ZIOPHARM Oncology - Griffin Securities
advertisement

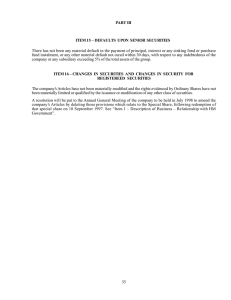
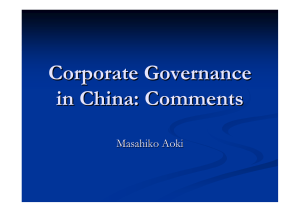
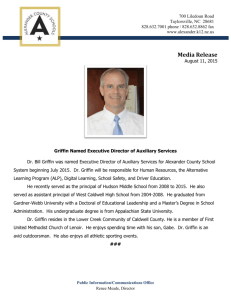
UPDATE REPORT Biotechnology Industry ● October 16, 2013 KEITH A. MARKEY, PH.D., M.B.A. 212-514-7914 KMARKEY@GRIFFINSECURITIES.COM ZIOPHARM ONCOLOGY (NASDAQCM: ZIOP) Gene therapy offers a promising, new paradigm for treating cancer. Ziopharm’s collaboration with Intrexon Corporation is beginning to pay off with encouraging data from clinical studies. Results from a Phase 1 trial of an interleukin-12 (IL-2) gene therapy provided evidence of safety and efficacy in patients with advanced melanoma. But that monogenic therapy is just the beginning, as multigenic therapies that generate several powerful cytokines and/or other anticancer molecules are in the development pipeline. The multigenic treatments should offer an economical and more effective approach to combating the multiple underlying genetic abnormalities associated with different cancers. The latest data set the stage for eight clinical trials to start over the next two years. Ziopharm will present results from four preclinical studies involving advanced gene therapies for cancer at an international meeting being held on October 19 – 23. All were designed to provide the foundation for future clinical studies. Ziopharm has numerous milestones approaching. We believe these will begin to demonstrate the Company’s intrinsic value and generate considerable interest in ZIOP shares. Two clinical trials testing an interleukin-12 gene therapy for advanced melanoma and recurrent/metastatic breast cancer will probably report interim data later this year and full data in 2014. Also, new studies will commence in the first half, targeting glioblastoma with the IL-12 gene therapy and melanoma and breast cancer with combination treatments. Partnering discussions may also prove fruitful in the months ahead. Licensing agreements may provide non-dilutive financing. The Company is seeking partners to complete development of its lead gene therapy and small molecule, legacy drugs. We believe the deals will help to finance the clinical research planned through 2015. We reiterate our BUY recommendation with a 12-month price target to $10.75. Share Price (10/15/2013) 52-Week Price Low / High Mkt. Capitalization (issued) Shares Outstanding (issued) 12-month Target Price Average Daily Volume (3 mos.) Website Est’d 2013 Earn’s (Loss)/shr Est’d 2014 Earn’s (Loss)/shr $4.09 $1.45 – $5.95 $341.6 million 83.52 million $10.75 900,991 www.ziopharm.com ($0.65) ($0.57) Ziopharm Oncology (NasdaqCM: ZIOP) is a clinicalstage company developing gene therapies via an exclusive channel collaboration focused on oncology with the synthetic biology specialist Intrexon Corporation. The most advanced drug is an adenoviral vector for the powerful cytokine interleukin12 that has shown promise against melanoma and breast cancer. The R&D pipeline includes multigenic therapies under ® control of the RheoSwitch Therapeutic System that Source: BigCharts.com may be delivered directly into a target tissue or via a genetically modified cell, such as a mesenchymal stem cell. An expansive number of molecules, including antibody fragments and immunomodulators, may be combined via controlled gene therapy. A few anticancer legacy drugs, including palifosfamide, darinaparsin, and indibulin available for licensing. The most advanced drug, palifosfamide is in a Phase 3 trial for small cell lung cancer. Griffin Securities, Inc., 17 State Street, New York, NY, 10004 www.GriffinSecurities.com Please Review Disclosures on Page 16 of this Research Report 1 Ziopharm Oncology October 16, 2013 TABLE OF CONTENTS Investment Thesis – Multiple Milestones Approach……………………………………………………………...3 The Long-Term Promise of DNA-Based Medicine ....................................................................................... 3 New Therapies & Indications in the Pipeline................................................................................................. 4 Clinical Studies to Yield Data Soon .............................................................................................................. 7 Treating Melanoma.................................................................................................................................... 7 Phase 2 Breast Cancer Trial ..................................................................................................................... 