March-April 2013 | Volume 15 | Issue 63 www.noiseandhealth.org
advertisement

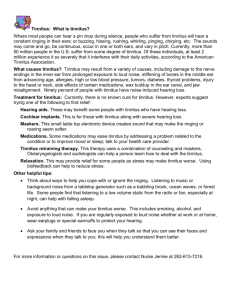
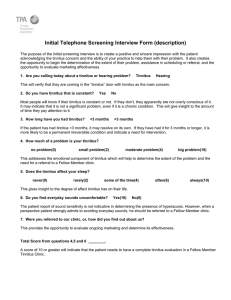
I ith & w SE d e A ex MB d In E, E N LI ED SC ISSN 1463-1741 Impact Factor® for 2011: 1.254 M Noise & Health • Volume 15 • Issue 63 • March-April 2013 • Pages 81-152 A Bi-monthly Inter-disciplinary International Journal www.noiseandhealth.org March-April 2013 | Volume 15 | Issue 63 No cochlear dead regions detected in non‑pulsatile tinnitus patients: An assessment with the threshold equalizing noise (sound pressure level) test Annick Gilles1,2,3, Dirk De Ridder4, Paul Van de Heyning1,2,3 Departments of Otorhinolaryngology and Head and Neck Surgery, Antwerp University Hospital, Edegem, 2Translational Neurosciences, Faculty of Medicine, Campus Drie Eiken, Antwerp University, Wilrijk, 3Tinnitus Research Initiative Centre, BRAI2N, Antwerp University Hospital, Edegem, Belgium, 4Surgical Sciences, Dunedin School of Medicine, University of Otago, New Zealand 1 Abstract One of the hypotheses on the etiology of non‑pulsatile tinnitus in normal or hearing impaired patients is the existence of sharp edged cochlear dead regions (DR) flanking normal functioning hair cells. The lack of inhibition of DR on the neighboring neurons may lead to hyperactivity. Currently the Threshold Equalizing Noise test (TEN test) is the reference test to clinically assess cochlear DR. To identify cochlear DR in patients with non‑pulsatile tinnitus with and without hearing loss using the TEN (sound pressure level)‑test. Data were obtained from adult patients with non‑pulsatile tinnitus visiting the Tinnitus Clinic of the University Hospital Antwerp. The TEN (SPL)‑test was performed to assess the presence of cochlear DR for test frequencies ranging from 0.5 to 8 kHz. A total of 55 ears of 33 subjects (15 male; 18 female) with non‑pulsatile tinnitus were included in the study. Subjects were divided into subgroups based on the audiometric configuration of hearing loss: Flat configuration (N = 23), high‑frequency gently sloping (N = 10) and high‑frequency steeply sloping (N = 22). In forty‑eight ears there was no evidence of cochlear DR. In seven ears the results were inconclusive. This occurred in patients with high‑frequency steeply sloping audiogram configurations. The present study does not support the TEN (SPL) test as a reliable tool for the detection of cochlear DR in a tinnitus population. Keywords: Dead regions, inner hair cells, non‑pulsatile, threshold equalizing noise, tinnitus Introduction A dead region (DR) can be defined as a region in the cochlea where the inner hair cells (IHCs) along the basilar membrane and/or neurons are non‑functioning or missing, resulting in the absence of basilar membrane vibration transduction to the brain at those places.[1,2] This does not mean that a particular tone is not audible. A tone producing peak vibration at a particular place on the basilar membrane can be detected by off‑place or off‑frequency listening provided that the stimulus is sufficiently loud. The tone will not be detected at its usual place on the basilar membrane but at an adjacent place where the IHCs are functioning more effectively.[2,3] The extent of a DR can be defined in 2 manners: Either by distance along the Access this article online Quick Response Code: Website: www.noiseandhealth.org DOI: 10.4103/1463-1741.110297 PubMed ID: *** 129 basilar membrane, described by the characteristic frequencies related to this place (e.g., a DR extending from 4000 to 10 000 Hz), or by the characteristic frequency (CF) of IHCs or neurons adjacent to the DR.[2] The presence of a DR can result in several problems such as abnormal pitch perception,[4] rapid loudness growth,[5] and distorted perception of pure tones.[6] In order to diagnose cochlear DRs, the Threshold Equalizing Noise (TEN) test was developed.[7] In this test a broadband masking noise (the TEN) is used which is spectrally shaped so that all auditory output filters contain an equal noise power. This means that, for subjects with normal hearing thresholds, the masked threshold for a pure tone is the same for all frequencies over the range of 250‑10 000 Hz. More specifically, the TEN level is specified as the level in a one‑Equivalent Rectangular BandwidthN (ERBN) (132 Hz) wide band centered at 1000 Hz, where ERBN stands for the average of the auditory filter as determined for young normal‑hearing subjects at moderate sound levels.