Blood Lead Levels in Mexico and Pediatric Burden of Disease
advertisement

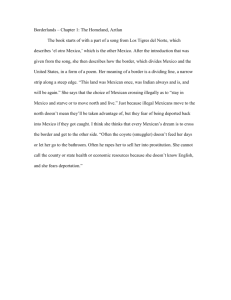
ARTICLES AND REVIEWS Blood Lead Levels in Mexico and Pediatric Burden of Disease Implications Jack Caravanos, DrPH, CIH, Russell Dowling, MPH, Martha María Téllez-Rojo, Dra, Alejandra Cantoral, ScD, Roni Kobrosly, PhD, MPH, Daniel Estrada, Manuela Orjuela, MD, ScM, Sandra Gualtero, MSc, Bret Ericson, MSc, Anthony Rivera, and Richard Fuller ABSTRACT Background: Although there has been success in reducing lead exposure with the phase-out of leaded gasoline, exposure to lead in Mexico continues to threaten the health of millions, much of which is from lead-based glazes used in pottery that leaches into food. Objectives: An extensive historical review and analysis of available data on blood lead levels in Mexican populations was conducted. We used a calculated geometric mean to evaluate the effect of lead on the pediatric burden of disease. Methods: An extensive bibliographic search identified 83 published articles from 1978 to 2010 with blood lead level (BLL) data in Mexican populations representing 150 data points from more than 50,000 study participants. Values from these publications were categorized into various groupings. We then calculated the incidence of disease and disability-adjusted life-years resulting from these BLLs using the World Health Organization’s burden of disease spreadsheets for mild mental retardation. Results: Reviewing all relevant studies, the geometric means of Mexican BLLs in urban and rural areas were found to be 8.85 and 22.24 ug/dL, respectively. Since the phase-out of leaded gasoline, the mean in urban areas was found to be 5.36 ug/dL and the average in rural areas is expected to be much higher. The U.S. Centers for Disease Control and Prevention’s (CDC) upper limit of blood lead in children under the age of 6 years is 5 ug/dL and the current U.S. average is 1.2 ug/dL. Our results indicate that more than 15% of the population will experience a decrement of more than 5 IQ points from lead exposure. The analysis also leads us to believe that lead is responsible for 820,000 disability-adjusted life-years for lead-induced mild mental retardation for children aged 0 to 4 years. Conclusion: Lead continues to threaten the health of millions and remains a significant cause of disability in Mexico. Additional interventions in reducing or managing lead-based ceramic glazes are necessary to protect the public health. Key Words: lead, blood lead level, burden of disease, children, DALY, disability-adjusted life-year, pottery, Mexico 2014 Icahn School of Medicine at Mount Sinai. Annals of Global Health 2014;80:269-277 INTRODUCTION 2214-9996/ª 2014 Icahn School of Medicine at Mount Sinai From the Environmental and Occupational Health Sciences Program, City University of New York, School of Public Health, New York, NY (JC); Blacksmith Institute, New York, NY (JC, RD, RK DE, SG, BE, AR, RF); Instituto Nacional de Salud Pública, Universidad No. 655 Colonia Santa María Ahuacatitlán, Cerrada Los Pinos y Caminera C.P. Cuernavaca, Morelos, México (MMT-R, AC); Department of Preventive Medicine, Icahn School of Medicine at Mount Sinai, New York, NY (RK); Departments of Pediatrics and Environmental Health Sciences, Columbia University, New York, NY (MO). Address correspondence to J.C.; e-mail: jcaravan@hunter. cuny.edu All authors declare they have no conflicts of interest. Funding for this article was provided by Blacksmith Institute, New York, NY. Supplemental material attached to journal articles has not been edited, and the authors take responsibility for the accuracy of all data. http://dx.doi.org/10.1016/j.aogh.2014.08.002 Mexico, with its extensive lead ore deposits and widespread use of lead-glazed pottery, has a long and unique history of lead exposure. Through technology and tradition, lead continues to threaten the health of millions living in the country. In 1990, Mexico began phasing out leaded gasoline and introduced unleaded fuels.1 Leaded gasoline was completely phased out in Mexico by 1997. The reduction of leaded gas has been linked to improved health outcomes,2,3 however other means of exposure still burden the people of Mexico. Mining and secondary smelting also pose occupational and environmental health risks. Mexico is the fifth largest producer of lead worldwide at 220,000 metric tons in 2013 and has reserves of more than 5.6 million tons.4 Three mining companies process lead ore from 13 mines operating in the states of Chihuahua, Coahuila, 270 Mexico Blood Lead Levels Durango, Guererro, Hidalgo, San Luis Potosi, Sinaloa, Sonora, and Zacatecas.5 Mexico is also one of the world’s top 5 exporters of silver, often mined alongside lead ore, and is a large producer, exporter, and recycler of lead-acid storage batteries commonly used in automobiles and lories.6,7 Leaded paints are a persisting health problem. The Comex Group, North and Central America’s fourth largest architectural paint manufacturer, and Sherwin Williams S.A. de C.V., operate in Mexico’s large paint and coatings production industry.8 A 2008 study revealed that all tested samples of enamel paint contained lead concentrations greater than 90 ppm (the regulatory limit in China and the United States); plastic paints on average contained 6 ppm.9 A secondary source of general lead exposure in the population is