Association of Serum Antibodies to Heat-Shock Protein 65
With Coronary Calcification Levels
Suggestion of Pathogen-Triggered Autoimmunity in Early Atherosclerosis
Jianhui Zhu, MD, PhD; Richard J. Katz, MD; Arshed A. Quyyumi, MD; Daniel A. Canos, MS;
David Rott, MD; Gyorgy Csako, MD; Alexandra Zalles-Ganley, BS; Jibike Ogunmakinwa, BS;
Alan G. Wasserman, MD; Stephen E. Epstein, MD
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
Background—Previous studies demonstrated an association between antibodies to mycobacterial heat-shock protein 65
(mHSP65) and carotid artery thickening. We examined whether mHSP65 antibodies are associated with levels of
coronary calcification that appear to reflect preclinical coronary artery disease (CAD).
Methods and Results—Serum specimens from 201 healthy asymptomatic subjects (52% male; mean age, 56.6 years)
undergoing electron-beam computed tomographic imaging were used to measure levels of mHSP65 and human HSP60
antibodies and antibodies to several infectious pathogens. We found that 84% of the study subjects had anti-mHSP65
IgG antibodies. Mean titers of mHSP65 antibodies were higher (1:394 versus 1:267, P⫽0.012) in individuals with than
in those without elevated levels of coronary calcium (calcium score ⱖ150). Increasing titers of mHSP65 antibodies were
significantly associated, in a dose-response manner, with elevated levels of coronary calcification. Individuals with the
highest titers of mHSP65 antibodies (ⱖ1:800) had an adjusted odds ratio (OR) of 14.3 for having elevated coronary
calcium (P⫽0.004). Association of mHSP65 antibodies with elevated coronary calcification levels was independent of
CAD risk factors after multivariate adjustment (P⫽0.037). Interestingly, mHSP65 antibody titers were correlated with
Helicobacter pylori infection (P⫽0.004), which maintained significance after adjustment for CAD risk factors and
seropositivities to other pathogens (adjusted OR, 3.1; 95% CI, 1.4 to 6.6). No association was found between antibodies
to human HSP60 and levels of coronary calcification.
Conclusions—Antibodies to mHSP65 are associated with elevated levels of coronary calcification and correlated with H
pylori infection, suggesting that pathogen-triggered autoimmunity plays a role in early atherosclerosis. (Circulation.
2004;109:36-41.)
Key Words: proteins 䡲 infection 䡲 calcification
A
therogenesis is a complex process, with multiple mechanisms contributing to its initiation and progression.
Autoimmunity is one of the more recently identified candidate mechanisms, with heat shock protein (HSP) identified as
a possible autoantigenic determinant.1,2 HSPs constitute a
group of highly conserved intracellular proteins that are
produced by prokaryotic and eukaryotic cells in response to
perturbations of the cell’s environment, such as those induced
by high temperature, infection, or mechanical stress. HSPs
aid in mediating the correct folding of intracellular proteins,
in transporting such proteins across membranes, and in
protecting cellular proteins from denaturation by environmental insults.
HSPs are regarded as being intracellular proteins. However, when overexpressed in response to stress, they could
translocate to and reside on the cell surface, where these
cryptic antigens could be detected by the immune surveillance system, thereby triggering an immune response. Under
certain conditions, they could be released from cells.1,2 It has
been proposed that HSPs may, over time, have deleterious
effects as a consequence of some of them having the capacity
to serve as autoantigens and play roles in diseases. Previous
studies have reported that elevated levels of HSP antibodies
are detected in patients with atherosclerosis,1,2 and antibodies
against HSPs cause cytotoxic effects on heat-stressed human
endothelial cells through complement activation or antibodydependent cellular cytotoxicity.3 We recently demonstrated a
significant association between antibodies targeted to human
HSP60 and both the presence and severity of clinically
significant coronary artery disease (CAD).4
Received April 14, 2003; de novo received August 1, 2003; revision received September 22, 2003; accepted September 22, 2003.
