Cardiovascular Research 61 (2004) 372 – 385
www.elsevier.com/locate/cardiores
Review
Mitochondrial permeability transition pore opening during myocardial
reperfusion—a target for cardioprotection
Andrew P. Halestrap *, Samantha J. Clarke, Sabzali A. Javadov 1
Department of Biochemistry and The Bristol Heart Institute, University of Bristol, Bristol BS8 1TD, UK
Received 28 May 2003; received in revised form 28 July 2003; accepted 29 July 2003
Time for primary review 14 days
Abstract
Reperfusion of the heart after a period of ischaemia leads to the opening of a nonspecific pore in the inner mitochondrial membrane,
known as the mitochondrial permeability transition pore (MPTP). This transition causes mitochondria to become uncoupled and capable of
hydrolysing rather than synthesising ATP. Unrestrained, this will lead to the loss of ionic homeostasis and ultimately necrotic cell death. The
functional recovery of the Langendorff-perfused heart from ischaemia inversely correlates with the extent of pore opening, and inhibition of
the MPTP provides protection against reperfusion injury. This may be mediated either by a direct interaction with the MPTP [e.g., by
Cyclosporin A (CsA) and Sanglifehrin A (SfA)], or indirectly by decreasing calcium loading and reactive oxygen species (ROS; key inducers
of pore opening) or lowering intracellular pH. Agents working in this way may include pyruvate, propofol, Na+/H+ antiporter inhibitors, and
ischaemic preconditioning (IPC). Mitochondrial KATP channels have been implicated in preconditioning, but our own data suggest that the
channel openers and blockers used in these studies work through alternative mechanisms. In addition to its role in necrosis, transient opening
of the MPTP may occur and lead to the release of cytochrome c and other proapoptotic molecules that initiate the apoptotic cascade.
However, only if subsequent MPTP closure occurs will ATP levels be maintained, ensuring that cell death continues down an apoptotic,
rather than a necrotic, pathway.
D 2003 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
Keywords: Ischaemic preconditioning; Mitochondrial potassium channels; Calcium overload; Reactive oxygen species; Apoptosis
1. Introduction
Mitochondria play critical roles in both the life and death
of cells. In healthy cardiac myocytes, their primary function
is the provision of ATP through oxidative phosphorylation
to meet the high energy demands of the beating heart.
Abbreviations: ANT, adenine nucleotide translocase; BKA, bongkrekic
acid; CAT, carboxyatractyloside; CsA, Cyclosporin A; CyP, cyclophilin;
DOG, 2-deoxyglucose; EDP, end diastolic pressure; IPC, ischaemic
preconditioning; LVDP, left ventricular developed pressure; MPT, mitochondrial permeability transition; MPTP, mitochondrial permeability
transition pore; PPIase, peptidyl-prolyl cis – trans isomerase; ROS, reactive
oxygen species; SfA, Sanglifehrin A; VAAC, voltage-activated anion
channel
* Corresponding author. Tel.: +44-117-928-8592; fax: +44-117-9288274.
E-mail address: a.halestrap@bristol.ac.uk (A.P. Halestrap).
1
Current address: Department of Physiology and Pharmacology,
University of Western Ontario, Medical Sciences Building, London,
Ontario, Canada N6A 5C1.
Glycolysis alone is unable to meet these demands even in
the resting state and inhibition of oxidative phosphorylation,
as occurs in anoxia or ischaemia, leads to impairment or
cessation of normal heart function. However, latent within
mitochondria, there exist mechanisms that, once activated,
convert the mitochondria from organelles that support the
life of the cell to those that actively induce both apoptotic
and necrotic cell death. The switch in roles, akin to the
conversion of Dr. Jekyll to Mr. Hyde, is mediated by the
opening of a nonspecific pore in the mitochondrial inner
membrane, known as the mitochondrial permeability transition pore (MPTP). This normally remains closed, but can
open under conditions of cellular stress with dire consequences. In this review, we will briefly summarise what is
known about the molecular mechanism of the MPTP and
why it opens during reperfusion. We will then describe the
techniques that have been used to measure pore opening in
the perfused heart, and how these experiments have led to
the proposal that the extent of pore opening is a critical
determinant of reperfusion injury. Finally, we will describe
0008-6363/$ - see front matter D 2003 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
doi:10.1016/S0008-6363(03)00533-9
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
how inhibiting MPTP opening is an effective strategy for
the protection of hearts from reperfusion injury.
2. The mitochondrial permeability transition pore
2.1. Causes and consequences of MPTP opening
Under normal physiological conditions, the mitochondrial inner membrane is impermeable to all, but a few,
selected metabolites and ions. However, under conditions
of stress, a nonspecific pore known as the mitochondrial
permeability transition pore can open in the mitochondrial
inner membrane that allows free passage of any molecule
of < 1.5 kDa [1– 3]. When the MPTP opens, the permeability barrier of the inner membrane becomes disrupted
with two major consequences. First, although all small
molecular weight solutes move freely across the membrane,
proteins do not and, as a result, they exert a colloidal
osmotic pressure that causes mitochondria to swell. Although the unfolding of the cristae allows the matrix to
expand without rupture of the inner membrane, the outer
membrane will break and lead to the release of proteins in
the intermembrane space such as cytochrome c and other
factors that play a critical role in apoptotic cell death (see
Section 3.2.1). Second, the inner membrane becomes freely
permeable to protons. This uncouples oxidative phosphorylation, causing the proton-translocating ATPase to reverse
direction and so actively hydrolyse ATP, rather than synthesis it. Under such conditions, intracellular ATP concen-
373
trations rapidly decline, leading to the disruption of ionic
and metabolic homeostasis and the activation of degradative enzymes such as phospholipases, nucleases, and proteases. Unless pore closure occurs, these changes will cause
irreversible damage to the cell, resulting in necrotic death.
Even if closure does occur, the mitochondrial swelling and
outer membrane rupture may be sufficient to set the
apoptotic cascade in motion. Thus, it is hardly surprising
that the MPTP is kept firmly closed under normal physiological conditions and is only activated under pathological
conditions. The key factor responsible for MPTP opening is
mitochondrial calcium overload (i.e., when mitochondrial
matrix [Ca2 +] is greatly increased), especially when this is
accompanied by oxidative stress, adenine nucleotide depletion, elevated phosphate concentrations, and mitochondrial
depolarisation [1,4]. These conditions are exactly those that
the heart experiences during postischaemic reperfusion, and
there is increasing evidence that MPTP opening is critical
in the transition from reversible to irreversible reperfusion
injury [1,4].
2.2. The molecular mechanism of the MPTP
For a detailed account of the molecular mechanism of
the MPTP, including the experimental evidence on which
this is based, the reader is directed to other recent reviews
from this and other laboratories [1,3,5]. As illustrated in
Fig. 1, the core components of the MPTP are the adenine
nucleotide translocase (ANT) and a mitochondrial cyclophilin D (CyP-D) that exhibits peptidyl-prolyl cis –trans
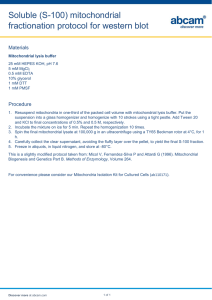
Fig. 1. The proposed molecular mechanism of the mitochondrial permeability transition pore. The probable sites of action of known effectors of pore opening
are shown in Table 1.
374
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
isomerase (PPIase) activity. Triggered by Ca2 +, whose
binding to the ANT is inhibited by adenine nucleotides,
this PPIase activity causes a conformational change of the
carrier that converts it into a nonspecific pore. Cyclosporin
A (CsA) acts as a potent inhibitor of MPTP opening
(K0.5 = 5 nM) by preventing CyP-D binding to the ANT.
Very recently, we have described another extremely potent
inhibitor of the MPTP, Sanglifehrin A (SfA), which is
unrelated to CsA [6]. SfA does not prevent CyP-D binding
to the ANT but does inhibit its PPIase activity (K0.5 < 5
nM), preventing it from facilitating the conformational
change of the ANT required for pore formation. An
important advantage of SfA is that, unlike the complex
of CsA with cytosolic cyclophilin A (CyP-A), the SfA –
CyP-A complex has no effect on the calcium-activated
protein phosphatase, calcineurin. Inhibition of the MPTP
by both SfA and CsA can be overcome at high [Ca2 +],
suggesting that the conformational change facilitated by
CyP-D can occur in its absence. Indeed, reconstitution
studies have shown that at high [Ca2 +], the purified ANT
can undergo a conformational change to produce a nonspecific channel in the absence of CyP-D, although the
sensitivity to [Ca2 +] is enhanced by its presence [7,8].
