Vol 09 / Issue 02 | Mar - Apr 2010
advertisement

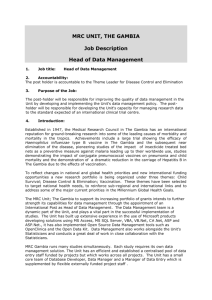
TAMANEWSLETTER Medical Research Council (UK) The Gambia TAMA: Wolof. n. a talking drum VOL: 09 ISSUE: 02 / Mar - Apr 2010 New vaccines showcased at Sukuta On Thursday 29th April 2010, Sukuta Health Centre opened its doors to the community and other key stakeholders in a programme themed ‘Working Together with the Community: Novel Vaccine Studies’. The programme was part of the efforts of the MRC field site in Sukuta to disseminate the findings of the various studies that have taken place at the site. The people, leaders of the community and MRC were brought together to foster a stronger relationship on ways of achieving better health through meaningful participation in future studies. Next page Communicating MRC’s vaccine studies in Sukuta: Saihou Bobb (field assistant); Dr Katie Flanagan, Head of Infant Immunology Team, MRC (UK) The Gambia WAPHIR: paving the way for a sub-regional HIV research network Story page 04 06 PneumoWAR Assessing the tools to fight meningitis 188 In conversation with Professor Brigid Heywood, OU Pro Vice Chancellor 20 MRC The Gambia: Centre of Excellence for PhD training 08 News from Caio 11 News from Keneba 13 News from Basse 15 Recent Unit Publications 26 HR News » Youngee Choi’s diary » Going to Caio: be prepared » Training: a Keneba initiative » SANTE: Spraying And Nets Towards malaria Elimination » » » » » Appraisals GEM and Team Awards Restructuring New staff & leavers Clinical Services staff say farewell New vaccines showcased at Sukuta Continued from page 1 The Open Day programme attracted more than 200 participants from within and outside The Gambia. The forum featured feedback from MRC scientists on various vaccine studies that have either taken place or are ongoing in Sukuta, or are planned for the near future: MVA85A: a new vaccine against TB The conventional vaccine against tuberculosis - BCG – is known to have limitations, particularly in this setting. This has led to the search for a new vaccine to reduce the burden of disease and death cause by TB. MRC (UK) The Gambia has successfully conducted a phase I study of a new TB vaccine called MVA85A. The vaccine was developed by researchers based in Oxford, and the work is being led by Dr Martin Ota and his team at MRC (UK) The Gambia. The findings showed that the new TB vaccine is safe and produces immune responses in Sukuta children, and does not interfere with responses to other vaccines also given in early infancy. These results provide important information required for further testing of this vaccine for efficacy in protecting against tuberculosis. Prevention of mother-to-child transmission of HIV An ongoing study is investigating how the human body responds to a novel HIV vaccine (MVA.HIVA) that aims to prevent transmission of HIV from mother-to-child during breastfeeding. This study, led in The Gambia by Dr Katie Flanagan and her team, is the first phase in the evaluation of this vaccine in healthy under-1 year old children from Sukuta. Similar studies are also being carried out in Nairobi, Kenya. The group that developed the vaccine, led by Professor Tomas Hanke, is based at Oxford University and was present at the Sukuta Open Day. This study is funded by the EU-European Developing Countries Clinical Trials Partnership, and includes capacity building elements such as staff training and the renovation of Sukuta Health Centre which took place in 2009. 02 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 The search for a malaria vaccine A novel malaria vaccine trial is soon to commence at Sukuta Health Centre. Malaria is responsible for more than 1 million deaths and between 300 and 500 million clinical cases each year, affecting mainly women and children in Sub-Saharan Africa. Presently, there is no effective vaccine against the malaria parasite, and this trial aims to test the safety and immune response to this candidate vaccine in adults, children and infants. The trial is being led by Dr Kalifa Bojang and his team at Sukuta Health Centre. The work is being funded by the EDCTP and the developers of the vaccine are based at Oxford University. Students of Sukuta Upper and Lower Basic Schools attending the Open Day programme MRC wishes to acknowledge the value and importance of the Sukuta community, the local government hospital staff, especially Ms Sally Savage – Principal Nursing Officer at Sukuta Health Centre and the Ministry of Health in working together in order to carry out these important vaccine trials. This is part of the overall global effort to develop safe and effective vaccines against the 3 major killer diseases, malaria, TB and HIV which will save millions of children’s lives. Professor Tumani Corrah officially opens the new EDCTP-funded building at Sukuta Health Paramount Chief, Alhaji Demba Sanyang Dr Kalifa Bojang, Principal Investigator, Sukuta malaria vaccine trial Ms Sally Savage (Aunty Sally), Principal Nursing Officer, Sukuta Health Centre remains a vital and active supporter of MRC’s studies at the Health Centre. Presenters at Sukuta Open Day: From left: Dr Muhammed Afolabi, Ms Jainaba Njie-Jobe, Dr Sarah Burl, Dr Adesina Owolabi and Dr Jane Adetifa MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 03 WAPHIR: paving the way for a sub-regional HIV research network Recently, Dr Assan Jaye received the welcome news that he, together with colleagues from Dakar and Bissau, won a 1.8 million Canadian dollar capacity building grant from the Global Health Research Initiative, Canada. The West African bid was one of four that won funding; the other winners were from Uganda, Kenya and South Africa. The award comes into effect in July 2010, and as Dr Jaye explains here, it will enhance MRC The Gambia’s plans to build a robust network of sub-regional partners. Building a shared resource ‘The grant is a four-year consortium award for the development of capacity in HIV clinical trials in Africa.’ Explains Dr Jaye. ‘Working with partners from Dakar, Bissau, Denmark, Oxford, Toronto and Montreal, we plan to amalgamate our regional cohorts and resources, with Dakar as the centre.’ ‘This West African Platform for HIV Intervention Research (WAPHIR) will develop partners’ biobank capabilities, expand population cohorts and pool shared resources. The partners are bringing a lot of expertise to the table: MRC has long been a hub for laboratory and other training Canadian Group in the sub-region; the Bacteriology and Virology groups at Cheikh Anta Diop University (Dakar) manage the large sex workers cohort and HIV laboratory platform; and Professor Pap Salif Sowe’s research and training centre of tropical infectious diseases in Dakar has extensive experience on clinical management of an ambulatory cohort. With the addition of the Caio cohort biobank resources and the Bissau cohort, we are poised to create an HIV network, by pooling resources and preparing the ground for vaccine trials and other research.’ ‘We intend to develop each site’s biobank resources. Each will retain their own biobanks, but we’ll be amalgamating the data at one source (Dakar). Access to data will be UCAD Senegal Laboratory Platforms Oxford Clinical Trials Support HIV cohorts bio-resources & Unified Database MRC Gambia BHP Guinea Bissau Tecnical Leadership Training & Research Danish Group 04 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 West African Platform for HIV Intervention Research (WAPHIR) A model for capacity strengthening WAPHIR: paving the way for a sub-regional HIV research network shared, with requests being made through a steering committee and our own ethics committee.’ Capacity ‘The grant includes capacity building components in laboratory management, clinical trials management, biobank and biomedical engineering management. We need to make sure that each of the sites has the ability to contribute on an equal footing. For example, Guinea Bissau is not as advanced as Dakar in terms of research expertise and infrastructure, so this proposal will really help them to participate fully in joint regional research initiatives.’ Towards improved laboratories ‘The grant will enable us to develop certain laboratory platforms for clinical trials such as cellular immunology. We’ll also be focusing on the quality processing of samples, good laboratory practice and quality management in general. We intend to transfer some basic technologies such as HLA typing, and we’ll be working on the development of Dakar’s virology platform as the centre for this. We also intend to share our successful biobank and biomedical engineering models with Dakar.’ Training ‘The award’s staff development component includes training to master’s level in areas such as clinical trials, immunology and virology. There are also PhD and post doc opportunities.’ A timely award ‘MRC UK has endorsed the setting up of a West African research network in principle. However, it would have been a massive challenge to start off without this grant, which will do so much to develop sub-regional research capacity. I hope that we will be able to achieve a lot in the next four years. I am very proud of this proposal and our success in winning this funding. And I’d like to end by thanking Professor Tumani Corrah for all his encouragement and support. He kept on urging me to be persistent and not to give up!’ Sub-regional partners fine tuning their vision for an HIV 2 network. From left: Ms Astou Cissé (Finance Manager, UCAD), Mr Abdulaziz Hane (Programme Officer, UCAD), Professor Souleymane Mboup (UCAD), Professor Tumani Corrah and Dr Assan Jaye (MRC The Gambia) MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 05 PneumoWAR: assessing the tools to fight meningitis Martin Antonio, Sheikh Jarju and Jacob Otu In April 2010 a team headed by Dr Martin Antonio made a site assessment visit to the Royal Victoria Teaching Hospital, Banjul, where they met Mr Pa Momodou C Jaye (Laboratory Manager), Ms Nelly Lloyd Evans (outgoing Head of Microbiology), Mr Baba K Fofana (new Head of Microbiology) and key hospital personnel who have a direct role in the PneumoWAR disease surveillance project. The purpose of the visit included an assessment of the hospital’s capacity to isolate and identify the three pathogens in question (S. pneumoniae, H. influenzae b and N. meningitidis). Sensitisation meetings with other stakeholders within this PneumoWAR site were also held. RVTH was given a questionnaire for the site assessment, which included questions on the use of standard operating procedures, and the visiting team was pleased to note that an SOP document was in place for the laboratories. Basic requirements, supplies and equipment were another area included in the questionnaire, and RVTH was found to have most of the essential reagents needed for the isolation and identification of the pathogens of PneumoWAR. The MRC team was received by Dr Tamsir Mbowe, the Chief Medical Director of the hospital. Dr Antonio gave Dr Mbowe a breakdown of PneumoWAR’s objectives and activities in the sub-region and its anticipated benefits to the community. The MRC Regional Reference Laboratory team has shared the recommendations arising from this visit with the RVTH team, and will continue to offer appropriate support and advice going forward. Jacob Otu (MRC TB group) shown above demonstrating laboratory techniques to sub-regional participants at the PneumoWAR workshop held at MRC The Gambia, February 2010 06 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 The Paediatric Bacterial Meningitis (PBM) Network is a sentinel based surveillance in selected countries that was established in 2001 with the support of WHO. The specific objectives of this network are to: • • • • Dr Martin Antonio, Unit Microbiologist and Principal Investigator, Pneumowar Provide evidence of Hib and Pneumococcal disease burden Generate data on S. pneumoniae serotypes circulating in the AFR region Support advocacy for the introduction of Hib and Pneumococcal vaccines Provide a framework to evaluate the impact following vaccine introduction WHO and partners are supporting a subregional reference laboratory (RRL) at the MRC (UK) The Gambia as part of regional efforts to strengthen pneumococcal surveillance in the West African region. The Regional Reference Laboratory (RRL) is working closely with the Ministries of Heath involved in WHOsupported PBM Network in 22 countries (selected on the basis of performance over the past three years, as well as likelihood of early uptake of new Pneumococcal vaccine). Ms Nelly Lloyd-Evans (outgoing Head of Microbiology, RVTH) and PneumoWAR workshop trainer. MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 07 News from Caio Tim Vincent Youngee Choi’s diary Youngee Choi is a 4th year medical student from Washington University in St Louis (USA) who came to Caio last autumn for a research project. Here she shares her experience. Coming to Caio was my first time in Africa. I came to investigate the neurologic sequelae of HIV-2 by conducting clinical neurologic exams. However, my two months in Caio provided me with so much more – experience in handling primary care issues as well as learning about rural Guinean life and culture. The latter is what I think will stick with me for years to come. Below are some highlights from my two months there. Settling in. Caio field site was set up in the late 1980s, after a French doctor working with commercial sex workers in a nearby town noticed that a high prevalence of HIV-2 women originated from Caio. A complete survey of Caio from 1988-89 showed that it has one of the highest rates of HIV-2 in the world; this is the reason why it was the perfect site for my research project. The local MRC staff are lots of fun, and they proved very adept at evaluating our study participants. In particular, I got to know Moises, one of the staff who plays the guitar. He and I had several flute-guitar jam sessions, and I also taught Moises the basics of playing the flute! October. From mid-October to November, traditional fighting takes place between fighters of Caio’s ten zones. It looks very much like wrestling, the goal being to put one’s opponent on his back. The fight takes place in a temporary enclosure made of wooden poles interlaced with string to form a ring. Drummers set up on one end of the ring, while referees go running around the periphery and blowing plastic whistles to excite the crowd. Little boys have their own fights at the edge of the ring, and are thwacked away by the refs with branches every so often. There isn’t really one clear winner. People take turns at fighting without any sort of elimination. First the men have their rounds of fights, followed by the women. There is no way I would want to end up fighting any of the women in Caio – they are quite buff! November. In Caio it has become tradition to have a dinner at the end of a study to thank the staff. Seeing as Thanksgiving fell on my last few days there, we decided to use this occasion as the thank you dinner. So we – a Brit (Tim Vincent), Korean (a US permanent resident), 20 Guineans and two guests from Scotland and Holland – sat down to an American Thanksgiving dinner! We feasted on baked chicken, mashed potatoes, baked squash, peanut butter cookies, doughnuts and a traditional Guinean dish of fish and rice! December 1. We celebrated World AIDS Day in Caio. Local schools put on plays about HIV, and health officials gave speeches emphasizing the availability of free HIV testing and counseling. There was also traditional dancing, a poetry contest, a condom demonstration and tug-of-war. A cow was slaughtered in honour of AIDS Day to feed all the schools and guests. The day ended with a party with the staff and their families. It was a wonderful way to spend my last evening in Caio. I really grew to love Caio and my coworkers, and I hope to be able to return one day. Youngee guiding Moises Gomez on the flute 08 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 News from Caio Going to Caio: be prepared To maximize visitors’ enjoyment of Caio, Tim Vincent and Carla van Tienen have provided a checklist to help you plan your stay. What’s in the visitors’ accommodation? Three separate bedrooms, each with two beds. Lighting is by generator during the day and there is solar powered light at night (no appliances at night). Sheets, pillows, pillow cases and soap are provided. One bathroom serves the three rooms with a toilet, hand basin and shower with hot and cold running water. There’s a kitchen with basic pots and pans, cutlery and crockery. There’s a gas cooker and a gas powered fridge/ freezer which is very efficient and very cold: the freezer section will hold about 10kg of frozen produce. Outside there’s a seating area with a dining table and chairs, plus armchairs and sofas for lounging. We’ve also got two or three bicycles for those who wish to explore What must you bring? Food supplies, insect repellent, a hand torch, books to read and walking shoes. You can get basic items such as oil, sugar, powdered milk, onions, chillies, bread, a few in-season vegetables, biscuits and beer/soft drinks in the village. Fish is available most days but often only the local cat fish. You should aim to bring meat, fresh fruit and vegetables, cereals, juices etc with you. What medicines should you pack? Obviously for visitors requiring treatment we have a good supply of essential medicines at the field station. There are also a couple of small pharmacies in the village with the basics. One thing we don't have is loperamide 2mg (imodium), and it’s always a good idea to travel with this. Also, we don't currently have a supply of coartem for malaria. We have chloraquine, fansidar and quinine but in the unfortunate event that you get malaria you might want to have an emergency treatment pack with you. Is the water drinkable from the tap? The water at the field station is from a sealed borehole on the site and is pumped up into a tank. The borehole is serviced regularly (every 5 years) and we have a good supply of clean drinking water direct from the tap (though it might be a bit warm). What’s the currency? Guinea-Bissau is in the CFA zone along with Senegal, Mali and others. The current exchange (as at 1/04/2010) is about 725 FCFA to the pound and about 250 dalasi to 5,000 FCFA. Of course this constantly changes but this has been the average over the last 6 months or so. What can visitors bring for the project or the village? The staff are always pleased to receive anything to do with the MRC, such as pens, pencils, T-shirts etc. So, if you're here doing a study and you have any 'give-aways' they would be very much appreciated. In terms of the village, just be prepared to join in with any activities going on, such as village meetings or ceremonies. It's always very much appreciated by the locals when visitors take part in, and take an interest in the culture. When is the best time to visit Caio? Any time is good to visit Caio, though if you're worried about road conditions, it’s probably best to stay away in the rainy season, July/August/September being the worst months. The best months temperature-wise are probably pretty much the same as The Gambia. From November through to March the humidity is low, the sun is shining and the nights are cool. Can you eat out in Caio? There are currently three establishments in the village which provide food, situated near the Bush Taxi stop/ mobile phone antenna. All will provide a