From the Cardiovascular Research Institute, Washington Hospital Center (J.Z., D.A.C., D.R., A.Z.-G., J.O., S.E.E.), and George Washington University
(R.J.K., A.G.W.), Washington, DC; Emory University Hospital, Atlanta, Ga (A.A.Q.); and the Clinical Center, National Institutes of Health, Bethesda,
Md (G.C.).
Drs Zhu and Epstein have applied for a patent relating to the use of heat-shock proteins as a diagnostic and prognostic marker of coronary artery disease.
Correspondence to Dr Jianhui Zhu, Cardiovascular Research Institute, Washington Hospital Center, 108 Irving St, NW, GHRB Room 217, Washington,
DC 20010. E-mail jianhui.zhu@medstar.net
© 2004 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org
DOI: 10.1161/01.CIR.0000105513.37677.B3
36
Zhu et al
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
The triggers for the postulated autoimmune responses
involving HSPs and atherogenesis are primarily conjectural.
Infection, however, appears to be a leading candidate. Bacteria express HSPs that are homologous to human HSPs, and
viruses, although not expressing HSPs, incorporate host HSP
into their membranes as they leave the host cell in the course
of their infectious cycles. It has thus been postulated that
infection induces antibodies that are targeted to pathogenderived HSPs but that cross-react with human HSP. When
human HSPs are overexpressed and are present on the surface
of endothelial cells, immunopathological processes inducing
atherogenic changes in the vessel wall may occur. The results
of several studies have been compatible with this concept. For
example, an association has been demonstrated between
antibodies to mycobacterial HSP65 (mHSP65) and carotid
artery thickening.5–7
On the basis of this reasoning, we hypothesized that
infection triggers early coronary vascular changes in the host
that predispose to the development of CAD and that these
changes are caused, at least in part, by antibodies targeted to
pathogen HSP but cross-reacting with human HSP60 presented on cells of the vascular wall. In testing the validity of the
hypothesis, we identified a group of healthy asymptomatic
individuals who were undergoing screening for CAD by
electron-beam computed tomographic imaging (EBCT) of the
coronary arteries and examined whether an association exists
between coronary calcification levels and the presence of
antibodies to pathogen-derived HSPs (for which we used a
standard pathogen HSP, mHSP65) and to human HSP60.
Methods
Subjects
Under a George Washington University IRB–approved protocol, 201
healthy asymptomatic individuals entered the study. They were
scheduled for an EBCT study at George Washington University. At
the time of the EBCT scanning, participants were asked to consent
and to have blood drawn.
Clinical Examination and EBCT
All participants underwent a clinical examination and completed
questionnaires on current and past exposure to traditional CAD risk
factors. EBCT provided a quantitative measure of coronary calcification. For the scans, ECG leads were placed, and the patient was
positioned supine in the gantry. A preview scan was obtained for
positioning the heart. The coronary artery scan acquisition protocol
for the Imatron EBCT scanner consisted of 30 to 32 levels from the
aortic valve to the ventricular apex, with each level 3 mm thick. Each
level was triggered by the subject’s ECG in end diastole (80% of the
RR interval). Coronary calcification was measured by use of the
Base Value Region of Interest software, and regions of interest were
confirmed manually. Scores were reported using the Agaston scoring
system. Calcium score was the prospectively defined cutoff value for
defining a level of coronary calcification as low (0 –10), medium
(11–149), or high (ⱖ150).
Infectious Serology
Serum samples were frozen at ⫺80°C. Serum IgG antibodies were
performed with ELISA kits: cytomegalovirus, herpes simplex virus
type 1 and type 2 (Wampole), Helicobacter pylori (Meridian
Diagnostics), Chlamydia pneumoniae (Savyon Diagnostics), and
hepatitis A virus (ETI-AB-HAVK, DiaSorin Inc). Serology values
identified as positive were determined according to the manufacturer’s instructions.
