Assessment and Treatment of Cognitive Deficits in Adults with Mood

V O L U M E 2 , I S S U E 4
Assessment and Treatment of Cognitive
Deficits in Adults with Mood Disorders:
Restoring Function
By Vina M. Goghari, PhD, RPsych, and Glenda M. MacQueen, MD, PhD, FRCPC
Major depressive disorder (MDD) and bipolar disorder (BD) are among the 10 most debilitating mental or physical illnesses in terms of number of healthy years lost to illness.
1 These
disorders have a major economic impact through both health costs and loss of work productivity.
2 Cognitive deficits are present and contribute to lower functional outcome in both MDD and BD.
3-5 Assessing and treating cognitive deficits are, therefore, important parts of recovery in mood disorders. This issue of Mood and Anxiety Disorders Rounds reviews the neuro psychiatric tests employed in the measurement of cognitive deficit associated with MDD and
BD, as well as the array of pharmacological and nonpharmacological treatment options.
Case Study
A 35-year-old female receptionist with bipolar I disorder, who has recently recovered from a depressive episode, continues to experience noticeable cognitive challenges (memory, attention, multitasking) that are causing her difficulty at work. Her psychiatrist refers the woman to a neuro psychologist for a thorough assessment.
Neuropsychological Assessment
The goals of neuropsychological assessment are to facilitate differential diagnosis, examine the effects of neurological, medical, and emotional disturbances on cognition and behaviour within the context of biopsychosocial factors, and monitor a person’s functioning over time.
Ultimately, this information is used to determine a person’s cognitive strengths and weakness to facilitate treatment planning. Strengths of neuropsychological tests include ease of use, standardization, normative samples for comparison, and documented reliability and validity. In addition to being used in clinical settings, many neuropsychological tests are used in research to measure various domains of cognitive functioning.
Common neuropsychological tests (Table 1)
Intelligence is “a very general mental capability that among other things, involves the ability to reason, plan, solve problems, think abstractly, comprehend complex ideas, learn quickly, and learn from experience” and holds practical importance as these skills have been found to be strongly associated with outcomes such as school attainment, job success, and even longevity.
6 The
Wechsler Adult Intelligence Scale – Fourth Edition (WAIS-IV) is a common measure of intelligence, and premorbid intelligence is routinely measured with the National Adult Reading Test
(NART/NART-Revised).
Cognitive screening tools measure general cognitive impairment, and many were developed specifically for screening and assessing dementia. In a neuropsychological assessment these tests would likely be used in conjunction with other tests. Commonly used measures include the
Mini-Mental State Examination (MMSE) or the more sensitive Montreal Cognitive Assessment
(MoCA) as screens for cognitive impairment and the Dementia Rating Scale – 2 and Repeatable
Battery for the Assessment of Neuropsychological Status as more in-depth measures.
Available online at www.moodandanxietyrounds.ca
CANMAT Advisory Board Executive
Sagar V. Parikh, MD, FRCPC
Education Chair, Toronto
Editor, Mood and Anxiety Disorders Rounds sagar.parikh@uhn.ca
Raymond W. Lam, MD, FRCPC
Executive Chair, Vancouver
Sidney H. Kennedy, MD, FRCPC
Depression Group Chair, Toronto
Lakshmi N. Yatham, MBBS, FRCPC,
MRCPsych (UK)
Bipolar Group Chair, Vancouver
Jitender Sareen, MD, FRCPC
Anxiety Group Chair, Winnipeg
Roger S. McIntyre, MD, FRCPC
Business & Research Development Chair,
Toronto
Roumen Milev, MD, PhD, FRCPsych, FRCPC
International Conference Chair, Kingston
CANMAT Board of Directors
Serge Beaulieu, MD, PhD, FRCPC
Montréal
Glenda MacQueen, MD, PhD, FRCPC
Calgary
Diane McIntosh, MD, FRCPC
Vancouver
Arun V. Ravindran, MB, PhD, FRCPC
Toronto
Canadian Network for
Mood and Anxiety Treatments
Education Office
Room 9M-329, Toronto Western Hospital
399 Bathurst St, Toronto, On
CANADA M5T 2S8
CANMAT – or the Canadian Network for Mood and
Anxiety Treatments – is a federally incorporated academically based not-for-profit research organization with representation from multiple
Canadian universities. The ultimate goal of
CANMAT is to improve the quality of life of persons suffering from mood and anxiety disorders, through conduct of innovative research projects and registries, development of evidence based and best practice educational programs and guideline/policy development.
