ACC Guidelines for Preoperative Testing: A Practical Approach in a

ACC Guidelines for Preoperative Testing: A Practical Approach in a Major Academic Center
Laureen L. Hill MD, MBA and Michael J. Andritsos, MD
CASE STEM
ID: 68 year old woman presents for TAH-BSO, lymph node dissection and tumor debulking for ovarian cancer.
PHx: HTN, Obesity (BMI 32), AODM, Hyperlipidemia, Hypothyroidism, GERD, TIA 2006
Meds: HCTZ, Glyburide, Lovastatin, Synthroid, Famotidine, ASA
SHx: Denies tobacco, alcohol, illicit drug use
FHx: Father died age 68, MI; Mother died age 72, stroke, CHF
ROS: SOB with one flight of stairs; Heartburn
PE: 160/82 SR 84 SpO2 96%
RRR no m/r/g. No bruits, no JVD
Breath sounds decreased at bases; no rales or wheezing
Abdomen obese, mildly distended
Extremities warm, 1+ dependent pitting edema
Neurological exam non-focal
QUESTIONS
1. What are the most relevant considerations in this patient’s initial preoperative evaluation?
2. Does she need additional cardiac work-up? If so, what would you request and why?
3. Does the fact that this patient has cancer influence your decision-making?
4. If she were instead presenting for an elective hip replacement, how would you proceed?
5. Would you consider her medically optimized? Why?
ANSWERS
1. According to the ACC/AHA guidelines and algorithm (1), this patient has no evidence of active cardiac conditions unless further investigation proves otherwise, (i.e. “heartburn” as angina equivalent, possible silent ischemia in this diabetic female). She has one clinical risk factor (diabetes mellitus), and one minor risk predictor (uncontrolled hypertension). The surgery is an intermediate risk procedure that poses moderate physiologic stress and risk with a potential for substantial blood loss and fluid shifts (2-4). The patient’s functional exercise capacity appears limited at this time and further investigation is warranted although given the patient’s age, obesity and existing co-morbidities we would anticipate that her functional capacity is not greater than 4 METS. Other considerations would include effects of her obesity on cardiopulmonary function, OSA risk and airway management, systemic manifestations of her diabetes, abnormal chest exam, perioperative plans for glucose control, suboptimal BP control and status of thyroid function.
2. A preoperative 12-lead ECG (Class IIb indication) would be reasonable in this patient with at least one clinical predictor undergoing intermediate risk surgery. In addition, this obese patient may have evidence of right heart strain from obesity-related obstructive sleep apnea, hypoventilation syndrome and/or restrictive lung disease. According to the guidelines, an abnormal ECG is a minor risk predictor and does not necessarily indicate further testing is warranted; however, pathologic Q waves would be considered a clinical risk factor that would be incorporated into treatment recommendations. In patients undergoing intermediate risk surgery with one or more clinical risk factors and marginal functional capacity, noninvasive testing may be warranted if it is likely to alter management. It is also reasonable to proceed
with surgery with good medical management including tight heart rate control, although the literature regarding beta blockade is conflicting in all but the high risk population undergoing vascular surgery and those already taking beta-adrenergic antagonists. (8)
3. The fact that the patient does have cancer may potentially alter management strategies. Depending on the degree of cancer invasiveness and aggressiveness, assessment should be curtailed to identify or optimize those abnormalities that may have the greatest immediate impact on patient care in the perioperative period.
4. Having an elective surgery affords the luxury of having time to prepare the patient for surgery by stabilizing disorders in a timely and efficient manner with proper clinical judgment. This entails optimizing the organ systems necessary for minimizing the risk associated with this surgery. Unlike the patient requiring more urgent cancer surgery, an elective patient in whom cardiac testing reveals high-risk coronary anatomy and in whom long-term outcome would be improved by coronary bypass grafting should generally undergo coronary revascularization before elective noncardiac surgery. Percutaneous coronary intervention (PCI) has no role in preoperative revascularization except in those patients with acute coronary syndrome where PCI is independently indicated. (1)
5. Further management to optimize blood pressure is warranted since this is an independent risk factor for perioperative myocardial ischemia and stroke. (1) Perioperative beta-blockade may not be beneficial in this patient with only one clinical risk factor undergoing intermediate risk surgery. Conflicting trial results (5-7) and the uncertainty of the potential harm of the perioperative use of beta-blockers make use of beta-blockers beneficial when they are prescribed only to patients in the Class I and IIa recommendations (8). For optimal effect when indicated, long-acting agents should be started days to weeks before the planned surgery and titrated to achieve heart rate goals. Statin therapy should be continued (Class I recommendation). (1, 9-10) Secondary prevention with low dose aspirin reduces the risk of stroke, myocardial infarction and cardiovascular death and its withdrawal prior to surgery may have deleterious effects. Low-dose aspirin may increase bleeding complications perioperatively. Aspirin increases the frequency of bleeding by approximately 50% but does not increase the level of severity of bleeding or the perioperative mortality due to bleeding complications with possible exceptions like prostatectomy or intracranial surgery. Conversely, discontinuation of low-dose aspirin may lead to stroke, myocardial infarction or cardiovascular death by exclusion of its cardioprotective effects and by rebound phenomenon. It is suggested that low-dose aspirin as a secondary prevention be only discontinued if the known or presumed bleeding risks are expected to be more or equally severe than the observed cardiovascular risk (myocardial infarction, stroke, peripheral vascular occlusion, or cardiovascular death) after withdrawal. (11)
References
1.
Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, Freeman WK, Froehlich
JB, Kasper EK, Kersten JR, Riegel B, Robb JF. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Circulation .
2007; 116:1971-1996.
2.
Halaszynski TM, Juda R; Silverman DG. Optimizing postoperative outcomes with efficient preoperative assessment and management. Crit Care Med . 2004; 32(4):S76-S86.
3.
Pasternack LR: Screening patients: Strategies and studies. In: Ambulatory Anesthesiology—A Problem-
Oriented Approach. McGoldrick K (Ed). Baltimore, Williams & Wilkins, 1995.
4.
Roizen MF: Preoperative testing. In: Handbook of Preoperative Assessment and Management. Schweitzer
BJ (Ed). Philadelphia, Lippincott, Williams & Wilkins, 2000.
5.
Juul AB, Wetterslev J, Gluud C, et al . Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo-controlled blinded multicenter trial. BMJ .
2006; 332:1482-1485.
6.
Yang H, Raymer K, Butler R, et al . The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J . 2006; 152:983–990.
7.
POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomized controlled trial. Lancet . 2008; 371:1839-1847.
8.
Brett AS. Coronary assessment before noncardiac surgery: current strategies are flawed. Circulation . 2008;
117:3145-3151.
9.
Daumerie G, Fleisher LA. Perioperative b-blocker and statin therapy. Curr Opin Anesthesiol . 2008; 21:60-
65.
10.
Hindler K, Shaw AD, Samuels J, et al . Improved postoperative outcomes associated with preoperative statin therapy. Anesthesiology . 2006; 105:1260-72.
11.
Burger W, Chemnitius JM, Kneissl GD, Rucker G. Low-dose aspirin for secondary cardiovascular prevention-cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation – review and meta-analysis. J Int Med . 2005; 257:399-414
12.
Stoelting RK, Dierdorf SF: Endocrine Diseases. In : Anesthesia and Coexisting Disease 4 th ed.
Philadelphia, Churchill Livingstone, 2002.
13.
Lipshutz AK, Gropper MA. Perioperative glycemic control. Anesthesiology. 2009; 110:408-21.
14.
Armstrong D. Ovaries and Fallopian Tubes. In : Abeloff’s Clinical Oncology, 4 th
ed. Abeloff MD, et al .
(Ed). Philadelphia, Churchill Livingston, 2008.
15.
Gregoratos G. Current guideline-based preoperative evaluation provides the best management of patients undergoing noncardiac surgery. Circulation . 2008; 117:3134-3144.
16.
. Halaszynski TM, Juda R; Silverman DG. Optimizing postoperative outcomes with efficient preoperative assessment and management. Crit Care Med . 2004; 32(4):S76-S86
17.
Dexter F. Design of appointment systems for preanesthesia evaluation clinics to minimize patient waiting times: a review of computer simulation and patient survey studies. Anesth Analg . 1999; 89:925-31
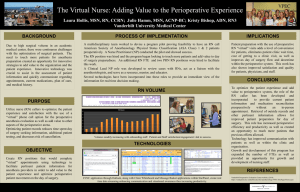
ACC/AHA Algorithm for cardiovascular evaluation (1)
Perioperative Risk Predictors (1)
Active Cardiac Conditions
Acute coronary syndromes
Decompensated heart failure
Significant arrhythmias
Severe valvular disease
Clinical Risk Factors
Hx of ischemic heart disease
Hx of compensated or prior HF
Hx of cerebrovascular disease
Diabetes mellitus
Renal insufficiency (Cr >2mg/dL)
Minor Risk Predictors
Age > 70
Abnormal ECG
Rhythm other than sinus
Uncontrolled HTN
Cardiac Risk of Noncardiac Surgical Procedures (1)
Risk Stratification
Vascular (reported cardiac risk > 5%)
Intermediate (reported cardiac risk 1-5%)
Low (reported cardiac risk
<1%)
Procedure Examples
Aortic and other major vascular surgery
Peripheral vascular surgery
Intraperitoneal and intrathoracic surgery
Carotid endarterectomy
Head and neck surgery
Orthopedic surgery
Prostate surgery
Endoscopic procedures
<1%) Superficial procedure
Cataract surgery
Breast surgery
Ambulatory surgery
Algorithm for Antiplatelet Agents (1)
So you’re in charge of the preoperative clinic……………now what??
Considerations in Starting / Managing a Preoperative Assessment Clinic
•
Define the entire scope of clinic services and functions within the organization o Anesthesiology evaluation o H&P completion o Laboratory orders and follow-up o Diagnostic workups and follow-up o Referrals for consultation and follow-up o Medical optimization o Preoperative chart preparation o Others?
• Define if clinic visits will be optional or mandatory o Impact on scheduling / staffing / workflow o Will patients be scheduled or walk-ins?
o If not mandatory, how will you incent surgeons to refer patients?
o How will patients not seen in clinic be evaluated prior to surgery? Inpatients?
o How do you handle patients travelling great distances to the institution?
• How will you staff the clinic and what type of providers will you use?
o Anesthesiologists / Internists / Others o Physicians / Advanced practice staff / Nurses / Med Assts / Pt Care Techs/ Pharm o Will all providers see all patient types or will you institute a triage process?
o Who will be responsible for management of the clinic?
• Guidelines / Protocols / Algorithms / Patient Instructions o Standardize practice within the clinic o Maintain a uniform approach within the department o Getting buy-in within the department and organization
• Who will bear the costs of the preoperative clinic?
o Department / Hospital / Partnership o Can you bill for professional services? Facility fees?