ceramic glazes used in traditional earthenware. Leaded glazes were first introduced by the Spanish in the 16th century and are still used widely.10 Unfortunately, the vast majority of Mexican ceramic kilns are wood-fired, as opposed to gas found elsewhere in the world, and do not reach the fusing/sintering temperatures necessary to vitrify lead glazes to where they are unleachable (temperature >1200 C). According to the only census to date, at least 10,000 pottery workshops use leaded glazes in wood-fired kilns.11 The problem is compounded because many workshops are connected to living and cooking areas, making area contamination prevalent. These workers and their families are most acutely at risk for lead poisoning and related illnesses. A much broader exposure occurs with the use of leadglazed ceramics in the home, for meal preparation and food storage. Lead can easily leach from the glaze into food, where it is ingested. This situation is aggravated by the Mexican diet, as lead is made more leachable by the presence of heat or slight acidity such as that of lime juice.12 Although lead-glazed pottery is abundant in Mexico, poorly constructed, low-fired glazes are especially a problem in rural areas where resources are scarce. Low-income communities often are disproportionately affected. Measuring the scope of lead contamination in Mexican communities is essential to fully characterize the country’s burden of disease. This in turn helps define interventions to mitigate exposures and alleviate adverse health outcomes. In the United States, the National Health and Nutrition Examination Survey (NHANES) of the Centers for Disease Control and Prevention regularly monitors blood lead levels (BLLs). Mexico has no comparable program. In the absence of comprehensive data, we conducted an extensive historical review, cataloging those studies that incorporate BLL testing in Mexican communities. To our knowledge, this is the first such literature survey of BLL tests in Mexico. The literature on health effects from lead exposure is extensive and definitive. Lead toxicity has been linked to various cognitive impairments, lowered IQs, cardiovascular effects, low birth weight, added economic costs, overall diminished life expectancy, and possibly even increased rates of violent crime.13-19 The second component of this paper calculates the pediatric burden of disease from lead using methods developed by the World Health Organization (WHO). Using values from the literature review, we generated the attributable disability-adjusted life-years (DALYs) for pediatric exposure to lead in Mexico. We also estimated the effect on IQ, broadly providing a comparison against the United States, a country that does not have extensive exposure to lead-glazed pottery. METHODS Historical Review and Data Selection As of January 2014, a PubMed search for lead AND levels AND Mexico yielded 484 articles. Various permutations were tested to ensure a large capture with these final search terms selected. We reviewed articles in English and Spanish, including only those most relevant to the study. Our selection criteria retained 83 papers as eligible for meta-analysis. A study was included in our analysis if the authors 1) collected BLL data from populations within Mexico; 2) upheld lead as a main focus; 3) included at least 30 participants; and 4) reported BLL data from either venous, capillary, or umbilical cord samples. Studies ineligible for our meta-analysis met one or more of the following exclusion criteria: 1) did not report any BLL data and exclusively sampled from bone, organs, or other tissues; 2) lead was not the main focus of the study; 3) BLL data were reported for Mexican populations existing outside of national Mexico; 4) the study was not directly human health related; 5) the number of study participants was less than 30; 6) the paper was out of print and/or irretrievable; and 7) the study did not contain a statistical mean or SD for the original data set. Figure 1 summarizes the inclusion and exclusion criteria for studies in our analyses. Exclusion criteria removed 82% of the studies from our initial search. Because many of the publications we selected included multiple unique samples (each with a unique estimated BLL), we hereafter refer to these individual estimates as “samples.” Subgroup Rationale Mean and SD data from the 83 studies were separated into subgroups for BLL analysis based on demographic and sampling information. Means were collected based on the initial year of data collection, not the study publication year. In cases where data was collected over a period of time, we used the middle year. In instances where no collection year was provided, we used the year before article submission. The meta-analysis included data for the following subgroups: sex (male and female), age, urbanicity, workforce exposures, and blood sample source (umbilical cord—hereinafter referred to as cord samples—and venous/capillary; see Fig. 1). 