher, the company saved the costs for an entire set of tools.
Reduced assembly and logistics costs provided further cost savings. If
required, AM enables further design modifications or product variants to
be implemented quickly at minimal cost.
Printing Technologies
While we do not intend to go into the specific details of various
technologies available1, we provide a brief overview of the
main technologies available today. A useful guide is the various
processes highlighted by the ASTM F42 committee and their
key documents such as F2792 “Standard Terminology for
Additive Manufacturing Technologies”:
1
For more detail, please see ‘Don’t Believe (All) The Hype’, by Ben Uglow, September 5, 2013
8
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 5
3D Printing Processes
Process
Binder Jetting
Directed Energy
Deposition
Material Extrusion
Material Jetting
Description
A liquid bonding agent is selectively deposited to join
powder materials
Focused thermal energy is used to fuse material by
melting as they are being deposited
Material is selectively dispensed through a nozzle or
orifice
Droplets of build material are selectively deposited
Sheet Lamination
Sheets of material are bonded to form an object
Vat
Photopolymerisation
Powder Bed Fusion
Liquid photopolymer in a vat is selectively cured by light
activated polymerization
Thermal energy selectively fuses regions of a powder
bed
Source: ASTM, Morgan Stanley Research
From our review of medical device literature, the more popular
MedTech processes include stereolithography for medical
models, whereby a controlled laser is used to cure a
photopolymer resin to shape the product from a 3D CAD
model. Other popular methods include using a laser to heat
and melt fine particles in a powder bed; dental companies
prefer to use this laser system because of the fine, detailed
nature that is possible. Some systems use an electron beam as
the energy source as this is usually faster, but the finish is less
compelling. With some medical devices such as orthopaedic
implants, a rough surface is desired, which is why some
manufacturers have selected electron beam melting (EBM).
While AM can show feature detail and surface finish similar to
metal castings, it cannot match the surface quality of
CNC-machined parts.
Materials Available
Materials currently available for 3D Printing fall into three high
level categories: plastics, metals and ceramics or derivatives.
Plastics
Plastics appear to be the most popular material for 3D Printing
and can be selected for the functional need in medical devices.
Properties to consider include biocompatibility, strength,
colour/transparency and sterilisation properties. Plastics can
typically be classified into two groups: thermoplastics or
thermoset plastic. Thermoplastics retain their properties and
can be repeatedly melted, hardened and re-melted. We would
argue that in many areas of medical device usage, the property
of re-melting is less useful. With thermoset plastics the object is
permanently set and cannot be re-melted.
Metals
The use of metals has been broadening over the years, and
medical device suppliers can chose from a wide range of
inputs. Historically, the most used metals from a
biocompatibility perspective have been titanium or titanium
alloys, cobalt-chrome and stainless steel, all of which are
available. Other materials available but not used widely in
medical devices are aluminium alloys, nickel-based alloys,
copper-based alloys, gold and silver.
Most 3D Systems that build metal parts melt the materials that
achieve close to 100% density. The topic of density is important
since less dense material is more prone to fracture toughness
and may fatigue earlier. This is an important consideration for
implantable medical devices that are load bearing, such as in
orthopaedic trauma.
Ceramics
Ceramic materials and blends are offered by a number of
manufacturers. From a MedTech perspective, biocompatible
materials are perhaps of the higher interest, given their
suitability for internal use. For instance, ceramics are currently
used in joint replacement.
Other Materials
New biocompatible materials such as bio-stable resins and
bio-degradable composites (comprising polyester/polyether
oligomers) can be used easily in AM machines. Other materials
that are available include polymeric materials such as PEEK
(high performance thermoplastic), which have been used in
orthopaedic spine for some time, or FRC (fiber reinforced
composite). The FDA very recently approved the first
non-metal 3D printed polymer for human implantation, namely
the OsteoFab Patient Specific Cranial Device from Oxford
Performance Materials. In this instance, an MRI scan is used to
acquire the exact shape of the patient’s skull in order to print
the best-fit implant.
Drawbacks
While AM can offer a wide range of benefits, there are several
weaknesses. At a high level this includes material limitations
(although most materials needed in medical devices are now
available), accuracy (room for improvement), roughness
(requires an additional process to produce smooth surfaces),
cost and speed of production, which may limit the uptake over
the medium term. We foresee improvements in all of these
areas over the medium term.
Patent Development – Medical Right Up
There
Data collected by Castle Island Co. and Wohlers shows that
the second largest AM related patent filings have been in the
Medical field at 29%, after Manufacturing at 38% (see Exhibit
6). In terms of patent applications (see Exhibit 7) Medical has
ranked no.1 for the past two years. This patent activity, in our
view, is indicative of the suitability of AM for MedTech industry,
and we expect the sector to be a key beneficiary of 3D Printing
technology over the medium term.
9
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 6
3D Printing Patents Issued – Medical Ranks 2nd Highest After Manufacturing
Sector
2006
2007
2008
2009
2010
2011
2012
Manufacturing
41%
37%
43%
41%
34%
34%
38%
Medical
24%
16%
18%
17%
25%
31%
29%
Technology
24%
27%
19%
26%
26%
22%
19%
Materials
7%
14%
14%
12%
10%
9%
10%
Tooling
1%
3%
2%
1%
4%
3%
2%
Software
1%
1%
1%
1%
0%
1%
1%
Business methods
1%
1%
1%
1%
1%
0%
1%
Utility
1%
0%
3%
1%
0%
0%
1%
Source: Castle Island Co. Wohlers Report 2013
Exhibit 7
3D Printing Patent Applications – Medical Ranks Top, Ahead of Manufacturing
Sector
2006
2007
2008
2009
2010
2011
Medical
22%
25%
32%
28%
35%
34%
2012
38%
Manufacturing
45%
40%
36%
37%
33%
33%
38%
Technology
16%
19%
19%
22%
17%
18%
15%
Materials
12%
11%
9%
9%
12%
10%
6%
Tooling
2%
2%
2%
0%
0%
2%
2%
Business methods
2%
1%
1%
2%
1%
1%
1%
Utility
1%
2%
1%
1%
1%
1%
1%
Software
1%
1%
0%
1%
1%
1%
0%
Source: Castle Island Co. Wohlers Report 2013
Exhibit 8
3D Printing – Process / Material Matrix
Material extrusion
Polymers, polymer blends
Composites 22
Metals
Graded/hybrid metals 3 3
Ceramics
Investment casting patters
Sand moulds and cores
Paper
√
√
Material jetting
Binder jetting
Vat
Photopolymerisation
√
√
√
√
√
√
√
√
√
√
√
√
√
√
Sheet lamination
√
1
√
√
Powder bed fusion
√
√
√
Directed energy
deposition
√
√
√
√
√
√
Source: Wohlers Associates. (1) The sheet lamination system from Solido, which is longer available commercially, used PVC. (2) Includes filled materials. (3) Hybrid materials are most typically
produced using ultrasonic additive manufacturing. Graded materials are produced with directed energy deposition systems.
10
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Where Do Opportunities Lie?
To maximise returns from emerging AM MedTech opportunities, we
believe it is important to be selective when choosing the sub-segments to
invest in. To rank the most compelling sub-sectors, we provide a
framework that looks at early versus late-stage product cycles and the
size of the opportunity. Early-stage medical devices should give
investors access to the 3D benefits more quickly, while the size of the
opportunity helps to determine the relevance to the sub-sector at hand.
We conclude that the areas investors should be focusing on are
Dentistry (focus on restorative), Orthopaedic Reconstructive (hips,
knees and small joints), Orthopaedic Trauma (cranio maxillofacial,
nails) and Prosthetics. For investors who are also willing to consider a
two- to five-year view, we would also include categories such as
Corrective Lenses, Advanced Wound Care and Stents.
Evaluation Framework
Our evaluation framework aims to identify MedTech areas that
could benefit the most from the AM opportunity. The framework
looks at two key characteristics:
Early versus Late Stage – we believe that medical
devices can be categorised as “early” or “late” stage.
We feel this categorisation is important since companies
that operate in the “early stage” are likely to benefit from
the potential AM printing opportunity sooner; and
Size of Opportunity – of equal importance is the size of
the AM opportunity for the medical device category. We
define the opportunity as broadly as possible and include
revenues, costs and working capital benefits. We feel this
broad definition is appropriate given that AM has the
potential to provide benefits to a company’s P&L, Balance
Sheet and Cash Flow. Given that AM in MedTech is still in
its infancy, making this prediction requires a degree of
guesswork.
Early Stage – Opportunity is Now
We believe early-stage medical technology relates to devices
that can benefit from AM over the short term, with no material
bottlenecks. This could relate to many different factors, such
as: a] availability of appropriate, reliable and efficient AM
machines and materials to make the medical device; b] a
benign regulatory environment that allows for quick product
approval times – as a general rule this applies to medical
devices that undergo a 510k approval process (equivalent)
versus something that is substantially new and requires a PMA;
and c] not R&D intensive nor requiring long-term clinical trials.
In our view, examples of early-stage medical device categories
are dentistry (crowns, bridges, implants, orthodontics) where
prosthetic teeth can be printed to suit the patient’s needs,
hearing aids where customised shells for in-the-ear solutions
can be made, Orthopaedic hips, knees, trauma and spine.
Other areas include Diagnostic Imaging, 3D models, Bench-top
Testing and Incontinence and Ostomy.
Mid Stage – Opportunity Increases Over Next 2-5
Years
We define the mid stage as an opportunity that is not as
immediate as early stage and requires another two to five years
of investment before the opportunity materialises. Areas that
may fall into this category include Corrective Lenses, Cochlear
Implants, General Capital Equipment and Stents.
Late Stage – Opportunity Likely to Take +10 Years
This relates to medical devices where there are material
bottlenecks to get AM-derived products to the market. For
example, in some areas current AM technology is inadequate –
including having the appropriate material. We would argue that
most of the categories in this segment relate to the organ
replacement opportunity, which appears still in the embryonic
stage, with many more years of costly research ahead before a
reliable and functional product is available. Once a reliable
product has been created, regulatory scrutiny is likely to be
exceptionally high, requiring large clinical trials over many
years to demonstrate that the technology is safe. Examples of
late stage opportunities include Blood Vessels, Bone
Replacement, Aesthetics, Kidney Replacement, Heart Valves
and total Heart replacement, Pancreas and Liver replacement.
Little Opportunity
Areas where we think AM will have little direct impact include
Biosciences, Clinical Nutrition, Defibrillators, Injectable
Generics, IVD, Pacemakers, Radiation Therapy and
Traditional Wound Care. There are likely to be indirect impacts,
which we discuss below, such as perhaps a reduced need for
defibrillator or pacemakers should it be possible to print fully
functioning 3D printed hearts.
Stocks to Focus on – Early vs. Late Stage
Among the stocks under coverage, we feel the areas that are
likely to be impacted the earliest by AM are:
11
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 9
Early, Mid & Late Cycle Comparisons
Early Stage (Now)
Mid Stage (2-5 Years)
Late Stage (+10 years)
Little Opportunity
3D Models
Bench-top Testing
Crowns & Bridges
Dental Implants
Dentures
Diagnostic Imaging
Exoskeleton
Hearing Aids
Orthodontics
Orthopaedic Recon
Orthopaedic Spine
Orthopaedic Trauma
Prosthetics
Corrective Lenses
Cochlear Implants
General Capital Equipment
Incontinence
Ostomy
Stents
Advanced Wound Care
Blood Vessels
Bone replacement
Dialysis (kidney replacement)
Aesthetics
Heart Valves
Heart Replacement
Diabetes (pancreas replacement)
Biosciences
Clinical Nutrition
Defibrillators
Injectable Generics
IVD
Pacemakers
Radiation Therapy
Traditional Wound Care
Source: Morgan Stanley Research
Dentistry – in a European context it is Nobel Biocare and
Straumann; in a US context Dentsply2 and Invisalign.
Hearing Aids – in a European context it is GN Store Nord,
Sonova and William Demant.
Orthopaedics – in a European context it is Smith &
Nephew. US companies include Stryker and Zimmer and
to some extent Medtronic3.
3D Models – there are no stocks under our coverage that
are noteworthy.
Size of Opportunity – Relative Analysis
We feel an equally important investment consideration as
“Early vs. Late Stage” medical devices is the size of the
opportunity. When defining the “Size of Opportunity” we make
the following important points:
2
3
Relative Size – when sizing the opportunity we are
referring to the opportunity relative to the existing market
of a company today and not the absolute opportunity.
Revenue and Costs – on offer are both revenue and cost
savings opportunities. In some instances, the ability to
reduce costs may be more significant than being able to
generate revenues from a new innovative product line.
Although AM is still relatively new, we believe the greater
opportunity for medical devices may be on revenues rather
than costs.
Disruptive Risk – in our forecasts, we are assuming that
all incumbents in the various sub-segments will take
advantage of the AM opportunity. In reality, some
companies will be late adopters and as such the AM
opportunity could turn out be a risk, especially if new
entrants offer disruptive products. We address disruptive
risk later in the report.
High Opportunity – Score of 8 or above
We have defined High Opportunity, to which we apply a score
of 8/10 or above, as including heart replacement, crowns &
bridges (moving towards a customised patient-specific
system), dialysis (kidney replacement compared to
hemodialysis or peritoneal dialysis), heart valves (rather than
using animal-based or mechanical valves), diabetes (pancreas
replacement rather than taking insulin shots) and bone
replacement (part of Orthopaedics). These relate to virtually all
revenue opportunities from improved technology. Within the
high opportunity segment, we feel cost savings are likely to
play less of a role.