rice dish and it depends on the availability what you get with it - chicken, fish, bush meat etc. Usually these dishes are 500 FCFA a plate. At this time of year you may also be lucky to get salad as well. Are there any cultural/behavioural rules you should be aware of? People generally don't like strangers taking their photos without asking. Always greet people when out and about. If you're introduced to a group, greet everyone by shaking their hand. If you're sharing food from a bowl, remember only use your right hand and never pass food to anyone with your left (pretty much as in The Gambia and elsewhere in West Africa). Unlike The Gambia drinking alcohol is a way of life here and you will most likely be offered local wine at some point. Even if you don't want to drink it's polite to take the drink and spill a little on the ground (for the spirits) before passing it on. MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 09 News from Caio Joaquim da Silva (Djoca) - Laboratory Technician/ nurse, HIV pre and post-test counsellor, ARV counsellor Second row: Antonio Pina Gouveia (Pina) - Mechanic Claudette Mendes - Domestic staff Third row: Aliu Sanha - Maintenance Julio Mendes (Mpas) - Ground staff Silvina da Silva - Fieldworker (Children and pregnancies) Ana Mendes - Domestic staff Fourth row: Fernando Camara - Fuel depot Charles Djata - Driver Front row: Tim Vincent - Station Head Alberto Salinha (Jordao) - Staff supervisor, data entry Elsa Fereira - Fieldworker (children and pregnancies) Luis Cubaba (vega) - Stores and communications Eva Mauricio - Domestic staff Kneeling: Nino da Costa - Ground staff Caio Staff. Back row: Alfredo da Costa (Djipan) - Fieldworker (census), HIV pre and post-test counsellor, ARV counsellor and fieldworker Justiano Gomes - Fieldworker (census) Carla and Tim on the benefits of conducting research in Caio • • • • • • It’s small scale so you can arrange and delegate all your work directly without loads of paperwork and bureaucracy It has a very dedicated and enthusiastic team The field site has a very good relationship with the village and the village elderly There’s an excellent database with up to date census data of the whole village that can easily be linked to the census data from the capital and all past studies. Caio has produced more than 25 papers in international peer reviewed journals You’ll be made to feel at home immediately, giving you an unforgettable experience. Caio’s uniqueness The community cohort of HIV patients (primarily HIV-2) has been followed for over 20 years. In addition, due to 10 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 the close ties with the Bandim Health Project in Bissau, there is a very thorough demographic system which is continually updated by the team of fieldworkers, with census data, vaccination and health status of children, and follow-up of pregnant women. The best equipped laboratory in Guinea Bissau The lab is equipped with a biohazard cabinet, 2 centrifuges, mixer and roller, CO2 incubator, 2 gas powered fridge/ freezers (freezer to -20C), 2 solar powered chest freezers to -20C, 1 small freezer to -70C, 1 microscope, and 1 partec flow cytometer for CD4 counts and percentages. A separate laboratory has been built for clinical analyses, but needs equipment. Connected to the outside world The office can provide computing facilities with printers and access to the internet via the local mobile GPRS system. News from Keneba Yankuba Sawo Training: a Keneba initiative The Keneba local training committee came into existence in June 2009. This was in response to requests for an independent body that would meet periodically to discuss staff training needs and consider applications. In addition, the committee offers career development advice to staff, helping them to identify courses that are both relevant to the unit’s research interests and at the same time contribute to the individual’s career progression. The membership of the committee cuts across all grades and sections of staff, and includes union representation. The committee meets quarterly to consider training applications. Ad hoc meetings are also held, should the need arise. Since the committee’s inception, there has been a great deal of interest in pursuing a variety of training opportunities. During the last financial year, the committee received 10 applications and approved sponsorship for 8 candidates. The majority of the courses approved were distance learning programmes; 2 short courses overseas were also sponsored. In addition, the committee approved a group IT training programme for various categories of staff and English proficiency classes for the non-literate staff. The Keneba Training Committee Here we meet two recent recipient’s of Keneba’s training funds. Bakary Sarr ‘A nurse by profession, I started working with MRC Keneba in June 2003. I am responsible for the nursing care of TB patients at our field station and I also attend the quarterly meetings of the National TB programme where we present and discuss the TB data from all the TB diagnostic centres in the country. Currently I am doing a Modular Diploma on Tuberculosis through an institute called Education for Health in the UK. I feel that this course will help me to improve the nursing care that I provide. In addition, The Nutrition group collaborates closely with various sectors including the Ministry of Health by providing primary health care services at the station, including TB diagnosis and care. Through this collaboration, the station was recently opened as an official TB diagnostics centre. This is a very big benefit for the station, because it will enable us to send our TB data directly to the National TB Programme and, through them, to international organizations. Through such international exposure, we could one day benefit from TB/nutrition projects. One day I hope to be a high calibre research nurse and conduct my own research, so this course is definitely relevant and useful. I have 100% confidence in the local training committee, because the members were selected by us and every section in the field station is represented. The committee is open to dialogue any time you need them and I admire that. Mustapha Ceesay ‘I joined the MRC in 1990 as a field assistant. I worked with short projects before joining the Calcium, Vitamin D and Bone Health Group. Because of my key involvement in MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 11 News from Keneba projects I was promoted to senior field assistant and then supervisor. I am now a research assistant in the Calcium Group. My main area is operating sophisticated bone imaging equipment (DXA, pQCT, X-ray and more recently the jumping mechanography). This equipment performs different but complimentary measurements, including bone, muscle and body composition measurements at different skeletal sites. I am currently studying for the Advanced Anatomy and Physiology level 3 Diploma by distance learning with Essential Training Solutions. This course is directly linked to my bone imaging work. A better understanding of the body parts and how they function will enable me to appreciate what we are doing as a research group. The course will also enable me to contribute to the data interpretation and discussions on new project areas. As a Bone Health Research Assistant, I feel this course will benefit myself and the Nutrition group by helping me to understand and carry out my work more effectively and efficiently and therefore contribute to the overall success of the project. I will be able to train other colleagues and help them do their work well. Also, the knowledge gained from this course will help me explain better to study participants what we are trying to do and the importance of our work to their health and global health in general. I aim to complete this course successfully and proceed to do the advanced level and possibly a master’s degree. What I like most about the committee is their encouragement and motivation for staff to take up courses and develop themselves. They want everyone to benefit from this training, without exception. And that’s important because good science cannot be achieved without well trained staff. To give a balanced perspective, we asked an applicant for training funds who was not successful on this occasion to give his opinion on the workings of the committee. Three of the recent beneficiaries of Keneba’s training fund. From left: Bakary Sarr, Yankuba Sawo, Michael Mendy 12 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 Lamin Sanyang ‘I have worked with the MRC since October 1988. I started as a field worker and I am now a senior field worker. I have worked in many projects, collecting data, administering supplements, collecting biological samples, recruiting subjects etc. I submitted an application for project management training. I felt this was very relevant to my job, as project management is all about organizing work activities and making sure the work is implemented as planned by the principal investigator. Project management also looks at working with and managing staff and other people, skills that I feel are relevant to me, as my ambition is to be a project manager, working closely with principal investigators. Even though I wasn’t successful, I am satisfied with the way selections were made. The committee has been helpful and given me sound advice. I realize that I had a problem in identifying the appropriate level of project management training and that was why the committee did not approve my application. So now I am searching for an appropriate course from the internet and I intend to apply to the committee again.’ News from Basse Dr Margaret Pinder SANTE: Spraying And Nets Towards malaria Elimination Can Indoor Residual Spraying provide additional protection against clinical malaria over current best practice? That’s the question being posed by a new study headed by Professor Steve Lindsay (Disease Control & Vector Biology Unit, LSHTM), and led in The Gambia by Dr Margaret Pinder (Epidemiologist). The field work, which commenced recently, is based in Basse and the surrounding villages spread over the Upper River Region. Margaret is responsible for liaising with the National Malaria Control Programme and local communities, developing SOPs, management of field teams, dayto-day management of the research clinician and data collection, including PCR, data cleaning, analysis and manuscript preparation. Here she explains the potential contribution of SANTE to MRC The Gambia’s disease control and elimination research efforts. The study questions whether current ‘best practice’ is indeed best. Yes. The current WHO recommendations for best practice for malaria control are that everyone at risk of getting malaria should sleep under an insecticide treated bed net (LLIN) and that they should have access to prompt effective treatment if sick with malaria. Courtesy call at the office of URR Commissioner Omar Khan. From left: Pa Cheboh Saine, Dr Margaret Pinder, Musa Jawara and Kebba Keita. Bed nets prevent mosquito bites only while one is in bed. However, spraying the inside walls of houses with insecticide (indoor residual spraying, IRS) also reduces mosquito bites before bedtime. In addition, it may have an extra effect at reducing malaria mosquito populations, and Musa Jawara (Unit Entomologist) is looking at this aspect in the study. DDT was used for vector control in the tropics fifty years ago. Why didn’t it succeed then in eradicating malaria – and why is it being resuscitated as a control measure now? Lamin Jarju (standing left) is on secondment to the project (6 months) DTT was very effective at eliminating malaria in from the National Malaria Control Programme. some areas with low levels of infection, and IRS has been effective at maintaining low malaria levels in it combines with our current tools. other countries such as South Africa. But in most cases DDT was stopped before malaria was eliminated, and then Resistance to DDT has been noted in the countries it tends to return rapidly. Eradication means that a disease bordering The Gambia. How does SANTE address this? is no longer present in the world; elimination that it is no We will be monitoring resistance to DDT, pyrethroids longer present in an area, such as a country. We need to (used on bed nets) and other insecticides during the aim for the latter and IRS is becoming popular as it is a study and compare these with measurements made by proven malaria control tool, and countries are adding it to their anti-malaria “arsenal”. Data is needed to see how well the Malaria Programme three years ago. We will test an MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 13 News from Basse alternative insecticide to DDT in a small scale pilot study. Together these results will help advise on the future choice of insecticide. What are the health economics components of the study? The main result from the study will be the number of cases of malaria stopped by IRS with DDT against a background of complete coverage with LLIN. The economic component will collect data on material and labour costs to calculate the cost of malaria cases stopped by the addition of IRS. What capacity building initiatives does the project include? Lamin Jarju, an NMCP Vector Control Officer, has joined the study to oversee the distribution of LLIN and IRS both years and he will gain in-depth training on IRS, the development of vector control management systems and insecticide resistance monitoring strategies, and application of the results. Together with Regional Health Teams, study nurses will provide refresher and on-the-job training for village health workers in the study area. The study also has a limited budget to train a local government employee(s), for example at the University of The Gambia, in Health Promotion Planning. How will the outcome of the study benefit decision makers? The results should influence decisions on malaria control policy by providing accurate measures of the additional benefits of using IRS with DDT together with current best practice, the cost of malaria cases stopped by this added intervention, up-to-date data on insecticide resistance in URR and the comparison of DDT with an alternative insecticide to guide its future use. 14 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 Study Manager Dr Margaret Pinder ‘the results should influence decisions on policy by providing accurate measures of the additional benefits of using IRS with DDT together with current best practice.’ Recent Unit Publications Summary by Dr Margaret Pinder Social perceptions of research: findings from the Larval Control Project This paper describes a malaria research project in The Gambia to provoke thinking on the social value of transnational research. The Larval Control Project (LCP) examined how effective a microbial insecticide was at reducing the density of malaria-transmitting mosquitoes and clinical malaria in Gambian children. To track cases of malaria the study involved the Village Health Workers (VHWs) who were supported by project nurses. In the current article we combine insights from ethnographic fieldwork conducted at the Medical Research Council (MRC) Laboratories in Farafenni from 2005 to 2009, open-ended interviews with project nurses, nurses and eight focus group discussions held with participant mothers in October 2007, to consider the social impact of the LCP's investigative method against the backdrop of several years of research activity. We found that while participants associated the LCP with the clinical care it provided, they also regarded the collaboration between the nurses and VHWs added additional benefits. Organised around the operational functions of the trial, these small-scale collaborations provided the platform from which to build local capacity. While ethical guidelines for medical research emphasise the considerations that must be added to experimental endeavour in southern countries (e.g. elaborating processes of informed consent, developing strategies of community engagement or providing therapeutic access to participants after the trial concludes), these findings suggest that shifting attention from supplementing ethical protocols to the everyday work of research -embedding ethics through scientific activity - may provide a sounder basis to reinforce the relationship between scientific rigour and social value. 'Like sugar and honey': The embedded ethics of a larval control project in The Gambia. Kelly AH, Ameh D, Majambere S, Lindsay S, Pinder M. Soc Sci Med. 2010 Mar 9. Summaries from PubMed Understanding TB in HIV infected people: vaccine development clues Tuberccul Tube u ossiss kills ls 2 m milililliliion p peo e pl eo p e pe p r year ar and infe in fect ctio ionn wi io with thh H HIV IV iiss th the mo m st potten e t kn know ow wn riiskk fac risk facto torr fo forr pr prog ogre ress ssio ionn to aact ctiv ivee TB iv TB. An An understand dingg of tthe he iimm mm mun u e re resp sponse spo onse tto TB Ags in HIV-infeect cted ed p pat atie ient ntss is required to develop optimal TB vaccines and diagnostics. The investigators assessed polyfunctional (IFNgamma(+)IL-2(+)TNF-alpha(+)) T cell responses to TB Ags in three groups of HIV-1-infected patients dependent on their TB status, CD4 counts, and anti-retroviral exposure. They found that although the proportion of IFN-gamma cells in response to TB Ags was higher in patients with low CD4 counts, the responding cells changed from a polyfunctional CD4(+) to a monofunctional CD8(+) response. The overall polyfunctionality of the cells was restored by 12 months of antiretroviral therapy and primarily involved CD4(+) T cells with an effector memory phenotype. These findings have major implications for diagnosis of TB and in vaccine development strategies for TB in HIV-1-infected patients. Polyfunctional CD4+ and CD8+ T Cell Responses to Tuberculosis Antigens in HIV-1Infected Patients before and after Anti-Retroviral Treatment. Sutherland JS, Young JM, Peterson KL, Sanneh B, Whittle HC, Rowland-Jones SL, Adegbola RA, Jaye A, Ota MO. J Immunol. 