Effect of Macrophage-Derived Apolipoprotein E on
Established Atherosclerosis in
Apolipoprotein E–Deficient Mice
Weibin Shi, Xuping Wang, Nicholas J. Wang, William H. McBride, Aldons J. Lusis
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Abstract—Apolipoprotein E– deficient (apoE⫺/⫺) mice have hyperlipidemia and develop spontaneous atherosclerosis in a
time-dependent manner. Although macrophage-derived apoE has been shown to prevent the development of
atherosclerosis in apoE⫺/⫺ mice, whether it would induce regression of established atherosclerosis is unknown. To
determine this, 8-week-old apoE⫺/⫺ mice were transplanted with apoE⫹/⫹ bone marrow. Four weeks after transplantation, when plasma cholesterol levels had reached normal levels, a group of mice (n⫽12) were killed and their aortic
lesions were measured and used as a baseline to judge regression. Twelve and 20 weeks after transplantation, aortic
lesion areas of the mice were 9340⫾2184 m2 (mean⫾SEM, n⫽8) and 12 211⫾1433 m2 (n⫽9), respectively, values
not significantly different from the lesion areas of the baseline mice (12 347⫾2487 m2; n⫽12, P⬎0.05). In contrast,
apoE⫺/⫺ mice reconstituted with apoE⫺/⫺ bone marrow developed severe atherosclerotic lesions (453 036⫾29 767 m2,
n⫽7) 20 weeks after transplantation. These data suggest that macrophage-derived apoE was insufficient to induce
significant regression of established atherosclerotic lesions in apoE⫺/⫺ mice, although it was sufficient to eliminate
hypercholesterolemia and prevent progression of aortic lesions. (Arterioscler Thromb Vasc Biol. 2000;20:2261-2266.)
Key Words: atherosclerosis 䡲 macrophages 䡲 apolipoprotein E 䡲 regression 䡲 bone marrow transplantation
P
revious studies have provided evidence that atherosclerosis can undergo regression in both humans and animal
models,1– 4 but results have varied greatly, depending on the
animal models used or the population investigated.5–7 Mice
are increasingly used in the study of atherosclerosis, and
certain mice such as apoE-deficient (apoE⫺/⫺) mice develop
all phases of lesions found in humans.8,9 Recently, several
studies have reported that atherosclerotic lesions of mice can
undergo considerable regression.10 –16
ApoE is a 34-kD glycoprotein that plays an important role
in lipoprotein metabolism.17 It mediates uptake and degradation of chylomicron and VLDL remnants by acting as a
ligand for the LDL receptor and the LDL receptor–related
protein.17,18 Although the vast majority of plasma apoE is
derived from the liver,19 –22 apoE is also synthesized by
macrophages in various organs.23,24 ApoE deficiency results
in severe hypercholesterolemia and diffuse atherosclerotic
disease in humans25 and in gene-targeted mice.8,9 Targeted
mice develop foam cell–rich fatty streaks in the aortic sinus
and proximal aorta by the age of 3 months, and after 5
months, fibrous lesions are present.26,27 Because apoE is
synthesized by monocytes/macrophages23,24 but not by granulocytes and lymphocytes,28 bone marrow transplantation
(BMT) has been used to examine the role of macrophage-derived apoE in atherosclerosis in vivo. Recent BMT studies
have shown that macrophage-derived apoE results in the
normalization of serum cholesterol levels and prevents the
development of atherosclerosis in apoE⫺/⫺ mice.29 –31 However, it is unknown whether macrophage-derived apoE can
induce regression of established atherosclerotic lesions. The
purpose of the present study was to determine the effect of
macrophage-derived apoE on established atherosclerosis in
apoE⫺/⫺ mice by BMT.
Methods
Mice
ApoE⫺/⫺ C57BL/6J mice and wild-type C57BL/6J mice were purchased from the Jackson Laboratory, Bar Harbor, Me. Mice were fed
with a regular chow diet and maintained in a temperature-controlled
room with a 12-hour light/dark cycle. All procedures were in
accordance with current National Institutes of Health guidelines and
were approved by the UCLA Animal Research Committee.