Medium Opportunity – Score of 5-7
We score medium opportunity at 5-7/10 and this includes
orthopaedics recon (hips, knees, small joints), blood vessels
(for use in occluded vessels or for transplants), corrective
lenses (e.g. printing the frame and lens in one go), dentures,
aesthetics, orthopaedic trauma (including CMF to repair
missing parts of the skull), advanced wound care (especially
printing living skin tissue for burns, diabetic ulcers and pressure
sores), prosthetics (customised solutions for people who have
lost upper and lower limbs) and stents. For the medium-term
opportunity, we feel the benefits are likely to be a combination
of product innovation and cost savings.
Covered by Steve Beuchaw
Covered by David Lewis
12
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Probably Irrelevant
Exhibit 10
Size of Opportunity
Segment
Size of Opportunity (1 - low; 10 = high)
Heart Replacement
Crowns & Bridges
Dialysis (kidney replacement)
Heart Valves
Diabetes (pancreas replacement)
Bone replacement
Blood Vessels
Orthopaedic Recon
Corrective Lenses
Dentures
Aesthetics
Orthopaedic Trauma
Advanced Wound Care
Prosthetics
Stents
Dental Implants
Exoskeleton
Orthodontics
Bench-top Testing
Diagnostic Imaging
General Capital Equipment
Orthopaedic Spine
3D Models
Cochlear Implants
Hearing Aids
Incontinence
Ostomy
Biosciences
Clinical Nutrition
Defibrillators
Injectable Generics
IVD
Pacemakers
Radiation Therapy
Traditional Wound Care
10
9
9
9
9
8
7
7
6
6
6
6
5
5
5
4
4
3
2
2
2
2
1
1
1
1
1
0
0
0
0
0
0
0
0
Source: Morgan Stanley Research estimates
Low Opportunity – Score of 4 or below
We rate low opportunity medical devices as four or lower out of
10, which in our view includes dental implants (e.g.
customisation or patient specific implants may not be that
relevant), exoskeletons (casts for broken bones, especially if
they require digital imaging), orthodontics (customisation is
useful, but may be more of a niche product), bench top testing,
diagnostic imaging (CT, MRI, PET), general orthopaedic spine
(pedicle screws, plates, spacers), 3D models, hearing aids
(shell manufacturing benefits from 3D printing have to a large
degree already been exhausted) and incontinence & ostomy
(customisation less relevant). Similar to the “medium
opportunity”, we feel the opportunity is a combination of
product innovation and cost savings.
We also have a category of sub-segments where AM is unlikely
to have a noticeable impact, which includes biosciences (blood
plasma, IVIG, Factor VIII), clinical nutrition, IVD, cardiac rhythm
management (pacemakers and defibrillators), radiation
therapy and traditional wound care.
Making the Selection
To help identify sub-segments within medical devices that can
meaningfully benefit from AM, we use a scatter diagram (see
Exhibit 11) that plots “Early vs. Late Stage” against the size of
“Size of Opportunity”. We see the most attractive combination
as “Early Stage” with “High Opportunity”; the opposite holds
true for the least attractive category, which we believe is “Late
Stage” with “Low Opportunity”.
Most Attractive Sub-segments
These segments include dentistry (crowns, bridges, dentures),
orthopaedic recon, orthopaedic trauma, and prosthetics. While
more details are provided later in the report, we highlight
orthopaedic reconstructive as a brief example, where
customised hip and knee joints in conjunction with lower
manufacturing costs and reduced working capital could provide
real upside for investors over the short to medium term.
Least Attractive Sub-segments
These segments include cochlear implants, hearing aids,
exoskeleton, orthopaedic spine and general capital equipment.
For these segments, we do not expect AM to have any material
benefits with respect to revenues or cost savings. For example,
within hearing aids AM has been used for the custom shell
manufacturing process for well over five years, and thus the
cost savings opportunity is already reflected in the P&L. In
general capital equipment, we see it as unlikely that AM will
provide product innovation or lower production costs for areas
such as hospital beds, heart-lung machines, anaesthesia
machines and so on.
Interesting Areas
We also highlight some potentially interesting areas that may
have huge potential but are subject to high levels of risk and
long dated. This category is typically associated with 3D
printing of spare body parts in the future, such as kidneys for
dialysis patients, pancreases for diabetics, heart valves, bones,
or perhaps even entire functioning hearts.
13
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 11
Medical Devices: Stage of Cycle vs. Size of Opportunity
Heart Replacement
10
MOST ATTRACTIVE
9
Heart Valves
Pancreas Dialysis
Crowns & Bridges
8
Bone Replacement
7
Size of Opportunity
Orthopedic Recon
Blood Vessels
Corrective Lenses
6
Dentures
Esthetics
Orthopedic Trauma
5
Advanced Wound Care
Stents
Prosthetics
4
Dental Implants Exoskeleton
3
Orthodontics
Orthopedic Spine
2
Diagnostic Imaging
Bench-top Testing
1
General Capital Equipment
Cochlear Implants
Incontinence & Ostomy
Hearing Aids
LEAST ATTRACTIVE
3D Models
0
0
1
2
Early Stage
3
4
5
Mid Stage
6
7
8
9
10
Late Stage
Source: Morgan Stanley Research estimates
14
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Example of AM Benefits
Costing Comparison
To provide more colour on how 3D printing could impact the
MedTech sector, we show an illustrative example of the cost
savings opportunity in Orthopaedics, using Smith & Nephew as
a case in point. As we highlighted earlier in the report, we
believe AM could provide two major benefits for the
orthopaedic industry:
When comparing costing of 3D printing we cite a study on “Application of
electron beam melting to titanium hip implants” by M Cronskär et al from
the Proceedings of the 19th International DAAAM Symposium 2008.
While the data is some years old, it nevertheless provides a useful insight
into the economic feasibility of using rapid manufacturing (in this instance
Arcam EBM technology) for implant manufacturers including such issues
as material consumption, manufacturing time and associated costs in
comparison to the conventional manufacturing methods. In this study,
the comparison has been done in cooperation with a Scandinavian
company (CC) that develops and manufactures customised hip stem
prosthesis using CNC methods. This was compared to seven solid
customised hip stem prosthesis designed by the CC at its site. In the
study, material, file preparation and manufacturing costs are taken into
account, while all other costs were taken to be the same in the two cases.
The results showed a cost comparison that was favourable for EBM; the
EBM-based manufacturing costs constituted about 65% of the
conventional costs. The table below provides relative cost comparisons:
Inventory Management – being able to manufacture a
customised implant on demand at short notice should
allow Smith & Nephew to lower its high inventory levels
and release cash to shareholders. While we acknowledge
that its customised cutting block solution of Visionaire
(also 3D printed) had the potential to offer similar benefits,
the impact on inventory so far appears immaterial.
Cost Reductions – data from Swedish-based Arcam
compared costing data of producing reconstructive
implants (in this instance the acetabular cup) using
electron beam melting with Ti-6AL-4V instead of the
conventional method of cast metal and forging using CNC
machines. The cost using its EBM technology was
€40-103 per cup (varies with cup size from 44 to 66) or a
€20-25 saving over the machined products. This reflects
less production waste (when machining 60-70% of original
material is scrapped) and no secondary process of
attaching the porous coating, which can cost €30-60 per
implant. For more detail on the cost savings opportunity,
see grey box.
Illustrative Example of Cost Reductions – High Level
Scenario
In our high level Smith & Nephew example, we make the
following assumptions:
Ortho COGS Share – we assume that orthopaedics
makes up 50% of Smith & Nephew’s group COGS. We
understand that the gross margin for orthopaedics is
broadly comparable to the rest of the business units.
Ortho COGS Reduction – we assume AM can reduce the
company’s orthopaedic reconstructive COGS by 25%,
which is slightly below the cost analyses of Arcam, an AM
solutions provider. We also base our observations on a
number of different papers including “Application of
electron beam melting to titanium hip implants” by M
Cronskär.
Comparing Areas – EBM Costs in % of Conventional Way
Material
File Preparation
Manufacturing
Total Cost
15%
8%
130%
65%
The authors concluded that the study strongly indicates that the EBM
manufacturing process of the customised medical implants is
commercially viable. The best commercial performance can be realised
in customised manufacturing, where most savings are achieved in
material costs and pre-processing (file preparation). We would add that
this was based on EBM technology from five years ago, and since then
significant efficiency improvements have been made.
In Exhibit 12 we highlight that a 25% reduction in Smith &
Nephew’s orthopaedics COGS would result in 2016 free cash
flow yield expanding from an estimated 8.4% to 11.4%. The
3.1% point improvement equates to ~35% increase in free
cash flow yield – significant.
15
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 12
Smith & Nephew – Reduction in COGS
Dec Y/E (US$mn)
FY12A FY13E FY14E FY15E FY16E
Group Inventory
901 962 1,003 1,040 1,078
Ortho Share of Inventory
70% 70% 70% 70% 70%
Inventory - Ortho
631 674
702 728 755
Sales - Ortho
2,178 2,107 2,165 2,209 2,251
COGS % of Sales
25% 25% 25% 25% 25%
COGS
545 527
541 552 563
Inventory / Sales - Current
29% 32% 32% 33% 34%
Inventory Turn - Current
0.86x 0.81x 0.79x 0.77x 0.76x
Free Cash Flow - Current
740 681
741 819 884
COGS Reduction - Potential
-2% -10% -25%
Inventory Turn Improvement - Potential
0%
0%
0%
COGS
530 497 422
EBIT Savings (before Tax)
11
55 141
Tax Rate
32% 32% 32%
EBIT Savings (after Tax)
7
38
96
Inventory Turn
0.79x 0.77x 0.76x
Inventory
674 585 384
Inventory - Cash Released
28
90 201
Free Cash Flow - Potential
776 946 1,180
Free Cash Flow per Share - Potential
0.88 1.08 1.36
Free Cash Flow Yield - Old
6.9% 6.4% 7.0% 7.8% 8.4%
Free Cash Flow Yield - New
7.4% 9.1% 11.4%
Improvement
0.4% 1.3% 3.1%
Source: Company data, Morgan Stanley Research; e = Morgan Stanley Research estimates
N.B. Excess cash used for share buybacks
We assume that incremental capex on 3D printing technology
can be offset by lower capex in its traditional manufacturing
process.
Illustrative Example – Improving Inventory
Management
In our high level Smith & Nephew example, we make the
following assumptions:
Ortho Inventory Share – we assume that ortho inventory
makes up 70% of Smith & Nephew’s group inventory. We
understand from speaking to the company that
orthopaedics is a significantly more intensive inventory
business than the rest of its divisions.
Ortho Inventory Reduction – we assume that AM can
reduce inventory by as much as 15%. Since we could not
find any studies on this topic for guidance, our assumption
should be seen only as an educated guess. The reduction
in inventory comes from a move to a ‘just-in-time’
manufacturing process, allowing for a meaningful
reduction in the number of stock keeping units.
In Exhibit 13 we highlight that a 15% improvement in Smith &
Nephew’s inventory turn, in addition to the reduction in COGS,
would boost free cash flow yield by an additional 0.3
percentage point to 11.7% in FY16e, an increase of 41%.
Conceptually, we believe it should be possible to raise
inventory turnover higher still.
Exhibit 13
Smith & Nephew – Increasing Inventory Turn
Dec Y/E (US$mn)
FY12A FY13E FY14E FY15E FY16E
Group Inventory
901 962 1,003 1,040 1,078
Ortho Share of Inventory
70% 70% 70% 70% 70%
Inventory - Ortho
631 674
702 728 755
Sales - Ortho
2,178 2,107 2,165 2,209 2,251
COGS % of Sales
25% 25% 25% 25% 25%
COGS
545 527
541 552 563
Inventory / Sales - Current
29% 32% 32% 33% 34%
Inventory Turn - Current
0.86x 0.81x 0.79x 0.77x 0.76x
Free Cash Flow - Current
740 681
741 819 884
COGS Reduction - Potential
-2% -10% -25%
Inventory Turn Improvement - Potential
5% 10% 15%
COGS
530 497 422
EBIT Savings (before Tax)
11
55 141
Tax Rate
32% 32% 32%
EBIT Savings (after Tax)
7
38
96
Inventory Turn
0.83x 0.85x 0.87x
Inventory
610 468 239
Inventory - Cash Released
92 142 229
Free Cash Flow - Potential
840 999 1,208
Free Cash Flow per Share - Potential
0.96 1.14 1.39
Free Cash Flow Yield - Old
6.9% 6.4% 7.0% 7.8% 8.4%
Free Cash Flow Yield - New
8.1% 9.6% 11.7%
Improvement
1.0% 1.9% 3.4%
Source: Company data, Morgan Stanley Research; e = Morgan Stanley Research estimates
N.B. Excess cash used for share buybacks
Valuation Impact – up to 35% Higher
Based on a high level DCF model and other metrics, Smith &
Nephew’s incremental cash flow generation in our case study
results in a valuation that is up to 35% higher. This assumes
the company could implement the AM benefits in full by FY16e,
which is unrealistic. Our example is therefore illustrative only.
What Does Smith & Nephew Think?
Our discussion with Smith & Nephew suggests that it is
exploring the opportunities that AM could offer over the mid- to
long term. While the company did not give specific details, it
appears to agree with our view that AM is more of an
opportunity in orthopaedics and less so in endoscopy and
wound care. Indeed, its customised cutting block for knees,
Visionaire, is its first product line produced through AM.
Although we do not have any precise information, we believe
the company is exploring AM in orthopaedic trauma as well as
reconstructive. However, the impact 3D printing has on S&N’s
financials depends largely on how fast it can implement the
technology available.
16
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Opportunity or Risk?
1.
Increased Competition – availability of 3D printing
solutions may attract new competitors to the market that
are focused on producing customised crowns and bridges.
