Apraxia of Speech Paper
advertisement

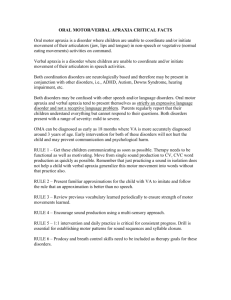
Treating Apraxia of Speech as a Result of Postencephalitic Parkinsonism Using Discourse Meghan C. Savage, Ph.D., Amanda L. Stead, Ph.D., and Paul R. Hoffman, Ph.D. Louisiana State University, Department of Communication Sciences and Disorders, Baton Rouge, Louisiana Keywords: apraxia, apraxia of speech, Postencephalitic parkinsonism, apraxia therapy, phoneme production Background: The purpose of this single-subject study was to investigate if phonologic placement treatment seated in spontaneous discourse would improve phonetic accuracy and increase intelligibility in an individual with postencephalitic parkinsonism resulting in apraxia of speech. Methods: The participant was a 60-year-old male with postencephalitic parkinsonism, oral and speech apraxia, and dysarthria. A single-subject ABAB design using pre- and posttesting and repeated measurement of phonemes during baseline and treatment was used. Phonological and visual supports were embedded within conversational discourse related to current events. Data were analyzed using visual inspection and effect sizes. Results: Results showed a treatment effect for all targeted phonemes as well as posttest measures of overall intelligibility. Assessment of Intelligibility of Dysarthric Speech scores rose from 0% to 24% intelligible at the single word level. Large effect sizes were found for all target phonemes, /b/ (d = 2.89), /m/ (d = 4.76), /r/ (d = 1.18) and /n/ (d = 1.94). Conclusions: A phonologically based treatment embedded in discourse was effective in facilitating basic verbal communication in a previously nonverbal individual. INTRODUCTION Apraxia of speech (AOS) is a neurogenic speech disorder caused by unilateral damage to the left cerebral hemisphere, which results in impaired positioning and movement of articulators during volitional production of speech. It can occur without significant weakness or neuromuscular slowness and in the absence of disturbances of conscious thought or language (Duffy, 2005). Clinical manifestations of AOS include problems of speech initiation; articulatory groping; reduced rate of speech; perseverations; slow transitions between sounds, syllables, and words; and disordered prosody (Wambaugh, Duffy, McNeil, Robin, & Rogers, 2006a). The majority of AOS treatments have been impairment oriented. Impairment-based approaches seek to remediate the underlying linguistic impairment using models of normal language and cognitive processing to structure units and levels of language organization for practice (Martin, Thompson, & Worrall, 2008). The basic tenet of this approach is that the primary access to language units is damaged. Therapy uses static noninteractive tasks that target the linguistic forms of language (Sarno, 2004). Speech tasks are presented in clinician-directed stimulus–response–feedback activities targeting an increased ability to access various sized language units. However, there is a need for more functional approaches to AOS Journal of Medical Speech-Language Pathology Volume 20, Number 2, pp. 35–42 Copyright © 2012 Delmar Cengage Learning 26537_ch04_ptg01_035-043.indd 35 8/2/12 2:01:57 PM 36 JOURNAL OF MEDICAL SPEECH-LANGUAGE PATHOLOGY, VOL. 20, NO. 2 treatments. Functional approaches, also termed social, participation, or psychosocial, address the consequences the disorder has on the person’s life. Intervention targets the use of speech and language to accomplish social needs in authentic, relevant, and natural contexts such as conversations (Simmons-Mackie, 2008b). The interventionist acts as a collaborator seeking to facilitate the person’s participation in the social context. Current AOS treatments, including articulatory kinematic, rate or rhythm, intersystemic facilitation or reorganization, and alternative or augmentative communication (Wambaugh, Duffy, McNeil, Robin, & Rogers, 2006b) are primarily impairment based and rooted in principles of motor learning. Motor learning typically involves intensive practice in repetition of movement patterns that are organized in hierarchies from simple to more complex (Austermann Hula, 2007; Maas et al., 2008; McNeil, Doyle, & Wambaugh, 2000). Articulatory-kinematic approaches currently demonstrate