Other proteins have been implicated in MPTP formation by
many workers including the outer membrane voltage-dependent anion channel (VDAC; also known as porin) and
the peripheral benzodiazepine receptor [1,3,5]. Although
there is debate over whether such proteins are essential
structural components or merely exert an important regulatory role, it does seem probable that the MPTP is
associated with contact sites between the outer and inner
mitochondrial membranes where VDAC and the ANT are
thought to interact [1,3,5].
Numerous factors can influence the sensitivity of MPTP
opening to [Ca2 +] and these are summarised in Table 1. Any
intervention that reduces adenine nucleotide binding to the
ANT enhances pore opening, including adenine nucleotide
depletion, matrix phosphate (competes for the nucleotide
binding site), and the conformational state of the ANT. The
latter can be influenced by specific ligands of the ANT such
as carboxyatractyloside (CAT; decreases matrix ADP binding affinity) and bongkrekic acid (BKA; increases matrix
ADP binding affinity) as well as by the membrane potential
(Dw). Of particular relevance to reperfusion injury, we have
shown that oxidative stress also sensitises the MPTP to
[Ca2 +] by antagonising adenine nucleotide binding, but in
addition, it increases CyP-D binding to the ANT. Low pH
( < 7) and Mg2 + inhibit MPTP opening by antagonising
Ca2 + binding [3,5]. The modes of action of two other potent
inhibitors of the MPTP are not clear. Trifluoperazine is a
potent inhibitor of the MPTP under energised, but not
deenergised, conditions and may act by altering surface
membrane charge and hence the voltage sensitivity of the
MPTP [3]. More recently, it has been shown that ubiquinone
Table 1
Proposed sites of action of known effectors of the mitochondrial permeability transition
Effect via change in CyP-D binding
to the ANTa
Activatory
Oxidative stress (e.g., reperfusion,
t-butyl hydroperoxide, or diamide)
or vicinal thiol reagents
(e.g., phenylarsine oxide) to
cross-link Cys159 with Cys256 of
the ANT
Increased matrix volume
Chaotropic agents
Inhibitory
CsA and some analogues
(e.g., Cyclosporin G,
6-methyl-ala-CsA, and
4-methyl-val-CsA)
SfA (inhibits PPIase activity
of CyP-D but not binding)
Effect via change in nucleotide
binding to the ANTa
Direct effect on Ca2 +
binding to the ANT
Unknown mode of action
Thiol reagents attacking Cys159
of ANT (e.g., eosine maleimide)
High pH
Some ubiquinone analogues
(e.g., decyl-ubiquinone,
ubiquinone 10)
Increase membrane potential
Low pH
‘‘m’’ Conformation of ANT
as induced by bongkrekic acid
Mg2 +, Mn2 +,
Sr2 +, Ba2 +
Some ubiquinone analogues
(e.g., ubiquinone 0,
2,5-dihydroxy-6-undecyl-1,
4-benzoquinone)
Trifluoperazine (may work
via membrane surface charge)
Oxidative stress (e.g., reperfusion,
t-butyl hydroperoxide, or diamide)
or thiol reagents (e.g., phenylarsine
oxide and eosine maleimide) that
modify Cys159 of the ANT
‘‘c’’ Conformation of ANT as
induced by carboxyatractyloside
Adenine nucleotide depletion
High matrix [Pi] and [PPi]
Depolarisation
Further details may be found in the text and in Refs. [3 – 5].
a
Note that both CyP-D binding and ADP binding exert their effects through changes in the sensitivity of the MPT to [Ca2 +].
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
analogues can act either as potent activators or inhibitors of
the MPTP perhaps by interacting with Complex 1 of the
respiratory chain, although how this might regulate the
MPTP remains uncertain [9].
3. The mitochondrial permeability transition pore opens
during reperfusion but not ischaemia
3.1. The conditions prevailing during ischaemia and
reperfusion favour pore opening
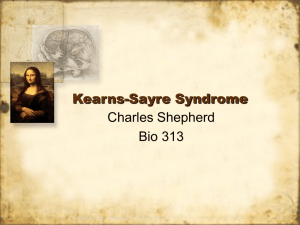
As reviewed elsewhere [4] and summarised in Fig. 2, the
conditions that occur during reperfusion are exactly those
that induce MPTP opening. In outline, the increase in
glycolysis that occurs during myocardial ischaemia causes
a progressive accumulation of lactic acid and drop in pHi
that will eventually inhibit further glycolytic flux and ATP
production. Activation of the Na+/H+ antiporter occurs as
the cell attempts to restore the pHi,, but in the process, it
becomes loaded with sodium, which cannot be pumped out
of the cell because the Na/K ATPase is inhibited by the lack
of ATP. Consequently, the activity of the Na+/Ca2 + antiporter, which usually pumps Ca2 + out of the cell, is reduced
or reversed and the cell becomes loaded with calcium. At
this point, ionic homeostasis can no longer be maintained,
intracellular [Na+] and [Ca2 +] begin to rise, and contracture
follows (reviewed in Ref. [10]). In addition, adenine nucleotides are degraded during ischaemia and the resulting
decrease in adenine nucleotide concentration, in conjunction
375
with the increased phosphate concentrations, will sensitise
MPTP opening to [Ca2 +] as outlined above. However,
because the pHi remains low, the MPTP will not actually
open, although if the period of ischaemia is sufficiently
prolonged, the heart will become irreversibly damaged
through the action of degradative enzymes such as phospholipases and proteases, which themselves will compromise mitochondrial function.
In order to salvage the ischaemic heart, it must be
reperfused, yet the very process of reperfusion may exacerbate the damage induced by ischaemia itself, as reflected
in changes in cell morphology typical of necrosis and the
release of intracellular enzymes. Another feature is the
appearance of swollen dysfunctional mitochondria that are
typical of those that have undergone the permeability
transition, and there are good theoretical reasons why this
should happen. Upon reperfusion, the mitochondria are
once again able to respire and generate a membrane
potential to drive ATP synthesis, but this also enables the
rapid accumulation of calcium within the mitochondria,
leading to calcium overload (see Ref. [10]). In addition,
there is a rapid and extensive production of reactive oxygen
species (ROS) as the inhibited respiratory chain is reexposed to oxygen. Conditions are now almost optimal for
MPTP formation since there is high intramitochondrial
[Ca2 +] and phosphate, oxidative stress, and depleted adenine nucleotide concentrations. The one restraining influence is the low pH i , but within a few minutes of
reperfusion, this returns to normal values and all restraints
on MPTP opening are removed.
Fig. 2. Factors leading to opening of the MPTP in reperfusion. Further details are given in the text.
376
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
3.2. Experimental demonstration that the MPTP opens
during reperfusion
In order to demonstrate directly that the MPTP only opens
during reperfusion and not during ischaemia, three distinct
approaches have been taken. First, fluorescence microscopy
of isolated cardiac myocytes subjected to simulated ischaemia and reperfusion has been used. In these studies, the
mitochondrial membrane potential was determined with
fluorescent dyes as a surrogate indicator of MPTP opening
[11]. Such dyes accumulate within the mitochondria in
response to the membrane potential and are released upon
depolarisation when the MPTP opens. Confirmation that any
depolarisation is caused by the opening of the MPTP is
usually provided by the ability of CsA, sometimes supplemented with trifluoperazine, to inhibit the process [12]. A
more sophisticated approach is to determine simultaneously
the distribution of another fluorescent dye, calcein (green
fluorescence), that can only cross the inner mitochondrial
membrane when the pore opens [13,14]. Although this
technique has been applied successfully to cardiac myocytes
subject to oxidative stress [15 – 17], the use of isolated cardiac
myocytes cannot accurately mimic the situation in the
ischaemic/reperfused heart.
Two techniques have been developed to determine the
extent of MPTP opening in the perfused heart. One, devised
by DiLisa et al. [18], is to determine the loss of mitochondrial
NAD+ that accompanies reperfusion as a surrogate indicator
of pore opening. Both mitochondrial and cytosolic NAD+ are
lost during reperfusion. The latter correlates with the extent of
lactate dehydrogenase release as might be predicted since this
reflects a breakdown of the plasma membrane permeability
barrier. The loss of NAD+ is inhibited by CsA, confirming
that it occurs as a result of MPTP opening, although it is
impossible to rule out that some of the CsA-sensitive pore
openings and disruption of mitochondria detected by this
technique actually occur during mitochondrial isolation rather than in situ [6,19]. Another approach, devised in this
laboratory, circumvents this potential problem by measuring
the mitochondrial entrapment of a radioactive marker, which
has been loaded into the cytosol of the heart.