Bone Marrow Transplantation
Female recipient apoE⫺/⫺ mice were lethally irradiated with a dose of
1000 rads from a cobalt source. Bone marrow cells were harvested
by flushing the femurs and tibias of male donor mice with Dulbecco’s modified Eagle’s medium containing 10% fetal bovine serum
and 5 U/mL heparin. Red blood cells were lysed with ACK buffer
(150 mmol/L NH4Cl, 61 mmol/L KHCO3, and 1 mmol/L Na2EDTA,
pH 7.3). The remaining cells were washed and suspended in
Dulbecco’s modified Eagle’s medium with 1% bovine albumin.
Received June 8, 2000; revision accepted July 17, 2000.
From the Department of Medicine (W.S., X.W., N.J.W., A.J.L.), Department of Microbiology and Molecular Genetics, and the Department of Radiation
Oncology (W.H.M.), School of Medicine, University of California, Los Angeles.
Correspondence to Aldons J. Lusis, Department of Medicine, UCLA School of Medicine, 47-123 CHS, Los Angeles, CA 90095-1679. E-mail
jlusis@medicine.medsch.ucla.edu
© 2000 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org
2261
2262
Arterioscler Thromb Vasc Biol.
October 2000
Each recipient mouse was injected with 107 bone marrow cells in 0.3
mL through the tail vein.
Experimental Protocols
At 8 weeks of age, female apoE⫺/⫺ mice (n⫽29) were reconstituted
with bone marrow cells from wild-type male C57BL/6J mice
(apoE⫹/⫹3apoE⫺/⫺) and maintained on a chow diet. Four weeks after
transplantation, a group of mice (n⫽12) were killed and served as the
baseline group by which to judge regression of atherosclerotic
lesions. The remaining mice were killed at 12 (n⫽8) or 20 (n⫽9)
weeks after transplantation for lesion analyses. In addition, a group
of age-matched, female apoE⫺/⫺ mice were transplanted with bone
marrow from male apoE⫺/⫺ mice (apoE⫺/⫺3apoE⫺/⫺) and maintained on a chow diet for 20 weeks (n⫽7).
Western Blot Analysis for ApoE
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
The presence of apoE in plasma was determined by Western blot
analysis. In brief, 1 L of plasma was separated by electrophoresis
on 12% SDS polyacrylamide gels and electrophoretically transferred
to nitrocellulose membranes. The membranes were incubated with a
polyclonal rabbit anti-mouse apoE antibody (BioDesign International) for 1 hour and then incubated for 0.5 hour with a horseradish
peroxidase– conjugated anti-rabbit secondary antibody. The signals
were detected by the enhanced chemiluminescent detection method
according to the manufacturer’s instructions (ECL Western blotting,
Amersham).
DNA Preparation and PCR of
Male-Specific Sequences
Overnight-fasted mice were bled from the retro-orbital vein under
isoflurane anesthesia. After centrifugation, the plasma was collected
and used for lipid analyses as indicated below. The blood cell pellet
was lysed in ACK buffer to remove red blood cells. DNA was
prepared by adding polymerase chain reaction (PCR) solution
(10 mmol/L Tris, pH 8.0; 2.5 mmol/L MgCl2; 1% Tween-20; and 0.4
mg/mL proteinase K) to each leukocyte pellet and incubating the
resulting mixture at 60°C for 2 hours followed by a 95°C incubation
for 20 minutes. PCR was performed to amplify a 250-bp sequence of
the Y chromosome.32 The upstream primer was 5⬘-GAG GGC CAT
GTC AAG CGC CCC ATG AATG-3⬘ and the downstream primer
was 5⬘-AGA CAC TGT GAA ATC GGG AGG CT-3⬘. The cycling
conditions were denaturing for 1 minute at 94°C, annealing for 1
minute at 62°C, and extension for 1 minute at 72°C.
Aortic Lesion Analysis
Methods for the quantification of atherosclerotic lesions in the aorta
were done as previously reported.33 In brief, the heart and proximal
aorta were excised and embedded in OCT compound. Serial 10-mthick cryosections from the middle portion of the ventricle to the
aortic arch were collected and mounted on poly-D-lysine– coated
slides. In the region from the appearance to the disappearance of the
aortic valves, every other section was collected. In all other regions,
every fifth section was collected. Sections were stained with oil red
O and hematoxylin, counterstained with fast green, and examined by
light microscopy.