[2] For example, if the TEN noise is presented at a dial level of 70 (corresponding to 70 dB/ERB), then thresholds, for normal hearing subjects, across a wide frequency range, measured in this noise should also be 70 dB SPL. Figure 1[2] illustrates the principle of the TEN test. Looking at the top panel, the solid curve represents the basilar Noise & Health, March-April 2013, Volume 15:63, 129-33 Gilles, et al.: Assessing dead regions in tinnitus patients a b Figure 1: Illustration of the principle of the Threshold Equalizing Noise test (TEN [SPL]) test. The basilar membrane vibration of a 1.5 kHz tone is represented by the solid curve. (a) The shaded area reflects a dead zone starting at 1.07 kHz. 40 dB of basilar membrane vibration is needed (long‑dashed line) in order to measure absolute thresholds below 1.07 kHz. The short‑dashed line represents the absolute threshold value of a 1.5 kHz tone, which is 67 dB. A threshold is measurable due to intact IHC’s adjacent to the dead region. (b) A TEN of 70 dB/ERBN is added to mask the 1.5 kHz tone at 67 dB. In case of a dead region, the intensity of the tone needs to be raised substantially in order to achieve audibility again. This figure was derived from Moore et al. 2004[7] membrane vibration pattern for a pure tone with a CF of.[1] 5 kHz, expressed by the maximum vibration at that frequency. The shaded area reflects the presence of a high‑frequency DR starting at approximately 1.07 kHz. To measure absolute thresholds for frequencies below 1.07 kHz, 40 dB of basilar membrane vibration is needed (long‑dashed line). As indicated by the short‑dashed line, the absolute threshold value of a 1.5 kHz tone (which falls within the DR) is 67 dB. A threshold is measurable because of the intact IHC’s adjacent to the DR (= off‑frequency listening). In the bottom panel a TEN of 70 dB/ERBN is added masking the 1.5 kHz tone at 67 dB. To make the tone audible again the level has to be increased so that basilar vibration just below the 1.07 kHz DR slightly exceeds 70 dB. A level of 97 dB is required in order to achieve audibility of the tone again. A normal hearing subject with no DR would have a masked threshold of approximately 70 dB. This figure shows that for the person with a DR, the masked threshold was 30 dB higher than the unmasked threshold (97 dB vs. 67 dB) and that the masked threshold was 27 dB higher than in the case where there was no DR (97 dB vs. 70 dB). This last remark demonstrates the two criteria that need to be fulfilled to determine a DR: (1) at least 10 dB of masking is required and (2) the masked threshold should be at least 10 dB higher than normal.[2] There are currently two commercially available TEN test versions: the TEN sound pressure level test (TEN-SPL) and the TEN hearing loss level test (TEN-HL).[2] They differ in 3 ways: Frequency range tested, amplitude characteristics of the TEN noise and the calibration. The TEN (SPL) test is calibrated in dB SPL and covers a frequency range of 250‑10 000 Hz. The TEN (HL) test is the modified version of the TEN (SPL), calibrated in dB HL which is easier to interpret as the audiometer is also calibrated in dB HL. The frequency range of the TEN (HL) is narrowed to 250‑4000 Hz and the TEN noise contains a lower Noise & Health, March-April 2013, Volume 15 crest factor. The present study aims to investigate whether cochlear DRs are more prevalent in patients suffering from tinnitus. Tinnitus, the perception of sound in the absence of an external acoustic sound source, poses a clinical problem for millions of people around the world.[8] The understanding of the pathological mechanism of tinnitus generation remains in the stage of hypothesis and conjecture. One of the hypotheses on the etiology of non‑pulsatile tinnitus is the existence of sharp edged cochlear DRs flanking normal functioning hair cells. The lack of inhibition of DRs on the neighboring neurons may lead to hyperactivity. Previous studies showed that tinnitus in the absence of measurable hearing loss at all frequencies or at the tinnitus frequency does not exclude cochlear/neural damage.