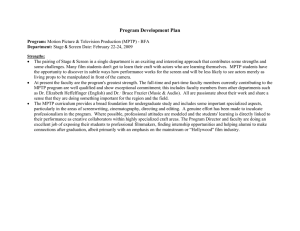
In this technique, illustrated in Fig. 3, Langendorffperfused hearts are first loaded with [3H]2-deoxyglucose
(3H-DOG), which accumulates within the cytosol as 3HDOG-6-phosphate (3H-DOG-P) but can only enter the
mitochondria when the MPTP opens [19]. The extent to
which the 3H-DOG-P enters the mitochondria can be
determined by their rapid isolation in the presence of
EGTA, which reseals the pores and so entraps the 3HDOG-P within the mitochondria. Measurement of the 3H
content of the mitochondria gives a quantitative value for
the extent of pore opening, provided that suitable controls
Fig. 3. The use of [3H]6-deoxyglucose to measure MPTP opening in the perfused heart.
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
and corrections are performed to account for variations in
the initial loading of the heart with 3H-DOG and the
recovery of intact mitochondria. The latter is determined
using citrate synthase and this measurement might also be a
useful refinement to the published NAD+ technique. As
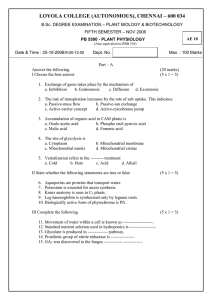
illustrated in Fig. 4, using the 3H-DOG entrapment technique, we have been able to confirm that the MPTP
remains closed during 30 min of ischaemia but opens upon
reoxygenation with a time course that reflects the return of
pHi from its ischaemic value of < 6.5 to preischaemic
values [19 – 21].
A potential advantage of the 3H-DOG entrapment technique over the NAD+ technique is that opening of the MPTP
during isolation will release any of the 3H-DOG-6P that
accumulated within the mitochondrial matrix as a result of
pore opening in situ. Thus, it should only detect mitochondria undergoing the permeability transition in situ rather
than during isolation. However, the DOG technique is not
without its own limitations. The most significant of these is
its inability to detect mitochondrial pore opening in cells
that have undergone extensive necrosis [22]. The permeability barrier posed by the plasma membrane of necrotic
tissues is compromised and mitochondrial integrity is totally
destroyed. Thus, all the 3H-DOG that might have been
entrapped in the cytosol and mitochondria will be lost
and not detected, leading to a major underestimate of pore
opening. Since the NAD+ technique relies on measuring
the loss of mitochondrial NAD+, it does not suffer this
disadvantage. However, the 3H-DOG technique does detect
cells that have not yet progressed to full necrosis but are
on their way and already exhibit compromised mitochondrial function through opening of the MPTP [22]. The
extent to which myocytes have already undergone necrosis
can be detected by classical techniques such as enzyme
release.
Fig. 4. Time dependence of MPTP opening during reperfusion. The
opening of the MPTP was detected using the DOG preloading technique.
Hearts were subjected to 30 min of global ischaemia before reperfusion for
the time shown. Data are taken from Ref. [21]. Parallel data for the pH of
the perfusate are taken from Ref. [22].
377
3.2.1. The MPTP can open transiently during reperfusion
with implications for apoptotic damage
Using the 3H-DOG entrapment technique, we were able
to demonstrate that some opening of the MPTP could be
detected during reperfusion after relatively short periods of
ischaemia (10 – 20 min) even though total recovery of LVDP
and ATP/ADP ratio was observed [19,20,23]. One explanation for this paradox would be that opening of the MPTP
was transient, and rapidly followed by resealing that would
enable total recovery of mitochondrial function and heart
performance. Unfortunately, if resealing of the MPTP does
occur, the entrapped 3H-DOG-P will remain within the
mitochondria and thus closure will not be detected. To
overcome this problem, hearts are loaded with 3H-DOG
after a period reperfusion to allow functional recovery. If
closure of pores does occur during reperfusion, mitochondrial 3H-DOG-P entrapment following postloading of 3HDOG should be less than with preloading. Using this
postloading technique, we demonstrated that 3H-DOG-P
entrapment was only about 50% of that seen with preloading, confirming that some pore closure had occurred.
Indeed, the extent of subsequent MPTP closure correlated
with the functional recovery of the heart [21]. Thus, it would
seem that if the insult caused by ischaemia/reperfusion is not
too great, mitochondria may undergo a transient permeability transition, followed by pore closure and entrapment of
the 3H-DOG-P. The closure probably occurs as a result of
the loss of matrix [Ca2 +] through the open pores and its
subsequent removal from the cytosol. However, this will
only occur if enough ‘‘healthy’’ mitochondria (without open
pores) remain in the cell to accumulate the Ca2 + released by
those with open pores. These healthy mitochondria will also
provide sufficient ATP to maintain the ionic homeostasis of
the cell. The balance between the number of ‘‘closed’’ and
‘‘open’’ mitochondria within any cell will be critical in
determining whether a cell lives or dies. If there are too
many ‘‘open’’ mitochondria, they will release more calcium
and hydrolyse more ATP than the ‘‘closed’’ mitochondria
can accommodate. In contrast, if there are sufficient
‘‘closed’’ mitochondria to meet the ATP requirements of
the cell and also to accumulate released calcium without
undergoing the permeability transition themselves, the
‘‘open’’ mitochondria will close again and the cell will
recover, at least in the short term.
However, transient pore opening may have longer-term
implications for the heart through inhibition of apoptosis
that are not apparent over the time scale of perfusion
experiments through the initiation of apoptosis. MPTP
opening is associated with mitochondrial swelling, outer
membrane rupture, and the release of proapoptotic factors
such as cytochrome c from the intermembrane space. Once
released, cytochrome c activates caspase 9, which in turn
activates caspase 3. This protease mediates the proteolytic
cleavage of a range of proteins responsible for the rearrangement of the cytoskeleton, plasma membrane, and
nucleus that are characteristic of apoptosis [24,25]. A major
378
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
Fig. 5. Scheme illustrating how the extent of MPTP opening and subsequent closure may determine whether cardiac myocytes die by necrosis, as in the centre
of an infarct, or apoptosis, as at the periphery. Further details may be found in the text.
distinction between apoptosis and necrosis is that the
former requires ATP whilst the latter occurs in its absence
[24,25]. Only if the MPTP opens sufficiently to cause
cytochrome c release but then closes again to ensure that
cellular ATP concentrations are maintained will the cell
undergo apoptosis. Too much MPTP opening and necrosis
will occur; too little opening and the cell recovers completely.
In this sense, the mitochondrion is acting as the judge and
executioner, the extent and duration of MPTP opening
determining whether or not the cell lives or dies and the
means by which it dies. It may be significant that the area
around the necrotic core of an infarct shows a ring of
apoptotic cell death [26,27]. Thus, in the core of the infarct,
all cells are necrotic, reflecting permanent MPTP opening and
mitochondrial disruption, whereas at the periphery, where
ischaemic insult is less severe, transient MPTP opening may
lead to apoptosis. This is illustrated in Fig. 5.
mediated either through direct inhibition of the pore with
agents such as CsA and SfA, or through an indirect effect
associated with a decrease in the factors responsible for
MPTP opening such as oxidative stress and mitochondrial
calcium overload. Recent data using H2O2-treated isolated
cardiac myocytes have suggested that a priming phase,
associated with mitochondrial swelling and cristae loss, but
not depolarisation, may precede MPTP opening and be a
target for myocardial protection [17]. The putative mitochondrial KATP channel opener, diazoxide (see Section 4.6), as
well as the ANT inhibitor BKA (see Section 4.2) have been
reported to inhibit this priming phase [28], although the
mechanisms involved remain obscure and are not easily
reconciled with recent data from this laboratory on the
mitochondrial matrix volume in the ischaemic heart and
reperfused heart [29].
4.1. Targeting CyP-D with Cyclosporin A and Sanglifehrin
A to inhibit the MPTP
4. The MPTP as a target for protecting hearts from
reperfusion injury
It would be predicted that if opening of the MPTP is a
critical factor in the transition from reversible to irreversible
reperfusion injury of the heart, inhibitors of pore opening
should offer protection. There is increasing evidence that
almost any procedure that reduces reperfusion injury is
associated with either a decrease in MPTP opening, or an
increase in subsequent pore closure. This effect may be
Nazareth et al. [30] were the first to demonstrate protection with CsA using an isolated cardiac myocyte model of
anoxia and reoxygenation, and, subsequently, this has been
confirmed by others [31,32]. Interestingly, in such cells, it
has been shown that there is a correlation between mitochondrial [Ca2 +] content and subsequent cell death [33,34].