Table 1: Commonly used adult neuropsychological tests that might be relevant to mood disorders
Domain Description
Intelligence
•
–
–
–
–
Wechsler Adult Intelligence
Scale – IV
(full scale IQ and 4 indices)
Verbal comprehension
Perceptual reasoning
Working memory
Processing speed
• National Adult Reading Test
(NART/NART-Revised)
•
•
•
•
•
•
•
•
•
•
•
•
•
Composed of 10 core subtests and 5 supplemental tasks
•
•
Similarities: abstract verbal reasoning
Vocabulary: ability to comprehend and verbally express words
Information: general knowledge
Comprehension: ability to apply abstract social rules
Block design: spatial perception, visual abstract problem solving
Matrix reasoning: nonverbal abstract problem solving, inductive/spatial reasoning
Visual puzzles: spatial reasoning
Picture completion: timed visual perception for details
Figure weights: quantitative and analogical reasoning
Digit span (forward, backward): attention, mental control
Arithmetic: attention while working with mathematical problems
Letter number sequencing: attention, mental control
Symbol search: visual perception, scanning speed
Coding: visual-motor coordination, motor/mental speed, working memory
Cancellation: visual-perceptual speed
Measures premorbid intelligence. Reading aloud a set of 50 words that can be irregular in terms of their grapheme–phoneme correspondences
Cognitive/dementia screening
• Mini-Mental State Examination or Montreal Cognitive
Assessment
• Dementia Rating Scale – 2
• Repeatable Battery for the
Assessment of
Neuropsychological Status
Brief 30-point questionnaire tests that are used to screen for cognitive impairment (eg, dementia).
Assess orientation to time and place, registration, attention and calculation, recall, language, repetition, and complex commands.
Measures overall level of cognitive functioning. Consists of 5 subscales, which provide additional information on specific abilities: attention, initiation/perseveration, construction, conceptualization, and memory.
For the detection and neurocognitive characterization of dementia, but also useful for other disorders with cognitive impairment. Assesses immediate and delayed memory, visuospatial/construction, language, and attention.
Attention and executive functioning
• Conners’ Continuous
Performance Test – II
• Trail Making Test
•
•
•
•
•
Wisconsin Card Sorting Test
Stroop Color-Word Test
Tower of London
–
–
Verbal Fluency
Category or semantic fluency
Letter or phonetic fluency
Ruff Figural Fluency Test
Memory
• Weschler Memory Scale – IV
Measures attention and impulsivity. Computerized test that requires a pressing of a button for all letters that are serially presented on the computer screen except an “X”.
Part A measures visual attention and requires connecting circles containing numbers sequentially.
Part B additionally measures task-switching and requires connecting circles containing both numbers and letter sequentially but with added component of alternating between number and letters.
Measures set-shifting and perseveration. Required to sort cards according to the different parameters
(form, shape, colour, number) found in all cards based on feedback (correct/incorrect) and the sorting principal change after a certain number of correct responses are attained.
Measures attention and cognitive control (ie, ability to inhibit an automatic response in favour of a task-relevant response). Reading aloud a list of colour words and a list of colours to name. Third list read aloud the colour in which a word is printed, ignoring the word, where the written colour name often differs for the colour in which it is printed.
Measures planning and problem solving. 2 sets of beads and boards with pegs are present with
2 unique arrangements. Required to recreate the same arrangement of beads on the board as the examiners’ arrangement by using the least number of moves to reposition the beads.
2 different types – category and letter – measure the spontaneous generation of verbal information.
– List all of the words in a specific category (eg, animals) in 60 seconds.
– List all the words that begin with a certain letter (eg, F, A, S) in 60 seconds.