[9] Previously the detection of DRs was reported in eight out of eleven subjects with normal hearing and non‑pulsatile tinnitus,[10] providing evidence for the theory that deafferentiation is also possible in tinnitus subjects with audiometrically normal hearing thresholds. In the present study we used the TEN (SPL) test in order to assess cochlear DRs in an adult population with non‑pulsatile tinnitus and various audiometric configurations. Methods Subjects Thirty‑three patients presenting with non‑pulsatile tinnitus in the University Hospital Antwerp (UZA) underwent the standard otorhinolaryngologic (ORL) and audiometric protocol for tinnitus. In addition, the TEN (SPL) test was performed in tinnitus ears only. The group consisted of fifteen male and eighteen female patients with a mean age of 51.7 ± 16.2‑years‑old (range 20‑73). Twenty‑two patients suffered from bilateral tinnitus while eleven patients perceived a unilateral tinnitus in either the right or left ear. 130 Gilles, et al.: Assessing dead regions in tinnitus patients Pure‑tone audiometry All patients received visual inspection of the eardrum by an ORL‑specialist. In addition, tympanometry was normal in all subjects so middle ear pathologies were excluded. According to current clinical standards (ISO 8253‑1, 1989), air conduction threshold were measured at 125, 250, 500, 1000, 2000, 3000, 4000, 6000 and 8000 Hz using a 2‑channel Interacoustics AC‑40 audiometer in a soundproof booth. Bone conduction thresholds were measured at 250, 500, 1000, 2000, 3000 and 4000 Hz. All the patients included in this study had a normal hearing or a sensorineural hearing loss (SNHL) as the air‑bone gap never exceeded 10 dB HL. For all the analyses only those ears in which tinnitus was perceived were included in this study. Tinnitus ears were divided into 3 categories in accordance with Demeester et al., (2009): A flat configuration, a high‑frequent gently sloping (HFGS) configuration and a high‑frequent steeply sloping (HFSS) configuration. To be categorized as a flat configuration, the difference between the mean thresholds of 250/500 Hz, the mean of 1 kHz/2 kHz thresholds, and the mean of 4 kHz/8 kHz should be less than or equal to 15 dB. A HFGS configuration is defined as an audiogram where the difference between the mean of 500 Hz/1 kHz thresholds and the mean of 4 kHz/8 kHz thresholds is greater than 15 dB but less than 29 dB. Finally, a HFSS configuration is present when the difference between the mean of 500 Hz/1 kHz thresholds and the mean of 4 kHz/8 kHz is 30 dB or more.[11] Of all tinnitus ears, 24 were categorized with a flat, 10 with a HFGS, and 21 with a HFSS configuration. Tinnitus analysis A Dutch validated version of the Tinnitus Questionnaire (TQ),[12] was completed by the majority of patients (four patients did not complete the questionnaire). The TQ was originally published by Goebel and Hiller.[13] who described the TQ as a global index of tinnitus‑related distress. Based on the total score on the TQ, patients are assigned to a distress category: Slight (0‑30 points: Grade 1), moderate (31‑46 points: Grade 2), severe (47‑59 points, grade 3) and very severe (60‑84 points, grade 4). played continuously and both volume unit (VU) meters were adjusted to read 0 dB. Absolute thresholds were measured using a final 2 dB‑step size to determine the threshold. Subsequently, the TEN was presented with a level of 70 dB and the masked thresholds were measured in a similar way. In case the absolute thresholds of a patient were 60 dB SPL or worse, the level of the TEN was raised. Therefore, the TEN provided at least 10 dB of masking at all times. A DR was considered present if the following criteria were both met.[7] • The masked threshold is at least 10 dB worse than the absolute threshold • The masked threshold is at least 10 dB worse than the masking noise (TEN) The results were categorized as positive (DRs present), negative (no DRs present) or inconclusive. Several situations can cause inconclusive results. Firstly, it may be impossible to produce 10 dB of masking in patients with severe or profound SNHL because the maximum output of the audiometer is reached. Therefore, the intensity of the TEN will not cause sufficient masking. Secondly, when the TEN level was considered as too loud by the patient, the level was lowered and did not provide sufficient masking, leading to inconclusive results. Finally, absolute and/or masked thresholds could not be measured in some patients with profound hearing loss at certain frequencies because of output limitations of the audiometer. Results The audiometric results are represented graphically in Figure 2 where mean absolute hearing thresholds