Winter 2014 - Medical School
advertisement

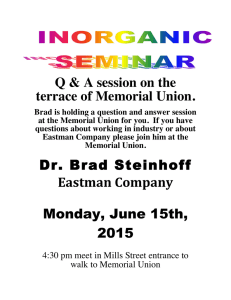
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| T I R R M E M O R I A L H E R M A N N .................................................................................................................... .................................................................................................................... THE INSTITUTE FOR REHABILITATION AND RESEARCH |W | | i| n| |t| e| |r| | 2| |0| 1| |4| | | | | IN THIS ISSUE 4 MESSAGE FROM THE CMO FEATURES 1Research Center Opening 5NIDRR Grant to Evaluate Memory Remediation with Donepezil Following Traumatic Brain Injury 6From Total Assist to Independence: Braxton Taylor Benefits from the Resources of TIRR Memorial Hermann’s Spinal Cord Injury Program 7Rehabilitation for Dysautonomia: TIRR Memorial Hermann and Children’s Memorial Hermann Hospital Collaborate to Treat a Complex Genetic Disorder 9Profiles in Caring: Lisa Thomas, CNS, RN, CRRN, APRN 10Techniques for Ensuring Active Engagement in Robotic Therapy of Upper Limb Function PERSPECTIVES ON RESEARCH 12Hair Cortisol: A Potential Biomarker of Emotional Distress among Persons with Traumatic Brain Injuries 16MESSAGE FROM THE CEO Digital Version To opt in for a digital version of this newsletter, please email tirrcommunications@ memorialhermann.org. TIRR Memorial Hermann Celebrates a Milestone with the Opening of a New Research Center TIRR Memorial Hermann opened its doors in 1959 as the Texas Institute for Rehabilitation and Research (TIRR), one of the country’s first rehabilitation hospitals. Over the span of 55 years, the institution has grown into a national leader in interdisciplinary rehabilitation, clinical care, education and research. Last fall, the hospital celebrated another milestone when the TIRR Memorial Hermann Research Center was completed and diverse research programs came together under one roof for the first time, creating new synergy between researchers, disciplines and programs. “Historically, our research programs have developed their protocols independently of each other,” says Mark Sherer, Ph.D., ABPP, FACRM, senior scientist and director of research at TIRR Memorial Hermann and a clinical professor in the departments of Physical Medicine and Rehabilitation at Baylor College of Medicine and UTHealth Medical School. “Because of the lack of space on our Campus, they were housed in several locations, including leased space outside the Texas Medical Center. Many of us had the idea of a research institute where cross-pollination of ideas could take place, but we had no idea that the possibility of renovating a building so close to the hospital would arise.” TIRR Memorial Hermann owned a long-vacant 42,000-square-foot building adjacent to the main hospital facility, purchased from UTHealth and formerly known as the UT Speech and Hearing Institute. During the 1970s and 1980s, the building housed Baylor College of Medicine research programs and TIRR Memorial Hermann offices in space leased from UTHealth. “The availability of a building so close to the hospital gave us the opportunity to bring all of our researchers together to promote synergy between the researchers themselves and also between the researchers and the hospital’s clinical team,” says Gerard Francisco, M.D., chief medical officer at TIRR Memorial Hermann and professor and chair of the department of Physical Medicine and Rehabilitation at UTHealth Medical School. “In most institutions research is conducted in silos that do not foster collaboration. Early on, we made the decision to change the status quo by designing an open layout that would New Research Center continues on page 2 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| New Research Center continued from page 1 encourage communication. We hope that bringing researchers in disparate disciplines together will change the way research is done in our field.” Lex Frieden, director of the Independent Living Research Utilization (ILRU) program, one of several research programs located in the new center, remembers the building before the renovation. “The original structure looked like a threestory, above-ground bunker. Concrete made the building seem chilling, and there were few windows, which gave it the uninviting feel of a fortress. The artificial lighting was old neon that gave off an eerie blue haze and made some people physically ill. Despite the fact that it was not a comfortable building, many talented people did good, meaningful work there. The new building gives a sense of reawakening that’s inspirational to people like me who knew it when it was old and tired. Suddenly, we see new space.” The dramatic transformation took more than three years to accomplish, from funding to finish. “We knew we needed to grow our Campus and also find room nearby for our researchers,” says Carl Josehart , CEO. “The old building was about the right size. We explored the idea of demolishing it and rebuilding, but we discovered it had good bones. It was structurally sound, and a renovation required a smaller investment, which felt fiscally responsible. It was also more environmentally friendly because we could repurpose an existing structure. We wouldn’t have sacrificed function to keep the building, but we wanted to honor the contributions that came out of it and breathe new life into it.” Funds raised through the Memorial Hermann Foundation’s successful Revolutionizing Neuroscience initiative helped make the renovation a reality. Filled with natural light, the new building invites interaction between the interior and exterior. An indoor dining room extends onto an outdoor patio, and its location across from Hermann Park allows researchers who work in one of the world’s largest medical centers to look outside and see green lawn and foliage. 2 TIRR MEMORIAL HERMANN Landscaping, color choices and photos of Hermann Park that decorate the 1st floor are among the elements that foster the idea of nature brought inside. Dr. Sherer remembers the building from his first tenure at TIRR Memorial Hermann and Baylor College of Medicine from 1991 to 1997. “It’s remarkable that we’ve been able to repurpose a building,” he says. “Few of the interior walls were structural, which allowed for their removal, creating an open space. An overhead walk connects our building to the hospital. These are separate buildings built at different times yet the overall effect pulls them together, creating the feeling that they were always connected.” Robots used for research and patient care Josehart calls the smooth move into the new building a testament to the thought that went into its planning and the success of the design in meeting the researchers’ needs. “There’s a sense that we’ve always been there,” he says. “People moved in and went right to work. Computers were on, and people were talking on the phone. No one looked lost. In designing the building and planning the move, we were able to use the same skills we use to help people plan for a smooth transition back to the community.” In the new building, researchers work together in the same space and share the same elevator, coffee room and copiers, offering opportunities for new relationships to develop. “The history of rehabilitation is replete with collaboration, which has led to breakthroughs in treatment and community reintegration,” Frieden says. “That same legacy applies to our move to the new building.” Internationally renowned academic physiatrist William H. Donovan, M.D., who retired as medical director of TIRR Memorial Hermann and chair of the department of Physical Medicine and Rehabilitation at UTHealth Medical School in 2009, after 28 years of service, says a long-term dream has finally been realized. “We recognized the benefits of having researchers close to clinicians but never had the opportunity to make that happen,” Dr. Donovan says. “TIRR Memorial Hermann has always excelled in translational research, taking knowledge gained through research and applying it in the clinical setting. The proximity of researchers studying traumatic brain injury and spinal cord injury fully integrates the hospital’s mission of research, teaching and clinical care. Close collaboration between researchers and clinicians was the original intention of TIRR Memorial Hermann’s founder, Dr. William A. Spencer. Were he alive today, he would surely be most pleased.” A sweeping, open pathway leads from the parking lot in front of the building to the doorway, inviting staff and visitors to enter. “It’s about a hundred steps from the hospital. You can leave the hospital through the back door, go down a sidewalk, take a right turn and you’re in the new building,” says Frieden. “It’s the personification of the vision of many people but Carl invested a lot of himself into making the research center a reality. He didn’t turn any screws or pound any nails, but he provided the leadership we needed. It’s a significant step forward for us as an institution.” Dr. Sherer considers it far more than a renovation. “Open space has replaced concrete cubicles, with a nice balance between privacy and connectedness,” he says. “If you want to stop by and talk to a colleague, you can. If you want to work uninterrupted in your office, you have privacy and quiet. It’s a rebirth.” u |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| TIRR Memorial Hermann Milestones 1951The Southwestern Poliomyelitis Respiratory Center opens in an annex to Harris County’s Jefferson Davis Hospital, the teaching hospital for Baylor College of Medicine, in response to the polio epidemic sweeping the nation. 