Measure spontaneous generation of unique designs. Connecting dots into different patterns.
•
•
Verbal List Learning Tasks
Rey-Osterrieth Complex
Figure
Includes 7 subtests: spatial addition, symbol span, design memory, general cognitive screener, logical memory, verbal paired associates, and visual reproduction. Performance is reported as 5 index scores: auditory memory, visual memory, visual working memory, immediate memory, and delayed memory.
Measures verbal learning and memory. All list-learning tasks involve being presented with a list of words and being asked to recall the words immediately and after a short and long delay.
Measures visuospatial memory, as well as executive functioning (planning, organization). Reproduce a complicated line drawing by reproducing it immediately from memory and after a delay, as well as copying it.
Attention and executive functioning.
Attention is a domain of cognition that involves concentrating on certain aspects of the environment. Executive functioning is a domain of cognition that includes processes such as working memory, planning, inhibition, mental flexibility, and controlling actions.
7
Common measures used in this domain include the Trail
Making Test, Conner’s Continuous Performance Test,
Wisconsin Card Sorting Test, Stroop Color-Word Test, Tower of London, Verbal Fluency, and Ruff Figural Fluency.
Memory is the process by which information is encoded, stored, and retrieved. It is assessed in both verbal and visual domains. Assessment tools include the Wechsler Memory
Scale-Fourth Edition, Verbal List Learning Task (eg, Rey
Auditory Verbal Learning Test, Hopkins Verbal Learning Test-
R, and California Verbal Learning Test-II), and Rey-Osterrieth
Complex Figure .
Limitations of neuropsychological tests
Although neuropsychological tests have many strengths, a few limitations are worth noting. First, most neuropsychological tests do not measure one cognitive domain, and hence may not measure a specific deficit. For example, although the
Trail Making Test, Part B is commonly thought of as a measure of task switching, it also measures visual attention, processing speed, and working memory among other processes.
Therefore, problems with these tasks may be representative of a generalized deficit that is often present in psychiatric samples rather than a specific deficit. Second, the normative samples for comparison for many of the tests can differ widely in the number of individuals used to derive the sample and representativeness of the sample. Finally, differences in motivation between impaired individuals and the individuals in the normative sample could also account for differences in scores. To bypass some of these criticisms, researchers often use cognitive tasks that have been developed experimentally to tap a specific process and equate their experimental and control conditions for difficulty. For example, the Cognitive
Neuroscience Treatment Research to Improve Cognition in
Schizophrenia (CNTRICS; http://cntrics.ucdavis.edu/ index.shtml) and the Cognitive Neuroscience Test Reliability
And Clinical applications for Schizophrenia (CNTRACS; http://cntrics.ucdavis.edu/publications.shtml) have been compiled for use in translational research aimed at improving outcomes in schizophrenia. Some of the tasks recommended for schizophrenia research may also be appropriate in mood disorders.
Review of Cognition in Major Depressive Disorder
(MDD) and Bipolar Disorder (BD)
In the last several years, a series of meta-analyses have examined cognitive deficits in MDD and BD. These are briefly reviewed.
Review of cognitive deficits in MDD
First-episode MDD versus controls and recurrent-episode
MDD.
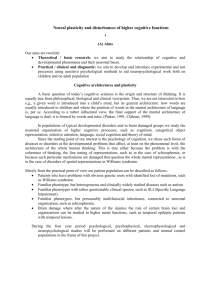
8 Pooled analysis of 15 independent samples (N=644 patients; mean age 39.4 years) revealed significant deficits in psychomotor speed, attention, visual learning and memory, task-switching, verbal fluency, cognitive flexibility compared to controls in patients with a first-episode of MDD. Working memory and verbal learning and memory did not discriminate between groups (Figure 1). This meta-analysis also demonstrated that executive functioning deficits were unrelated to illness severity and therefore may represent a trait marker for MDD. In contrast, psychomotor speed, visual and verbal learning and memory, and working memory were associated with illness severity measures, such as mood and inpatient status. Furthermore, neuropsychological findings were not found to be more severe in patients with recurrent-episode MDD compared to patients in their first episode.
MDD severity.