271 Annals of Global Health Among age groups, the categories were defined as infant (<1 year), child and adolescent (1-14 years), and adult (15þ years). Cord blood samples, presumably taken at birth, were classified as infant along with any venous or capillary blood samples taken within the participant’s first year of life. In cases when a study did not meet our range or criteria, it was defined as “not specified.” The population density of the data collection area was used to determine “urbanicity” for each study. We used the US Census Bureau’s definition of an urbanized area (a population density of 1,000 people per square mile) to categorize each study.13 In many cases, this was a fairly straightforward assessment. For instance, any study where data were collected from Mexico City, the study was immediately coded as “urban.” Conversely, in obviously rural areas with very sparse populations (such as agricultural areas), the studies were coded as “rural.” For “suburban” areas or small cities where population density could not be determined from a Web search, our study coordinator in Mexico made the final decision. This only applied to four cases. Occupational exposure was defined as any cohort of participants that was exposed to lead due to work (typically for 8 hours/day). According to Haz-Map from the US National Institutes of Health (NIH), this includes any worker involved in mining, smelting, manufacturing with lead, ceramic or pottery workers, or painters using leaded paint. Studies involving radiator repair workers and lithographic print shop workers who were included in this review were also considered to have occupational exposure. Blood sample source was determined by distinguishing cord blood samples from venous and capillary samples. As previously noted, cord blood samples were grouped together with venous or capillary samples taken from children under the age of 1 year in a general “infant” category. Figure 1. Summary of studies included and excluded in the literature review. We excluded 82% of the articles reviewed from the literature. years included (Fig. 2). To assess temporal trends in BLLs, we created scatterplots of each study’s GM BLL against the initial year of data collection (Fig. 3 and 4). These scatterplots included a LOESS (local regression) regression Sex Female 9.5 (7.7−11.4) Male 18.5 (11.1−25.9) Meta-analysis of BLLs Due to the typically skewed distribution of blood lead data we analyzed geometric mean (GM) data. In cases where studies presented natural scale BLLs, we employed a previously described method to convert natural scale means to geometric means.14 Overall and subgroup means were calculated by weighting individual study results by their inverse variance.15,16 We tested for heterogeneity of study means through the Q statistic. If the Q statistic was statistically significant, we employed a random-effects model; otherwise we employed fixed-effects model. When analyzing subgroups (e.g., males or females), we provided Q statistic results for each subgroup and report metaregression results to test whether subgroup results differ with statistical significance. Because of the large number of constituent studies in the meta-analysis, we created a forest plot that illustrates only the overall and subgroup summary results for all Age Infant 6.5 (5.5−7.6) Child 9.7 (8.6−10.8) Adult 10.9 (8.1−13.6) Urbanicity Urban 8.9 (8.1−9.6) Rural 22.2 (13.5−31.0) Workforce Exposure Occupational 32.8 (20.2−45.5) Non−Occupational 8.9 (8.2−9.5) Blood Sample Source Cord 6.4 (5.5−7.4) Venous/Capillary 10.9 (9.4−12.5) 0 10 20 30 40 Geometric Means of Blood Lead with 95% CI's (ug/dL) Figure 2. Forest plot of all available data (150 samples). 272 Mexico Blood Lead Levels conducted with R ¼ 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria), using the “metafor” package. For all analyses, results were considered significant at P < .05. Figure 3. Scatterplot of all available data with smoothed regression lines for urban and rural sample locations.*Dot size is proportionate to the inverse variance of each sample’s estimate. The dotted-line intersecting this figure denotes the most recently available US average BLL of 1.2 mg/dL, given in geometric mean for a 95% CI. The shaded area between 1990 and 1997 indicates the total period of the tetraethanol (leaded gasoline) phase out in Mexico. line that was weighted by each study estimate’s inverse variance. The US blood lead GM of 1.2 ug/dL from 2009 to 2010 was included in the plot (as a horizontal dotted line), for visual comparison.17 A semitransparent rectangle was added to highlight the entire period of leaded gasoline phase out in Mexico (1990-1997). Our analysis was Calculating Disability-Adjusted Life-Years and IQ Impact. DALYs are a combination of 2 metrics, namely years lived with disability (YLD) and years of life lost (YLL) from a disease or health condition.18 For lead in children, we focused on mild mental retardation (MMR) as the main disability associated with increased lead exposure. Because MMR is not inherently fatal, we did not consider YLL in our analysis. To calculate YLD, the duration of the disease in years was multiplied by a disability weight (DW), which ranges from 0 to 1, indicating severity. In YLD calculations, a DW of 0 indicates perfect health, whereas a DW of 1 would indicate a full year lost to death. By way of example, low vision cataracts have a DW of 0.170 and untreated asthma has a DW of 0.043. MMR due to lead has a DW of 0.361.19 Two WHO DALY lead poisoning spreadsheets were used to calculate the DALYs from lead exposure. The first spreadsheet calculates the incidence of MMR and requires entering an estimate for the GM BLL (with a geometric SD). This spreadsheet calculates the number of children above the MMR threshold of 70 IQ points who would drop into the MMR range due to leadinduced cognitive impairment and presents the rate of lead-induced MMR per 1000 population. It also incorporates a regional adjustment ratio for MMR since Table 1. Details on Subgroups Within All 150 Samples Subgroups Within Samples Number of Samples, % Sex Female 61 (40.7) Male 20 (13.3) Not specified Age 69 (46) Infants 23 (15.3) Children and adolescents 61 (40.7) Adults 56 (37.3) Not specified 10 (6.7) Urbanicity Urban Rura Not specified 132 (88) 18 (12) 0 (0) Workforce exposures Occupational Nonoccupational Figure 4. Scatterplot of all available data with smoothed regression lines for occupation and nonoccupational exposure.