1959TIRR, the Texas Institute for Rehabilitation and Research, opens its doors in the Texas Medical Center. As polio becomes less of a universal threat, the hospital focuses on the rehabilitation of patients with spinal cord deterioration caused by disease or trauma, pioneering the interdisciplinary team approach to rehabilitation. 1962TIRR establishes its Spinal Cord Injury Program and is designated a national Rehabilitation Research and Training Center (RRTC) for Rehabilitation Medicine by the Vocational Rehabilitation Administration of the U. S. Department of Health, Education and Welfare. Research conducted through its affiliation with Baylor College of Medicine makes the hospital an international leader in improving patient care. 1963TIRR becomes an important early research partner with NASA. 1964TIRR founder and director William A. Spencer, M.D., is named Physician of the Year by President Lyndon Johnson’s Commission on Employment of the Handicapped. 1970An annex to TIRR, acquired through donated funds, increases the hospital’s inpatient bed capacity and makes possible a unique residential program. 1972TIRR’s Spinal Cord Injury Program is named a Model Spinal Injury Treatment System. The Cooperative Living Program and the Maximum Independence Center, the nation’s first residential independent living programs for people with severe physical disabilities, are started at an annex near downtown Houston. 1977The Independent Living Research Utilization (ILRU) program is established as a national resource center providing research, training and technical assistance. 1978The hospital changes its name to The Institute for Rehabilitation and Research to emphasize its national and international service. 1984TIRR opens its inpatient Brain Injury Program. 1985The National Institute on Disability and Rehabilitation Research (NIDRR) designates TIRR as a national Research and Training Center on Independent Living. 1987NIDRR names the hospital’s Brain Injury Program a Model System. 1990U.S.News & World Report announces its first America’s Best Hospitals list. TIRR is named in this nationwide survey of physicians and has been included every year since. The innovative Challenge Program begun at TIRR as part of the Brain Injury Program, in keeping with TIRR’s philosophy of community-based service programming. 1992The Southwest Disability and Business Technical Assistance Center (DBTAC), one of 10 federally designed regional technical assistance centers on the Americans with Disabilities Act (ADA), is TIRR Memorial Hermann Journal is published four times a year by TIRR Memorial Hermann. Please direct your comments or suggestions to Editor, TIRR Memorial Hermann Journal, TIRR Memorial Hermann, 1333 Moursund, Houston, TX 77030, 713.797.7229. Carl E. Josehart, CEO Gerard Francisco, M.D. Chief Medical Officer Mary Ann Euliarte, RN, M.S.N., M.B.A., CRRN Chief Nursing Officer /Chief Operations Officer Mark Sherer, Ph.D., ABPP, FACRM Director of Research Susan Thomas, Editor Karen Kephart, Writer Steve Stanley, Designer established at TIRR. 1993UTHealth Medical School establishes a department of Physical Medicine and Rehabilitation. TIRR affiliates with the medical school that same year. 1996The departments of Physical Medicine and Rehabilitation at Baylor College of Medicine and UTHealth Medical School form the Baylor/UTHealth PM&R Alliance. 2001 Outpatient Rehabilitation opens at the Kirby Glen Center. 2006TIRR joins the Memorial Hermann Health System and becomes TIRR Memorial Hermann, one of 12 hospitals in the not-for-profit system known for clinical expertise, patient-centered care, leading-edge technology and innovation. 2012 TIRR Memorial Hermann begins the creation of a comprehensive, integrated rehabilitation network extending beyond the Texas Medical Center to outlying communities in the Greater Houston area. 2013 T he TIRR Memorial Hermann Research Center opens adjacent to the hospital, uniting the hospital’s research programs under one roof and creating an integrated Campus where the critical components of clinical care and research come together for the benefit of patients. Material in this publication may not be reproduced in whole or part without permission from TIRR Memorial Hermann. Winter 2014 We have opportunities for outstanding rehabilitation professionals. If you are interested in joining our team at U.S.News & World Report’s No. 3 rehabilitation hospital, contact Derrick Anderson, recruitment consultant, at 713.797.7281 or derrick.anderson@memorialhermann.org All available opportunities can be viewed at memorialhermann.org. www.tirr.memorialhermann.org, www.ilru.org T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 3 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| M F FEATURES MESSAGE FROM THE CMO As Braxton Taylor’s story illustrates, it takes an entire team to guide a patient from illness or injury to a return to meaningful participation in Gerard E. Francisco, the community. M.D., CMO There is no one right way to accomplish that goal; we do it by working together to touch each aspect of the individual’s life. That collaborative approach is mirrored in our research program. The new TIRR Memorial Hermann Research Center houses professionals in four seemingly disparate labs who work together synergistically to bring innovations to the bedside, the therapy gym, the outpatient care setting and the community. Investigators in the Neurorecovery Research Center, the Brain Injury Research Center, the Spinal Cord Research Program and the Independent Living Research Utilization program share the common goal of transforming lives and instilling hope in people whose lives have been significantly altered by illness or injury. Those shared goals create fertile ground for the discovery of solutions that will reduce activity limitations and participation restrictions on the individual level, and remove environmental and social barriers in the community. Rehabilitation doesn’t stop when a patient walks out our door. It ends only when the people we treat are valued participants in the world around them. Gerard E. Francisco, M.D. Chief Medical Officer TIRR Memorial Hermann Chair, Department of Physical Medicine and Rehabilitation UTHealth Medical School Save the Date: June 6-8, 2014 Advancing Wellness and Independence After Spinal Cord Injury Spinal Cord Symposium A multidisciplinary course for rehabilitation professionals to learn more about spinal cord injury. A variety of topics are available from which professionals from each discipline can choose to best match their individual learning needs and the needs of their healthcare settings. The goal is to provide teaching so that each professional can practice effectively in any setting that serves persons with spinal cord injury. Who should attend? Physicians, occupational therapists, physical therapists, speech-language pathologists, registered nurses, case managers, social workers, respiratory therapists and neuropsychologists. TIRR Memorial Hermann Friday, June 6, 11:30 a.m. – 5:30 p.m. Saturday, June 7, 8 a.m. – 5 p.m. Sunday, June 8, 8:30 a.m. – 12:30 p.m. To receive more information, please email: tirrcommunications@memorialhermann.org FEATURED IN THIS ISSUE Rhonda Abbott, PT Administrative Director Director of Therapy Services and Clinical Programs Brain Injury and Stroke, Spinal Cord Injury and Specialty Rehabilitation Programs David B. Arciniegas, M.D. Senior Scientist, Medical Director for Brain Injury Research, TIRR Memorial Hermann Executive Director of the Beth K. and Stuart C. Yudofsky Division of Neuropsychiatry and Professor, Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine Adele Bosquez, PT, D.P.T., ATC, LAT Physical Therapist, Spinal Cord Injury and Specialty Rehabilitation Programs Teresa Cramer, PT, D.P.T., PCS Pediatric Clinical Coordinator TIRR Memorial Hermann Outpatient Rehabilitation at the Kirby Glen Center Jessica Dalmolin, D.P.T. Physical Therapist, TIRR Memorial Hermann Adult and Pediatric Outpatient Rehabilitation at the Kirby Glen Center 4 TIRR MEMORIAL HERMANN Matthew Davis, M.D. Clinical Director, Spinal Cord Injury Program William H. Donovan, M.D. Former Medical Director, TIRR Memorial Hermann Former Chair, Department of PM&R, UTHealth Medical School Gerard E. Francisco, M.D. Chief Medical Officer and Director of the NeuroRecovery Research Center Professor and Chair of the Department of PM&R, UTHealth Medical School Lex Frieden Senior Scientist, Director, Independent Living Research Utilization Professor of Biomedical Informatics and Professor of Rehabilitation, UTHealth Medical School Professor of Rehabilitation, Baylor College of Medicine Carl Josehart Chief Executive Officer System Executive for Rehabilitation Services Marcia K. O’Malley, Ph.D. Senior Scientist, Director of Rehabilitation Engineering, TIRR Memorial Hermann Associate Professor of Mechanical Engineering and Materials Science, Rice University Director of the Mechatronics and Haptic Interfaces (MAHI) Lab, Rice University Adjunct Associate Professor of PM&R, Baylor College of Medicine Adjunct Associate