In their review of 14 studies, 9 the authors determined that performance on tasks of verbal memory, executive functioning, and processing speed, but not semantic fluency or visual spatial memory, was negatively associated with increasing illness severity.
MDD with psychosis versus MDD without psychosis.
10 As revealed in 5 studies (N=325; 150 MDD no psychosis, 175
MDD psychosis), the presence of psychotic symptoms was associated with greater impairment in visual spatial tasks, attention/working memory, psychomotor speed/dexterity, executive function, and memory compared to patients without psychosis.
Case Study (cont.)
The neuropsychologist begins by conducting an interview with the client, gathering information on her personal and family history of psychiatric and medical disorders, social and educational background, and developmental history.
The client recounts having her first depressive episode
approximately 10 years ago, followed by 4 other depressive episodes and 2 manic episodes. She reports being on lithium and that it is working well for her. She does not meet the
criteria for a depressive, manic, or mixed episode. The client also reports significant anxiety related to falling behind at work and perceived judgment from her supervisor.
Additionally, she indicates that she has discontinued her exercise routine since her depressive episode began.
Behavioural observations suggest mood is euthymic, although affect is somewhat restricted.
The client is cooperative throughout testing and completes each presented task. A thorough battery of tests is selected including 4 subtests of the WAIS-IV, measuring vocabulary, working memory, processing speed, and perceptual reasoning; tests of attention and executive functioning; and tests of visual and verbal memory. Additionally, to measure current mood symptoms, the client completes self-reported measures assessing current depression and anxiety. Consistent with the client’s report, her scores are found to be in the low-average range on measures of attention and executive functioning, memory, language and perceptual generation, working memory, processing speed, and perceptual reasoning compared to peers of the same gender, age, and educational background. Verbal intelligence is found to be in the highaverage range. Depression scores are in the low end of the moderate range and anxiety scores are in the moderate range.
Figure 1: Meta-analytic results of cognition in first-episode major depressive disorder compared to controls
0.6
0.5
0.4
0.3
0.2
0.1
0
Psycho m oto r
Speed
Atte n tio n Vis ua l
Le arn i n g an d
Me m o r y
T a sk
S w itchi n g
Ve r b a l
Fl u e n cy
Cog n itive
Flexibility
W o r ki n g
Me m o r y
Ve r b a l
Le arn i n g an d
Me m o r y
Adapted with permission from Lee RS et al. J Affect Disord . 2012;140(2):113-124. Copyright © 2012.
Review of cognitive deficits in bipolar disorder
Euthymic BD versus controls. Several meta-analyses have examined cognitive deficits in euthymic patients with BD. One recent meta-analysis (28 studies; 1026 euthymic bipolar disorder patients and 1384 healthy comparison subjects) demonstrated that all domains of cognitive functioning had medium to large effect sizes for impairment in euthymic BD compared to controls, save verbal intelligence, suggesting that crystalized intelligence may remain more intact.
11 Surprisingly, this metaanalysis of 28 studies demonstrated that as age and duration of illness increased, the magnitude of cognitive deficits decreased. Gender was found to have no impact on the effect sizes, whereas greater education was related to less impairment. Overall executive functioning was more impaired in individuals with a poor clinical course compared to a good clinical course.
BD-II versus controls.
12 In this quantitative review of
9 studies (263 patients with BD-II and 415 healthy controls), patients with BD-II demonstrated significant cognitive deficits in global cognition, executive function, visual memory, verbal memory, planning, and working graphic variables did not impact the effect sizes.
BD-I versus BD-II. global cognitive ability, executive function, visual memory, and verbal memory than patients with BD-I in an analysis of 11 studies (444 patients with BD-I and 285 patients with BD-II).
12
Patients with BD-II had better
Attention, planning, and working memory did not differentiate the groups.
Impact of psychosis. The authors of this meta-analysis of 11 studies (N=774; 435 patients with psychotic BD and 339 patients with nonpsychotic BD) 13 found that patients with psychosis had worse global cognition, executive function, verbal memory, working memory and planning compared to BD patients without psychosis.
Attention and visual memory did not differentiate between groups. A greater number of manic episodes were also associated with lower global cognition.