9 Investment Concerns and Risks ................................................................................................................. 11 Financial Forecasts & Valuation ................................................................................................................. 12 Revenue Sources .................................................................................................................................... 12 Annual Income Statements҂ .................................................................................................................... 14 Quarterly Income Statements҂ ................................................................................................................ 14 Balance Sheet҂ ........................................................................................................................................ 15 Valuation Analysis ................................................................................................................................... 15 Disclosures .................................................................................................................................................. 16 GRIFFIN SECURITIES EQUITIES RESEARCH 2 Ziopharm Oncology October 16, 2013 INVESTMENT THESIS – MULTIPLE MILESTONES APPROACH Ziopharm is at the forefront of developing mono- and multi-genic therapies to treat the multigenic disease, cancer. The lead molecule, which causes cells to express the potent cytokine interleukin-12 under the control of an activator ligand, is being tested against advanced melanoma and breast cancer. Interim data from those trials is expected to be announced in late 2013, followed by complete results in 2014. In the meantime, the Company will make four presentations at the International Conference on Molecular Targets and Cancer Therapeutics that demonstrate the considerable utility of the underlying platforms created by its collaborator, Intrexon Corporation. We believe this preclinical research will constitute the basis for some of the eight investigational new drug applications that Ziopharm has scheduled to file over the next two years. These important milestones, plus others related to partnering discussions and its legacy programs involving small-molecule drugs, are shown in Table 1. We believe they will stimulate interest in Ziopharm stock and thereby help to raise the valuation of the shares to our 12-month price target of $10.75 a share. Table 1. Upcoming Ziopharm Milestones Source: Ziopharm Oncology presentation at the BIO Investor Forum, October 2013 THE LONG-TERM PROMISE OF DNA-BASED MEDICINE Over the next five years, investors can look forward to a broad range of therapies emerging from the Ziopharm-Intrexon team’s application of synthetic biology to the multiple malignancies that have eluded modern medicine. Our optimism stems from the proof-of-concept studies that will be presented at the upcoming meeting and from the unique properties of the drug-discovery platform that enables economically feasible therapies, combining cytokines, antibodies, and/or decoy proteins, to target specific types of cancer. The promise of this disruptive technology is perhaps best understood from Figure 1, which shows the multiple combinations of effector molecules and cells that may be used strategically to attack malignant cells and the microenvironment that permits them to survive and proliferate. GRIFFIN SECURITIES EQUITIES RESEARCH 3 Ziopharm Oncology October 16, 2013 Figure 1. The unique toolset available to the Ziopharm-Intrexon team. DNA-based medicine offers the opportunity to intervene in multiple ways to halt malignant cell survival. The approaches highlighted in yellow are the effectors, cells, and anti-tumor functions related to potential therapies developed thus far and are discussed in various levels of detail in this report. Source: Source: Ziopharm Oncology presentation at the BIO Investor Forum, October 2013 NEW THERAPIES & INDICATIONS IN THE PIPELINE Ziopharm has four posters based on preclinical research scheduled for presentation at the AACR/NCI/EORTC International Conference on Molecular Targets and Cancer Therapeutics that will be held on October 19 – 23. Three expand the applications of synthetic biology to innovative therapies for cancer and the fourth sets the stage for an upcoming clinical trial targeting a brain malignancy, glioblastoma. However, it is possible that any or all of the preclinical work summarized below could support clinical development in the next two years. Abstract