Professor of PM&R, UTHealth Medical School Angelle Sander, Ph.D. Director, Brain Injury Research Center, TIRR Memorial Hermann Associate Professor of PM&R, Baylor College of Medicine Mark Sherer, Ph.D., ABPP, FACRM Senior Scientist, Director of Research and Director of Neuropsychology, TIRR Memorial Hermann Clinical Professor of PM&R, Baylor College of Medicine and UTHealth Medical School Lisa Thomas, CNS, RN, CRRN, APRN Director of Clinical Education, TIRR Memorial Hermann and the Memorial Hermann Rehabilitation Network Affiliated with TIRR Memorial Hermann TIRR Memorial Hermann Awarded NIDRR Grant to Evaluate Memory Remediation with Donepezil The National Institute on Disability and Rehabilitation Research (NIDRR) has awarded $3 million to TIRR Memorial Hermann to perform a five-year study to determine whether the medicine donepezil is an effective treatment for memory deficits resulting from traumatic brain injury (TBI). Memory deficits are among the most common chronic and functionally important consequences of TBI. Basic science studies and clinical trials suggest that persistent deficits in verbal memory are associated with chronically reduced levels of the neurotransmitter acetylcholine in the brain. While medications, such as donepezil, that increase the amount of acetylcholine in the brain appear to improve memory and other cognitive problems, research conducted to date has not provided the level of evidence needed to establish best practices. Investigators at TIRR Memorial Hermann hope evidence gained from the new trial will influence the practices of prescribing healthcare providers and contribute knowledge that will improve the lives of persons with TBI and their families. Entitled “Multicenter Evaluation of Memory Remediation after TBI with Donepezil” (the MEMRI-TBI-D Study), the 10-week trial will evaluate the effects of 10 milligrams of donepezil, administered daily, on verbal memory problems among adults with TBI in the subacute or chronic recovery period. The study will enroll 160 persons with TBI and functionally important memory problems at four study sites across the country. Principal investigator/project director for the MEMRI-TBI-D Study is David B. Arciniegas, M.D., senior scientist and medical director for brain injury research at TIRR Memorial Hermann and executive director of the Beth K. and Stuart C. Yudofsky Division of Neuropsychiatry at Baylor College of Medicine. Neuropsychologist Angelle Sander, Ph.D., director of the Brain Injury Research Center at TIRR Memorial Hermann and associate professor of physical medicine and rehabilitation at Baylor College of Medicine, is co-principal investigator. Drs. Arciniegas and Sander are joined by co-investigator Mark Sherer, Ph.D., ABPP, FACRM, director of research and director of neuropsychology at TIRR Memorial Hermann and clinical professor of physical medicine and rehabilitation at Baylor College of Medicine. As the recipient of the grant, TIRR Memorial Hermann will lead a national team of collaborators at Spaulding Rehabilitation Hospital in Boston, Moss Rehabilitation Research Institute in Philadelphia, Indiana University in Indianapolis and Craig Hospital in Englewood, Colo. “We’re fortunate to bring this group of investigators together to conduct this clinical trial,” Dr. Arciniegas says. “The MEMRI-TBI-D Study capitalizes on the extensive successful research on brain injury rehabilitation within and between the participating centers. It also will benefit from this groups’ expertise in the study of pharmacologic and rehabilitative treatments for cognitive problems resulting from traumatic brain injuries.” The announcement of the grant coincides with the opening of the TIRR Memorial Hermann Research Center, the new home of the Brain Injury Research Center (BIRC). BIRC was founded in the 1980s to conduct research that improves outcomes for persons with brain injuries. The principal goal of research conducted at the Center is to reduce barriers to daily function and enable persons with TBI to return to full participation in life. The goals of the MEMRI-TBI-D Study complement those of other research projects under way at BIRC. “Our aim is to determine if donepezil, a medicine that addresses one of the chronic neurochemical deficits produced by traumatic brain injury, improves memory performance in persons with TBI,” Dr. Arciniegas says. “If this treatment is successful, persons with memory problems after TBI will experience improvements in day-to-day memory.” Enrollment will begin in spring 2014; each study site will enroll 10 participants per year over the 48-month period of active recruitment. “The quality of the evidence yielded by this study will directly affect the way healthcare providers serve persons with memory problems after TBI,” Dr. Arciniegas says. “Since donepezil is available in a generic form, it also offers the promise of an affordable treatment option for many persons with TBI and their families. If donepezil is found to be effective in individuals with memory problems after TBI, we hope that these findings will inform the practices of rehabilitation programs across the country and internationally.” u T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 5 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| From Total Assist to Independence: Braxton Taylor Benefits from the Resources of TIRR Memorial Hermann’s Spinal Cord Injury Program When 20-year-old Braxton Taylor arrived at TIRR Memorial Hermann in August 2013, he was unable to walk, transfer, eat or manage other activities of daily living without total assistance. When he was discharged on Halloween, he could walk with assistance and was independent in most aspects of daily care, a tribute to his motivation and the resources of TIRR Memorial Hermann’s Spinal Cord Injury Program. Born with Arnold-Chiari malformation, Taylor began to experience symptoms – weakness on the right side and headaches – when he was in high school. A neurological disorder of the cerebellum, the part of the brain that controls balance, Arnold-Chiari malformation occurs when parts of the cerebellum and brain stem are pushed downward into the foramen magnum, a funnel-like opening to the spinal canal, and into the upper part of the spinal canal. The result is pressure on the cerebellum that can affect functions controlled by this area of the brain and block the flow of cerebrospinal fluid (CSF) to and from the brain. Diagnosed in 2008, Taylor has had neurosurgery every year since then for treatment of the disorder and related conditions. In July 2013, he suffered a cerebral hemorrhage in the left frontal lobe of the brain that left him with hemiplegia. “Braxton was admitted to the Spinal Cord Injury Program because so many of his needs paralleled those of our cord injury patients, but in fact, he benefited from nearly every inpatient program we have,” says Adele Bosquez, PT, D.P.T., ATC, LAT, a physical therapist in the Spinal Cord Injury and Specialty Rehabilitation Programs. “In complex cases like Braxton’s, it truly takes an entire team.” Led by physical medicine and rehabilitation specialist Lisa Wenzel, M.D., Taylor’s 6 TIRR MEMORIAL HERMANN team included therapists, nurses, case managers and social workers who practice a unified, interdisciplinary approach to patient care. “I had big goals and worked hard to accomplish them,” says Taylor, who has completed three semesters at St. Mary’s University in San Antonio and plans to begin online courses to continue his education in the interim. “The team at TIRR Memorial Hermann was really good at helping me get there. My main goal was to be able to walk and live more independently, and they threw everything they had at me. The variety of equipment was very cool.” Among the tools he worked with is the Bioness Vector Elite Gait and Safety System™, a harness support device that runs on a ceiling track, allowing him to practice walking over ground while his therapists gradually decreased the amount of his weight the device was carrying. “When patients are relearning how to walk, one of the significant barriers to progress is fear of falling,” says Matthew Davis, M.D., clinical director of the Spinal Cord Injury Program. “The Vector takes away that risk and gives our staff the comfort and assurance that the patient is safe. It’s particularly useful for developing competency in patients with incomplete spinal cord injury and those like Braxton who have the potential to walk again.” Taylor also benefited from other technologies, including the Hocoma Armeo®Spring, an ergonomic arm exoskeleton with integrated springs that enhances function and neuromuscular control; FES Bike, which applies small electrical pulses to paralyzed muscles to restore or improve their function; specially designed knee-ankle-foot orthoses (KAFOs) that stabilize the joints and assist the muscles of the leg; and an Ekso™ exoskeleton, a wearable bionic suit that enables individuals with lower-extremity weakness to stand and walk over ground to improve strength, mobility and endurance. In occupational therapy, Taylor worked to improve his balance. “Braxton has good, strong core musculature, but his sense of balance is off,” says Bennett Cope, OTR. “We worked on finding his center of balance and realigning it, and later began working on functional tasks, such as dressing, eating and other