Immunohistochemical Analyses of
Atherosclerotic Lesions
Immunohistochemical analyses of atherosclerotic lesions in the
aortic root were performed as previously described.33 In brief,
10-m-thick cryosections were fixed in acetone and incubated with
a rabbit polyclonal antibody to mouse apoE or a rat monoclonal
antibody to mouse macrophages, MOMA-2 (Accurate Chemicals),
followed by incubation with biotinylated anti-rabbit or anti-rat
secondary antibodies. Signals were detected with peroxidase chromogen kits (Vector Laboratories). We used an FITC-labeled polyclonal antibody to human smooth muscle cell actin (Sigma) to detect
smooth muscle cells in the lesions.
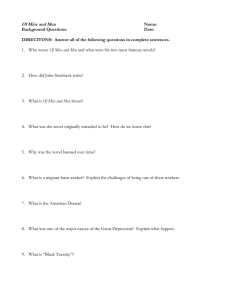
Figure 1. A, Western blot analysis of plasma apoE in apoE⫺/⫺
mice 2 weeks after BMT. One microliter of undiluted plasma
was electrophoresed on 12% SDS gels, transferred to nitrocellulose membranes, and probed with a polyclonal antibody to
mouse apoE. Lanes 1 through 6, mice transplanted with wildtype bone marrow; lanes 7 through 9, mice transplanted with
apoE⫺/⫺ bone marrow; lane 10, positive control (plasma from
wild-type mice). B, PCR of DNA extracted from the peripheral
blood of female apoE⫺/⫺ mice 2 weeks after transplantation to
amplify a 250-bp sequence of the Y chromosome. Lane 1,
100-bp ladder; lanes 2 through 8, samples from transplanted
mice; lane 9, negative control (female mouse DNA); lane 10,
positive control (male mouse DNA).
Plasma Lipid Measurements
Enzymatic assays for total cholesterol, HDL cholesterol, and triglyceride were performed in 96-well plates on a Biomek 2000 automated
laboratory workstation (Beckman Instruments, Inc) as described.34
Measurements on plasma samples were performed in triplicate with
known control samples on each plate to ensure accuracy.
Statistical Analysis
Plasma lipid levels were expressed as mean⫾SEM, with n indicating
the number of mice. Atherosclerotic lesion areas were expressed as
values of individual mice. ANOVA was used to compare differences
in atherosclerotic lesions and lipid levels among different groups of
mice over time. Differences were considered statistically significant
at P⬍0.05.
Results
Reconstitution of Recipient Bone Marrow
ApoE was detected by Western blot analysis in the plasma of
apoE⫺/⫺ mice reconstituted with wild-type bone marrow as
early as 2 weeks after transplantation (Figure 1A). In contrast,
apoE was absent in apoE⫺/⫺ mice reconstituted with apoE⫺/⫺
bone marrow. Moreover, because male mice containing XY
chromosomes were used as donors for the female recipients,
we designed primers to genotype a segment of the Y
chromosome. As shown in Figure 1B, 2 weeks after transplantation, the Y chromosome was detected by PCR in
peripheral leukocytes of recipient mice.
Effect of BMT on Plasma Lipids
Reconstitution of apoE⫺/⫺ mice with wild-type bone marrow
resulted in dramatic changes in plasma cholesterol and
triglyceride levels (Figure 2). Two weeks after transplantation, plasma total cholesterol and triglyceride levels were
significantly reduced and HDL cholesterol levels increased
(
P⬍0.05). By 4 weeks after transplantation, plasma total
cholesterol, triglyceride, and HDL cholesterol levels had
reached normal levels. In contrast, in apoE⫺/⫺3apoE⫺/⫺
mice, plasma total cholesterol levels gradually increased,
from 334⫾11 mg/L (mean⫾SEM) before transplantation to
556⫾24 mg/L 20 weeks after transplantation. There was a
significant decrease in triglyceride levels 2 weeks after
Shi et al
ApoE and Atherosclerosis in Mice
2263
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Figure 3. Atherosclerotic lesion areas in cross sections of aortic
root from apoE⫺/⫺ mice transplanted with apoE⫹/⫹ or apoE⫺/⫺
bone marrow. Each point represents a mean lesion area per
section from 1 mouse. Mice were fed a chow diet during the
experiment and were killed at 4, 12, and 20 weeks after transplantation. ApoE⫺/⫺3⫺/⫺ represents mice transplanted with
apoE⫺/⫺ bone marrow and killed 20 weeks after transplantation.
