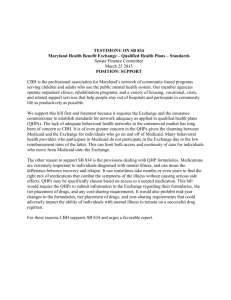
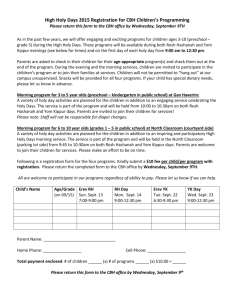
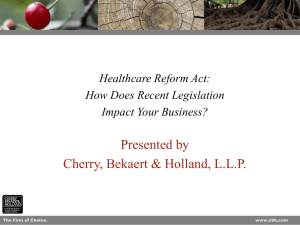
Claims - DBHIDS
advertisement

4.1 cl aims department Claims Submission Policies and Procedures ncreasingly, local, state and federal governments have sought clinical and cost data to more carefully monitor the use of public health care funds. In order to comply with governmental mandates for information, managed care organizations such as CBH have had to request more detailed and complex claims data from providers. I We recognize that this often poses an ardous task. Nevertheless, submission of accurate claims information in a timely manner is an essential part of the provider's role in delivering care, tracking clinical activity and maintaining fiscal stability. For this reason, CBH is committed to working with providers to help the process go as smoothly and efficiently as possible. We welcome your comments and suggestions on how to further improve the process. In this chapter, we provide general and specific policy and procedural statements pertaining to the submission of claims to CBH. If we can assist you with any additional information, please contact the Claims Department at (215) 413-7125. Submitting Claims to CBH Provider shall bill CBH for Covered Services rendered to Enrollees, in the manner specified in this section. Provider shall submit "Clean Claims" no more than 90 days following the date of service for Covered Services. In the event Provider is pursuing Coordination of Benefits, provider must obtain a final determination from the primary payor dated no more than 180 days following the date of service and submit a clean claim to CBH within 90 days after receipt of a determination from the primary payor. "Unclean Rejected Claims" must be resubmitted as clean claims within the time requirements stated herein. CBH reserves the right to make no payments for claims received beyond the time requirements stated herein. Definitions: clean claim: A clean claim shall mean a claim that can be processed without requiring additional information from the provider of the service or from a third party. A clean claim does not include: claims pended or rejected because they require additional information either from a provider or from internal sources (i.e., claims pended for a determination of third-party liability, etc.); a claim under review for medical necessity; or a claim submitted by a provider reported as being under investigation by a governmental agency, the City of Philadelphia or DBH/CBH for fraud or abuse. However, if under investigation by the City or DBH/CBH, the Department of Public Welfare (DPW) must have prior notice of the investigation. unclean rejected claim: An unclean rejected claim shall mean a claim that is returned to the provider or third party for additional information. clean rejected claim: A clean rejected claim shall mean a claim that is returned to the provider or third party due to ineligible recipient or service. WWW.DBHIDS.ORG cl aims department 4.2 Verification of Eligibility: In order to receive payment for services rendered, providers must check the member’s eligibility. Providers can access the DPW’s daily eligibility file by phone by calling (800) 766-5387. Providers may also use the various methods described on DPW’s website: Go to http://www.dpw.state. pa.us/Partners Providers/PROMISe/003675036.htm and click on the "Eligibility Verification Information" link. Authorized Services: The authorization process and the claims process are closely related. (See Authorization section for details on the authorization process.) For all services requiring an authorization, the provider will need to obtain an authorization number prior to submitting a claim. A claim form without a required authorization number will be rejected. (If filed manually, the claim will be returned.) Non-Authorized Services: All laboratory services (600-level services) and most outpatient services do not require an authorization. When completing the claim forms, these non-authorized services must have a Blanket Authorization Number (BAN) placed in the authorization number field. Please refer to Schedule A of the Provider Agreement to identify the non-authorized services and the corresponding BAN. There are sample claim forms at the end of this chapter available for reference. Pricing and Information Modifiers: Certain services (both authorized and non-authorized) require pricing and/or information modifiers. Please refer to Schedule A to identify the services which require modifiers. When completing the claim form, place the pricing modifier in the first modifier field and the information modifier in the second modifier field. There are sample claim forms at the end of this chapter available for reference. Entering the Correct Year Format: When completing the UB-04 or CMS-1500 (08-05) claim forms, the provider must use the complete four-digit year. For example, enter the full year as “2011” rather that ’11. Any manual claims submitted without the full year date format will be returned. Billing for Consecutive Days - "Span Billing": When billing for per diem services that were provided on consecutive days, the provider does not need to enter each individual date of service on the claim form, but may “span bill” the entire period of service. “Span billing” means that the provider notes on the claim the dates that treatment began and ended and the number of units of service provided. DBH/CBH PROVIDER MANUAL REV.2011 4.3 cl aims department OTE EN PLEAS Both the "service begin" date and the "service end" date must be within the authorized period. The day of discharge from inpatient treatment does not count for units of service. Billing for Non-Consecutive Days: When billing for non-consecutive days within a particular authorization period, the provider must note each date of service individually. OTE EN PLEAS Do not span date for non-consecutive days of service or non-per diem services. Such claims will be rejected. Requirements for Provider Signature: The provider rendering the service must sign all invoices for claims, whether they are submitted manually or electronically. The signature certifies that the service has been rendered according to Medical Assistance (MA) regulations. Methods of signing claims: The following are acceptable methods of signing claims: For Paper Claims: An actual handwritten authorization signature of the provider directly on the signature line of the invoice. The provider’s initials or printed name are not acceptable signatures. A signature stamp of the provider placed directly over the signature line of the invoice is acceptable, if the provider authorizes its use and assumes responsibility for the information in the invoice. An actual handwritten authorization signature of the provider directly on the MA-307 Invoice Transmittal Form, a form used to certify that treatment services have been delivered by the provider. WWW.DBHIDS.ORG cl aims department 4.4 For Claims submitted via modem: An electronic certification is incorporated into the submission process. non-compliance: All claims received that do not meet the provider signature requirements will not be processed. These claims will be returned to the provider for correction. Third Party Liability (TPL) Billing: Third Party Liability (TPL) refers to specific entities, such as Medicare, Blue Cross and parties other than CBH that may be liable for all or part of a client’s health care expenses. When thirdparty resources are available to cover behavioral services provided to Medicaid recipients, CBH is the “payor of last resort.” For all services requiring prior authorization, the provider should obtain an authorization number from a DBH/CBH Care Manager prior to submitting a claim. This applies regardless of whether CBH is the primary payor or if it is Medicare or any other insurance carrier. Please also note that providers should obtain authorization numbers at the time clients are admitted to a facility. Once it is determined that a client has other insurance, the bill should be sent first to the primary insurance carrier(s) for payment consideration. CBH will consider for payment all balances for behavioral health services that are unpaid by the other insurance carriers. Before CBH can consider a TPL claim for payment, the provider must submit the completed claim form, the Explanation of Benefits (EOB), or the denial letter(s) sent to the provider by any and all other carriers. The claim must be fully considered and resolved with the primary carrier before it is billed to CBH. If the services are rejected by the primary carrier due to missing, incomplete, or incorrect information, the service must be re-billed to the primary carrier before CBH will consider payment. The EOB, or the denial letter(s) must be the final determination. If the primary carrier rejects the