the highest levels of evidence ( Wambaugh, 2010). Articulatory-kinematic approaches involve practice in production of: individual phonemes and syllables (Knock, Ballard, Robin, & Schmidt, 2000; Raymer, Haley, & Kendall, 2002), single words (Knock, et al., 2000; LaPointe, 1984; Wertz, 1998), nonwords (Katz, Bharadwaj, & Carstens, 1999; Maas, Barlow, Robin, & Shapiro, 2002), phrases, and sentences. The clinician provides visual and auditory stimulation before each patient response. Articulation placement cues have been presented in drawings (Raymer et al., 2002), verbal instructions (Wambaugh, Kalinyak-Fliszar, West, & Doyle, 1998; Wambaugh, Martinez, McNeil, & Rogers, 1999; Wambaugh, West, & Doyle, 1998), video-taped models (Aten, 1986), Prompts for Restructuring Oral and Muscular Phonetic Targets (PROMPT) (Bose, Square, Schlosser, & van Lieshout. 2001; Square, Martin & Bose, 2001), and visual modeling (Wambaugh et al., 1998; Wambaugh et al., 1999; Wambaugh, West, & Doyle, 1998). Models of syllables and words have been presented in contrastive consonant vowel (CV) pairs (Wertz, LaPointe, & Rosenbek, 1984), blocked presentation of repeated syllables or words, or randomly. Other treatments such as Sound Production T r e a t m e n t ( S P T ) ( Wa m b a u g h , 2 0 1 0 ) a n d Phonomotor Treatment (Kendall, Rodriguez, Rosenbek, Conway, & Gonzalez Rothi, 2006) have been shown to be effective. In SPT, eight to 10 vowel or consonant sounds are selected based on individual performance. Each sound is targeted one at time. Stimuli increase in complexity from monosyllabic and multisyllabic words to phrases and sentences. Treatment for each sound is continued until the criterion is met. Sound production is facilitated using modeling, repetition, minimal pair contrast, integral stimulation, articulatory placement cueing, and verbal feedback in a response contingent hierarchy (Wambaugh, 2010). Data indicate that SPT improves articulation accuracy in trained and untrained words (Wambaugh et al., 1998; Wambaugh et al., 1999; Wambaugh, 2004; Wambaugh, 2006a, 2006b). Some generalization has been found for sounds similar in place and manner to the targeted sounds. For targets that reached a high level of accuracy during treatment, maintenance effects were found 1 to 2 months after treatment. Kendall et al. (2006) conducted a single-subject design to examine a phonomotor treatment for an individual with apraxia and aphasia. Pictures of mouths depicting articulatory placement were used to cue individual sound production. The study also used auditory discrimination, verbal production, mental practice, and tactile and kinesthetic modalities to target sound production. After 104 hours of therapy, the individual was able to produce individual sounds, but targets did not generalize to multisyllabic words and discourse. Although targets did not generalize, discourse production became less effortful, and the patient reported increased ease of communication and community integration (Kendall et al., 2006). Functional interventions are based in the holistic nature of learning. Life experiences are considered to be interactive contexts for learning, motivation, and participation. Learning is best when learners take responsibility for defining what they want to learn, know why they have to learn something before they undertake it, and are internally motivated to learn things that will help them cope effectively with real-life situations (Kimbarow, 2007). The present study investigates an intervention incorporating the use of visual cues to speech sound production and modeling to aid in accessing phonological units, a common strategy of impairment-based interventions, within a conversational discourse structure, a common practice of functional approaches. It is a test of the hypothesis that speech production practice in meaningful contexts is a potentially efficacious strategy that should be compared with the traditional hierarchical strategy. Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 36 8/2/12 2:01:57 PM TREATING APRAXIA OF SPEECH USING DISCOURSE METHODS Participant 37 and BNT from audio and video recordings. The Apraxia Battery for Adults-Second Edition (ABA-2; Dabul, 2000), which measures the presence and severity of apraxia, was used to assess the presence of oral, speech, and limb apraxia. The presence of oral apraxia was characterized as moderate. No limb apraxia was found. RH was rated severe on diadochokinetic rate, utterance time, increasing word length, and repeated trials, leading to a rating of severe for speech apraxia. The participant, RH, was a 60-year-old African American man who presented with postencephalitic parkinsonism, oral apraxia, apraxia of speech, dysphagia, and hypokinetic dysarthria. Premorbidly, RH had been a resident physician at a local charity hospital. He contracted encephalitis in 1972 while administering vaccinations. Initial magnetic resonance imaging results showed lesions in the substantia nigra region, consistent with the diagnosis of parkinsonism. He did not develop any cognitive impairments or language disorders as a result of the encephalitis. Immediately after contracting encephalitis, RH maintained the ability to use speech, but as the disease ran its course, he lost the ability to volitionally control his speech mechanism and has been primarily mute for 20 years. RH has been receiving therapy for several years to address concerns with dysphagia. At the time of the intervention, RH’s primary mode of communication was through the use of an Alternative Augmentative Communication (AAC) device, a DynaWrite. Because he did not have any cognitive impairment, his typed output consists of complete intelligible sentences. He participates in higher level intelligent conversations by typing his responses. His vocal output consisted of a high-pitched /e/ vowel produced when excited. When asked to imitate a single word, RH exhibited groping behaviors, inconsistent productions, and delayed initiation of phonation for 5 seconds or longer. At the time of the study, he was taking the following medications: Drovan, Nexium, Flomax, Levoxyl, Sinemet, Baclofen, and Zetia. Phonemic targets were based on a variety of factors including errors recorded on the BNT, a phonemic inventory, frequency of occurrence in the English language, order of acquisition, and necessity. In addition, literature on motor learning theory and the underlying pathophysiology was taken into account, resulting in six target sounds, including /r, b, t, m, n, d/. These target sounds were probed in single-word naming of picture cards for three sessions before the initiation of treatment. Five photographic noun picture cards for each phoneme were randomly presented to RH. He was asked to name each picture and was given adequate time to respond. If he self-corrected or produced numerous productions, the last correct response was scored. A response was considered accurate if he correctly produced the initial phoneme of the target picture. No prompts were given at any time. Based on performance on baseline probes, /t/ and /d/ were omitted from the training because of zero baseline performance. Upon completion of baseline probing, treatment was initiated. All sessions were conducted at the patient’s place of residence. Assessments Experimental Design RH’s speech production was measured by administration of The Assessment of Intelligibility of Dysarthric Speech (AIDS; Yorkston, Beukelman, & Traynor, 1984). Because RH had such limited output, only the Single Word Intelligibility subtest of the AIDS was administered. Single-word intelligibility was 12% when judged using multiple choices and 0% when scored by transcription. The Boston Naming Test (BNT) (Goodglass & Kaplan, 2001), a 60-item picture-naming test, was administered to assess his phonetic inventory of initial sounds. RH was 27% accurate on initial phonemes on the BNT. An unfamiliar judge blind to the time (pretest or posttest) of the speech samples scored the AIDS The study was an ABAB design. The first phase (A1) consisted of the three sessions to collect baseline data on probe items. In the treatment phase B1, seven sessions were conducted until RH reached 80% accuracy on target phonemes. Following in phase A2, the treatment was withheld for three sessions, and again three baseline probes were taken. In phase B2, three additional treatment sessions were provided for a total of 10 treatments. Before the initiation of treatment, the participant expressed to the researchers that he enjoyed discussing current