Dobutamine stress echocardiography: A sensitive indicator of
advertisement

394
JACC Vol . N, No 2
February 1992'Iso-aui
Dobutamine Stress Echocardiography : A Sensitive Indicator of
Diminished Myocardial Function in Asymptomatic DoxorubicinTreated Long-Term Survivors of Childhood Cancer
SCOTT E . KLEWER, BS, STANLEY J . GOLDBERG, MD, FACC,
RICHARD L . DONNERSTEIN, MD, FACC, ROBERT A . BERG, MD, JOHN J. HUTTER, JR ., MD
Tucson, Arizona
Doxorubicin is an effective anticancer chemotherapeutle agent
known to cause acute and chronic cardiomyepathy . To develop a
more sensitive echocardiographic screening test for cardiac damage due to desarubicto, a cohort study was performed using
dobutandne infusion to differentiate asymptomalk long-term survivors of childhood cancer treated with doxorubicin from healthy
control subjects . Echocardiographir data from the experimental
group of 21 patients (mean age 16 t 5 years) treated from 1 .6 to
14,3 years (median 5 .3) before this study with 27 to S32 mg/m' of
dosorubicin (mean 196) were compared with echocardklgraphic
data from 12 normal age-matched control subjects . Graded
dobutamine infusions of 0 .5, 2.5, 5 and 10 pg/kg per min were
administered . Echorardiographic Doppler studies were per,
formed before infusion and after 15 min of infusion at each rate .
Dobulamine Infusion at 10 pglkg per min was discontinued after
six studies secondary to a 50% incidence rate of adverse symp ,
terns.
The most important findings were that compared with values
In control subjects, end-systolic left ventricular posterior wall
dimension and percent of left ventricular posterior wall thickening
in doxorubkhe4reated patients were decreased at baseline study
and these findings were more clearly delineated with dobutamine
stimulation . End-systolic left ventricular posterior wall dimension
at baseline for the doxorubkia-orated group was Il s 1 .9 mm
versus 13.1 z 1 .5 mm for control subjects (p < 0 .01) . End-systolic
left ventricular posterior wall dimension at the S-pg/kg per min
dobutamine infusion for the doxorublein-treated group was 14 .1
t 2.4 mm versus 19 .3 s 2.6 mm for control subjects (p < 0.01).
Percent left ventricular posterior wall thickening at baseline for
the doxorubieles-treated group was 78 t 18% versus 97 t 13% far
the control group (p < 0.01). Percent left ventricular posterior
wall thickening at itte 5-p/kg per min dobutamine infusion for
the doxorubicin-treated group was 121 37% versus 185 20%
for the control group in < 0.01). Decreased left ventricular
shortening fraction and Increased left ventricular end-systolic
meridional wall stress were demonstrated in doxorubkin-treattd
patients only during dobatamine infusion . No differences were
found between results in control subjects and deco ublcin-treated
patiens for measured diastolic variables.
Thos, usymptom ate long-term survivors of childhood cancer
treated, with doxorubicia may have latent decreased cardiac
performance That is undetected by community used echucardlographic methods, Including rest left ventricular xhneOning fray
Doxorubicin (Adniamycin) is a widely employed and effective chemotherapeutic agent, but dose-related cardiotoxicity
limits its usage (1-10). Numerous noninvasive methods .
including radionuclide angiography and echocardi braphic
assessments of systolic and diastolic function (10-19), have
been utilized to detect subclinical doxorubicin-induced cardiomyopathic changes. Dobutamine stress echocardiography was recently reported (20) to be an accurate noninvasive diagnostic technique for detecting cardiac dysfunction
in adults with coronary artery disease . Our purpose was to
determine if inotropic challenge with dobutamine could
unmask in asymptomatic doxorobicin-treated long-term survivors of childhood cancer echocardiographic abnormalities
in cardiac function not present in healthy normal control
subjects .
From the University of Arizona College of Medicine and Steele Memorial
Children's Research Center. Tucson. Arizona. This study was supported
by
the Pediatric Cardiology Research Fund . the Cancer Research Fond . and the
National Institutes of Health Short Term Research Training for Students in
Health Professional Schools . University of Arizona College of Medicine .
Tucson . Arizona .
Manuscript received May I, 1991 : revised manuscript received August 28.
1991 . accepted September 6, 1991 .
Mdress for eondnts : Stanley I . Goldberg, MD. Department of Pediatrics
(Cardiology). University of Arizona College of Medicine, 1501 Noah Campbell Avenue, Tucson, Arizona 85724 .
01992
ton goad left ventricularend-systetk merludlmW
wao stress.
Our
data establish that evaluation of eD ventricular systolic fe canon
by end-systolic posterior woll dimension, posterior wall thickening, rod-systolic merHbnat
wall
stress and shortens g fraction
measured during laotropic stimulation with dohutmtdae provides
a sensitive technique far examining the cardiac status of asymptomatic doxo ubkiu-treated patients .
(J Am Coil Cardiaf 1991;/9;394-401)
Methods
Study subjects. The study group consisted of children
and young adults previously treated with doxorubicin at our
by The American College of Canho!ogy
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
0775-109719051 . a1
IACC Vol. 19 . N9 . 2
Fesmary 1992 .394-4111
KLEW ER ET AL .