claim, the primary carrier’s internal appeals process must be exhausted before CBH will consider the claim for payment. It is important that the provider’s bill matches the EOB information. This applies to the billed amount, beginning and ending dates, Medicare approved amount, and other insurance paid amount, Medicare deductible and the Medicare co-insurance amount. If the EOB form is larger than letter size, please reduce the EOB to 8-1/2” by 11” in size. Please include a copy of the EOB with each claim. Do not attach several claims to one EOB. TPL Medicare Inpatient Claims: When submitting Medicare and other insurance carriers’ third-party liability claims for one inpatient stay, CBH requires separate claim forms for each authorization number issued for the various levels of care during the stay. Be sure to use the appropriate authorization number on each claim. DBH/CBH PROVIDER MANUAL REV.2011 4.5 cl aims department Once you receive your Medicare or other insurance EOB, complete the UB-04 Claim Form for each authorized period. The billed charges must be for the authorized period. Attach a copy of the EOB to each claim prior to submitting to CBH. It is essential to submit these claims together to ensure proper processing. Exhausted Medicare Inpatient Lifetime Psychiatric Days: If the member’s lifetime psychiatric days have been exhausted, manually submit both the Medicare Part A and Part B EOBs with the claim form. The Medicare Part A EOB must show the Medicare Lifetime Exhaustion rejection code. If you do not have the Medicare Part A EOB, you must submit the HIQA Inquiry Form from the Medicare system. However, the Medicare HIQA Inquiry Form will only be accepted if the inquiry date is the admission date or the date on which the benefits exhausted during the stay, or should be covered in the Date of Earliest Billing (DOEBA) or Date of Last Billing (DOLBA) time period. For Medicare Part B, you must use the appropriate value code in Field 39 on the UB-04 Claim Form to indicate the Medicare Part B payment. The Part B value amount on each claim must reflect only the portion that applies to the dates of services on each claim. Medicare Remittance Advices/ Other Insurance Carrier Remittance Advices For CBH to process Medicare claims correctly, the following information is needed on the remittance advices: 1. 2. 3. 4. 5. 6. 7. 8. From and Thru Date Total Days (Cost Days) Covered Days Non-Covered Days Total Charges Covered Charges Non-Covered Charges Remark Codes and description of remark codes For CBH to process commercial insurance carriers and Medicare Advantage Plans claims, the following information is needed on the remittance advices: 1. 2. 3. 4. 5. From and Thru Date Total Days Covered Days Non-Covered Days Remark Codes and description of remark codes If you or your vendor is unable to include this data on your remittance advices, please add the information to your explanation of benefits. This will help to assure that your claims are processed and paid correctly. Otherwise, we may have to reject your claim to allow you to correct and resubmit the claims with all of the necessary requirements. WWW.DBHIDS.ORG cl aims department 4.6 ACT 62 Pennsylvania Mandate for Autism As of 7/1/09, DPW requires that private insurers pay for the first $36,000 of the cost of covered behavioral services for children age 21 and under with Autism Spectrum Disorders. Each month when the employer group renews, the children become a part of the program. All of the benefits must be coordinated with the primary carrier until the first $36,000 is paid out for covered services for the contract year. After the primary carrier pays $36,000 for the contract year, CBH will pay as the primary for those services for the rest of that contract year. The $36,000 benefit starts again each year when the employer group renews the contract with the primary carrier. It is the responsibility of the provider to contact the parents and the primary carrier of each client with an Autism Spectrum disorder to determine whether or not they have the Pennsylvania Mandate for Autism, ACT 62. If the client has the ACT 62 mandate, the benefits must be coordinated with the primary carrier for all levels of care, except the ones noted below that CBH will continue to pay as the primary. Once the EOB and/or final determination letter is obtained, the claims must be submitted manually along with a copy of an EOB/final determination letter attached to each claim. If a client is being seen, and CBH does not have a record of the ACT 62 benefit, and later finds out retro back that the client has the ACT 62 benefits, all the claims will be identified for which CBH should not have paid as the primary carrier, and the claims will be backed out. Please note that in order for us to consider these claims for payment, the benefits must be coordinated with the primary carrier. There must be a final determination submitted with each claim. Two denial reasons have been set up to be used when the final determination has not been submitted, or is not correct. The rejection reasons are “Act 62 Coordinate Benefits” or “ACT 62 Determination not acceptable”. If the primary carrier denies the services as a non-covered benefit, CBH will pay as the primary. Also, if the services are being denied because they are provided in the school, currently, CBH is paying as the primary carrier. If the client is receiving the same level of care (service) on the same day in two different place of service, and the primary only covered some of the units of service, you must bill all of the units together. It must be noted on the EOB and/or final determination letter how many units were covered, and how many units were not covered. If the claims are submitted separately, one will pay and the other one will reject as being previously paid. CBH will continue to pay as the primary for the following levels of care: a. 450 b. 550 c. 700 d. 800 e. 900 All of the other levels of care must be coordinated with the primary carrier, before they can be considered for payment by CBH. DBH/CBH PROVIDER MANUAL REV.2011 4.7 cl aims department Post-Payment Recoveries According to the City of Philadelphia’s contract with the Commonwealth of Pennsylvania DPW, CBH is required to take all reasonable measures to ensure that CBH is the payor of last resort when other third-party resources are available to cover the cost of medical services. When CBH becomes aware of payments made on behalf of CBH clients who have valid thirdparty resources, post-payment recoveries will be pursued. If a provider is identified as having received an inappropriate payment, a post-payment recovery letter will be sent to the provider. Providers who receive such letters are required to bill the primary carrier(s) and resubmit the claim along with a copy of the recovery letter and the final determination for CBH review and processing. These should not be submitted as regular adjustments. They should be sent to the attention of the CBH staff that is handling the recovery. If CBH does not receive a response within 60 days from the date of the letter on the status of the recovery, CBH will automatically backout the claims. The provider has 90 days from the date the payment has been retracted to submit the claims and EOB and/or final determination letter to CBH for processing. The Commonwealth of Pennsylvania (DPW) will pursue all cases that CBH is unable to recover. Member Co-Payment Prohibition Federal law prohibits treatment providers from requesting co-payments from MA recipients in the Commonwealth of Pennsylvania. Billing CBH members for co-payments for services is also in violation of the CBH Provider Agreement. Where to Mail Claims All manual claims must be sent via the U.S. Postal System or delivery service to: CBH, Claims Department, 801 Market Street, 7th Floor, Philadelphia, PA 19107. Hand-deliveries will not be accepted. WWW.DBHIDS.ORG cl aims department 4.8 Filing Electronic Claims Filing claims electronically helps providers minimize data entry errors after submission, ensure information is legible, and expedite the processing of their claims. In order to submit claims electronically, the provider must have the appropriate software. Please refer to the CBH website, www.dbhids.org for the necessary information regarding the submission of electronic claims. On the website under “HIPAA Resources,” you will find the following key information: � � � � Browser Interface Manual CBH Companion Guide 837 Professional CBH Companion Guide 837 Institutional CBH Companion Guide 835RA Prior to any initial electronic claims submission to CBH, contact Provider Relations at (215) 4137660 for specific information needed to create an electronic file and to coordinate the submission of the test file. A sample of the electronic file submission, adjudication and payment cycle can be found on page 4.34. Filing Manual Claims