Heat-Shock Protein and Preclinical Atherosclerosis
37
Serum Anti-HSP65 and Anti-HSP60 Antibodies
IgG antibodies against mHSP65 or human HSP60 were determined
by ELISA. In brief, 96-well microtiter plates were coated with 5
g/mL recombinant mHSP65 or human HSP60 (StressGen Biotechnologies Corp) in 100 L carb/bicarb buffer (pH 9.6) per well at 4°C
overnight. After washing and blocking with 3% BSA in PBS at room
temperature for 3 hours, plates were incubated with 100-L serum
samples diluted in serum diluent (Wampole) to 1 in 50 at room
temperature for 1 hour. The plates were incubated with horseradish
peroxidase– conjugated goat anti-human IgG diluted 1 in 10 000 with
PBS after a further wash, and 100 L chromogen/substrate solution
containing tetramethylbenzidine (Wampole) was then added to
wells. Absorbance at 450 nm was measured after 10 minutes after
addition of the stopping solution (Wampole). After correction for
background absorbance, a serum sample was considered positive for
antibodies against mHSP65 or human HSP60 if the optical density
exceeded a prospectively defined cutoff value. This cutoff value was
calculated from the negative and positive control absorbance values.
The positive sample was further diluted to 1:200, 1:400, and 1:800.
The OD value assigned to the antibody titer was that which was read
from the 1:50 dilution.
Serum CRP Levels
Serum C-reactive protein (CRP) was measured by fluorescence
polarization immunoassay technology (TDxFLEx analyzer, Abbott
Laboratory). With this assay, 95% of healthy individuals (n⫽202)
had a CRP level of ⱕ0.5 mg/dL, and 98% had levels ⱕ1.0 mg/dL,
in their sera. The between-run coefficient of variation of this assay
(n⫽31) was 4.3% and 2.2% at mean levels of 1.10 mg/dL and 2.94
mg/dL, respectively.
Statistical Analysis
Categorical data were analyzed by the 2 test or Fisher’s exact test.
All tests were 2-sided. The dichotomous variable indicating that the
high coronary calcification level (calcium score ⱖ150) was modeled
as a function of other factors was determined by use of multiple
logistic regression. The odds ratio (OR) with 95% confidence
interval (CI) was used as a measure of likelihood of an elevated
coronary calcification level being present in patients with a given
risk factor compared with those without that factor, or as a multiplicative factor for each unit increase in age or titers of antibodies to
mHSP65 and to human HSP60. The covariates considered were age,
male gender, smoking, diabetes, hypercholesterolemia (total cholesterol ⬎240 mg/dL), hypertension (arterial pressure ⬎140/
90 mm Hg), family history of CAD, CRP levels, and seropositive
status to infections as well as antibodies to mHSP65 and to human
HSP60. All covariates were examined as predictors of the elevated
coronary calcification levels in univariate analyses and as a group in
one multivariate model.
Results
Characteristics of Study Subjects
A total of 201 subjects were studied. Men constituted 52% of
the cohort. Their ages ranged from 27 to 79 years (mean,
56.6; median, 56.0 years). Table 1 presents the baseline
characteristics of the study subjects in each of the calcium
score subgroups. There were 39 individuals (20%) with
EBCT evidence of high levels of coronary calcium (calcium
score ⱖ150). As shown in Table 2, the elevated coronary
calcium score was independently associated with age and
male gender by both univariate and multivariate analysis. The
positive association between high coronary calcification and
diabetes and hypercholesterolemia were found after adjustment for traditional risk factors.
38
Circulation
January 6/13, 2004
TABLE 1. Baseline Characteristics of Subjects in Each
Calcium Score Subgroup
Calcium Score*
Risk Factor
Low
(n⫽107)
Medium
(n⫽54)
High
(n⫽39)
Age, y (mean⫾SD)
54.6⫾9.6
57.1⫾9.5
61.3⫾8.0†
Male gender, %
40.2
61.1†
69.2†
Smoking, %
34.6
42.6
33.3
Diabetes, %
3.7
3.7
10.3
1Cholesterol, %
55.1
66.7
74.4
Hypertension, %
28.0
31.5
38.5
Family history of CAD, %
53.3
61.1
61.5
1CRP (⬎0.5 mg/dL)
13.2
11.3
5.3
*Calcium score: low (0 –10), medium (11–149), and high (ⱖ150).
†P⬍0.01 vs the low calcium score group.
