Discrete Wavelet Transform-Based Method for Automatic

2014 Fifth International Conference on Intelligent Systems, Modelling and Simulation
Discrete Wavelet Transform-Based Method for Automatic Evaluation of
Sleep-Disordered Breathing Using Photoplethysmography
Hyo-Ki Lee, Ilgang Heo, Seongsoo Yang, Kyoung-Joung Lee
Department of Biomedical Engineering
Yonsei University
Wonju, Republic of Korea ilovehyoki@yonsei.ac.kr, ilgangheo88@yonsei.ac.kr, seongsooyang@gmail.com, lkj5809@yonsei.ac.kr
Abstract —This study proposed the discrete wavelet transform
(DWT)-based method for automatic evaluation of sleepdisordered breathing (SDB) in patients with sleep apneahypopnea syndrome using photoplethysmography (PPG). The method is based on the fact that the amplitude and pulse rate waveform of PPG reflect vasodilation and vasoconstriction generated by autonomic nervous system (ANS). Thus the amplitude and pulse rate waveform were induced from PPG and they were applied to DWT based on the Coiflet 3 wavelet with order 7. The apnea-hypopnea index (AHI) induced by the proposed method was compared with that measured by a sleep technician. Fifteen patients were participated in this study and correlation statistics revealed significantly high correlation coefficient, indicating good to excellent validity ( r = 0.97, p <<
0.001). This study indicated that the proposed simple method would be useful in sleep monitoring system and may provide clinical insights when the designing a portable and inexpensive sleep monitoring system.
nervous system [7]. This phenomenon is generated when apnea and hypopnea occurs and it reflects in PPG data as a change of the signal amplitude fluctuation and pulse rates [8].
The aim of this study is to propose an automatic method for evaluating SDB using amplitude and pulse rate extracted from the PPG data. The method is based on the fact that PPG data reflects vasodilation and vasoconstriction generated by the automatic nervous system (ANS) as well as the combined effects of the parasympathetic and sympathetic nervous systems. A basic premise is that the performance of the PPG data would be comparable to the results manually labeled by sleep technician. If this premise is accepted, the method would be applicable to the low-cost portable PSG or continuous positive airway pressure (CPAP) system to be used easily at home.
II.
M ETHODS
Keyword—sleep apnea; discrete wavelet transform (DWT); photoplethysmography (PPG)
I.
I NTRODUCTION
Sleep-disordered breathing (SDB) is characterized by an abnormal alterations of breathing pattern. SDB regards as recurrent episodes of reduced (hypopnea) or absents (apnea) respiratory airflow caused by collapse or obstruction of the upper airway [1]. It becomes progressively more prevalent with increasing age and is recognized as a cause of a higher morbidity and mortality task [2, 3].
For evaluating SDB, polysomnography (PSG), which contains simultaneous monitoring of multiple physiologic recordings such as electroencephalogram, electrocardiogram
(ECG), electrooculogram, electromyogram, respiratory airflow signals and photoplethysmogram (PPG), is internationally considered as the gold standard [4]. However, it is labor-intensive, time-consuming, very expensive and technically complex, and it also includes specialized equipment for acquisition of various physiologic recordings
[5].
A few researches for evaluating SDB employed PPG data obtained by measuring the optical components from a pulse oximeter since the PPG data is simple and useful to analyze cardiovascular activity and to evaluate peripheral circulation
[6]. The PPG data provides the information related to arterial vasoconstriction or vasodilation caused by the autonomic
A.
Populations and data acquisition
Totally 50 patients with sleep apnea-hypopnea syndrome
(SAHS) underwent a full-night PSG study at the sleep center of the Samsung Medical Center (Seoul, Republic of Korea)
All patients provided written consent to participate (Table I).
PPG data acquired at a sampling rate of 100 Hz with 16bit resolution during full-night PSG recordings performed using a commercial recording system (N7000, Embla System
Inc., USA) and sleep diagnostic software (RemLogic 2.0,
Embla System Inc., USA). The PPG data were preprocessed with 10-point moving average filtering to decrease unwanted background noise. All sleep-related events were manually labeled by an experienced clinical technician and then a physician reviewed and confirmed the labeled events.
B.
Automatic SDB detection
Amplitude and pulse rate waveform of PPG were employed as features to detect apneas and hypopneas. The amplitude was computed as a magnitude of the difference between peak point and trough point of each period of PPG
TABLE I. D ETAILED I NFORMATION OF P ATIENTS
Data set (AHI)
Mild-to-moderate (5~30)
Severe (30~)
Patients [F/M] Age (years) BMI (kg/m
2
) AHI (/hr)
25 [5/20]
25 [2/23]
58.7±10.8
54.8±10.1
25.7±3.7
26.9±3.3
21.6±5.6
50.8±14.0
BMI: body mass index, AHI: apnea-hypopnea index;
The range for age, BMI and AHI were presented as mean ± standard deviation.