Providers filing manual claims must use one of two printed claim forms designated for that purpose. Please refer to Schedule A of your CBH Provider Agreement for all contractual services and the appropriate CPT codes, pricing and information modifiers, and BANs. This section provides specific information about which forms are to be submitted for the specific types of treatment. It also provides examples of each form. inpatient claims, UB-04 claim form: All inpatient hospital or RTF-Accredited claims must be submitted using the UB-04 Claim Form. outpatient claims, cms-1500 (08-05) claim form: All other claims must be submitted using the CMS-1500 (08-05) Claim Form. DBH/CBH PROVIDER MANUAL REV.2011 4.9 cl aims department Claims Form Guidelines The succeeding section provides specific details on the use of the UB-04 and CMS-1500 (08-05) Claims Forms. Following is an index: UB-04 Inpatient Billing Provider Information, Compensable Service and Patient Information........................................4.8 UB-04 Inpatient Billing Third Party Liability (TPL) Billing.....................................................................................................4.9 CMS-1500 (08-05) Outpatient Information, Provider Name and Compensable Medical Services..................................4.11 CMS-1500 (08-05) For Outpatient TPL Billing Information, Provider Name and Compensable Medical Services......4.12 Common Causes for Claim Rejections and Remedies for Providers.........................................................................4.18 - 4.20 Specific Claims Submission Information Completion of the UB-04 Claim Form The UB-04 Claim Form is used when an inpatient (hospital inpatient or RTF Accredited) stay has occured. Revenue Codes are used exclusively on the UB-04 claim form. (See sample UB-04 Claim Forms later in this section.) Listed below are the specific fields that must be completed on the UB-04 Claim Form before submitting it to CBH for processing. Remember that all services require an authorization number for billing and only one authorization number per claim form is allowed. When an item is "not applicable," do not use zero. Leave it blank. See the PROMISe Desk Reference for assistance in the completion of the UB-04 Claim Form on pages 4.23 and 4.24. WWW.DBHIDS.ORG cl aims department 4.10 UB-04 PATIENT INFORMATION, PROVIDER NAME, AND COMPENSABLE BEHAVIORAL HEALTH SERVICES Form Locator Field Name Form Locator 1 Billing Provider Name, Address, and Telephone Number 3a Patient Control Number 46 Units of Service 4 Type of Bill (See UB-04) Desk Reference for Hospitals 47 Total Charges 6 Statement Covers Period 47 (23) Total Charges 8a Patient Name 50 Payor Name (Enter the name of each payor organization from which the provider might expect some payment for the bill) Patient Address 56 NPI # (Enter the 10-digit National Provider Identifiier) 10 Patient Birth Date 58 Patient Name 12 Admission Date 60 Patient Number (Enter the 10-digit MA Number) 13 Admission Hour 63 Treatment Authorization Number (CBH Authorization Number) 14 Admission Type (See UB-04 Desk Reference for Hospitals) 67 Principal Diagnosis Code 16 Discharge Hour 69 Admitting Diagnosis Code 17 Patient Status (See UB-04 Desk Reference for Hospitals) 76 Attending Physician NPI# (Enter the 10digit National Provider Identifier) OR QUAL (Enter Attending Physician License Number) Value Codes and Amount (Value Codes must be entered in numeric sequence, starting in From Locators 39a thru 41a, 39b thru 41b, 39c thru 41c, and lastly 39d thru 41d. (See UB-04 Desk Reference for Hospitals) 80 CBH Provider Number 9a-d 39a-41d 42 Revenue Code (See CBH Schedule A) 43 Revenue Code Description 45 (23) Field Name Creation Date (Enter the claim creation date) Each batch of claims submitted MUST be accompanied by 1 (one) properly completed Signature Transmittal Form (MA307) DBH/CBH PROVIDER MANUAL REV.2011 4.11 cl aims department UB-04 INPATIENT THIRD PARTY LIABILITY (TPL) BILLING When using the UB-04 Claim Form for inpatient TPL billing, the fields in the chart below must be completed. The standard fields must also be completed. See Explanation of the Completion of the UB-04 on page 4.26; sample UB-04 – Inpatient Third Party Liability (TPL) Claim Form on page 4.26, and Explanation of Benefits (EOB) for Inpatient UB-04 Third Party Liability (TPL) on page 4.27. UB-04 Inpatient Third Party Liability (TPL) Billing Form Locator 39-41 50 Field Name Form Locator Field Name Value Codes and Amounts (Deductible and coinsurance values, if applicable) 51 Health Plan ID Payer’s name (Enter the name of each payer organization from which the provider might expect some payment for the bill) 54 Prior Payment (Enter the covered charges amount on the EOB (for Medicare, or the other insurance carrier’s payment amount) 55 Estimated Amount Due (Enter the estimated amount you expect to be paid by CBH) ! When using the UB-04 Claim Form to bill for inpatient services, the following information must be retrieved from the EOB and indicated on the form: Information To Be Retrieved From EOB Field No. On UB-04 Claim Form Service From/Thru 6 Covered Days 39-41 Deductibles 39-41 Covered Charges for billed period for Medicare and the other insurance payment amount for other insurance carriers. 54 WWW.DBHIDS.ORG cl aims department 4.12 Completion of the CMS-1500 (08-05) Claim Form The CMS-1500 (08-05) Claim Form is primarily used for outpatient services. WHEN TO USE THE CMS-1500 (08-05) CLAIM FORM The CMS-1500 (08-05) Claim Form may be used when filing a claim for the following behavioral health services: � � � � � � � � � � Outpatient psychiatric treatment Non-hospital services (3a, 3b, 3c) Outpatient drug and alcohol (D&A) treatment services Residential treatment facilities (non-accredited) Psychiatric partial hospital programs (acute and maintenance) Behavioral health rehabilitation services for children Intensive outpatient programs (IOP) Consultations Methadone maintenance Laboratory services The chart on the following page lists the specific fields that must be completed on the CMS-1500 (08-05) Claim Form before submitting it to CBH for processing. Never use zeros in fields for items that are not applicable. Leave spaces blank. E PLEAS NOTE The CMS-1500 (08-05) Paper Claim Form has room for 6 lines of service, but CBH's claims system can only accept 4 lines of service per claim. Use no more than 4 lines of service on the CMS-1500 (08-05) Claim Form. DBH/CBH PROVIDER MANUAL REV.2011 4.13 cl aims department CMS-1500 (08-05) Outpatient Information, Provider Name, and Compensable Behavioral Health Services Form Locator Field Name Form Locator Field Name 1 Type of Claim (Place an X in the Medicaid box) 23 Prior Authorization Number (CBH Authorization Number or BAN Number) 1a Patient Number 24a Date of Service (note begin and end date) 2 Patient Name 24b Place of Service (see OMHSAS Desk Reference) 3 Patient Birth Date 24d Procedure Code (In the first section of the block, enter the procedure code that describes the service provided. In the second section of this block, enter the pricing modifier, when applicable. In the third to fifth sections of this block, enter up to three information modifiers, when applicable. Failure to use the appropriate modifier (s) in the appropriate blocks will result in claim denial.) 5 Patient Address 24e Diagnosis Pointer 12 Patient's or Authorized Person's Signature and Date 24f Usual Charges 17 Name of Referring or Prescribing Practitioner 24g Units of Service 17a Referring or Prescribing Practitioner License Number (enter the first portion of this block, enter two-digit qualifier that indicates the type of ID:) OB = license number ID = 13 digit Provider ID Number in the second portion enter the license number or the 13 digit Provider ID Number of the referring or prescribing practitioner named in Block 17. 