Treatment Options to Improve Cognition
The strong correlation between cognition and functional outcomes such as maintaining a relationship and performing at work underscores improving cognition as a key goal in psychiatric disorders. When aiming to enhance cognitive function in patients with mood disorders, it is important to consider several function-inhibiting factors. It is important to ensure that patients have normal thyroid function when targeting cognitive symptoms. Primary sleep disorders may exacerbate cognitive problems and need to be ruled out in patients with mood disorders.
Exces sive use of alcohol or illicit substances can also have a negative impact on cognition, and patients need to understand that it may be impossible to improve cognitive function in the face of ongoing substance abuse. Medications such as benzodiazepines may also have a negative impact on cognition; patients may need to evaluate whether the benefit of these and other hypnotic medications outweigh the negative impact on cognition. The cumulative cognitive burden of both the physical illnesses and the medications taken to manage them may be substantial, partic ularly in older patients or those with coexisting illnesses. Optimized treatment of physical illnesses, such as blood glucose control in patients with diabetes or optimized airway flow in patients with chronic obstructive pulmonary disease, may be important adjuncts to treatment.
Lithium
Lithium is primarily used in the treatment of BD, particularly for mania. A meta-analysis by Wingo et al
(12 studies; N=539) 14 demonstrated that lithium treatment was associated with a small but significant deficit in immediate verbal learning and memory and creativity. In contrast, delayed verbal memory, visual memory, atten-
tion, executive function, processing speed, and psycho motor performance were not significantly affected.
Selective serotonin reuptake inhibitors (SSRI) and selective serotonin norepinephrine reuptake inhibitors (SNRI)
A small meta-analysis (3 studies; N=122) 15 found evidence for an improvement on one domain of executive functioning (Stroop test performance) during antidepressant treatment in patients with MDD without psychosis; however, further research on more domains of cognition are needed.
Lamotrigine
Two reviews of studies in BD suggest lamotrigine does not impair cognition, with some evidence suggesting benefits.
16,17 Other anticonvulsant medications (valproic acid, carbamazepine, topiramate) have been associated with negative effects on cognition.
16,17
Atypical antipsychotics
A review of atypical antipsychotic use in BD suggests that antipsychotics have shown more negative effects on cognition as compared to lithium and anticonvulsants.
16
More research has been conducted in schizophrenia, with mixed evidence. The National Institute of Mental
Health’s Clinical Antipsychotics Trials of Intervention
Effectiveness (CATIE) trial 18 found no significant differences after treatment in any cognitive domains with risperidone, olanzapine, quetiapine, or ziprasidone in schizophrenia compared to perphenazine; small beneficial effects were present for all groups.
Cognitive remediation
Cognitive remediation is a promising strategy to increase cognitive ability. It typically involves training on mental processes and tasks.
19 A meta-analysis of 7 studies
(N=104) 20 of cognitive remediation in patients with affective disorders found a medium effect size (0.44) for pre-post cognitive change after training. In support of these findings, our recent study found increases in brain activity as measured by functional neuroimaging after 10 weeks of cognitive training in 38 patients with mood disorders.
21 These increases were seen in prefrontal, temporal, and parietal regions during working memory task and increased activations in the hippocampus in recollection memory task after the training.
Exercise
Exercise may have a positive effect on cognition, both in healthy people and in those with a mood disorder. The hypothesized neural mechanisms through which exercise might exert cognitive benefits include increased neuronal survival and functioning, decreased inflammation, improved vascular function, and reduced levels of stressrelated neuroendocrine responses.
22,23 A few studies have suggested that patients with MDD derive cognitive benefit from exercise; 24,25 however, improved cognition is not a uniformly consistent finding.
26
Fatty acids
Multiple cross-sectional and prospective surveys have reported a protective role of erythrocyte membrane polyunsaturated fatty acids, in particular docosahexaenoic acid (DHA), against cognitive decline.
27 While few studies have specifically examined the relationship between erythrocyte lipid composition and cognition in adults, deficiencies in
Ω
-3 polyunsaturated fatty acids such as DHA have adverse effects on cognition, 27 while supplementation with
Ω
-3 polyunsaturated fatty acids may be beneficial to cognitive function.