CARDIAC EVALUAtoON BY DOROTAMINE ECHOCARDIOGRAPHY
institution for childhood cancers. Control subjects were
healthy normal siblings of the doxorubicin-treated group or
age-matched volunteers . Subjects gave informed consent .
and if the subject was a minor, parents also gave consent
according to a protocol approved by the institutional Human
Subjects Committee, Because the objective was to evaluate
asymptomatic doxorubicin-treated patients. patients with
congenital heart disease, cardiac failure and arrhylhmias and
those taking cardiac medications were excluded . Pregnancy
in patients and control subjects was excluded by urine
beta-human chorionic gonadotropin test .
Standard measurements. Age . height and weight were
obtained and body surface area was computed (21) for each
subject. During the period of study, heart rate aid rhythm
were monitored continuously ; bled pressure was measured
every 5 min by sphygmomanometry .
Echncardlography. Echocardiographic examiners were
unfamiliar with the clinical states of the subjects . The heart
was imaged with a Biosound ND256-8 or Hitachi CVC-151
echocardiographic system . A baseline two-dimensional
echocardiohraphic assessment was performed to rule out
structural heat, disease . Parasternai shun-axis view-, of the
left ventricle were imaged to assess symmetry of contraction
(16) . M-mode echocardiograms of the left ventricle from the
parastemal short axis were recorded in a standard manner
(22).. gain was adjusted initially to reveal only pericardia!
mahon, then gradually increased to image left ventricular
posterior wall motion . Apical four-chamber planes that
provided good visualization of the mitral anutus and leaflets
were obtained by placing subjects in the left lateral decubitus
position. With the subjects in this positron, Doppler examination of mitral flow velocity was performed with the rangegated pulsed Doppler technique; the ultrasourd beam was
aligned as parallel to flow as possible with the sample volume
positioned at the tips of the mitral leaflets . From this position
it was also possible to record a diminished amplitude of
aortic valve closure for measurement of left ventricular
isovolumetric relaxation time . Recordings were registered at
the rate of 100 min/s . Doppler flow velocity in the ascending
aorta and aortic diameter for computation of aortic flow were
obtained from the suprasternal notch by using a 25° off axis
transducer designed for this purpose (23) .
Dobutamine infusion. After baseline recordings were obtained, continuous dobutamine infusion was initiated at
0.5 ,ag/kg per min and increased to 2 .5, 5 and 10 pg/kg per
min. To attain steady state dobutamine concentration, dobutamine was infused at each rate for 15 min before echocardiographic examination (24) and the echocardiogram was
performed between the 15th and 20th min . The infusion rate
was increased after completion of the Doppler echocardiographic studies at each dobutamine dose .
Dobulamine infusion was terminated because of any of
these complications : I) arrhythmias ; 2) an increase in blood
pressure >30% above baseline values or a decrease to >20%
below baseline ; 3) an increase in heart rate >40% above
baseline ; and 4) significant subject discomfort or anxiety .
395
Echocardiographic measurements, Left ventricular cavity
and posterior free wall dimensions at end-diastole (LV ro
and LVPW EO) and end-systole (LVES and LVPW ES) were
measured in cm according to American Society of Echocardiography criteria (22) with an average of 3 to 5 cycles
reported . Left ventricular shorts ing fraction (SF) was computed according to the method of Gutgesell et al . (25) with
the equation
SP =
loo%
x ILVEn - LVES)ILVEO .
Left ventricular posterior wall percent chickening
(%,LVPW,mek,,,;ra), which is independent of body surface
area (26), was calculated by this equation :
7.LVPW
4 = 10017, x
ILVPWES - LVPWc0)/LVPWea .
Left ventricular end-systolic meridional wall so, .ss
g/cm2 was calculated according to the method
(ESsraess) in
of Grossman et al . (27,28) with use of this equation :
ESSwess =
[I 1 .35)(MBP)(LVc
)1 / [(4)(LVPWES)(I + LVPWESILVES)) ,
where MBP = mean blood pressure as an estimate of
end-systolic pressure in mm Hg and 1 .35 is the factor to
convert pressure from mm Hg to g/cm 2 . Mean blood pressure was estimated by the equation MBP = (2DBP +
SBP)/3 . where DBP = diastolic blood pressure and SBP =
systolic blood pressure . Left ventricular isovolumetric relaxation time was measured with a digitizer at a 1Gsolution of
I ms from aortic valve closure to the first upstroke of
diastolic mitral flow velocity . Mitral deceleration time was
measured from the peak of the mitral inflow wave to the
point where the extrapolated deceleration velocity crossed
baseline. Peak mitral E and A wave filling velocities were
measured according to the method of Nishimura et al . (29) .
Ascending aortic flow was measured and computed by the
method of Locher et al. (30) with an average of 9943 cycles
reported. Angular correction was not used because alignment with flow in all planes was possible.
Statistical analysts . Data for the study group were compared with those for the control group by using the unpaired
Student r test . Simple linear regression was utilized in the
experimental group to assess the relation between echocardiographic measurements and doxorubicin cumulative dose,
age during doxorubicin treatment and time since last doxornbicin dose. All data are reported as mean values t SD.
Results
Study subjects (Table 1) . The control group was composed of 12 normal, healthy subjects (9 male, 3 female) aged
10 to 22 years (mean 18 4) . The study group consisted of
21 patients (12 male, 9 female) aged 9 W dl years (mean 16 t
5) who had been previously treated with doxorubicin for a
variety of childhood neoplasms . Cumulative doxorubicin
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
396
Kf.FWERFTAL.
CARDIAC EVALUATION BY DDLGTAMINE ECIIOCARDIOGRAPHY
IACC Vel . 19 . Nu. 2
February 199291/-401
Table 3 . Doxorubicin Patien! Data'
Do . .rubicin
Patient
No.