B127: Pharmacodynamics and functionality of RheoSwitch regulated immunomodulatory proteins, expressed from a multigenic embedded cellular bioreactor following intramuscular electroporation in mice. Malignant growth is a multigenic disease that is not readily treated with monotherapies. Ziopharm has examined the anticancer activities of three immunomodulators, human interleukin-12 (IL-12), interferon-α (INF-α), and a CTLA-4 decoy, in single, dual, and triple combinations in gene therapies controlled by Intrexon’s RheoSwitch. (See next page for a discussion of these molecules.) Expression of the immunomodulators was controlled via oral administration of the activator ligand veledimex (INXN-1001). Expression of seven transgenes in cell cultures and in vivo were compared: three encoding for each gene of interest, three containing a combination of two genes of interest, and one plasmid expressing all three immunomodulators. A single intramuscular injection and electroporation of the transgenes, followed by administration of INXN-1001, increased levels of IL-12, INF-α, and/or CTLA-4 decoy. No expression was seen in cell culture or in vivo absent the activator ligand. This research shows for the first time the feasibility of systemic expression of three immunomodulators from a single RheoSwitch-controlled multigenic construct. GRIFFIN SECURITIES EQUITIES RESEARCH 4 Ziopharm Oncology October 16, 2013 IL-12 or interleukin-12 is a multifunctional cytokine that influences innate and adaptive immunities, notably regulating cell-mediated immune responses. Specifically, it promotes the production of the cytokine interferon-γ, which has multiple effects including inhibiting blood vessel formation, and it stimulates the proliferation and cytotoxic activities of both natural killer cells and T cells.1 (See also Figure 5 on page 8.) Preclinical research has indicated that IL-12 has potent anticancer activity, but due at least in part to dose-limiting adverse side effects its clinical usefulness has been limited.2 Thus far, IL-12 has not been approved for commercial sale. INF-α or interferon-α is a cytokine that causes inflammation that can be either beneficial (e.g., alerting the immune system to an infectious agent or malignant growth) or harmful (e.g., autoimmune diseases, such as systemic lupus erythematosus and colitis). The molecule also stimulates hematopoietic stem cell cycling to maintain the immune cell balance.3 INF-α has been approved for treating cancer.4 And a longacting INF-α (a pegylated version) has been created to provide a more sustained effect. CTLA-4 or cytotoxic T-lymphocyte antigen-4 is an immunomodulatory agent that down-regulates activation of T-cells.5 Its expression is elevated in many tumors to prevent an immune attack, and multiple variants have been identified in various cancers, including lung, oral carcinoma, and breast.6,7,8 A decoy against this molecule interferes with its function and thereby enhances immune surveillance and activity against malignant cells. No therapies targeting CTLA-4 have been approved thus far. Abstract C234: Regulated immunomodulators expression using the RheoSwitch Therapeutic System platform in human mesenchymal stem cells. We find the thrust of this research to be truly innovative – it utilizes the natural proclivity of stem cells to home into areas of tissue damage to deliver an immunotherapeutic gene. Stem cells are probably attracted to malignant growths, much as they are to traumatized tissue by cytokines that signal a part of the body is in need of repair.9 Moreover, the persistence of mesenchymal stem cells in the body is typically measured in months. As such, we believe they are an excellent delivery vehicle for a gene therapy against cancer. The research conducted by Ziopharm and Intrexon demonstrates that human mesenchymal stem cells may be transduced to create genetically modified stem cells that are phenotypically similar to the original cells based upon marker expression. The transduction was achieved with adenoviral vectors for either human or mouse IL-12 with an efficiency of about 90% and with a multiplicity of infection of 20,000/cell. Expression of the cytokine, which was controlled in the expected off-on-off kinetics of a RheoSwitch, was observed for up to 53 days when the activator ligand INXN-1001 was added to or removed from the culture medium. Another experiment tested the expression of three immunomodulators human IL-12, human INFα, and CTLA4 decoy in single, dual, and triple combinations in genetically modified mesenchymal stem cells. Expression of these molecules was controlled by the RheoSwitch and activator ligand, and the human IL- 1 Trinchieri, G. Interleukin-12 and the regulation of innate resistance and adaptive immunity. Nat Rev Immunol (2003); 3(2): 133. Car, BD, et al. The toxicology of Interleukin-12: A review. Toxicol Pathol (1999); 27(1): 58. 