In this laboratory, we were able to demonstrate protection by
CsA in the Langendorff-perfused heart model of reperfusion
injury [20,23] and, subsequently, by SfA [6,22]. Thus, as
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
Fig. 6. Protection of hearts from reperfusion injury by Cyclosporin A and
Sanglifehrin A. Note that 3H-DOG entrapment was measured using the
preloading protocol. Data are taken from Refs. [6,21] where further details
may be found.
illustrated in Fig. 6, in the presence of 0.2 AM CsA or SfA,
the recovery of haemodynamic function during reperfusion
was greatly improved, as reflected by higher left ventricular
developed pressure (LVDP) and lower end diastolic pressure
(EDP) (an indicator of contracture whose elevation reflects
elevated [Ca2 +]), whilst greatly reduced release of intracellular lactate dehydrogenase confirmed that there was less
necrotic cell damage. In addition, the CsA-treated hearts
exhibited higher ATP/ADP ratios and lower AMP levels [6].
More recently, it has been demonstrated that CsA can
significantly reduce infarct size in a coronary occlusion
379
model of reperfusion injury, even when added only at
reperfusion [35]. Taken together, these data strongly support
the direct inhibition of the MPTP by CsA and SfA as being
an effective means of inhibiting reperfusion injury. Thus, it
is somewhat surprising that in experiments in which these
agents produced significant functional protection of hearts
from reperfusion injury, the 3H-DOG technique showed
only a modest reduction in MPTP opening [22]. In contrast,
under similar conditions, the use of mitochondrial NAD+
content as an indicator of MPTP opening showed a greater
inhibitory effect of CsA [18]. However, DiLisa et al. did not
account for the presence of broken mitochondria in their
mitochondrial fraction. Since we have shown that CsA and
SfA significantly increase the recovery of citrate synthase in
the mitochondrial pellet, this may account for at least some
of the differences between the two techniques. Indeed, when
the better recovery of intact mitochondria from hearts
treated with CsA and SfA was accounted for using the
recovery of citrate synthase activity in the mitochondrial
fraction, these agents were found to give a 35– 50% decrease in 3H-DOG entrapment, more in line with the data
obtained with the NAD+ technique [22]. Another important
feature of the 3H-DOG entrapment technique is that it
measures only MPTP opening that occurs in situ, whereas,
as outlined above (Section 3.2), the mitochondrial NAD+
content may also reflect breakage of mitochondria as a result
of MPTP opening during their isolation, and this is thought
to be less in the CsA-treated hearts [6,19,22].
We have recently recognised another factor that contributes towards the lack of correlation between the protective
effects of CsA and SfA on the recovery of haemodynamic
function and MPTP opening measured with the 3H-DOG
entrapment technique [22]. A major limitation in the use of
CsA and SfA as inhibitors of the MPTP is that both agents
fail to inhibit pore opening when mitochondria are exposed
to a sufficiently strong stimulus [6,19]. The elevated matrix
calcium, oxidative stress, and adenine nucleotide depletion
that accompany reperfusion after a period of ischaemia
provide just such conditions [4,36]. However, as reperfusion
continues and intracellular [Ca2 +] and reactive oxygen
species decline again, SfA and CsA may be able to block
the MPTP totally, leading to better recovery of mitochondrial function than in control hearts. This is reflected in
improved haemodynamic function (LVDP and EDP) and
less necrotic damage (LDH release and reduced infarct size).
Without such protection, more cells will progress towards
necrosis, leading to the disruption of the plasma membrane,
loss of ionic homeostasis, and release of LDH and cytosolic
3
H-DOG-P. The resulting massive influx of calcium into
these cells will then cause all their mitochondria to undergo
the permeability transition and release their entrapped 3HDOG-P. Hence, totally necrotic cells will lose both cytosolic
and mitochondrial 3H-DOG-P, and so the presence of open
mitochondria in such cells will not be not detected [22].
This may explain why the postloading technique fails to
detect a decrease in pore opening with SfA and CsA [22]
380
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
despite the improvement in heart function and decrease in
LDH release [6,22]. It must also be recognised that factors
other than disruption of mitochondrial function may lead to
impaired haemodynamic function of the heart (stunning) in
otherwise healthy myocytes. Thus, regimes that decrease
stunning will cause an improvement in haemodynamic
function without a measurable decrease in pore opening.
4.1.1. Limitations in the use of CsA
It is important to note that in addition to the limitations
discussed above, there are two other major drawbacks to the
use of CsA. First, it can potentially exert additional undesirable effects on the heart through inhibition of calcineurinmediated processes [37]. This drawback can be overcome
by the use of CsA analogues that are without effect on
calcineurin such as [MeAla6]CsA and 4-methyl-val-CsA
and by SfA [6,18,19]. The second problem is that CsA is
only protective within a narrow concentration range, the
optimal concentration of CsA for protection being about 0.2
AM with protection, declining again at higher concentrations
[18,19,23]. This decline may partly reflect inhibition of
calcineurin-dependent processes in the heart, but may also
involve the emerging role of cyclophilins in the response of
cells to oxidative stress. Thus, Doyle et al. [38] used
antisense technology to knock out cytosolic cyclophilin
(CyP-A) in cardiac myocytes and demonstrated that these
cells were more sensitive to oxidative stress than control
myocytes, but exhibited greater protection by CsA. Furthermore, overexpression of CyP-D has been shown to increases
the resistance of cells to oxidative stress-induced cell
damage [39]. There is a paradox here in that CyP-D is a
component of the MPTP, and thus its overexpression might
be expected to exacerbate damage, rather than offer protection. However, CyP-A has been shown to bind to peroxiredoxin IV and activate its peroxidase activity that uses
thioredoxin to reduce H2O2 [40]. In addition, thioredoxin
binds specifically to a cyclophilin in chloroplasts similar to
CyP-D and reduces an intramolecular disulphide bond
formed on oxidative stress [41]. Thus, it seems likely that
CyP-D may play a dual role, protecting the mitochondria
from oxidative stress initially, but if the insult becomes
overwhelming, protection is reversed as the MPTP is
activated and cell death ensues.
4.2. Targeting the MPTP with bongkrekic acid and
ubiquinone derivatives
It is well established that BKA is a potent inhibitor of the
MPTP in isolated mitochondria (see Section 2.2) and there
are many reports of its use to inhibit pore opening in
cultured cells (see Refs. [3,5]) including cardiac myocytes
[15,28,42]. However, the primary action of BKA is to
inhibit the export of ATP from the mitochondria to the
cytosol and thus it is not appropriate for use in the heart,
which is dependent on oxidative phosphorylation and the
export of ATP from the mitochondria into the cytosol to
drive contraction. The same considerations apply when
using atractyloside to demonstrate a role for MPTP opening
in reperfusion injury and studies where this has been
attempted should be treated with caution [35,43,44]. Some
ubiquinone derivatives have been described as potent inhibitors of the MPTP [9], and we have investigated the action
of Coenzyme Q0 (2,3-dimethoxy-5-methyl-p-benzoquinone) on the Langendorff-perfused heart (Samantha Clarke,
unpublished data). Unfortunately, we found that at 50 AM,
the concentration reported to give maximal inhibition of the
MPTP [9], this compound caused the heart to stop beating
almost immediately. Even at 10 AM, a concentration that has
relatively little effect on the MPTP, the performance of the
heart was impaired, especially following ischaemia and
reperfusion.
4.3. Na+/H+ antiporter inhibitors may target the MPTP by
reducing calcium load and maintaining low intracellular
pH during reperfusion
A potent inhibitor of MPTP opening is low pH (see
Section 2.2), and several groups have demonstrated that
maintaining an acidic extracellular pH during reoxygenation
after a period of anoxia can protect cells from damage (see
Ref. [45]). This is consistent with the observation that the
MPTP opens during reperfusion only after the low pHi of
ischaemia is restored to normal [21]. In contrast, acid pH
during the ischaemic phase is detrimental, probably because
Na+/H+ exchange is stimulated, loading the heart with Na+
and Ca2 +. Inhibitors of the Na+/H+ exchanger such as
amiloride and cariporide are thought to protect hearts from
reperfusion injury by reducing the accumulation of Na+ and
Ca2 + during the ischaemic phase (see Refs. [46,47]). However, there may be an additional effect during reperfusion
associated with a slower return of pHi to normal physiological values (see Refs. [48,49]). Either mechanism would
ultimately inhibit the opening of the MPTP. However, in
preliminary experiments using the 3H-DOG entrapment
technique, we have been unable to demonstrate any inhibition of MPTP opening during reperfusion by either amiloride or cariporide added prior to and during ischaemia and
reperfusion (Samantha Clarke, unpublished data). Nevertheless, both agents did give protection under these conditions
whether measured by haemodynamic function or lactate
dehydrogenase release. As noted for CsA and SfA (Section
4.1), this does not rule out the inhibition of MPTP opening,
but rather may indicate that the major effect is seen in the
number of cells undergoing necrosis that are not detected by
the 3H-DOG technique.