28 Poly unsaturated fatty acid supplementation has also been reported to improve symptoms in BD, 29 although it is not yet clear whether cognitive function is enhanced. In
MDD, the evidence on cognition has been more mixed.
Antypa et al 30 found an improvement in emotional decision making in recovered individuals; however, no such benefit was seen for other domains of cognition in recovered or depressed individuals in their study or by
Rogers et al.
31
Acetylcholinesterase inhibitors
Acetylcholinesterase inhibitors exert a beneficial effect on cognition by blocking acetylcholinesterase and enhancing cholinergic function. This class of agents was prescribed initially to enhance cognition in patients with Alzheimer disease and has more recently been used in psychiatric disorders, primarily schizophrenia.
32
Although preliminary evidence in smaller, uncontrolled studies of patients with BD shows some promising results, no such benefit was revealed by the majority of larger, better controlled studies in schizophrenia.
17
More promising preliminary results are suggested for MDD. Our group conducted a randomized, double-blinded, placebo-controlled pilot study of galantamine in MDD patients.
33 The galantamine-treated group (n=9) had numeric improvement on depression and cognitive measures compared with the placebo-treated group (n=10), although the groups did not differ statistically.
33 Another recent double-blind, placebo-controlled study of galantamine in patients during the course of electroconvulsive therapy found cognitive improvement for delayed memory, but not other cognitive domains.
34
Stimulants
Psychostimulants increase brain activity, thereby elevating alertness, mood, and awareness. Primarily used in attention deficit hyperactivity disorder (ADHD), stimulants have been demonstrated to facilitate broad areas of cognition. Modafinil is recommended as a second-line choice for comorbid BD and ADHD.
35 Modafinil, a wakefulness agent, has been investigated in a few studies in schizophrenia. Open trials of modafinil added to antipsyexecutive function, working memory, and visual memory.
17 Given, the findings in schizophrenia, modafinil may be of use in patients with mood disorders as well, but further research is needed.
17
Case Study (cont.)
The neuropsychologist recommends that the client break up tasks into smaller components to reduce reliance on executive processing and memory, and that she resume her exercise routine. He refers her for cognitive-behavioural therapy to help manage remaining subthreshold depression symptoms and to develop a plan to manage anxiety, which is likely further hindering her work performance. She was educated that lithium may be playing a small role in some of her cognitive deficits and is encouraged to continue to discuss medication management with her psychiatrist.
Conclusion
Both MDD and BD are associated with persistent cognitive deficits in at least a portion of patients. These cognitive deficits can be measured using standardized neuropsychological tests.
Given the role of cognition in facilitating superior day-to-day functioning, treatment of cognitive deficits are necessary to reduce the human and economic costs of the disorders.
Currently, most psychotropic medications do not improve or may actually worsen cognitive deficits. Further research is needed in patients with mood disorders to evaluate the efficacy of psychostimulants, fatty acid supplementation, and other agents such as N-acetylcysteine. Newer nonpharmacological interventions, such as cognitive remediation therapy and exercise, suggest beneficial effects and are associated with minimal risk. The evaluation and targeted treatment of cognitive deficits in patients with mood disorders needs to be incorporated as routine components of a comprehensive treatment plan.
Dr. Goghari is an Associate Professor, Departments of
Psychology and Psychiatry, University of Calgary, and a registered neuropsychologist, Calgary, Alberta. Dr. MacQueen is a
Professor, Department of Psychiatry, University of Calgary,
Calgary, Alberta, and an Adjunct Clinical Professor, University of Toronto, Toronto, Ontario.
References:
1.
World Health Organization. The Global Burden of Disease: 2004 Update. Part 3 - Disease inci-
2.
dence, prevalence and disability. Geneva (Switzerland): WHO Press; 2008.
Goeree R, Farahati F, Burke N, et al. The economic burden of schizophrenia in Canada in
3.