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
Anti-mHSP65 and Anti-Human HSP60 Antibodies
Versus Coronary Calcification
In our study cohort, 166 of 198 (84%) had anti-mHSP65 IgG
antibodies with titers between 1 in 50 and 1 in ⱖ800 (mean,
1:292), and 144 of 198 (73%) had anti-human HSP60
antibodies with titers between 1 in 50 and 1 in ⱖ800 (mean,
1:229). There was a correction between mHSP65 and human
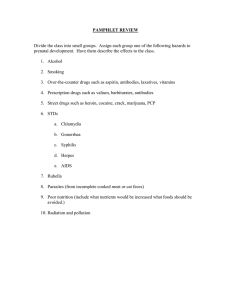
HSP60 antibodies (r⫽0.193, P⫽0.006). Figure 1 presents the
prevalence of anti-mHSP65 and anti-human HSP60 seropositivity in each of the calcium score subgroups. There was an
increased prevalence of anti-mHSP65 antibodies, but not
anti-HSP60, in the high calcium score group compared with
the low calcium score group (P⫽0.039).
Further analysis showed that in the anti-mHSP65 seropositive group, 22% of individuals had high coronary calcium
scores, whereas in the seronegative group, 6% had elevated
scores (P⫽0.036). Mean titers of mHSP65 antibodies were
higher in individuals with than in those without high coronary
calcium (1:394 versus 1:267, P⫽0.012). Association of
mHSP65 antibodies with high coronary calcification was
independent of established CAD risk factors, including age,
male gender, smoking, diabetes, hypercholesterolemia, hypertension, family history of CAD, and CRP levels (adjusted
Figure 1. Prevalence of anti-mHSP65 and anti-human HSP60
seropositivity in each calcium score subgroup. Calcium score:
low (0 –10), medium (11-149), and high (ⱖ150). Ab⫹ indicates
antibody seropositivity. *P⫽0.039 vs low calcium score group.
OR, 5.53; 95% CI, 1.17 to 26.09). Increasing titers of
mHSP65 antibodies were also significantly associated, in a
dose-response manner, with elevated levels of coronary
calcification after multivariate adjustment (Figure 2). However, no association between either the presence of human
HSP60 antibodies or increasing human HSP60 antibody titers
and elevated levels of coronary calcification was observed
(all P⬎0.05, data not shown).
Anti-mHSP65 Antibodies and CAD Risk Factors
Table 3 presents associations between anti-mHSP65 antibodies and CAD risk factors. We found that neither the presence
of anti-mHSP65 antibodies nor increasing anti-mHSP65 antibody titers were associated with traditional CAD risk factors
(all P⬎0.05).
Anti-mHSP65 Antibodies and Infection
Associations of mHSP65 antibodies with infections, including seropositivity to cytomegalovirus, C pneumoniae, H
pylori, hepatitis A virus, and herpes simplex virus type 1 and
type 2, were analyzed. Interestingly, serum antibody titers to
mHSP65 correlated with H pylori infection. The prevalence
TABLE 2. Association of Presence of High Coronary
Calcification With Traditional CAD Risk Factors
Multivariate†
Risk Factor
Univariate P
OR (95% CI)
P
Age, 10 y*
0.001
4.2 (2.3–7.7)
⬍0.001
Male gender
0.013
8.6 (2.9–25.7)
⬍0.001
Smoking
0.649
0.6 (0.3–1.6)
0.322
Diabetes
0.094
7.5 (1.5–37.4)
0.013
1Cholesterol
0.077
2.5 (1.0–6.4)
0.047
Hypertension
0.264
0.9 (0.4–2.2)
0.852
Family history of CAD
0.526
1.7 (0.7–3.9)
0.204
1CRP (⬎0.5 mg/dL)
0.200
0.2 (0.04–1.1)
0.067
*In 10-year increments of age.
†Adjusted covariates: age, male gender, smoking, diabetes, hypercholesterolemia, hypertension, family history of CAD, and elevated CRP levels.
Figure 2. Adjusted OR for high coronary calcification in various
mHSP60 antibody titer groups. When adjusted for traditional
CAD risk factors, OR for high coronary calcification increased
with increasing titers of anti-mHSP65.