2166-0662/14 $31.00 © 2014 IEEE
DOI 10.1109/ISMS.2014.41
206
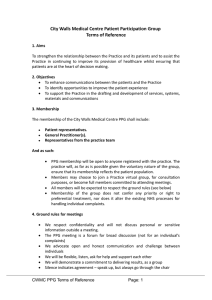
Figure 1. Representation of four-level wavelet decomposition and reconstruction tree data. The pulse rate was calculated as the time difference between two consecutive peak points of PPG data. Although the original sampling frequency of the PPG data was 100 Hz, extracted amplitude and PR waveform are unevenly sampled discrete data. Thus, analysis of amplitude and pulse rate data is in need of some signal processing for conversion to evenly sampled discrete time.
To obtain evenly sampled discrete data, we employed a linear interpolation method with a resampling frequency of 1
Hz. The resampling frequency was decided in order to extract respiratory-related signal from the amplitude and pulse rate data.
Discrete wavelets transform (DWT) based on the Coiflet
3 wavelet with order 7 used as the mother wavelet was employed in order to decompose the discrete data into a set of approximate and detailed coefficient of level up to 7 [9].
The reconstruction of detailed coefficients was computed up to level 7 and the reconstructed decomposition at level 3 (0 to 0.125 Hz) was selected as the wavelet feature for amplitude waveform and that at level 4 (0 to 0.0625 Hz) was selected for pulse rate waveform. Figure 1 illustrates the wavelet decomposition and reconstruction tree.
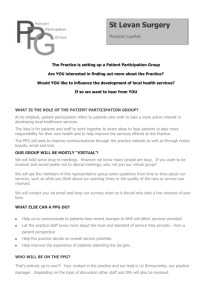
Figure 2 shows the amplitude and pulse rate waveform and their wavelet-filtered data when the apneas and hypopneas occur, and also presents the nasal pressure data and oxygen saturation for annotation of apneas and hypopneas. Since the apnea is related to peripheral vasoconstriction due to increasing sympathetic activity in
PPG data, the amplitude reduction occurs after the apnea and hypopnea take place for a certain period of time and the pulse rate during apnea and hypopnea is relatively lower than that during normal respiration as the wavelet-filtered data.
Detection of apneas and hypopneas was performed based on DWT-filtered both amplitude and pulse rate waveform as following steps:
Step 1: detect trough points of amplitude waveform
Step 2: detect trough points of pulse rate waveform
Step 3: expect that apnea or hypopnea is within two consecutive trough points of amplitude waveform if one trough point of pulse rate waveform is existed between two consecutive trough points of amplitude waveform
Step 4: recognize as apnea or hypopnea if time interval of two consecutive trough points of amplitude waveform where the apnea or hypopnea is expected to exist is within 30 to 120 seconds
III.
R ESULTS AND D ISCUSSION
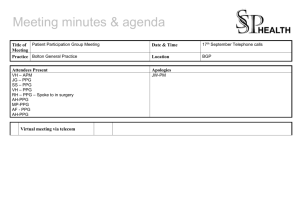
Correlation statistics using Pearson’s correlation coefficient were employed to determine validity of the PPGbased measurement by comparing the apnea-hypopnea index
(AHI: the number of apnea and hypopnea per hour of sleep) obtained from a manually annotation and a proposed automatic method. Statistical significance was considered at p < 0.05. Figure 3 depicts the relationship between the AHI compared by annotation and that estimated by the proposed
PPG-based method. The mean values of annotated AHI and estimated AHI were 36.2±18.1 events/hour and 32.6±13.1 events/hour, respectively. Correlation analysis revealed significantly high correlation coefficient, indicating good to
Hypopnea Apnea Wavelet-filtered data
Nasal pressure data
Amplitude of PPG
104
100
Pulse rate of PPG
(bpm)
96
92
95
85
SpO2 (%)
196.5
197 197.5
198 198.5
199
Time (minites)
199.5
200 200.5
201 201.5
Figure 2. Nasal pressure data, amplitude of PPG and its wavelet-filtered waveform, pulse rate of PPG and its wavelet-filtered waveform, and oxygen saturation (SpO2) waveform during apnea, hypopnea and normal breathing. Manually labeled apnea and hypopnea highlighted as shaded area.
