Estrogen Receptor- Signals Left Ventricular
advertisement

Estrogen Receptor- Signals Left Ventricular Hypertrophy
Sex Differences in Normotensive Deoxycorticosterone
Acetate-Salt Mice
Dennis Gürgen, Björn Hegner, Angelika Kusch, Rusan Catar, Lyubov Chaykovska, Uwe Hoff,
Volkmar Gross, Torsten Slowinski, Andrey C. da Costa Goncalves, Ulrich Kintscher,
Jan-Åke Gustafsson, Friedrich C. Luft, Duska Dragun
Abstract—We found earlier that deoxycorticosterone acetate-salt treatment causes blood pressure–independent left ventricular
hypertrophy, but only in male mice. To test the hypothesis that the estrogen receptor- (ER) protects the females from left
ventricular hypertrophy, we treated male and female ER-deficient (ER⫺/⫺) mice and their male and female littermates
(wild-type [WT]) with deoxycorticosterone acetate-salt and made them telemetrically normotensive with hydralazine. WT
males had increased (⫹16%) heart weight/tibia length ratios compared with WT females (⫹7%) at 6 weeks. In ER⫺/⫺ mice,
this situation was reversed. Female WT mice had the greatest heart weight/tibia length ratio increases of all of the groups
(⫹23%), even greater than ER⫺/⫺ males (⫹10%). Echocardiography revealed concentric left ventricular hypertrophy in
male WT mice, whereas ER⫺/⫺ females developed dilative left ventricular hypertrophy. The hypertrophic response in
female ER⫺/⫺ mice was accompanied by the highest degree of collagen deposition, indicating maladaptive remodeling.
ER⫹/⫹ females showed robust protective p38 and extracellular signal–regulated kinase 1/2 signaling relationships compared
with other groups. Calcineurin A expression and its positive regulator myocyte-enriched calcineurin-interacting protein 1
were increased in deoxycorticosterone acetate-salt female ER⫺/⫺ mice, yet lower than in WT males. Endothelin increased
murine cardiomyocyte hypertrophy in vitro, which could be blocked by estradiol and an ER agonist. We conclude that a
functional ER is essential for inducing adaptive p38 and extracellular signal–regulated kinase signaling, while reducing
maladaptive calcineurin signaling in normotensive deoxycorticosterone acetate female mice. Our findings address the
possibility of sex-specific cardiovascular therapies. (Hypertension. 2011;57[part 2]:648-654.) ● Online Data Supplement
Key Words: estrogen receptor-, heart 䡲 hypertrophy 䡲 fibrosis 䡲 calcineurin 䡲 p38 MAPK 䡲 ERK1/2
F
flammatory and profibrotic responses. In contrast, female
DOCA mice maintained their initial physiological adaptive
cardiac phenotype despite mineralocorticoid and salt challenge. We now wished to test whether ER-related effects
contributed to these observations. We hypothesized that intact
ER signaling is an intrinsic female sex-related mechanism
required for adaptive cardiac responses in response to mineralocorticoid challenge. We focused on mitogen-activated
protein kinase (MAPK) and calcineurin-related signaling
pathway in our model and maintained normal blood pressure
in the DOCA-salt groups with hydralazine treatment.
emales seem to be relatively protected from cardiovascular disease on the basis of animal and human studies;
estrogens could play a role.1–3 Clinical trials using estrogens
for improving cardiovascular health were disappointing, perhaps because of poor estrogen receptor (ER) isoform selectivity and specificity.4 The 2 functional isoforms, ER␣ and
ER, are expressed in the myocardium.5 Receptor-mediated
effects of estrogens on cardiomyocyte biology are injury or
stimulus dependent,4,6 which, in turn, implicates activation of
distinct, sex-dependent, signaling pathways and gene expression programs.7 We described recently a sex-specific dimorphism in cardiac adaptation in response to deoxycorticosterone acetate (DOCA)-salt and showed that this response was
independent of blood pressure.8 Male mice developed left
ventricular hypertrophy (LVH) that was linked to activation
of a calcineurin-dependent pathway, which increased proin-
Materials and Methods
Details are available in the online Data Supplement at
http://hyper.ahajournals.org.
Received November 1, 2010; first decision December 1, 2010; revision accepted January 12, 2011.
From the Department of Nephrology and Intensive Care Medicine Campus Virchow-Klinikum (D.G., B.H., A.K., R.C., L.C., U.H., D.D.) and Center for
Cardiovascular Research Medical Faculty (D.G., B.H., A.K., R.C., L.C., U.H., U.K., D.D.), Charité Berlin, Berlin, Germany; Experimental and Clinical Research
Center (V.G., A.C.d.C.G., F.C.L.), Charité Berlin, Berlin, Germany; Max-Delbrück Center for Molecular Medicine (V.G., A.C.d.C.G., F.C.L.), Berlin, Germany;
Department of Nephrology Campus Charité Mitte (T.S.), Berlin, Germany; Department of Biology and Biochemistry (J.-Å.G.), University of Houston, Houston, TX.
D.G. and B.H. contributed equally to this work.