Zhu et al
Heat-Shock Protein and Preclinical Atherosclerosis
TABLE 3. Association of Presence and Absence of mHSP65
Antibodies With Traditional CAD Risk Factors
Anti-mHSP65 IgG
Risk Factor*
Age, y
Male gender
Seronegative
Seropositive
P†
56.9⫾9.7
56.5⫾9.6
0.824
46.9
52.4
0.566
Smoking
40.6
36.4
0.648
Diabetes
6.3
4.8
0.666
1Cholesterol
50.0
Hypertension
21.9
64.2
32.7
0.129
0.224
Family history of CAD
53.1
57.6
0.642
1CRP (⬎0.5 mg/dL)
9.4
11.6
1.000
*Data are mean⫾SD or percentage of patients.
†Univariate analysis.
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
of seropositivity to H pylori infection was 9.2% in the
subgroup with mHSP65 antibody titers of 1:50 to 1:200,
11.1% in the subgroup with antibody titers of 1:400, and
26.3% in the subgroup with antibody titers of 1:800 or more,
compared with 6.3% in individuals without mHSP65 antibodies (P for trend⫽0.004). A significant association between H
pylori IgG seropositivity and mHSP65 antibody titers remained after adjustment for CAD risk factors (Figure 3). No
correlation between either the presence of mHSP65 antibodies or the increase of antibody titers and other infectious
agents was found (all P⬎0.05, data not shown).
H pylori Infection and Coronary
Calcification Level
As shown in Table 4, although H pylori IgG antibodies were
not significantly associated with elevated coronary calcification levels on univariate analysis, the positive association
between H pylori infection and coronary calcification was
found on multivariate analysis after adjustment for CAD risk
factors and seropositivities to other infectious pathogens
(adjusted OR, 3.03; 95% CI, 1.0 to 9.17).
Figure 3. Adjusted OR for H pylori seropositivity in various
mHSP60 antibody titer groups. When adjusted for traditional
CAD risk factors, OR for H pylori seropositivity increased with
increasing titers of anti-mHSP65.
39
TABLE 4. Association of Coronary Calcification Scores of
<150 or >150 With IgG Seropositivity to 6
Infectious Pathogens
Coronary Calcification
Score
Antibodies, %
⬍150
ⱖ150
P
Adjusted* P
Cytomegalovirus
49.1
56.4
0.410
0.968
Chlamydia pneumoniae
76.6
67.6
0.255
0.494
Helicobacter pylori
10.7
20.5
0.110
0.050
Hepatitis A virus
27.2
46.2
0.026
0.333
Herpes simplex virus type 1
56.0
64.1
0.357
0.713
Herpes simplex virus type 2
32.7
43.6
0.201
0.254
*Adjusted covariates: age, male gender, smoking, diabetes, hypercholesterolemia, hypertension, family history of CAD, elevated CRP levels, and seropositivities to other infectious pathogens as described in Table 4.
Discussion
Several lines of evidence suggest that autoimmune mechanisms play a role in atherogenesis, and the important work of
Xu et al1,5,6 and Mayr et al7 suggests that HSP may be one of
the immune targets in this pathophysiological process. Evidence also suggests that infection may contribute to the
triggering of these autoimmune responses through antibodies
that, although developing in response to infection and targeted to pathogen-derived HSPs, cross-react with highly
homologous self-HSPs. Evidence compatible with this includes studies demonstrating that immunization with recombinant mHSP65 induces atherosclerotic lesions in normocholesterolemic rabbits,8 elevated levels of mHSP65 antibodies
are significantly associated with carotid atherosclerosis, and
mHSP65 antibodies derived from human serum cross-react
with human HSP60.5–7 Additional evidence for the biological
relevance of pathogen-stimulated antibodies to atherosclerosis derives from the demonstration that antibodies to chlamydial HSP60 isolated from human serum are cytotoxic to
heat-stressed human endothelial cells7 and the recent demonstration by Perschinka et al9 that antibodies to microbial
HSP60/65 recognize specific epitopes on human HSP60 that
are present in the arterial wall of healthy young individuals.