*Dot size is proportionate to the inverse variance of each sample’s estimate. The dotted-line intersecting this figure denotes the most recently available US average BLL of 1.2 mg/dL, given in geometric mean for a 95% CI. The shaded area between 1990 and 1997 indicates the total period of the tetraethanol (leaded gasoline) phase out in Mexico. Not specified 10 (6.7) 140 (93.3) 0 (0) Blood sample source Cord blood Venous/capillary Not specified 16 (10.7) 134 (89.3) 0 (0) 273 Annals of Global Health Table 2. Subgroup Analysis of All 150 Samples Estimated Subgroup Geometric Subgroup Q Statistic Model Type Mean in ug/dL (with 95% CI) Sex (test for differences between subgroups: P ¼ .0009) Female Q ¼ 3862.80, df ¼ 60, P < 0.0001 Random-effects model 9.52 (7.67e11.36) Male Q ¼ 7867.66, df ¼ 19, P < 0.0001 Random-effects model 18.47 (11.05e25.89) Age (test for differences between subgroups: P ¼ 0.05) Prenatal/infant Children and adolescents Q ¼ 118.063, df ¼ 22, P < 0.0001 Q ¼ 2487.51, df ¼ 60, P < 0.0001 Random-effects model Random-effects model 6.54 (5.46e7.61) 9.70 (8.64e10.77) Adult Q ¼ 5428.29, df ¼ 55, P < 0.0001 Random-effects model 10.87 (8.10e13.63) Urbanicity (test for differences between subgroups: P < 0.0001) Urban Q ¼ 3898.77, df ¼ 131, P < 0.0001 Random-effects model 8.85 (8.09e9.62) Rural Q ¼ 5305.46, df ¼ 17, P < 0.0001 Random-effects model 22.24 (13.54e30.95) Workforce exposures (test for differences between subgroups: P < 0.0001 ) Occupational Q ¼ 3410.03, df ¼ 9, P < 0.0001 Random-effects model Nonoccupational Q ¼ 3624.74, df ¼ 139, P < 0.0001 Random-effects model Blood sample source (test for differences between subgroups: P ¼ 0.04) 32.84 (20.19e45.50) 8.85 (8.17e9.52) Cord blood Q ¼ 42.19, df ¼ 15, P ¼ 0.0002 Random-effects model 6.45 (5.52e7.38) Venous/capillary Q ¼ 13046.88, df ¼ 133, P < 0.0001 Random-effects model 10.91 (9.36e12.47) the incidence of noncongenital causes of MMR, such as anemia and meningitis, varies in different regions of the world. Additionally, the spreadsheet calculates the percentage of individuals with BLLs greater than 5 mg/dL using the size of the population and mean BLL from the population. This BLL was determined by the historical review described earlier. The GM of 6 blood lead samples from studies in Mexico with data collection occurring in 2000 or later where only general community level exposure to lead in children and adolescents could be ascertained. The second spreadsheet uses the incidence data and various population values (e.g., age groups, total population) to calculate overall DALYs and DALYs per 1000 children associated with lead-induced MMR. There is no DW associated with decrement of IQ points that does not result in MMR. DALY calculations typically incorporate only the lead-induced cognitive impairment resulting in MMR.20 A child who develops MMR from lead at birth and has a life expectancy of 80 years is said to have lived 28.9 YLDs because 80 years 0.361 equals 28.9 Although the calculation of DALYs from lead typically involves calculating YLL, which represents the premature mortality from a disease, from increases in blood pressure and the resulting cardiovascular disease, we did not include this component because the analysis is limited to children younger than age 4 years. Therefore, our DALY calculations represent solely the morbidity associated with lead exposure at these sites and does not incorporate any premature mortality associated with lead exposure. Using the initial WHO spreadsheet, we calculated the decrement of IQ points from the estimated BLLs and DALYs resulting from incident cases of MMR. This spreadsheet employed a previously developed model (2005) that documented a reduction of IQ points equal to e2.70 ln (concurrent BLL).21 Sensitivity Analysis We performed a sensitivity analysis by calculating DALYs using different discount rates and age weights. Calculation of DALYs typically incorporates a 3% discount rate due to the societal preference of a healthy year of life now versus in the future, and nonuniform age weights due to the relative societal value of certain ages.22 The notation DALYs(r,K) signifies which discount rate (r) and age weight (K) is used. We present our primary results in DALYs(3,1) including both the 3% discount rate and the full age weight. We also present DALYs(3,0) with only the 3% discount rate and DALYs(0,0) without any weighting. RESULTS Analysis of All Available Data The final data set reviewed for meta-analyses included 83 studies with participants from throughout Mexico, and resulted in 150 data samples. The data samples ranged from years 1978 to 2010, wherein years were used to define the period of sample collection and not