3 Essers, MA, et al. INFalpha activates dormant haematopoietic stem cells in vivo. Nature (2009); 458(7240): 904. 4 Mocellin, S, et al. Interferon alpha adjuvant therapy in patients with high-risk melanoma: A systemic review and meta-analysis. J Natl Cancer Inst (2010); 102(7): 493. 5 Sotomayor, EM, et al. In vivo blockade of CTLA-4 enhances the priming of responsive T cells but fails to prevent the induction of tumor antigen-specific tolerance. Proc Natl Acad Sci USA (1999); 96(20): 11476. 6 Antczak, A, et al. CTLA-4 expression and polymorphism in lung tissue of patients with diagnosed non-small-cell lung cancer. BioMed Res Intl (2013); Article ID 576486. 7 Bharti, et al. Functional genetic variants of CTLA-4 risk of tobacco-related oral carcinoma in high-risk North Indian population. Hum Immunol (2013); 74(3): 348. 8 Zhang, B, et al. Genetic variants associated with breast-cancer risk: comprehensive research synopsis, meta-analysis, and epidemiological evidence. Lancet Oncol (2011); 12(5): 477. 9 Nakamizo, A, et al. Human bone marrow-derived mesenchymal stem cells in the treatment of gliomas. Cancer Res (2005); 65(8): 3307. 2 GRIFFIN SECURITIES EQUITIES RESEARCH 5 Ziopharm Oncology October 16, 2013 12 and INFα were found to be fully bio-functional. At the time of the abstract’s preparation the function of the CTLA4 decoy was being tested. This research shows that mesenchymal stem cells retained their natural phenotype after transduction, yet they were capable of expressing the three immunomodulators from single and multigenic constructs. Based on the natural characteristics of these cells, Ziopharm and Intrexon have created a genetically modified cell that will deliver RheoSwitch-controlled, single or multiple cancer immunotherapies directly to tumors. Thus, the collaborators have created a gene therapy with an appropriate delivery vehicle for combating cancer anywhere in the body. Abstract B247: Integration of a modularized protein engineering technology and the RheoSwitch Therapeutic System platform to develop high affinity trastuzumab single chain variable fragment-Fc proteins for gene therapy applications. This research was conducted to demonstrate the utility of a platform for the conversion and assay of monoclonal antibodies into functional single chain variable fragment-Fc fusion proteins that may be encoded as a gene therapy. The molecule contains an antigen-binding region (the single chain variable fragment, scFv) and the constant portion, Fc, of a normal antibody that enables it to interact with proteins of the complement system. (See Figure 2.) The scFv module must be designed for each cancer antigen, such as trastuzumab’s target, human epidermal growth factor receptor-2 (HER-2), which is associated with breast cancer, while the Fc module may be used with any/all such therapies. Figure 2. Structures of a Normal Antibody Source: www.abdesignlabs.com The collaborators used this platform to create a version of trastuzumab (sold by Roche as Herceptin®) and compared the fusion protein with the commercially available antibody. The results showed that the affinity of the scFv-Fc protein expressed by genetically modified cell lines was comparable to that of trastuzumab (Kd: 0.15 nM versus 0.08 nM, respectively) and that the antibody-dependent, cell-mediated cytotoxicities of the two molecules were similar (EC50: 3.6 ng/mL versus 0.94 ng/mL, respectively). In a separate experiment, the platform was used to create a vector for two scFv-Fc molecules having the antigen-binding regions of trastuzumab and cetuximab (an antibody that binds to the epidermal growth factor receptor with a specific gene mutation and that is sold by Bristol-Myers Squibb and Eli Lilly as Erbitux®). The RheoSwitch-controlled multigenic vector was transduced into a myocyte cell line and expression of the two scFv-Fc proteins was controlled by the activator ligand. The results demonstrate the feasibility of creating inducible multigenic antibody therapies for the treatment of cancer. Abstract B298: The controlled expression of IL-12 as an immunotherapeutic treatment of glioma through the use of the RheoSwitch Therapeutic System platform. Details of this research were not