Figure 2. Effects of BMT on plasma total cholesterol (A), HDL
cholesterol (B), and triglyceride (C) levels in apoE⫺/⫺ recipient
mice. Plasma lipid levels were measured before and 2, 4, 12,
and 20 weeks after transplantation. ApoE⫺/⫺ mice were transplanted with bone marrow from either apoE⫹/⫹ or apoE⫺/⫺ mice.
Values are mean⫾SE of 7 to 12 mice. *P⬍0.05 vs
apoE⫺/⫺3apoE⫺/⫺.
transplantation (P⬍0.05). Plasma HDL cholesterol levels
were not significantly altered after transplantation.
Effect on Aortic Atherosclerotic Lesion Areas
The size of atherosclerotic lesions at the aortic root was
quantified by light microscopy. The apoE⫹/⫹3apoE⫺/⫺ mice
that were killed 4 weeks after transplantation had an average
lesion area per section of 12 347⫾2487 m2 (mean⫾SEM,
n⫽12; Figure 3). Twelve and 20 weeks after transplantation,
the average lesion areas of apoE⫹/⫹3apoE⫺/⫺ mice were
9340⫾2185 m2 (n⫽8) and 12 211⫾1433 m2 (n⫽9), respectively. Compared with mice that were killed 4 weeks
after transplantation, aortic lesion areas did not show a
significant increase or decrease in mice that were killed at 12
and 20 weeks after transplantation (P⬎0.05). In contrast,
apoE⫺/⫺3apoE⫺/⫺ mice developed severe atherosclerosis 20
weeks after transplantation, with an average lesion area of
453 036⫾29 767 m2 per section (n⫽7).
Effect on Morphology of Atherosclerotic Lesions
In mice that were killed 4 weeks after transplantation, aortic
lesions consisted primarily of macrophage-derived foam cells
(Figure 4). Smooth muscle cells were undetectable in the
lesions, and there were no fibrous caps. In mice that were
killed 12 weeks and 20 weeks after transplantation, aortic
lesions were flatter and had developed thin, fibrous caps in
about half of the mice. Macrophage-derived foam cells were
still the main cellular component of the lesions. Smooth
muscle cells were observed in the fibrous caps. In contrast,
mice reconstituted with apoE⫺/⫺ bone marrow developed
advanced lesions containing numerous smooth muscle cells,
calcification, and necrotic areas.
ApoE Expression in Atherosclerotic Lesions
Immunohistochemistry analysis showed that apoE was abundantly expressed in atherosclerotic lesions of the apoE⫺/⫺
mice reconstituted with wild-type bone marrow (Figure 5). In
contrast, apoE was not detected in lesions of those apoE⫺/⫺
mice reconstituted with apoE⫺/⫺ bone marrow.
Discussion
The principal aim of the present study was to evaluate
whether macrophage-derived apoE was sufficient to induce
significant regression of established atherosclerotic lesions in
apoE-deficient mice by BMT. Wild-type and apoE-deficient
mice were used as bone marrow donors for apoE-deficient
mice. We found that repopulation of cells in BMT-treated
mice with normal hematopoietic cells eliminated hypercholesterolemia and prevented progression of the lesions but did
not induce significant regression of established atherosclerosis in apoE-deficient mice.
BMT leads to the replacement of recipient tissue macrophages by macrophages of donor origin.35 Bone marrow cells
accumulate in the liver, spleen, and bone marrow several
hours after injection.36,37 By 4 weeks after transplantation,
⬎95% of macrophages in the bone marrow were of donor
2264
Arterioscler Thromb Vasc Biol.