article publication year. The BLL GMs for various subgroups are shown in Figure 2 for comparison. The dotted line indicates the current reference level for elevated blood lead as described by the CDC of 5 ug/dL.23 No international reference dose currently exists, although WHO and others use the CDC standard. GMs by subgroup are as follows: sex (males 18.5 mg/dL, females 9.5 mg/dL); age (infants 6.5 mg/dL, children and adolescents 9.7 mg/dL, adults 10.9 274 Mexico Blood Lead Levels Table 3. Geometric Means from 9 “General Exposure” Samples Collected from 2000 Onward Year of Initial Data Collection Primary Author 2000 Gomaa† 2000 Afeiche M† 2000 Study Sample Size Geometric Mean (with 95% CI)* 100 5.97 (5.44e6.56) 1000 3.02 (2.9e3.15) Torres Alanis† 207 10.55 (9.97e11.16) 2001 Lamadrid-Figueroa 207 5.22 (4.81e5.66) 2002 Ettinger 670 3.95 (3.94e3.96) 2002 2004 Vanitha Janakiraman Téllez-Rojo MM† 31 566 6.04 (4.72e7.72) 3.97 (3.79e4.16) 2004 Téllez-Rojo MM† 752 4.71 (4.5e4.93) 2004 Téllez-Rojo MM† 583 4.66 (4.44e4.88) Overall results: Q statistic: Q ¼ 30.69, df ¼ 8, P ¼ 0.002. Estimated overall geometric mean (with 95% CI) from random-effects model: 5.36 (3.90e6.82) ug/dL. *95% CI’s calculated from geometric standard deviations provided in manuscript. † Pediatric populations included in subset meta-analysis. mg/dL); urbanicity (urban 8.9 ug/dL, rural 22.2 ug/dL); workforce exposure (occupational 32.8 ug/dL, nonoccupational 8.9 ug/dL); blood sample source (umbilical cord 6.4 mg/dL, venous/capillary 10.9 mg/dL). Figures 3 and 4 depict scatterplots with LOESS regression lines for Mexican rural populations (GM 22.2 mg/dL) and urban populations (GM 8.9 mg/dL), and occupational exposure (GM 32.8 mg/dL) and nonoccupational exposure (GM 8.9 mg/dL), respectively. A dotted line intersecting Figure 2 and 3 references, for comparison, the most recently measured average BLL for the United States at 1.2 mg/dL.24 This value is given in GM with 95% confidence interval. A marker for the years 1990 to 1997 bisects Figures 2 and 3, indicating the total period of the tetraethanol (leaded gasoline) phase out in Mexico. We provide further information regarding the 150point data set in Tables 1 and 2. Here we show the composition of group populations in relation to the entire data set; therefore each subgroup totals 150 samples. More studies sampled females than males (61 of the 150 studies, 40.7% vs male 13.3% and not specified 46%). Other trends in study samples featured urban populations (88% of studies) for nonoccupationally exposed groups (93.9% of studies) tested through venous/capillary sampling (89.3% of studies). Analysis of Studies Since 2000 We analyzed recent samples (i.e., data collected since 2000) for relative comparison with modern lead toxicity standards. In all, 36 samples (GMs) met the inclusion criterion. To reflect the outcomes of general exposure, studies in which participants were at risk for occupational exposure or increased community exposures were removed from the analysis. Therefore, our general exposure analysis does not include studies in which participants faced possible increased exposure due to living near smelters, used lead-acid battery facilities, mine-tailing zones, mining regions, metal foundries, radiator repair shops, lithographic print shops, metal recycling facilities, or industrial zones. Nine samples were included in the final meta-analysis (N ¼ 4,116). The GM for BLLs in included studies since 2000, after weighting individual study results by their inverse variance, is 5.36 mg/dL. This result slightly exceeds the 5 mg/dL US Table 4. Subgroup Analysis of 9 Samples Estimated Subgroup Geometric Subgroup Q Statistic Model Type Mean in ug/dL (with 95% CI) Age (test for differences between subgroups: P ¼ 0.56) Prenatal/infant Q ¼ 1.61, df ¼ 3, P ¼ 0.66 Fixed-effects model 4.86 (3.71e6.01) Child and adolescent Adult Q ¼ 20.43, df ¼ 1, P < 0.0001 Q ¼ 1.77, df ¼ 2, P ¼ 0.41 Random-effects model Fixed-effects model 6.81 (0e14.18) 4.89 (3.60e6.18) Blood sample source (test for differences between subgroups: p ¼ 0.98) Cord blood Q ¼ 0.66, df ¼ 1, P ¼ 0.42 Fixed-effects model 5.35 (3.76e6.94) Venous/capillary Q ¼ 30.02, df ¼ 6, v < 0.0001 Random-effects model 5.37 (3.49e7.25) Overall results among 6 “general exposure” samples collected from 2000 onward that only included children, adolescents, or infants: Q statistic: Q ¼ 27.95, df ¼ 5 P < 0.0001. Estimated overall geometric mean (with 95% CI) from random-effects model: 5.52 (3.35e7.68) ug/dL, Geometric SD: 2.70. 275 Annals of Global Health Table 5. Inputs for Calculation of Lead Poisoning MMR DALYs Population (N) 117,886,000 Population (0-4 y) 11,573,000 Regional adjustment ratio 2.70 Incidence of MMR (0-4, per 1000) 5.98 Blood lead level Geometric mean BLLeSD 5.52 2.70 DALY, disability-adjusted life-year; MMR, minor mental retardation. recommended intervention level. Details are shown in Table 3. Analysis of Subgroups Since 2000 Due to the limited sample size of studies since 2000, only the age- and blood-sample category subgroups were analyzed under the Q statistic, viewable in Table 4. Each of these studies analyzes urban populations with nonoccupational exposures to lead. Studies since 2000 sample infants (4 samples, N ¼ 2,001), children and adolescents (2 samples, N ¼ 1,207), and adults (3 samples, N ¼ 908). Estimated subgroup GMs were as follows: infant, 