available at the time of this writing, due to an embargo on the data. However, we believe the Company tested its adenoviral vector for IL-12, controlled by the RheoSwitch, against a deadly brain cancer. As shown in Figure 3, preclinical results have indicated that the vector has good activity against a glioma model. Accordingly, the foundation has been laid for a clinical study focusing on brain cancer that is scheduled to commence early next year. GRIFFIN SECURITIES EQUITIES RESEARCH 6 Ziopharm Oncology October 16, 2013 Figure 3. Kaplan-Meier survival plots related to a mouse glioma model treated with an IL-12 gene therapy. Glioma is deadly cancer that results in death of the animal within 55 days after implantation of the cells. Administration of Ad-RTS-IL12 or dendritic cells genetically modified with RTS-IL12 (DC-RTS-IL12) on day 5 and daily dosing with activator ligand (AL) resulted in 100% survival up to 80 days post-glioma cell implantation. Controls included dendritic cells (DC) or AL alone, both of which had no effect. Similarly, the two therapeutic agents without the AL had little/no effect. Source: Source: Ziopharm Oncology presentation at the BIO Investor Forum, October 2013 CLINICAL STUDIES TO YIELD DATA SOON Ziopharm is conducting two Phase 2 clinical trials of its lead gene therapy, Adv-RTS-IL-12, as a treatment for advanced melanoma and for breast cancer. Interim data will likely be available later this year and final results should be released in 2014. That information may lead to a licensing agreement, but it probably will also serve as basis for a combination trial(s) of the therapy that is scheduled to start in the first half of next year. Descriptions of the two ongoing trials follow: TREATING MELANOMA The Phase 2 trial was initiated in October 2012 upon completion of a Phase 1 dose-escalation study that reported clinical activity in five of the seven patients treated at the two highest doses tested.10 An example of the therapy’s efficacy is presented in Figure 4, showing a tumor at three time points, on cycle 1 day 1 (start of activator ligand treatment), cycle 1 day 15 (prominent inflammation in the vicinity of the tumor) and cycle 2 day 1 (no observable tumor). Each patient received an intratumoral injection of Ad-RTS-IL12 on day 1 of each 21-day cycle and INXN-1001 (5mg, 20mg, 100mg or 160mg) on days 1 – 7. Figure 4. A Tumor Response to Ad-RTS-IL1210 The four doses of ligand tested yielded a dose-dependent increase in serum levels of IL-12 (ranging from 50pg/mL (5mg INXN-1001 cohort) to 420pg/mL (160mg INXN-1001 cohort) and a similar increase in 10 Linette, GP, et al. A phase 1 open-label study of Ad-RTS-hIL-12, an adenoviral vector engineered to express hIL-12, in combination with an oral activator ligand in subjects with unresectable stage III/IV melanoma. 2013 ASCO Poster #3022. GRIFFIN SECURITIES EQUITIES RESEARCH 7 Ziopharm Oncology October 16, 2013 levels of the cytokine interferon-γ that is induced by IL-12 (100pg/mL – 1000pg/mL). At the highest doses of activator ligand, CD3+ and cytotoxic CD8+ T cells were increased by 7- and 4-fold respectively relative to the levels observed in low-dose cohorts. Most patients experienced immune-related adverse events that are typical with a “cytokine storm” and include fever and chills (73%), fatigue (60%), and vomiting (33%).11 However, unlike the severity seen with prior clinical studies of IL-12, the patients rapidly recovered after INXN-1001 administration ended. The Phase 2 trial, whose design is outlined in Table 2, is being conducted to expand upon the findings of the Phase 1 study by providing a more in-depth assessment of the effects of the gene therapy at a molecular level and on the clinical outcome. Table 2. Melanoma Phase 2 Trial Design Brief Title Safety study of adenovirus vector engineered to express hIL-12 in combination with activator ligand to treat melanoma NCT Number NCT 01397708 Summary This study involves two investigational drugs, an activator ligand (INXN-1001) in combination with an adenovirus vector engineered to express hIL-12. IL-12 is a protein that may enhance the immune system’s ability to kill tumor cells and may interfere with blood flow to the tumor. Estimated Enrollment 30 stage III or IV melanoma patients Estimated Primary Completion Date January 28, 2014 Intervention Ad-RTS-hIL-12 – approximately 1.0 x 10 viral particles per injection one intratumoral injection per study cycle maximum of 6 study cycles INXN 1001 1 dose cohorts at a single dose of 160 mg/day 7 oral daily doses