activities of daily living. He’s a very, very smart kid with a strong work ethic. We could tell from day one that he was very practical in his approach to rehabilitation. He threw in ideas of his own and would never say no to anything we asked of him in a therapy session. I’d see him doing his homework after his sessions, and he worked with his nurses to stay on top of his care. When he was admitted, he was only able to take one or two bites of food unassisted. When he left, he could eat on his own.” Taylor participated in TIRR Memorial Hermann’s community dining program, in which patients with spinal cord injury and others dine in a group at local restaurants to regain confidence. As part |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| of the hospital’s community reintegration program, he attended an outing at the University of Houston focused on overcoming barriers to returning to school. He also joined FAME (Functional Arm Movement for Everyone), a program focused on increasing awareness and functional use of the impaired upper extremity. “A social worker made sure he and his family were aware of other programs he qualified for,” Bosquez says. “We helped him find transportation near home and gave him resource information for the Texas Department of Assistive and Rehabilitative Services.” Cope and Bosquez worked with Taylor to find an appropriate wheelchair. “He didn’t want a power wheelchair because of the size and weight, but he didn’t have the strength to use a manual wheelchair,” Cope says. “We found the right manual chair for him and added a power function for maximum independence.” A week before discharge, he participated in an in-house pass program that allowed his mother, Rosalyne Taylor, to stay with him for 24 hours to develop a hands-on understanding of the help he would need at home. “We’ve always had a good Spinal Cord Injury Program, and with all the technology we’ve added, we can offer our patients much more today than we could even a year ago,” Bosquez says. Terree Funesti, RN, WCC, CRRN, clinical manager of the Spinal Cord Injury Unit, remembers Taylor as a “real gentleman who told his nurses every day how much he appreciated them. We really liked him, and like many young people, he fit into our unit like family. The beauty of rehabilitation nursing is that we see inpatients through their entire experience at the hospital. They come to us in such an acute condition and we help them gain their independence medically so they can get downstairs to the gym. Encouraging them to use the skills they learn in therapy and watching them transition from total assistance to independence is incredibly rewarding for us as nurses.” Rhonda Abbott, PT, administrative director of therapy services and clinical programs, points to Taylor’s case as exemplary. “This is one of many cases in which we all pull together with the patient in unique, personalized ways to truly address function, community and meaningful participation,” she says. “We have the ability to do it all at TIRR Memorial Hermann, but what really makes us special is having creative therapists who can identify a young man’s needs and come up with a program designed to meet his specific goals. Making a difference in lives like Braxton’s and those who love him is where it’s at.” Taylor says he’s come a long way in a relatively short period of time. “I walk with a walker and a little assistance to help with my balance issues,” he says. “I wouldn’t be where I am today without TIRR Memorial Hermann and my faith. They’re all great people to work with – motivating and very supportive.” u Rehabilitation for Dysautonomia: TIRR Memorial Hermann and Children’s Memorial Hermann Hospital Collaborate to Treat a Complex Genetic Disorder Eighteen-year-old Justin Lamb is one of many patients to benefit from a unique collaboration between TIRR Memorial Hermann and the pediatric neurology and pediatric cardiology services at Children’s Memorial Hermann Hospital. Working together, the two institutions have developed a program that provides a complete continuum of care for children and adolescents with dysautonomia, a complex genetic disorder that affects the autonomic nervous system and can cause life-threatening medical complications. “Dysfunction of the autonomic nervous system can cause a number of health problems related to the functions it controls, including heart rate, blood pressure, digestive tract peristalsis and Justin Lamb celebrates his 18th birthday sweating, among other things,” says pediatric neurologist Ian Butler, M.D., Adriana Blood Professor in Neurology and director of the division of Child and Adolescent Neurology at UTHealth Medical School, who with pediatric cardiologist Mohammed Numan, M.D., operates a combined child neurology and cardiology clinic for dysautonomia patients at Children’s Memorial Hermann Hospital. “Because of the complexity of the disorder and array of symptoms it produces, these kids are easy to miss and difficult to diagnose. Like Justin, they end up going from specialist to specialist. Years may pass before their parents have a conclusive diagnosis.” Dysautonomia continues on page 8 T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 7 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Dysautonomia continued from page 7 Born in 1995 at 36 weeks, Justin had health challenges from birth. “He had severe GI symptoms, so we saw a gastroenterologist,” says his mother Meredith Lamb. “He had migraines that were treated by his pediatrician. Later he developed some problems with walking, but his health issues never dramatically improved or worsened until he contracted the H1N1 flu virus in 2009. The flu started a downward spiral that we later learned is characteristic of dysautonomia.” From influenza, Justin went to pneumonia and pleurisy. When he developed more serious problems with walking and began posturing his hands strangely, his mother took him to an orthopedist, who recognized his symptoms as neurological and referred them to Dr. Butler. On one visit to Dr. Butler, Lamb mentioned that her son had experienced dizziness, which, along with his overall presentation, prompted the neurologist to consider dysautonomia. He referred Justin to Dr. Numan for a tilt-table test, the gold standard for diagnosis of the disorder. Patients are strapped to the tilt table lying flat, then tilted upright to about 70 degrees. The 30-minute test is considered positive if the patient experiences symptoms associated with a drop in blood pressure, such as fainting or cardiac arrhythmia. “The tilt-table test reproduces the clinical manifestations of dysautonomia, giving us a clear indication that the autonomic nervous system is malfunctioning,” says Dr. Numan, an associate professor in the division of Pediatric Cardiology at UTHealth Medical School. “This is particularly important because it’s very common for dysautonomia patients to be misdiagnosed with psychological disorders. They suffer from overwhelming fatigue. They have nausea that’s not always explainable. They complain bitterly of pain in their shoulders, back and legs. Some complain of tingling in their hands and feet. The body is trying to compensate for lack of oxygenated blood, and it shuts down blood flow to muscles and non-vital organs. Their physicians order one diagnostic test after another. When there 8 TIRR MEMORIAL HERMANN are no findings – a common occurrence with dysautonomia – the disorder is mislabeled as psychogenic. But the kids are suffering, and they get depressed when they’re unable to find help.” After the tilt-table test, Justin was diagnosed with dysautonomia. Dr. Numan also found an atrial septal defect of the heart and closed the hole in an endovascular repair in December 2011. For Justin and other children and adolescents with dysautonomia, acute care is only the first step in treatment. “These children become deconditioned very quickly,” Dr. Butler says. “We use medications to increase the vascular volume to the brain because the blood tends to pool in the legs and pelvis. Many are in physical therapy. When we started looking for a medical home for our dysautonomia patients, it seemed natural to approach TIRR Memorial Hermann. We contacted hospital leadership, and they put together a round table. We discovered we were speaking the same language. We do tilt-table testing; they use a tilt table therapeutically. Our patients do well in aquatic therapy; they have a strong aquatic program. It was a good fit.” Teresa Cramer, PT, D.P.T., PCS, pediatric clinical coordinator at TIRR Memorial Hermann Outpatient Rehabilitation at the Kirby Glen Center, spent time observing the two physicians and their patients in clinic and learned about symptoms and health issues. “This is familiar territory for us,” Cramer says. “Frequently, patients with traumatic brain injury or spinal cord injury have autonomic nervous system dysfunction. Dysautonomia symptoms can range from very mild to very debilitating, and these patients need specialized care. We put together a core team to work with Drs. Butler and Numan, and trained our staff using what we learned from them and from the pertinent rehabilitation literature. The result is a multimodal approach to therapy that provides dysautonomia patients with the help they need consistently.” Jessica Dalmolin, D.P.T., was Justin’s physical therapist