Age (yrV
Gender
WI
lkgl
H:
(cm)
BSA
(roc)
Cancer
Type
Total Dose
(mg/ml)
Age (yr)
During Rx
Tin, (yrl
Sire. Ra
13
14
I5
16
17
18
19
20
21
220
23
24
25
26
27
28
19
30
31
32
33
22/F
12/F
13Rd
17/1'
Ill/H
10/,0
10117
9.94
20/51
13,711
12311.
121F
13117
19'F
15/1,
161F
21/M
27/M
21194
2WM
91M
52
48
51
51
35
62
43
45
76
79
4'
49
59
71
39
62
52
89
62
66
34
16'
144
144
154
IM
144
142
145
/60
163
144
146
156
163
146
164
161
189
156
170
136
1 v
1 .36
1 .4
1 .47
1 .16
1 .52
1 .29
1 .34
1 .85
1 .85
1.28
1 .39
1 .58
1 .77
1 .26
1 .67
1 .53
2 .16
161
1.77
1 .13
ALL
Ewing
Wilms
0veo
NHL
Hodgkin
ALL
ALL
ALL
Hodgkin
ALL
ALL
ALL
ALL
ALL
0srer
ALL
NHL
NHL
ALL
ALL
27
61
86
100
too
104
194
110
120
121
168
172
183
232
238
242
242
1 6,
425
489
532
154
1o
3 .3
14 .6
4 .9
79
5 .8
4 .3
7.3
23
10.3
2 .4
5 .3
2 .4
4 .3
5 .6
108
10
11 .1
8A
5
8 .5
15 .3
59
19.8
131
15
7.2
183
75
18
4 .1
7 .9
5 .1
4 .3
9.8
5 .6
9.1
171
14.3
2.6
1 .6
'Clinical details of patients previously treated wish doxambicin for cancer in childhood . Patient numbers correspond to the patient numbers in
Figure I (Subjects 1 to 12 are control subjects). Patients are listed in order of increasing doxombicin dose . tRaOenl 22 received 2,040 rods of mediasttnal
inadutiun. ALL = acme lymphoblastic leuk :mia BSA = body surface area : Ewing = Ewing sarcoma ; Hodgkin = Hodgkin disease; Ht = height : NHL =
non-Hodkkins lymphoma ; Octeo = oitso,anewus: Rx = treatment. Wilms = Wilms tumor ; Wt - weight.
doses ranged from 27 to 532 mg/m7 (mean 196 s 137) . The the first six studies (four in patients . two in control subjects).
time elapsed since the last dose of doxorubicin ranged from At this infusion rate three of the six subjects met exclusion
1 .61o 14 .3 years (mean 6 .1 3.6, median 5.3).
criteria, including initiation of ventricular bigeminy in a
Dobutamine dose . Administration of 10 pug/kg per min of
control subject, premature ventricular and atria) complexes
dobutamine as part of the protocol was discontinued after
in one study patient and choking, sweating and shortness of
Table 2 . Hemodynamic Results in 33 Subjects'
Dobutamine Dose
Ha on line
Doxmubicin
Control
0.5 0038 per min
Duaomhicia
Control
2.5 icglkg per min
Doxombicin
Control
5 pglkg per min
13oxumbtein
Control
10 pg/kg per min
Doxombicin1
Controls
HR
Ibeatslmin)
in
MBP
. Hg)
CI
(liters/min per m 2 1
SVI
imVbeat per mi t
66 0 9
66 x 16
91 _ if.
84 x 8
4 .5 < 13
4 .6 1 1 .2
69 x 19
72 x 16
66 0 9
65 0 18
84 x 9
85 0 8
4 .9 0 1 .4
5 - 1 .3
74 - 20
77 0 153
67 _ 9
64 x 19
88 x 9
88 9 '
5 .5 o 1 .3
5 .3 x Ll
82 _ 20
83 ° '5
71
67
0
11
17
90 0 9
92 x 8
5.9 - 1 .5
6 - 1 .5
83 z 20
91 : 16
98
88
0
13
3
90- 5
90 0 2
7.1 x 1.3
7.7 0 3.5
73 - 14
88 x 3
0
t
'Summary of hemodynamic data in doxombieimtreated patients In = 211 and control subjects (n = 12) at rest and
during dobutamine stress lest . No statistically significant diifenences were found between the dox0mbicin treated
patients and control subjects . Values are mean values 4: I SD. In = 4; to = 2 ; CI = cardia, index ; HR = heat rate.
MBP = mean blood press- SVI = stroke volume tries
.
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
IACC Vol. 19. No . 2
Febrvary 1992 :394-401
KLEWER ET AL.
CARDIAC EVALUATION DY DORUTAMINE ECHOCARDIOGRAPHY
397
Table 3. Dobutamine Stress Echcca :dograpoy Results*
Dobutannne Dose
0aselmo
Doxonlbi•m
Control
0 .5 py'kg per in
Doxorubaln
Canvnl
2 .5 pgAg per in
Dcxorubicin
Control
50 tokg tier min
Doxomhicin
Control
10 04/kg per min
Dnxombwint
('mural
SF
/'. V°WTH
LVESS
(Wed)
LVPWES
In
.)