4.86 ug/dL; child and adolescent, 6.81 ug/dL; adult 4.89 ug/dL; cord blood, 5.35 ug/dL; and venous/capillary blood, 5.37 ug/dL. IQ Deficits Associated with MMR from Lead Given the GM of 5.52 ug/dL (calculated from the 6 general exposure samples collected from 2000 onward in infants, children, and adolescents), IQ deficits associated with MMR from lead exposure were calculated as well. In a random sample of 1000 Mexican children, 156 (>15%) are expected to have a reduction of more than 5 IQ points due to lead exposure. Another 221 (>20%) are expected to have a reduction of more than 2 IQ points due to lead exposure. In its most severe cases of generalized exposure, lead is expected to cause 44 of 1000 children to have a decrease of nearly 7 IQ points. BLLs and DALYs After completing all calculations within the WHO spreadsheets for DALYs associated with lead poisoning and MMR, it was determined that the incidence rate of MMR due to lead in children aged 0 to 4 in Mexico is 5.98 per 1000 children, viewable in Table 5. The GM of 5.52 ug/dL was determined by calculating a geometric mean from 6 general exposure samples collected from 2000 onward that only included children and infants. Including a 3% discount rate and the full age weight, this amounts to 820,548 DALYs from lead-induced MMR for children aged 0 to 4 years in Mexico. Applying a 3% discount rate and no age weight, the amount is 749,839 DALYs for the same group. Without either a discount rate or age weight, this number increases to 1,920,962 DALYs. Adjustment of discounting and age weights offers a range of estimates while reflecting the relative social values of age groups.25 When compared with other sources of morbidity and mortality for children in Mexico, the DALYs associated with lead-induced MMR are extremely significant. DISCUSSION Because our meta-analysis summary represents GMs from all data within the period between 1978 and 2010, we consider this a comprehensive “historical” review. Analyses of subgroups were also essential, as some populations are predisposed to practices that lead to greater lead exposure. Our results fall in line with the expected trends in lead exposure. Furthermore, blood was chosen as the ideal sample medium for measuring lead levels most accurately. Bone also sequesters lead; however the half-life of lead in bone is approximately 20 years.26 Therefore, bone does not accurately depict the level of existing lead exposure. However, high bone lead concentrations can continue to leach Pb into the blood where systemic effects can continue. As anticipated, the GM for BLLs in males was significantly higher than the average for females; the overall average BLL for males was about 1.9 times higher than that of females. Although women make up the majority of lead-glazed pottery workers, smelting and recycling are primarily male-dominated professions in Mexico. These occupational exposures are the likely cause for the elevated levels in males. The meta-analysis showed average BLLs increased with age. This is not surprising given the half-life of lead in blood is approximately 1 month (28-36 days).27 Lead exposure from pottery is ubiquitous throughout the country, especially in poorer communities. Occupational exposures and trace levels from pre-1990 leaded gasoline are other possible exposure sources. The use of lead-glazed pottery is more common in rural areas than in urban zones.28 Additionally, lead smelting activity occurs at much higher frequencies in rural areas. Therefore, the significantly higher GMs for rural BLLs (roughly 2.5 times higher than in urban areas; overall 22.24 and 8.85 ug/dL, respectively) met our general expectations. Workforce Exposure Scatterplot In our analysis of workforce exposure, every study was classified as occupational or nonoccupational as previously described. The smoothed regression line for nonoccupational studies shows a modest and relatively steady decrease since our first data collection year of 1978. Occupational, on the other hand, appears to shows a sharp decline. This can be explained by a number of factors. First, there are several outliers in the beginning of our data collection period from the 1970s and 1980s that are necessary to show the full picture of our studies that 276 Mexico Blood Lead Levels Table 6. Relative Ranking of Childhood DALYs in Mexico Cause Lead poisoning I. Communicable, maternal, DALY 820,000 1,890, 000 perinatal, and nutritional conditions Infectious and parasitic diseases Tuberculosis sexually transmitted diseases 340,000 3000 8,000 excluding HIV Diarrheal diseases 179,000 Hepatitis 5000 Malaria <1000 Respiratory infection 301,000 Perinatal conditions (low birth weight, neonatal inf) 1,059,000 Nutritional deficiency (protein, 189,000 iodine, vitamin A, iron) II. Noncommunicable diseases Malignant neoplasms Diabetes mellitus Neuropsychiatric conditions 2,260,000 79,000 2000 715,000 (depression, bipolar, epilepsy, alcohol use, multiple sclerosis, was expected that urban blood lead samples would be lower than rural samples. Recent Sample Analysis GMs analyzed after 2000 with only community-level exposure yielded an overall GM of 5.36 ug/dL. Furthermore, for 6 general exposure samples in infants, children, and adolescents, the GM was calculated to be 5.52 ug/dL. Although the data included in the 6 samples that were used to calculate our final GM were not explicitly