28 Total charges (enter total sum of 24f, 1 thru 4 in dollars and cents) 17b Referring or Prescribing Practitioner NPI # (enter the 10 digit National Provider Identifier number) 31 Signature of physician, date claim was submitted or Signature Transmittal Form MA-307 21 Diagnosis (enter the most specific 3, 4, or 5 digit ICD-9-CM code that describes the diagnosis) 33 Billing Provider Name and Address 33a NPI # (enter the 10 digit NPI number of billing provider) WWW.DBHIDS.ORG cl aims department 4.14 CMS-1500 (08-05) Third Party Liability (TPL) Billing When completing the CMS-1500 Claim Form for TPL billing, the following must be completed. The standard fields must also be completed as described on the previous page under Explanation of Completion of the CMS-1500 Claim Form on page 4.11. See sample CMS-1500 (08-05) - Outpatient Third Party Liability (TPL) on page 4.32. CMS-1500 (08-05) For Patient TPL Billing Information, Provider Name, and Compensable Medical Services Field # Field Name Field # 9 Other Insured's Name (Another health insurance secondary to insurance in block 11) 11b Employer's Name or School Name (if applicable) 9a Other Insured's Policy or Group Number (if applicable) (other than MA) 11c Insurance Plan Name or Program Name (other than MA) 9b Other's Insured's Date of Birth (if applicable) 24f Usual Charges (The amounts must agree with the other plan's EOB) 9c Employer's Name or School Name (if applicable) 28 Total Charges (Enter total sum of lines 24f, lines 1 thru 4 in dollars and cents) 11 Primary Insurance (other than MA) policy number (if applicable) 11a Insured's Date of Birth (if applicable) REMINDER Field Name When billing for payment of Medicare deductibles and/or coinsurances for services covered by MA, the provider must use the appropriate MA Procedure Code. DBH/CBH PROVIDER MANUAL REV.2011 4.15 cl aims department Processing Payments When a provider submits a claim to CBH, it goes through several stages of review and processing, as described below: Claims Processing Cycle Adjudication process: CBH will adjudicate 100% of clean claims within 45 days and adjudicate 100% of all claims within 90 days. Adjudicate means to pay or reject a claim. payment of claims: Payment will be mailed in the form of a check to the address designated by the provider in the provider information form. Changes in address must be reported in writing under the signature of the Chief Executive Officer to CBH's Chief Executive Officer, 801 Market Street, 7th Floor, Philadelphia, PA 19107. claims reports: Whether a claim is accepted, rejected or pended, claims reports will be made available to the provider explaining the reasons for the action taken on the claim. (Learn more and see samples in the following section under Claims Reports.) Claims Adjustments On occasion, after a payment has been issued, either CBH Claims staff or the provider may detect an error in the processing of the claim that was paid. The adjustment process deals with the correction of those claims that have been through the adjudication cycle and been paid. If a claim has been rejected and not yet paid, it is not subject to an “adjustment.” Only those claims that have already been paid can be adjusted. Claims adjustments generally occur for the following reasons: Claim was submitted and paid twice. Claim was paid at a wrong rate. Claim was paid for the wrong date(s) of service. Claim was paid at a wrong level of care. Claim was submitted with excessive units of service within time period. Services were span billed with overlapping days on more than one claim. A Compliance audit was conducted. Post Payment recoveries Adjustments must be received within the claims submission timeframes noted on page 4.1 WWW.DBHIDS.ORG cl aims department 4.16 Submitting Adjustments Manually Complete and submit the following: A Claims Adjustment Request Form - Note the invoice number(s) and the invoice line(s) in the space that is provided or attach a copy of the payment detail clearly indicating the line requiring an adjustment Corrected Claim(s) Form The EOB for TPL Claims • Submitting Adjustments Electronically (Where No TPL is Involved) Complete and submit the following: Back-outs only: For claims back-outs of more than 10 invoice lines, a CD must be submitted using Excel, and must only contain the invoice numbers (first column) and line(s) (second column). One adjustment form must be submitted with each CD. Back-out and Reprocess: For claims back-outs of more than 10 invoice lines, a CD must be submitted using Excel, and must contain the invoice numbers (first column) and line(s) (second column). For the related claims reprocessing, submit new claims via FTP once you have confirmation of the original claim reversal. One adjustment form must be submitted with each CD. The top two copies of the Claims Adjustment Request Form must be mailed with the appropriate support documents to: CBH, Claims Department, Attention: Adjustments, 801 Market Street, 7th Floor, Philadelphia, PA 19107. Pended Claims Pended claims are those claims that are put on temporary hold to assure that CBH is the payor of last resort for members that have other primary coverage in addition to MA. It also determines if the services are covered by a third party payor. TPL Claims will pend when: The provider indicates on the claims form that the member has another coverage. The provider submits an EOB along with the claim. During the processing of the claim, CBH's eligibility file, as transmitted by the Pennsylvania DPW, indicates that the client is covered by another insurance. DBH/CBH PROVIDER MANUAL REV.2011 4.17 cl aims department The provider will receive a Rejection Report listing those claims that have pended after the adjudication process. To avoid disruptions to treatment of children, BHRS claims will first pend, but will be released for payment by CBH within two weeks. Rejected/Denied Claims CBH may reject or deny a claim for a variety of reasons. In some cases, crucial claims information, such as dates, authorization numbers or client information, may be missing or incorrect. In addition, the provider may not have submitted the claim to the primary payor. When rejecting a claim, CBH will provide a Rejected/Denied Claims Report listing those claims that have been rejected/denied after the adjudication process. Providers are encouraged to carefully review the original claims, the Rejected/Denied Claims Reports, and to make any necessary corrections or revisions, and when appropriate, resubmit the claims for payment. ! One of the most common causes for claims rejection is entering date information incorrectly. When entering inpatient treatment days, please enter the date of admission as the "begin date" and the day of discharge as the "service end" date, but count the length of the stay according to the number of "nights" of stay. The day of discharge is not counted as a day of treatment. Claims Appeals Process There are three categories of claims rejections that providers may appeal. The processes for each category are described separately. APPEALING REJECTED CLAIMS FOR THIRD PARTY LIABILITY (TPL) CAUSED BY DISCREPANCIES BETWEEN THE ELIGIBILITY VERIFICATION SYSTEM (EVS) AND THE CBH CLAIMS SYSTEM If the provider accesses the EVS information and it indicates that the client does not have TPL coverage, but during processing of the claim, the CBH system detects such coverage and consequently rejects the claim, within 90 days from the date of the rejection the provider must do the following: WWW.DBHIDS.ORG cl aims department 4.18 Note the invoice number(s) and the invoice line(s) with the specific TPL rejection reason or send a copy of the rejection report with the TPL rejection reason. Make a copy of the eligibility information that notes the client does not have TPL coverage. Make a copy of all outstanding claims along with any other evidence of non-coverage by a third party. Mail the above to the CBH Claims Department, 801 Market Street, 7th Floor, Philadelphia, PA 19107. Clearly write on the envelope "TPL Discrepancy." CBH will then perform a manual review of the client's coverage. If it is determined that the client has no TPL coverage. CBH will reprocess the claim and make the necessary system adjustments. If it is found that the client does have TPL coverage CBH will return the claim to the provider along with the name of the primary carrier and policy number. The provider must obtain a final determination from the primary payor dated no more then 180 days following the date of the TPL Discrepancy continuation letter issued by CBH to the provider. The provider must submit a clean claim to CBH within 90 days after receipt of the final determination from the primary payor. APPEALING REJECTED CLAIMS FOR "recipient not eligible" caused by discrepancies between the evs and the cbh claims system If the provider accesses the eligibility information and it indicates that the client is eligible for treatment on a particular date, but during the processing of the claim CBH does not show the individual to be eligible and rejects the claim, within 90 days from the date of rejection the provider must do the following: Make a copy of the rejection report that notes the eligibility rejection. Make a copy of the eligibility information that notes the client was CBH eligible to receive service on the date(s) indicated on the claim. Prepare a new clean claim for the service(s) performed. Mail the above to the CBH Claims Department, 801 Market Street, 7th Floor, Philadelphia, PA 19107. Clearly write on the envelope "Eligibility Rejection Appeal." The claims will be handled by CBH in one of the following ways: If the claim was rejected within the last month, it will be overridden and appear on the next Payment Detail. DBH/CBH PROVIDER MANUAL REV.2011 4.19 cl aims department If the claim rejection is older than one month, we will re-enter the newly submitted claim(s) after the eligibility