at TIRR Memorial Hermann Outpatient Rehabilitation at the Kirby Glen Center. “With dysautonomia patients we emphasize cardiovascular exercise to increase blood flow to the muscles in positions that decrease orthostatic stress, including supine, prone, recumbent and sitting positions,” she says. “As they build up tolerance we add more upright exercise, incorporating yoga, Pilates and light weights, as well as balance and stretching exercises. We slowly progress to a standing position. They exercise with a heart rate monitor so we can track their exertion during the session, and we ask them to monitor their symptoms at home by keeping a journal. They record any exercise they do at home, how long they slept, if they had any lightheadedness, headaches or brain fog after their therapy session. If they’re exhausted the day after their session, we know we have to adjust their therapy program. The journal helps us personalize treatment to their particular needs.” Justin’s journal gave Dalmolin a good picture of what he experienced during the week he kept it. “He’s a great kid with a really supportive mom,” she says. “She let him lead and take charge of his own treatment, but if he had questions, she was there to help. Like many kids with dysautonomia, Justin was very in tune with his body and well educated about the disorder. He was willing to work hard and was not afraid to let me know when symptoms or fatigue got the best of him. His mom is a great advocate for him and for the dysautonomia population.” Meredith Lamb and her family, including 24-year-old son Marc who has a milder form of dysautonomia, are committed to raising awareness about the disorder. In May 2013, they formed the Lamb Foundation for Dysautonomia Research to raise funds in support of studies being conducted at Children’s Memorial Hermann Hospital and UTHealth Medical School. Drs. Butler and Numan have several research projects under way or completed, including the role of histamine and mast cells in dysautonomia, cerebrospinal fluid neurotransmitters, immunomodulation treatment protocols and DNA studies utilizing whole exome analysis of families. It’s not uncommon for more severe |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| cases of dysautonomia to rob teenagers of their high school years. “Justin still has good days and bad days,” his mother days. “The bad days made him miss his entire high school experience. He tried to go back to school twice but became sick and came home again. We did an online high school program and he did pretty well in his sophomore year, but then he was too sick to keep up. We tried home schooling. He will get his GED, and we will move on. “Dr. Butler, Dr. Numan and TIRR Memorial Hermann are family now,” Lamb adds. “We spent years going from specialist to specialist. We’re very grateful for the help we’ve found.” u Justin resumed physical therapy and began aquatic therapy at TIRR Memorial Hermann-The Woodlands’ new outpatient center in December 2013. TIRR Memorial Hermann accepts physician referrals for children and adolescents with dysautonomia at several locations in Houston. To refer a patient for rehabilitation, please call 1.800.44.REHAB (73422). Profiles in Caring: Lisa Thomas, CNS, RN, CRRN, APRN It’s no surprise that Lisa Thomas was recognized in 2013 as a Good Samaritan Foundation Excellence in Nursing Bronze Medalist, an award program created to recognize “nursing’s best and brightest.” An advanced practice nurse and clinical nurse specialist in adult health, she brings energy, expertise and enthusiasm to her role as director of clinical education for TIRR Memorial Hermann and the hospital’s growing citywide rehabilitation network. “With our strong emphasis on standards of practice and quality improvement at TIRR Memorial Hermann, we’re working in a rapidly changing environment,” says Thomas, who oversees four educators, library services and education resources. “With every change, whether it’s a new policy, a new process or a new product, there’s an educational component we have to address with nurses, therapists and residents. Because the hospital is constantly expanding the boundaries of rehabilitation with new knowledge and new techniques, we stay busy as educators.” Thomas grew up with a scientific bent. “I’ve always enjoyed the sciences in general, and I considered different disciplines before deciding to become a nurse,” she says. She had a strong role model in her grandmother, a diploma-trained nurse with the Memorial Sisters of Charity who retired after 50 years of service, the last 20 of which she spent at The University of Texas MD Anderson Cancer Center as an oncology nurse. Thomas’s first exposure to rehabilitation came when she was in high school in Alvin, Texas. “My grandfather had a stroke and moved into my parents’ home, where he lived for the next 20 years,” she says. “His presence raised my awareness of caregiver challenges and care coordination issues. I was impressed by how much improvement his early rehab stay made in his recovery.” After graduating from high school, Thomas received a full scholarship to the University of Houston pre-pharmacy program. When she made the decision to become a nurse, she transferred to The University of Texas Medical Branch at Galveston, completing her bachelor’s in nursing in 1994. She was employed by hospitals in Houston, Vero Beach, Florida, and Dallas, before accepting a position as a weekend staff nurse at TIRR Memorial Hermann in 2003. She was soon promoted to the newly created position of weekend night operations administrator, a role that provided her a first glimpse of the big picture and raised her awareness of the need for process improvements. In her new position, she began staff education and auditing of results, as well as patient and family education. In 2005, while working at the rehabilitation hospital, she was accepted into the Master of Science Clinical Nurse Specialist-Adult Health program at Texas Woman’s University (TWU). She graduated, was certified as a clinical nurse specialist and applied for licensure through the state as an advanced practice nurse in 2009. She completed final coursework for her post-master’s certification in nursing education that same year. She was still a weekend operations administrator when she brought a clinical group from TWU to TIRR Memorial Hermann, serving as adjunct faculty for them. When she transitioned to a fulltime education role, she helped train her adjunct replacement. The hospital continues to host students from TWU. Actively engaged in research, Thomas is currently working on a collaborative project to examine the experience of amputees who see themselves in the mirror for the first time following their amputation. “This is a powerful patient experience that crosses multiple disciplines, including physical therapy, occupational therapy and nursing,” she says. “Our research partner at TWU has examined the experience of women after mastectomy in ways that help them recover and form a new view of themselves. We’re very interested in investigating how these findings might apply to patients who have undergone upper- or lowerextremity amputation.” The first in her family to earn a bachelor’s degree, Thomas is currently enrolled in the Doctor of Nursing Practice program at UTHealth School of Nursing, with an expected graduation date of May 2015. Designed for nursing executives, the program encourages a broader, more Profiles in Caring continues on page 12 T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 9 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Techniques for Ensuring Active Engagement in Robotic Therapy of Upper Limb Function S By Marcia K. O’Malley, Ph.D. High intensity and high repetition upperlimb movements are necessary for recovery of function following neurological injury, since such actions are capable of inducing brain and spinal plasticity. Robotic devices are uniquely suited for delivering such intensive, repetitive therapy. However, studies have shown that passively moving the limb through prescribed trajectories is not necessarily efficacious. In order to derive maximum benefit from robotassisted rehabilitation, it is critical that the implemented control algorithms, which govern how the robotic device and the participant interact, promote the participant’s active engagement in therapy. My research group at Rice University has been developing novel approaches for ensuring cognitive engagement of the patient during robotic rehabilitation of the upper limb following stroke or incomplete spinal cord injury. In this article I present several techniques that we have used, including the development of objective measures of motor impairment that can be used for frequent feedback to the therapist and patient regarding their progress, robotic control architectures intended to promote engagement and intentful movements by the participant, and the design and implementation of compliant robotic hardware systems that facilitate novel control approaches such as interaction control. In our early work (Celik et al., 2010), we analyzed the correlations between four clinical measures (Fugl–Meyer upper extremity scale, Motor Activity Log, Action Research Arm Test and Jebsen-Taylor Hand Function Test) and four robotic measures (smoothness of movement, trajectory error, average number of target