2004. Curr Med Res Opin . 2005;21(12):2017-2028.
McIntyre RS, Cha DS, Soczynska JK, et al. Cognitive deficits and functional outcomes in major depressive disorder: determinants, substrates, and treatment interventions. Depress
Anxiety . 2013;30(6):515-527.
4.
5.
6.
7.
Bearden CE, Woogen M, Glahn DC. Neurocognitive and neuroimaging predictors of clinical outcome in bipolar disorder. Curr Psychiatry Rep . 2010;12(6):499-504.
Andreou C, Bozikas VP. The predictive significance of neurocognitive factors for functional outcome in bipolar disorder. Curr Opin Psychiatry . 2013;26(1):54-59.
Gottfredson LS. Mainstream science on intelligence: An editorial with 52 signatories, history, and bibliography (Reprinted from The Wall Street Journal , 1994). Intelligence.
1997; 24:13-23.
Chan RC, Shum D, Toulopoulou T, Chen EY. Assessment of executive functions: review of instruments and identification of critical issues. Arch Clin Neuropsychol. 2008;23(2):201-216.
8.
9.
Lee RS, Hermens DF, Porter MA, Redoblado-Hodge MA. A meta-analysis of cognitive deficits in first-episode Major Depressive Disorder. J Affect Disord . 2012;140(2):113-124.
McDermott LM, Ebmeier KP. A meta-analysis of depression severity and cognitive function.
J Affect Disord . 2009;119(1-3):1-8.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
Fleming SK, Blasey C, Schatzberg AF. Neuropsychological correlates of psychotic features in major depressive disorders: a review and meta-analysis. J Psychiat Res. 2004;38(1):27-35.
Mann-Wrobel MC, Carreno JT, Dickinson D. Meta-analysis of neuropsychological functioning in euthymic bipolar disorder: an update and investigation of moderator variables.
Bipolar Disorders. 2011;13(4):334-342.
Bora E, Yucel M, Pantelis C, Berk M. Meta-analytic review of neurocognition in bipolar II disorder. Acta Psychiatr Scand.
2011;123(3):165-174.
Bora E, Yucel M, Pantelis C. Neurocognitive markers of psychosis in bipolar disorder: a meta-analytic study. J Affect Disord.
2010;127(1-3):1-9.
Wingo AP, Wingo TS, Harvey PD, Baldessarini RJ. Effects of lithium on cognitive performance: a meta-analysis. J Clin Psychiatry.
2009;70(11):1588-1597.
Wagner S, Doering B, Helmreich I, Lieb K, Tadic A. A meta-analysis of executive dysfunctions in unipolar major depressive disorder without psychotic symptoms and their changes during antidepressant treatment. Acta Psychiat Scand.
2012;125(4):281-292.
Dias VV, Balanza-Martinez V, Soeiro-de-Souza MG, Moreno RA, Figueira ML, Machado-
Vieira R, Vieta E. Pharmacological approaches in bipolar disorders and the impact on cognition: a critical overview. Acta Psychiat Scand. 2012;126(5):315-331.
Goldberg JF, Chengappa KN. Identifying and treating cognitive impairment in bipolar disorder. Bipolar Disord . 2009;11(Suppl 2):123-137.
Keefe RSE, Bilder RM, Davis SM, et al. Neurocognitive effects of antipsychotic medications in patients with chronic schizophrenia in the CATIE trial. Arch Gen Psychiatry . 2007;64(6):
633-647.
Jaeggi SM, Buschkuehl M, Jonides J, Perrig WJ. Improving fluid intelligence with training on working memory. Proc Natl Acad Sci U S A. 2008;105(19):6829-6833.
Anaya C, Martinez Aran A, Ayuso-Mateos JL, et al. A systematic review of cognitive remediation for schizo-affective and affective disorders. J Affect Disord. 2012;142(1-3):13-21.
Meusel LA, Hall GB, Fougere P, McKinnon MC, MacQueen GM. Neural correlates of cognitive remediation in patients with mood disorders. Psychiatry Res. 2013;214(2):142-152.
van Praag H, Shubert T, Zhao C, Gage FH. Exercise enhances learning and hippocampal neurogenesis in aging mice. J Neurosci. 2005;25(38):8680-8685.