information is updated in our system. The re-submitted claim(s) will go through our normal adjudication process. E PLEAS NOTE The override for eligiblity applies only to claims that were submitted and rejected for "Recipient Not Eligible." It does not apply to authorization requests that were denied because of ineligibility. APPEALING claims for late submission beyond the timely submission requirements If CBH receives a claim or Adjustment Request Form beyond the timely submission requirements noted on page 4.1, the claim or adjustment form will reject or be returned to the provider due to late submission. Claims or adjustments rejected or returned for late submission may be appealed only due to processing errors made by CBH. The following requirements are necessary in order to be eligible for appeal: Provider had submitted a clean claim within the required timeframes. CBH had improperly processed the clean claim causing an incorrect payment or a rejection only resulting from CBH's processing error. Provider resubmits the clean claim (along with an Adjustment Request Form for incorrect payments) within 90 days from the date of the incorrect payment or rejection. for tpl claims only A letter addressed to the Claims Appeals Specialist indicating the specific cause of the rejection or incorrect payment due to CBH's error. A copy of the rejection report that notes the rejection reason caused by CBH's error or a copy of the payment detail that notes the incorrect payment made due to CBH's error, and A copy of the claim and EOB for TPL claims. If the appeal is due to untimely final EOB, documentation is needed. Documentation must be submitted to explain or show why the final determination could not be obtained timely. Mail all claims appeals to the attention of CBH Claims Appeals Specialist, 801 Market Street, 7th Floor, Philadelphia, PA 19107. Clearly write on the envelope "Claims Appeal." WWW.DBHIDS.ORG cl aims department 4.20 The following chart lists the most frequent causes for claims to be rejected and the remedies for providers. common causes for claim rejectionS and remedies for providers rejection description cause remedy 1. If exact same date(s) of service(s) for same person was previously paid, claim will reject. Check to ensure no data entry error was made. 2. When a provider submits two claims for separate units of service within the same billing period, the second claim will reject if the first claim form has referenced the entire billing period. (For example, a provider has authorization for 30 units from 1/1/08 to 1/31/08. Claim #1 is submitted for 15 units used on 1/1 to 1/15, but references 1/1 to 1/31 on the claim form. If a second claim is submitted for the remaining 15 units with service dates 1/16 to 1/31, the second claim will be rejected because it is covering a period that was already paid, and therefore appears to the system to be an overlapping bill.) Submit a Claims Adjustment Request Form for the initial claim indicating that only a portion of the entire billing period and units of service were used. Also resubmit a corrected claim reflecting the entire billing period. 1. This may occur when all authorized units were paid, and the provider submitted a claim for additional units. 2. If the initial authorization was zeroed out or cancelled, the claim will be rejected for this reason. Check to see if additional date(s) of service for additional units are under another authorization number. If so, resubmit the claim using the corrected authorization. If additional units are needed for the same individual, the CBH Care Manager must approve extending authorization. Then provider can resubmit a claim for the added units. Or, a new authorization may be issued and the provider can re-submit the claim with the correct authorization for payment. Invalid or unknown recipient ID number. If a claim was submitted with the wrong recipient number or no number, the claim will reject. Check to ensure no data entry error was made. Re-submit with the correct CIS number. Recipient was not eligible for service on a specified date. These claims have been rejected because according to CBH records, the client was not eligible for service on that date. Re-submit with proof of eligibility. Attach eligibility information for that date of service for correct processing. Send claims to the attention of the Claims Department "Eligibility Rejections." Billed dates of service do not match authorized dates of service. If a claim is submitted for service dates outside the authorization period, this error will appear. (For example, if the authorization period is for 1/1/08 to 2/1/08 and the claim submitted is for 2/5/08, the claim will be rejected.) Check the authorization report for the correct authorization number for this date of service. Re-submit the claim for the correct period or obtain a corrected authorization. Claim line was previously paid. No units of service left for this authorization DBH/CBH PROVIDER MANUAL REV.2011 4.21 cl aims department rejection description cause remedy Invalid primary ICD-9 Behavioral Diagnosis Code Diagnosis code is not considered valid by CBH, was not correctly entered, or was missing on the claim. Use the correct ICD-9 code number, for proper payment. Contact Provider Relations at (215) 413-7660 if you need assistance. Invalid or unknown authorization number The claim was submitted either with no authorization number, an incorrect authorization number, or no BAN or an incorrect BAN. Check to ensure no data entry error was made. Re-submit with correct authorization number or BAN. Client is not the same as client referenced in authorization This rejection will typically appear Refer to authorization report to check when the client number in the claim for accuracy of client number or form is not the same as the client num- authorization number. ber on the authorization. This rejection will also appear with the "Invalid or unknown recipient number," and with "Invalid or unknown authorization number." Provider is not the same as provid- Provider number billed is not the same Re-submit the correct provider number as the one referenced in the authoriza- that was authorized, or request that er of authorization referenced tion. the authorization be changed. Service is not the same as service of authorization referenced. Service is not the same as the service referenced in the authorization. Claim report will indicate wrong service was used. (The claim was submitted with the incorrect authorization or the incorrect CPT or revenue code.) This rejection will also appear with "Invalid or unknown authorization number." Re-submit with the correct authorization or the correct CPT or revenue code. Claim is no longer eligible for payment: late submission Claim is submitted beyond the timely submission requirements. Refer to Claims Appeals Process section of the manual. Unknown or invalid case number Case is not opened. Reference Case Open Process in Authorization section of this manual. Cannot match provider to service for specific date Discrepancy in the Contract Schedule A for that level of care Verify the billing combination matches your Schedule A. Contact Provider Relations at (215) 413-7660 if you need assistance. No-known cross-reference for NPI to provider ID Provider submitted claims with NPI number which is not connected to CBH number Re-submit with the correct NPI number that is connected to CBH number. Blanket Authorization Numbers 1000 are being replaced Claims submitted with the old blanket authorization number Re-submit with the correct 9-digit blanket authorization number WWW.DBHIDS.ORG 4.22 cl aims department rejection description cause remedy No known cross-reference of NPI to authorized provider identification number. Provider submitted wrong authorization numbers for billed NPI numbers Re-submit with correct NPI number that is connected to CBH number issued to the authorization Non-Electronic claim with Invalid/ Unknown provider NPI Provider submitted incorrect NPI number not listed on their Contract Schedule A Re-submit with correct NPI number Electronic claim with Invalid/Unknown provider NPI Provider submitted incorrect NPI number not listed on their Contract Schedule A Re-submit with correct NPI number Claim without NPI provider ID Claim submitted without NPI number Re-submit with the correct NPI number Claims Reports Below are brief descriptions of the available claims reports via download from the CBH EDI Browser: The Payment Detail Report lists all paid services. The Rejected/Denied/Pended Claims Report refers to all claims that will not be paid by CBH as submitted. It lists pended claims, warnings, and the reasons for denials and rejections along with their corresponding amounts. OTE EN PLEAS For help in understanding your rejected claims report, see Common Causes for Claims Rejection and Remedies for Providers. DBH/CBH PROVIDER