I VPWED
(mrnl
IVRT
(in"
MDT
(ms)
E
(rm!wl
(-10
NA
min
-_0 34 0.05
0 .37-005
78 n 181
97I3
68 ' 21
56- '4
II 19*
Iii-1 .5
6 .2 1
1,70.9
60 0 12
58 10
167 30
16029
61 -t. 22
770 II
30 10
38 x 11
2 .1 0.4
210.4
0 .37 ' 1.0b
9 .390.07
WI ' '_17
127 23
58 e 17
46 It
11 .9 ' 21
14.E_2
6'
6
53 II
56!10
171 ' 25
165x24
65 0 23
71x24
33 11
3711
2 + 0.4
2.200 .6
041 0 0 .00
0.46
112 321
155-1h
SO n 191
36'9
13 .1 2 .Y
17 .1'2 .1
6.3 : 1
67
50 x i2
4908
159 . 28
158x28
69 191
89!21
32 ' 81
399
2 .1 03
2 .350.4
0.45 0 .061
9.51 0 .05
121 0 377
185 _ 20
47 171
28 18
14 .1 24t
1'; ' _ 2 6
6.5 1 .3
6 .8 + 0 8
42 0 11
47 ' 9
142 30
155 5 31
81 *- 27
98 x 26
39 14
44 12
2.2 0.5
2.3 0.4
0.44 . 011
053 -- 003
91 /0'
1N - 20
40 191
17 _ 2
1
6 .6 u.8
6 % - 114
34 !8
157 ! 53 78 36
51 32
1 .7 0.3
49 18
77 0 9
2.1 + 0 .5
132 ' 5
36 ! 4
tp
<
'Unless otherwise ooAd, u = 21 doxomEdn-veered paliests and 12 wmrol subjects,
0,01 and Sp < 0.05 relative to vala .- in control subjects . $n =
:2s + 2 .61
16 .8 ' 04
4; I n = 2 . Values are mean values SD . A = morel flow velocity at the time of auial ccm :e,on . 0 = initial peak mar.' flow velocity : FJA ratio = ratio of peak
mural Bow velocity to mural flow ve:ocity at the time otatnal coerraclion . IVRT = is volumetric relaxation time ; LVESS = end-systolic wall stress ; LVPWED
- left ventrcular eud ,diastolic posterior wail thickness; LVPWES = left ventricular end-,yuoIw pus' anion wall mwkness; MDT = mural deceleralion time .
7tLVPWrt1 = percent left -I-b, posenor wall Ihick.ning; SF - shaite.mg trot-. .
67 . 15 kg for the control group (p = 0 .05). Mean body
surface area was 1 .52 `. 0.26 m 2 for the study group and 1 .76
0.27 ns for the control group (p = 0.02) . Hemodynamic
data are summarized in Table 2.
echocardiographic measurements (Table 3). Figure I
shows standardized changes in echocardiographic measurements and Figure 2 demonstrates individual changes from
No arrhythmia, symntems or other exclusion criteria were encountered at the lower infusion rates in
any study subject .
Standard measurements . Age was not significantly different between the groups. Mean height was 154 t 13 cm for
the study group and 168 14 cm for the control group (p =
0 .008) . Mean weight was 56 15 kg for the study group and
breath in another.
o --
zoo -
0
c
o e
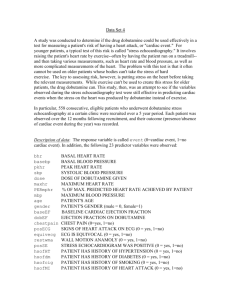
Flame 1 . Standardized percent left ventricular (LV) posterior wall (PW) thick-
o
'y
0
il0o- • •
"0
son e e ao 0 0
0°
a .. - _ .
. 00 0 00 Q
°
° a0 0
_In* _
su o
TI
1 1 1
1
i° 1{{ 1 1 1 11111111111
120 -
ening, end-systolic wall stress and percent shortening traction at baseline (kill =~ 60=
m
and during the 5-N4/kg per min dobutamine infusion (right) for each subject .
Dashed lines indicate 2 SD of control
data . Control subjects (n = 12) are
marked by solid squares; doxombicin0
treated padenis (n = 21) are marked by
60
open diamonds and are listed in ase-ndT
ing order of cumulative doxorubicin dose
50 as in Table I .
•
0 0
-
o
--- o1
I
I
I
I
I
I
1
I
. .
• •°
00
oo°oo
00
o°ac°o
0
00
0
O
O
0 °00
°
00
• 0000
- - - - - -O . -0- 2 -9O
r
10
1 11111
1111
' l l
1 1 1 1 1 1
0 3 6 9 ,'e 15 IC 21 24 27 30 33 0 3 6 9 11 15 16 21 24 27 30 33
•
30 ~'~
0
o °
-IIIII
I I I I I I
- - - - -- - - - - - - - _
-
0-no-
O o
5ublect oember
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
Subject number
CLEWUU UT AL .
CARDIAC EVALUATION BY LK)BUTAMINE EC71(XARDIOGRAPHY
398
W
C
IACC Vo1 . 19, No . 2
pebnary 1992:790-001
200
I
d
uP
r
i
>
'oo-
J
e
0
0
Jo III
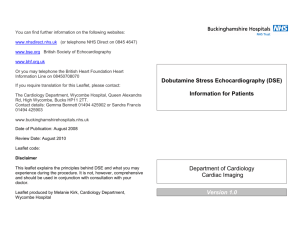
Figure 2. Data for percent left ventricular posterior wall thickening, shortening fraction and end-systolic wall stress
for control subjects and doxombicinueaied paients plotted by each subject s baseline values . The solid bar
depicts the baseline value and the
iwtcbrd Iran depict
. !he value during
the 5-µg'kg per min ddaotnbi_ia ~.nfasion . Abbreviations as in Figure I .