Cotman CW, Berchtold NC, Christie LA. Exercise builds a healty brain: key roles of growth factor cascades and inflammation. Trends Neurosci. 2007;30(9):464-472;.
Vasques PE, Moraes H, Silveira H, Deslandes AC, Laks J. Acute exercise improves cognition in the depressed elderly: the effect of dual-tasks. Clinics (Sao Paulo). 2011;66(9): 1553-1557.
Kubesch S, Bretschneider V, Freudenmann R, et al. Aerobic endurance exercise improves executive functions in depressed patients. J Clin Psychiatry. 2003;64(9):1005-1012.
Hoffman BM, Blumenthal JA, Babyak MA, et al. Exercise fails to improve neurocognition in depressed middle-aged and older adults. Med Sci Sports Exerc. 2008;40(7):1344-1352.
Luchtman DW, Song C. Cognitive enhancement by omega-3 fatty acids from child-hood to old age: findings from animal and clinical studies. Neuropharmacology. 2013;64:550-565.
Karr JE, Alexander JE, Winningham RG. Omega-3 polyunsaturated fatty acids and cognition throughout the lifespan: a review. Nutr Neurosci. 2011;14(5):216-225.
Turnbull T, Cullen-Drill M, Smaldone A. Efficacy of omega-3 fatty acid supplementation on improvement of bipolar symptoms: a systematic review. Arch Psychiatr Nurs. 2008;22(5):
305-311.
Antypa N, Smelt AHM, Strengholt A, Van der Does AJW. Effects of omega-3 fatty acid supplementation on mood and emotional information processing in recovered de pressed individuals. J Psychopharmacol. 2012;26(5):738-743.
Rogers PJ, Appleton KM, Kessler D, et al. No effect of n-3 long-chain polyunsaturated fatty acid (EPA and DHA) supplementation on depressed mood and cognitive function: a randomised controlled trial. Br J Nutr. 2008;99(2):421-431.
Cummings JL. Cholinesterase inhibitors: A new class of psychotropic compounds. Am J
Psychiatry. 2000;157(1):4-15.
Elgamal S, MacQueen G. Galantamine as an adjunctive treatment in major depression. J Clin
Psychopharm. 2008;28(3):357-359.
Matthews JD, Siefert CJ, Blais MA, et al. A double-blind, placebo-controlled study of the impact of galantamine on anterograde memory impairment during electroconvulsive therapy. J ECT. 2013;29(3):170-178.
Bond DJ, Hadjipavlou G, Lam RW, et al. The Canadian Network for Mood and Anxiety
Treatments (CANMAT) task force recommendations for the management of patients with mood disorders and comorbid attention-deficit/hyperactivity disorder. Ann Clin Psychiatry.
2012;24(1):23-37.
The authors stated that they have no disclosures to report in association with the contents of this issue.
Change of address notices and requests for subscriptions to Mood and
Anxiety Disorders Rounds are to be sent by mail to P.O. Box 310, Station
H, Montreal, Quebec H3G 2K8 or by fax to (514) 932-5114 or by e-mail to info@snellmedical.com. Please reference Mood and Anxiety Disorders
Rounds in your correspondence. Undeliverable copies are to be sent to the address above. Publications Post #40032303
A PARTNERSHIP FOR INDEPENDENT MEDICAL EDUCATION
Mood and Anxiety Disorders Rounds is made possible through independent sponsorships from
Lundbeck Canada Inc.
AstraZeneca Canada Inc.
•
Bristol-Myers Squibb Canada
•
Pfizer Canada Inc.
© 2014 CANMAT or the Canadian Network for Mood and Anxiety Treatments, which is solely responsible for the contents. Publisher: SNELL Medical Communication Inc. in co operation with CANMAT. Mood and Anxiety Disorders Rounds is a trademark of SNELL Medical Communication Inc.
All rights reserved. The administration of any therapies discussed or referred to in Mood and Anxiety Disorders Rounds should always be consistent with the recognized prescribing information in Canada.
SNELL Medical Communication Inc.
is committed to the development of superior Continuing Medical Education.
144-011E