MANUAL REV.2011 4.23 cl aims department Sample Forms The succeeding section provides reference materials as well as samples of claims forms and reports: Claims Adjustment Request Form..............................................................................................................................................4.22 PROMISe UB-04 Desk Reference for Hospitals..............................................................................................................4.23 - 4.24 UB-04 Inpatient Claim Form.......................................................................................................................................................4.25 UB-04 Inpatient Third Party Liability (TPL) Claim Form.......................................................................................................4.26 Explanation of Benefits (EOB) for Inpatient UB-04 Third Party Liability (TPL).................................................................4.27 Pennsylvania Office of Mental Health and Substance Abuse Services (OMHSAS) Desk Reference OMHSAS Desk Reference - Provider Types.............................................................................................................4.28 - 4.29 OMHSAS Desk Reference - Modifiers.................................................................................................................................4.29 OMHSAS Desk Reference - HIPAA Place of Service Codes.............................................................................................4.30 assistance in completion of the outpatient and cms-1500 (08-05) CMS-1500 (08-05) - Outpatient Claim Form........................................................................................................................4.31 CMS-1500 (08-05) - Outpatient Third Party Liability (TPL) Claim Form........................................................................4.32 Explanation of Benefits (EOB) for CMS-1500 (08-05) Outpatient Third Party Liability (TPL) ....................................4.33 WWW.DBHIDS.ORG cl aims department DBH/CBH PROVIDER MANUAL REV.2011 4.24 4.25 cl aims department PA PROMISe™ Provider Handbook 837 Institutional/UB-04 Claim Form UB-04 Desk Reference for Hospitals These values are valid for paper claim submission on the UB-04 Claim Form only. Condition Codes (continued) X3 Hysterectomy Acknowledgment Form (MA 30) X4 Medicare Denial on File X5 Third Party Payment on File X6 Restricted Recipient Referral Form X7 Medical Documentation for Hysterectomy Y0 Newborn Eligibility Y3 Copay Not Collected Y6 Third Party Denial on File Type of Bill Codes (Form Locator 4) INPATIENT ONLY: First Digit 1 Type of Facility – Hospital Second Digit 1 Bill Classification – Inpatient Third Digit 0 Non Payment/Zero Claim 1 Admit through Discharge Claim 2 Interim – First Claim 7 Replacement of Prior Claim 8 Void/Cancel of Prior Claim OUTPATIENT ONLY: First Digit 1 Type of Facility – Hospital Second Digit 3 Bill Classification – Outpatient 4 Bill Classification – Hospital Special Treatment Room Third Digit 0 Nonpayment/Zero Claim 1 Admit through Discharge Claim 7 Replacement of Prior Claim 8 Void/Cancel of Prior Claim Patient Status Codes (Form Locator 17) 01 Discharge to home or self-care – Routine Discharge 02 Discharged/transferred to another hospital for inpatient care 03 Discharged/transferred to a skilled nursing facility 04 Discharged/transferred to an intermediate care facility 05 Discharged/transferred to another type of institution for inpatient care 07 Left against medical advice or discontinued care 20 Expired 30 Still a patient Admission Type (Form Locator 14) 1 Emergency Admission 2 Urgent Admission 3 Elective Admission 4 Newborn Admission 5 Trauma Admission (Emergency Admission) Occurrence Codes (Form Locators 31–34) 01 Auto Accident 02 No Fault Accident 03 Accident/Tort Liability 04 Accident/Employment Related 05 Other Accident 06 Crime Victim 24 Date Insurance Denied 25 Date Benefits Terminated By Primary Payer A3 Benefits Exhausted B3 Benefits Exhausted C3 Benefits Exhausted DR Disaster Related Condition Codes (Form Locators 18–28) 02 Condition is Employment Related 03 Patient is Covered by Insurance Not Reflected Here 05 Lien Has Been Filed 60 Day Outlier 77 Provider accepts or is obligated/required to a contractual agreement or law to accept payment by primary payer as payment in full A1 EPSDT A4 Family Planning Outpatient AA Abortion Consent (MA 3) – Rape AB Abortion Consent (MA 3) – Incest AD Abortion Consent (MA 3) – Danger to Life AI Sterilization Patient Consent Form (MA 31) B3 Pregnancy X2 Medicare EOMB on File Provider Handbook UB-04 Occurrence Span Codes (Form Locator 35–36) 71 Prior Stay Dates 74 Non-covered Level of Care/Leave of Absence (JCAHO RTF only) MR Disaster Related 1 January 14, 2008 WWW.DBHIDS.ORG cl aims department PA PROMISe™ Provider Handbook 837 Institutional/UB-04 Claim Form Value Codes (Form Locators 39–41) 06 Medicare Blood Deductible 14 No Fault, Including Auto/Other 15 Worker’s Compensation 16 PHS or Other Federal Agency 38 Medicare Blood Deductible Pints Furnished 39 Medicare Blood Deductible Pints Replaced 47 Any Liability Insurance 66 Patient Pay 80 Covered Days 81 Non-Covered Days 82 Co-insurance Days 83 Lifetime Reserve Days, Inpatient Only A1 Deductible Payer A A2 Coinsurance and Lifetime Reserve Payer A A7 Copayment, Payer A B1 Deductible Payer B B2 Coinsurance and Lifetime Reserve Payer B B7 Copayment, Payer B X0 Medicare Part B Present on Admission (POA) Indicator Codes (Form Locators 67, 67 A-Q) INPATIENT ONLY: Y Yes, present at the time of inpatient admission N No, not present at the time of inpatient admission U Unknown, documentation is insufficient to determine if condition was present at time of inpatient admission W Clinically undetermined, provider is unable to clinically determine whether condition was present at time of inpatient admission or not 1 Exempt from POA reporting Claims Adjustment Reason Codes (Form Locator 80) 8001 Changing the Patient Control Number 8002 Changing the Covered Dates 8003 Changing the Covered/Non covered Days 8004 Changing the Admission Dates/Time 8005 Changing the Discharge Times 8006 Changing the Status 8007 Changing the Medical Record Number 8008 Changing the Condition Codes (sometimes to make claim an “outlier” claim) 8009 Change the Occurrence Codes 8010 Changing the Value Codes 8011 Change the Revenue Codes 8012 Change the Units Billed 8013 Change the Amount Billed 8014 Change the Payer Codes 8015 Change the Prior Payments 8016 Change the Prior Authorization Number 8017 Change the Diagnosis Codes 8018 Change the ICDN Codes and Dates 8019 Change the Phys. ID Numbers 8020 Changed the Billed Date Patient’s Relationship to Insured Codes (Form Locator 59) 01 Spouse 04 Grandparent 05 Grandchild 07 Niece/Nephew 10 Foster Child 15 Ward of the Court 17 Step Child 18 Patient is Insured 19 Natural Child/Insured Financial Responsibility 20 Employee 21 Unknown 22 Handicapped Dependent 23 Sponsored Dependent 24 Minor Dependent of a Minor Dependent 29 Significant Other 32 Mother 33 Father 36 Emancipated Minor 39 Organ Donor 40 Cadaver Donor 41 Injured Plaintiff 43 Natural Child/Insured does not have Financial Responsibility 53 Life Partner G8 Other Relationship Please note that the Patient’s Relationship to Insured Codes are the same codes used electronically in the 837I. Provider Handbook UB-04 DBH/CBH PROVIDER MANUAL REV.2011 2 January 14, 2008 4.26 4.27 cl aims department 1 2 3a Pat. Cntl # Provider Name Type of Bill b Med. Rec. # Address Telephone Number 5 111 6 Fed. Tax No. Patient Name a 9 Doe, Jane b Patient Address b 11 Birthdate Admission Sex 12 Date 13 Hr 10-10-47 3-01-07 Occurrence Code Date Occurrence Code Date 31 32 11 14 2 15 Type 16 Src 33 DHR 18 17 34 Occurrence Code Date a 3-10-07 1234 Maple Lane c Philadelphia Stat d PA e 19121 19 20 01 21 22 23 24 25 26 35 Occurrence Code Date 27 30 29 Condition Codes 18 7 Statement Covers Period From Through 3-1-07 8 10 4 90876543 28 ACDT state 36 Occurrence Span Code From Through 37 Occurrence Span Code From Through a b 39 40 Value Codes Code Amount 38 a b 80 41 Value Codes Code Amount Value Codes Code Amount 9 c d 42 43 Rev cod 114 44 Description Inpatient 45 HCPCS/Rate/HIPPS code 46 Serv. 9 Serv. units 47 Total Charges 9750 00 48 Non-covered charges 49 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 PAGE ____ OF _____ 50 51 Payer Name CBH 58 6-1-07 CREATION DATE 52 Health Plan ID 53 Rel Info Asg. Ben. 54 9750 TOTALS 55 Prior Payments 56 Est. Amt Due 57 NPI Other Prv ID 59 Insured’s Name P. Rel 60 61 Insured’s Unique ID 1023456789 62 Group Name 00 23 9876543210 A 1234567890002 B C Insurance Group No. A B 63 64 Treatment Authorization Codes 7000000 66 69 DX 65 Document Control Number 68 290.3 Admit DX 290.3 74 Principal Procedure Code Date c Other Procedure Code Date 70 71 Patient Reason DX b a Other