Correspondence to Duska Dragun, Department of Nephrology and Intensive Care Medicine, Augustenburger Platz 1, 13353 Berlin, Germany. E-mail
duska.dragun@charite.de
© 2011 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org
DOI: 10.1161/HYPERTENSIONAHA.110.166157
648
Gürgen et al
***
5
***
1.0
4
3
2
1
0
DOCA +
salt + hydralazine
649
B
**
***
Water/Lean (ratio))
mol/l)
Potassium Serum (mm
A
Estrogen Receptor- and LVH
0.8
0.6
0.4
0.2
0.0
-
+
-
-
-/-
+/+
ERβ Genotype
+
MAP telemetric (mm Hg)
160
-
Baseline
+
-/-
+/+
Male
C
+
DOCA +
salt + hydralazine
ERβ Genotype
-
+
-
+
-
-/-
+/+
Female
Male
Uni-Nx+salt
DOCA+salt+hydralazine
+
+/+
-
+
-/-
Female
150
140
130
120
110
100
90
ERβ
ERβ
80
70
-10 -7
-4
-1
2
5
8
2
5
8
-/-/-
Male
Female
11 14 17 20 23 26 29 32 35 38 41
experimental time (days)
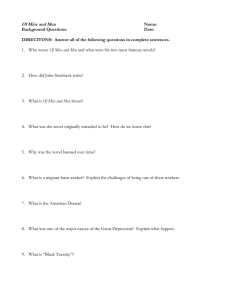
Figure 1. A, Serum potassium concentrations in response to DOCA. B, Volume and water relationships in body composition studies. C,
Hydralazine blunted DOCA ⫹ salt-induced blood pressure increases in both sexes; telemetric blood pressure recordings (mean⫾SEM;
n⫽5 per group). *P⬍0.05; **P⬍0.01; and ***P⬍0.001.
Animals
Local authorities approved the studies that were performed according
to American Physiological Society guidelines. Ten-week– old male
and female ER knockout mice with C57Bl/6J background9 and
their wild-type (WT) littermates underwent unilateral nephrectomy
and received 1% saline for drinking. Male and female mice of both
genotypes, that is, WT and ER knockout mice, were allocated to
either sham operation (unilateral nephrectomy ⫹ salt) or subcutaneous implantation of a DOCA pellet (75 mg of DOCA per
pellet; Innovative Research of America) with 60-day release time.
Animals with DOCA pellets were additionally treated with 250
mg/L of hydralazine (Sigma-Aldrich) in their drinking water to
prevent a DOCA-induced increase in blood pressure (DOCA ⫹
salt ⫹ hydralazine).
After 6 weeks, body composition analysis, echocardiography, and
invasive blood pressure measurements were performed. Blood samples were taken, and hearts were excised, weighed, and divided for
analyses. For analysis of body composition, conscious mice were
placed in a nuclear magnetic resonance spectroscopy device,
EchoMRI-100 for mice (Echo Medical Systems), and measurements
were repeated 3 times. Total body water content was related to lean
mass to account for sex and genotype differences in adipose tissue.
Telemetric recordings were performed in 5 additional female and 5
additional male ER knockout mice as described previously.10
Echocardiography
Mice were anesthetized with isoflurane. A high-resolution Vevo770
echocardiography system (mouse specific transducer RMV707B, 15
to 45 MHz, VisualSonics) was used. M-mode tracings were recorded
from the short-axis view at the high papillary muscle level. The
following parameters were assessed in end-systolic and end-diastolic
situation: thickness of the interventricular septum, left ventricular
posterior wall thickness, and left ventricular inner diameter. Ejection
fraction and fractional shortening were calculated with Vevo
Software (VisualSonics).
Histology and Morphometry
Collagen was stained with picrosirius red according to a standard
protocol. Stained area was calculated as percentage per field of
vision at ⫻400 magnification in 10 random fields of vision per
section (n⫽6 per group).
Analysis of Gene Expression (Quantitative RT-PCR)
Total RNA was extracted, purified, and reverse transcribed into
cDNA with random hexamer primers as described previously.8
Real-time PCR was performed in the Applied Biosystems 7500 Fast
Real-Time PCR system (Applied Biosystems). The relative amount
of gene transcript was calculated by the cycle threshold method using
the Applied Biosystems 7500 System version 1.2.3 software and
normalized for the endogenous reference (2 microglobulin).
Western Blot Analysis
Equal amounts of protein per sample (n⫽8 to 14 per group) were
separated and transferred onto nitrocellulose membranes (GE
Healthcare). Specific bands were quantified with ImageJ 1.43
software (http://rsbweb.nih.gov/ij/download.html). Phosphorylated
proteins were normalized to ␣-tubulin as loading control. Three
protein standards were included for calibration on each blot.
HL-1 Cell Culture and Induction of Hypertrophy
The HL-1 cell line derived from murine female atrial cardiomyocytes11 were kindly provided by W. Claycomb (Louisiana State
Hypertension
March 2011, Part 2
University, Health Sciences Center, New Orleans, LA). As indicated,
10 nmol/L of ß-estradiol (Sigma), or 10 nmol/L of diarylpropionitrile
(Tocris Bioscience) were added for 24 hours preceding hypertrophic
stimulation. For induction of hypertrophy, cells were exposed to 20
nmol/L of endothelin 1 (ET-1; Sigma) in serum-free supplemented
199 mol/L (Sigma) in the presence of ß-estradiol, diarylpropionitrile,
or solvents for 48 hours.
A
Assessment of Cell Size by Flow Cytometry
In 3 independent experiments, 20 000 propidium iodide–negative
cells per treatment condition were analyzed in flow cytometry
forward scatter (FACSCalibur, Becton Dickinson). GeoMean values
of histogram plots were used for statistical analysis.