hits per minute and mean tangential speed) used to assess motor recovery. Data were gathered as part of a hybrid robotic and traditional upper extremity rehabilitation program for nine stroke patients. Smoothness of movement and trajectory error, temporally and spatially normalized measures of movement quality defined for point-topoint movements, were found to have significant moderate to strong correlations Validation of real-time trajectory recalculation. The subject initially moves faster than the desired trajectory, causing several recalculations with corresponding decrease in total allocated time. After a transient, the total time remains roughly constant at 0.8 s. 10 TIRR MEMORIAL HERMANN with all four of the clinical measures. The strong correlations suggest that smoothness of movement and trajectory error may be used to compare outcomes of different rehabilitation protocols and devices effectively, provide improved resolution for tracking patient progress compared to only pre- and post-treatment measurements, enable accurate adaptation of therapy based on patient progress, and deliver immediate and useful feedback to the patient and therapist. More recently, we have focused on the development of novel control algorithms that govern how the robot and participant interact during robot-assisted upper limb therapy (Pehlivan et al., 2013). A class of controllers named “assist-as-needed” addresses the requirement of promoting active engagement by providing only appropriate assistance during movement execution. Often, these controllers depend on the definition of an optimal movement profile, against which the participant’s movements are compared. We have proposed an assist-as-needed controller that introduces a novel feedback gain modification algorithm, making the controller adaptive. By modifying the gains of the feedback part of the adaptive controller directly, we are able to change the action of the adaptive controller based on the amount of error allowed during movement execution, while simultaneously estimating the forces provided by the participant that contribute to movement execution. We have also implemented a real-time trajectory generation algorithm based on a physiologically optimal and experimentally validated asymmetric wrist movement profile. The feedback gain modification and trajectory generation algorithms have been experimentally validated with our custom RiceWrist robotic rehabilitation system, with the modified assist-asneeded adaptive controller decreasing its feedback control action when a subject moothness of movement and trajectory error, temporally and spatially normalized measures of movement quality defined for point-to-point movements, were found to have significant moderate to strong correlations with all four of the clinical measures. shifts his behavior from passively riding along with the robot during movement to actively engaging and initiating movements to the desired on-screen targets. Finally, we have proposed the inclusion of physical compliance in our robotic hardware in order to enable implementation of interaction control techniques (Sergi et al., 2013). In the rehabilitation scenario, such control schemes assist motion by applying variable levels of mechanical assistance, with the capability of adapting to and capitalizing on the residual contributions of the subjects. Moreover, evidence from human trials with stroke subjects (Hogan et al., 2006) and from preliminary studies on animal models of spinal cord injury (R. van den Brand et al., 2012) confirms the hypothesis that interaction control schemes are more capable of promoting plasticity through mechanical interaction compared to motion control. In force-feedback interaction control, the force of interaction between the robot and the environment is measured and fed back to the controller driving the actuators, which specifies new desired force or position/velocity commands. In a Series Elastic Actuation (SEA) architecture (Williamson, 1995; Robinson, 2000), compliant elements with deflection/force measurement capabilities are intentionally introduced in series between the actuator and the load, effectively acting as a mechanical filter that decouples the non-linearities of geared actuators from the output and enables implementation of force-feedback control laws. The introduction of physical compliance with well-known properties enables the deployment of accurate interaction control schemes, thus mimicking the traditional therapistbased physical therapy, essentially based on the adaptive and compliant transfer of support forces. We have developed a prototype version of our RiceWrist robotic device (Gupta et al., 2008) that incorporates series elasticity, and we will be clinically evaluating its performance in the near future. Whether we leverage the sensors on the robotic device to compute performance measures that track participant performance throughout therapy and provide frequent feedback to the therapist and the individual as a means of motivating their engaged participation in therapy, or implement novel hardware design and control architectures enabling active physical interaction between patient and robot, the overall objective is the same – to motivate the participant to remain cognitively and physically engaged during the course of robotic upper-limb therapy, in order to facilitate maximum recovery of movement coordination. u (ICORR), Seattle, Washington, June 24-26, 6 pages. Celik, O., M.K. O’Malley, C. Boake, H. Levin, N. Yozbatiran, and T. Reistetter. (2010) Normalized Movement Quality Measures for Therapeutic Robots Strongly Correlate with Clinical Motor Impairment Measures, IEEE Transactions on Neural Systems and Rehabilitation Engineering 18(4): 433-444. Marcia O’Malley, Ph.D. is director of reha- Gupta, A., M. K. O’Malley, V. Patoglu, and C. Burgar, “Design, Control and Performance of RiceWrist: A Force Feedback Wrist Exoskeleton for Rehabilitation and Training,” The International Journal of Robotics Research, vol. 27, no. 2, pp. 233–251, Feb. 2008. Hogan, N. et al., “Motions or muscles? Some behavioral factors underlying robotic assistance of motor recovery,” The Journal of Rehabilitation Research and Development, vol. 43, no. 5, p. 605, 2006. Robinson, D.W., “Design and Analysis of Series Elasticity in Closedloop,” PhD thesis, MIT, pp. 1–123, Dec. 2000. Sergi, F., M. Lee, and M.K. O’Malley (2013) Design of a series elastic actuator for a compliant, parallel wrist rehabilitation robot, Proceedings of the IEEE International Conference on Rehabilitation Robotics (ICORR), Seattle, Washington, June 24-26, 6 pages van den Brand, R., et al., “Restoring Voluntary Control of Locomotion after Paralyzing Spinal Cord Injury,” Science, vol. 336, no. 6085, pp. 1182–1185, May 2012. Williamson, M.M. “Series Elastic Actuators,” PhD thesis, MIT, pp. 1–83, Sep. 1995. bilitation engineering at TIRR Memorial Hermann. An associate professor in the Mechanical Engineering and Materials Science department and director of the Mechatronics and Haptic Interfaces (MAHI) Lab at Rice University, Dr. O’Malley is a co-founder of Houston Medical Robotics. She holds a joint appointment in computer science at Rice, and is an adjunct associate professor in the departments of Physical Medicine and Rehabilitation at both Baylor College of Medicine and UTHealth Medical School. At Rice, her research interests focus on the issues that arise when humans physically interact with robotic systems. She is former chair of the IEEE Technical Committee on Haptics and a former associate editor for the IEEE Transactions on Haptics. Pehlivan, A.U., F. Sergi, and M.K. O’Malley (2013) Adaptive Control of a Serial-inParallel Robotic Rehabilitation Device, Proceedings of the IEEE International Conference on Rehabilitation Robotics T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 11 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Profiles in Caring continued from page 9 holistic view of nursing practice that includes leadership style, administrative practices, navigation of the healthcare system and proper placement of patients across the continuum of care. The program aligns well with her professional interests. “It’s about getting the right care to the right people at the right time,” she says. “That’s a major focus across the Memorial Hermann Health System, and at TIRR Memorial Hermann, we’re interested in sharing what we’ve learned with other rehabilitation providers. As educators, we have a unique opportunity to drive change that impacts both individual patients and whole populations.” In addition to providing clinical education to hospital and system staff members, Thomas makes quality improvement presentations at state and national conferences. She also works with nurses from four different schools who complete rotations at TIRR Memorial Hermann – students at TWU, Houston Baptist University, Houston Community College and San Jacinto Community College. “I like having the opportunity to give new nurses a broader view of our profession that extends to other disciplines,” she says. “I also find a lot of satisfaction in helping to improve quality across the entire continuum of care. We don’t stop measuring outcomes when patients leave the hospital. It’s important to help each patient meet his or her individual goals for return to function or adaptation