One of the solutions available would be EnvisionTEC, a
company that has the ability to build crowns or multiple unit
bridges for long-term temporaries. The materials available
include E-Dent, which is a glass-filled photopolymer. The
French company, Phenix Systems, offers a PXS & PXM
Dental that offers rapid manufacturing of dental prosthesis
using laser sintering of Cobalt-Chromium. In our view,
additional materials would need to be developed to make it
more suitable for long-term final restorations. For
companies such as Sirona4, this may provide increased
competition compared to its chair-side CEREC milling
system.
2.
Customers Internalise Production – similar to our
reasoning with dental implants above, we see it as
reasonable that more and more dentists may chose to use
chair-side 3D printing solutions to make customised
crowns and bridges. This improves customer service and
more of the value chain can be kept in house.
In our analysis so far we have assumed that all incumbents will
embrace 3D printing and thus that it equates to more of an
opportunity than a risk. However, in practice, the situation may
turn out very differently, with some incumbents being late
adopters, in which case AM may pose more of a risk than an
opportunity to the business model. In a worst case scenario,
AM could turn out to be disruptive technology. We highlight
some potential short-term and long-term examples below.
Short-term Examples – Dental & Orthopaedics
We look at two examples of short-term disruptive potential in
dentistry and orthopaedics.
Dental Implants – we believe AM could drive two potential
disruptions over the mid term:
1.
2.
Increased Competition – smaller implant manufacturers
may start to use 3D printing machines to come up with
unique dental implant or abutment designs that previously
were not possible with CNC machines. Larger companies
may not be as nimble as smaller ones in rapidly adopting
new technologies, held back by relying heavily on their
long-term clinical track record of well established
technologies. Furthermore, 3D printing may also open up
competition to high-margin product lines of
suprastructures (e.g. screw retained dentures, bars, etc),
which in the past was limited to only a number of dental
implant manufacturers, including Nobel Biocare, which
arguably has been one of the pioneers in this field.
Customers Internalise Production – as the dental
implant chains grow, such as US based ClearChoice (who
now has over 30 centres), the ability to print your own
dental implant solution could result in significant cost
savings; this may be initially more applicable for
abutments and later for implants. For instance, the gross
margin achieved by Nobel Biocare or Straumann on a
dental implant/abutment is estimated by Morgan Stanley
to be over 80%. As an example, an implant that is
purchased by a dental practitioner for $300 costs no more
than $50 to make and package (we think it could be as low
as $30). The ability for a large dental practice to print its
own implant could therefore be a very significant way of
increasing profitability, notwithstanding the regulatory
filings that need to be adhered to.
Orthopaedics – we believe 3D printing could cause three
potential disruptions over the medium term:
1.
Competition – it could add new entrants to the market.
New competition could come from a variety of different
competitors, including smaller medical device companies
setting up efficient 3D printing work stations, large medical
device companies wishing to enter the recon market in a
disruptive way, or hospitals/surgical centres printing their
own orthopaedic products.
2.
Manufacturing Decentralisation – with 3D printers being
small enough, hospitals and surgical centres may find it
compelling to print orthopaedic products themselves,
partly because it would enhance their ability to provide
customised implants for their patients. Effectively, the
industry could follow the dental prosthetics market,
whereby more and more dentists are using chair-side
systems to produce ‘just-in-time’ solutions, rather than
outsourcing the production to a dental lab or a centralised
manufacturing facility owned by third-party providers, such
as Nobel Biocare or Straumann. A decentralised
production trend would disrupt the long-established
practice of manufacturers such as Smith & Nephew,
building products centrally and shipping them to clients.
How decentralised manufacturing could work from a
Crowns & Bridges – we believe 3D printing could have two
potential disruptions over the medium term:
4
Covered by Steve Beuchaw
17
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
3.
regulatory perspective is unclear, and would require some
guidance statements from regulators such as the FDA.
Capacity – limited surgical capacity for doctors to cater for
the demand; and
Service Model – decentralisation of manufacturing may
also have implications for the salesforce service model in
the orthopaedics industry. Today, a sales person is very
much involved, among other things, in making sure the
implants are ready for surgery, lining up the devices neatly
on a trolley ready for the nurse to roll into the operating
theatre. In a decentralised model, internally produced
implants may be handled by the hospital staff.
Reimbursement – the cost may be prohibitive for
government payers or private health insurers for broader
application.
The aforementioned points may or may not happen, but they
provide food for thought as to what changes the orthopaedic
industry may see over the mid term.
An Example of Potential Long-term Change
Given that many researchers believe that printing functional
human organs on 3D printers is probably over 10 years away, it
is fair to suggest that this is more of a long-dated example of
AM being potentially disruptive to an incumbent business
model. But out of interest we highlight the hemodialysis
industry and its key player, Fresenius Medical Care, which
has gradually built up or acquired infrastructure to operate
3,160 clinics worldwide at end 2012, to provide blood cleaning
services for patients with end-stage-renal disease. This has
resulted in a net goodwill balance of $11.4 billion.
Our review of the AM literature suggests that there has been no
material disruptive technology that has changed the status quo
in the MedTech sector. However, we highlight one area where
AM has a material and rapid impact on workflow. In the hearing
aid sub-sector, AM has changed the way custom shells are
made for in-the-ear hearing aids.
Traditional Way of Hearing Aid Shell Manufacturing
Historically, most hearing aid companies used a 10-step
process to produce a custom shell, as shown in Exhibit 15
below (highlighted in Changing with the Times: Applying Digital
Technology to Hearing Aid Shell Manufacturing by Richard
Cortez et al).
Traditional Hearing Aid Shell Manufacturing
FMC – Headline Numbers
2012
Product
3,309
Service
10,492
Group Revenue
13,800
Goodwill
11,422
Clinics (#)
AM Disruptive Example – Hearing Aids
Exhibit 15
Exhibit 14
Dec Y/E ($mn)
We would not therefore reflect any of these potential
longer-term challenges from AM in our valuation of Fresenius
Medical Care. In our DCF valuation we continue to use a
terminal growth rate of +1%.
3,160
Source: Company Data, Morgan Stanley Research
The gold standard for end stage renal dialysis patients is to
have a kidney transplant, but due to the low number of kidney
donors, this is currently not practicable. Theoretically, the
creation of a fully functioning 3D printed kidney could reduce
the need for hemodialysis services and put FMC’s business
model under pressure over time; it could also result in asset
write-downs. However, there are several obstacles aside from
the actual ability to produce a working organ that may limit the
uptake of 3D printed kidneys, such as:
Patient Health – not all ESRD patients are well enough to
undergo a highly invasive surgery;
Source: “Changing with the Times: Applying Digital Technology to Hearing Aid Shell
Manufacturing” – Francis Kuk
18
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
In the Exhibit above, a] highlights a cost of the impression
being made; b] ear impressions trussed to the model size; c]
the impression is dipped in wax; d] a hydrocolloid cast of the
impression is done; e] acrylic resin is poured into the
hydrocolloid cast; f] excess acrylic resin is drained from
hydrocolloid cast; g] trimming of faceplate end; h] vent is laid
into the shell; i] finished shell is ready to have electronics
inserted. The process overall is time consuming and labour
intensive, making the production of a custom shell expensive.
Exhibit 16
3D Printing of Custom Hearing Aid Shell
AM Way of Shell Manufacturing
With AM, the impression is scanned and the custom shell is
made in a more automated way. Specifically, three steps are
typically used to create a custom shell: 1] an ear impression is
scanned by a 3D printer; 2] a modeller make adjustments to the
virtual model in the software package; and 3] shell is printed on
a 3D printer.
Source: Copyright Widex
The advent of digital technology in conjunction with AM has
increased the accuracy and consistency of custom shell
manufacturing. With the added benefit of lower production
costs and faster turnaround times, this has led to mass
adoption of AM technology in recent years.
19
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
AM Opportunities and Limitations by Sub-sector
In this section we provide more detailed commentary on AM applications
by MedTech sub-sector, examining opportunities and limitations. We
also provide feedback from companies under our coverage on the
degree of AM utilisation today. The details provided are not meant to be
comprehensive but rather a broad overview of which areas of medical
devices may be more suited than others. Areas covered are:
– Cardiovascular
– Corrective Lenses
– Dentistry
– Dialysis
– Diagnostic Imaging
– Hearing Aids
– Hospital Supplies
Dr. Chandra at the University of Rochester has been tackling
this problem by using patient scans to create a 3D printed
version of the patient’s own aneurysm, allowing the physician
to make a better assessment of the medical condition. This can
be done by taking the 3D model of the aneurysm and stressing
it to rupture. This patient-specific diagnosis allows the
healthcare system to avoid unnecessary surgeries, which is
good for the patient and reduces costs. Dr. Chandra highlights
that the longer-term goal is to be able to repair aneurysms
tailored to the specific patient.
The ultimate long-term goal would be, as science identifies the
characteristics of the patient’s blood vessel, to quickly create
medical devices that are compatible in material properties with
those of the patient’s blood vessels, to allow for the most
natural replacement for their aneurysm.
– Incontinence & Ostomy
Heart Valves
– In-vitro Diagnostics
Efforts are underway to use 3D printing in heart valve
replacement. Different technologies are being pursued, one of
which is embryonically inspired heart valve regeneration
engineering. The aortic valve is a complex, heterogeneous
structure designed to ensure unidirectional blood flow and to
provide blood to the heart through coronary ostia. At Cornell
University’s Department of Biomedical Engineering, hydrogels
are being used to develop a tissue engineering strategy that
combines micro CT imaging, custom algorithms and 3D
printing to generate cell-seeded valve constructs.
– Orthopaedics
– Radiation Therapy
– Wound Care
While there are many other areas of MedTech, we have focused on
areas that broadly fall under our coverage.
Cardiovascular
For cardiovascular, we have found interesting literature on
aneurysms, heart valves, entire heart and blood vessels. We
suspect other areas of cardiovascular are also being
researched for AM.
Aneurysms
Aneurysms cause a high of number of deaths around the world.
In the US, abdominal aortic aneurysms are one of the 10 most
common causes of death in men over 55. They are an
enlargement in the lower part of the major blood vessel
supplying the body; if an aneurysm splits, or ruptures, it can
lead to life-threatening internal bleeding. Researchers are
working on patient-specific diagnosis and treatment for the
condition. The diagnosis goes beyond just diagnosing the
aneurysm; once a patient has been diagnosed the question
arises whether the aneurysm is likely to rupture at some point.
Entire Heart
Efforts are already underway to create a total “bioficial” heart, a
goal that could be attained within 10 years, according to
Executive and Scientific Director, Professor Stuart Williams of
the Cardiovascular Innovation Institute (a collaboration
between the University of Louisville and the Jewish Heritage
Fund for Excellence). Professor Williams was involved in
building a 3D printer called BioAssembly Tool, which uses
human cells and biologically safe glue, with the main interest in
creating blood vessels, cardiac structures and ultimately hearts
to fight cardiovascular disease.
Tissues are created using cells derived from an individual’s fat
and extracted with a machine. The cells go into the
BioAssembly Tool, and the living cells are mixed with glue that
eventually dissolves inside the body. The printer rebuilds the
structure, which can than be implanted into the body.
According to the researcher, building the heart requires five
parts, namely valves, coronary vessels, microcirculation,
20
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
contractile cells and the organ’s electrical system. Professor
Williams thinks the bioficial heart could cost about $100,000 in
today’s dollars.
Blood Vessels
Provided in Exhibit 17 below is an illustrative example of a 3D
bio printer, which replaces the "normal" printing materials with
"Bio-ink", which can be made out of living human cell culture in
a gel medium to promote cell growth. The cells eventually grow
together forming the desired shape.
Exhibit 17
3D Printer – Illustrative Example
Corrective Lenses
Unsurprisingly, the development of 3D printing in the
ophthalmological glasses market has been almost exclusively
focused around the frames for glasses. Indeed, we have been
told by Luxottica management that the company uses 3D
printing extensively in the product design stage of its frame
manufacturing. Despite this, there has been little focus on the
development of 3D printing technology for the more complex
task of lens production. The principal difficulty in the production
of 3D printed lenses is one of precision, where even the lower
end for ophthalmological glasses is a standard that 3D printers
struggle to match. There has been a degree of work attempting
to resolve this issue with interpolation5, where a sheet is
stretched over the lens to smooth the surface; however, these
experiments appear to have failed to reach the necessary level
of accuracy for prescription lenses.
In June 2013, however, the world’s first 3D printed glasses with
lenses were produced by LUXeXcel. The company’s
proprietary “Printoptical” technology allows for the printing of
smooth functional lenses and frame in a single print job. The
technology prints optical structures using modified wide format
industrial inkjet equipment, where transparent droplets of a
UV-curable polymer are jetted and then cured by strong
UV-lamps that are integrated onto the print head.
Exhibit 18
LUXeXcel has produced the first set of fully 3D
printed glasses in the world
Source: Christopher Barnatt, explainingthefuture.com
Our discussion with Sorin suggests that within its Heart Valve
business unit, 3D printing is extensively used for rapid
prototyping. The company uses external vendors for this,
which provides a fast and reliable service. Sorin also
highlighted some limitations, including that accuracy is pretty
limited but improving, mechanical properties are low, which
makes it difficult to predict the final performance, surface
finishing is modest and only a few polymers can be used, none
of which it believes is suitable for implantation.
Source: LUXeXcel,
The feedback for its Cardiac Rhythm Management division
highlighted that 3D printing is used more for prototyping,
comparing shapes and sizes of implantable devices, and
challenging and optimising integration of sub-systems.
Overall it appears the cardiovascular industry is using 3D
printing primarily for prototyping, which is not expected to
change over the short to medium term.