12
HW/TL (mg/mm)
650
***
***
***
8
6
4
2
0
DOCA +
salt + hydralazine
-
+
-
+
-/-
+/+
-
B
*
0.8
+
-
+
-/-
+/+
Male
LVPWd (m
mm)
All of the data are shown as mean⫾SEM with 3F-ANOVA for
sex-genotype treatment interaction, and appropriate 2F-ANOVA
analyses were conducted for all of the data sets. Only significant
interactions with a P value ⬍0.05 are given with partial Eta-squared
(p2) as a measure of effect size. For comparison of multiple groups,
1-way ANOVA was performed followed by posttesting with the
Bonferroni multiple comparisons test. Cell culture results were
analyzed by 2-sided t test. Significance was accepted at P⬍0.05,
P⬍0.01, and P⬍0.001. All of the tests were performed using PASW
Statistics 18.0.0 (SPSS Inc) for Windows.
*
10
ERβ Genotype
Statistical Analysis
***
Female
*
*
**
0.6
0.4
0.2
Results
0.0
DOCA +
salt + hydralazine
ERβ Genotype
G
t
-
+
-
+
-//
+/+
-
C
+
-
+
-//
+/+
Male
Female
*
5.0
4.0
LVIDd
d (mm)
We first addressed possible sex- or genotype-associated confounders in responses to DOCA salt. DOCA-salt treatment
caused potassium losses in all of the groups compared with
unilateral nephrectomy mice receiving 1% saline without sex- or
genotype-related differences (Figure 1A). MRI-determined body
composition analyses demonstrated unchanged water:lean ratios,
thereby excluding volume retention in all of the treatment groups
(Figure 1B). The findings confirmed that the DOCA-salt model
is characterized by sodium retention without water retention.12
Unilateral nephrectomy ⫹ salt did not alter blood pressure
(Figure 1C). The vasodilator hydralazine prevented blood pressure increase on DOCA addition (Figure 1C). ER⫺/⫺ females
displayed a trend toward hypotensive values between week 2
and week 4 compared with ER⫺/⫺ males, without reaching
statistical significance. This difference lessened toward the end
of the experiment.
WT littermates of ER⫺/⫺ mice developed DOCA ⫹
salt-induced LVH under normotensive conditions, as in our
earlier study with C57BL/6J mice.8 Male WT mice tended to
greater heart weight:tibia length ratios than female WT mice
(Figure 2A). ER⫺/⫺ females developed the highest heart
weight:tibia length ratios, exceeding those observed in WT
males (Figure 2A). Echocardiography revealed increased left
ventricular wall and septum thicknesses in all of the DOCA
animals except for ER⫺/⫺ females (Figure 2B and Table).
ER⫺/⫺ female mice instead developed increased left ventricular diameters (Figure 2C).
Sirius red staining indicative of collagen deposition and
myocardial fibrosis revealed the most prominent fibrotic
areas in ER⫺/⫺ DOCA-salt females. A similar yet less
pronounced picture was found in WT males, and there was
almost absent fibrosis in WT females (Figure 3A and 3B).
Sex-dimorphic activation of calcineurin signaling may be
instrumental for induction of maladaptive hypertrophy.8 Very
high expression levels of the regulated calcineurin subunit
A were observed in DOCA male but not female WT mice
3.0
2.0
1.0
0.0
DOCA +
salt + hydralazine
ERβ Genotype
-
+
-
+
-/-
+/+
Male
-
+
+/+
-
+
-/-
Female
Figure 2. A, Heart weight:tibia length ratio (HW/TL). 3F-ANOVA
for sex-genotype-treatment interaction: p2 ⫽0.098, P⫽0.003;
2F-ANOVA for genotype-treatment interaction within females:
p2 ⫽0.189, P⫽0.002; 2F-ANOVA for sex-treatment interaction
within ER⫺/⫺: p2 ⫽0.203, P⫽0.006. B, Left ventricular posterior wall thickness in diastole (LVPWd) increased in all of the
DOCA except for ER⫺/⫺ females. 3F-ANOVA for sex-genotypetreatment interaction: p2 ⫽0.090, P⫽0.025; 2F-ANOVA for genotype-treatment interaction within females: p2 ⫽0.182,
P⫽0.021; 2F-ANOVA for sex-treatment interaction within
ER⫺/⫺: p2 ⫽0.372, P⫽0.004. C, Left ventricular inner diameter in diastole (LVIDd) increased only in female DOCA ER⫺/⫺
mice and was unchanged in the other groups. 2F-ANOVA for
genotype-treatment interaction within females: p2 ⫽0.147,
P⫽0.044. *P⬍0.05; **P⬍0.01; and ***P⬍0.001.
(Figure 4A). ER⫺/⫺ females showed a nonsignificant increase in calcineurin subunit A transcripts compared with
WTs (Figure 4A), whereas ER⫺/⫺ males showed the opposite trend in terms of decreased transcripts compared with
Gürgen et al
Table.