4.4. Targeting the MPTP with free radical scavengers
including pyruvate and propofol
Reducing oxidative stress through the use of free radical
scavengers is known to offer some protection against
reperfusion injury [50]. Such agents may directly inhibit
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
the opening of the MPTP by preventing oxidative crosslinking of critical cysteines on the ANT (see Ref. [5]).
However, there may also be indirect effects on MPTP
opening since oxidative stress is known to inhibit plasma
membrane ion pumps, leading to perturbation of ionic
homeostasis and calcium overload [51]. We have investigated the effects of two free radical scavengers on MPTP
opening, pyruvate [21] and the anaesthetic propofol [52],
and, in both cases, we have shown that their cardioprotective effects are associated with diminished opening of the
MPTP.
4.4.1. Pyruvate
The ability of pyruvate to protect hearts and other tissues
against ischaemia/reperfusion anoxia/reoxygenation injury
has been known for many years and may, in part, be
mediated by its free radical scavenging activity [21,53,54].
In addition, pyruvate is a superior fuel for the heart during
reperfusion because, unlike glucose or glycogen, it does not
require ATP for activation before it can be metabolised. We
have confirmed that 10 mM pyruvate added before ischaemia and maintained during reperfusion greatly improves the
functional recovery of hearts, and that this is associated
with a major reduction in MPTP opening during the initial
stages of reperfusion. Furthermore, postloading experiments demonstrated that as reperfusion continued, almost
all the ‘‘open’’ mitochondria subsequently resealed [21].
These data provide further evidence that once opened, the
MPTP can close again and allow hearts to recover fully
during reperfusion, provided the initial insult is not too
great. During the course of these experiments, it became
apparent that pyruvate also caused a greater accumulation
of intracellular lactic acid during ischaemia and slowed the
return of pHi during reperfusion to normal values from the
low values of ischaemia [21]. There is also direct evidence
from nuclear magnetic resonance (NMR) studies that pyruvate causes a decrease in pHi in a low-flow model of
ischaemia [55]. In view of the inhibitory effect of low pH
on the MPTP, this might provide yet another mechanism by
which pyruvate can protect the heart against reperfusion
injury.
4.4.2. Propofol
The anaesthetic propofol is frequently used during
cardiac surgery and in postoperative sedation [56]. It acts
as a free radical scavenger and may also inhibit plasma
membrane calcium channels (see Ref. [52]). In addition, at
concentrations higher than used clinically, propofol may
inhibit the MPTP directly [57]. Propofol has been shown
by others to protect the Langendorff-perfused heart against
reperfusion injury [58] and damage caused by H2O2-induced oxidative stress [59]. We have used the 3H-DOG
technique to confirm that this protection is accompanied by
less opening of the MPTP in situ [52]. Furthermore,
mitochondria isolated from the propofol-treated hearts
exhibited less pore opening than control mitochondria
381
exposed to the same [Ca2 +]. However, when propofol
was added to isolated heart mitochondria at the same
concentration as used in the heart perfusion (2 Ag/ml, a
concentration typically used in clinical anaesthesia), no
inhibition of MPTP opening was observed [52], suggesting
that that the protective effect of propofol may be secondary
to the decreased oxidative stress and calcium overload. We
have also demonstrated a cardioprotective effect of propofol on the functional recovery of the working rat heart
following cold cardioplegic ischaemic arrest, a model that
is closer to the situation experienced in open heart surgery
[52]. Most recently, we have extended these studies to an in
vivo pig model of cardiopulmonary bypass with warm
blood cardioplegia that closely matches current clinical
practice. Here, too, normal clinical concentrations of propofol improve functional recovery of the heart, reduce
troponin I release, and maintain higher tissue ATP levels
[60].
Whatever the exact mechanisms involved, both pyruvate
and propofol provide examples of reagents whose protection
of the heart from reperfusion injury is accompanied by a
decrease in MPTP opening in vivo. These data suggest that
propofol and pyruvate may be a useful adjunct to the
cardioplegic solutions used in cardiac surgery.
4.5. Elevated extracellular [Mg2+] may protect hearts by
inhibiting the MPTP
Magnesium is well known to protect hearts from ischaemia and reperfusion injury and seems most effective when
present at high concentrations (>8 mM) during the reperfusion phase [61 – 63]. The available evidence suggests that
the protective effect involves extracellular Mg2 +, since
intracellular [Mg2 +] increases very little even at greatly
increased [Mg2 +] in the perfusion medium [62,64]. It is
generally accepted that it exerts its protective effects by
inhibiting L-type calcium channels and the Na+/Ca2 + antiporter, thus decreasing calcium overload [61,62]. Indeed,
other inhibitors of plasma membrane or mitochondrial
calcium channels such as verapamil and ruthenium red
derivatives have been shown to protect hearts from reperfusion injury in this manner (see Ref. [4]). There are also data
to suggest that the presence of supraphysiological [Mg2 +]
prior to ischaemia exerts an antioxidant effect during reperfusion [63]. Taken together, these data would suggest that
protection afforded by elevated [Mg2 +] may also involve
the inhibition of MPTP opening.
4.6. Protection by ischaemic preconditioning involves
inhibition of MPTP opening
One of the most effective ways to protect the heart
against reperfusion injury is to subject them to brief ischaemic periods with intervening recovery periods before the
prolonged period of ischaemia is initiated. Such ‘‘ischaemic
preconditioning’’ is associated with two phases of protec-
382
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
tion: an immediate effect and a ‘‘second window’’ that
occurs 24 –48 h later [65]. The exact mechanisms involved
in preconditioning are still being debated, but several
processes have been implicated. The longer-term effects
are probably caused by stimulation of the transcription of
specific genes, perhaps through a mechanism activated by
free radicals and stress-activated protein kinases. Of particular interest may be the up-regulation of heat shock proteins
since recent data have shown that heat shock specifically
up-regulates the expression of liver mitochondrial Hsp25
and this is associated with desensitisation of MPTP opening
to Ca2 + and HgCl2 in isolated mitochondria [66]. It is also
known that heart mitochondria from mice in which Hsp25 is
down-regulated are more sensitive to MPTP opening and
also exhibit hallmarks of oxidative stress including oxidatively damaged ANT [67]. The mechanisms responsible for
the short-term effects of preconditioning include the activation of protein kinase C (PKC). This may be mediated either
by reactive oxygen species released during the short intervening reperfusion periods, or by factors released during the
brief ischaemic periods such as adenosine, bradykinin,
noradrenaline, and opioids. Thus, PKC inhibitors and free
radical scavengers antagonise IPC, whilst adenosine agonists and PKC activators mimic the effect (see Refs.
[65,68,69]). The ultimate target of these kinases is unknown, although it may be significant that activation of
PKCq and its translocation to mitochondria has been
reported to be important for preconditioning [70,71]. There
is also evidence for an involvement of sulphonylureasensitive KATP channels, since KATP channel openers such
as diazoxide can mimic IPC whilst blockers such as glibencamide inhibit [72,73]. Furthermore, PKC-dependent
activation of plasma membrane KATP channels by IPC has
been demonstrated [74].
As we have noted previously [2], if the extent of MPTP
opening is a critical factor in determining the extent of
reperfusion injury, it would be predicted that IPC should
reduce the amount of pore opening. Indirect evidence
obtained using isolated cardiac myocytes and mitochondria
has implicated the inhibition of the MPTP in both calciumand diazoxide-mediated preconditioning [32,35,75]. We
have recently used the 3H-DOG technique to demonstrate
directly that IPC inhibits the MPTP in the Langendorffperfused heart [22]. IPC not only reduced the opening of the
MPTP during the early phase of reperfusion (measured with
3
H-DOG preloading) but also increased subsequent pore
closure (measured with 3H-DOG postloading) as illustrated
in Fig. 7. However, MPTP opening in isolated mitochondria
from preconditioned hearts showed a greater sensitivity
towards calcium than mitochondria from control hearts
[22], implying that the inhibition of MPTP opening in situ
by IPC is probably indirect. It may well be mediated either
through a decrease in calcium loading of the cardiac
myocyte or a decreased production of ROS upon reperfusion, both of which are observed in response to ischaemic
and diazoxide-mediated preconditioning (see Ref. [22] for
Fig. 7. Protection of hearts from reperfusion injury by ischaemic
preconditioning is accompanied by decreased MPTP opening. Two 5-min
ischaemic periods with intervening recovery were used for preconditioning
before 30 min of global isothermic ischaemia and then reperfusion.
Mitochondrial 3H-DOG entrapment was measured in nonischaemic hearts
and following reperfusion using both the preloading and postloading
protocols as indicated. Error bars represent the S.E. for eight observations.