Even though the material is deposited in discrete drops, the
resulting surface is smooth, as the time between jetting the
droplets and the application of the UV light gives the polymer
time to flow and for each droplet to lose it spherical form. This
means that optical quality surfaces may be formed with no post
processing
5
Producing Lenses with 3D Printers, Christopher Olah
21
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 19
LUXeXcel’s Printoptical technology allows for 3D
printed lenses without the need for post processing
Dentistry
Dentistry is a broad area, and as such we explore 3D printing in
the various sub-segments such as Prosthetics, Implants and
Orthodontics. At a high level, the interest in 3D printing comes
with the general shift in digital dentistry, helped by oral
scanners. By combining oral scanning with CAD/CAM and 3D
printing, dentists and lab owners may one day be able to
accurately and quickly produce crowns, bridges, stone models
and a range of orthodontic appliances for the dental office. The
benefits could include savings on labour, improved quality,
precision and less rework. Going forward, the most significant
advances in 3D printing may come from new materials.
Crowns & Bridges
Source: LUXeXcel,
Lenses under LUXeXcel’s Printoptical system can be printed to
a thickness of up to 2mm, which we believe could
accommodate the majority of Rx prescriptions. Despite this, we
have yet to see another operator make progress on printing
quality prescription lenses, and there is minimal information
available on the underlying quality of the product. Although
Wohlers Report 2013 highlights LUXeXcel’s technology as an
‘emerging technology’, it is unclear whether modern lens films
that offer properties such as anti-reflection and scratch can be
applied to the process. Over time we expect research to focus
on this area, as well as the development of vari/multi-focal
lenses; however, it appears unlikely that AM will have a
material impact on the corrective lens industry short term.
Our discussion with Essilor suggests that it monitors the 3D
printing space closely but doesn’t foresee any major changes
in its supply chain or manufacturing.
AM is well suited for making crowns and bridges, which are
typically high-value items and require customisation to suit the
individual’s needs. The German company, EnvisionTEC, is
one example of a company that has the ability build crowns or
multiple unit bridges for long-term temporaries; the materials
available include E-Dent, which is a glass-filled photopolymer.
Phenix Systems’ PXS & PXM Dental offers rapid manufacture
of dental prosthesis using laser sintering of Cobalt-Chromium.
Implants/Suprastructures
A number of companies have been using AM to produce dental
implants or suprastructures. For instance, LayerWise through
its division DentWise allows for design freedom for
implant-supported restorations. The materials used are a high
strength titanium or cobalt-chromium alloys, which can be
produced with high accuracy of better than 20 micron.
Exhibit 20
LayerWise Uses AM for Suprastructures
Source: LayerWise/Dentwise
We are also seeing the emergence of custom-built implants
using AM, with the Italian company Leader Italia offering an
interesting product. The company claims that Tixos is the first
and unique implant in the world manufactured through a direct
laser metal forming technique by microfusion of titanium
particles.
22
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 21
Leader Italia – 3D Printed Dental Implant
At this stage, it is hard to see 3D printing replacing milling in
dentistry. The two technologies are likely to exist side by side
for the foreseeable future, as there are some things that milling
can do that 3D printing cannot. We suspect one of the ultimate
goals would be to have 3D printing produce the final restoration
straight from the machine, but it appears that we are many
years away from that.
Straumann highlighted that it is a user of 3D printing
technology but more for use in temporaries, models and
prototypes. It currently finds that the technology is not precise
or fast enough to make it suitable for ceramic crowns and
bridges. Our discussion with Nobel Biocare suggests that it is
using 3D printing as a testing device for its Procera.
Dialysis
Source: Leader Italia
Orthodontics
3D printing is already used in orthodontics, where US listed
Invisalign offers a 3D printed alternative to fixed braces. We
understand that Invisalign prints over 60,000 sets of
transparent custom-made moulds, which the wearer changes
every two weeks to realign the teeth. One of the more talked
about companies that produces solutions in digital orthodontics
is Stratasys.
Dentures
Partial and full dentures are seeing an increased usage with 3D
printing. EOS is launching a partial framework solution using its
direct laser metal sintering technology. Technicians who want
to use AM to produce dentures are able to access 3Shape’s
Denture Design software.
Other Areas
3D printing solutions from companies like EnvisionTEC are
able to make drill guides, temporaries and models. For guides,
the company offers the material called Clear Guide, which is a
water clear material. For models, the company can offer
E-Denstone. It should also be noted that until recently most drill
guides have been limited to larger companies, such as Nobel
Biocare, which had custom software and invested in expensive
equipment. That is changing, with one of the larger 3D players
in dentistry, 3D Systems, offering the MP3000, which when
paired with open drill guide software allows virtually anyone to
start producing guided surgery templates.
The kidneys are two organs that perform life-sustaining roles of
cleaning the blood by removing waste and excess fluid and
maintaining the balance of salt and minerals in the blood. In
some patients, the kidneys become damaged, usually as a
result of diabetes and / or hypertension. The kidneys could
eventually stop functioning, which would lead to death. To
survive, these patients either need a kidney transplant or to
receive dialysis treatment. Since there is a significant organ
shortage, most end-stage renal disease patients visit a dialysis
centre three times a week to remove waste and excess water
from their blood. 3D printers may hold the key to successfully
producing the first transplantable kidneys for humans. Before
3D bioprinting hit the market, researchers were using pig
kidneys as scaffolds to hold human kidney cells; however, this
never resulted in a kidney that could be successfully
transplanted into a human.
Today, it appears that several research groups are
spearheading the development of a kidney using 3D printing,
with The Wake Forest Institute for Regenerative Medicine
receiving a great deal of media attention. Dr. Anthony Atala is
the lead researcher at Wake Forest. Currently the clinician is
using a 3D bioprinter to create small prototype kidneys (see
Exhibit 22) to study their performance; at this stage the organ
produces a urine-like substance. Limitations today include an
uphill battle to get around a patient rejecting the organ and
getting it to function as well as real kidneys.
23
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 22
Exhibit 23
3D Printed Kidney
3D printed patient hearts, using data from MRI
scans, are helping doctors prepare for surgery
Source: Wake Forest School of Medicine
Michael Renard (Executive VP for commercial operations at
San Diego based Organovo) commented in the dezeen
magazine (19 May 2013) that it is currently possible to print
small pieces of tissue, but that the problem lies in scaling this
and creating a vascular system that delivers oxygen to the cells
and removes carbon dioxide. He further added that printed
organs such as kidneys are a long way away: “In the next 10
years it is possible that printed supplemental tissues, ones that
aid in regeneration – such as nerve grafts, patches to assist
heart condition, blood vessel segments or cartilage for a
degenerating joint will make it to the clinic. But more advanced
replacement tissues will most likely be in 20 years or more”.
Source: © Materialise
Another example is provided by the Kobe University School of
Medicine, which is also using 3D printing to model facsimiles of
patients’ organs in preparation for surgeries. The use of CT and
MRI diagnostic imaging equipment, with 3D printers that can
handle multiple materials, has allowed the creation of
transparent textured organs that provide doctors with an
intricate view of the internal structure of patient’s organ.
Exhibit 24
Our discussion with Fresenius Medical Care suggests that 3D
printing is only used in prototyping parts, design and a little bit
on the R&D side. Overall it appears that 3D printing may not
have a meaningful impact on the dialysis industry over the
short to medium term.
A 3D printed liver, with clear tissue to allow
examination of the internal structure
Diagnostic Imaging
Diagnostic Imaging is principally composed of MRI (Magnetic
Resonance Imaging) systems, Ultrasound systems, X-ray
systems, Mammography equipment, CT (Computer
Tomography) systems, and nuclear imaging systems. There
have been a number of recent examples of diagnostic imaging
equipment being used, in conjunction with 3D printing, to
prepare surgeons more effectively for complex surgeries.
For example, doctors at the Children’s National Medical Centre
in Washington are using data from CT or ultrasound scans of
patients to replicate the organs of those individuals, reflecting
their particular intricacies and deformities. These replicas have
been made of a number of different materials, allowing doctors
to place a suture or push a needle through it, with realistic
tissue structure such as soft heart valves and intermittent bone.
This allows practice of procedures, without involving the
patient, as well as diagnosis of complications and conditions.
Source: Photo credit: Tech-On!, Nikkei Business Publications, Inc
We expect the integration of 3D printing and diagnostic
imaging to continue over the long term. However, the cost of
producing implantable products for the time being still appear
very costly. For instance, Dr Sugimoto at the Kobe University
School of Medicine created the printed liver in Exhibit 24, with
an Object Connex printer that costs between $250,000 and
$500,000 depending on the model. As 3D printing evolves, we
24
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
expect relative costs to decrease, pushing the use of
diagnostic imaging in this area forward. Overall it should be
noted that 3D printing is unlikely to drive a material increase in
the demand for diagnostic imaging equipment. Rather, we
think the installed base should be sufficient to enable the
adoption of 3D printing.
in just 60-90 minutes. The machine is relatively small with a
weight of 85kg. Depending on the build size and complexity,
the cost of a hearing aid 3D printer can vary from $20,000 to
$150,000. In 2013, Widex appears to have manufactured the
world’s smallest hearing aid using CAMISHA (Computer Aided
Manufacturing of Individual Shells for Hearing Aids).
Hearing & Hearing Devices
Batteries
The hearing aid industry has been one of the early adopters of
3D printing technology with customised shells. New areas of
research include battery technology and ‘growing’ ears.
Custom Shells
3D printing has been widely used in the manufacture of hearing
aids for over five years to make customised housing for
in-the-ear hearing aids and is now widely adopted by most
hearing aid manufacturers. For example, Starkey introduced
3D printers 10 years ago and now has 30 printers across seven
facilities worldwide. One of the first was Materialise, which
collaborated with Phonak in 2000. Since then a large range of
biomedical materials have been approved with various skin
tones and other colours.
The standard shape of batteries available for hearing aids
today has a material influence on its size and look. With 3D
printing this could change. Scientists at Harvard University and
the University of Illinois appear to be among the first to
fabricate a battery using a 3D printer, focusing on the creation
of a very small microbattery as highlighted in Exhibit 26 below.
Exhibit 26
3D Printed Battery
Exhibit 25
Hearing Aids – 3D Printing of Custom Shells
Source: Jennifer A. Lewis, Harvard University
A custom 3D printer was used with a printing nozzle size of 30
microns, to produce two comb-like shapes and laid down in an
interlocking pattern to function as the two electrodes. The
finished battery, less than a millimetre wide, was placed in an
electrolyte solution. In the Harvard press release it stated: “The
electrochemical performance is comparable to commercial
batteries in terms of charge and discharge rate, cycle life and
energy densities. We’re just able to achieve this on a much
smaller scale”. With the onset of such technology, batteries
could be made to conform to the shape and size of the desired
hearing aid. Furthermore, it could also impact how the
integrated circuit with a battery could be manufactured.
Source: EnvisionTEC, Inc
One of the AM manufacturers whose products have become
quite widely used in hearing aids is EnvisionTEC, which has
been working with Sonova since 2005. The Perfactory 4 DSP
XL with ERM is capable of producing 65 shells / 47 ear moulds
Ears
In February 2013, Cornell University in New York announced it
has used 3D printing to create an artificial ear for treating a
congenital deformity called microtia, where the ear is
underdeveloped or had to be removed due to cancer or was
25
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
lost in an accident. Later in the year Princeton University
developed a bionic ear that could offer more than just improved
cosmetics and offer improved hearing (Exhibit 27).
Exhibit 27
3D Printed Bionic Ear
however, research work by Chenlong Zhang et al.6 points to
the potential. The work done by the team was to assess the
cost reduction opportunity from creating optical laboratory
equipment from 3D printing as opposed to purchasing from a
manufacturer. The study found that this method could reduce
the cost of many optical components by 97% or more.
Exhibit 28
Optical equipment produced in the test using 3D
printing
Source: Frank Wojciechowski/Princeton University/fwphoto@optimum.net
Researchers 3D printed a blend of calf cells, hydrogel and an
integrated coiled antenna made from silver nanoparticles. The
assembly does not resemble a natural ear that closely, but it
does an interesting job merging organic and synthetic material.
The rudimentary solution also allows the possibility of
expanding hearing beyond normal human levels; in this case it
can pick up radio waves.
Our discussions with GN Store Nord, Sonova and William
Demant suggest that their current involvement with 3D printing
is on the custom shell side, which has been a core part of their
business practices for years. William Demant highlighted that it
started back in 2006/07 and it now has 3D printing technology
in all of its larger production facilities. This has resulted in the
consolidation of ITE production facilities into larger hubs, since
overhead for support & maintenance and utilisation of the
equipment is better in larger facilities. Sonova made similar
comments that 3D printing has led to consolidation of custom
shell manufacturing. GN Store Nord highlighted that all of its
custom shells are made using 3D printing technology and that,
going forward, more 3D technology will be used in its R&D
functions. Overall, outside of custom shell manufacturing, there
appears little other excitement within the industry for other
applications in hearing aids.
Hospital Supplies
Hospital supplies is a broad category and, for the purposes of
the stocks under coverage, includes injectable generics,
clinical nutrition, infusion pumps, syringes and other general
supplies. There has been little evidence of material
development of 3D printing in hospital supplies to date;
Source: Zhang C, Anzalone NC, Faria RP, Pearce JM (2013) Open-Source 3D-Printable
Optics Equipment. PLoS ONE 8(3): e59840. doi:10.1371/journal.pone.0059840
While not directly comparable to hospital supplies, the
successful production of optical equipment suggests that there
is potential for an expansion into hospital equipment.
While Getinge did not provide detailed feedback on 3D
printing, it is our view that it may be used for prototyping for
some of its capital equipment. However we do not believe that
3D printing is used in the actual production process.