of patients with a flat (N = 24), a HFGS (N = 10) and HGSS (N = 21) are shown. A full tinnitus analysis was performed on 31 ears of 21 patients (10 with bilaterally tinnitus, 11 with unilateral tinnitus). Table 1 shows the results of the tinnitus analysis after pitch matching as well as the tinnitus type (pure tone or noise‑like). In addition, Table 2 shows the scores for VAS and TQ. The Secondly, patients had to score their tinnitus loudness on a Visual Analogue Scale (VAS) going from 0 (no tinnitus) to 10 (tinnitus extremely loud). Finally, tinnitus pitch and intensity were determined through tinnitus analysis using pitch matching and loudness matching procedures. Threshold equalizing noise (SPL) procedure The TEN (SPL) test was performed in all fifty‑five tinnitus ears using an original TEN (SPL) CD played by a CD player (Sony CDP‑XE270) and presented through a TDH‑39 supra‑aural earphone. First, the audiometer was connected to the CD player output plug. Input channel 1 on the audiometer was selected on the left side, and channel 2 was selected on the right side. The first track on the CD, a calibrating tone, was 131 Figure 2: Graphical illustration of the mean audiometric results of the three subgroups (flat, high‑frequent gently sloping and high‑frequent steeply sloping audiometric configurations) of the tinnitus patients Noise & Health, March-April 2013, Volume 15 Gilles, et al.: Assessing dead regions in tinnitus patients majority of patients experienced a high‑pitched tinnitus and mostly a noise‑like character. The tinnitus loudness was scored on a VAS by nineteen of the thirty‑three patients (of which in 11 patients with bilateral tinnitus, the VAS was also scored bilaterally). Tinnitus intensity was measured in 26 patients and 29 patients completed the TQ of which eight patients were categorized with a degree 1, 10 with a 2nd degree, 9 with a 3rd and 2 with a 4th degree. Because of time shortcomings in the daily clinical practice, all (TQ, VAS and tinnitus analysis) were not always done completely. Therefore, Tables 1 and 2 do not contain data of all ears of all patients on which the TEN (SPL) was applied. In patients suffering from bilateral tinnitus, the TEN (SPL) test was performed in both ears. In patients with unilateral tinnitus, TEN (SPL) was performed in the affected ear only. Figure 3 shows the mean masked threshold per frequency in 70 dB SPL of TEN (or more in subjects where the unmasked threshold exceeded 60 dB SPL). The mean masked thresholds were 10 dB SPL or more better than the ‘normal’ masked threshold (which would be 70 dB SPL in 70 dB TEN) for all frequencies meaning that the tone was audible even at a level much lower than the TEN level. As one of the criteria for a DR states that the masked threshold should be at least 10 dB worse than the unmasked threshold, no DRs were found in these patients. Therefore, the outcome of most TEN (SPL) tests were negative. Nevertheless, four patients showed inconclusive results at certain frequencies. In one patient with a symmetric HFSS audiogram configuration and bilateral non‑pulsatile tinnitus, the unmasked threshold could not be measured bilaterally upwards from 2 kHz because of audiometer output limitation as the unmasked threshold exceeded 120 dB HL. In three other patients with a HFSS configuration (two patients with bilateral tinnitus and one with unilateral tinnitus), the unmasked threshold were measured but the TEN noise could not be set loud enough to provide sufficient masking. Therefore the results in these patients remained inconclusive for a DR located in the high frequencies. An oversight of inconclusive results along with the reason of inconclusiveness is given in Table 3. Discussion It has been suggested that tinnitus is often accompanied by severe (IHCs damage in certain cochlear regions, even in the absence of measurable hearing loss.[9,10] Severe IHC damage causes deafferentiation and therefore DRs in the cochlea. In the present study tinnitus patients with different audiometric configurations and hearing thresholds (going from normal hearing to profound hearing loss) were tested for DRs by use of the TEN (SPL) test. In the study of Weisz et al., (2006) a normal hearing student population suffering from tinnitus was tested of which eight out of eleven subjects were identified with a DR.[10] In another study, in which the TEN (HL) test was applied, 15% of tinnitus patients with normal hearing sensitivity had positive TEN results, indicative for a DR.