Estrogen Receptor- and LVH
651
Weights and Echocardiographic Assessment of Left Ventricle (MeanⴞSEM)
WT Male,
Uni-Nx⫹Salt
Parameter
Body weight, g
Heart weight, mg
WT Male,
DOCA⫹Salt
ER⫺/⫺
Male,
Uni-Nx⫹Salt
ER⫺/⫺
Male,
DOCA⫹Salt
WT Female,
Uni-Nx⫹Salt
WT Female,
DOCA⫹Salt
ER⫺/⫺
Female,
Uni-Nx⫹Salt
21.2⫾0.4†
23.7⫾0.3*†
22.3⫾0.5†
23.2⫾0.6†
155.0⫾4.1*‡
26.2⫾0.5
27.4⫾0.6
25.6⫾0.3
27.6⫾0.6
124.3⫾1.8
151.1⫾3.4*
136.3⫾4.4
158.7⫾4.7*
116.2⫾2.0
ER⫺/⫺
Female,
DOCA⫹Salt
139.5⫾2.6*
119.3⫾2.7†
HW/BW, mg/g
4.75⫾0.07
5.53⫾0.14*
5.34⫾0.21
5.71⫾0.16
5.49⫾0.10†
5.90⫾0.09
5.35⫾0.12
6.67⫾0.23*†‡§
IVSs, mm
0.66⫾0.02
0.79⫾0.02*
0.71⫾0.05
0.84⫾0.03
0.70⫾0.02
0.94⫾0.06*
0.72⫾0.06
0.66⫾0.02‡
IVSd, mm
0.63⫾0.02
0.70⫾0.01
0.62⫾0.03
0.71⫾0.02
0.63⫾0.01
0.77⫾0.03*
0.63⫾0.03
0.58⫾0.02‡
LVPWs, mm
0.58⫾0.02
0.75⫾0.05*
0.61⫾0.02
0.81⫾0.02
0.59⫾0.02
0.82⫾0.08*
0.63⫾0.05
0.60⫾0.03
LVPWd, mm
0.49⫾0.03
0.59⫾0.02*
0.52⫾0.02
0.68⫾0.03*
0.50⫾0.02
0.64⫾0.04*
0.54⫾0.02
0.53⫾0.02
LVIDs, mm
3.48⫾0.09
3.24⫾0.11
3.35⫾0.06
3.21⫾0.28
3.21⫾0.05
3.01⫾0.13
2.92⫾0.14
3.17⫾0.1
LVIDd, mm
4.42⫾0.04
4.47⫾0.09
4.44⫾0.04
4.50⫾0.18
4.17⫾0.04
4.36⫾0.08
4.01⫾0.09
4.37⫾0.09*
FS, %
21⫾1.4
28⫾1.2
24⫾1.6
28⫾3.5
23⫾0.8
30⫾2.1*
27⫾2.1
28⫾1.7
EF, %
43⫾2.5
54⫾1.9*
48⫾2.7
53⫾5.2
47⫾1.4
57⫾3.1*
53⫾3.2
53⫾2.7
Uni-Nx indicates unilateral nephrectomy; HW, heart weight; BW, body weight; IVSs, interventricular septum (systole); IVSd, interventricular septum (diastole); LVPWs,
left ventricular posterior wall (systole); LVPWd, left ventricular posterior wall (diastole); LVIDs, left ventricular inner diameter (systole); LVIDd, left ventricular inner
diameter (diastole); FS, fractional shortening; EF, ejection fraction.
*P⬍0.05 for DOCA⫹salt vs Uni-Nx control of the same sex and genotype.
†P⬍0.05 for female vs male of the same genotype and treatment group.
‡P⬍0.05 for ER⫺/⫺ vs ER⫹/⫹ of the same sex and treatment group.
§P⬍0.05 for DOCA⫹salt female ER⫺/⫺ vs DOCA⫹salt male ER⫹/⫹.
WTs. We next assessed transcription of a calcineurin target
gene, the 1.4 isoform of myocyte-enriched calcineurininteracting protein (MCIP1.4), which reflects calcineurin
activity.13 This gene showed mRNA regulation that paralleled
the calcineurin subunit A expression (Figure 4B).
Signaling via the ␣-isoform of p38 mitogen-activated
protein kinase (p38MAPK) has been linked to protection
from LVH-related fibrosis and cardiac dysfunction in several
LVH models.14,15 In contrast to all of the groups of male
animals with only minimal p38MAPK phosphorylation, WT
females had strikingly high levels of phosphorylated
p38MAPK, which was low in ER⫺/⫺ control and DOCAtreated females (Figure 4C). Strong constitutive extracellularregulated kinase 1/2 (ERK1/2) signaling is required for
regulation of balance between eccentric and concentric
growth.16 In contrast to all of the groups of male mice with
**
14
**
12
**
***
***
B
WT DOCA +
salt + hydralazine
ERβ
β-/- DOCA +
salt + hydralazine
Male
Sttained Area/VF (%)
16
Discussion
Our major finding is that absence of ER in normotensive
DOCA-salt mice leads to maladaptive dilative cardiac fibro-
10
8
6
4
2
0
DOCA +
salt + hydralazine
ERβ Genotype
-
+
-
+
-/-
+/+
Male
-
+
+/+
-
+
Female
A
moderate amounts of phosphorylated ERK1/2, female DOCA
WT mice had high levels of phosphorylated ERK1/2, which
was greatly reduced in female ER⫺/⫺ mice (Figure 4D).