nationally representative, they are the best representation of general exposure lead in Mexican infants, children, and adolescents based on the recent literature. If this sample is any indication of the overall BLL mean, it means that children in Mexico have BLLs that are on average 4.7 times higher than their US counterparts (recent NHANES studies have shown the levels to be around 1.17 ug/dL).29 The upper value of the reference range is defined as 97.5% of the sampled population (1-5-year-old children in the United States). In 2012, this upper limit was estimated to be 5 ug/dL. A calculated GM of 5.52 means that nearly half of the population of Mexican children is above a value that has been demonstrated to negatively affect children’s intelligence and behavior. To compare, this is only 2.5% of children in the United States. drug use, migraine) Cardiovascular diseases 37,000 DALYs and IQ Deficits Asthma 185,000 Genitourinary diseases 39,000 Oral conditions (dental caries, 116,000 Our analysis indicates that more than 820,000 DALYs result from lead-induced MMR in Mexican children (after accounting for a 3% discount rate and full age weight). This represents an enormous source of disability in Mexico. As Table 6 shows, lead in Mexico causes more DALYs than neuropsychiatric conditions (715,000), infectious and parasitic diseases (340,000), respiratory infections (301,000), nutritional deficiency (189,000), and all injuries (473,000), among other illnesses. Lead exposure also likely results in significant IQ decrements that do not result in MMR and are therefore not captured by the DALY metric. We estimate that 15% of the population aged 0 to 4 will experience an estimated IQ decrement of more than 5 points from lead exposure, resulting in more than 8.6 million lost IQ points in Mexico for this population. periodontal disease) III. Injuries Road traffic accidents 473,000 121,000 Falls 51,000 Drownings 36,000 Other unintentional injuries 211,000 Intentional injuries (self-inflicted, 37,000 violence, war) met inclusion criteria. Additionally, only 10 samples reviewed could be classified as solely “occupational.” Therefore, this precipitous decrease in the average occupational BLLs should be reviewed cautiously. Urbanicity Scatterplot Figure 3 uses all 150 samples included in our review and every study was classified as urban or rural. The biggest sources of lead exposure in rural areas of Mexico are believed to be from the use of lead-glaze pottery, smelting, and pottery making itself. In urban areas, pottery making and residual dust from leaded gasoline have historically been the biggest sources, although lead-glazed ceramics are most likely the most significant source. In rural areas, many studies reviewed focused on subpopulations of increased exposure, such as artisanal communities, where BLLs in children are extremely high. Therefore, it Limitations There are several limitations in our analysis. Most significant among them is our reliance on a limited number of reports. In the absence of a more comprehensive dataset, we used a finite number of studies in our approach and developed estimates that we then applied to the entire Mexican population. We believe this approach, used elsewhere, is useful and illuminating, given that a large, population-based sampling of blood lead was never conducted. Similarly, many of the studies we used focused on populations known to be exposed to higher levels of environmental lead, meaning they were targeted studies and not always random population samplings. We articulated this difference by disaggregating general exposure from elevated exposure (Table 5); however, 277 Annals of Global Health the net number of general exposure population studies was limited. Finally, we assumed that the primary risk factor for elevated BLLs in the general population of Mexico was exposure to leaded ceramic glazes. We accounted for this by indicating the relative decline in leaded gasoline and lack of other known exposure pathways. This link could be better verified through further study. CONCLUSION Data compiled from 83 studies, representing 150 data points from more than 50,000 study participants, demonstrated a trend of elevated BLLs in Mexico between 1978 and 2010. The public health implications of lead contact even at low levels are predicted to have severe and chronic effects with continued exposure. Although comprehensive national data are unavailable for average population BLLs in Mexico, recent data (studies since 2000) suggests lead exposure remains a national-level public health concern. Although blood lead has decreased significantly in Mexico over the past 35 years, it remains significantly elevated. The post-leaded gasoline average BLL is still more than 4.5 times higher than the level in the US (5.52 vs 1.2 ug/dL). We estimate that this will result in 820,000 DALYs and 8.6 million fewer IQ points from leadinduced MMR in Mexican children aged 0 to 4 alone. In 2013, the Mexican Secretariat of the Interior officially censured the use of lead in ceramics.30 Affordable and effective alternative glazes exist, although uptake by artisanal cermacists has been slow. Barriers are both economic and cutural in nature. A more aggressive approach focused on both the consumer and producer might begin to make progress on this severe and insidious risk to the health of the Mexican population. Other major sources of lead—mining, smelting, and paints—compound exposure rates and health outcomes. A nationwide public health program is necessary to monitor lead levels in children that can identify hot spots and other sources of exposure for the general population, and offer intervention where needed. References 1. Environmental Protection Agency. Implementer’s Guide to Phasing Out Lead In Gasoline. 