N
E
120 *00-
a
N
m
N
m
80 -
3
o
ao
y
C
W
J
Controls
Treated Patlenta
baseline values . End-systolic left ventricular posterior wall
dimension and percent left ventricular posterior wall thickening were the must consistent factors for differentiating
study and control subjects at rest and during each dobutamine infusion . Individual changes in percent left ventricular posterior wall thickening from baseline to peak dobutamine stress were statistically decreased in the doxorubicintreated patients when compared with changes in control
subjects (44 27% vs. 88 21%r) (p < 0 .01). The mean left
ventricular shortening fraction in doxorubicin-treated subjects was not different from that in control subjects at rest
but demonstrated significantly lower (r < 0.05 and p < 0 .01)
values compared with those of control subjects receiving
moderate doses (2 .5 and 5 ;.tg1kg per min, respectively) of
dobutamine . Individual changes in left ventricular shortening fraction front baseline to peak dobutamine stress were
not significantly different in the doxorubicin-treated group
when compared with changes in the control group (0 .12
0 .05 vs. 0.14 0.07).
Mean end-systolic stress was significantly higher (p <
0 .01) at dobutamine infusion rates of 2 .5, 5 and 10 µglkg per
min in the doxorubicin-treated group compared with mean
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
KLEWER ET AL,
CARDIAC EVAI .IIATIDN BY D09UTAMINE ECHOCARDIOGRAPHY
JA CC Vol. 19 . No. 2
February 1992 .994-401
Table 4 . Relation of Dose Results to Doxombicin
Treatment History'
Dobwam,ne Infu4on Sale
lµp'kg per mint
11aeeline
0 .5
2 .5
5
doss
0-2
0.12
412
0 .26
0' 11
022
0 .08
0 .05
0 .13
03
11-05
0 .1 ;
Total dotornbiem dose
Age dung lie
Time since Rx
LVE55
Total doxorubicin dose
Age dur'ag Rx
Time since Rx
0.07
024
11112
0 .03
0-!2
oat
0 .16
0.24
0101
a .21
(,!!I
0.17
0.1
019
0.24
O. V,'
0 .24
0.31
0.16
0 .25
0 .26
li. R
0.1
SF
To al doxowbicin
Age during Rr.
[ .me ce Rx
7.LVPWIR
'Correlation values U1 for simple linear regressiml analysis of echocardiographic measurements versus cemulalive doxorubicin dose, age at Ome of
dotanrbicin tr. .-nent and lime elapsed sine, Izsl doxurubi,r: : treatment . No
correlation was statistically significant . Rx therapy . other abbreviations as
in Table 3.
values in the coutroi group . Individual changes in left ventr c .
ular end-systolic meridional wall stress from baseline to peak
dobutamine stress were similar for doxorubicin-treated patients and control subjects (-21 t 13 vs . -28 t 13 gfcm2 ) tp =
NS) . Individual subject data for percent left ventricular posteriorwall thickening, shortening fraction and end-systolic stress
at baseline study and at the 5-µgfkg per min dobutamine
infusion rate are plotted in Figure I . Mean mitral E and A flow
velocities at the 2 .5 p4tg per min dobatamine infusion rate
had significantly greater amplitudes (p < 0.05) in the control
group than in the study group, but the mean mitral E to initial
A ratio at this level did not differ significantly between the two
groups . Heart rate, mean blood pressure, indexed cardiac
output and stroke volume, end-diastolic left ventricular posterior wall dimension, left ventricular isovolumetric relaxation
and mitral deceleration times, and the ratio of mitral E to mitral
A velocities were not significantly different when mean study
patient and control subject data were compared at baseline or
at any level of dobutamine infusion .
Relation of echocardiographie measurements to doxorubicin treatment history (Table 4) . No echocardingrnphic measurement was significantly related to total doxoruhicin dose,
patient age at time of treatment or time elapsed since doxorubicin treatment at rest or at any dobutamine infusion level .
Correlation values for variables found to be significantly different from control values (shortening fraction, percent left
ventricular posterior wall thickening and left ventricular endsystolic meridional wall stress) are shown in Table 4 .
Discussion
Decreased end-systolic left ventricular free wall dimension and percent posterior wall thickening, a measure that
3 99
reduces dependence or, body surface area (26), were the
most sensitive indicators of prior doxoruhicin exposure .
Decreased shortening fraction and increased left ventricular,
end-systolic wall stress, indexes that are reported to become
markedly abnormal with clinical doxorubicin-induced congestive heart failure (31-34), were demonstrated only during
moderate dose dobutamine infusions in our asymptmnatic
study group . End-diastolic left ventricular free wall dimension was not significantly different between the two groups ;
such a difference might be expected if substantial myocardial
fibrosis were present in the doxorubicin-treated patients.
Doxorubkin cardiotoxicity . Doxorubicin cardiotoxicity
has been recognized for almost 2 decades (1) . Dose-related
cardiotoxicity occurs in most patients as demonstrated by
abnormal endomyocardial biopsy findings (2-6) . Early histopathologic changes include cardiomyocytn sarcoplasmic
reticulum swelling, myofibrilisr dropout and cytoplasmie
vacuolation . These changes may progress to diffuse myocyte
damage and frank necrosis . Hisiopathologic changes precede clinical myocardiopathy (2-6,10) . In most patients
;ome deterioration in cardiac function is shown by noninvasive techniques during doxorubicin treatment (10-13) . Generally, improvement does not occur during the year after
treatment with doxorubicin, although some exceptions are
reported (9,32) .