For Fresenius SE, AM has no implications for its German
hospital business, which makes up 18% of its Group EBIT
adjusted for minorities. For its FMC subsidiary, which makes up
31% of Group EBIT, 3D printing is only used in prototyping
parts, design and marginally on the R&D side. For its hospital
supplies business called Kabi (51% of EBIT), which is primarily
focused on clinical nutrition and injectable generics, AM is in
our view irrelevant. As such, we think AM is likely to have no
material impact on Fresenius SE.
6
Zhang C, Anzalone NC, Faria RP, Pearce JM (2013) Open-Source 3D-Printable Optics
Equipment. PLoS ONE 8(3): e59840. doi:10.1371/journal.pone.0059840
26
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Incontinence & Ostomy
We have found little evidence for the development of 3D
printing within the Incontinence & Ostomy markets; however,
there are some signs that it may develop in the medium term.
We note that Coloplast has a 3D printer, used for prototyping,
in its product development department, though it is unclear
how widespread this is or the degree of its use.
Exhibit 29
3D printer at Coloplast (LFS), Polyvinvl Alcohol (RHS)
Source: Coloplast, Wikipedia
We would also note the high level of compatibility between 3D
printers and plastics, which are mostly used for Incontinence &
Ostomy products, including Polyvinyl Alcohol (PVA).
Our discussion with Coloplast suggests that 3D printing is
more of a prototyping opportunity and is unlikely to have a
material impact on the company or its market segments over
the medium term.
Reconstructive Joints
With orthopaedic joint replacements, we are currently
observing two avenues for 3D printing:
Guided Surgery
Customised Implants
Guided Surgery – 3D printing is already used as a
visualisation tool to pre-plan surgery in joint replacement.
Surgeons use a patient-specific drill and saw guide to
improve accuracy in placing hip & knee implants, with systems
offered by all major competitors. In a European context, Smith
& Nephew offers Visionaire, which was launched in 2009.
Physical Joint – a number of products are already available.
For instance, Stockholm-listed Arcam AB offers a metal
powdered bed fusion technology called Electron Beam Melting
(EBM). The company states that EBM is used for production of
standard as well as custom orthopaedic implants, with a
cost-efficient production process for both press-fit and
cemented implants. The cost efficiency is particularly
noticeable for volume production of press-fit implants with
advanced Trabecular Structures. Solid and porous sections of
the implant are built in the same step, eliminating the need, for
example, to apply plasma sprayed porous materials through
expensive secondary processes.
Exhibit 30
Arcam: 3D Printing of Custom Implant Surface
(EBM)
In-vitro Diagnostics
Following our review of the literature, we found little evidence
that AM is a useful technology in the in-vitro diagnostic
sub-sector. This has been confirmed by our discussions with
IVD companies, where the use is limited to rapid prototyping of
some hardware devices and components. Specifically our
discussion with bioMerieux suggests that the 3D printing is
limited to the machines.
Orthopaedics
Source: Arcam
Orthopaedics is a broad based area, and as such we explore
3D printing in the various sub-segments of joint replacement,
trauma, craniomaxillofacial, spine and prosthetics.
Arcam documented in a recent investor presentation that
producing a Ti-6AL-4V acetabular cup was more cost effective
than the conventional method: the cost using EBM was
€40-103 per cup (varies with cup size from 44 to 66) or a
27
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
€20-25 over the machined products. This is the result of less
production waste (when machining 60-70% of original material
is scrapped) and no secondary process of attaching the porous
coating, which can cost €30-60 per implant.
Exhibit 32
OsteoFab Patient Specific Cranial Device
The Arcam EBM machines utilise a high power electron bream,
which splits into more beams and generates the energy
needed for high melting capacity. According to the company,
the process results in stress-relieved components with material
properties better than cast and comparable to wrought metal.
In Europe orthopaedic implants containing EBM technology
were CE marked in 2007, and in February 2011 implant
manufacturers using EBM received regulatory approval from
the FDA for certain products. Orthopaedic companies that are
using the EBM technology are Adler Ortho, Lima-Lto and
Exactech.
Trauma / Craniomaxillofacial
AM already plays an important role in craniomaxillofacial
(CMF), following an accident where part of the bone structure
around the head may have been destroyed. Using 3D printing
in titanium powder allows, for example, the production of a
lower jaw, with cavities that allow for muscle reattachment and
grooves for the regrowth of nerves. In this case the product was
produced by LayerWise, who produces products for medial
and dental indications.
Source: Oxford Performance Materials, LLC
Spine
The use of 3D printing appears to be less proficient than in joint
reconstruction. While some companies have launched spinal
spacers printed in titanium, most of the focus appears to be on
printing 3D spine models to help in the diagnosis or planning for
surgery, especially in deformity cases.
Prosthetics
Exhibit 31
LayerWise uses AM in Orthopaedics
US-based Bespoke Innovations creates custom prosthetics
using a 3D printer, which builds a solution based on the unique
shape of a particular user.
Exhibit 33
Custom Made Prosthetics – Bespoke Innovations
Source: LayerWise/Dentwise
Earlier in 2013 the FDA for the first time awarded 501(k)
clearance for an AM polymer implant, for a product called
OsteoFab Patient Specific Cranial Device, manufactured by
Oxford Performance Materials in the US. The implant is made
from PEKK, which is an ultra high performance polymer used in
biomedical implants. While Oxford Performance Materials sold
PEKK as a raw material or in semi-finished form, it began
developing AM technology in 2006.
Source: Bespoke Innovations
28
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exoskeleton
JAECO Orthopaedic and Stratasys produce a WREX
(Wilmington robotic exoskeleton arm) which is a functional
upper limb orthosis designed to enhance movement for
individuals with neuromuscular disabilities. The device is made
up of a customised butterfly-patterned jacket and arms that are
3D printed in durable ABS plastic.
To help broken bones, researchers are looking at 3D printers to
produce an exoskeleton brace as an alternative to the
traditional cast, offering lightweight, lifestyle benefits such as
having a shower. As highlighted in Exhibit 34 below, the Cortex
developed by Victoria University graduate is a prototype, which
could offer such benefits. The idea is that a patient fitted with
the Cortex has an X-ray taken of the injured arm or leg. A
computer would then assess the optimal pattern and structure
for the cast.
Exhibit 34
3D Printed Cast – Replacing Traditional Cast?
Although the company did not go into specifics, it did suggest
that 3D printing may have an interesting future in orthopaedics,
both from a production and inventory management perspective.
Our discussions with Ossur suggests that the company uses
3D printing technology extensively in its R&D setting, mostly for
testing new ideas and product development. The company
comments that it has already seen a decrease in its time to
market, and should the technology advance to the point where
it can print structural reinforcements and multiple materials, it
would use the technology for direct manufacturing.
Radiation Therapy
There are two key areas in which 3D printing has begun to
manifest itself within Radiotherapy: compensator blocks and
shells. Prior to the advent of asymmetric collimators,
compensator blocks offered the only means of varying dose
intensity across the treatment beam area. Compensators offer
the advantage that they are not subject to the temporal
fluctuations of smaller sub-fields associated with Multileaf
Collimators (MLCs). The conventional way to manufacture the
blocks, using milling machines, has been an important
drawback when compared to the MLC method, due to high
operational and production costs.
Exhibit 35
Compensator blocks used in Radiotherapy
treatment
Source: Victoria University
Bone Replacement
Researchers are using 3D printing that could aid the regrowth
of damaged or diseased bones. At the Washington State
University, the research group’s optimised ProMetal 3D printer
builds dissolvable scaffolds utilising a ceramic compound
coated with a plastic binding agent, which serves as a blueprint
for tissue growth. Although the team has already spent four
years fine-tuning the process and having achieved positive
results testing on rats and rabbits, there are still 10-12 years to
go, according the project’s co-author, before orthopaedic and
dental surgeons could be offered a printed bone replacement
for use in humans.
Our discussion with Smith & Nephew suggests that AM is an
area it is very familiar with, given its Visionaire product line that
is made with the assistance of 3D printing technology.
Source: dotdecimal
A recent study performed at the Biomedical Engineering
Department of the University of Brasilia7 suggests that this key
drawback may be addressed using 3D printing. A fluency map
was generated by a commercial treatment planning system,
which was then converted into a mould and printed using a 3D
printer, while the final block was achieved by filling the mould
with cerrobend alloy. The block was tested using dosimetric
films to compare the measured dosage to that predicted by the
7
Use of 3D-printers to create Intensity-Modulated Radiotherapy Compensator Blocks,
Biomedical Engineering Department, University of Brasília, 2012
29
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
planning system. This comparison showed good conformity
among eight dose profiles from each situation, with a maximum
RMS error of 8.84 % for the tested profiles. This suggests that
the 3D printers can be effectively used to manufacture IMRT
compensator blocks. The main advantage of this approach is
that it can be fully conducted inside a radiotherapy facility,
resulting in lower costs and production times.
the prospect of a material movement into 3D printing as a likely
game-changer for the industry. We can, however, envisage a
number of other ancillary products to the radiotherapy process,
much like with patient shells / masks, being tested in a 3D
printing environment.
3D printing has also been using in the production of shells.
Immobilisation of patients undergoing brain or head and neck
radiotherapy is normally done through the use of Perspex
thermoplastic devices that require direct moulding to the
patient anatomy. Mould rooms can be distressing for patients
and shells made in this manner do not always fit perfectly.
Tests by a group of UK researchers8 managed to successfully
create fitting shells from CT and MRI data for two volunteers,
using a 3D printer, with the group hypothesising that virtual
patient data could replace mould room visits.
Wound care covers a number of different indications, ranging
from simple cuts to more difficult-to-treat areas such as burn
wounds or pressure ulcers. There have been a number of
interesting developments in 3D printing that have the potential
to shake up the current treatment method of wound care,
though we believe the technology is at least three to five years
away from human testing.
Exhibit 36
Examples of finished shells for radiotherapy
Wound Care
Skin Printing
A team of bioprinting researchers led by Anthony Alata at the
Wake Forest School of Medicine have been developing a skin
printer. In initial experiments, 3D scans of test injuries were
taken from mice, the data from which was used to control a
bioprint head that sprayed skin cells, a coagulant, and collagen
onto the wounds. On average, the wounds healed in two to
three weeks compared to about five or six weeks in a control
group – a promising result. Indeed, funding for the project has
come, in part, from the US military, which is keen to develop
in-situ bioprinting to help heal wounds on the battlefield.
Exhibit 37
Skin printing on mice wounds showed a material
improvement over the control group
Source: Patient information website of Cancer Research UK:
www.cancerresearchuk.org/cancerhelp
Our conversations with Elekta indicate that the company has a
3D printer which uses lithography to create plastic models of
mechanical parts. The company makes life size or reduced
scale plastic components that allow it to physically evaluate its
designs before committing to expensive tooling and
manufacturing investment. The type of 3D printing that is used
is not new emerging technology but more of what has been
around for some time. From our perspective, given the nature,
complexity, and scale of linear accelerators, we do not consider
8
Production of 3D printer-generated radiotherapy treatment shells using DICOM CT, MRI or
3D surface laser scan - Acquired STL files: Preclinical feasibility studies
Source: Wake Forest School of Medicine,
Wake Forest has also been working on burn wounds. With
traditional skin grafts, many burn patients do not have enough
unburned skin to harvest for grafts, which the developing 3D
printer addresses. In the project, the group places cells in vials
that are then printed directly onto the wound, after a laser first
scans the wound to “map” its dimensions. Again, mice with
burn wounds healed in 3 weeks versus the control group of five
weeks.
30
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 38
A test for 3D printing on burn victims using an
artificial limb
Source: Wake Forest School of Medicine,
While current research in the area is encouraging, tests on
human patients remain around three to five years away. We
would also highlight that it is unclear how 3D printing may
interact with other complex wounds such as pressure ulcers.
Much of the current research in the space surrounds creation of
vascular skin (such as that carried out at the Aalto University
BIT Research Centre), as well as the challenge of how to
ensure skin receives a ready supply of nutrients. Although
there are some clear hurdles to overcome, in the long term it is
possible that 3D printing may play a disruptive role in the
wound care space, assuming these difficulties are overcome.
testing. While glass and silicone offer good transparency, the
accuracy of the models place limitations on the validity of the
results produced, and the process is expensive as the models
are either made by hand or injection moulding.
Regulators in the US have recently made recommendations for
using more clinically relevant bench top models, in which 3D
printing can play a major role. Although not new, there is a
greater push to use digital human data captured via diagnostic
imaging technology such as computed-tomography (CT) or
magnetic resonance imaging (MRI). This method allows
engineers to identify design flaws more quickly, which
otherwise may only become apparent at a later stage in animal
or human clinical trials. Hence, R&D productivity and time to
market could potentially help the MedTech industry going
forward.
One company that is focused on 3D models is Belgium-based
Materialise, which offers a service called HeartPrint (Exhibit 39
below) which makes, among other things, cardiovascular
bench top models.
Exhibit 39
Materialise HeartPrint 3D Heart Model
It appears that Smith & Nephew’s wound care focus is less on
3D printing and more about growing its market share in
negative pressure wound therapy and executing on its
Healthpoint acquisition. With the recent acquisition of
Healthpoint, the company strengthened its position in the
bioactive wound care business. Besides purchasing
Collagenase SANTYL (enzymatic debrider) for dermal ulcers
and burns, it also acquired pipeline product HP802-247, which
is its next generation bioactive therapy.
Other Areas
Other areas that we have come across during our research
include bench top testing and a broader discussion on organ
replacement.
Bench Top Testing – R&D Productivity and Time to
Market
Traditionally, bench top models in medical devices, particularly
for cardiovascular applications, have either been made of
blown glass for rigid parts or out of silicone for softer tissue.
Medical device researchers at companies would take the glass
or the silicone model and use it for early product performance
Source: © Materialise
The Materialise technology is not limited to cardiology; it can be
used for virtually any human organ, including the brain (Exhibit
40). These models are also likely to have an impact on
education and training, as well as address an ethical dilemma.