1999. Available at: http://www.epa.gov/ international/air/pdf/EPA_phase_out.pdf. Accessed April 24, 2014. 2. World Health Organization. Childhood lead poisoning. 2006. Available at: http://www.who.int/ceh/publications/leadguidance.pdf. Accessed April 3, 2014. 3. Schnaas L, Rothenberg S, Flores M, et al. Blood lead secular trend in a cohort of children in Mexico City (1987e2002). Environ Health Perspect 2004;12:1110e5. 4. US Geological Survey. Mineral commodity summary. 2014. Available at: http://minerals.usgs.gov/minerals/pubs/country/2011/myb3-2011mx.pdf. Accessed February 12, 2014. 5. Perez AA, US Geological Survey. The mineral industry of Mexico 2011 minerals yearbook: Mexico. 2011. Available at: http://minerals.usgs. gov/minerals/pubs/mcs/2014/mcs2014.pdf. Accessed July 2, 2011. 6. Guberman D. 2011 Minerals yearbook: lead advance release US geological rurvey. 2013. Available at: http://minerals.usgs.gov/minerals/pubs/ commodity/lead/myb1-2011-lead.pdf. Accessed May 7, 2013. 7. USGS. Mineral commodity summaries Reston, Virginia. 2013. Available at: http://minerals.usgs.gov/minerals/pubs/mcs/2013/mcs2013. pdf. Accessed May 7, 2014. 8. IPEN. Lead in new decorative paints. 2009. Available at: http://ipen. org/sites/default/files/documents/global_paintstudy-en.pdf. Accessed July 22, 2014. 9. IPEN. Global study to determine lead in Decorative paints in 10 countries. 2009. Available at: http://ipen.org/documents/globalstudy-determine-lead-new-decorative-paints-10-countries. Accessed July 22 2014. 10. Charleton TH. Contemporary Central Mexican ceramics: a view from the past. Man 1976;11:517e25. 11. FONART. Cómo detectar la presencia de plomo en cazuelas, olla, platos y jarros de barro esmaltado? 2009. Available at:http://alfareria.org/sites/ default/files/images/ManualPruebas.pdf. Accessed April 17, 2014. 12. Feldman N, Lamp C, Craigmill A. Lead leaching in ceramics difficult to predict. Calif Agriculture 1999;53:20e3. 13. U.S. Department of Health and Human Services. 2013. Health information technology: how is rural defined? Available at: http:// www.hrsa.gov/healthit/toolbox/RuralHealthITtoolbox/Introduction/ defined.html. 14. Higgins JPT, White IR, Anzures-Cabrera J. Meta-analysis of skewed data: combining results reported on log-transformed or raw scales. Statist Med 2008;27:6072e92. 15. Lipsey MW, Wilson D. Practical Meta-Analysis. Thousand Oaks, CA: Sage Publications; 2001. 16. Whitehead A. Meta-analysis of Controlled Clinical Trials. Chichester, UK: Wiley; 2002. 17. Centers for Disease Control and Prevention. National report on human exposure to environmental chemicals (updated tables, September 2013). 2013. Available at: http://www.cdc.gov/exposurereport/. Accessed April 22, 2014. 18. World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: WHO; 2009. 19. World Health Organization. Global burden of disease 2004 update: disability weights for diseases and conditions. 2004. Available at: http://www.who.int/healthinfo/global_burden_disease/GBD2004_ DisabilityWeights.pdf. 20. Schwartz J. Low-level lead exposure and children’s IQ: a meta-analysis and search for a threshold. Environ Res 1994;65:42e55. 21. Lanphear BP, Hornung R, Khoury J, et al. Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect 2005;113:894. 22. World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. 2009. Available at: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_ report_full.pdf. 23. The 5 ug/dL reference level is based on the 97.5th percentile of the National Health and Nutrition Examination Survey, or NHANES, blood lead distribution in children. CDC updates the reference value every four years using the two most recent NHANES surveys. Available at: http://www.cdc.gov/nceh/lead/ACCLPP/blood_lead_levels.htm. 24. Agency for Toxic Substances & Disease Registry. Lead Toxicity: What is the Biological Fate of Lead? August 20, 2010. Avilable at: http://www. atsdr.cdc.gov/csem/csem.asp?csem¼7&po¼9. Accessed May 6, 2014. 25. Mathers CD, Salomon JA, Ezzati M, Begg S, Vander Hoorn S, Lopez AD. Sensitivity and uncertainty analyses for burden of disease and risk factors estimates. In: Lopez AD, Mathers CD, Ezzati M, et al., eds. Global Burden of Disease and Risk Factors. Washington DC: World Bank; 2006:399e426. 26. Rabinowitz MB. Toxicokinetics of bone lead. Environ Health Perspect 1991;91:33e7. 27. Agency for Toxic Substances & Disease Registry. Lead toxicity: what is the biological fate of lead? Available at: http://www.atsdr.cdc.gov/ csem/csem.asp?csem¼7&po¼9. Accessed May 6, 2014. 28. Lilia AA, Badillo F. Environmental Lead in Mexico: Reviews of Environmental Contamination and Toxicology. New York: Springer; 1991:1e49. 29. US Environmental Protection Agency. Blood lead. Available at: http:// cfpub.epa.gov/roe/indicator_pdf.cfm?i¼63. Accessed April 24, 2014. 30. SEGOB. Limitaciones y especificaciones sanitarias para el uso de los compuestos de plomo. 2014. Available at: http://www.dof.gob.mx/ nota_detalle.php?codigo¼5343154&fecha¼02/05/2014.