Invasive endomyrcardial biopsy studies in doxorubicintreated patients have demonstrated that higher doses of
doxorubicin are more frequently associated with clinically
apparent cardiatoxieny . However. some patients tolerate
maximal doses without acute toxicity ; others develop congestive heart failure at relatively low doses (3,5) . A high
cumulative doxorubicin dose, a longer interval since completion of doxorubicin therapy, and age <4 years at the time
of doxorubicin treatment are reported (34) to be significant
risk factors for increased left ventricular problems in longterm cardiac follow-up of children treated with doxorubicin
for acu[~ lymphoblastic leukemia. The echocardiographic
findings in our patients did not correlate linearly with doxorubicin ox,e, interval since doxorubicin therapy or age
during doxorubicin treatment . This was not surprising because interactions among these variables are complex, and
our selected group included no patients with known doxorubicin cardiotoxicity .
Correlation of prior studies with the present study. Numerous noru.vasivc methods have been investigated to
detect doxorubicin cardiotoxicity. Echocardiographically
measured left ventricular shortening fraction generally decreases with increasing doxorubicin doses, but usually it is
within the normal range unless cardiotoxicity is severe
(4,5,13,15) . End-systolic left ventricular wall stress is a
relatively preload-independent measure of the force opposing left ventricular shortening (;5). Abnormalwall stress has
been reported in doxorubicin-teemed patients (34,35) . Alterations in left ventricular diastolic function in the setting of
-ormal systolic indexes have been reported in doxoruhicin •
treated patients (17,ld). Marchandise et al. (18) demon-
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
400
KLEWER ET AL.
CARDIAC EVALUATION BY
IACC Vol 19. No . 2
February 1992 :394-ant
DOBCVAMINE ECHOCARDIOGRAPHY
steated prolonged isovolumetric relaxation time, decreased
mitral E velocity and EIA ratio an .l decreased deceleration
rate with normal shortening fraction and velocity of circumferential shortening . These studies of diastolic function in
doxombicin-treated patients were performed 51 year after
treatment. Our findings do not indicate the presence of
diastolic dysfunction in long-term asymptomatic survivors .
Increasing numbers of children are surviving childhood
cancer because of doxorubicin therapy, only to suffer late
onset anthracycline cardiotoxicity . Recent reports (33,3638) have focused on congestive heart failure, ventricular
tachycardia and sudden death occurring >5 years after
doxombicin treatment. Goorin et al . (33) reported that
patients whose first episode of clinical congestive heart
failure developed >6 years after completion of doxombicin
therapy maintained appropriate left ventricular internal dimcnsioi,.s with somatic growth but had diminished left ventricular systolic free wall dimension . These investigators
postulated that the resultant elevated wall stress contributed
to a reduction in left ventricular performance and to congestive heart failure (33) . Lipshultz et al. (34) reported similar
findings in 115 patients treated I to 15 years previously with
doxombicin for acute lymphoblastic leukemia . They hypothesized that loss of cardiac myocyles during doxombicin
therapy in childhood might result in inadequate left ventricular mass and clinically important heart disease in later
years . Our asymptomatic doxombicin-treated patients had a
significantly diminished end-systolic left ventricular free wall
distension at rest . However, the mean difference between
doxombicin-treated patients and control subjects was only
2 mm . Diminished end-systolic left ventricular free wall
dimension in the doxcrubicin-treated group was more clearly
demonstrable during dobutamine stimulation (14 .1 2.4 cm
for the doxombicin-treated group vs. 19.3 . 2 .6 em for the
control group at 5 jag/kg per min of dnbutamine) .
Rationale of method of dobutamine testing . Dynamic
stress testing has long been used to detect occult cardiac
dysfunction in adults with coronary artery disease (39) .
Recently, pharmacologic stress echocardiography using dipyridamole, adenosine and dobutamine has been utilized .
Dobutamine is a relatively short-acting beta, agonist with
primarily inotropic action at low doses and it seems an ideal
drug for studying cardioselective responses to catecholamines. Dobutamine stress echocardiography using graded
dobutamine infusions of 5 to 40 µglkg per min has similar
diagnostic accuracy in coronary artery disease to that of
other proved methods (20,40-42) . Generally, dobutamine
infusion is increased in 2- to 3-min increments until clinical
end points are attained . To clearly delineate hemodynamic
responses at each dobutamine infusion rate, we evaluated
cardiac function when plasma dobutamine concentrations
were at steady state, after 15 min of infusion at each infusion
rate . Our data suggest that a dobutamine infusion rate of
10 Aglkg per min is associated with a high incidence (50%) of
adverse effects in asymptomatic children and young adults .
Furthermore, the 15-min dobutamine infusion at 5 yegiikg per
min was safe and useful for effective isotropic stimulation in
our subjects.
Accounting for differences In body size . Oor doxorubicintreated patients were similar in age to the control group but
were significantly shorter and lighter in weight . Size differences between study patients ant control subjects occurred
because 1) the objective was age matching, 21 the male to
female ratio was higher in the control group, and 31 some of
the study patients had been treated with corticosleroids .
resulting in diminished growth potential, Accordingly . echocardiographic measures that are not dependent on body
surface area were used to assess cardiac function .
Limitations, The present investigation had cc it- n limitations . Our youngest study subject was 9 ;ears old; therefore
we cannot comment on the suitability of thl : test for younger
cancer patients . The clinical implications of these echocardiographic findings are not clear because we do not have
long-term cardiac follow-up data on these patients . Future
evaluation of the clinical status in these currently osymptomatic doxorubicin-treated patients will be essential .