October 2000
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Figure 4. Representative light photomicrographs of aortic atherosclerotic lesions
in apoE⫺/⫺ mice transplanted with
apoE⫹/⫹ or apoE⫺/⫺ bone marrow. Sections were stained with oil red O and
hematoxylin (A, B, C), an anti-mouse
macrophage antibody MOMA-2 (D, E, F),
or an FITC-labeled antibody to smooth
muscle cell actin (G, H, I). The first and
second columns represent lesions from
mice transplanted with apoE⫹/⫹ bone
marrow and killed at 4 and 20 weeks,
respectively, after transplantation. The
third column represents lesions from mice
transplanted with apoE⫺/⫺ bone marrow
and killed at 20 weeks after transplantation. Original magnification, ⫻25.
origin.29 In the present study, we observed that apoE was
present in the peripheral circulation as early as 2 weeks after
transplantation, and by 4 weeks, macrophage-derived apoE
was sufficient to normalize plasma lipid levels of apoEdeficient recipient mice. As in previous studies,38,39 we used
male mice as bone marrow donors for female recipients so
that engraftment of bone marrow could be verified by
genotyping male-specific makers of the Y chromosome.
Because donor and recipient mice were derived from the
same inbred strain, graft-versus-host disease would not occur.
Moreover, all recipient mice were healthy throughout the
experiment.
Although macrophages produce only a small percentage
(⬇10%) of plasma apoE, this amount is sufficient to reverse
hypercholesterolemia and elevate plasma HDL levels.29,30
Our present findings are consistent with this observation. The
finding that BMT induced a decrease of plasma triglyceride
levels in apoE⫹/⫹3apoE⫺/⫺ mice is consistent with that of a
previous study.31 The temporary decrease at 2 weeks was
probably caused by the transplantation procedure, because it
was also observed in apoE⫺/⫺3apoE⫺/⫺ mice.
Previous studies29 –31 and our present study have indicated
that after transplantation, a period of 4 weeks is required for
macrophage-derived apoE to achieve its full therapeutic
effect in apoE-deficient recipients. During this period, as
peripheral tissues are reconstituted with apoE-expressing
macrophages, plasma cholesterol levels gradually fall but
atherosclerotic lesions continue to progress. We observed a
significant increase in atherosclerotic lesion size, from
2613⫾781 m2 at the time of transplantation to
12 347⫾2487 m2 4 weeks after transplantation. Therefore,
selecting atherosclerotic lesions at 4 weeks after transplantation as the baseline seems an appropriate standard by which
to judge regression in apoE-deficient mice. In the present
experiment, apoE-deficient mice received transplantation at 8
weeks of age, and by the time their bone marrow was
replaced with donor marrow, they were 12 weeks of age.
Nakashima et al27 reported that apoE-deficient mice of this
age develop fatty streak lesions. Indeed, we observed that
atherosclerotic lesions of these mice consisted primarily of
macrophage-derived foam cells and that smooth muscle cells
and fibrous caps were absent in the lesions.
One important finding of the present study is that 16 weeks
after plasma lipid levels were normalized, the size of the
atherosclerotic lesions was not significantly reduced in apoEdeficient mice. This finding is consistent with the notion that
the regression of atherosclerotic lesions is a slow process.
Indeed, in the rhesus monkey model, Tucker et al5 did not
Figure 5. Immunohistochemical analysis of
apoE expression in aortic atherosclerotic
lesions of apoE⫺/⫺ mice transplanted with
apoE⫺/⫺ (A) or wild-type (B) bone marrow.
Sections were stained with a polyclonal rabbit
anti-mouse apo E antibody. Original magnification, ⫻40.
Shi et al
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
find definite evidence of regression after 4 months on a
low-fat diet. Kokatnur et al40 reported that experimental
atherosclerosis in rhesus monkeys showed evidence of regression only after treatment with a low-fat diet for 64 weeks.
However, Tsukamoto et al16 recently reported that liverdirected gene transfer and hepatic expression of human
apoE3 in chow-fed, apoE-deficient mice resulted in an almost
complete regression of fatty streaks within 6 weeks, whereas
expression of human apoE4 reduced cholesterol levels to the
same extent as apoE3 but did not induce significant regression. That study suggests that effects beyond the reduction of
plasma cholesterol levels are required to induce regression.
