OEIS complex with craniofacial
advertisement

A.'11eric:ln .J ournal of Mcdical Genctics 53:21-23
(19~4)
Brief Clinical Report
OElS ComplexWith;Craniofacial
f\nomalies-.. DefJdI::O'f Blastogenesis?
~1utosh Haldat·..Anit" K. Shann",
hubha.R. Phadke, Anita Jain, and S.S. Ag"rwal
Postgraduate Ins/illite of Medical Sciences, Lucknow, India
:Irll~~(!nt nr_!t-[~dic.al Genetics, S~nja~ :~andhi
Ww rJ~port ,C1n 'b. 3i-wcck Tetus with hydro·
ct:ph:d U~, ,hypcrtclorism. microtia,. ShOl"t
H.eck, vcdeb:caL and rib defects, scoliosis,
0;npb(ll~cdc, .exstrophy of bladdeI\,abscnt
€:xt~:"~);d genitalia and pubic raIni, impcrfo·
l".!tc anus, rliuphragmatic hernia, dcfectivp.·
lnhu!:Jtion of lung-s, single kidney, bicornu- .
atc uterus, o.nd flexion deformities of the
limos. 8im.itor cxtcn5ivc anomalies in the'
rostr.::ll and c£ludnl regions were described
hy Russell' ct ai. [Pediatrics, 67:176-182,
,!)611 "nd Stew"rt et al. LAm J Med Genet,
.1:',,12&--l29, 19931. The p"tients described by
them h:.1d a combination of the oculo-auriculo·vertebral sequencc (GAY) and caudal
deficiency sequence, whereas the patient rc·
ported here can best be described as " combination of OAY and OElS (omphalocele,
exstrophy of bladder, impcrfor~tc ·anus,
spin::l defects) complexes; The widespread
malformations .seen in our, patient may be
Lhe rosult of "n en-or during blastogenesis.
.i' 19::H Wilcy-Lis.s, Inc.
IrJi:Y \VOHDS: bI3,Stogencsls, GElS. cculo~uricuio-vertebralscqtlenC~,
"xial mesoderm"ldyspIasia
INTRODUCTION
.J. c(lmbiliation of severe congc!1ital anomalies of the
c!";)nifti regio;:l. (corresponding to the oculo-at.:ri~uio-.... c:rtd.. nlllOAVJ se:quence) Hnd caudal rcgion (:-csembling
thr: c::li.idJ! JeHcic.:nc.l' :)r~c.;,ucrlc~} v,,·as described !J't
l\L;~:F':1.i ct 3l. [19811 Hnd Sl~w:lrt.ct cd. f19~J:31. TI1!~ t~rT~~
"~:.;:i.:t mC:j/):.krm:ll d.y::.phlsiu" wa'~ used by Hussdl Cl al.
Hccc!vd lfir
~.by
puhlit.:rl~ion t~o\·N:llh·:"
1, 1993:
r":\'i~:lflli f':' ~,,;\' .:':~
I ~l, 19tH.
r\ddfC:::S reprint rcqlll~sl~ III Dr. Anita K. Sh;mTl:.l. ,\".. . .:!:>I.::l~l
PrOrC:iSOr, Depllrtmt'nl or i\tl:Jic:..! i Gc·ndics, S:l.pjo.y. G:wdhi }'u:\l·
I;racL:ule In.sliu:lC
Ml'dil.::.d :)l"I\'lICt:S. H~cb:.m:li RO:ld, L:.Jckl:IIW
- 2'150 l-i , INO£A,
or
© 19!1·1 Wilcy-Liss, Inc.
[19811 to describe lhis condition .. Here, we.report on a
fetus who combine.s the crq.nird a.namnljcs·sll~[~cs.t.iv~.tll'
GAV· sequence and cut:.dnl anomalies re:-i{~mbling' Lhc
~mphalocclc-extrophy of bladder,' imnc:rfor;lte <in~'3.
and spine def~cl:5 (OEIS) compicx n.nd".sugg,~s:. thn~"a
dcrcct. acring· hlast.og·e:n~sis may be resp(~nsib:t: fur
thesc: r:nalrormatinuE,
'
.