Our hypothesis is that infection triggers early coronary
vascular changes in the host that predispose to the development of CAD and that these changes are caused, at least in
part, by antibodies targeted to pathogen HSP but crossreacting with human HSP60 presented on cells of the vascular
wall. To identify a cohort of individuals with early coronary
atherosclerosis, we studied clinically healthy individuals
undergoing a screening study for preclinical CAD by using
EBCT for the detection of coronary artery calcification.
Previous studies have suggested that coronary calcification
detected by EBCT is associated with traditional CAD risk
factors and predicts preclinical CAD.10 –16 Compelling evidence appears in the literature that coronary calcification,
detected by EBCT, can appear before there is significant
coronary luminal narrowing and therefore before clinical
evidence of CAD. This fact suggests that coronary calcification is not a “severe endpoint of atherogenesis” but rather
begins developing, at least in some people, much earlier than
40
Circulation
January 6/13, 2004
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
previously suspected. Although the pathogenesis of this early,
preclinical calcification is not understood, infection has been
suggested to have a role in the development of calcification.17
In the present study, we found that anti-mHSP65 antibodies were significantly increased in the individuals with high
levels of coronary calcium (calcium score ⱖ150). Association of mHSP65 antibodies with elevated coronary calcification levels was independent of established CAD risk factors,
and individuals with the highest titers of mHSP65 antibodies
(ⱖ1:800) had an adjusted OR of 14.3 for having elevated
coronary calcium (P⫽0.004). However, there was no association of anti-human HSP60 antibodies with elevated levels of
coronary calcium. The lack of such an association for
anti-human HSP60 antibodies in our asymptomatic cohort
might be explained by the fact that autoreactivity to selfHSP60 might develop gradually during disease progression.
This would be in line with a recent report by Perschinka et al,9
who identified several human HSP60 epitopes presented in
the arterial wall of young healthy individuals and demonstrated the recognition of an increasing epitope number on
human HSP60 by bacterial HSP antibodies during the progression of atherosclerosis.
Interestingly, we also found that serum antibody titers to
mHSP65 were significantly correlated with H pylori infection, which remained after adjustment for CAD risk factors
and seropositivities to other infectious pathogens. H pylori
produces a 58-kDa HSP that has been shown to stimulate a
strong immune response in patients with gastritis and those
with gastric cancer.18,19 Circulating antibodies to the HSP60
family in patients with H pylori infection have been reported.20 Recently, a positive association between H pylori
infection and elevated levels of mHSP65 antibodies in patients with carotid thickness has been demonstrated by Mayr
et al.21 We demonstrated, in addition to the correlation
between mHSP65 antibodies and H pylori infection, a positive association between antibodies to H pylori infection and
coronary calcification. Thus, our findings and others suggest
that H pylori HSP may contribute to atherogenesis by
inducing anti–H pylori HSP antibodies that, because of the
homology between H pylori HSP with the human HSP,
cross-react with host HSP and induce immunopathology by
molecular mimicry.
One of the limitations of the present study was the lack of
measurement of IgA antibodies for C pneumoniae infection.
Several recent studies have reported that the presence of IgA
is a better marker than IgG antibodies for chronic C pneumoniae infection, because IgG antibodies to C pneumoniae
often reflect previous exposure rather than ongoing chronic
infection. Mayr et al22 demonstrated that IgA antibodies to C
pneumoniae were associated with carotid and femoral atherosclerosis and were correlated with antibodies to mycobacterial HSP65. Similarly, Huittinen et al23 found that high levels
of C pneumoniae IgA but not IgG antibodies were associated
with the risk of coronary events and were also associated with
human HSP60. In addition, although we found a positive
association between antibodies to H pylori infection and
coronary calcification, there are several important considerations for associations of H pylori infection with atherosclerosis. First, certain factors, such as age and low socioeco-
nomic status,24 are related to both H pylori infection and the
presence of cardiovascular disease. An association of H
pylori infection with cardiovascular disease could be influenced by these confounding factors. Second, H pylori strains
bearing the cytotoxin-associated gene A seem to be more
decisive for their pathogenic contribution in atherosclerosis,
although the mechanisms are unknown.21,25 Moreover, smoking is a stress factor for endothelial cells. Evidence has
indicated that both active and passive cigarette smoking is
associated with endothelial dysfunction, and endothelial abnormalities may predispose to the atherogenic and thrombotic
problems associated with cigarette smoking.26 However, no
association of smoking with the levels of coronary calcification and calcium score was found in the present study,
suggesting that the mechanisms leading to endothelial dysfunction and to coronary calcification differ.