2010 Apr 30. Studying pneumococcal carriage To prepare for national introduction of a pneumococcal vaccine of restricted valency, the investigators studied the pattern of nasopharyngeal carriage of Streptococcus pneumoniae and its transmission in Gambian villages over time. Nasopharyngeal swab specimens were collected every 2 weeks from 158 villagers in 19 households in 2 villages over one year. The investigators studied the prevalence and duration of S. pneumoniae carriage, the effect of household size and composition on carriage, and sequence typespecific carriage within and between households. It was found that 97% of children and 85% of adults carried S. pneumoniae at some time. Fiftythree serotypes were represented among 1522 isolates. Carriage was more common among children than adults for all serotypes studied except 9V. There was an overall trend toward MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 15 Recent Unit Publications shorter carriage with increa easi assiiing ng age ng ge (P = .0 043 43) an a d significant differences in carrri r agge du durraatition ionn beetttwe ween ween we e serotypes. For most serotype pes, s thhee o odd dds off beeiingg a dd carrier were greater if theree were weeree other therr car th arri rieerrs inn ri rier the household. The prevalence of of car arri riaag ri age va vaari ried ri ied e by serotype. Most notably, serotyp y e 5 caarr rria iaaggee occurred in only 1 village and was transientt. Multilocus sequence typing of serotype 6B isolates from 1 village revealed 8 different sequence types and strong evidence of nonrandom distribution among households (P < .001). Study by sequence type suggested household spread starting most commonly in children, followed by spread to adults. This longitudinal carriage study in Gambian villages provides unique information on the pattern of spread of S. pneumoniae in rural Africa and a baseline for evaluatingg the impact p of the introduction of pneumococcal conjugate vaccine into the region. Transmission of Streptococcus pneumoniae in rural Gambian villages: a longitudinal study. Hill PC, Townend J, Antonio M, Akisanya B, Ebruke C, Lahai G, Greenwood BM, Adegbola RA. Clin Infect Dis. 2010 Jun 1;50(11): 1468-76. Immune system: ‘remembering’ malaria infection Longitudinal cohort studies are important to describe the dynamics of naturally acquired antibody response profiles to defined Plasmodium falciparum malaria antigens relative to clinical malaria episodes. In children under 7 years of age in The Gambia, serum IgG responses were measured to P. falciparum merozoite antigens AMA1, EBA175, MSP1(19), MSP2 and crude schizont extract, over a 10-month period. Persistence of antibody responses was measured in 152 children during the dry season when there was virtually no malaria transmission, and 103 children were monitored for new episodes of clinical malaria during the subsequent wet season when transmission occurred. Children who experienced clinical malaria had lower antibody levels at the start of the study than those who remained free from malaria. Associations between dry season antibody persistence and subsequent wet season antibody levels suggested robust 16 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 immu im muno n lo logi ggiicaal m meemory mo ory ry res espo pons po ons nses es. Me es. Mean an annttibod ib bod dy leevveels elss to al alll an anttiiggeens n wer ere eellev ere e at ated ed by th ed thee end off the o he wett seaason so on in in chiild ldre ren who exxperiennced ced ce clliinnic clin ical al mal alaarriaa; ea each each ch of tthhes e e chhildr illd drren en had a bo b oos ostteed anntit bo body dy res espo ons n e to o at at le leas astt on as one an antittiigen. I alll chi In hildre ld dren, n ant n, ntibod ib bod odyy avid vid dittiees w weere llow o er aga ow gaainnst MSP2 MS P tha hann ot othe her an antitige geenss, a di d ffer errence ence that did no n t change throughout the study period or in relation to clinical malaria episodes Boosting antibody responses to Plasmodium falciparum merozoite antigens in children with highly seasonal exposure to infection. Akpogheneta OJ, Dunyo S, Pinder M, Conway DJ. Parasite Immunol. 2010 Apr;32(4):296-304. Regulation of severe malaria: more genetic signposts With the functional demonstration of a role in erythrocyte invasion by Plasmodium falciparum parasites, implications in the aetiology of common conditions that prevail in individuals of African origin, and a wealth of pharmacological knowledge, the stimulatory G protein (Gs) signal transduction pathway presents an exciting target for anti-malarial drug intervention. Having previously demonstrated a role for the G-alpha-s gene, GNAS, in severe malaria disease, the investigators sought to identify other important components of the Gs pathway. Using metaanalysis across case-control and family trio (affected child and parental controls) studies of severe malaria from The Gambia and Malawi, the investigators sought evidence of association in six Gs pathway candidate genes: adenosine receptor 2A (ADORA2A) and 2B (ADORA2B), beta-adrenergic receptor kinase 1 (ADRBK1), adenylyl cyclase 9 (ADCY9), G protein beta subunit 3 (GNB3), and regulator of G protein signalling 2 (RGS2). The study amassed a total of 2278 cases and 2364 controls. Allele-based models of association were investigated in all genes, and genotype and haplotype-based models were investigated where significant allelic associations were identified. Although no significant associations were observed in the other genes, several were identified in ADORA2A. The most significant association was observed at the rs9624472 locus, where the G allele (approximately 20% frequency) appeared to confer enhanced risk to severe malaria [OR = 1.22 (1.09-1.37); P = 0.001]. Further investigation of Recent Unit Publications t e AD th ADOR ORA A2 2A ge gennee reg egio io on iss rreq equi eq uire reed d to to val alid alid idat atee thee as assso ociiat atiio onnss iide dent de ntifi nt ifified hheere re,, annd to to iide dent ntififyy annd fuunncctition onal a lyy chhaara al ract cter errizze th eriz the re r sp pon onsi sibl b e ca c us u al a vaari ria t(s). Thhe re rian resuults ltts pr prov ovid idee furt furt rthe herr ev he e id iden ence cee suupp p orrttiing n a rol ole of the Gs signnal ttra rans nsdu duct ctio tionn p thhwa pa w y in the regulation of severe malaria, and request further exploration of this pathway in future studies. Further evidence supporting a role for gs signal transduction in severe malaria pathogenesis. Auburn S, Fry AE, Clark TG, Campino S, Diakite M, Green A, Richardson A, Jallow M, Sisay-Joof F, Pinder M, Molyneux ME, Taylor TE, Haldar K, Rockett KA, Kwiatkowski DP. PLoS One. 2010 Apr 1;5(4):e10017. a bir at irth th.. Fl Flan nag agan an KL, Halliday A, Burl S, Landgraf K JJag K, agne ne YJ,J,J Noh oho-Konteh F, Townend J, Miles DJ,, vaan de DJ derr San Sande nd M, Whittle H, Rowland-Jones S Placental malaria: its effects on babies’ health Placental malaria (PM), a frequent infection of pregnancy, provides an ideal opportunity to investigate the impact on immune development of exposure of the foetal immune system to foreign Ag. The investigators looked at the effect of PM on the regulatory phenotype and function of cord blood cells from healthy Gambian newborns and peripheral blood cells from their mothers, and analyzed for effects on the balance between regulatory and effector responses. Using the gold standard for classifying PM, the researchers further distinguished between resolved infection and acute or chronic PM active at the time of delivery. They show that exposure to malarial Ag in utero results in the expansion of malaria-specifi c FOXP3(+) Treg and more generalized FOXP3(+) CD4(+) Treg in chronic and resolved PM, alongside increased Th1 proinflflflfl ammatory responses (IFN-gamma, TNF-alpha,IFN-gamma:IL-10) in resolved PM infection only. These observations demonstrate a clear effect of exposure to malarial Ag in foetal life on the immune environment at birth, with a regulatory response dominating in the newborns with ongoing chronic PM, while those with resolved infection produce both regulatory and infl ammatory responses. The findings might explain some of the adverse effects on the health of babies born to women with PM. The effect of placental malaria infection on cord blood and maternal immunoregulatory responses MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 17 In conversation with Professor Brigid Heywood Brigid Heywood is the Pro-Vice Chancellor (Research) of the Open University, UK. In March she made a site visit to MRC The Gambia. Here Brigid introduces herself and gives her assessment of the unit. My background I am a scientist. I started out in life sciences and medicine; I completed a first degree in chemistry, I then went on to study human biology for my PhD at Liverpool Medical School. I gradually migrated through a career of materials chemistry, but with an interface directly into medicine. My research area is the growth of crystals. I have a lot less time than I would like so research is now something that I probably do in the small bits of spare time I can muster. I used to have a very large group of over thirty people, and I finished my last full time PhD student last year. So for the first time in 25 years I am not surrounded by PhD students associated with my research group, but I remain at heart an academic. My expertise as a senior officer of a university is in the procurement and management of research at large scale. I think it’s important for my connection with my role to retain my research interests. So I keep them as much out of personal interest as I do out of showing that I have professionally relevant skills. 