CLINICAL REPORT
. The pretcnTI. feLus WRS the fourth p'rcgrianC); o( r. ~~(j~
year-old Itlotht:r 2,;ld '31-year·old rat.her. 1'his Hinou
couple was non-consanguineous and Lhcre was no fo'lmily history of 0 similar m,,!formotion. Their Jirst horn
was then "n 8·your·old healthy boy fullowed by 2 stillbirths each at 8 months of gestation, none having nny
extern,,1 anomalies. During the present pregnancy tho
mother wos non·diabetic and there was no history of exposure to any known teratogen. r'\.n ultrasound examination at 30 weeks gestation, carried out. because of
oligohydramnios, showed hydrocephal,," r."d pIaoe:1t"
praevia. The pregnancy was tcrminot:..'d Dt 31 wcel,s l:>v
ceSi1rean section Rnd the nw.lformed G~iJJbol'!\ ir:.fc.n."t
wns reierreu to the genetics unit.
The infant weighed 2,200 g and c!"own hLlcl lcr',gth
was 27 cm (spu;-ious because of scoliof,iti). The e:-:lcrn:t1
anomalies in the cranial re:g1on were hydroccDh..: ks
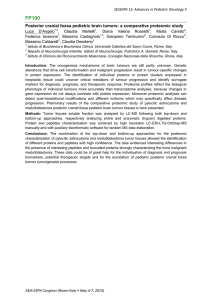
(occipito frontal circumference 39 ern), faciai 3$Y711;netry, microtia, hyperlelorism, micrognathia, and gll1g;val hype! pinsia (Fig. 1). The I=yes \v€:re ncrnlHJ. TiHl:'I.:
W2.S mnrked scclios:£, The infraumbilicnl Dart of the (i~\.
tericr abdominal woll \';8.S iibsc:1l l};-;,d ~'. Ji1s!~tec! of a
n .: pt\ll'cd cmphalo..~cl~ cO::ila·i.~inz E\"~l' iUH.! p,"J'L Ir.fuinrlj' the biaddcr w?~ ev~rt~d 2ild 11 blind e,11o;lic !O\ljl
could be sern u~sid0 H. S:·:ternai .c:e:--.~lnJin ' . . er€: a~se~t
and thCi..:l \'In~ l~() :':;l:1i op::ning tFi;;. 2). Lower it:ll;l-=:;
::;h(Jwcu hila:c:-:li t:l!:l-'e~; l~qU:i'I'.• ·.laru5 wilh ~h':d,..,:,; d.. :··
iormi~y tli.. i~;ps :md k!~~~~,
.
R~r.i!;5:·r:~hic C':-::!'~lin;i.~iiJ;: cir.~C1..;mt:ntc'l.i t!:e pi '':::::Cli(~:
oi ~c\'::!l'i' S\;{I;;!l~i:;. ll':p!: \·I.. ~·tt~b!',lP ip,. the U !JU':'j" I htl:';~:·;::
}'e:gior:, n::!r ·1l\~mb:1l' l:,:,! . tr.Qr~tl:. j'li~iOil oneil k',Vf::' :-il.l :;
ar,(: ;l:"'~er"l puhic 1',:011 (?ig. ~j).
Oil.HlIW·;.i ..;)' t.ile hyd\'occph~\lt'~-s"~va5 tQnnl'ln~:d by ,he
prC3e!\C~ (II' P::·ll~.~ly e7"!lnrgcu !:.H.:::nd "'(;litric:~\:: .. :~nd thin
w:'li!eu t~n·bral helni~phel'c~. Addilion~l aUI.O!-l~Y l:no·
ing::-; incltl<:f'\; diaphragmatic hcrnitl with spleen lying-
Ho.Jdar ct 0.1.
)2
or p("h'i~ showinJ.:" :\unllrm:ll ~;lcrum. ulIlI~:,ili("d
Ibdil,~r:lph
Fit:" 3"
puL.ic r;lnli. -1 IUllIb"r vcrt("hr:lc, :Hld
hypopl:l~i"
or 10\\'cr
rih~
un the
rit:hl.
Fig_ 1.