ET-1 has been implicated as a mediator in DOCA-salt–
associated end-organ damage17 and has been used as a hypertrophic stimulus for in vitro experiments by means of the female
mouse cardiomyocyte HL-1 cell line. Fluorescence-activated
cell sorter forward scatter analysis demonstrated a 7.5-fold
increase in cardiomyocyte cell size with ET-1 alone indicative of
cellular hypertrophy (Figure 5). The addition of ß-estradiol to the
culture medium or selective ER stimulation with diarylpropionitrile largely prevented the prohypertrophic effect of ET-1.
-/-
Female
Figure 3. A, Morphometric analysis of Sirius red–stained heart sections revealed collagen deposition in all of the DOCA ⫹ salt ⫹ hydralazine groups with highest amounts in female ER⫺/⫺ mice. 3F-ANOVA for sex-genotype-treatment interaction: p2 ⫽0.280,
P⫽0.024; 2F-ANOVA for genotype-treatment interaction within females: p2 ⫽0.530, P⫽0.017. B, Representative microphotographs of
Sirius red stainings showing all of the DOCA ⫹ salt ⫹ hydralazine groups. *P⬍0.05; **P⬍0.01; and ***P⬍0.001.
Hypertension
CnAβ m
mRNA (AU)
A
500
400
300
200
120
March 2011, Part 2
***
**
***
B
90
60
30
0
DOCA +
salt + hydralazine
ERβ Genotype
-
+
-
+
-/-
+/+
-
-/-
**
18
***
12
6
4
2
0
DOCA +
salt + hydralazine
+
ERβ Genotype
-
+
-
+
-/-
+/+
-
***
***
D
4.0
3.2
2.4
1.6
0.8
0.0
+
-
+
-/-
+/+
Male
Female
4.8
pERK
K1/2/α-Tubulin
pp38M
MAPK/α -Tubulin
-
**
Female
***
***
4.8
+
+/+
Male
C
24
MCIP1.4 m
mRNA (AU)
652
*
**
*
4.0
3.2
2.4
1.6
0.8
0.0
- 44 kDa
- 38 kDa
pp38MAPK
- 53 kDa
α-Tubulin
DOCA +
salt + hydralazine
ERβ Genotype
-
+
-
+
-/-
+/+
Male
-
+
+/+
-
+
-/-
Female
pERK1/2
- 42 kDa
- 53 kDa
α-Tubulin
DOCA +
salt + hydralazine
ERβ Genotype
-
+
-
+
-/-
+/+
Male
-
+
+/+
-
+
-/-
Female
Figure 4. A, Calcineurin A- (CnA-) isoform mRNA levels strongly increased in DOCA WT males. 3F-ANOVA for sex-genotypetreatment interaction: p2 ⫽0.182, P⫽0.001; 2F-ANOVA for genotype-treatment interaction within males: p2 ⫽0.317, P⫽0.003;
2F-ANOVA for sex-treatment interaction within WT: p2 ⫽0.381, P⫽0.001. B, MCIP1.4 gene expression, a direct transcriptional downstream target of CnA- served for assessment of calcineurin activity. MCIP1.4 mRNA levels paralleled those of CnA-. 3F-ANOVA for
sex-genotype-treatment interaction: p2 ⫽0.157, P⫽0.007; 2F-ANOVA for genotype-treatment interaction within males: p2 ⫽0.223,
P⫽0.041; 2F-ANOVA for sex-treatment interaction within WT: p2 ⫽0.420, P⫽0.001. C, Low phosphorylation levels of p38MAPK in all
of the groups of male animals independent of genotype and treatment. High phospho-p38 levels in all of the WT females and loss of
p38MAPK in female ER⫺/⫺ to the levels similar in all of the male groups. 2F-ANOVA for sex-genotype interaction within controls:
p2 ⫽0.459, P⬍0.001; 2F-ANOVA for sex-genotype interaction within DOCA: p2 ⫽0.401, P⬍0.001. D, Phosphorylation levels of
ERK1/2 were highest in control and DOCA-treated WT females. Striking loss of phosphorylated ERK1/2 levels of ER⫺/⫺ female
groups. 2F-ANOVA for sex-genotype interaction within controls: p2 ⫽0.363, P⫽0.001; 2F-ANOVA for sex-genotype interaction within
DOCA: p2 ⫽0.326, P⫽0.002. *P⬍0.05; **P⬍0.01; and ***P⬍0.001.
sis in female mice, implicating a regulatory role of ERrelated signaling pathways in blood pressure–independent
cardiac remodeling processes. Conversely, the prohypertrophic effect of ET-1, a neurohormonal effector of cardiac
remodeling in DOCA-salt injury, was abolished by treatment
with an ER-selective agonist in vitro. Loss of protective
p38MAPK and ERK1/2 signaling facilitated induction of the
calcineurin pathway, which contributed to adverse cardiac
remodeling in normotensive DOCA ER-deficient female
mice.
ER deletion is associated with hypertension in both male
and female mice, implicating ER as an important regulatory
factor of blood pressure maintenance.18,19 Similarly, treatment with a selective ER agonist showed antihypertensive
properties.20 Sex-related differences in blood pressure as a
possible confounder were minimized in our study to focus on
ER-related effects in response to mineralocorticoid excess.
Female ER-deficient mice showed a trend toward lower
blood pressure values in response to vasodilator treatment in
the middle of follow-up. Dysfunctional signaling resulting in
adverse cardiac remodeling and compromised cardiac function, as reflected by absent increased ejection fraction and
fractional shortening observed in DOCA-treated ERdeficient females, probably accounted for this observation.