Animals are still widely used for training and are often involved
in R&D. Animal experiments are difficult to realise in large
numbers, for reasons of cost and ethics. Hence, a major effort
is under way to move towards biomodels for surgical training.
31
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 40
Materialise HeartPrint 3D Brain Model
blood vessels into the tissue. As a result, the scientists created
a network of places that they wished vessels to grow into, so
they would be ‘piping’ into the tissue and these were printed in
3D out of sugar. Sugar was described by the researchers as
useful material, which can be dissolved away in the presence
of living tissue and is very friendly to biological tissue.
Liver – the same researchers highlighted that with sugar,
thicker tissue could be built, such as a liver. Although the
printed liver was never implanted, they could show that one
could use a 3D printer to print an arbitrary network of vessels
for any tissue shape or any network of blood vessels, and then
surround them with liver cells. Professor Birchall, a surgeon
scientist at University College London, highlighted that the
researchers answered a lot of the fundamental problems in
tissue engineering. Organovo, a US-based company that
specialises in the development of 3D-printed biological
materials, prints functioning human liver tissue.
Japan - Implications for MedTech Space
Source: © Materialise, courtesy of Masayuki Hirata, Department of Neurosurgery, Osaka
University Medical School, Japan
Organ Replacement
The idea of using 3D printing for creating replacement organs
has been much debated over the years. Indeed, scientists
have long been experimenting with 3D printing of cells and
blood vessels, building up tissue structure layer by layer with
artificial cells. Dr. Jordan Miller at the University of
Pennsylvania highlighted in June 2012 that the big challenge in
understanding how to grow large artificial tissue is how to keep
all the cells alive in the engineered tissues. It has been noticed
that when you put a lot of cells together they take nutrients and
oxygen from neighbouring cells, which then suffocate and die.
The body’s cardiovascular system, i.e blood vessels, solves
this issue with natural cells and tissues. Provided below is a
brief overview of some of the developments that have come to
our attention:
Synthetic Vascular System – a group of scientists from the
University of Pennsylvania and the Massachusetts Institute of
Technology built a synthetic vascular system that mimics a
human cardiovascular system, by creating a place where the
future artificial blood vessels would be located. The technique
is similar to creating the shape of a vase in wax, surrounding it
with molten metal and then melting the wax away. But instead
of using wax, the researchers used sugar. Professor Bhatia
stated that so far it has been difficult to make organs big
enough to provide useful function. The clinician highlights that
if you implant tissue thicker than about a millimetre it becomes
difficult to provide enough nutrients without also engineering
The competition to develop 3D printing is focused largely in
Europe and the US, with Japanese makers appearing to lag
behind. The Ministry of Economy, Trade & Industry, conscious
of the need for government to push development, plans to build
multi billion yen funds into the overall budget appropriation
request for fiscal 2014. A super-precision 3D system
development project is underway from the current year (fiscal
2013), which aims to develop Japan-made 3D printers with a
ten-fold improvement in productivity in five years.
The trend for medical applications of 3D printing outlined earlier
can also be seen partly in Japan. A point to add is that many of
Japan’s medical device makers excel in products that exploit
electronic technology, such as X-ray CT scanners, MRI
scanners and endoscopes, and that 3D models of internal
organs using 3D printing should contribute significantly to
simulations of surgical procedures that involve such devices.
A Role in the Spread of New Surgical Techniques
In particular, surgical techniques using endoscopes have
proliferated rapidly in recent years, and 3D models of internal
organs generated by 3D printing now play a key role as a
training tool for doctors regarding new techniques. Operations
using laparoscopes have hitherto been performed for
appendectomies and cholecystectomies, but the scope has
recently been broadening to new areas including splenectomy,
prostate removal and ovarian resections. If 3D printing helps to
reduce the training hurdles for doctors, the benefits in terms of
medical economics will be considerable as these methods of
treatment spread and become more familiar to patients.
32
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Exhibit 41
Covidien: Composite Data - Still Considerable
Scope for Spread of Minimally-invasive Surgery
Procedure
% Minimally Invasive
Surgery
% Energy
Procedures
>80%
<20%
<20%
<20%
<20%
NA
NA
NA
NA
<30%
<20%
NA
<25%
<60%
Cholecystectomy
Hernia Repair
Hysterectomy
Colorectal
Thoracic
Head & Neck
Bariatric
structure, tumour size, and thus the potential risk (of
haemorrhaging, etc.) can be identified. 3D printing can also
provide a decision-making tool in selecting the optimal surgical
treatment for patients.
Exhibit 44
Head-mounted Monitor Launched by Sony
Source: Covidien, Morgan Stanley Research
Exhibit 42
Penetration Requires Clearing Technological
Hurdles
Pros
Cons
Reduced scarring
Reduced post-op pain
Shortened hospital stay
Technological hurdle for doctors
Lengthy surgery
Requires electric scalpels and other
special equipment
Requires general anaesthetic
Specific complications in laparoscopic
surgery
Can be hard to recover removed items
Early return to normal activities
Fewer post-op adhesions
Expanded surgical field
Source: Morgan Stanley Research
Source: Sony, Morgan Stanley Research
Exhibit 45
3D endoscope from Olympus
Exhibit 43
Range of Endoscopic Surgery has Broadened in
Recent Years
Endoscopic Surgery by Type
160 (thou. cases)
140
120
100
80
60
Source: Olympus, Morgan Stanley Research
40
Summary
For the Japanese MedTech space, we see there no direct
beneficiaries from 3D printing. However with the help from 3D
printed models, physicians should find it easier to learn new
surgical techniques. In this context, we believe Olympus would
benefit as it is one of major players in minimally invasive
treatment using endoscopy.
20
Abdomen (inclu. GI)
Respiratory
Gynecology
Urology
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
0
Others
Note: Figures are based on survey by Japan Society for Endoscopic Surgery. 2011 survey
involved 1,244 institutions.
Source: Journal of Japan Society for Endoscopic Surgery, Morgan Stanley Research
A role in Customised Surgery
Devices that allow stereo viewing of the relevant organs during
surgery have recently been gaining attention, with Olympus
launching a 3D surgical endoscope this April for the first time in
18 years, and Sony launching a head-mounted monitor able to
process image signals from an endoscope as a 3D/2D display
in July. In 2D imaging to date it has been difficult to identify the
depth of internal organs, but 3D imaging can lead to improved
accuracy and speed in operations.
For example, if a pre-op 3D model of the diseased organ is
produced by 3D printing based on biological data from a patient
that has undergone an X-ray CT or MRI scan, the organ
Pharma Companies
Our European pharma team did a brief survey with the pharma
companies under their coverage. Overall, it appears that 3D
printing is currently not much of a discussion point in the
European pharma industry and thus less relevant compared to
MedTech. Both Merck and Novartis suggested that 3D
printing was not meaningful for their businesses. Novo
Nordisk highlighted that it has used 3D printing technology in
the medical device R&D function for a number of years and
found the technology quite useful. But it does not see many
other areas where it would use 3D printing technology in the
near term.
33
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Limitations to Opportunities
In this section we explore some high level limitations to the AM
opportunities for Medical Devices. These include regulatory issues,
which are likely to evolve over time, the current state of the technology
and design & training. These challenges are not insurmountable, but will
take time to address. We feel the regulatory environment offers the
greatest uncertainty.
40736) establishes a UDI system, whereupon every device is
required to have a unique identification code physically marked
on the device. The code is to help facilitate a number of factors,
including consumer information, FDA tracking, and product
recalls. The UDI is set to be phased in over the next six years
and will bring with it a number of complications:
How will a UDI apply to home printed goods? As an
example, 3D printed prosthetics – and other class I devices
– will need their own UDI, the application of which in the
users’ home seems difficult / improbable.
In February 2013 a woman received a 3D printed
implantable replacement jaw (Telegraph). If hospitals are to
print 3D customisable devices on the fly, how is this to work
with a UDI system?
Regulatory Issues
On initial inspection, the regulatory environment for the 3D
printing of medical technology devices appears well
developed. Over the past five years there have been a number
of 3D printed products that have gained marketing clearance
from the FDA through its 501(k) pre-market notification or full
pre-market approval (PMA) process. Examples include:
Metal Hip Implant - the first FDA clearance of a metal 3D
printed implant in September 2010, when it approved a hip
implant produced by orthopaedic firm Exactech.
PEKK Cranial Implant - the first FDA 501(k) clearance of
an AM polymer implant. The cranial implant is made from
PEKK (polyetherketoneketone), and was manufactured by
Oxford Performance Materials.
PEEK Spinal Implant - FDA approval of DiFusion
Technologies’ PEEK (polyetheretherketone) based spinal
implant system.
Exhibit 46
An example of a code-based UDI label from the
FDA’s Unique ID System
Source: Medtronic
These developments hide the lack of progress made on more
fundamental questions of control surrounding 3D printing. The
recent level of press attention regarding the world’s first 3D
printed gun (e.g. The Telegraph, Wall Street Journal, The
Economist), has brought control and ethical considerations into
focus, and while we recognise the fundamental difference to
medical devices, these too have the capability for harm if not
controlled. With no current regulations surrounding the ability
for consumers to print replicate 3D medical devices, we would
expect the FDA and other bodies to examine the area in more
detail over the coming years.
Under the current regulatory system there also exist other
practical issues and considerations. As an example, on the 19
November 2012, the FDA updated its proposed rule covering
unique device identifiers (UDI). The proposed rule (77 FR
While these challenges are by no means insurmountable, we
believe they adequately illustrate the degree of work and
thought remaining to be done on the regulatory side. We would
argue that further penetration of 3D printing into medical
devices is predicated on the development of a strong
foundation of regulatory control, as with the rest of the medical
device industry.
State of Technology
While there have been strong gains in 3D printing development
over the past number of years, the capabilities of the
technology remain a limiting factor on adoption. Key
weaknesses in the technology preventing penetration include:
34
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Structural Strength – Traditionally manufactured parts
remain stronger than those created from 3D printing. With
processes like injection moulding, there is an even strength
across the part due to a consistent material structure. In 3D
printing, however, because items are built up in clean
“layers”, there is a laminate weakness as the layers bond
less strongly on the Z axis as they do on the X and Y plane.
This may prove a significant issue for implantable devices,
which are expected to last a number of years and withstand
a range of different stressors.
Surface Finish – While many pictures suggest 3D printed
plastics offer a gloss or smooth finish, this is normally the
result of post-processing, often involving labour and / or
chemicals such as acetone. For medical grade devices, a
smooth finish may be required and, if products are printed
in a hospital, additional staff / training may be required to
manually finish the device.
Speed – Many items printed can still take hours or days to
print. While the process could be expedited by increasing
layer thickness, this comes at a cost of surface and finish
quality. While future developments may overcome this
hurdle, it should be noted that the chemical properties of
materials such as ABS (Acrylonitrile butadiene styrene)
currently present a challenge. These materials can only be
extruded at a certain rate before key chemical properties
are destroyed, a barrier facing Fluid Deposition Modelling
for top-end machines at the moment.
Materials – Current 3D printers can broadly only print in
one material at one moment in time. Metals and plastics
normally cannot be printed together for example, as their
melting temperatures are hundreds, or indeed thousands of
degrees apart. We would argue the inability to print multiple
materials together is a key hurdle facing the adoption of the
technology.
This list is certainly not exhaustive, and while we expect
technological development to overcome many of these
hurdles, it is not a given that all will be dealt with, or in the
immediate future. With many of the devices produced by our
coverage universe featuring a broad range of intricate
electronics and moving parts, we would argue we appear quite
some distance from, say, 3D printing a functioning hearing aid
in totality.
Design and Training
3D printers naturally need a model, normally a CAD model, of
the design of the required product in order to be able to process
it. This represents something of a barrier to entry for consumer
and hospitals, especially in the production of bespoke or
customised medical devices.
Exhibit 47
CAD software complexity remains a barrier to entry
for mass acceptance and design
Source: Graphic provided courtesy of Gemvision Corporation, LLC (www.gemvision.com). All
rights reserved
Hospitals – Using the example of an orthopaedic implant,
while MRI or other input data may be able to give a base CAD
(computer aided design) model for the hospital, adjustments to
this will likely be necessary to accommodate for errors and
unique design issues. Doctors are unlikely to have the time or
inclination to learn how to use CAD software, or the intricacies
of design, where for example things like tolerances must be
taken into account – i.e. a 15mm shaft will not fit into a 15mm
hole. This suggests that hospitals may either have to send
base scans offsite to experts, or to employ them in-house, both
of which add to the relative cost of the end device and the time
it takes for production.
Consumers – Consumers face a similar issue. While the
end-user is unlikely to attempt to design their own implant or
hearing aid, even basic medical devices would require a
degree of prior knowledge. For example, consumers could
download pre-designed CAD files from open-source websites;
however, this would require knowledge of precisely what is
needed, while many of these files are currently unmoderated
and may well not be safe to use.
While we acknowledge that software usability is likely to
improve over time, and that the quality of predesigned CAD
files online are likely to improve, we continue to see the training
and expertise required to design bespoke medical devices as a
key barrier to entry.
35
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Companies Currently Involved
Below we list the publicly quoted companies that have a material
exposure in healthcare 3D printing. It is not an exhaustive list, but rather a
high level summary of companies that we have come across in our
research. None of the companies is a pure play in Medical Devices.
3D Systems Corporation
Description
3D Systems is a leading global provider of 3D content-to-print
solutions, including 3D printers and materials. The company is
listed on the New York Stock Exchange under the ticker DDD,
and in July had a market capitalisation of $4.3bn. The company
saw full year revenues of $127mn in fiscal 2012, and currently
has around 226 worldwide sales, application and service staff.