207
Figure 2. Scatter plot of correlation of AHI between annotated by a technician and estimated by the DWT-based method using PPG
excellent validity ( r = 0.97, p << 0.001). The method provided acceptable results for automatic evaluation of SDB in comparison to the manually annotated apneas and hypopneas events.
Previous studies presented various portable monitoring applications for evaluating SDB using PPG. Some of them employed PPG data in conjunction with other sensor data.
Pulse transition time variability (PTTV) was utilized to discriminate SAHS [9]. Both heart rate variability and amplitude of PPG were applied for SAHS screening [10].
However, these methods require absolutely ECG recording that can be uncomfortable during full-night sleep owing to a need of attaching additional sensors.
The proposed method would be useful to the low-cost and portable SDB monitoring system during overnight sleep at home, since PPG data may acquire easily, simply and cheaply and its processing could be realized in real-time with a low computation cost. Moreover, the method would be helpful for more accurate evaluation of SDB in CPAP system.
This study should take into account some limitations to realize results. Since the wake stage was depended upon the manually labeled annotation of sleep stages when the statistical analysis in wake stage was excluded, this study proposes another method for the classification between sleep and wake stages. Moreover, this study invites further research with more databases to generalize the method and additional annotation of another sleep technician to avoid subjective judgment of sleep-related events.
This study may provide clinical insights when the designing a portable and inexpensive real-time SDB monitoring system for patients with SAHS since the PPG data is a simple and useful for monitoring cardiovascular activity as well as respiratory activity.
A
CKNOWLEDGMENT
This work was supported by the Technology Innovation
Program (10040408, Development of CPAP for sleep apnea) funded by the Ministry of Trade, Industry and Energy
(MOTIE, Korea).
R EFERENCES
[1] C. Ventaka, S. B. Venkateshiah, “Sleep-disordered breathing during pregnancy,” J. Am. Board. Fam. Med., vol. 22, Mar.-Apr. 2009, pp.
158-168, doi:10.3122/jabfm.2009.02.080057.
[2] P. V. Tishler, E. K. Larkin, M. D. Schluchter, S. Redline, “Incidence of sleep-disordered breathing in an urban adult population: the relative importance of risk factors in the development of sleepdisordered breathing,” JAMA, vol. 289, May. 2003, pp. 2230-2237, doi: 10.1001/jama.289.17.2230.
[3] N. M. Punjabi, B. S. Caffo, J. L. Goodwin, D. J. Gottlieb, A. B.
Newman, G. T. O'Connor, D. M. Rapoport, S. Redline, H. E. Resnick,
J. A. Robbins, E. Shahar, M. L. Unruh, J. M. Samet, “Sleepdisordered breathing and mortality: a prospective cohort study,” PLoS
Med., vol. 6, Aug. 2009, e1000132, doi:10.1371/journal.pmed.
1000132
[4] B. V. Vaughn, P. Giallanza, “Technical review of polysomnography,”
Chest, vol. 134, Dec. 2008, pp. 1310-1319, doi:10.1378/chest.08-
0812.
[5] B. Xie, H. Minn, “Real-time sleep apnea detection by classifier combination,” IEEE Trans. Inf. Technol. Biomed., vol. 16, May. 2012, pp. 469-477, doi:10.1109/TITB.2012.2188299.
[6] J. Allen, “Photoplethysmography and its application in clinical physiological measurement,” Physiol. Meas., vol. 28, Mar. 2007, pp.
R1-39, doi:10.1088/0967-3334/28/3/R01.
[7] R. P. Schnall, A. Shlitner, J. Sheffy, R. Kedar, P. Lavie, “Periodic, profound peripheral vasoconstriction—a new marker of obstructive sleep apnea,” Sleep, vol. 22, Nov. 1999, pp. 939-946.
[8] A. Graps, “An introduction to wavelets,” IEEE Comput. Sci. Eng., vol. 2, Jun. 1995, pp. 50-61, doi: 10.1109/99.388960.
[9] E. Gil, R. Bailón, J. M. Vergara, P. Laguna, “PTT variability for discrimination of sleep apnea related decreases in the amplitude fluctuations of PPG signal in children,” IEEE Trans. Biomed. Eng., vol. 57, May. 2010, pp. 1079-1088, doi: 10.1109/TBME.2009.
2037734.
[10] E. Gil, M. Mendez, J. M. Vergara, S. Cerutti, A. M. Bianchi, P.
Laguna, “Discrimination of sleep-apnea-related decreases in the amplitude fluctuations of PPG signal in children by HRV analysis,”
IEEE Trans. Biomed. Eng., vol. 56, Apr. 2009, pp. 1005-1014, doi:
10.1109/TBME.2008.2009340.
208