Mouse apoE is similar to human apoE3 in term of the 2
polymorphic amino acids.41 The reasons for the discrepancy
between the data of Tsukamoto et al16 and ours are unclear.
One possible explanation is that gene transfer resulted in
more apoE production than did BMT. Indeed, Desurmont et
al11 observed that regression of fatty streak lesions in apoE⫺/⫺
mice 6 months after injection of the adenovirus encoding
human apoE cDNA was dependent on plasma apoE
concentration.
Hyperlipidemia plays an important role in the progression
of atherosclerosis. However, elimination of hyperlipidemia
alone seems insufficient to induce regression of atherosclerosis. Indeed, our failure to observe a significant reduction of
atherosclerotic lesions 16 weeks after normalization of
plasma lipid levels suggests that treatments other than normalizing plasma lipid levels are necessary to induce significant regression of atherosclerosis.
Acknowledgments
This work was supported by National Institutes of Health grant
HL-30568. The authors thank Yishou Shi for technical help.
References
1. Armstrong ML, Warner ED, Connor WE. Regression of coronary atherosclerosis in rhesus monkeys. Circ Res. 1970;27:59 – 67.
2. Rossouw JE. Lipid-lowering interventions in angiographic trials. Am J
Cardiol. 1995;76:86C–92C.
3. Sacks FM, Gibson CM, Rosner B, Pasternak RC, Stone PH. The influence
of pretreatment low density lipoprotein cholesterol concentrations on the
effect of hypocholesterolemic therapy on coronary atherosclerosis in
angiographic trials: Harvard Atherosclerosis Reversibility Project
Research Group. Am J Cardiol. 1995;76:78C– 85C.
4. Wagner WD, Clarkson TB. Effect on regression potential of atherosclerosis produced by intermittent or continuous hypercholesterolemia. Atherosclerosis. 1977;27:369 –381.
5. Tucker CF, Catsulis C, Strong JP, Eggen DA. Regression of early cholesterol-induced aortic lesions in rhesus monkeys. Am J Pathol. 1971;65:
493–514.
6. Stone PH, Gibson CM, Pasternak RC, McManus K, Diaz L, Boucher
T, Spears R, Sandor T, Rosner B, Sacks FM. Natural history of
coronary atherosclerosis using quantitative angiography in men, and
implications for clinical trials of coronary regression: the Harvard
Atherosclerosis Reversibility Project Study Group. Am J Cardiol.
1993;71:766 –772.
7. Blankenhorn DH, Hodis HN. George Lyman Duff Memorial Lecture:
arterial imaging and atherosclerosis reversal. Arterioscler Thromb. 1994;
14:177–192.
8. Plump AS, Smith JD, Hayek T, Aalto-Setälä K, Walsh A, Verstuyft JG,
Rubin EM, Breslow JL. Severe hypercholesterolemia and atherosclerosis
in apolipoprotein E-deficient mice created by homologous recombination
in ES cells. Cell. 1992;71:343–353.
ApoE and Atherosclerosis in Mice
2265
9. Zhang SH, Reddick RL, Piedrahita JA, Maeda N. Spontaneous hypercholesterolemia and arterial lesions in mice lacking apolipoprotein E.
Science. 1992;258:468 – 471.
10. Linton MF, Babaev VR, Gleaves LA, Atkinson JB, Fazio S. Regression
of atherosclerosis in apolipoprotein E deficient mice after bone marrow
transplantation. Circulation. 1996;94(suppl I):I-519. Abstract.
11. Desurmont C, Caillaud JM, Emmanuel F, Benoit P, Fruchart JC, Castro
G, Branellec D, Heard JM, Duverger N. Complete atherosclerosis
regression after human apoE gene transfer in apoE-deficient/nude mice.
Arterioscler Thromb Vasc Biol. 2000;20:435– 442.
12. Tangirala RK, Tsukamoto K, Chun SH, Usher D, Puré E, Rader DJ.
Regression of atherosclerosis induced by liver-directed gene transfer of
apolipoprotein A-I in mice. Circulation. 1999;100:1816 –1822.