per study cycle (up to 6 cycles) Primary Outcomes Safety and tolerability of intratumoral injections of Ad-RTS-hIL-12 at a constant dose in combination with inter-cohort escalating doses of INXN-1001 Evaluation of the incidence, intensity, and type of adverse events, including clinically significant Secondary Outcomes Determine a recommended dose of INXN-1001 for further study in combination with AdRTS-hIL-12 Obtain preliminary anti-tumor activity according to RECIST 1.1 criteria Evaluate the immunological effect of the treatment in terms of cellular and tumoral responses Evaluate the extent of uptake of of Ad-RTS-hIL-12 into tumor cells and tumor-infiltrating immune cells Eligibility Criteria Inclusion criteria Unresectable stage III or IV melanoma, other than ocular melanoma A minimum of 2 accessible nonvisceral lesions or palpable tumor-involved lymph nodes Expected survival of at least 6 months Exclusion criteria Prior cancer therapy within 28 days prior to first Ad-RTS-hIL-12 dose; steroid or other immunosuppressive therapy Infection requiring antibacterial, antifungal or antiviral therapy within 2 weeks of the first dose of study drug HIV infection, symptomatic brain metastases, or other clinically active malignant disease 12 Given the estimated completion date, the trial’s final results should be available by early spring. 11 Nemunaitis, J. Nonclinical and Phase I clinical studies with a regulated adenoviral gene delivery of IL-12 show promising clinical activity in unresectable stage III/IV melanoma. Presented at the ASGCT Meeting, June 2013. GRIFFIN SECURITIES EQUITIES RESEARCH 8 Ziopharm Oncology October 16, 2013 PHASE 2 BREAST CANCER TRIAL There is ample evidence suggesting that Ziopharm’s IL-12 gene therapy will benefit patients with breast cancer. Intratumoral administration of a liposomal preparation of the cytokine in a preclinical model has found that the cytokine reactivates quiescent memory T cells to proliferate and produce interferon-γ (INFγ).12 That is in keeping with the central role that INF-γ plays in mediating some of the effects of IL-12, as shown in Figure 5.13 Figure 5. Interferon-γ plays a central role in mediating many anticancer effects of IL-12. Cells that respond to IL-12 by producing INF-γ include natural killer-T cells (NKT), natural killer cells (NK), CD4 T helper cells, and cytotoxic CD8 T cells. IL-12 increases T cell priming, effector function, and cell survival. INF-γ helps to reduce new blood vessel formation and extracellular matrix remodeling, which is important in facilitating malignant cell proliferation. INF-γ also increases chemokines with anticancer activities and antigen processing (LMP 2 and LMP7 proteasome subunits). Source: Del Vecchio, M, et al. 13 Other studies have shown that IL-12 alters myeloid-derived suppressor cells in the vicinity of tumors in a preclinical breast cancer model and an adenoviral vector for the cytokine significantly increased animal survival.14 Similarly, an IL-12-based gene therapy delivered via herpes simplex virus proved effective against cancer metastases in the brain, while two combination drugs involving an IL-12 DNA gene therapy and anti-angiogenesis treatments (an antibody against vascular endothelial growth factor, VEGF, and a gene therapy for murine angiostatin) had an additive effect against breast cancer models.15,16,17 The results of these preclinical studies not only provide a basis for Ziopharm’s ongoing Phase 2 breast cancer trial, but also for the development of multigenic therapies including vectors for IL-12 and/or a VEGF sdFvFc. 12 Simpson-Abelson, MR, et al. IL-12 delivered intratumorally by multilamellar liposomes reactivates memory T cells in human tumor microenvironments. Clin Immunol (2009); 132(1): 71. 13 Del Vecchio, M, et al. Interleukin-12: Biological properties and clinical application. Clin Cancer Res (2007); 13(16): 4677. 14 Steding, CE, et al. The role of interleukin-12 on modulating myeloid-derived suppressor cells, increasing overall survival and reducing metastasis. Immunology (2011); 133(2): 221. 15 Cody, JJ, et al. Preclinical evaluation of oncolytic ∆γ1 34.5 herpes simplex virus expressing interleukin-12 for therapy of breast cancer brain metastases. Int J Breast Cancer (2012); 2012: Article ID 628697. 16 Gyorffy, S, et al. Combined treatment of a murine breast cancer model with type 5 adenovirus vectors expressing murine angiostatin and IL-12: A role for combined anti-angiogenesis and immunotherapy. J Immunol (2001); 166(10): 6212. 