to disability and improved quality of life.” u P PERSPECTIVES ON RESEARCH Hair Cortisol: A Potential Biomarker of Emotional Distress among Persons with Traumatic Brain Injuries By David B. Arciniegas, M.D. In our National Institute on Disability and Rehabilitation Research-supported study of acceptance and commitment therapy (ACT) for the treatment of emotional distress among persons with traumatic brain injury (TBI) in the subacute and chronic recovery periods, we are performing a pilot study of an innovative method of assessing a physiological correlate of emotional distress through sampling of cortisol levels attained from hair samples of the study participants. Chronic psychological stress produces similarly chronic over-activation of the body’s stress-response system. Cortisol is a component of that stress-response system, the levels of which are increased during periods of high stress. Although 12 TIRR MEMORIAL HERMANN short-term increases in cortisol can help the body manage illness or injury effectively, long-term increases in cortisol levels are associated with a broad range of adverse health effects that compromise physical and emotional wellbeing and function. In the context of TBI, longterm increases in serum cortisol levels may, quite literally, add insult to injury. Hair cortisol sampling enables evaluation of the average levels of serum cortisol produced over the month preceding sampling. Cortisol circulating in the bloodstream is incorporated into hair at the time it is produced by hair follicles. Once it is incorporated into the hair, it does not diffuse out of it as hair grows or as it is exposed to the elements or hair products (e.g., shampoo, conditioner). As a result, the amount of cortisol in the hair serves as a stable marker of the average levels of cortisol circulating in the blood at the time during which that hair is produced. For the vast majority of people who have hair on the scalp vertex – the very back of the top-most part of the head – that hair is produced at a rate of about 1 centimeter per month. Measuring the amount of cortisol in a 1 cm sample (50 to 100 strands of hair) allows us to estimate the average daily levels of cortisol circulating during the month over which that segment of hair was produced. When that 1 cm hair sample is taken from the segment closest to the scalp, hair cortisol levels provide an estimate of the average daily levels of circulating cortisol during the month preceding sampling. The sampling method is cosmetically benign, and is usually unnoticeable to even the most appearance-conscious individuals. To put a sample of 50 to 100 strands of hair in context, most people lose at least 50 to 100 hairs from their head every day. Accordingly, most people do not notice a loss of hair in this amount when the sampling for hair cortisol level determination is performed. Additionally, the sample is obtained by making a part in the hair (for those wearing their hair long enough to part) and by using thinning shears to obtain hairs at the base |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| of the part. The use of thinning shears leaves cosmetically unchanged the area under the parted hair from which the sample is taken. Using this cortisol sampling method, we will be evaluating the correlation between hair cortisol levels among persons with TBI and scores on the Brief Symptom Inventory 18 (BSI 18). The BSI 18 is a short, self-report assessment of depressive, anxious and physical symptoms that are common among persons experiencing emotional distress, including persons with TBI. The BSI 18 asks participants to report on the levels of symptoms they experienced over the last seven days. We will be asking the group of participants in the hair cortisol portion of our study also to report on their level of symptoms over the last month. If we observe a correlation between proximal 1 cm segment hair cortisol levels and BSI 18 scores, then we will have identified a biomarker of emotional distress among persons with TBI. This biomarker will help us understand the biological effects of emotional distress by providing us with a quantifiable estimate of the level of activity of the immune system associated with emotional health/ A ACCOLADES TIRR Memorial Hermann was featured as an ROI Case Study in the American Nurses Credentialing Center’s Pathway to Excellence™ e-Newsletter distributed on October 10, 2013. The hospital’s outcomes were cited as “continually exceeding expectations” with a below-average fall rate, a five-year track record of no cases of ventilator-associated pneumonia (VAP), fewer catheter-associated urinary tract infections (CAUTIs), fewer pressure ulcers and an increase in CRRN (certified rehabilitation registered nurse) certifications. “Our nurses are driving process change for the good of patients and staff, and gaining recognition for their David B. Arciniegas, M.D., is senior scientist and medical director for brain injury research at TIRR Memorial Hermann and executive director of the Beth K. and Stuart C. Yudofsky Division of Neuro- psychiatry and professor of psychiatry, neurology and physical medicine and rehabilitation at Baylor College of Medicine. He is co-investigator in a novel innovative preliminary investigation of the effectiveness of acceptance and commitment therapy (ACT) for reducing emotional distress, improving healthrelated quality of life and increasing participation in the community for persons with TBI. If the study is successful, it will provide a foundation for future multicenter comparative effectiveness trials in which ACT can be evaluated in comparison to traditional cognitive behavioral therapy and psychotropic medications. The principal investigator of the trial is Angelle Sander, Ph.D., director of the Brain Injury Research Center (BIRC) at TIRR Memorial Hermann. Additional co-investigators on this project are Mark Sherer, Ph.D., ABPP, FACRM, director of research and director of neuropsychology at TIRR Memorial Hermann, and BIRC researchers Kacey Maestas, Ph.D., and Allison Clark, Ph.D. Please contact Dr. Arciniegas at david. arciniegas@bcm.edu with questions or comments about the hair cortisol aspect of the ACT study. outstanding work,” says Mary Ann Euliarte, RN, CRRN, COO/CNO. Meilani Mapa, M.D., assistant professor and vice chair of the department of Physical Medicine and Rehabilitation at UTHealth Medical School, represented TIRR Memorial Hermann and UTHealth PM&R at The University of Texas System Meilani Mapa, M.D. Clinical Safety and Effectiveness Conference and Recognition Event held in September 2013 at the Grand Hyatt Hotel in San Antonio. The conference, entitled “Building the Bridge: Public Policy and Public Health Effect Health Care Reform,” brought together doctors, clinicians and students from across the UT System. Dr. Mapa presented her quality improvement project “Reducing Acquired Urinary Tract Infections on the Inpatient Rehabilitation Unit” with Viola Hysa, M.D., who will complete her residency at the Baylor College of Medicine/UTHealth Alliance for Physical Medicine and Rehabilitation in 2014. Staff of the Brain Injury Research Center won two of three awards presented for posters at the 90th annual meeting of the American Congress of Rehabilitation Medicine held in Orlando, Florida, in November 2013. “A preliminary model of social integration and emotional Accolades continues on page 14 distress. It also may provide a biomarker with which to evaluate the biological effects of psychotherapy, including ACT or medications, for depressive and anxious symptoms among persons with TBI. In other words, measuring hair cortisol levels may facilitate identification of the neurobiology of emotional distress and the effects of psychological and pharmacologic treatments on the body’s stress-response system. The NIDRR-supported study of ACT for emotional distress among persons with TBI is in its very early stages. When we begin enrolling participants, we also will begin the hair cortisol-sampling component of that study. We anticipate acquiring data sufficient for testing of the relationship between hair cortisol levels and BSI 18 scores in the next one to two years. Once analyzed, these data will be submitted for peer review and possible publication in a brain injury rehabilitation-oriented journal. u T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 13 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| delegate-at-large to the Texas Physical Therapy Association. Accolades continued from page 13 functioning for persons with TBI,” the second place winner, was authored by Monique Pappadis, CHES, CCRP Margaret A. Struchen,Ph.D. Monique Pappadis, CHES, CCRP, Margaret Struchen, Ph.D., Angelle Sander, Ph.D., and Diana Mazzei, LPC. Authors Lynne Davis, Ph.D., Angelle Sander, Ph.D., Jay Bogaards, CCRP, and Monique Pappadis, won third place for “MPAI-4 discrepancy ratings of abilities predict memory and executive functioning performance after traumatic brain injury.” The TIRR Memorial Hermann Pharmacy was one of only nine sites in the United States selected by the American Society of HealthSystem Pharmacists to participate in the 2014-15 Antimicrobial Angelle Sander, Ph.D. Stewardship Impact Program. Led by Carolyn Alessi, the project will involve an interdisciplinary team: Susan Loughlin, Pharm.D., BCPS, Terree