In conclusion, this study demonstrated that mHSP65 antibodies are associated with elevated levels of coronary calcification in clinically healthy individuals and correlated with
H pylori infection. This finding is especially interesting when
it is considered that antibodies to human HSP60 were not
associated with calcifications in this asymptomatic cohort,
whereas they are associated with CAD in a symptomatic
patient cohort.4 These results suggest that pathogen-triggered
autoimmunity deriving from the generation of anti-mHSP65
antibodies cross-reacting to host HSP60 plays a role in early
atherosclerosis and that autoreactivity to self-HSP 60 might
develop gradually during disease progression. Although this
study examined associations between coronary calcification,
mHSP60 antibodies, and H pylori infection, the question of
whether anti-HSP immunity has a role in the calcification
process, a possible mechanism for elevation of coronary
calcification, would be a very worthy subject of future
investigations.
References
1. Xu Q. Role of heat shock proteins in atherosclerosis. Arterioscler Thromb
Vasc Biol. 2002;22:1547–1559.
2. Pockley AG. Heat shock proteins, inflammation, and cardiovascular
disease. Circulation. 2002;105:1012–1017.
3. Schett G, Xu Q, Amberger A, et al. Autoantibodies against heat shock
protein 60 mediate endothelial cytotoxicity. J Clin Invest. 1995;96:
2569 –2577.
4. Zhu J, Quyyumi AA, Rott D, et al. Antibodies to human heat-shock
protein 60 are associated with the presence and severity of coronary artery
disease: evidence for an autoimmune component of atherosclerosis. Circulation. 2000;103:1071–1075.
5. Xu Q, Willeit J, Marosi M, et al. Association of serum antibodies to
heat-shock protein 65 with carotid atherosclerosis. Lancet. 1993;341:
255–259.
6. Xu Q, Kiechl S, Mayr M, et al. Association of serum antibodies to
heat-shock protein 65 with carotid atherosclerosis: clinical significance
determined in a follow-up study. Circulation. 1999;100:1169 –1174.
7. Mayr M, Metzler B, Kiechl S, et al. Endothelial cytotoxicity mediated by
serum antibodies to heat shock proteins of Escherichia coli and
Chlamydia pneumoniae: immune reactions to heat shock proteins as a
possible link between infection and atherosclerosis. Circulation. 1999;
99:1560 –1566.
8. Xu Q, Kleindienst R, Schett G, et al. Regression of arteriosclerotic lesions
induced by immunization with heat shock protein 65– containing material
in normocholesterolemic, but not hypercholesterolemic, rabbits. Atherosclerosis. 1996;123:145–155.
9. Perschinka H, Mayr M, Millonig G, et al. Cross-reactive B-cell epitopes
of microbial and human heat shock protein 60/65 in atherosclerosis.
Arterioscler Thromb Vasc Biol. 2003;23:1060 –1065.
Zhu et al
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
10. Guerci AD, Spadaro LA, Goodman KJ, et al. Comparison of electron
beam computed tomography scanning and conventional risk factor
assessment for the prediction of angiographic coronary artery disease.
J Am Coll Cardiol. 1998;32:673– 679.
11. Schmermund A, Denktas AE, Rumberger JA, et al. Independent and
incremental value of coronary artery calcium for predicting the extent of
angiographic coronary artery disease: comparison with cardiac risk
factors and radionuclide perfusion imaging. J Am Coll Cardiol. 1999;34:
777–786.