17 Rakhmilevich, AL, et al. Treatment of experimental breast cancer using interleukin-12 gene therapy combined with anti-vascular endothelial growth factor receptor-2 antibody. Mol Cancer Ther (2004); 3(8): 969. GRIFFIN SECURITIES EQUITIES RESEARCH 9 Ziopharm Oncology October 16, 2013 Information on the Company’s clinical trial evaluating the IL-12 adenoviral vector against breast cancer is provided in Table 3. Table 3. Breast Cancer Phase 2 Trial Design Brief Title A randomized, open-label study of Ad-RTS-IL-12 monotherapy or in combination with palifosfamide in patients with recurrent/metastatic breast cancer and accessible/visible lesions NCT Number NCT01703754 Summary This is a two-part, Phase 2 randomized, safety and efficacy study involving recurrent/metastatic breast cancer with accessible lesions. The first part is a safety run-in for Ad-RTS-IL-12 alone arm and palifosfamide alone arm that will report out by early next year. This will be followed by a combination therapy in a safety run-in arm. The second part is an efficacy evaluation of Ad-RTS-IL-12 as a monotherapy and in combination with the standard-of-care medicines. Estimated Enrollment 68 patients with recurrent/metastatic breast cancer Estimated Primary Completion Date December 2015 (final data collection for primary outcome measure) Intervention Ad-RTS-hIL-12 with the oral activator ligand Palifosfamide, IV administration Primary Outcomes Safety and tolerability of study drug therapy based on the type and rate of adverse events 16-week progression free survival rate, calculated as the number of subjects who had not progressed or died prior to 16 weeks from the date of their first dose, divided by the number of subjects in the study arm Secondary Outcomes Objective response rate by modified RECIST v1.1 Number of patients achieving a confirmed partial or complete response according to modified RECIST v1.1 Clinical benefit rate: proportion of patients with a complete response, partial response, or stable disease Estimate of progression free survival at 24 weeks post-initiation of therapy Pharmacodynamic tumor markers in tumor tissue samples that may correlate with objective tumor response and/or clinical outcome Eligibility Criteria Inclusion criteria Histologically or cytologically confirmed adenocarcinoma of the breast, either locally recurrent or metastatic disease with injectable lesions. Locally recurrent must not be amenable to surgical resection or radiation with curative intent. Disease progression on at least 1 prior systemic chemotherapy + biologic experimental therapy Adequate bone marrow reserve, liver function and renal function. ECOG performance score of 0, 1, or 2. Exclusion criteria HER2/neu-positive cancer Concomitant anticancer therapies, including endocrine therapies Any condition limiting an immune response, immunosuppressive therapy, meningeal carcinomatosis, hypersensitivity to the study drugs or localized infection at the site of the injectable lesion site Results from the first part of this trial, which are expected by early 2014, should provide information that may help in the design of a breast cancer study evaluating a combination therapy scheduled to commence shortly thereafter. GRIFFIN SECURITIES EQUITIES RESEARCH 10 Ziopharm Oncology October 16, 2013 INVESTMENT CONCERNS AND RISKS For a complete description of risks and uncertainties related to Ziopharm Oncology’s business, see the “Risk Factors” section in Ziopharm’s SEC filings, which can be accessed directly from the SEC Edgar filings at www.sec.gov. Potential risks include: Stock risk and market risk: There is a limited trading market for the Company’s common stock. There can be no assurance that an active and liquid trading market will develop or, if developed, that it will be sustained, which could limit one’s ability to buy or sell the Company’s common stock at a desired price. Investors should also consider technical risks common to many small-cap or micro-cap stock investments, such as small float, risk of dilution, dependence upon key personnel, and the strength of competitors that may be larger and better capitalized. New and rapidly changing field: The pharmaceutical and biotechnological markets are rapidly evolving, and research and development are expected to continue at an accelerated pace with increased frequency. Other companies are also actively engaged in the development of therapies to directly or indirectly treat those disorders being pursued by Ziopharm. These companies may have substantially greater research and development capabilities, as well as