Whether ER-related effects could have modulated the response to hydralazine was beyond the scope of our study.
A dominant cardioprotective role of ER, but not ER␣, in
the cardiac adaptation to pressure load was demonstrated in
Cell Size Increase to Control (%)
Gürgen et al
10
*
*
8
6
4
2
0
ET-1
ET-1 + E2
ET-1 +
ERβ-Agonist
Figure 5. Cell size assessment in a female mouse cardiomyocyte cell line (HL-1) by fluorescence-activated cell sorter analysis. Increase in HL-1 cell size on ET-1 stimulation (20 nmol/L for
48 hours). Estradiol or the specific ER agonist diarylpropionitrile acted antihypertrophically.
several studies using either selective receptor-deficient animals.21,22 Similar findings resulted from interventions with
selective receptor agonists.20,23 ER-deficient female mice
have estradiol levels similar to their WT littermates.24 Most
studies have focused on the transverse aortic constriction
model.25 This model features an initial adaptive response to
compensate for elevated ventricular pressures to normalize
wall stress. In contrast, cardiac remodeling in the normotensive DOCA-salt model is induced by local and systemic
actions of DOCA (mimicking aldosterone) and ET-1 on
cardiomyocyte biological responses.26 The heart seems to
have an ability to sense distinct forms of mechanical loading
and to initiate unique signaling mechanisms to induce different forms of hypertrophy.27,28 Biomechanical stress and
neurohormonal factors are major triggers of intracellular
pathways. In normotensive mice, DOCA salt and ET-1
induce sexually dimorphic hypertrophic phenotypes characterized by a mixture of concentric and eccentric LVH with
perivascular fibrosis in WT male mice and eccentric LVH
with perivascular fibrosis in ER-deficient females. Both
cardiac phenotypes can be found in patients with chronic
renal dysfunction experiencing an increasingly important
clinical condition recognized as chronic cardiorenal syndrome.29 In contrast to concentric LVH, molecular mechanisms responsible for eccentric hypertrophy are far less
investigated and mostly limited to pure volume-overload
models.30 Different signaling events occurring during the
development of physiological versus pathological hypertrophy and dysregulation of prohypertrophic signaling cascades
are implicated in the transition process from hypertrophy to
failure.27
The involvement of the activated calcineurin pathway in a
blood pressure–independent manner was shown previously to
be restricted to male DOCA-salt mice.8 We found only a
weak increase in calcineurin with concomitant upregulation
of calcineurin regulating protein MCIP1.4 in hearts of ERdeficient DOCA females. The fibrotic response and collagen
I and III distributions were particularly prominent in the
hearts of ER-deficient DOCA-salt females. However, the
magnitude of increase in calcineurin signaling was not similar
Estrogen Receptor- and LVH
653
to that observed in DOCA-salt male WT mice. Similar
changes in collagen type I and III expression profiles and
perivascular fibrosis have been observed in hearts of ovariectomized rats exposed to volume overload after aortocaval
shunt,31 implicating the importance of estrogen-mediated
signals for protecting against eccentric cardiac hypertrophy
and fibrosis. Thus, intact ER could not only attenuate
activation of mediators of maladaptive hypertrophy but also
could be important for the maintenance of protective signals
controlling their activation. This finding is underscored by the
strong p38MAPK phosphorylation detected only in female
WT mice. The response was lost in their ER-deficient
littermates. Studies in cardiac-specific p38MAPK transgenic
mice demonstrated a critical role of p38 for cardiomyocyte
survival.14 Moreover, reduced p38 signaling promoted cardiomyocyte growth through enhanced calcineurin signaling.15
Because the amount of phosphorylation was similar in both
DOCA-salt females and uninephrectomized salt females and
because both stimuli may be considered as stressors for the
cardiovascular system, active p38MAPK could represent a
part of female sex-intrinsic and estrogen-related adaptive
signaling transduced via ER. Similar findings in ERK1/2
activation, together with protective cytosolic32 rather than
nuclear phosphorylated ERK1/2 localization in hearts of
female WT mice, could represent a protective signaling
program. Selective ERK1/2 activation in the heart is correlated with relatively benign forms of hypertrophy in Gq
protein transgenic mice.33 ET-1 mediates cardiac hypertrophy
and fibrosis via ETA-receptor in DOCA-salt hypertension.34
The ETA receptor belongs to G protein– coupled receptors,
and its downstream signals require Gq.35 Data from the
present study suggest that estradiol-mediated protective
stress-kinase programs modulated induction of the maladaptive calcineurin pathway, which was responsible for a mild
and adaptive cardiac phenotype in female mice with intact
ER. In vitro data, in which the antihypertrophic effect of an
ER agonist was similar to that of estradiol in ET-1–
stimulated female mouse cardiomyocytes, were consistent
with this idea.
Focusing solely on ER-related effects could be a potential
weakness of our study. Activation of ERK1/2 may lead to
activation of ER␣ and may induce ligand-independent activation of ER␣. ER␣ could theoretically provide cardioprotection.36 Nevertheless, our major finding was that loss of
ER-related protective signaling results in maladaptive cardiac remodeling. The findings are not consistent with overcompensated ER␣ actions. The instrumental antihypertrophic
action of ER was further demonstrated in cell-culture
studies.