Data are taken from Ref. [22] where further details may be found.
detailed references). Indeed, our own data suggest that such
an indirect mechanism of inhibiting the MPTP may be more
effective at protecting hearts from reperfusion injury rather
than targeting the MPTP directly with CsA or SfA [22]. This
may reflect the inability of CsA and SfA to inhibit the
MPTP when matrix calcium concentrations and oxidative
stress are high as may occur in the initial phase of reperfusion [19,76].
In contrast to our own data suggesting that IPC exerts its
effects on the MPTP indirectly, Baines et al. [44] have very
recently provided evidence that PKCq may interact directly
with VDAC to cause its phosphorylation and consequent
inhibition of MPTP opening. However, there are aspects of
this study which need clarification, especially the quantification of the inhibition of MPTP opening in isolated
mitochondria and the ability of added PKCq to cause
inhibition in the absence of added ATP. Furthermore, the
in vitro phosphorylation of VDAC was performed using a
glutathione-S-transferase fusion protein in free solution and
without either detergent or added phospholipids. Under
these conditions, the conformation state of VDAC, which
is normally embedded in the outer membrane, may well be
far removed from its native state.
4.6.1. Mitochondrial KATP channels and ischaemic
preconditioning
It was originally proposed that the opening of the
plasma membrane KATP channel might hyperpolarize the
cell and lead to a shorter action potential duration (APD)
and calcium loading. However, data obtained with a range
of KATP channel openers showed a poor correlation between their effect on APD and their protective effects and,
in recent years, the emphasis has shifted towards a role for
the putative mitochondrial KATP channel in IPC [72,77].
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
One reason for this is that diazoxide protects hearts at
concentrations much lower than reported to open the
plasma membrane KATP channel, but similar to values
reported for the mitochondrial KATP channel. Furthermore,
protection was inhibited by 5-hydroxydecanoate (5-HD), an
agent reported to be a specific inhibitor of the mitochondrial KATP channel (but see below). However, on several
counts, these data are not totally convincing. First, there are
reports that diazoxide can work at much lower concentrations on the plasma membrane KATP channel when ADP
is present (as it will be in the cell) [78]. Second, the
opening of a mitochondrial K+ channel would depolarize
mitochondria (inhibiting oxidative phosphorylation) and
induce K+ cycling (effectively increasing ATP demand).
Yet published data suggest the opposite to be the case [79]
as might be predicted for a protective agent. Third, recent
reports have shown that in knockout mice lacking the
plasma membrane potassium channel Kir6.2, neither IPC
nor diazoxide was able to offer protection from reperfusion
injury [80,81]. Fourth, diazoxide has been shown by
several workers to inhibit succinate dehydrogenase activity
and hence respiration supported by the citric acid cycle
[29,82 –84]. This inhibition of respiration might be responsible for the increased mitochondrial production of ROS
observed with diazoxide treatment [85 –87], with the ROS
then mediating IPC [68,88]. Fifth, 5-HD cannot be used as
a specific mitochondrial KATP channel inhibitor since it is a
racemic mix of D-isoforms and L-isoforms of a substituted
fatty acid that can be activated to its coenzyme A derivative
and then act as either a substrate or inhibitor of fatty acid hoxidation [29,83,89,90]. Sixth, in isolated heart mitochondria incubated under conditions that mimic the in vivo
situation, we have been unable to demonstrate any effect of
diazoxide, 5-HD, glibencamide, and a range of other
putative mitochondrial KATP channel openers or blockers
on light scattering or isotopic measurements of matrix
volume [84].
These considerations have led us to question whether
such mitochondrial KATP channels have any significance in
regulating heart mitochondrial function [84]. That is not to
say that mitochondrial potassium channels may not play an
important role in regulating mitochondrial function under
some conditions. Indeed, we have provided extensive evidence that there is a calcium-activated potassium channel in
liver mitochondria that is involved in mediating the increase
in matrix volume occurring in response to hormones such as
glucagon and adrenaline. This plays an important role in the
stimulation of the respiratory chain by these hormones [91].
Furthermore, we have shown that IPC and ischaemia itself
can increase the matrix volume of heart mitochondria in
situ, leading to a stimulation of respiratory chain activity
that may represent an important adaptation to maintain rates
of respiration during hypoxia [29]. However, this effect is
not prevented by 5-HD, again implying that the proposed
mitochondrial KATP channel is not involved. Others have
very recently provided evidence for such a calcium-activate
383
K+ channel in heart mitochondria that is distinct from the
KATP channel [92].
5. Conclusions
The opening of the MPTP converts the mitochondrion
from an organelle that provides ATP to sustain heart
function into an instrument of cell death by apoptosis if
the insult is mild, to necrosis if the insult is profound.
Whatever the final pathway of cell death, pharmacological
interventions that can inhibit MPTP opening and enhance
pore closure, either directly (CsA and SfA) or indirectly
(propofol, pyruvate, and preconditioning protocols), provide
protection from reperfusion injury. In cardiac surgery, pharmacological agents can be administered prior to ischaemia,
enabling them to exert their effects on mitochondria prior to
ischaemia and reperfusion. However, in restoring flow to a
blocked coronary artery, either with clot-busting enzymes or
angioplasty, it will be more difficult to ensure that the drug
is in place in the critical early stage of reperfusion. In a rat
coronary ligation model, there is evidence that CsA can act
when added at reperfusion that is promising [35], but the
nonspecific effects of CsA and its narrow therapeutic
window (see Section 4.1.1) represent a severe limitation.
A major goal is the development of novel, specific, and
potent inhibitors of the MPTP that can enter the heart
rapidly and hopefully reach the ischaemic area from the
collateral circulation.
Acknowledgements
This work was supported by project grants from the
British Heart Foundation to A.P.H. and an International
Exchange Fellowship from the Royal Society to S.A.J.
References
[1] Crompton M. The mitochondrial permeability transition pore and its
role in cell death. Biochem J 1999;341:233 – 49.
[2] Halestrap AP. The Mitochondrial Permeability Transition: its molecular mechanism and role in reperfusion injury. In: Brown GC, Nicholls DG, Cooper CE, editors. Mitochondria and cell death. Biochemical Society Symposia, vol. 66. London: Portland Press; 1999.
p. 181 – 203.
[3] Halestrap AP, McStay GP, Clarke SJ. The permeability transition pore
complex: another view. Biochimie 2002;84:153 – 66.
[4] Halestrap AP, Kerr PM, Javadov S, Woodfield KY. Elucidating the
molecular mechanism of the permeability transition pore and its role
in reperfusion injury of the heart. Biochim Biophys Acta 1998;1366:
79 – 94.
[5] Halestrap AP, Brenner C. The Adenine Nucleotide Translocase: a
central component of the mitochondrial permeability transition pore
and key player in cell death. Curr Med Chem 2003;10:1507 – 25.
[6] Clarke SJ, McStay GP, Halestrap AP. Sanglifehrin A acts as a potent
inhibitor of the mitochondrial permeability transition and reperfusion
injury of the heart by binding to cyclophilin-D at a different site from
Cyclosporin A. J Biol Chem 2002;277:34793 – 9.
384
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
[7] Halestrap AP, Doran E, Gillespie JP, O’Toole A. Mitochondria and
cell death. Biochem Soc Trans 2000;28:170 – 7.
[8] Brustovetsky N, Tropschug M, Heimpel S, Heidkamper D, Klingenberg M. A large Ca2 +-dependent channel formed by recombinant
ADP/ATP carrier from Neurospora crassa resembles the mitochondrial permeability transition pore. Biochemistry 2002;41:11804 – 11.
[9] Walter L, Nogueira V, Leverve X, Heitz MP, Bernardi P, Fontaine E.
Three classes of ubiquinone analogs regulate the mitochondrial permeability transition pore through a common site. J Biol Chem 2000;
275:29521 – 7.
[10] Silverman HS, Stern MD. Ionic basis of ischaemic cardiac injury:
insights from cellular studies. Cardiovasc Res 1994;28:581 – 97.
[11] Duchen MR, McGuinness O, Brown LA, Crompton M. On the involvement of a Cyclosporin-A sensitive mitochondrial pore in myocardial reperfusion injury. Cardiovasc Res 1993;27:1790 – 4.
[12] Lemasters JJ, Nieminen AL, Qian T, Trost LC, Herman B. The mitochondrial permeability transition in toxic, hypoxic and reperfusion
injury. Mol Cell Biochem 1997;174:159 – 65.
[13] Lemasters JJ, Trollinger DR, Qian T, Cascio WE, Ohata H. Confocal
imaging of Ca2 +, pH, electrical potential, and membrane permeability
in single living cells. Methods Enzymol 1999;302:341 – 58.