Areas of Focus
3D Systems is focused on providing 3D content-to-print
solutions including 3D printers, print materials and on-demand
custom parts services for professionals and customers. The
company also provides CAD, reverse engineering and
inspection software tools and consumer 3D printers, apps and
services. The company is well spread across its business units,
with around one-third of group revenues accounted for by each
of Printers, Materials, and Services. 3D Systems’ significant
recent launch was its second generation of a home 3D printer,
the Cube, as well as its next generation desktop printer,
CubeX.
Arcam
Description
Arcam provides Additive Manufacturing solutions for the
production of metal components, principally for the Aerospace
and Orthopaedic Implant industries. The company is listed on
the NASDAQ OMX Stockholm, under the ticker ARCM, and in
July had a market capitalisation of SEK1,743mn. Revenues in
full year fiscal 2012 were SEK139mn, up 29% from 2011 sales
of SEK 108mn. The company employs around 50 full time staff.
Areas of Focus
Arcam continues to focus on its Electron Beam Melting
technology, where fully dense metal components are built up
layer by layer from metal powder that has been melted by a
powerful electron beam. In 2013 Arcam released its Q10,
designed for industrial production of orthopaedic implants, and
specifically created to meet the implant industry’s need for high
productivity, with a simple interface and high resolution
printing.
ExOne
Description
ExOne is a global provider of 3D printing machines and printed
products to industrial customers. The company is listed on the
NASDAQ under the ticker XONE, and in July had a market
capitalisation of $817mn. Full year revenues in 2012 were
$29mn. ExOne currently employs 131 full time staff.
Areas of Focus
ExOne’s business primarily consists of manufacturing and
selling 3D printing machines and printing products to
specifications for its customers using its in-house 3D printing
machines. The company offers pre-production collaboration
and print products for customers through its PSCs, located in
the United States, Germany, and Japan. ExOne focuses on
printing capacity, where it believes it has the leading-edge (as
measured by build box size and printhead speed).
Organovo
Description
Organovo designs and creates functional, three-dimensional
human tissues for medical research and therapeutic
applications. The company is listed on the NYSE MKT under
the ticker ONVO, and in July had a market capitalisation of
$239mn. The company saw full year revenues of $1.2mn in
fiscal 2012, and currently operates with around 35 full time
employees.
Areas of Focus
Organovo’s current focus is on research and development,
progressing towards the commercial launch of its first product,
expanding the applications of its platform technology, and
improving the capabilities of its 3D bioprinter. The company’s
most prominent achievement has been surrounding its 3D
Liver project. As a world first, three-dimensional human liver
tissues were generated, consisting of multiple cell types
arranged in defined patterns that reproduce key elements of
native live structure and biological behaviour.
36
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Stratasys
Areas of Focus
Description
Stratasys Ltd. was formed in 2012 by the merger of Stratasys
Inc. and Objet Ltd. and is materially focused on the continued
integration of these two entities. The company’s business
model is centred on manufacturing 3D printers and materials
that create prototypes and manufactured goods directly from
3D CAD files or other 3D content. The company’s 3D printers
are based on its proprietary FDM and PolyJet technologies,
and is one of the world’s largest publically quoted pure-play
players in the 3D printing space.
Stratasys is a global provider of three-dimensional printing
solutions, offering a range of 3D printing systems, resin
consumables and services. The company is listed on NASDAQ
under the ticker SSYS, and in July had a market capitalisation
of $3,335mn. Revenues in the full year fiscal 2012 were
$215mn, and the company currently employs around 1,130
staff in 17 facilities around the world.
37
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Morgan Stanley Blue Papers
Morgan Stanley Blue Papers address long-term, structural business changes that are reshaping the fundamentals of entire
economies and industries around the globe. Analysts, economists, and strategists in our global research network collaborate in the
Blue Papers to address critical themes that require a coordinated perspective across regions, sectors, or asset classes.
Recently Published Blue Papers
Commercial Aviation
A Renewed Lease of Life
July 22, 2013
Wholesale & Investment
Banking Outlook
Global Banking Fractures:
The Implications
April 11, 2013
Emerging Markets
What If the Tide Goes
Out?
June 13, 2013
Releasing the Pressure
from Low Yields
Should Insurers Consider
Re-risking Investments?
March 15, 2013
Japan and South Korea
The Yen Tide Does Not
Lift All Boats
May 30, 2013
Global Autos
Clash of the Titans: The
Race for Global Leadership
January 22, 2013
Global Steel
Steeling for Oversupply
May 23, 2013
Big Subsea Opportunity
Deep Dive
January 14, 2013
US Manufacturing
Renaissance
Is It a Masterpiece or a
(Head) Fake?
April 29, 2013
eCommerce Disruption: A
Global Theme
Transforming Traditional
Retail
January 6, 2013
Natural Gas as a
Transportation Fuel
Energy Market Wild Card
April 16, 2013
China – Robotics
Automation for the People
December 5, 2012
Global Semiconductors
Chipping Away at
Returns
April 15, 2013
Global Emerging Market
Banks
On Track for Growth
November 19, 2012
38
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Social Gambling
Click Here to Play
November 14, 2012
Financials: CRE Funding
Shift
EU Shakes, US Selectively
Takes
May 25, 2012
Key Secular Themes in IT
The China Files
The Logistics Journey Is Just
Beginning
April 24, 2012
Any
Monetizing Big Data
September 4, 2012
Chemicals
‘Green is Good’ – The
Potential of Bioplastics
August 22, 2012
Solvency
The Long and Winding Road
March 23, 2012
MedTech & Services
Emerging Markets:
Searching for Growth
August 6, 2012
Wholesale & Investment
Banking Outlook
Decision Time for Wholesale
Banks
March 23, 2012
Commercial Aviation
Navigating a New Flight
Path
June 26, 2012
Banks Deleveraging and
Real Estate
Implication of a €400-700bn
Financing Gap
March 15, 2012
Mobile Data Wave
Who Dares to Invest, Wins
June 13, 2012
The China Files
China’s Appetite for Protein
Turns Global
October 25, 2011
Global Auto Scenarios
2022
Disruption and Opportunity
Starts Now
June 5, 2012
The US Healthcare Formula
Cost Control and True
Innovation
June 16, 2011
To find downloadable versions of these publications and information on Other Morgan Stanley reports, visit
www.morganstanley.com
39
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Disclosure Section
Morgan Stanley & Co. International plc, authorized by the Prudential Regulatory Authority and regulated by the Financial Conduct Authority and the
Prudential Regulatory Authority, disseminates in the UK research that it has prepared, and approves solely for the purposes of section 21 of the
Financial Services and Markets Act 2000, research which has been prepared by any of its affiliates. As used in this disclosure section, Morgan
Stanley includes RMB Morgan Stanley (Proprietary) Limited, Morgan Stanley & Co International plc and its affiliates.
For important disclosures, stock price charts and equity rating histories regarding companies that are the subject of this report, please see the
Morgan Stanley Research Disclosure Website at www.morganstanley.com/researchdisclosures, or contact your investment representative or
Morgan Stanley Research at 1585 Broadway, (Attention: Research Management), New York, NY, 10036 USA.
For valuation methodology and risks associated with any price targets referenced in this research report, please email
morganstanley.research@morganstanley.com with a request for valuation methodology and risks on a particular stock or contact your investment
representative or Morgan Stanley Research at 1585 Broadway, (Attention: Research Management), New York, NY 10036 USA.
Analyst Certification
The following analysts hereby certify that their views about the companies and their securities discussed in this report are accurately expressed and
that they have not received and will not receive direct or indirect compensation in exchange for expressing specific recommendations or views in
this report: Michael Jungling, Yukihiro Koike, Patrick Wood.
Unless otherwise stated, the individuals listed on the cover page of this report are research analysts.
Global Research Conflict Management Policy
Morgan Stanley Research has been published in accordance with our conflict management policy, which is available at
www.morganstanley.com/institutional/research/conflictpolicies.
Important US Regulatory Disclosures on Subject Companies
As of August 30, 2013, Morgan Stanley beneficially owned 1% or more of a class of common equity securities of the following companies covered in
Morgan Stanley Research: Fresenius Medical Care.
Within the last 12 months, Morgan Stanley managed or co-managed a public offering (or 144A offering) of securities of Medtronic Inc., Stryker
Corporation.
Within the last 12 months, Morgan Stanley has received compensation for investment banking services from Dentsply International Inc., Medtronic
Inc., Stryker Corporation.
In the next 3 months, Morgan Stanley expects to receive or intends to seek compensation for investment banking services from Dentsply
International Inc., Fresenius Medical Care, GN Store Nord A/S, Medtronic Inc., Nobel Biocare, Smith & Nephew, Sonova Holding AG, Stryker
Corporation, William Demant Holding, Zimmer Holdings, Inc..
Within the last 12 months, Morgan Stanley has received compensation for products and services other than investment banking services from
Dentsply International Inc., Fresenius Medical Care, Medtronic Inc., Stryker Corporation.
Within the last 12 months, Morgan Stanley has provided or is providing investment banking services to, or has an investment banking client
relationship with, the following company: Dentsply International Inc., Fresenius Medical Care, GN Store Nord A/S, Medtronic Inc., Nobel Biocare,
Smith & Nephew, Sonova Holding AG, Stryker Corporation, William Demant Holding, Zimmer Holdings, Inc..
Within the last 12 months, Morgan Stanley has either provided or is providing non-investment banking, securities-related services to and/or in the
past has entered into an agreement to provide services or has a client relationship with the following company: Dentsply International Inc.,
Fresenius Medical Care, Medtronic Inc., Smith & Nephew, Straumann Holding AG, Stryker Corporation.
Morgan Stanley & Co. LLC makes a market in the securities of Dentsply International Inc., Fresenius Medical Care, Medtronic Inc., Sirona Dental
Systems Inc., Smith & Nephew, Stryker Corporation, Zimmer Holdings, Inc..
The equity research analysts or strategists principally responsible for the preparation of Morgan Stanley Research have received compensation
based upon various factors, including quality of research, investor client feedback, stock picking, competitive factors, firm revenues and overall
investment banking revenues.
Morgan Stanley and its affiliates do business that relates to companies/instruments covered in Morgan Stanley Research, including market making,
providing liquidity and specialized trading, risk arbitrage and other proprietary trading, fund management, commercial banking, extension of credit,
investment services and investment banking. Morgan Stanley sells to and buys from customers the securities/instruments of companies covered in
Morgan Stanley Research on a principal basis. Morgan Stanley may have a position in the debt of the Company or instruments discussed in this
report.
Certain disclosures listed above are also for compliance with applicable regulations in non-US jurisdictions.
STOCK RATINGS
Morgan Stanley uses a relative rating system using terms such as Overweight, Equal-weight, Not-Rated or Underweight (see definitions below).
Morgan Stanley does not assign ratings of Buy, Hold or Sell to the stocks we cover. Overweight, Equal-weight, Not-Rated and Underweight are not
the equivalent of buy, hold and sell. Investors should carefully read the definitions of all ratings used in Morgan Stanley Research. In addition, since
Morgan Stanley Research contains more complete information concerning the analyst's views, investors should carefully read Morgan Stanley
Research, in its entirety, and not infer the contents from the rating alone. In any case, ratings (or research) should not be used or relied upon as
investment advice. An investor's decision to buy or sell a stock should depend on individual circumstances (such as the investor's existing holdings)
and other considerations.
Global Stock Ratings Distribution
(as of August 31, 2013)
For disclosure purposes only (in accordance with NASD and NYSE requirements), we include the category headings of Buy, Hold, and Sell
alongside our ratings of Overweight, Equal-weight, Not-Rated and Underweight. Morgan Stanley does not assign ratings of Buy, Hold or Sell to the
stocks we cover. Overweight, Equal-weight, Not-Rated and Underweight are not the equivalent of buy, hold, and sell but represent recommended
relative weightings (see definitions below). To satisfy regulatory requirements, we correspond Overweight, our most positive stock rating, with a buy
recommendation; we correspond Equal-weight and Not-Rated to hold and Underweight to sell recommendations, respectively.
Stock Rating Category
Overweight/Buy
Equal-weight/Hold
Not-Rated/Hold
Underweight/Sell
Total
Coverage Universe
Investment Banking Clients (IBC)
% of
% of % of Rating
Total
Count
Count Total IBC Category
978
1280
114
510
2,882
34%
44%
4%
18%
400
491
28
137
1056
38%
46%
3%
13%
41%
38%
25%
27%
40
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
Data include common stock and ADRs currently assigned ratings. An investor's decision to buy or sell a stock should depend on individual
circumstances (such as the investor's existing holdings) and other considerations. Investment Banking Clients are companies from whom Morgan
Stanley received investment banking compensation in the last 12 months.
Analyst Stock Ratings
Overweight (O). The stock's total return is expected to exceed the average total return of the analyst's industry (or industry team's) coverage
universe, on a risk-adjusted basis, over the next 12-18 months.
Equal-weight (E). The stock's total return is expected to be in line with the average total return of the analyst's industry (or industry team's) coverage
universe, on a risk-adjusted basis, over the next 12-18 months.
Not-Rated (NR). Currently the analyst does not have adequate conviction about the stock's total return relative to the average total return of the
analyst's industry (or industry team's) coverage universe, on a risk-adjusted basis, over the next 12-18 months.
Underweight (U). The stock's total return is expected to be below the average total return of the analyst's industry (or industry team's) coverage
universe, on a risk-adjusted basis, over the next 12-18 months.
Unless otherwise specified, the time frame for price targets included in Morgan Stanley Research is 12 to 18 months.
Analyst Industry Views
Attractive (A): The analyst expects the performance of his or her industry coverage universe over the next 12-18 months to be attractive vs. the
relevant broad market benchmark, as indicated below.