Perspectives
Mineralocorticoids and salt overload are major cardiac stressors in patients with renal dysfunction that also commonly
feature gonadal dysfunction.37 Targeting ER with selective
receptor agonists could provide an additional therapeutic
option.
Acknowledgments
We thank Jennifer Pützer, Maria Schmidt, Philine Wagner, Ilona
Kamer, and Marc Eigen for expert technical assistance.
654
Hypertension
March 2011, Part 2
Sources of Funding
The Deutsche Forschungsgemeinschaft Research Group FOR1054,
DR 498/1-1, and graduate school training grants GK 754 II and III
supported these studies.
Disclosures
None.
References
1. Neugarten J, Acharya A, Silbiger SR. Effect of gender on the progression
of nondiabetic renal disease: a meta-analysis. J Am Soc Nephrol. 2000;
11:319 –329.
2. Konhilas JP, Leinwand LA. The effects of biological sex and diet on the
development of heart failure. Circulation. 2007;116:2747–2759.
3. Mendelsohn ME, Karas RH. The protective effects of estrogen on the
cardiovascular system. N Engl J Med. 1999;340:1801–1811.
4. Mendelsohn ME, Karas RH. Molecular and cellular basis of cardiovascular gender differences. Science. 2005;308:1583–1587.
5. Grohe C, Kahlert S, Lobbert K, Stimpel M, Karas RH, Vetter H, Neyses
L. Cardiac myocytes and fibroblasts contain functional estrogen
receptors. FEBS Lett. 1997;416:107–112.
6. Peter I, Shearman AM, Vasan RS, Zucker DR, Schmid CH, Demissie S,
Cupples LA, Kuvin JT, Karas RH, Mendelsohn ME, Housman DE,
Benjamin EJ. Association of estrogen receptor gene polymorphisms
with left ventricular mass and wall thickness in women. Am J Hypertens.
2005;18:1388 –1395.
7. Coylewright M, Reckelhoff JF, Ouyang P. Menopause and hypertension:
an age-old debate. Hypertension. 2008;51:952–959.
8. Karatas A, Hegner B, de Windt LJ, Luft FC, Schubert C, Gross V, Akashi
YJ, Gürgen D, Kintscher U, da Costa Goncalves AC, Regitz-Zagrosek V,
Dragun D. Deoxycorticosterone acetate-salt mice exhibit blood pressureindependent sexual dimorphism. Hypertension. 2008;51:1177–1183.
9. Krege JH, Hodgin JB, Couse JF, Enmark E, Warner M, Mahler JF, Sar M,
Korach KS, Gustafsson JA, Smithies O. Generation and reproductive
phenotypes of mice lacking estrogen receptor. Proc Natl Acad Sci
U S A. 1998;95:15677–15682.
10. Gross V, Tank J, Obst M, Plehm R, Blumer KJ, Diedrich A, Jordan J, Luft
FC. Autonomic nervous system and blood pressure regulation in rgs2deficient mice. Am J Physiol Regul Integr Comp Physiol. 2005;288:
R1134 –R1142.
11. Claycomb WC, Lanson NA Jr, Stallworth BS, Egeland DB, Delcarpio JB,
Bahinski A, Izzo NJ Jr. Hl-1 cells: a cardiac muscle cell line that contracts
and retains phenotypic characteristics of the adult cardiomyocyte. Proc
Natl Acad Sci U S A. 1998;95:2979 –2984.
12. Titze J, Bauer K, Schafflhuber M, Dietsch P, Lang R, Schwind KH, Luft
FC, Eckardt KU, Hilgers KF. Internal sodium balance in doca-salt rats: a
body composition study. Am J Physiol Renal Physiol. 2005;289:
F793–F802.
13. Ni YG, Berenji K, Wang N, Oh M, Sachan N, Dey A, Cheng J, Lu G,
Morris DJ, Castrillon DH, Gerard RD, Rothermel BA, Hill JA. Foxo
transcription factors blunt cardiac hypertrophy by inhibiting calcineurin
signaling. Circulation. 2006;114:1159 –1168.
14. Nishida K, Yamaguchi O, Hirotani S, Hikoso S, Higuchi Y, Watanabe T,
Takeda T, Osuka S, Morita T, Kondoh G, Uno Y, Kashiwase K, Taniike
M, Nakai A, Matsumura Y, Miyazaki J, Sudo T, Hongo K, Kusakari Y,
Kurihara S, Chien KR, Takeda J, Hori M, Otsu K. P38␣ mitogen-activated protein kinase plays a critical role in cardiomyocyte survival but not
in cardiac hypertrophic growth in response to pressure overload. Mol Cell
Biol. 2004;24:10611–10620.
15. Braz JC, Bueno OF, Liang Q, Wilkins BJ, Dai YS, Parsons S, Braunwart
J, Glascock BJ, Klevitsky R, Kimball TF, Hewett TE, Molkentin JD.
Targeted inhibition of p38 MAPK promotes hypertrophic cardiomyopathy through upregulation of calcineurin-nfat signaling. J Clin Invest.
2003;111:1475–1486.
16. Kehat I, Davis J, Tiburcy M, Accornero F, Saba-El-Leil MK, Maillet M,
York AJ, Lorenz JN, Zimmermann WH, Meloche S, Molkentin JD.
Extracellular signal-regulated kinases 1 and 2 regulate the balance
between eccentric and concentric cardiac growth. Circ Res. 2011;108:
176 –183.