13. Murayama T, Yokode M, Kataoka H, Imabayashi T, Yoshida H, Sano H,
Nishikawa S, Nishikawa S, Kita T. Intraperitoneal administration of
anti-c-fms monoclonal antibody prevents initial events of atherogenesis
but does not reduce the size of advanced lesions in apolipoprotein
E-deficient mice. Circulation. 1999;99:1740 –1746.
14. Kozarsky KF, Donahee MH, Glick JM, Krieger M, Rader DJ. Gene
transfer and hepatic overexpression of the HDL receptor SR-BI reduces
atherosclerosis in the cholesterol-fed LDL receptor– deficient mouse.
Arterioscler Thromb Vasc Biol. 2000;20:721–727.
15. Gijbels MJ, van der Cammen M, van der Laan LJ, Emeis JJ, Havekes LM,
Hofker MH, Kraal G. Progression and regression of atherosclerosis in
APOE3-Leiden transgenic mice: an immunohistochemical study. Atherosclerosis. 1999;143:15–25.
16. Tsukamoto K, Rajendra Tangirala R, Chun SH, Puré E, Rader DJ. Rapid
regression of atherosclerosis induced by liver-directed gene transfer of
apoE in apoE-deficient mice. Arterioscler Thromb Vasc Biol. 1999;19:
2162–2170.
17. Mahley RW. Apolipoprotein E: cholesterol transport protein with
expanding role in cell biology. Science. 1988;240:622– 630.
18. Beisiegel U. Receptors for triglyceride-rich lipoproteins and their role in
lipoprotein metabolism. Curr Opin Lipidol. 1995;6:117–122.
19. Zannis VI, Cole FS, Jackson CL, Kurnit DM, Karathanasis SK. Distribution of apolipoprotein A-I, C-II, C-III, and E mRNA in fetal
human tissues: time-dependent induction of apolipoprotein E mRNA
by cultures of human monocyte-macrophages. Biochemistry. 1985;24:
4450 – 4455.
20. Williams DL, Dawson PA, Newman TC, Rudel LL. Synthesis of apolipoprotein E by peripheral tissues: potential functions in reverse cholesterol transport and cellular cholesterol metabolism. Ann N Y Acad Sci.
1985;454:222–229.
21. Driscoll DM, Getz GS. Extrahepatic synthesis of apolipoprotein E. J
Lipid Res. 1984;25:1368 –1379.
22. Linton MF, Gish R, Hubl ST, Bütler E, Esquivel C, Bry WI, Boyles
JK, Wardell MR, Young SG. Phenotypes of apolipoprotein B and
apolipoprotein E after liver transplantation. J Clin Invest. 1991;88:
270 –281.
23. Basu SK, Brown MS, Ho YK, Havel RJ, Goldstein JL. Mouse macrophages synthesize and secrete a protein resembling apolipoprotein E.
Proc Natl Acad Sci U S A. 1981;78:7545–7549.
24. Basu SK, Ho YK, Brown MS, Bilheimer DW, Anderson RG, Goldstein
JL. Biochemical and genetic studies of the apoprotein E secreted by
mouse macrophages and human monocytes. J Biol Chem. 1982;257:
9788 –9795.
25. Ghiselli G, Schaefer EJ, Gascon P, Brewer HB Jr. Type III hyperlipoproteinemia associated with apolipoprotein E deficiency. Science. 1981;
214:1239 –1241.
26. Reddick RL, Zhang SH, Maeda N. Atherosclerosis in mice lacking apo E:
evaluation of lesional development and progression. Arterioscler Thromb.
1994;14:141–147.
27. Nakashima Y, Plump AS, Raines EW, Breslow JL, Ross R. ApoEdeficient mice develop lesions of all phases of atherosclerosis throughout
the arterial tree. Arterioscler Thromb. 1994;14:133–140.
28. Lin CT, Xu YF, Wu JY, Chan L. Immunoreactive apolipoprotein E is a
widely distributed cellular protein: immunohistochemical localization of
apolipoprotein E in baboon tissues. J Clin Invest. 1986;78:947–958.