Cruni01( rC;Jon_ Nole hydroccph:llus :lnd
H-V~'r~'
microll'L
in the thorax; bilaterally hypoplastic, bilobcd lungs
(combined weight 17 gJ; unilobular livcr; .singlc kidney
on right side; and bicornuate utcru~" The heart was
normal and the histologic ~tructure of lung~, li\"cr, kidney, and spleen W<:lS normal for gest\l.liono.l age_
Chromo~omal nnalv::iis is not available bCl."au~c the
fetal tissue did noL gr~w"
DISCUSSION
\Ve have dcscribed \l. fetus with multiple congenital
anomalies anecting both the cranial and caud;"ll regions. Russell et 01. 119311 and Stewart ~t "I. 119931
have described similor patients_ Thc findings in our p:\tient nnd those of previous authors are $umrnarised in
Table 1.
The cranial malfornwlions of the present ca~c appear
to represent the OAY sequence because of lht, presence
ofmic:-otin, facial asymmetry. and vertehral defccls but
the fctu~ did not have any epibulbar dennoids rJl" of.:ular
TABLE I. Clinic;,l
Wilh
i\li1nircslnLion~of 1'atients
··A.'\ial1\h·~(ldcl"!nalDy~p1<lsi;I"'~
Hu~~cll
Ch;1rnClcri~tic
.\btern:d agt·
St'X
Binh \\"t-ighllJ.!1
F:lci:li ;HlOfllalit,s
cl al.
StL'\\":ll"l
cl :11_
!'n:~t'nt
119811
I I~!):lI
(::ISL'
:30
:!H
:!(i
~l
~I
(0'
:'UJOO
:lllhll
~.:WU
+
+
..,.
+
+
,
+
,
+
.,.
.,.
,
•
-------- -- -------_."-
,\s·'mmc.'lr\'
Pr~' :lllricubr skir.
t:11.: ;\IU1lia
+
Epil;ulh:tr dt,t"llloid
J.lypcrt t'!ol"i:-:nl
Short Ilt'I,:k
fh'dulld:1ll1 nt'ck
i-
.,.
.
~kin
Skt'lt'lal ;\fllllll"lit·:-:;
\'l'rtl'hr:d
h,~i(lns
NR
:\ntllll:lli~'~
~:!cr:t1 aJ.:~'nl'~i~
Hi!>
Talipl':' t'quilltl-'I.":lru:-:;
Fll'xillll llt,flll"lIlit\'
Ht'Il:t1 :llllllll:dil'S '
__ \~l·llt':<i. ..
.,.+
,.
,.
,
i-
,
+
Singlt, kidney
NH.
:\!>nlH"llI:1! ('xtt'l"n:l!
gt-llit:,lia
Ab:-:(.'nl unJc~t'cndcd
...
+
NA
tc~tl'~
C:lrdio\".:\:-:cubr :tIHltn:tlit,S
I)L'~lt"O\"l'r$itJl\/VSl)
+
()Ihl'l"~
Ilydru<:t'ph:dll~
+
+
:-\"nal :\lrl'::.i:l
Audiliul\:lllindil\g~ in
tilt"
prt"~('111 t':l::'l'
:\h:<l'nl puhlic r:\ll1i
.,
E~Olllllh;lln::.
E~:<t rophy hladder
;-
,
>
Di:lphr:lgll1:1tic lH:rnia
Bil'ornu:lll' ut('I"U~
Fi~,
2,
Lllwt'r ;lUUOI1Wrl ;lllU pl~rinl."Ulll showil1\.: l·\~tr-"phy hLulr,h-r.
:\b~l.'nl (·:\t~-nl:d .I-:~·l1il;lli:\, :lnd illlpl'rfl/r:ll\' alln:,"
cohlll!c loop_
..
NA
':\H" II" rt·,-,.nl: :-.;,\ - IIt.l :11'1.lil'ahl.. :
illJ.: al.':I-I1(.
+
OEIS With Craniofaei,,1 Anom"lies
annmnlicM. However, lite OAV scquencc·is knnwn to be
\"nriahlc in its clinical presentation, the mildc:o>t IIf
which may be the presence or a unilateral c;n litg
[Roll nick and [(aye, I!J!) II. Our patienl also had hydrocephalus, which was described by Hussell el al.ll%11
in their patient.
Unlike the cranial a,;omalies, the caudal anomalies
in this retus were quite different from tho.se reported in
the previous cases. The caudal anonwlies in the cases
reported hy l(ussell et al. 119811 and Slewarl· el al.