[14] In our normal hearing subjects with tinnitus (N = 16 ears), no DRs were identified. It has been reported earlier that it is more likely that IHC damage/ loss is involved in subjects where the hearing loss exceeds 55 to 60 dB.[15] Furthermore, it has been found that a DR is more prevalent in subjects with a hearing loss exceeding 55 to 60 dB SPL.[3,14] In addition, severe high‑frequency hearing loss or high frequency steeply sloping audiograms are more associated with DRs and positive TEN findings. Several studies found a greater prevalence of DRs in subjects with a steep slope.[3,16] The present study was not able to confirm these findings as also those ears with a HFSS audiogram configuration (N = 22) showed negative TEN results. However, as mentioned earlier and elucidated in Table 3, in four patients with a HFSS configuration, unmasked or masked thresholds could not be obtained in seven tinnitus ears because of audiometer output limitations. Here the TEN Table 1: tinnitus characteristics of 31 measured tinnitus ears: pitch and tinnitus type 0.125 0.75 Ears 1 2 1 1 Pitch (kHz) 1.5 2 4 2 1 9 6 5 8 9 9 1 Tinnitus Type PT N 11 20 PT= pure tone; N= noise Table 2: Mean scores for the VAS, tinnitus intensity (in dB SL) and TQ, including standard deviations for N (=amount) out of the 33 patients VAS Mean 5.74 SD 2.25 N=19 dB SL Mean SD 7.73 8.53 N= 26 TQ Mean SD 37.55 16.47 N= 29 Table 3: Oversight of inconclusive results at a particular frequency with reasoning for the categorizing as ‘inconclusive' Figure 3: Mean difference between the masked thresholds and the Threshold Equalizing Noise test noise given for all TEN (SPL) test frequencies of all ears with measurable thresholds (48 ears of 29 patients) Noise & Health, March-April 2013, Volume 15 Patient #8 #8 #24 #24 #25 #26 #26 Ear Right Left Right Left Left Right Left Frequency 8 kHz 8 kHz 4 kHz to 8 kHz 2 kHz to 8 kHz 6 kHz to 8 kHz 4kHz to 8 kHz 8 kHz Reason Unmasked threshold not measurable Unmasked threshold not measurable Insufficient TEN noise Insufficient TEN noise Insufficient TEN noise Insufficient TEN noise Insufficient TEN noise 132 Gilles, et al.: Assessing dead regions in tinnitus patients findings remained inconclusive. The problem of the amount of inconclusive results of the TEN (SPL) test has been previously reported by Hornsby and Dundas (2009) where in 80% of the ears inconclusive results were found for at least one frequency and 30% at three frequencies or more.[3] Vinay and Moore (2007) also noted that it is more likely to have inconclusive results when the audiometric thresholds exceed 85 dB HL.[14] The TEN (HL) test can be presented at higher levels without distortion and might therefore reduce the amount of inconclusive results.[2] Nevertheless, in the present study, the TEN (SPL) was deliberately chosen over the TEN (HL) because of the wider frequency range. Furthermore, as tinnitus analysis showed that most patients included in this study, perceived a high pitched tinnitus, we were especially interested in the cochlear preservation at those frequencies. Thirty‑two ears of the patients included in the present study, were characterized as a HFGS (N = 10) or a HFSS (N = 22) configuration. As mentioned before, patients with high‑frequency steeply sloping audiometric configurations are more likely to have a DR in that area. Such results were not found by the current study. As the present study aimed to assess the TEN (SPL) as a clinical tool for the explanation of tinnitus, the question arises whether cochlear DRs are necessary for a tinnitus percept. It has been shown that immediately after acute (impulse) noise trauma in military personnel, 88% of the soldiers perceived a noise‑induced tinnitus.[16] The presence of cochlear DRs was determined by the use of psychophysical tuning curves (PTCs), which is considered as a more reliable tool by some authors.[17] It has been shown that immediately after acute impulse noise trauma in military personnel 70% of the soldiers had DRs, 50% of which recovered partially or completely (narrowing or disappearing of the DR zone) after some time. The high prevalence of DRs after noise trauma may be involved in noise‑induced tinnitus. However, the fact that some patients with tinnitus had no DRs and some patients with DRs had no tinnitus supports the hypothesis that the presence of a DR is neither necessary nor sufficient to induce tinnitus.