In-Line (I): The analyst expects the performance of his or her industry coverage universe over the next 12-18 months to be in line with the relevant
broad market benchmark, as indicated below.
Cautious (C): The analyst views the performance of his or her industry coverage universe over the next 12-18 months with caution vs. the relevant
broad market benchmark, as indicated below.
Benchmarks for each region are as follows: North America - S&P 500; Latin America - relevant MSCI country index or MSCI Latin America Index;
Europe - MSCI Europe; Japan - TOPIX; Asia - relevant MSCI country index.
.
Important Disclosures for Morgan Stanley Smith Barney LLC Customers
Citi Research publications may be available about the companies or topics that are the subject of Morgan Stanley Research. Ask your Financial Advisor or use
Research Center to view any available Citi Research publications in addition to Morgan Stanley research reports.
Important disclosures regarding the relationship between the companies that are the subject of Morgan Stanley Research and Morgan Stanley Smith Barney LLC or
Morgan Stanley or any of their affiliates, are available on the Morgan Stanley Wealth Management disclosure website at
www.morganstanley.com/online/researchdisclosures.
For Morgan Stanley specific disclosures, you may refer to www.morganstanley.com/researchdisclosures.
Each Morgan Stanley Equity Research report is reviewed and approved on behalf of Morgan Stanley Smith Barney LLC. This review and approval is conducted by the
same person who reviews the Equity Research report on behalf of Morgan Stanley. This could create a conflict of interest.
Other Important Disclosures
Morgan Stanley & Co. International PLC and its affiliates have a significant financial interest in the debt securities of Dentsply International Inc., Fresenius Medical Care,
Medtronic Inc., Stryker Corporation.
Morgan Stanley is not acting as a municipal advisor and the opinions or views contained herein are not intended to be, and do not constitute, advice within the meaning
of Section 975 of the Dodd-Frank Wall Street Reform and Consumer Protection Act.
Morgan Stanley produces an equity research product called a "Tactical Idea." Views contained in a "Tactical Idea" on a particular stock may be contrary to the
recommendations or views expressed in research on the same stock. This may be the result of differing time horizons, methodologies, market events, or other factors.
For all research available on a particular stock, please contact your sales representative or go to Matrix at http://www.morganstanley.com/matrix.
Morgan Stanley will make certain research products and announcements available only on the Matrix platform. For access to Matrix, please contact your sales
representative or go to Matrix at http://www.morganstanley.com/matrix.
Any access and/or use of Morgan Stanley Research are subject to Morgan Stanley's Terms of Use (http://www.morganstanley.com/terms.html). By accessing and/or
using Morgan Stanley Research, you are indicating that you have read and agree to be bound by our Terms of Use (http://www.morganstanley.com/terms.html). In
addition you consent to Morgan Stanley processing your personal data and using cookies in accordance with our Privacy Policy and our Global Cookies Policy
(http://www.morganstanley.com/privacy_pledge.html), including for the purposes of setting your preferences and to collect readership data so that we can deliver better
and more personalised service and products to you. To find out more information about how Morgan Stanley processes personal data, how we use cookies and how to
reject cookies see our Privacy Policy and our Global Cookies Policy (http://www.morganstanley.com/privacy_pledge.html).
If you do not agree to our Terms of Use and/or if you do not wish to provide your consent to Morgan Stanley processing of your personal data or using cookies please do
not access our research.
Morgan Stanley Research does not provide individually tailored investment advice. Morgan Stanley Research has been prepared without regard to the circumstances
and objectives of those who receive it. Morgan Stanley recommends that investors independently evaluate particular investments and strategies, and encourages
investors to seek the advice of a financial adviser. The appropriateness of an investment or strategy will depend on an investor's circumstances and objectives. The
securities, instruments, or strategies discussed in Morgan Stanley Research may not be suitable for all investors, and certain investors may not be eligible to purchase or
participate in some or all of them. Morgan Stanley Research is not an offer to buy or sell any security/instrument or to participate in any trading strategy. The value of and
income from your investments may vary because of changes in interest rates, foreign exchange rates, default rates, prepayment rates, securities/instruments prices,
market indexes, operational or financial conditions of companies or other factors. There may be time limitations on the exercise of options or other rights in
securities/instruments transactions. Past performance is not necessarily a guide to future performance. Estimates of future performance are based on assumptions that
may not be realized. If provided, and unless otherwise stated, the closing price on the cover page is that of the primary exchange for the subject company's
securities/instruments.
The fixed income research analysts, strategists or economists principally responsible for the preparation of Morgan Stanley Research have received compensation
based upon various factors, including quality, accuracy and value of research, firm profitability or revenues (which include fixed income trading and capital markets
profitability or revenues), client feedback and competitive factors. Fixed Income Research analysts', strategists' or economists' compensation is not linked to investment
banking or capital markets transactions performed by Morgan Stanley or the profitability or revenues of particular trading desks.
Morgan Stanley Research is not an offer to buy or sell or the solicitation of an offer to buy or sell any security/instrument or to participate in any particular trading strategy.
The "Important US Regulatory Disclosures on Subject Companies" section in Morgan Stanley Research lists all companies mentioned where Morgan Stanley owns 1%
or more of a class of common equity securities of the companies. For all other companies mentioned in Morgan Stanley Research, Morgan Stanley may have an
investment of less than 1% in securities/instruments or derivatives of securities/instruments of companies and may trade them in ways different from those discussed in
Morgan Stanley Research. Employees of Morgan Stanley not involved in the preparation of Morgan Stanley Research may have investments in securities/instruments or
derivatives of securities/instruments of companies mentioned and may trade them in ways different from those discussed in Morgan Stanley Research. Derivatives may
be issued by Morgan Stanley or associated persons.
With the exception of information regarding Morgan Stanley, Morgan Stanley Research is based on public information. Morgan Stanley makes every effort to use reliable,
comprehensive information, but we make no representation that it is accurate or complete. We have no obligation to tell you when opinions or information in Morgan
Stanley Research change apart from when we intend to discontinue equity research coverage of a subject company. Facts and views presented in Morgan Stanley
Research have not been reviewed by, and may not reflect information known to, professionals in other Morgan Stanley business areas, including investment banking
personnel.
Morgan Stanley Research personnel may participate in company events such as site visits and are generally prohibited from accepting payment by the company of
associated expenses unless pre-approved by authorized members of Research management.
Morgan Stanley may make investment decisions or take proprietary positions that are inconsistent with the recommendations or views in this report.
41
MORGAN STANLEY RESEARCH
September 05, 2013
MedTech: 3D Printing – A Solution for Innovation
To our readers in Taiwan: Information on securities/instruments that trade in Taiwan is distributed by Morgan Stanley Taiwan Limited ("MSTL"). Such information is for
your reference only. The reader should independently evaluate the investment risks and is solely responsible for their investment decisions. Morgan Stanley Research
may not be distributed to the public media or quoted or used by the public media without the express written consent of Morgan Stanley. Information on
securities/instruments that do not trade in Taiwan is for informational purposes only and is not to be construed as a recommendation or a solicitation to trade in such
securities/instruments. MSTL may not execute transactions for clients in these securities/instruments. To our readers in Hong Kong: Information is distributed in Hong
Kong by and on behalf of, and is attributable to, Morgan Stanley Asia Limited as part of its regulated activities in Hong Kong. If you have any queries concerning Morgan
Stanley Research, please contact our Hong Kong sales representatives.
Morgan Stanley is not incorporated under PRC law and the research in relation to this report is conducted outside the PRC. Morgan Stanley Research does not
constitute an offer to sell or the solicitation of an offer to buy any securities in the PRC. PRC investors shall have the relevant qualifications to invest in such securities
and shall be responsible for obtaining all relevant approvals, licenses, verifications and/or registrations from the relevant governmental authorities themselves.
Morgan Stanley Research is disseminated in Brazil by Morgan Stanley C.T.V.M. S.A.; in Japan by Morgan Stanley MUFG Securities Co., Ltd. and, for Commodities
related research reports only, Morgan Stanley Capital Group Japan Co., Ltd; in Hong Kong by Morgan Stanley Asia Limited (which accepts responsibility for its contents);
in Singapore by Morgan Stanley Asia (Singapore) Pte. (Registration number 199206298Z) and/or Morgan Stanley Asia (Singapore) Securities Pte Ltd (Registration
number 200008434H), regulated by the Monetary Authority of Singapore (which accepts legal responsibility for its contents and should be contacted with respect to any
matters arising from, or in connection with, Morgan Stanley Research); in Australia to "wholesale clients" within the meaning of the Australian Corporations Act by
Morgan Stanley Australia Limited A.B.N. 67 003 734 576, holder of Australian financial services license No. 233742, which accepts responsibility for its contents; in
Australia to "wholesale clients" and "retail clients" within the meaning of the Australian Corporations Act by Morgan Stanley Wealth Management Australia Pty Ltd (A.B.N.
19 009 145 555, holder of Australian financial services license No. 240813, which accepts responsibility for its contents; in Korea by Morgan Stanley & Co International
plc, Seoul Branch; in India by Morgan Stanley India Company Private Limited; in Indonesia by PT Morgan Stanley Asia Indonesia; in Canada by Morgan Stanley Canada
Limited, which has approved of and takes responsibility for its contents in Canada; in Germany by Morgan Stanley Bank AG, Frankfurt am Main and Morgan Stanley
Private Wealth Management Limited, Niederlassung Deutschland, regulated by Bundesanstalt fuer Finanzdienstleistungsaufsicht (BaFin); in Spain by Morgan Stanley,
S.V., S.A., a Morgan Stanley group company, which is supervised by the Spanish Securities Markets Commission (CNMV) and states that Morgan Stanley Research has
been written and distributed in accordance with the rules of conduct applicable to financial research as established under Spanish regulations; in the US by Morgan
Stanley & Co. LLC, which accepts responsibility for its contents. Morgan Stanley & Co. International plc, authorized by the Prudential Regulatory Authority and regulated
by the Financial Conduct Authority and the Prudential Regulatory Authority, disseminates in the UK research that it has prepared, and approves solely for the purposes
of section 21 of the Financial Services and Markets Act 2000, research which has been prepared by any of its affiliates. Morgan Stanley Private Wealth Management
Limited, authorized and regulated by the Financial Conduct Authority, also disseminates Morgan Stanley Research in the UK. Private UK investors should obtain the
advice of their Morgan Stanley & Co. International plc or Morgan Stanley Private Wealth Management representative about the investments concerned. RMB Morgan
Stanley (Proprietary) Limited is a member of the JSE Limited and regulated by the Financial Services Board in South Africa. RMB Morgan Stanley (Proprietary) Limited is
a joint venture owned equally by Morgan Stanley International Holdings Inc. and RMB Investment Advisory (Proprietary) Limited, which is wholly owned by FirstRand
Limited.
The information in Morgan Stanley Research is being communicated by Morgan Stanley & Co. International plc (DIFC Branch), regulated by the Dubai Financial Services
Authority (the DFSA), and is directed at Professional Clients only, as defined by the DFSA. The financial products or financial services to which this research relates will
only be made available to a customer who we are satisfied meets the regulatory criteria to be a Professional Client.
The information in Morgan Stanley Research is being communicated by Morgan Stanley & Co. International plc (QFC Branch), regulated by the Qatar Financial Centre
Regulatory Authority (the QFCRA), and is directed at business customers and market counterparties only and is not intended for Retail Customers as defined by the
QFCRA.
As required by the Capital Markets Board of Turkey, investment information, comments and recommendations stated here, are not within the scope of investment
advisory activity. Investment advisory service is provided in accordance with a contract of engagement on investment advisory concluded between brokerage houses,
portfolio management companies, non-deposit banks and clients. Comments and recommendations stated here rely on the individual opinions of the ones providing
these comments and recommendations. These opinions may not fit to your financial status, risk and return preferences. For this reason, to make an investment decision
by relying solely to this information stated here may not bring about outcomes that fit your expectations.
The trademarks and service marks contained in Morgan Stanley Research are the property of their respective owners. Third-party data providers make no warranties or
representations relating to the accuracy, completeness, or timeliness of the data they provide and shall not have liability for any damages relating to such data. The
Global Industry Classification Standard (GICS) was developed by and is the exclusive property of MSCI and S&P. Morgan Stanley bases projections, opinions, forecasts
and trading strategies regarding the MSCI Country Index Series solely on public information. MSCI has not reviewed, approved or endorsed these projections, opinions,
forecasts and trading strategies. Morgan Stanley has no influence on or control over MSCI's index compilation decisions. Morgan Stanley Research or portions of it may
not be reprinted, sold or redistributed without the written consent of Morgan Stanley. Morgan Stanley research is disseminated and available primarily electronically, and,
in some cases, in printed form. Additional information on recommended securities/instruments is available on request.
Morgan Stanley Research, or any portion thereof may not be reprinted, sold or redistributed without the written consent of Morgan Stanley.
Morgan Stanley Research is disseminated and available primarily electronically, and, in some cases, in printed form.
Additional information on recommended securities/instruments is available on request.
L20011
42
MORGAN STANLEY RESEARCH
MORGAN STANLEY BLUE PAPER
The Americas
1585 Broadway
New York, NY 10036-8293
United States
Tel: +1 (1)212 761 4000
© 2013 Morgan Stanley
Europe
20 Bank Street, Canary Wharf
London E14 4AD
United Kingdom
Tel: +44 (0)20 7425 8000
Japan
4-20-3 Ebisu, Shibuya-ku
Tokyo 150-6008
Japan
Tel: +81 (0)3 5424 5000
Asia/Pacific
1 Austin Road West
Kowloon
Hong Kong
Tel: +852 2848 5200