events. Therefore, to ensure the treatment was personally relevant and highly motivating for the participant, target phonemes were Procedure Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 37 8/2/12 2:01:57 PM 38 JOURNAL OF MEDICAL SPEECH-LANGUAGE PATHOLOGY, VOL. 20, NO. 2 addressed in conversational discourse discussing current events. RH participated in the conversational discourse by typing his utterances using the DynaWrite. When he typed a response that contained a target phoneme, phonological support was provided to produce the sound. Phonological support for the target phonemes included the use of Phonic Faces (letters superimposed on drawings of faces to cue an aspect of phoneme production) (Norris, 2001), photographs of mouths depicting articulatory placement taken of the investigators, tactile cues specific to the phoneme being targeted, and auditory input of the phoneme (see Appendix). The interaction between the investigator and participant continued in a conversational discourse structure for approximately 30 minutes or until each target had been elicited between 40 and 50 times. The investigator facilitated the production of the target phoneme during the course of the conversation using direct elicitation. An example interaction is exhibited below. Topic: Proposed federal bailout of Wall Street Target phoneme: /f/ Setup: Investigator will begin by introducing the topic and reading a short related article. Investigator: “What did you think about this article?” RH: types “fine” Investigator: (points to phonic face card) “See how she is biting her lip, ffffffffff. Now you try.” RH: “-ine” Investigator: (Model correct placement and give tactile cue of /f/) “Feel the airflow.” “Try biting your lip and blowing.” RH: “Fine” (Repeated numerous productions) RH: “The Fed is wrong.” (produced with an appropriate [f] sound; this response was typed by RH, and only the target phoneme word was phonated) Investigator: “The Fed is wrong; they need to come up with a better plan.” RESULTS A treatment effect in this design would be demonstrated by an increase from A1 to B1 when the intervention is first applied, a decline from B1 to A2 when the intervention is removed, and a second increase from A2 to B2. This pattern was clearly shown for production of the labials /b/ and /m/ and less clearly for linguals /r/ and /n/ (see Table 1 for data on all phonemes). Percent correct production of both /b/ and /m/ during every session during B1 was higher than every session in A1. Percent correct productions in all of the sessions of A2 were below all of the sessions in B1. Finally, the averages in all of the sessions of B2 were higher than all of the sessions of A2 (Figure 1). Correct production of the lingual sounds /r/ and /n/ both show a delay in treatment effect (Figure 2). A1 scores for /r/ fall from 100% to 40% followed by similarly variable responses in the first two sessions of B1. However, the final five sessions of B1 were higher than the final sessions of A1. In similar fashion, /n/ production stayed stable during the first two sessions of B 1 and then rose in the final sessions of B1. Both /r/ and /n/ declined as expected when the treatment was removed in A2 and then rose again in B2. Although the baseline phases do not demonstrate stable behaviors, which is a weakness of the study, the levels achieved during treatment were higher than the baseline and withdrawal phases. TABLE 1. Individual Target Data for Intervention r (%) b (%) m (%) n (%) Baseline 1 100 40 20 60 Baseline 2 Baseline 3 40 40 0 20 20 40 40 60 Tx 1 86 71 86 60 Tx 2 36 57 50 27 Tx 3 88 64 100 72 Tx 4 100 53 45 68 Tx 5 89 71 88 70 Tx 6 Tx 7 69 100 75 100 73 81 83 83 Withdrawal 1 25 33 13 25 Withdrawal 2 Withdrawal 3 29 45 38 42 33 29 40 43 Tx 8 46 83 63 73 Tx 9 Tx 10 83 92 89 83 75 71 71 100 1.18 27.27 2.89 16.18 4.76 9.95 1.94 13.44 Effect size d SD A SD, standard deviation; Tx, treatment. Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 38 8/2/12 2:01:58 PM 39 TREATING APRAXIA OF SPEECH USING DISCOURSE 120 100 80 60 40 20 9 10 Tx Tx Tx W 7 ith dr aw W l ith dr aw W l ith dr aw l Tx 8 6 5 Tx Tx 3 4 Tx Tx 1 2 Tx 3 Tx e 2 in e in se l Ba se l Ba Ba se l in e 1 0 m b Figure 1. Probe data and treatment (Tx) data for /b/ and /m/. 