12. Arad Y, Spadaro LA, Goodman K, et al. Prediction of coronary events
with electron beam computed tomography. J Am Coll Cardiol. 2000;36:
1253–1260.
13. Newman AB, Naydeck BL, Sutton-Tyrrell K, et al. Coronary artery
calcification in older adults to age 99: prevalence and risk factors. Circulation. 2001;104:2679 –2684.
14. Haberl R, Becker A, Leber A, et al. Correlation of coronary calcification
and angiographically documented stenoses in patients with suspected
coronary artery disease: results of 1,764 patients. J Am Coll Cardiol.
2001;37:451– 457.
15. Mielke CH Jr, Shields JP, Broemeling LD. Risk factors and coronary
artery disease for asymptomatic women using electron beam computed
tomography. J Cardiovasc Risk. 2001;8:81– 86.
16. Park R, Detrano R, Xiang M, et al. Combined used of computed
tomography coronary calcium scores and C-reactive protein levels in
predicting cardiovascular events in nondiabetic individuals. Circulation.
2002;106:2073–2077.
17. Kajander EO, Ciftcioglu N. Nanobacteria: an alternative mechanism for
pathogenic intra- and extracellular calcification and stone formation. Proc
Natl Acad Sci U S A. 1998;95:8274 – 8279.
Heat-Shock Protein and Preclinical Atherosclerosis
41
18. Dunn BE, Roop RM, Sung CC, et al. Identification and purification of a
cpn60 heat shock protein homolog from Helicobacter pylori. Infect
Immun. 1992;60:1946 –1951.
19. Macchia G, Massone A, Burroni D, et al. The Hsp60 protein of Helicobacter pylori: structure and immune response in patients with gastroduodenal disease. Mol Microbiol. 1993;9:645– 652.
20. Barton SGRG, Winrow VR, Rampton DS, et al. Circulating antibodies to
the 60-kD heat shock protein (hsp) family in patients with Helicobacter
pylori infection. Clin Exp Immunol. 1998;112:490 – 494.
21. Mayr M, Kiechl S, Mendall MA, et al. Increased risk of atherosclerosis is
confined to CagA-positive Helicobacter pylori strains: prospective results
from the Bruneck study. Stroke. 2003;34:610 – 615.
22. Mayr M, Kiechl S, Willeit J, et al. Infection, immunity, and atherosclerosis: associations of antibodies to Chlamydia pneumoniae, Helicobacter
pylori, and cytomegalovirus with immune reactions to heat-shock protein
60 and carotid or femoral atherosclerosis. Circulation. 2000;102:
833– 839.
23. Huittinen T, Leinonen M, Tenkanen L, et al. Autoimmunity to human
heat shock protein 60, Chlamydia pneumoniae infection, and inflammation in predicting coronary risk. Arterioscler Thromb Vasc Biol. 2002;
22:431– 437.
24. Mendall MA, Goggin PM, Molineaux N, et al. Childhood living conditions and Helicobacter pylori seropositivity in adult life. Lancet. 1992;
339:896 – 897.
25. Pasceri V, Cammarota G, Patti G, et al. Association of virulent Helicobacter pylori strains with ischemic heart disease. Circulation. 1998;97:
1675–1679.
26. Puranik R, Celermajer DS. Smoking and endothelial function. Prog
Cardiovasc Dis. 2003;45:443– 458.
Association of Serum Antibodies to Heat-Shock Protein 65 With Coronary Calcification
Levels: Suggestion of Pathogen-Triggered Autoimmunity in Early Atherosclerosis
Jianhui Zhu, Richard J. Katz, Arshed A. Quyyumi, Daniel A. Canos, David Rott, Gyorgy Csako,
Alexandra Zalles-Ganley, Jibike Ogunmakinwa, Alan G. Wasserman and Stephen E. Epstein
Downloaded from http://circ.ahajournals.org/ by guest on October 2, 2016
Circulation. 2004;109:36-41; originally published online December 8, 2003;
doi: 10.1161/01.CIR.0000105513.37677.B3
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2003 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circ.ahajournals.org/content/109/1/36
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located,
click Request Permissions in the middle column of the Web page under Services. Further information about
this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/