18 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 My university The OU has 4,500 staff and we are located in a seventy two acre campus in Milton Keynes, 50 minutes north of London. The OU is unique in the UK for two things: it’s the largest university by a significant margin; we currently have just under a quarter of a million registered students (the next largest would be Manchester which has about 45,000). Secondly we were the first university to commit to providing higher education to anybody who wished it, regardless of their qualifications. So there are no entry qualifications into the institution and the majority of our teaching – 98% - is provided through a model which is called open supported learning - all educational provision is provided through a distance education model. Each student has an assigned tutor that they can contact on line at any time they want. And for some courses they meet their tutors physically once a month and meet their tutor peer group as well. Visiting The Gambia In my role as Pro-Vice Chancellor, I am responsible for all doctoral training for the OU. We have just over a thousand registered PhD students, 300 of whom belong In conversation with Professor Brigid Heywood to affiliated research centres. MRC The Gambia is one of our connected, affiliated research centres. We have another one in Kenya, some in SE Asia, America and we have a whole series scattered across Europe and the UK. They are mainly elite research centres that focus almost exclusively on conducting research. So they are not typical of academic university based institutions where they have a teaching responsibility. But they have a large commitment to high quality, focused research so most of them are medical research centres, and most of them have a commitment to capacity building and succession planning - succession both in terms of the skills for a particular discipline or technical area and also in terms of capacity building within a country. We support that as part of the mission of the university and my responsibility here is to do reviews, which is the equivalent of a quality assurance audit, to make sure that the approach you take to your doctoral training on site meets with our quality assurance standards. Currently, I am visiting all 30 odd centres round the world. I am trying to make sure we help the sharing of best practices in terms of how you support and develop your doctoral candidates. One of the exciting things has been to put something that I’ve read quite a lot about into a human picture of what the centre looks like and why your model works for you in a particular way. Doing well MRC The Gambia gets a ‘gold star’ for the quality of the doctoral students’ experience. From my perspective the unit’s got excellent completion rates – one of the best of any affiliated research centre we have. I now understand why: MRC The Gambia has an incredibly robust, critical way of selecting suitable candidates. So it’s the sheer effort you put in to make sure those you recruit are fit for purpose in the sense of being candidates who will be suitable for doctoral training and will make it worthwhile that you should invest so much resource – human and financial. Could do better The world of research is very competitive and what it requires is an evidence base. Funders want to see evidence of due diligence on the quality of the research environment. That includes the physical environment: equipment that’s fit for purpose, effective investment of money; a very robust research environment that acknowledges what good quality research is. I suspect MRC The Gambia knows all of this like the oxygen that you breathe, but how do you prove it? You have built up a language, culture where everything is done in a certain way, but you couldn’t evidence that to someone outside the four walls of your compound. So you must be able to narrate and connect with a framework for articulating your research environment – and that includes training. Word of mouth is 20th century. You need a framework that is documented and evidence based. This is not only because the OU will demand it, but also because increasingly, research funders require the different points of evidence to be there. All this will be seen as a criticism but it isn’t quite. It was clear when I met staff that they could articulate what they were doing and why. They’ve got most of that information in some form or another. Unfortunately too much of that is in their heads or transpires as part of ‘water cooler’ conversations. So one of my recommendations is that you need to put a system of guidance documents in place, and the staff community needs to participate in creating these guidance documents, so that everyone will have a sense of ‘ownership’ over them. Final thoughts It’s been a really enjoyable, inspirational experience, but quite humbling to see a little part of my university contributing in a small way to a very successful centre. And underlying that is a training environment of the very highest quality. Many of the technical staff I talked to while walking around the campus were able to explain very clearly what they were doing, why they were doing it and what their role in the process was. So that speaks to anyone who’s spent 30 odd years in education. MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 19 MRC The Gambia: Centre of Excellence for PhD training MRC The Gambia has trained many PhDs over the years from all over the world. Here we feature three recent success stories: from Cameroon, Kenya and the United Kingdom Meet Louis University. Marie Yindom who recently defended his PhD sucessfully at Oxford Mrs. Mireille Kwekam Yindom, Mr. Georges Kenko Yindom, Mr. Nathan Fozeu Yindom, Ms Claire Sussussi Yindom, and Dr. LM Yindom Louis’s journey I came to The Gambia in February 2001 armed with a Fellow of the Institute of Biomedical Sciences of Nigeria after my studies at the University of Jos, Plateau State, Nigeria [I am from Cameroon originally]. I worked with RVTH for six months, and was ready to go to Ireland to do an MSc when I got the job of managing the MRC’s HLA typing laboratory from October 1st 2001. Fortunately Ulster University agreed that I could do my MSc by distance learning instead, which I did and finished successfully in 2003. Introducing new methods at the unit In 2005, I visited Professor Mary Carrington’s lab at the National Cancer Institute, Maryland to learn new techniques for HLA typing by sequencing. We’d been doing HLA typing by PCRSSP (sequence specific priming) for a number of years, which involved the use of huge amounts of synthesised primers to identify the different HLA alleles. And since HLA is one of the most polymorphic regions of the human genome, we were using close to 500 different primers to HLA type each DNA sample, a huge amount of work. When I returned to The Gambia from Prof Carrington’s lab, Professor Sarah Rowland-Jones and I discussed the possibility of introducing this technology (HLA typing by the Sequence-based method) at the unit. Around that same time, EDCTP launched a call for two PhD Fellowships and I was encouraged to apply. I wrote a proposal and submitted in November 2005. In March 2006 I was selected for one of two EDCTP PhD fellowships under the supervision of Professor Rowland-Jones, Professor Carrington and Professor Robert Walton (then head of 20 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 MRC The Gambia: Centre of Excellence for PhD training MRC’s Genetics group). I was then registered with the Open University in the UK for my PhD from October 2006. My proposal focused around sequencing highly polymorphic regions of the human genome and relating them to susceptibility to HIV 2 infection and disease progression. This became one of the main drivers for the acquisition of a sequencing facility which is a state-of-theart technology in this unit. Caio The title of my PhD project was ‘Human Leukocyte Antigens (HLA) and Killer Immunoglobulinlike Receptors (KIR) in HIV-2 infection’. I chose HIV 2 - and Caio as my focal point - because a lot was known already about HLA and KIR in HIV 1 (although most of what we knew came from developed world), but virtually nothing about HIV 2. The Caio HIV cohort is one of the best resources that this Unit has and second to none in the world with regards to HIV 2 research. As there were no ‘high tech’ facilities in Caio, we collected blood samples and shipped them to Fajara for DNA extraction, quantification and storage in the Unit’s Biobank. We subsequently used those DNAs for immunogenetics and other studies looking at variations in the human genome that could influence the way people respond to infection or progression to disease (AIDS) when infection is established. HIV Long term non-progression: looking for clues Genetic typing is used to determine the genetic makeup of individuals with the aim to understand whether certain genotypes predispose people to, or protect them against certain infections, e.g. HIV. It can also provide a clue as to who is likely to progress with the disease faster or slower. Looking specifically at the HLA genes on human chromosome 6, we were interested in variations in that portion of the human DNA in a homogenous population to see whether we could relate specific variations to the outcome of HIV infection or disease progression. Studies from this unit and elsewhere have shown that a significant number of individuals infected with HIV 2 do not progress to full blown AIDS at the same rate as their HIV 1 infected counterparts and they have been called long-term non-progressors (LTNP). We still do not understand fully why this group of people accommodate the HIV 2 virus for a very long time (15-20 years) without coming down with the disease (AIDS). The HIV 2 and 1 viruses are closely related: they share between 30-60% similarities in many of their genes and both target the same cell for destruction, so you’d expect that they’d behave the same way while in their host. But we’ve realised that there are people in Caio that have been infected with HIV 2 for well over two decades and are still going about their businesses comfortably. This scenario is very rare in HIV-1. So we are trying to find out if the genetic makeup of these LTNPs could explain to some extend why their immune system can successfully manage the virus for that long time. We do this by studying the HLA loci in chromosome 6, with particular reference to HLA class I loci (HLA-A, HLA-B, and HLA-C), which have long been associated with how the body functions immunologically to protect itself from infections. This formed the first part of my PhD work. Natural killers The second part of my thesis was the study of Killer Immunoglobulin-like Receptors (KIR) in relation to susceptibility to HIV 2 infection and progression to AIDS. These are specialized receptors that are found on the surfaces of Natural Killer (NK) cells. NK cells are a sub set of white blood cells which are specialised in protecting the body from infection. They are the soldiers of the body