120 100 80 60 40 20 r 10 Tx 9 Tx dr aw W l ith dr aw W l ith dr aw l Tx 8 7 W ith Tx 6 Tx 5 Tx 4 Tx 3 Tx 1 2 Tx Tx 3 e lin e 2 se Ba lin se Ba Ba se lin e 1 0 n Figure 2. Probe data and treatment (Tx) data for /r/ and /n/. Effect sizes were calculated for each of the treatment sounds by comparing the scores in the A phases with the scores in the B phases. Large effect sizes were found for all target phonemes /b/ (d 2.89), /m/ (d 4.76), /r/ (d 1.18), and /n/ (d 1.94) (see Table 1). The effect size calculation for single-subject design was taken from Robey, Schultz, Crawford, and Sinner (1999) as follows: ES XBXA SA X with the bar over it is the mean and S is the standard deviation. The subscript z should be subscript A. Before treatment, the patient was 0% intelligible at the single-word level as measured by the AIDS. After treatment, the patient was 24% intelligible at the single-word level. This intelligibility was judged by an unfamiliar listener and included words that contained nontargeted sounds. In a 1-month follow-up, RH and his family reported a marked increase in spontaneous word productions at home. He reportedly used spontaneous single words to request, greet, and comment on his surroundings. Many of the words he used during the 1-month follow-up contained word initial sounds that were not trained during the intervention, such as “hello,” “goodnight,” and “thanks.” Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 39 8/2/12 3:40:08 PM 40 JOURNAL OF MEDICAL SPEECH-LANGUAGE PATHOLOGY, VOL. 20, NO. 2 DISCUSSION The current study sought to combine the theories of adult learning and articulatory-kinematic approaches into a treatment for a person with postencephalitic parkinsonism resulting in severe apraxia of speech. This treatment incorporated the use of visual cues embedded in spontaneous discourse for a client-centered approach. RH demonstrated the core speech features of AOS, including inconsistency, groping, and increased durations. Before the intervention, RH had nonfunctional speech output and difficulty initiating single phonemes. Pretesting indicated that RH’s speech was severely compromised by the presence of oral and speech apraxia and dysarthria. Without the support of external cues, RH was unable to produce any spontaneous intelligible speech. Initial consonants were deemed as an appropriate target for intervention because of RH’s difficulty with initiation. It was believed that by targeting frequently occurring word initial phonemes during conversational discourse, RH would be able to use some words to communicate verbally. Consistent with AOS treatment literature, multiple phoneme targets were chosen based on their maximum impact in spoken language. Because of the severely impaired nature of RH’s output, four sounds were chosen for intervention: /b, n, r, m/. Although one of the clinical features of AOS is its inconsistency from day to day and even word-to-word, the treatment used in this study increased consistent accurate productions for all target sounds. RH demonstrated positive treatment effects and large effect sizes on each target phoneme. The individual sound treatment also increased the patient’s overall intelligibility by 24%. In addition to increased target sound productions and single-word speech intelligibility, RH’s family members and caregivers reported that he demonstrated a marked number of spontaneous words or utterances. This anecdotal report led the investigators to be encouraged about the treatment’s generalization given the fact that RH had been essentially nonverbal for nearly 20 years. This study demonstrated that a top-down approach to apraxia treatment could improve overall communication. Although Kendall et al. (2006) and Wambaugh (2010) demonstrated that improved articulation can be achieved by targeting sounds and words, this study extends the previous research by illustrating that seating target phonemes within personally relevant discourse production can increase articulatory production of target sounds. Both previous research and the current study achieved minimal carryover onto untrained targets and increased social communication success, but unlike previous research, the current study achieved rapid communication gain (10 hours) in a person who was previously nonverbal. It is possible that