29. Linton MF, Atkinson JB, Fazio S. Prevention of atherosclerosis in apolipoprotein E-deficient mice by bone marrow transplantation. Science.
1995;267:1034 –1037.
30. Boisvert WA, Spangenberg J, Curtiss LK. Treatment of severe hypercholesterolemia in apolipoprotein E-deficient mice by bone marrow transplantation. J Clin Invest. 1995;96:1118 –1124.
31. Van Eck M, Herijgers N, Yates J, Pearce NJ, Hoogerbrugge PM, Groot
PH, Van Berkel TJ. Bone marrow transplantation in apolipoprotein
E-deficient mice: effect of apoE gene dosage on serum lipid concen-
2266
32.
33.
34.
35.
Arterioscler Thromb Vasc Biol.
October 2000
trations, -VLDL catabolism, and atherosclerosis. Arterioscler Thromb
Vas Biol. 1997;17:3117–3126.
Gubbay J, Collignon J, Koopman P, Capel B, Economou A, Munsterberg
A, Vivian N, Goodfellow P, Lovell-Badge R. A gene mapping to the
sex-determining region of the mouse Y chromosome is a member of a
novel family of embryonically expressed genes. Nature. 1990:346:
245–250.
Qiao JH, Xie PZ, Fishbein MC, Kreuzer J, Drake TA, Demer LL, Lusis
AJ. Pathology of atheromatous lesions in inbred and genetically engineered mice: genetic determination of arterial calcification. Arterioscler
Thromb. 1994;14:1480 –1497.
Hedrick CC, Castellani LW, Warden CH, Puppione DL, Lusis
AJ. Influence of mouse apolipoprotein A-II on plasma lipoproteins in
transgenic mice. J Biol Chem. 1993;268:20676 –20682.
Longo DL, Davis ML. Early appearance of donor-type antigen-presenting
cells in the thymuses of 1200 R radiation-induced bone marrow chimeras
correlates with self-recognition of donor I region gene products.
J Immunol. 1983;130:2525–2527.
36. Takezawa RI, Watanabe Y, Akaike T. Direct evidence of macrophage
differentiation from bone marrow cells in the liver: a possible origin of
Kupffer cells. J Biochem. 1995;118:1175–1183.
37. Hendrikx PJ, Martens CM, Hagenbeek A, Keij JF, Visser JW. Homing of
fluorescently labeled murine hematopoietic stem cells. Exp Hematol.
1996;24:129 –140.
38. Blomberg M, Rao S, Reilly J, Tiarks C, Peters S, Kittler E, Quesenberry
P. Repetitive bone marrow transplantation in nonmyeloablated recipients.
Exp Hematol. 1998;26:320 –324.
39. Eglitis MA, Mezey E. Hematopoietic cells differentiate into both
microglia and macroglia in the brains of adult mice. Proc Natl Acad Sci
U S A. 1997;94:4080 – 4085.
40. Kokatnur MG, Malcom GT, Eggen DA, Strong JP. Depletion of aortic
free and ester cholesterol by dietary means in rhesus monkeys with fatty
streaks. Atherosclerosis. 1975;21:195–203.
41. Rajavashisth TB, Kaptein JS, Reue KL, Lusis AJ. Evolution of apolipoprotein E: mouse sequence and evidence for an 11-nucleotide ancestral
unit. Proc Natl Acad Sci U S A. 1985;82:8085– 8089.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Effect of Macrophage-Derived Apolipoprotein E on Established Atherosclerosis in
Apolipoprotein E−Deficient Mice
Weibin Shi, Xuping Wang, Nicholas J. Wang, William H. McBride and Aldons J. Lusis
Arterioscler Thromb Vasc Biol. 2000;20:2261-2266
doi: 10.1161/01.ATV.20.10.2261
Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272
Greenville Avenue, Dallas, TX 75231
Copyright © 2000 American Heart Association, Inc. All rights reserved.
Print ISSN: 1079-5642. Online ISSN: 1524-4636
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://atvb.ahajournals.org/content/20/10/2261
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the
Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of the Web
page under Services. Further information about this process is available in the Permissions and Rights
Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online
at:
http://atvb.ahajournals.org//subscriptions/