and are among the first cells to come in contact with any foreign substance, be it a bacterium, a virus or a parasite, that crosses the skin or mucus membrane and gain access into the body. We now know that these special types of white blood cells have several receptors, which help them distinguish between normal body cells (“self”) and foreign substances (also referred to as “non-self”). NK cells identify anything in our body that wasn’t there originally and try to mop it up and destroy it with the help of other body’s immune machineries. They are also able to distinguish between healthy/normal body cells and those that are aged or dying or becoming cancerous and help the immune system get rid of those aged or cancerous cells. In doing this, MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 21 MRC The Gambia: Centre of Excellence for PhD training they use the receptors on their cell surfaces as sensors to sense other body cells looking for their ligands which happen to be HLA class I molecules. The presence or absence of these ligands (molecules) leads to a cascade of signals in the NK cell which will either hinder that NK cell from killing the target (ie the other cell) or stimulate the NK cell to attack and kill that target. For our study, we were interested in identifying genes that encode (make) KIR receptors. Those genes are located on human chromosome 19, within a highly polymorphic region called the Leukocyte Receptor Complex (LRC). We looked for the presence or absence of 15 KIR genes in infected and uninfected individuals, trying to relate their gene profiles to susceptibility to HIV 2 and/or protection against disease progression. Contributing towards vaccine and drug development We used HIV 2 as a conduit to understanding the main destroyer which is HIV 1. HIV 1 and 2 are essentially very similar although they behave differently before the onset of AIDS. So if we find something informative in our HIV 2 model of LTNPs by identifying what protect them from rapid progression to AIDS, it could be very helpful in curtailing the spread of HIV-1. Such information could also inform vaccine and pharmaceutical companies to develop interventions that will save people from both HIV 1 and HIV 2. Looking forward I’d love to continue HIV research and fortunately I can do my work using archived samples. But essentially my work in immunogenetics is cross cutting and I can apply it in any field irrespective of disease or pathogen. These days I am busy writing grant applications to attract some funds to continue with my line of research. My interest is in host immunogenetics of infectious diseases and not limited to HIV alone. My future direction will depend upon what’s good for my family and not just me. My wife and kids have been very supportive for the past three and half years of my PhD work, travelling from one place to another and I think their welfare is now a priority to me, particularly with regards to the line of studies they will like to follow. I’d like to thank the MRC, without whom I wouldn’t have had this opportunity to do my PhD. I’d also like to thank the EDCTP for sponsoring my research; they’ve been very supportive – I can’t recall anything request from me that they’ve turned down. And of course the study participants: without them this work would not have been possible. Currently, I am writing papers for publication and I do get back to Caio from time to time to give feedback to the community through the Caio field staff. So many people at the unit have been supportive with ideas and prayers and I remain grateful to them. So I definitely will never regret coming to the MRC. Sarah Burl was awarded her PhD in mid 2009. After seven years in The Gambia she is leaving in June to pursue postdoc opportunities in the UK. About Sarah My background is both academic and professional - both in the UK and Canada. I came out of science and worked in the biotechnology industry as a consultant for three years in London working with start up companies. During that time I met my partner Martin Holland who then came out to The Gambia. At that time the company I was working in was being disbanded, so I came to The Gambia intending to stay for just a few months, and ended up staying seven years. In fact, I got a job with the TB group a week after my arrival. 22 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 MRC The Gambia: Centre of Excellence for PhD training Finding a research passion in the Gambia [Once I’d started working with the TB group], I realised that this area of research was incredibly interesting, so I ended up doing a PhD. I had considered doing a PhD before but I’d never felt like I was working on something I was so interested in I’d want to spend the rest of my life studying it. Vaccination and the environment My PhD was based on BCG vaccination in early life, looking at the immunogenicity of the vaccine. We wanted to know why the vaccine is not very effective in this environment. One of the theories is that the BCG vaccine is masked by your immune Dr Sarah Burl taking time out from a conference in Turkey responses to other things, particularly the environment. Environmental mycobacteria induce an immune response and the mycobacteria have very similar profiles to the BCG vaccine itself, so if you are exposed to these first before receiving BCG, the response to the vaccine may be reduced. We vaccinated a group of children at birth and delayed the vaccine in the other group to four and a half months. I’d like to reiterate that the vaccine is recommended to be taken within the first year of life, so it was within the recommended time frame. Children vaccinated at 4 and a half months would have been exposed to environmental mycobacteria, which we found by looking at their in vitro responses to mycobacteria at that age. Their responses were different from those vaccinated with BCG at birth. When we compared the two groups at the same time point post vaccination (i.e. 4½ months), we found reduced interferon gamma, IL17 and IL6 responses in the group vaccinated at 4 and a half months. We can’t say that protection is reduced, but the lack of IFNg and its receptor has been associated with reduced protection in humans. However when we compared the groups at 9 months of age the responses were similar. This may also be due to a waning of the response 9 months post vaccination in those vaccinated at birth. Also, responses to mycobacteria prior to vaccination were observed, so it would suggest that there could be some interaction, explaining why the responses in the delayed group were reduced. A PhD at MRC The Gambia: pros and cons You have the expertise and the interest of people here in the same subject area you wish to work on. You also have all the material you need to work on here – the samples and technology. You can do everything in one spot and that’s been the major advantage for a subject area of this type. However, it can feel a bit isolated here which makes going to conferences essential to discuss your work with others around the world in your own field of interest. In a big university in a large city you would have the opportunity to mix with more people and attend many more seminars from internal and external scientists although the interest of those around you may be much broader. Looking forward I am planning to move to London, UK in June. There may be future opportunities to continue collaborating with MRC The Gambia which I would really like to do. I’ve been doing work on tolllike receptors and I’d like to continue doing that. I’ve just completed a pilot study since my PhD MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 23 MRC The Gambia: Centre of Excellence for PhD training so I’d quite like to continue with a larger study and maybe write a fellowship for my own funding to do that here but based in London, although nothing is final for me at the moment. London is probably not somewhere I’d end up long term but I think it will be a good opportunity for work at this stage of my career. I am not looking forward to the long commute (at least 3 h daily); that’s an advantage of being here – a five minute cycle to work and fewer distractions so you can work very hard more easily here and still have a nice lifestyle. And I am not looking forward to having to wear socks every day… I’ll miss… The light and the weather. And the interactions with people working in similar fields. I’ve had quite a lot of independence here. I’ve been able to be involved in different areas such as managing the labs and training including tutoring some of the BSc and Foundation degree students. Here there are a lot of other aspects of the academic world than just sitting in the lab doing bench work. It’s a lot more applicable to real life. It’s been great having the opportunity to be in an academic area and utilise other skills as well. I will miss many people who I have met and/ or worked with over the years in The Gambia but hope to stay in touch and continue with possible collaborations in the future. Clayton Onyango defended his PhD in early May. He joined MRC The Gambia in 2005 as a scientific officer and went on to win an MRC doctoral fellowship in 2006. Clayton left the MRC on 30th March with his family to take up a new appointment back home with the Wellcome Trust at Kilifi, Kenya, but before he left he told us his story. Clayton’s background I have a Masters degree in biotechnology from Kenyatta University, where I did my thesis on the molecular virology of yellow fever. I was working as a research assistant on viral hemorrhagic fevers, when I got the job with Dr Abraham Alabi at MRC The Gambia. He’d won an EDCTP senior career fellowship award to develop an HIV viral load assay. After a year, Abraham and I were successful in getting the viral load assay up and running; initially we thought it would take us two years but we were able to work much faster. Along the way came Dr. Matthew Cotten with whom we wrote a proposal and secured my MRC PhD studentship. So in 2006, I registered with the OU and I’ve just finished; I am doing my viva on 10th May in The Gambia. HIV 2 The topic of my PhD is the characterisation of variations in TRIM5alpha HIV-2 pathway that associate with disease progression. In simple terms, we were interested in any changes in the HIV-2 capsid (p26) protein that would account of the varied disease outcome observed in HIV-2. The study identified a variety of p26 that associate with viral load. And because we know viral load plays an important role in HIV disease we were able to pinpoint this to changes to p26 that actually attributed to either increased or low viraemia in infected persons. Answers from a ‘weaker’ infection For a long time, HIV researchers have been trying to understand exactly how HIV can be contained by the body and how research can lead to vaccines that will help contain the virus. 