Conclusions. Asymptomatic doxombicin-treated patients
may have cardiac damage undetected by commonly used
methods. End-systolic left ventricular free wall dimension
and percent left ventricular posterior wall thickening were
decreased in doxorubicin-treated patients at rest compared
with values in control subjects, but dobutamine infusion
magnified these differences . Other rest echocardiographic
measures of systolic and diastolic function were similar for
asymptomatic doxombicin-treated patients and control subjects . h: particular, shortening fraction and end-systolic left
ventricular wall stress were abnormal only during isotropic
stimulation in our asymptomatic doxombicin-treated group .
Percent left ventricular posterior wall thickening and endsystolic left ventricular meridional wall stress appear to be
more sensitive than shortening fraction for differentiating
individual doxorubicin-treated patients from control subjects
during moderate inotropic stimulation with dobutamine . Our
data suggest that dobutamine stress echocardiography is a
useful noninvasive technique for examining the cardiac
status of doxombicin-treated patients, and should be considered for monitoring these patients on a long-term basis .
References
1 . Lerrak E. Pithal . Rosenheim 5 . Gottlieb JA . A clinicopathologic analysis
of adriamycin cardiotoxicity . Cancer 1973432:302-14 .
2 . Cones EP. Lutman G . Wanka 1 . et al. Adxamycin INSC-123R71 cardictoxicity: a clinicopathologic correlation . Cancer Chemother Rep Part 3
1975.6:215-25 .
3. Bristow MR . Mason JW . Billingham ME. Daniels JR. Dose-effect and
structure-function relationships in doxombicin cardiomyopathy . Am
Hear 1 1981:102 :709- Is.
4. Billingham ME . Mason JW. Bristow MR . Daniels JR. Anthracydine
cadiamyopathy monitored by morphologic changes . Cancer Treat Rep
1978 ;62 :865-72.
5 . Mason 1W . Bristow MR. Billingham ME- Daniels JR . Invasrce and
noplnvasive methods forassessing Adnamycin cardiatoxic effects in man :
superiority or hislopathologic assessment using endomyocardial biopsy .
Cancer Treat Rep 1978 ;62:857-64.
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016
JACC
Vol. W. No . 7
Fcrmary l097,a4_ 401
KLEWER
ET A[ . .
401
CARDIAC EVALUATION HY DOBUTAMINE ECHOCARDIOGRAPHY
6 . Br blow MR. Mann 1W, Billina`um ME . Danieis JR. Doxomblcin
oardiomyoperhy: Evaluation by phonocardiogmphy . eadomy-od,al h,
aptly, rd
A ., 1.1- Mad IIJ7110,169 75
7, Haiazun JF, Wagner HR, Galena 1F . bntks LF. Daeeorunian cardiac
toxicity in children with acute lymphoblanie leukemia . Cancer 1974 :53:
545-54 .
8. GiLadaea AC. Mantel C, Tan C7, Wall- N, Stemberg SS. Murphy
ML 1'he cardlranxirny of Adnamucm and ds no,b,cin in children .
Cancer 19715 :37:100-8,
9 . Daarht AM, Renew KM . CoMman A . a W . Congestive bean failure ace
to Adnamycin aardiaroxie ty its re oral history in children . CarI& 1963A2 :2910-6,
. Feiedonc MA . 13oadeck MJ, Biif,,gh, n MF, Ride, AK . Doxorubnm
cardunnaieily : serial endomyocaMial , .op,se, and systolic time Intervals.
LAMA 1978241 :1603-6 .
11 . Bloom KR, Dim RM, WIhams CM, Softy MJ. Gfibben MA . Echocardiography in Adnamycin -do-toxicity
. Canar 1978 .41 :1265-9
12 . AleaapdCr J, Dainiak N, B, .Lor HI, ct al . Serial assnsmeei of reverubicin eard :oroxinty with ces.su nrive radionudlde angiographv . N Engl I
Med 1979,810178-83 .
11, hwy GA . lonosSl . Enodron ML Gaiivl . Crier F) Stomacher cardiac
evolution of paten's receiving Adriamycin . Cancer Treat Rep 1978:62.
91.5-22.
14. Hnnderson IC . Sloss ll, Judge N, Blare TH. Fed F Ill . Serial studio of
cardiac function in patients recervmg Adnamyein . Cancer Teed Rep
1978x,2:9239 .
15 Hailer 11 Jr. Sahn Ol. WanBendee JIM . Camahan Y . Evaluation of the
cerac effects of desernbicin by corm echocardiography . Am J Di, Child
081 :135:653-7 .
15. Goldberg SJ, Retire 11 Jr, Feldman L, Goldberg SM . lwo sensitive
echocardiographic techniques for detecting doxombicin twatery . Sled
Pediatr Oncol 1983 ;10172-7,
17 . Lee BH, Goodenday LS, Muswick G1 . Yasnoff WA . Leighton RE. Skrl
RT, Alterations in left ventricular diastolic function with doxorubicin
therapy . I Am Coll Cardiol 1987 .9:184-8.
18 . Marchandise B. Schroeder E . Bosly A . et al. Early detection of dnxombiein orndiolonwity : intn- •t rf coupler e:hocardiographic analysis of left
venlricalclIling dvaamics . Am hear J 1989 .118 :92-8 .
19 . Choi BW. Banger HJ, Sehwanz PE, er aL Serial radionuclide assessment
of dooo abieen cardiononicnty in cancer patients with abnormal baseline
resting Jell ventricular performance. Am Heart J 1983 ;106:638-43 .
JO Mazeika PK, Nadazdin A, Daklo CM . Diagnostic acveracy of debutemile stress echoardiegraphy ir, neraaary disease lobster . Circulation
1990 :821supp11111:111-393.