Procedure Code Date Other Procedure Code Date d e Other Procedure Code Date Other Procedure Code Date 72 PPS Code 654321 81CC a b c d A B C 73 ECI 75 76 Attending NPI Last 77 Operating 78 Other 79 Qual MD123456 Qual First NPI Last Other Last 1123456789 First NPI Last Remarks C Employer Name Qual First NPI Qual First WWW.DBHIDS.ORG 4.28 cl aims department 1 2 3a Pat. Cntl # Provider Name Telephone Number b 10 a Patient Name 11 Birthdate Type of Bill b Med. Rec. # Address 8 4 908771132 5 9 Doe, John b Admission Sex 12 Date 13 Hr 2-5-59 5-22-07 Occurrence Code Date Occurrence Code Date 31 09 32 14 2 15 Type 16 Src 33 DHR 13 17 34 Occurrence Code Date Fed. Tax No. 20 First Street c Philadelphia 01 5-30-07 d PA e 19111 18 19 20 X2 21 22 23 24 25 26 35 Occurrence Code Date 27 30 29 Condition Codes Stat 7 Statement Covers Period From Through 5-22-07 a Patient Address 111 6 28 ACDT state 36 Occurrence Span Code From Through 37 Occurrence Span Code From Through a b 40 39 Value Codes Code Amount 38 a b A1 41 Value Codes Code Amount 992 00 80 Value Codes Code Amount 8 c d 42 43 Rev cod 124 44 Description Inpatient 45 HCPCS/Rate/HIPPS code 46 Serv. 8 Serv. units 47 Total Charges 8000 00 48 Non-covered charges 49 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 PAGE ____ OF _____ 50 51 Payer Name Medicare CBH 58 Health Plan ID 123456 59 Insured’s Name 6-1-07 CREATION DATE 52 P. Rel 60 53 Rel Info Asg. Ben. 54 55 Prior Payments 1996 61 Insured’s Unique ID 111456789 8000 TOTALS 00 56 Est. Amt Due 992 57 NPI Other Prv ID 00 62 Group Name 00 23 9876543210 A 1234567890002 B C Insurance Group No. A B 63 64 Treatment Authorization Codes 8000000 66 69 DX Employer Name 68 296.34 Admit DX 296.34 74 Principal Procedure Code Date c Other Procedure Code Date 80 65 Document Control Number C 70 71 Patient Reason DX b a Other Procedure Code Date Other Procedure Code Date d e Other Procedure Code Date Other Procedure Code Date 72 PPS Code 75 76 Attending NPI Last 77 Operating 765341 81CC a b c d DBH/CBH PROVIDER MANUAL REV.2011 78 Other Other Last Qual Qual First NPI Last 79 1123460889 First NPI Last Remarks 73 ECI Qual First NPI Qual First MD654321 A B C cl aims department 4.29 EXPLANATION OF BENEFITS (EOB) FOR INPATIENT UB-04 THIRD PARTY LIABILITY (TPL) (Sample) Patient Control Number RC RC REM REM PROF COMP OUTCO CAPCD DRG CAP AMT DRG# MSP PAYMT NCOVD CHGS COVD CHGS COINSURANCE INTEREST ESRD NET ADJ PAT REFUND HCPCS AMOUNT PER DIEM RATE CONTRACT ADJ FIFTH AVENUE PLACE, PITTSBURGH, PA 15222 TEL# 412-255-7000 PART A PAID DATE: 6/18/08 REMITN: 147 PAGE 1 Patient Name ICN Number REM VERITUS MEDICARE SERVICES FEEL GOOD HOSPITAL HIC Number RC .00 8000.00 .00 345.00 4442.05 DRG OUT AMT FROM DT THRU DT NACHG HICHG TOB DENIED CHGS .00 NET REIMB DEDUCTIBLES B3 .00 992.00 .00 .00 .00 992.00 .00 .00 .00 .00 8000.00 .00 .00 .00 . 00 4442.05 1996.00 .00 . 00 4442.05 Covered charges .00 .00 8000.00 .00 . 00 .00 .00 .00 1996.00 1996.00 .00 .00 .00 Deductible .00 992.00 Net Reimbursement Co-insurance DRG OPR AMT 01 HA02 REM 111 COVDY NCOVDY N 8 8 A2 RC COST 1575179 CLM STATUS Doe, John 19815609540204 QC 8 8 Covered days 8 Service from/thru 123456789A 05/22/2007 05/30/2007 1 Subtotal Fiscal Year 2007 Subtotal Part A 8 .00 WWW.DBHIDS.ORG cl aims department 4.30 omhsas desk reference - provider types Provider Type Provider Type Description Provider Type 01 Inpatient Facility 010 011 013 018 019 022 027 183 07 24a 08 Capitation Clinic 09 CRNP 093 548 549 559 11 Mental Health/Substance Abuse 110 111 112 113 114 115 116 117 118 119 123 127 128 129 131 132 133 134 184 548 549 559 16 Nurse 162 17 Therapist 174 175 19 Psychologist 190 548 549 559 DBH/CBH PROVIDER MANUAL REV.2011 080 081 082 084 110 184 548 549 559 Provider Speciality Description Acute Care Hospital Private Psychiatric Hospital RTF (Accredited) Hospital Extended Acute Psychiatric Inpatient Unit D&A Rehabilitation Hospital/Unit Private Psychiatric Unit RTF (Accredited) Unit Hospital-Based Medical Clinic Managed Care Organization-Behavioral Health Federally Qualified Health Center Rural Health Clinic Independent Medical/Surgical Clinic Methadone Maintenance Psychiatric Outpatient D&A Outpatient Therapeutic Staff Support Mobile Therapy Behavioral Specialist Consultant CRNP Therapeutic Staff Support Mobile Therapy Behavioral Specialist Consultant Psychiatric Outpatient Community Mental Health Outpatient Practitioner - Mental Health Partial Psychatric Hospital - Children Partial Psychiatric Hospital - Adult Family Based Mental Health Licensed Clinical Social Worker Licensed Social Worker Mental Health Crisis Intervention Mental Health - OMHSAS Psychiatric Rehabilitation D&A Outpatient D&A Intensive Outpatient D&A Partial Outpatient D&A Medically Monitored Halfway House D&A Medically Monitored Detox D&A Medically Monitored Resid., Short Term D&A Medically Monitored Resid., Long Term Outpatient D&A Therapeutic Staff Support Mobile Therapy Behavioral Specialist Consultant Psychiatric Nurse Art Therapist Music Therapist General Psychologist Therapeutic Staff Support Mobile Therapy Behavioral Specialist Consultant 4.31 cl aims department Provider Type Provider Type Description Provider Type Provider Speciality Description 21 Case Manager 138 212 221 222 D&A Targeted Case Manager MA Case Management Mental Health TCM - Resource Coordination Mental Health TCM - Intensive 28 Laboratory Physician 280 Program Exception Community Residential Rehabilitation 340 52 56 Residential Treatment Facility 560 Independent Laboratory Psychiatry & Neurology Therapeutic Staff Support Mobile Therapy Behavioral Specialist Consultant Program Exception Child Residential Service - 3800 (Group Home) Community Residential Rehabilition - Mental Health (Host Home) Residential Treatment Facility (Non-Accredited) 31 34 339 548 549 559 520 523 omhsas desk reference - modifiers Modifiers Modifier Descriptions Modifiers Modifier Descriptions AH Clinical Psychologist TF Intermediate Level of Care EP TG Complex/High-Tech Level of Care TJ HE Services Provided as Part of Medicaid EPSDT Program Child/Adolescent Program Adult Program, Non-Geriatric Mental Health Program HF Substance Abuse Program UA Program Group, Child and/or Adolescent Follow-up Service Individualized Service Provided to More than One Patient in Same Setting Licensed Children's Program HG Opiod Addiction Treatment Program UB Behavioral Health Pricing Modifier HK UC Pilot Program HO Specialized Mental Health Program for High-Risk Populations Master's Degree Level UK Someone Other than the Client (Collateral) HP Doctoral Level U1 Psychiatric HQ Group Setting U2 Medicare/TPL Contractual Disallowance HT Multi-Disciplinary Team U7 Pricing Modifier HW Funded by State Mental Health Agency U8 Pricing Modifier SC Medically Necessary Service or Supply HA HB TS TT WWW.DBHIDS.ORG cl aims department 4.32 omhsas desk reference - hipaa place of service codes Use only the HIPAA Place of Service (POS) Codes listed below when submitting claims to DBH/CBH. These are the codes expected by DPW for DBH/CBH services. Do not use any other codes listed in the 837 Professional Billing Guide from the Commonwealth of Pennsylvania. POS Place of Service Description POS Place of Service Description 11 Office 50 Federally Qualified Health Center 12 52 22 Home Mobile Unit Inpatient Hospital Outpatient Hospital 23 Emergency Room - Hospital 65 Psychiatric Facility - Partial Hospital ICF/MR Psychiatric Residential Treatment Facility Non-Residential Substance Abuse Treatment Facility End-Stage Renal Disease Treatment Facility 24 Ambulatory Surgical Center 72 Rural Health Clinic 31 Skilled Nursing Facility 81 Independent Laboratory 32 Nursing Facility 99 Other POS 49 Independent Clinic 15 21 DBH/CBH PROVIDER MANUAL REV.2011 54 56 57 4.33 cl aims department CARRIER 1500 (Sample CBH) HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA PICA MEDICARE (Medicare #) MEDICAID X TRICARE CHAMPUS (Sponsor’s SSN) (Medicaid #) GROUP HEALTH PLAN (SSN or ID) CHAMPVA (Member ID#) OTHER 1a. INSURED’S I.D. NUMBER FECA BLK LUNG (SSN) 3. PATIENT’S BIRTH DATE MM DD YY 5. PATIENT’S ADDRESS (No., Street) 6. PATIENT RELATIONSHIP TO INSURED Brown, Lily 625 Daisy Street Self CITY STATE Philadelphia PA M F Child Spouse 4. INSURED’S NAME (Last Name, First Name, Middle Initial) SEX 28 1935 03 19122 7. INSURED’S ADDRESS (No., Street) Other 8. PATIENT STATUS STATE CITY Single Married Other Employed Full-Time Student Part-Time Student TELEPHONE (Include Area Code) ZIP CODE 0123456789 (ID) 2. PATIENT’S NAME (Last Name, First Name, Middle Initial) (For Program in Item 1) ZIP CODE ( 215 ) 222-0000 TELEPHONE (Include Area Code) ( ) 9. OTHER INSURED’S NAME (Last Name, First Name, Middle Initial) 10. IS PATIENT’S CONDITION RELATED TO: 11. INSURED’S POLICY GROUP OR FECA NUMBER a. OTHER INSURED’S POLICY OR GROUP NUMBER a. EMPLOYMENT? (Current or Previous) a. INSURED’S DATE OF BIRTH MM DD YY NO YES b. OTHER INSURED’S DATE OF BIRTH MM DD YY b. AUTO ACCIDENT? SEX PLACE (State) c. EMPLOYER’S NAME OR SCHOOL NAME c. OTHER ACCIDENT? c. INSURANCE PLAN NAME OR PROGRAM NAME NO YES d. INSURANCE PLAN NAME OR PROGRAM NAME d. IS THERE ANOTHER HEALTH BENEFIT PLAN? 10d. RESERVED FOR LOCAL USE YES READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. 