[14] Bernardi P, Scorrano L, Colonna R, Petronilli V, DiLisa F. Mitochondria and cell death—mechanistic aspects and methodological issues.
Eur J Biochem 1999;264:687 – 701.
[15] Zorov DB, Filburn CR, Klotz LO, Zweier JL, Sollott SJ. Reactive
oxygen species (ROS)-induced ROS release: a new phenomenon accompanying induction of the mitochondrial permeability transition in
cardiac myocytes. J Exp Med 2000;192:1001 – 114.
[16] Katoh H, Nishigaki N, Hayashi H. Diazoxide opens the mitochondrial
permeability transition pore and alters Ca2 + transients in rat ventricular myocytes. Circulation 2002;105:2666 – 71.
[17] Akao M, O’Rourke B, Teshima Y, Seharaseyon J, Marban E. Mechanistically distinct steps in the mitochondrial death pathway triggered
by oxidative stress in cardiac myocytes. Circ Res 2003;92:186 – 94.
[18] DiLisa F, Menabo R, Canton M, Barile M, Bernardi P. Opening of the
mitochondrial permeability transition pore causes depletion of mitochondrial and cytosolic NAD(+) and is a causative event in the death
of myocytes in postischemic reperfusion of the heart. J Biol Chem
2001;276:2571 – 5.
[19] Griffiths EJ, Halestrap AP. Mitochondrial non-specific pores remain
closed during cardiac ischaemia, but open upon reperfusion. Biochem
J 1995;307:93 – 8.
[20] Halestrap AP, Connern CP, Griffiths EJ, Kerr PM. Cyclosporin A
binding to mitochondrial cyclophilin inhibits the permeability transition pore and protects hearts from ischaemia/reperfusion injury. Mol
Cell Biochem 1997;174:167 – 72.
[21] Kerr PM, Suleiman MS, Halestrap AP. Reversal of permeability transition during recovery of hearts from ischemia and its enhancement by
pyruvate. Am J Physiol 1999;276:H496 – 502.
[22] Javadov SJ, Clarke SJ, Das M, Griffiths EJ, Lim KHH, Halestrap AP.
Ischaemic preconditioning inhibits opening of the mitochondrial permeability transition pore in situ via an indirect mechanism. J Physiol
(Lond) 2003;549:513 – 24.
[23] Griffiths EJ, Halestrap AP. Protection by Cyclosporin A of ischemia
reperfusion-induced damage in isolated rat hearts. J Mol Cell Cardiol
1993;25:1461 – 9.
[24] Martinou JC, Green DR. Breaking the mitochondrial barrier. Nat Rev,
Mol Cell Biol 2001;2:63 – 7.
[25] Zimmermann KC, Green DR. How cells die: apoptosis pathways.
J Allergy Clin Immunol 2001;108:S99 – 103.
[26] Fliss H, Gattinger D. Apoptosis in ischemic and reperfused rat myocardium. Circ Res 1996;79:949 – 56.
[27] Anversa P, Cheng W, Liu Y, Leri A, Redaelli G, Kajstura J. Apoptosis
and myocardial infarction. Basic Res Cardiol 1998;93:8 – 12.
[28] Akao M, O’Rourke B, Kusuoka H, Teshima Y, Jones SP, Marban E.
Differential actions of cardioprotective agents on the mitochondrial
death pathway. Circ Res 2003;92:195 – 202.
[29] Lim KHH, Javadov SA, Das M, Clarke SJ, Suleiman MS, Halestrap
AP. The effects of ischaemic preconditioning, diazoxide and 5-hydroxydecanoate on rat heart mitochondrial volume and respiration.
J Physiol (Lond) 2002;545:961 – 74.
[30] Nazareth W, Yafei N, Crompton M. Inhibition of anoxia-induced
injury in heart myocytes by Cyclosporin-A. J Mol Cell Cardiol 1991;
23:1351 – 4.
[31] Griffiths EJ, Ocampo CJ, Savage JS, Stern MD, Silverman HS. Protective effects of low and high doses of Cyclosporin A against reoxygenation injury in isolated rat cardiomyocytes are associated with
differential effects on mitochondrial calcium levels. Cell Calcium
2000;27:87 – 95.
[32] Xu MF, Wang YG, Hirai K, Ayub A, Ashraf A. Calcium preconditioning inhibits mitochondrial permeability transition and apoptosis.
Am J Physiol 2001;280:H899 – 908.
[33] Miyata H, Lakatta EG, Stern MD, Silverman HS. Relation of mitochondrial and cytosolic free calcium to cardiac myocyte recovery after
exposure to anoxia. Circ Res 1992;71:605 – 13.
[34] Griffiths EJ, Ocampo CJ, Savage JS, et al. Mitochondrial calcium
transporting pathways during hypoxia and reoxygenation in single
rat cardiomyocytes. Cardiovasc Res 1998;39:423 – 33.
[35] Hausenloy DJ, Maddock HL, Baxter GF, Yellon DM. Inhibiting mitochondrial permeability transition pore opening: a new paradigm for
myocardial preconditioning? Cardiovasc Res 2002;55:534 – 43.
[36] Suleiman MS, Halestrap AP, Griffiths EJ. Mitochondria: a target for
myocardial protection. Pharmacol Ther 2001;89:29 – 46.
[37] Periasamy M. Calcineurin and the heartbeat, an evolving story. J Mol
Cell Cardiol 2002;34:259 – 62.
[38] Doyle V, Virji S, Crompton M. Evidence that cyclophilin-A protects
cells against oxidative stress. Biochem J 1999;341:127 – 32.
[39] Lin DT, Lechleiter JD. Mitochondrial targeted cyclophilin D protects
cells from cell death by peptidyl prolyl isomerization. J Biol Chem
2002;277:31134 – 41.
[40] Lee SP, Hwang YS, Kim YJ, et al. Cyclophilin A binds to peroxiredoxins and activates its peroxidase activity. J Biol Chem 2001;276:
29826 – 32.
[41] Motohashi K, Kondoh A, Stumpp MT, Hisabori T. Comprehensive
survey of proteins targeted by chloroplast thioredoxin. Proc Natl Acad
Sci U S A 2001;98:11224 – 9.
[42] Murata M, Akao M, O’Rourke B, Marban E. Mitochondrial ATPsensitive potassium channels attenuate matrix Ca2 + overload during
simulated ischemia and reperfusion—possible mechanism of cardioprotection. Circ Res 2001;89:891 – 8.
[43] Xu MF, Wang YG, Ayub A, Ashraf M. Mitochondrial K-ATP channel
activation reduces anoxic injury by restoring mitochondrial membrane
potential. Am J Physiol 2001;281:H1295 – 303.
[44] Baines CP, Song CX, Zheng YT, et al. Protein kinase C epsilon
interacts with and inhibits the permeability transition pore in cardiac
mitochondria. Circ Res 2003;92:873 – 80.
[45] Lemasters JJ. The mitochondrial permeability transition and the calcium, oxygen and pH paradoxes: one paradox after another. Cardiovasc Res 1999;44:470 – 3.
[46] Karmazyn M, Sostaric JV, Gan XT. The myocardial Na+/H+
exchanger—a potential therapeutic target for the prevention of myocardial ischaemic and reperfusion injury and attenuation of postinfarction heart failure. Drugs 2001;61:375 – 89.
[47] Avkiran M, Gross G, Karmazyn M, Klein H, Murphy E, Ytrehus K.
Na+/H+ exchange in ischemia, reperfusion and preconditioning. Cardiovasc Res 2001;50:162 – 3.
[48] Vandenberg JI, Metcalfe JC, Grace AA. Mechanisms of intracellular
pH recovery following global ischaemia in the perfused heart. Circ
Res 1993;72:993 – 1003.
[49] Allen DG, Xiao XH. Role of the cardiac Na(+)/H(+) exchanger
during ischemia and reperfusion. Cardiovasc Res 2003;57:934 – 41.
[50] Dhalla NS, Elmoselhi AB, Hata T, Makino N. Status of myocardial
antioxidants in ischemia – reperfusion injury. Cardiovasc Res 2000;
47:446 – 56.
A.P. Halestrap et al. / Cardiovascular Research 61 (2004) 372–385
[51] Fuller W, Parmar V, Eaton P, Bell JR, Shattock MJ. Cardiac ischemia
causes inhibition of the Na/K ATPase by a labile cytosolic compound
whose production is linked to oxidant stress. Cardiovasc Res 2003;
57:1044 – 51.
[52] Javadov SA, Lim KHH, Kerr PM, Suleiman MS, Angelini GD, Halestrap AP. Protection of hearts from reperfusion injury by propofol is
associated with inhibition of the mitochondrial permeability transition. Cardiovasc Res 2000;45:360 – 9.