[16] These findings fit the suggestion that OHCs might be of more importance than IHCs in the generation of tinnitus as in a previous study in a group of normal hearing tinnitus patients 85% demonstrated abnormal transient otoacoustic emissions, of which only 15% abnormal TEN (HL) findings.[18] In conclusion, tinnitus is a common phenomenon in modern society. While the etiology of tinnitus remains elusive in many cases, research is needed in order to identify a possible causative factor. One of the hypotheses on non‑pulsatile tinnitus is the presence of cochlear DR leading to central hyperactivity. If DR can be identified by use of the TEN test, the present study does not support the concept that DR are necessary for tinnitus. Therefore, the use of the TEN test as a diagnostic tool in a tinnitus population might be of limited value. The authors would like to point out that the present study does not designate the TEN test to be unreliable as a whole but as a result of the present findings the TEN test does not provide a useful tool in the diagnostics of tinnitus patients. Further research with the TEN test in tinnitus patients is necessary in order to confirm these findings. 133 Acknowledgments This research was supported by the Stavros Niarchos Foundation and a TOP‑BOF project of the University Antwerp. Address for correspondence: Mrs. Annick Gilles, University Hospital Antwerp, Wilrijkstraat 10, 2650 Edegem, Belgium. E‑mail: annick.gilles@UZA.be References 1. Moore BC, Glasberg BR. A model of loudness perception applied to cochlear hearing loss. Aud Neurosci 1997;3:289‑311. 2. Moore BC. Dead regions in the cochlea: Conceptual foundations, diagnosis, and clinical applications. Ear Hear 2004;25:98‑116. 3. Hornsby BW, Dundas JA. Factors affecting outcomes on the TEN (SPL) test in adults with hearing loss. J Am Acad Audiol 2009;20:251‑63. 4. Huss M, Moore BC. Dead regions and pitch perception. J Acoust Soc Am 2005;117:3841‑52. 5. Malicka AN, Munro KJ, Baker RJ. Diagnosing cochlear dead regions in children. Ear Hear 2010;31:238‑46. 6. Huss M, Moore BC. Dead regions and noisiness of pure tones. Int J Audiol 2005;44:599‑611. 7. Moore BC, Huss M, Vickers DA, Glasberg BR, Alcántara JI. A test for the diagnosis of dead regions in the cochlea. Br J Audiol 2000;34:205‑24. 8. Henry JA, Dennis KC, Schechter MA. General review of tinnitus: Prevalence, mechanisms, effects, and management. J Speech Lang Hear Res 2005;48:1204‑35. 9. Kujawa SG, Liberman MC. Adding insult to injury: Cochlear nerve degeneration after temporary noise‑induced hearing loss. J Neurosci 2009;29:14077‑85. 10.Weisz N, Hartmann T, Dohrmann K, Schlee W, Norena A. High‑frequency tinnitus without hearing loss does not mean absence of deafferentation. Hear Res 2006;222:108‑14. 11. Demeester K, van Wieringen A, Hendrickx JJ, Topsakal V, Fransen E, Van Laer L, et al. Prevalence of tinnitus and audiometric shape. B‑ENT 2007;3:37‑49. 12. Meeus O, Blaivie C, Van de Heyning P. Validation of the Dutch and the French version of the Tinnitus Questionnaire. B‑ENT 2007;3:11‑7. 13. Goebel G, Hiller W. The tinnitus questionnaire. A standard instrument for grading the degree of tinnitus. Results of a multicenter study with the tinnitus questionnaire. HNO 1994;42:166‑72. 14.Vinay, Moore BC. Prevalence of dead regions in subjects with sensorineural hearing loss. Ear Hear 2007;28:231‑41. 15. Liberman MC, Dodds LW. Single‑neuron labeling and chronic cochlear pathology. III. Stereocilia damage and alterations of threshold tuning curves. Hear Res 1984;16:55‑74. 16.Etchelecou MC, Coulet O, Derkenne R, Tomasi M, Noreña AJ. Temporary off‑frequency listening after noise trauma. Hear Res 2011;282:81‑91. 17. Summers V, Molis MR, Müsch H, Walden BE, Surr RK, Cord MT. Identifying dead regions in the cochlea: Psychophysical tuning curves and tone detection in threshold‑equalizing noise. Ear Hear 2003;24:133‑42. 18. Thabet EM. Evaluation of tinnitus patients with normal hearing sensitivity using TEOAEs and TEN test. Auris Nasus Larynx 2009;36:633‑6. How to cite this article: Gilles A, De Ridder D, Van de Heyning P. No cochlear dead regions detected in non-pulsatile tinnitus patients: An assessment with the threshold equalizing noise (sound pressure level) test. Noise Health 2013;15:129-33. Source of Support: Nil, Conflict of Interest: None declared. Noise & Health, March-April 2013, Volume 15