12. PATIENT’S OR AUTHORIZED PERSON’S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below. SIGNED DATE 14. DATE OF CURRENT: MM DD YY ILLNESS (First symptom) OR INJURY (Accident) OR PREGNANCY(LMP) 17a. OB John, M. M. D. 17b. NPI 19. RESERVED FOR LOCAL USE 05/24/2007 SIGNED MD123456X O123456789 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES MM DD YY MM DD YY FROM TO 20. OUTSIDE LAB? YES 21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY (Relate Items 1, 2, 3 or 4 to Item 24E by Line) 1. If yes, return to and complete item 9 a-d. NO 13. INSURED’S OR AUTHORIZED PERSON’S SIGNATURE I authorize payment of medical benefits to the undersigned physician or supplier for services described below. 15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS. 16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION DD YY MM DD YY MM DD YY GIVE FIRST DATE MM FROM TO 17. NAME OF REFERRING PROVIDER OR OTHER SOURCE 304 F b. EMPLOYER’S NAME OR SCHOOL NAME NO YES F M SEX M PATIENT AND INSURED INFORMATION 1. 03 $ CHARGES NO 22. MEDICAID RESUBMISSION CODE ORIGINAL REF. NO. 3. 23. PRIOR AUTHORIZATION NUMBER MM 1 05 DATE(S) OF SERVICE From To DD YY MM DD 24 07 05 YY B. C. PLACE OF SERVICE EMG 24 07 4. D. PROCEDURES, SERVICES, OR SUPPLIES (Explain Unusual Circumstances) CPT/HCPCS MODIFIER HF H0018 11 10101010 E. DIAGNOSIS POINTER F. 160 1 H. G. 00 I. J. RENDERING PROVIDER ID. # EPSDT ID. Family Plan QUAL. DAYS OR UNITS $ CHARGES 2 NPI 2 NPI 3 NPI 4 NPI 5 NPI 6 NPI 25. FEDERAL TAX I.D. NUMBER SSN EIN 26. PATIENT’S ACCOUNT NO. 27. ACCEPT ASSIGNMENT? (For govt. claims, see back) YES 31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS (I certify that the statements on the reverse apply to this bill and are made a part thereof.) SIGNED 06/01/2007 DATE 32. SERVICE FACILITY LOCATION INFORMATION NO 28. TOTAL CHARGE $ 160 00 29. AMOUNT PAID Name & Address a. NUCC Instruction Manual available at: www.nucc.org NPI b. NPI 1123457789 a. 30. BALANCE DUE $ 33. BILLING PROVIDER INFO & PH # PHYSICIAN OR SUPPLIER INFORMATION 2. 24. A. $ ( ) b. APPROVED OMB-0938-0999 FORM CMS-1500 (08/05) WWW.DBHIDS.ORG 4.34 cl aims department CARRIER TPL 1500 (Sample CBH) HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA PICA MEDICARE (Medicare #) MEDICAID X TRICARE CHAMPUS (Sponsor’s SSN) (Medicaid #) GROUP HEALTH PLAN (SSN or ID) CHAMPVA (Member ID#) OTHER 1a. INSURED’S I.D. NUMBER FECA BLK LUNG (SSN) 3. PATIENT’S BIRTH DATE MM DD YY 5. PATIENT’S ADDRESS (No., Street) 6. PATIENT RELATIONSHIP TO INSURED Brown, Lily 03 625 Daisy Street Self CITY STATE Philadelphia PA M F Child Spouse 4. INSURED’S NAME (Last Name, First Name, Middle Initial) SEX 28 1935 19122 7. INSURED’S ADDRESS (No., Street) Other 8. PATIENT STATUS STATE CITY Single Married Other Employed Full-Time Student Part-Time Student TELEPHONE (Include Area Code) ZIP CODE 0123456789 (ID) 2. PATIENT’S NAME (Last Name, First Name, Middle Initial) (For Program in Item 1) ZIP CODE ( 215 ) 222-0000 TELEPHONE (Include Area Code) ( ) 9. OTHER INSURED’S NAME (Last Name, First Name, Middle Initial) 10. IS PATIENT’S CONDITION RELATED TO: 11. INSURED’S POLICY GROUP OR FECA NUMBER a. OTHER INSURED’S POLICY OR GROUP NUMBER a. EMPLOYMENT? (Current or Previous) a. INSURED’S DATE OF BIRTH MM DD YY 123456789A b. OTHER INSURED’S DATE OF BIRTH MM DD YY b. AUTO ACCIDENT? SEX Medicare d. IS THERE ANOTHER HEALTH BENEFIT PLAN? 10d. RESERVED FOR LOCAL USE YES READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. 12. PATIENT’S OR AUTHORIZED PERSON’S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below. DATE 14. DATE OF CURRENT: MM DD YY ILLNESS (First symptom) OR INJURY (Accident) OR PREGNANCY(LMP) 17a. OB John, M. M. D. 05/24/2007 SIGNED 17b. NPI MD123456X O123456789 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES MM DD YY MM DD YY FROM TO 19. RESERVED FOR LOCAL USE 20. OUTSIDE LAB? YES 21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY (Relate Items 1, 2, 3 or 4 to Item 24E by Line) 304 If yes, return to and complete item 9 a-d. NO 13. INSURED’S OR AUTHORIZED PERSON’S SIGNATURE I authorize payment of medical benefits to the undersigned physician or supplier for services described below. 15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS. 16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION DD YY MM DD YY MM DD YY GIVE FIRST DATE MM FROM TO 17. NAME OF REFERRING PROVIDER OR OTHER SOURCE 1. F c. INSURANCE PLAN NAME OR PROGRAM NAME NO YES SIGNED 1935 NO c. OTHER ACCIDENT? d. INSURANCE PLAN NAME OR PROGRAM NAME 28 SEX M PLACE (State) b. EMPLOYER’S NAME OR SCHOOL NAME YES F M c. EMPLOYER’S NAME OR SCHOOL NAME 03 NO YES PATIENT AND INSURED INFORMATION 1. 03 $ CHARGES NO 22. MEDICAID RESUBMISSION CODE ORIGINAL REF. NO. 3. 23. PRIOR AUTHORIZATION NUMBER MM 1 12 DATE(S) OF SERVICE From To DD YY MM DD 27 06 12 YY B. C. PLACE OF SERVICE EMG 4. D. PROCEDURES, SERVICES, OR SUPPLIES (Explain Unusual Circumstances) CPT/HCPCS MODIFIER F. 90 H. G. I. 00 1 NPI 2 NPI 3 NPI 4 NPI 5 NPI 6 90 25. FEDERAL TAX I.D. NUMBER SSN EIN 26. PATIENT’S ACCOUNT NO. 27. ACCEPT ASSIGNMENT? (For govt. claims, see back) YES 31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS (I certify that the statements on the reverse apply to this bill and are made a part thereof.) SIGNED 01/01/07 DATE 32. SERVICE FACILITY LOCATION INFORMATION $ 90 NPI 00 29. AMOUNT PAID $ 33. BILLING PROVIDER INFO & PH # Name & Address a. NUCC Instruction Manual available at: www.nucc.org DBH/CBH PROVIDER MANUAL REV.2011 NO 00 28. TOTAL CHARGE NPI b. NPI 0123457789 a. J. RENDERING PROVIDER ID. # EPSDT ID. Family Plan QUAL. DAYS OR UNITS $ CHARGES 1 99242 27 06 11 101010100 E. DIAGNOSIS POINTER ( PHYSICIAN OR SUPPLIER INFORMATION 2. 24. A. 30. BALANCE DUE 27 18 $ ) b. APPROVED OMB-0938-0999 FORM CMS-1500 (08/05) cl aims department 4.35 From 2 Yr. 5 Amount Applied To 3 Amount Amount Codes Service EXPLANATION OF MEDICARE BENEFITS To Deductible 0.00 Approved 54.36 6 Co- ins. 6.80 8 Paid 7 50% of this Provider Medicare Amount 27.18 Medicare Pays 54.36 Medicare Provider Paid 50% of this Medicare Pays 90.00 Billed 51/1 Co-ins Page: 1 27.18 Check Number: 034432427 54.36 Date Paid: 1/24/08 PLC/TYP 4 EXPLANATION OF BENEFITS (EOB) FOR CMS 1500 OUTPATIENT THIRD PARTY LIABILITY (TPL) (Sample) No. XACT Medicare Services Proced. 1 Health Insurance Claim When Patient Mo./Day 7 Amount Applied 12/27 Amount 12/27 Mo./Day Svcs. 1 Code 90862 Number/Control No. Acct. #493848 Amount * Claim Totals Number of To Deductible Amt. 6.80 Week Ending: 1/24/08 0.00 Apprv’d 54.36 Provider Number: 111111 90.00 Billed 1 Claims 36736321446-00 123456789A Name B. Lee Total SUMMARY XXY Mental Health 1234 N. 100th Street Philadelphia, PA 19121 WWW.DBHIDS.ORG • • Sunday 7 File Submission. Adjudication and Payment Example Tuesday 9 Provider receives Response Files TA1, 997 for Filename1.txt. These response files are available on CBH’s FTP Browser Application by 10:00 AM. Filename1.txt moves into Adjudication Provider Submits Filename2.txt Provider submits Filename3.txt. Saturday 6 Provider’s Filename2.txt moves into Adjudication Saturday 13 Friday 5 Electronic Payment detail and rejection reports available by 10:00 AM. Friday 12 Saturday 20 Thursday 4 Provider receives Response Files TA1, 997 for Filename2.txt. These response files are available on CBH’s FTP Browser Application by 10:00 AM. Thursday 11 Friday 19 Wednesday 17 Check sent to Provider will include payments for Filename1.txt Posting of approved adjudicated claims normally occurs. Wednesday 10 Thursday 18 Wednesday 3 November Provider submits Filename1.txt Files normally submitted by 11:30 PM will be adjudicated the next day. Rejection results from Filename3.txt are available by 10:00 AM. Tuesday 2 Filename3.txt moves into adjudication Tuesday 16 Monday 8 Monday 15 Monday 1 A provider submits three text files: filename1.txt (blue), filename2.txt (yellow), and filename3.txt (purple) in two weeks. Adjudication takes place on Mondays, Tuesdays and Fridays, and checks are issued 8 to 12 days later. * Provider receives Response Files TA1, 997 for Filename3.txt. These response files are available on CBH’s FTP Browser Application. Rejection reports for Filename2.txt are available by 10:00 AM. Sunday 14 Check sent to Provider will include Payments for Filename2.txt And payments for Filename3.txt * As noted this is a “Normal Schedule”. CBH will post notifications on the CBH EDI Browser when deviations to this schedule occur. CBH’s contractual obligation is to pay clean claims within 45 days. DBH/CBH PROVIDER MANUAL REV.2011 4.36 cl aims department