Funesti, ADN, WCC, CRRN, Lindsay Toenges, Diana Mazzei, M.A., CIC, Lisa Wenzel, LPC M.D., Ben Portnoy, M.D., Audrey Wanger, Ph.D., and Lourdes Cuellar, RPh. Rhonda Abbott, PT, administrative director and director of therapy services and clinical programs, has been elected 14 TIRR MEMORIAL HERMANN Heather Taylor, Ph.D., and Glendaliz Bosques, M.D., are Rhonda Abbott, PT Heather Taylor,Ph.D. co-investigators of a new study under way at TIRR Memorial Hermann and UTHealth Medical School. Entitled Pediatric Multicenter Evalu ation of Notable SCI Outcome Instruments, the three-year study is funded by the Craig Neilsen Foundation. u I IN PRINT Park WH, Li S. Responses of finger flexors and extensors to TMS during isometric contraction. Muscle Nerve, Nov 2013;48(5):739-44. u O ON THE PODIUM Adair C, Phillips D. Seven Meaningful Days. Educational session presented at the Texas Occupational Therapy Association Annual Conference, Sugar Land, Texas, November 2013. Cooper Hay C, Scully T, Sieber R, Vanlandingham C. Catherine Cooper Hay, OTR Using the iPad in Occupational Therapy Brain Injury Rehabilitation. Educational session presented at the Mountain Central Conference of the Texas Occupational Therapy Association, Sugar Land, Texas, November 2013. Gutierrez A , Thayer B. Educational Classes for Spanish-speaking Patients with Spinal Cord Injuries. Educational session presented at the 39th Annual Ann Gutierrez,RN, Association of CRRN, CBIS Rehabilitation (ARN) National Education Conference, Charlotte, N.C., October 2013. Gutierrez A , Reimers A . Target Zero for Catheterassociated Becky Thayer, M.S.N., Urinar y Tract RN, CRRN Infections (CAUTIs). Educational session presented at the 39th Annual Association of Rehabilitation (ARN) National Education Conference, Charlotte, N.C., October 2013. Hartman L . Neuro-IFRAH Certification Course in the Treatment and Management of Adults with Hemoplegia from a Stroke or Brain Injury. A 14-day educational session presented at TIRR Memorial Hermann, Houston, October and November 2013. Jennings J. Advancing Rehabilitation of the Upper Julie Jennings, Extremity after PT, NCS SCI: Innovation and Stimulation. Presented at the Academy of Spinal Cord Injury Professionals (ASCIP) Educational Conference, Las Vegas, Nev., September 2013. Martin L, Shields C. Vestibular Assessment and Treatment in Individuals with Concussion. Course presented at the |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Texas Physical Therapy Association Annual Conference Student Conclave, Arlington, Texas, October 2013. Sander AM. A systematic approach to treating family caregivers of persons with traumatic brain injury. Invited lecture presented at the Contemporary Forums conference, Brain Injuries: A Multidisciplinary Approach to Rehabilitation, Washington, D.C., October 2013. Sander AM. Addressing sexual functioning in rehabilitation of persons with traumatic brain injury. Invited lecture presented at the Contemporary Forums conference, Brain Injuries: A Multidisciplinary Approach to Rehabilitation, Washington, D.C., October 2013. Taylor HB, Robinson-Whelen S, Hughes RB, Wenzel L , Nosek MA. Examining the MHI-5 as a Depression Screening Measure. Invited presentation at Lisa Wenzel, M.D. the American Congress of Rehabilitation Medicine 90th Annual Conference, Orlando, Fla., November 2013. Taylor HB, Robinson-Whelen S, Hughes RB, Wenzel L , Nosek MA. Depression and Depression Treatment of Women with Spinal Cord Injury: Are We Doing Enough? Invited presentation at the American Spinal Cord Injury Association 40th Anniversary Meeting, Chicago, Ill., May 2013. Thomas H. Development and Validation Process for the Spiritual Wellness Assessment. Educational session presented at the Academy of Spinal Cord Injury Professionals Annual Conference, Las Vegas, Nev., September 2013. Young K , Davis K , Euliarte MA . Management of Breastfeeding with Spinal Cord Injury: China’s Story. Educational session presented at the 39th Annual Association of Rehabilitation (ARN) National Education Conference, Charlotte, N.C., October 2013. u P POSTER PRESENTATIONS Davis LC, Sander AM, Bogaards JA , Pappadis MR. MPAI-4 discrepancy ratings of abilities predict memory and executive functioning performance after traumatic brain injury. Presented at the 90th Annual Meeting of the Lynne Davis,Ph.D. American Congress of Rehabilitation Medicine, Orlando, Fla., November 2013. De Joya A , Taylor K. The Effect of Circuit Training in a Modified Constraint Induced Movement Therapy Program. Presented at the 90th Annual Meeting of the American Congress of Rehabilitation Medicine, Orlando, Fla., November 2013. Giardina M. Altering Shank Kinematics in Midstance via AFO Design to Improve Gait Speed and Endurance in an Individual with TBI. Presented at the Texas Physical Therapy Association Annual Conference, Arlington, Texas, October 2013. Pappadis MR, Struchen MA , Sander AM, Mazzei D. A preliminary model of social integration and emotional functioning for persons with TBI. Presented at the 90th Annual Meeting of the American Congress of Rehabilitation Medicine, Orlando, Fla., November 2013. Martin L , Shields C. Vestibular Assessment and Treatment in Individuals with Concussions for the Student Conclave. Taylor K , De Joya A . The Effect of Circuit Training in a Modified Constraint Induced Movement Therapy Program. Presented at the 90th Annual Meeting of the American Congress of Rehabilitation Medicine, Orlando, Fla., November 2013. Thomas H. Development, Pilot, and Validation Process of a Spiritual Wellness Assessment. Poster presentation at the George Washington Institute of Spirituality and Health, Washington D.C., July 2013. u About TIRR Memorial Hermann TIRR Memorial Hermann is a 119-bed nonprofit rehabilitation hospital, a network of outpatient therapy clinics, a rehabilitation medical home and a network of inpatient rehabilitation units. Founded in 1959, the Texas Medical Center facility has been named one of America’s Best Hospitals by U.S.News & World Report for 24 consecutive years. Rehabilitation teams at the hospital provide services for individuals with strokes, brain injuries, spinal cord injuries, amputations and neurodegenerative diseases. TIRR Memorial Hermann is creating a comprehensive, integrated rehabilitation network beyond the Texas Medical Center, in outlying communities where people live and work. TIRR Memorial Hermann Outpatient Rehabilitation on the Campus of Memorial Hermann Memorial City, TIRR Memorial Hermann Outpatient Rehabilitation on the Campus of Memorial Hermann Northwest and TIRR Memorial Hermann-The Woodlands further extend services that have been offered at TIRR Memorial Hermann Outpatient Rehabilitation at the Kirby Glen Center since the southwest Houston facility opened in 2001. TIRR Memorial Hermann is one of 12 hospitals in the not-for-profit Memorial Hermann Health System. Memorial Hermann is known for world-class clinical expertise, patient-centered care, leadingedge technology and innovation. The system, with its exceptional medical staff and more than 20,000 employees, serves Southeast Texas and the Greater Houston community. T H E I N S T I T U T E F O R R E H A B I L I TAT I O N A N D R ES E A R C H 15 Memorial Hermann Health System Nonprofit Org. U.S. POSTAGE PAID Permit No. 3156 Houston, TX 7737 Southwest Freeway Houston, TX 77074 tirr.memorialhermann.org M MESSAGE FROM THE CEO When I was recruited to TIRR Memorial Hermann in 2006, one of my first tasks was to guide an independent rehabilitation hospital as it transitioned to its Carl E. Josehart, CEO new role as a member of the 12-hospital Memorial Hermann Health System. I felt the great sense of responsibility that comes with being entrusted with a national treasure. During more than 50 years of service, TIRR Memorial Hermann has played a leadership role in the history of Houston and the history of rehabilitation. To move forward as The Institute for Rehabilitation and Research and pave the way for future contributions to our discipline, we knew we needed to harness the synergy created by uniting all our research programs under one roof. The new TIRR Memorial Hermann Research Center rises three stories into the Houston sky about 100 steps from our hospital. From funding to finish, the dramatic transformation of an abandoned building took nearly three years to complete. By renovating a part of our history, we’re celebrating our past and honoring the contributions that came out of it. The third-story bridge connecting the research center and hospital represents more than access: it reinforces our triple mission of clinical care, education and research in a way that will sustain us well into the future. Bridges are built for crossing from one side to the other. While we were breathing new life into an old building, we were also positioning TIRR Memorial Hermann as the anchor for a rehabilitation network grounded in excellence and stretching across Houston. As our patients have taught us, reinventing ourselves is not easy, but it’s a necessary endeavor if we are to move ahead. To learn more about TIRR Memorial Hermann and our healthcare providers, visit our company page at LinkedIn.com TIRR is a registered trademark of TIRR Foundation. Carl E. Josehart Chief Executive Officer TIRR Memorial Hermann System Executive for Rehabilitation Services Memorial Hermann Health System 4406407