these results were achieved because the intervention was functionalparticipation based. Although traditional research focuses on individuals with single disorders, the individual who participated in this study presented with multiple confounding speech disorders. Because AOS can often co-occur with other speech and language impairments, it is necessary to investigate if our current treatments extend to those individuals with multiple impairments. This can provide for better clinical service to the neurogenic population. One of the limitations of this study was that the probe data should have been collected throughout the baseline and treatment phases. However, this study does demonstrate a consistent difference in producing phonemes in a supported conversational context (during intervention) as opposed to confrontational naming (during baselines). This is a phase 1 study whose aim was to determine whether a treatment effect could be demonstrated. Therefore, although the study’s findings cannot be generalized, they do provide preliminary evidence that would lead to further research for this treatment. Future investigations into AOS should further examine the effects of various linguistic contexts on increasing accurate speech productions. It is also necessary for future investigations to assess maintenance effects. Given that the level of AOS treatment research is preliminary, it is necessary to engage in systematic replication and clinical trials. Acknowledgments We would like to thank RH for giving us his time and trust to participate in this treatment study. We would also like to thank Dr. Hugh Buckingham and Dr. Neila Donovan for providing guidance on this manuscript. Address Correspondence to Meghan C. Savage, Ph.D., Louisiana State University, Department of Communication Sciences and Disorders, 63 Hatch Hall, Rm 71, Baton Rouge, LA, PHONE: (225) 620-5807 e-mail: meg.collins.e@gmail.com Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 40 8/2/12 2:02:01 PM TREATING APRAXIA OF SPEECH USING DISCOURSE REFERENCES Aten, J. (1986). Aphasia and severe apraxia of speech: Charting the treatment course. In R. Marshall (Ed.), Case studies in aphasia rehabilitation (pp. 119–132). Austin, TX: Pro-Ed. Austermann Hula, S. (2007). Current directions in treatment for apraxia of speech: Principles of motor learning. Perspectives on Neurophysiology and Neurogenic Speech and Language Disorder, 17(3), 3–6. Bose, A., Square, P., Schlosser, R., & van Lieshout, P. (2001). Effects of PROMPT therapy on speech motor function in a person with aphasia. Aphasiology, 15(8), 767–785. Dabul, B. (2000). Apraxia Battery for Adults (2nd ed.). Austin, TX: Pro-Ed. Duffy, J. (2005). Motor speech disorders: Substrates, differential diagnosis, and management (2nd ed.). St. Louis: Elsevier. Goodglass, H., & Kaplan, E. (2001). Boston Naming Test (2nd ed.). Baltimore: Lippincott, Williams & Wilkins. Katz, W. F., Bharadwaj, S. V., & Carstens, B. (1999). Electromagnetic articulatory treatment for an adult with Broca’s aphasia and apraxia of speech. Journal of Speech, Language and Hearing Research, 42(6), 1355–1366. Kendall, D., Rodriguez, A., Rosenbek, J., Conway, T., & Gonzalez Rothi, L. (2006). Influence of intensive phonomotor rehabilitation on apraxia of speech. Journal of Rehabilitation Research and Development, 43(3), 409–418. Kimbarow, M. (2007). Integrating life participation approaches to aphasia treatment with adult learning theory: A synergistic approach. Topics in Language Disorders, 27(4), 318–323. Knock, T., Ballard, K., Robin, D., & Schmidt, R. (2000). Influence of order of stimulus presentation on speech motor learning: A principled approach to treatment for apraxia of speech. Aphasiology, 14(5/6), 653–668. LaPointe, L. (1984). Sequential treatment of split lists: A case report. In J. Rosenbek, M. McNeil & A. Aronson (Eds.), Apraxia of speech: Physiology, acoustics, linguistics, management (pp. 141–153). San Diego: College-Hill Press. Maas, E., Barlow, J., Robin, D., & Shapiro, L. (2002). Treatment of sound errors in aphasia and apraxia of speech: Effects of phonological complexity. Aphasiology, 16(4/5/6), 609–622. Maas, E., Robin, D., Austermann Hula, S., Freedman, S., Wulf, G., Ballard, K., et al. (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech-Language Pathology, 17(3), 277–298. Martin, N., Thompson, C., & Worrall, L. (2007). Aphasia rehabilitation: The impairment and its consequences. San Diego: Plural Publishing. 