17. Matsumura Y, Fujita K, Miyazaki Y, Takaoka M, Morimoto S.
Involvement of endothelin-1 in deoxycorticosterone acetate-salt-induced
hypertension and cardiovascular hypertrophy. J Cardiovasc Pharmacol.
1995;26(suppl 3):S456 –S458.
18. Forster C, Kietz S, Hultenby K, Warner M, Gustafsson JA. Characterization of the ER⫺/⫺ mouse heart. Proc Natl Acad Sci U S A. 2004;
101:14234 –14239.
19. Zhu Y, Bian Z, Lu P, Karas RH, Bao L, Cox D, Hodgin J, Shaul PW,
Thoren P, Smithies O, Gustafsson JA, Mendelsohn ME. Abnormal
vascular function and hypertension in mice deficient in estrogen
receptor. Science. 2002;295:505–508.
20. Arias-Loza PA, Hu K, Dienesch C, Mehlich AM, Konig S, Jazbutyte V,
Neyses L, Hegele-Hartung C, Heinrich Fritzemeier K, Pelzer T. Both
estrogen receptor subtypes, ␣and, attenuate cardiovascular remodeling
in aldosterone salt-treated rats. Hypertension. 2007;50:432– 438.
21. Skavdahl M, Steenbergen C, Clark J, Myers P, Demianenko T, Mao L,
Rockman HA, Korach KS, Murphy E. Estrogen receptor- mediates
male-female differences in the development of pressure overload hypertrophy. Am J Physiol Heart Circ Phisiol. 2005;288:H469 –H476.
22. Babiker FA, Lips D, Meyer R, Delvaux E, Zandberg P, Janssen B, van
Eys G, Grohe C, Doevendans PA. Estrogen receptor protects the murine
heart against left ventricular hypertrophy. Arterioscler Thromb Vasc Biol.
2006;26:1524 –1530.
23. Pedram A, Razandi M, O’Mahony F, Lubahn D, Levin ER. Estrogen
receptor-{} prevents cardiac fibrosis. Mol Endocrinol. 2010;24:
2152–2165.
24. Lindberg MK, Alatalo SL, Halleen JM, Mohan S, Gustafsson JA, Ohlsson
C. Estrogen receptor specificity in the regulation of the skeleton in female
mice. J Endocrinol. 2001;171:229 –236.
25. Fliegner D, Schubert C, Penkalla A, Witt H, Kararigas G, Dworatzek E,
Staub E, Martus P, Ruiz Noppinger P, Kintscher U, Gustafsson JA,
Regitz-Zagrosek V. Female sex and estrogen receptor- attenuate cardiac
remodeling and apoptosis in pressure overload. Am J Physiol Regul Integr
Comp Physiol. 2010;298:R1597–R1606.
26. Ammarguellat F, Larouche I, Schiffrin EL. Myocardial fibrosis in
doca-salt hypertensive rats: effect of endothelin et(a) receptor
antagonism. Circulation. 2001;103:319 –324.
27. Heineke J, Molkentin JD. Regulation of cardiac hypertrophy by intracellular signalling pathways. Nat Rev Mol Cell Biol. 2006;7:589 – 600.
28. Bernardo BC, Weeks KL, Pretorius L, McMullen JR. Molecular distinction between physiological and pathological cardiac hypertrophy:
experimental findings and therapeutic strategies. Pharmacol Ther. 128:
191–227.
29. Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal
syndrome. J Am Coll Cardiol. 2008;52:1527–1539.
30. Opie LH, Commerford PJ, Gersh BJ, Pfeffer MA. Controversies in
ventricular remodelling. Lancet. 2006;367:356 –367.
31. Voloshenyuk TG, Gardner JD. Estrogen improves timp-mmp balance and
collagen distribution in volume-overloaded hearts of ovariectomized
females. Am J Physiol Regul Integr Comp Physiol. 2010;299:R683–R693.
32. Lorenz K, Schmitt JP, Schmitteckert EM, Lohse MJ. A new type of
erk1/2 autophosphorylation causes cardiac hypertrophy. Nat Med. 2009;
15:75– 83.
33. Minamino T, Yujiri T, Terada N, Taffet GE, Michael LH, Johnson GL,
Schneider MD. Mekk1 is essential for cardiac hypertrophy and dysfunction induced by gq. Proc Natl Acad Sci U S A. 2002;99:3866 –3871.
34. Schiffrin EL. Role of endothelin-1 in hypertension and vascular disease.
Am J Hypertens. 2001;14:83S– 89S.
35. Watts SW. Endothelin receptors: what’s new and what do we need to
know? Am J Physiol Regul Integr Comp Physiol. 2010;298:R254 –R260.
36. Kato S, Endoh H, Masuhiro Y, Kitamoto T, Uchiyama S, Sasaki H,
Masushige S, Gotoh Y, Nishida E, Kawashima H, Metzger D, Chambon
P. Activation of the estrogen receptor through phosphorylation by
mitogen-activated protein kinase. Science. 1995;270:1491–1494.
37. Vecchio M, Navaneethan SD, Johnson DW, Lucisano G, Graziano G,
Querques M, Saglimbene V, Ruospo M, Bonifati C, Jannini EA, Strippoli
GF. Treatment options for sexual dysfunction in patients with chronic
kidney disease: a systematic review of randomized controlled trials. Clin
J Am Soc Nephrol. 2010;5:985–995.