[53] Deboer LWV, Bekx PA, Han LH, Steinke L. Pyruvate enhances recovery of rat hearts after ischemia and reperfusion by preventing free
radical generation. Am J Physiol 1993;265:H1571 – 6.
[54] Mallet RT. Pyruvate: metabolic protector of cardiac performance. Proc
Soc Exp Biol Med 2000;223:136 – 48.
[55] Cross HR, Clarke K, Opie LH, Radda GK. Is lactate-induced myocardial ischaemic injury mediated by decreased pH or increased intracellular lactate? J Mol Cell Cardiol 1995;27:1369 – 81.
[56] Bryson HM, Fulton BR, Faulds D. Propofol—an update of its use in
anesthesia and conscious sedation. Drugs 1995;50:513 – 59.
[57] Sztark F, Ichas F, Ouhabi R, Dabadie P, Mazat JP. Effects of the
anaesthetic propofol on the calcium-induced permeability transition
of rat heart mitochondria: direct pore inhibition and shift of the gating
potential. FEBS Lett 1995;368:101 – 4.
[58] Kokita N, Hara A, Abiko Y, Arakawa J, Hashizume H, Namiki A.
Propofol improves functional and metabolic recovery in ischemic
reperfused isolated rat hearts. Anesth Analg 1998;86:252 – 8.
[59] Kokita N, Hara A. Propofol attenuates hydrogen-peroxide induced
mechanical and metabolic derangements in the isolated rat heart.
Anesthesiology 1996;84:117 – 27.
[60] Lim KHH, Modi P, Nicholson E, et al. A pig model of warm-blood
cardioplegic arrest to investigate the cardioprotective effects of propofol. J Physiol 2001;536P:82P.
[61] Suleiman MS. New concepts in the cardioprotective action of magnesium and taurine during the calcium paradox and ischaemia of the
heart. Magnes Res 1994;7:295 – 312.
[62] Lareau S, Boyle AJ, Stewart LC, et al. The role of magnesium in
myocardial preservation. Magnes Res 1995;8:85 – 97.
[63] Maulik M, Maulik SK, Kumari R. Importance of timing of magnesium administration: a study on the isolated ischemic – reperfused rat
heart. Magnes Res 1999;2:37 – 42.
[64] Headrick JP, McKirdy JC, Willis RJ. Functional and metabolic effects
of extracellular magnesium in normoxic and ischemic myocardium.
Am J Physiol 1998;275:H917 – 29.
[65] Schulz R, Cohen MV, Behrends M, Downey JM, Heusch G. Signal
transduction of ischemic preconditioning. Cardiovasc Res 2001;52:
181 – 98.
[66] He L, Lemasters JJ. Heat shock suppresses the permeability transition
in rat liver mitochondria. J Biol Chem 2003;278:16755 – 60.
[67] Yan LJ, Christians ES, Liu L, Xiao X, Sohal RS, Benjamin IJ. Mouse
heat shock transcription factor 1 deficiency alters cardiac redox homeostasis and increases mitochondrial oxidative damage. EMBO J
2002;21:5164 – 72.
[68] VandenHoek TL, Becker LB, Shao ZH, Li CQ, Schumacker PT.
Reactive oxygen species released from mitochondria during brief hypoxia induce preconditioning in cardiomyocytes. J Biol Chem 1998;
273:18092 – 8.
[69] Fryer RM, Auchampach JA, Gross GJ. Therapeutic receptor targets of
ischemic preconditioning. Cardiovasc Res 2002;55:520 – 5.
[70] Fryer RM, Wang YG, Hsu AK, Gross GJ. Essential activation of
PKC-delta in opioid-initiated cardioprotection. Am J Physiol 2001;
280:H1346 – 53.
[71] Baines CP, Zhang J, Wang GW, et al. Mitochondrial PKC epsilon and
MAPK form signaling modules in the murine heart—enhanced mitochondrial PKC epsilon – MAPK interactions and differential MAPK
activation in PKC epsilon-induced cardioprotection. Circ Res 2002;
90:390 – 7.
[72] Oldenburg O, Cohen MV, Yellon DM, Downey JM. Mitochondrial K-
[73]
[74]
[75]
[76]
[77]
[78]
[79]
[80]
[81]
[82]
[83]
[84]
[85]
[86]
[87]
[88]
[89]
[90]
[91]
[92]
385
ATP channels: role in cardioprotection. Cardiovasc Res 2002;55:
429 – 37.
Peart JN, Gross GJ. Sarcolemmal and mitochondrial K(ATP) channels
and myocardial ischemic preconditioning. J Cell Mol Med 2002;6:
453 – 64.
Zhu Z, Li YL, Li DP, He RR. Effect of anoxic preconditioning on
ATP-sensitive potassium channels in guinea-pig ventricular myocytes.
Pflugers Arch 2000;439:808 – 13.
Korge P, Honda HM, Weiss JN. Protection of cardiac mitochondria by
diazoxide and protein kinase C: implications for ischemic preconditioning. Proc Natl Acad Sci U S A 2002;99:3312 – 7.
Halestrap AP, Woodfield KY, Connern CP. Oxidative stress, thiol
reagents, and membrane potential modulate the mitochondrial permeability transition by affecting nucleotide binding to the adenine nucleotide translocase. J Biol Chem 1997;272:3346 – 54.
Grover GJ, Garlid KD. ATP-sensitive potassium channels: a review of
their cardioprotective pharmacology. J Mol Cell Cardiol 2000;32:
677 – 95.
D’hahan N, Moreau C, Prost AL, et al. Pharmacological plasticity of
cardiac ATP-sensitive potassium channels toward diazoxide revealed
by ADP. Proc Natl Acad Sci U S A 1999;96:12162 – 7.
Takeo S, Nasa Y. Role of energy metabolism in the preconditioned
heart—a possible contribution of mitochondria. Cardiovasc Res
1999;43:32 – 43.
Suzuki M, Sasaki N, Miki T, et al. Role of sarcolemmal K-ATP
channels in cardioprotection against ischemia/reperfusion injury in
mice. J Clin Invest 2002;109:509 – 16.
Suzuki M, Saito T, Sato T, et al. Cardioprotective effect of diazoxide
is mediated by activation of sarcolemmal but not mitochondrial
ATP-sensitive potassium channels in mice. Circulation 2003;107:
682 – 5.
Grimmsman T, Rustenbeck I. Direct effects of diazoxide on mitochondria in pancreatic B-cells and on isolated liver mitochondria.
Br J Pharmacol 1998;123:781 – 8.
Hanley PJ, Mickel M, Loffler M, Brandt U, Daut J. K-ATP channelindependent targets of diazoxide and 5-hydroxydecanoate in the heart.
J Physiol (Lond) 2002;542:735 – 41.
Das M, Parker JE, Halestrap AP. Matrix volume measurements challenge the existence of diazoxide/glibencamide sensitive KATP channels in mitochondria. J Physiol 2003;547:893 – 902.
Pain T, Yang XM, Critz SD, et al. Opening of mitochondrial K-ATP
channels triggers the preconditioned state by generating free radicals.
Circ Res 2000;87:460 – 6.
Liu YG, O’Rourke B. Opening of mitochondrial K-ATP channels
triggers cardioprotection are reactive oxygen species involved? Circ
Res 2001;88:750 – 2.
Forbes RA, Steenbergen C, Murphy E. Diazoxide-induced cardioprotection requires signaling through a redox-sensitive mechanism. Circ
Res 2001;88:802 – 9.
Baines CP, Goto M, Downey JM. Oxygen radicals released during
ischemic preconditioning contribute to cardioprotection in the rabbit
myocardium. J Mol Cell Cardiol 1997;29:207 – 16.
Hanley PJ, Gopalan KV, Lareau RA, Srivastava DK, von Meltzer M,
Daut J. Beta-oxidation of 5-hydroxydecanoate, a putative blocker of
mitochondrial ATP-sensitive potassium channels. J Physiol 2003;547:
387 – 93.
Lim KHH, Javadov SJ, Das M, Clarke SJ, Suleiman S-M, Halestrap
AP. The effects of ischaemic preconditioning, diazoxide and 5-hydroxydecanoate on rat heart mitochondrial volume and respiration.
J Physiol (Lond) 2002;545:961 – 74.
Halestrap AP. The regulation of the matrix volume of mammalian
mitochondria in vivo and in vitro, and its role in the control of mitochondrial metabolism. Biochim Biophys Acta 1989;973:355 – 82.
Xu WH, Liu YG, Wang S, et al. Cytoprotective role of Ca2 +-activated
K+ channels in the cardiac inner mitochondrial membrane. Science
2002;298:1029 – 33.