21 . Haycock GB . Schwarlz CJ, Wisdosky DH . Geometric method for
emeadi ngbody surface area : a height-weight formula validated in infants .
cWdeen, add adults. I Pediatr 1974:93:62-6.
22. Soles D1, DeMaris A, KissloJ . W'eyman A . Recommendations regarding
quoeimrion in M-mode echocardiography: results of a survey of echocardiegraphic measurements. Circulation 1978;58:1072-83.
23 . GnbJbmg 51, Allen HD, MarvGR, Mien CJ . Doppler Echevnfdiayraphy .
Philadelphia: Lice & Fehiger, 1985 :x1-2.62-3 .
24. Pedhury IF. Hahih DM . Martinet AM. Threshnld_s for the physiologic
effects of adeenergic agents . a mdhodolo&c appraisal. Ova Phermacal
Then 1990 ;14:[15-24 .
2$. Gutgesell HP. Paluet M . Out DF . McNamara DG . Evaluation of left
ventricular vze and laaction by echocardiography : Isaltv i. -anal
[hddrer. Circulation 1977:% :457-62,
26 . Harm- wL 'e- ! . Gar din JM, Help- 81, MKay J . Waken NJ,
Echxa.rdiographic measurerinmi in eernml subjectss grawih-remled
changes that occur between infancy and early adulthood . Cirulauon
1978;51178-85 .
Z7, orossman W . Jones D . Mcfaune LP, Wall sues, and patterns of
hypertrophy in the human, left areleide . I Clot Inane' 1975;5h 96-64 .
28 . Brodie BR . McLacnin LP, Grossman W, Combined hemodsnamiealtramnic method toe studying left ventrcular wall stress : comparison
with anyior_yi,7 . Am I Cafdiol 1976 ;37:664-70,
29. Nishimura RA, Abel MD, Hole LK, Tap], AI . Assesnmeul of diastolic
function of the heart ; background and current applicatiunu o€ Doppler
echocardiography . Pan 11 . Clinical studies. Mayo Clin Pro, l1E9:64:Il 1204 .
10 . Loeber CP . Goldberg SI, Allen DID . Doppler cchocardicgmplhic cagop,eison of flows distal to the four cardiac valves. J Am Call Cardiol
19971 :299_72.
31 . rliar•°.ni . .llo T. Meyer RA . Wang KY, Sager C . Kaplan S . Dovambicir
cardiotoxicity in children . 1 Pedialr 1989;9745-5o.
32. frown AB, Crouse VL, Evans W, Takabaahi M, Siegel SE . Recovery of
Icfl ventricular function following diseenGmatioe of anlhacyeline ehe
mutherupy in children . Pedeafncs 1981 ;68:61-'l,
33. Goonn AM, Chauvenet AR, Pony-Aruyde ,AR, Cent 1. McKone R,
Lievhullz SE. Initial congestive heart faillae, six to lea Sears after
doxonihicie chemotherapy for childhood cancer J Pediatr 199x1:116
I'A--7 .
34. Lipshullz SE, Colan SD. Gerber RD, Paez-Ataydc AR . Sagan SE,
Sanders SP . Late cardiac effects of dosorubic:n therapy far acute
lymphoblastc leukenua in childhood . N Eagl J Med 1991 :324:808-15,
3J . Boa.. KM, Green Lid, Grnssmaa W. Bneanwald UP,.,
-Maul
end-syslelic stress-ehonening and anon,-length nelarioos in humans :
annual values and sensitivity to inetrepic slate . Am I Candid 198, :50 :
1301-4 .
36. Freter CE. Lee TC . Billiegham MP: . Chek L. Bnstaw MR Doxorubiun
cardiac toxicity manifesting seven years after Beatnenl : case repine and
w . Am 1 Med 1986 :80:483-5.
37. Liphulie SE . Cola . SD, Walsh EP, Sanders SP, SaUce 5E . Ventricular
„6„-a•n ia _ d sodden .rr.y .t_.d death i" late s,_;.,ieers of chad
_.-e
Imahgnancy treated with daxam8icie labslrl . Pedeutr flee 1W'7'7 :145A.
38. Swisher, L, Socialism F . Murphy L, Catalina toxicity 4-20 yearn dmr
completing anthmcydine therapy (abnlni, Proc Am Soc Clin Orient
1989 :8 :296.
39. Robb GP, Marks HH. Postexereise eledrocardiogmm in atIeeroxlem!ic
hean disease : its value in diagnosis and prognnais . JAMA 1957.950:91826.
40, Martin 7, Seaworlh 1, Jchns 1. Pupa L. Codas W . Comparison of
adenosine, dipyridamale, and dobutamine cress echocardiography for
the detection of coronary artery disease leSStrl . 1 Am Coil Candid
1991 ;17:277A .
41- Segoe DS, Berkovitz KE . Sawuds SG, el a3. Comparison of dohnlamine
sirens echowrdiaeaphy with dabammine stress SPEC'f idadluen imaging
for deletion rd coronary anety disease (abor) . I Am Call Candid
1991117:277A .
42 . Salustn .A, Fiorclli PM . Poxeoli MM, Cats F, Roelmtdr 1, Suthcdl.rd GR.
A comparison of debuttunine and highAs se dipyrsdarede stress echoeardtogrphy in the diagnosis of coronary artery li- .case labor) . Cirtdalien
I990R2lsuppl IIIlalI 191 .
Downloaded From: https://content.onlinejacc.org/ on 10/01/2016