24 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 MRC The Gambia: Centre of Excellence for PhD training pandemic. We think the lessons we’ve learnt from studying HIV-2 (that seems to be a weaker infection than HIV1) can be used to help design better studies on HIV 1. Moving on I’ve got a three year appointment with the Wellcome Trust in Kilifi. I am moving away from HIV research for the meantime and I’ll be working on respiratory viruses especially those infecting children. KEMRI-Kilifi has a large cohort of children and mothers. Well established studies in the Kilifi cohorts include epidemiology of different diseases, but we seek to boost the virology arm over the period of my stay in Kilifi. Dr Clayton Onyango: From time to time we’d like to come back and show Mercy The Gambia: a peaceful home where she was born We’ll miss The Gambia. It’s been a hospitable place for my family and we are going back to Kenya where life is fast paced. You have to behave like a Kenyan to survive in Kenya. Gambians really love people – they love each other and they love foreigners. In fact, my last daughter Mercy was born in The Gambia; she has a Gambian birth certificate and a Kenyan passport, so from time to time we’d like to come back and show her where she was born and how life is here. Farewell and final thoughts Recently, there have been many structural challenges that have affected us all at MRC The Gambia. Currently we don’t have a clear picture of the future of HIV research at the unit and this has been a particular issue for me and my lab team. However, I hope that in spite of all the changes, the good things and the warmth will continue. I am proud to say that I am a product of MRC The Gambia; undoubtedly, MRC has contributed a lot towards my career. I want to thank Prof Corrah for offering the enabling environment for me to do my PhD, because it was quite a challenge being a member of staff and taking up a studentship. And I’d like to thank Drs Assan Jaye and Matthew Cotten, Professors Sarah Rowland Jones and Hilton Whittle. They encouraged and supported me through tough times; I will never forget them and I thank them very much -I hope in future we can still work together. I must thank my wife Consolata who has been there for me throughout…And my children for putting up with my late homecoming and travelling while I was studying. Jerre Jeff to you all. MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 25 HR NEWS Kalilu Dibba & Kathy Hill Appraisals The appraisal documents have been sent out to Appraisers and Senior Reviewers. The performance review period is from March 2009 to February 2010. The exercise will be in two phases: A2 – C3 staff – 08/04/2010 to 10/05/2010 D1 – E2 staff – 11/05/2010 to 10/06/2010 HR is appealing to all Appraisers and Senior Reviewers to adhere to the above schedule. If this is not possible due to staff being absent from the Unit could you please inform Kalilu Dibba, Assistant HR Manager so he note this in our records. GEM and Team Awards The deadline for submission of nominations has been extended to 31st May 2010. All nominations must reach the HR office on or before this date. Restructuring The restructuring exercise has now been completed and all staff have been notified of their status. HR would like to thank staff for their patience and understanding during this difficult period. Following the restructuring exercise organograms are now being developed for each department/section to reflect the new structure. New Staff Isatou Ndow Data Entry Clerk Level 1 Maudo Samba Jallow Data Entry Clerk Level 1 Anta Gibba Data Entry Clerk Level 1 Mansour H.B Njie Data Entry Clerk Level 1 Bintou Jobe Data Entry Clerk Level 1 Deyda Njie Data Entry Clerk Level 1 Ismaila Kanteh Data Entry Clerk Level 1 Abdoulie Gibba Data Entry Clerk Level 1 Ousman Ceesay Data Entry Clerk Level 1 Sariba Jammeh Data Entry Clerk Level 1 Safiatou Bah Data Entry Clerk Level 1 Lawrence Gibba Data Entry Clerk Level 1 Abdul Khalie Muhammad Trainee Data Manager/Statistician 26 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 HR News Shola Able-Thomas Laboratory Technician Grade 1 Sainey Senghore Laboratory Technician Grade 1 Haddy Faal Laboratory Technician Grade 1 Gilleh Thomas Data Manager Abdoulie Jatta Assistant Data Manager Ramatoulie Jobe State Enrolled Nurse Modou O Cham Data Entry Clerk Level 1 Abdoulie Bandeh Field Assistant Leavers Ebou Manneh Driver Ebou Senghore Yard Attendant Bedy Baldeh Yard Attendant Anna Colley Cleaner Saikou Dumbuya Field Supervisor Ousman Ceesay Data Entry Clerk Level 1 Biram Saidybah Field Assistant Kebba Dibba Field Station Projects Officer Mohammed Bandeh Senior Field Assistant Bunja Kebbeh Nurse Field Work Coordinator Zainab Kalokoh Laboratory Technician Grade 1 Sanie Sesay Research Clinician The following long serving staff members officially retired on 31st March 2010 after many years distinguished service at the Unit; Lamin Fatty Electrician Adama Sidebeh Auxiliary Nurse Abdou Colley Auxiliary Nurse Sally Ann Clements Cook Emelia Gomez Housekeeper We wish them a happy and restful retirement. MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 27 HR News Clinical Services staff say farewell On 31st March, four long-standing members of staff of the Clinical Services Department retired – Ms Sally Ann Clements (Cook), Mrs Emilia Gomez (Housekeeper), Mr Abdou Colley and Ms Adama Sidebeh (Auxiliary Nurses). Here are some images from their tearful send-off party. Ms Sally Ann Clements receiving her parting gift from Sister Isatou Marenah Adama with Mamina Bojang (SRN nurse) Deputy Matron Ilene Carayol drying the tears of Mrs Emelia Gomez Professor Hilton Whittle and Ms Adama Sidibeh Mrs Gomez and Musa Sawaneh (Acting Transport Manager) Sally Ann with colleagues Mr Abdou Colley 28 MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 HR News Meet Abdoulie Jadama, who joined the MRC in March 2010 as a Project Manager (External Grants). ‘I am a Certified Project Management Professional (PMP) born in Gimansari Bah, Upper Badibou District, North Bank Region, The Gambia. I started my early academic and professional career in Agriculture and Rural Development. I did my Higher Diploma in Agriculture and Rural Sociology at the Gambia College. Upon completion in 1997, I joined the Department of Agricultural Services (DAS) as Senior Agricultural Officer. Later that year I was seconded to support the Decentralised Rural Development Programme funded by the European Union at Kerewan Area Council as Project Support Officer-Agriculture and Natural Resources Management. Prior to leaving (SRDR), in 2003 I joined the Management Development Institute to pursue my Diploma in Management Studies. In 2004 I returned to (DAS) under the Soil Management Unit attached to the Lowland Agricultural Development Programme (LADEP) as Programme Specialist Conservation. In September 2007 I went to the University of Bedfordshire (UK) to do my MBA. I later worked with Action for Employment in the UK as a Programme Support Officer/ Coordinator. From January 2009 to September 2009 I registered with the Project Management Institute in United States of America for my Certified Project Management Professional (PMP) qualification.’ Welcome, Abdoulie. We wish you a productive and successful time in a department that is scheduled to become much busier over the coming years. Obituary Mr Silaba Drammeh passed away on 5th April 2010 at the MRC ward at Fajara after a long illness. He was laid to rest on 6th April 2010 at Wellingara. A large number of MRC staff led by the Matron of Clinical Services turned out to pay their last respects to Mr Drammeh. Silaba Drammeh joined the Unit on 25th July 1978 and worked continuously until his death. Several speakers at the funeral described his admirable personality and piety. Colleagues at MRC will remember his gentility and diligence. May his soul rest in perfect peace. MRC TAMA - VOL: 09 ISSUE: 02 / Mar - Apr 2010 29 Your Feedback Please! Tama – the Newsletter of MRC (UK) The Gambia – is for everyone who is interested in our work and our community. We are keen to receive feedback and suggestions for new features from our readers. So if you have any comments, please let us know. Email: tama@mrc.gm TAMA EDITORIAL BOARD Alison Offong Maimuna Mendy Bouke de Jong Kathy Hill Pa Tamba Ngom Fanding P Njie TAMANEWSLETTER VOL: 09 ISSUE: 02 / Mar - Apr 2010 Medical Research Council (UK) The Gambia Atlantic Road, Fajara P. O. Box 273 Banjul The Gambia Communications Tel. 4495 442 Ext. 2306 Email: communications@mrc.gm Web: www.mrc.gm © Medical Research Council 2010