41 McNeil, M., Doyle, P. J., & Wambaugh, J. (2000). Apraxia of speech: A treatable disorder of motor planning and programming. In S. Nadeau, L. Gonzalez Rothi, & B. Crosson (Eds.), Aphasia and language: Theory to practice (pp. 221–266). New York: The Guilford Press. Norris, J. (2001). Phonic faces. Baton Rouge, LA: Elementory.com. Raymer, A., Haley, K., & Kendall, D. (2002). Overgeneralization in treatment for severe apraxia of speech: A case study. Journal of Medical Speech-Language Pathology, 10(4), 313–317. Robey, R., Schultz, M., Crawford, A., & Sinner, C. (1999). Single-Subject clinical-outcome research: Designs, data, effect sizes, and analyses. Aphasiology, 13(6), 445–473. Sarno, M. T. (2004). Aphasia therapy: Historical perspectives and moral imperatives. In J. Duchan & S. Byng (Eds.), Challenging aphasia therapies: Broadening the discourse and extending the boundaries (pp. 19–32). New York: Psychology Press. Simmons-Mackie, N. (2008a). Intervention for a case of severe apraxia of speech and aphasia: A functionalsocial perspective. In N. Martin, C. Thompson & L. Worrall (Eds.), Aphasia rehabilitation: The impairment and its consequences. San Diego: Plural. Simmons-Mackie, N. (2008b). Social approaches to aphasia intervention. In R. Chapey (Ed.), Language intervention strategies in aphasia and related neurogenic communication disorders (5 ed., pp. 290–318). Baltimore: Lippincott, Williams & Wilkins. Square, P., Martin, N., & Bose, A. (2001). The nature and treatment of neuromotor speech disorders in aphasia. In R. Chapey (Ed.), Language intervention strategies in aphasia and related neurogenic communication disorders (pp. 847–884). Baltimore: Lippincott, Williams, & Wilkins. Wambaugh, J. (2004). Stimulus generalization effects of sound production treatment for apraxia of speech. Journal of Medical Speech-Language Pathology, 12(2), 77–97. Wambaugh, J. (2010). Sound production treatment for acquired apraxia of speech. Perspectives on Neurophysiology and Neurogenic Speech and Language Disorders, 20(3), 67–72. Wambaugh, J., Duffy, J., McNeil, M., Robin, D., & Rogers, M. (2006a). Treatment guidelines for acquired apraxia of speech: A synthesis and evaluation of the evidence. Journal of Medical Speech-Language Pathology, 14(2), xv–xxxiii. Wambaugh, J., Duffy, J., McNeil, M., Robin, D., & Rogers, M. (2006b). Treatment guidelines for acquired apraxia of speech: Treatment descriptions and recommendations. Journal of Medical SpeechLanguage Pathology, 14(2), xxxv–lxvii. Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 41 8/2/12 2:02:01 PM 42 JOURNAL OF MEDICAL SPEECH-LANGUAGE PATHOLOGY, VOL. 20, NO. 2 Wambaugh, J., Kalinyak-Fliszar, M., West, J., & Doyle, P. J. (1998). Effects of treatment for sound errors in apraxia of speech and aphasia. Journal of SpeechLanguage, and Hearing Research, 41, 425–743. Wambaugh, J., Martinez, A., McNeil, M., & Rogers, M. (1999). Sound production treatment for apraxia of speech: Overgeneralization and maintenance effects. Aphasiology, 13(9-11), 821–837. Wambaugh, J., West, J., & Doyle, P. J. (1998). Treatment for apraxia of speech: Effects of targeting sound groups. Aphasiology, 12(7/8), 731–743. Wertz, R. (1998). A case of aphasia, apraxia of speech, and apraxia of phonation. In N. Helm-Estabrooks & A. Holland (Eds.), Approaches to the treatment of aphasia (pp. 11–36). San Diego: Singular Publishing Group. Wertz, R., LaPointe, L., & Rosenbek, J. (1984). Apraxia of speech in adults: The disorder and its management. Orlando, FL: Grune & Stratton. Yorkston, K., Beukelman, D., & Traynor, C. (1984). Assessment of Intelligibility of Dysarthric Speech. Austin: Pro-Ed. Submit a manuscript online – www.cengage.com/community/JMSLP 26537_ch04_ptg01_035-043.indd 42 8/2/12 2:02:01 PM Appendix: Examples of Phonological Support Visual Cues c a n d y Phonic Faces (Norris, 2001) Photographs of mouths depicting articulatory placement taken of the investigators Journal of Medical Speech-Language Pathology Volume 20, Number 2, p. 43 Copyright © 2012 Delmar Cengage Learning 26537_ch04_ptg01_035-043.indd 43 8/2/12 5:29:46 PM