[19931 resembled the caudal deficiency sequence,
whereas in our patient they resembled the OEIS com·
plex {Carey et aI., 19781.
.
The malfornmlions in our pnticnt were SC\'crc,
extensive, midline, and mullis}'slcmic: hence. n likely
CXpli\natiun is it defecl of hlasluljcnesi:i. During bla::'tog"enesis the enlire embryo "cpl'esenls n single dt'\"(~lop.
mental field nnd any "hit" during this period can result
in widespread anomalies which arc severe in nature.
usually of the midline nnd frequently incompatible
wilh life IOpitz, 199;1I.
A gcncnlliscd G.lteration in mcsOdCl-m.1.1 cell migration dUl'ing the primith"c slreak period has be('n postut~ted to c<J,usc the nlalfllrnwtions described ~s -axial
mesodermal d)'splosio" and OEIS Illussell et 01. 19RI;
i\loore and \Vca\'cr, 19~1O: \Vinler f.lnd Barait:-:cr, IV91 L
However, these m:df"orlll:ltions can also he adl~qllal('ly
explained as dl'fct:ls or bl;tslugenesi:L
23
Although hath OAV and OEIS cnrnplcxc.'s nrc pre·
:'oumcu tn be dcfecL... IIr hbst'lg'encsis IOpitz, ) ~)9:.s I, G.
combination of both in the :'G.mc patient hns not been
described before. The patient described by us bridll'es
this gap and further suppnrL< the role or defecth'e blastogenesis in the occulTrncc of mG.lfQrmaUons described
as OEIS ond OAY complexes, as well as axial mesodermal dY5plnsia spectrum.
nEFEH8NCES
C;m:y .IC. GrCl'nbarn
n.
11:111 un t 19;5I; The OEIS Gnnlplcx 10m"
phalncdc. EXl'lrUph)·. Impl·rrur:.lc Anll~, Spinal 1J,·rl.-t:lSI. New
Yurl..: A!:In It Lil's, Inc.. li,r th ..· Na(iUlIiII Fllulltblinll-l\f~lrch or
I>inH"~. IW:O;\S 1·116Ih::!;-,:I-:W:I.
),Inorl' C ..\. \\"I';I\'('r nil f I !l!IIII~ Ex~t 1'lIl'hy ur dual';! ~l·lIlH·IIl·I'. hI' HtI.\·~('
),1I.1\·d I: "Hirth Ilt-rt'cts Ent·ydfll'l·tlia.~(h("nl: B1:wkwl"ll S,'it,lttitic
l'uhlic;ltl"n:" pp 1l..$~(;·I!I.
I >PIIl. .1)'1, I !1!I:II: n1:lS~Of,.:CIH"::iS and I Ill' ~I'rilllary Fil"!d- in HUlUan Dc·
\"t"!I'PIIU·lll. Nt,\\" York: ..\Ian H. U:,:,. Inc.• rur t1H' N:lliun:d FOlllld:ltlon-:-'1:lrch ornin!',;. HIl:O..\S :!!J 111~;J-:I7.
RlIllnick Bit. I';IY(" ·Cl 119!11l1: Ol'ultl-;lUril'ulu-\"i'rtchral anum:'!l)"_ In
BUyH' ),IL led): -13irl-h nC'r~'l'(~ Enc~·c1l1pcdi;t.- Oxrllrtl: l3Iackwelt
~('i!'ntlfic I'ublicnlilln~. PP I:!':!-I:!;..$_
nf), Bull ~l.r I J!IHI J: The :ax!:'!1
:,pl·c(ru01. Pcdi:lt ric~ {i,: I,li- 1:->2.
RU,,:':j·J1I,J. \\\::I\"cr
:'1<1
mc"~(Jdcrnl
dyz;pl:J.-
Ste\\":art F.J. ~l'l'in i':C. Brown ~ (lll!J:II: Axial nlc:,mlcrllt:ll dysplasia
":'pl'Clnlnl. Am J ~Icd Gt'net ·l:i:-l:!.li-l:!.!).
\\'lIlh'r le,1. llar:Jitser M r 1!I~JlI: -;\l11ltiplc Conf,.:cnit;d AnolOaliC's. A
Iha~ntl~tlr Cnnllll"ndilllll.- l.und"Il: Chapman and Ilall :\It'dkal,
p ;i·l.