significantly greater marketing, financial, and human resources abilities than Ziopharm. Products still in development phases: Successful development of the therapies in the R&D pipeline is uncertain, despite the science underpinning the programs. Product development costs and timelines can vary significantly for each product candidate and are difficult to accurately predict. In addition, products in development that appear to be promising may not reach commercialization for various reasons, including failure to achieve regulatory approvals, safety concerns, and/or the inability to be manufactured at a competitive cost. Funding requirements: It is difficult to predict the Company’s future capital requirements. Ziopharm may need additional financing to continue funding the research and development of its products and to expand its business. There is no guarantee that it can secure the desired future capital or, if sufficient capital is secured, that current shareholders will not suffer significant dilution. Regulatory risk: Various statutes and regulations govern or influence the manufacturing, safety, labeling, storage, recordkeeping and marketing of each product. The lengthy process of seeking approval and the subsequent compliance with applicable statutes and regulations require the expenditure of substantial resources. Any failure to obtain, or any delay in obtaining, regulatory approvals could materially adversely affect Ziopharm’s business. There is no guarantee that Ziopharm’s products will be approved by the U.S. Food and Drug Administration (FDA) or international regulatory bodies for marketing in the U.S. or abroad. Licensing risk: Ziopharm intends to outlicense its legacy small molecule drugs for clinical development and commercialization by partners. This strategy may not yield significant upfront fees or subsequent royalties to offset costs of the gene therapy program. In addition, the Company plans to seek a partner(s) to commercialize at least its initial gene therapies and genetically modified cells. Accordingly, the timing of their development and commercialization will not be under the control of the Company. GRIFFIN SECURITIES EQUITIES RESEARCH 11 Ziopharm Oncology October 16, 2013 FINANCIAL FORECASTS & VALUATION Our financial forecasts and valuation analysis are based on the Company’s lead drug for three indications, melanoma, breast cancer, and glioblastoma. Our model also takes into consideration Ziopharm’s financial obligation under its ECC with Intrexon and its strategy to outlicense its drugs for final development and commercialization by licensees. REVENUE SOURCES We have broken down our estimates for melanoma and breast cancer indications into the United States and “other developed countries” as defined by the U.S. Census Bureau to allow for differences in pricing and rates of acceptance of the novel gene therapy. In contrast, we have made a single set of assumptions related to glioblastoma, based on “all developed countries”. The assumptions related to the therapy’s acceptance are provided in the boxes below for each indication/geographic population. A discussion of the assumptions is provided in the closing portion of this section. Melanoma – United States Year penetration starts Starting penetration rate Years between penetration start and peak Peak penetration Duration of peak penetration in years Retention rate in decline years Stage of development 2017 8% Incidence 76,690 Percent addressable 5 40% Price per patient 6 90% Phase 2 15% Market growth rate 2.5% $84,000 Treatment price growth 3% Royalty rate 30% Probability of commercialization 25% Melanoma – Other Developed Countries Year penetration starts Starting penetration rate Years between penetration start and peak Peak penetration Duration of peak penetration in years Retention rate in decline years Stage of development 2017 3% Incidence 92,368 Percent addressable 9 15% Price per patient 6 90% Phase 2 15% Market growth rate 2.5% $60,000 Treatment price growth 3% Royalty rate 30% Probability of commercialization 25% Breast Cancer – United States Year penetration starts Starting penetration rate Years between penetration start and peak Peak penetration Duration of peak penetration in years Retention rate in decline years Stage of development 2018 3% Incidence 234,580 Percent addressable 5 27% Price per patient 4 90% Phase 2 38% Market growth rate 2.5% $84,000 Treatment price growth 3% Royalty rate 30% Probability of commercialization 25% Breast Cancer – Other Developed Countries Year penetration starts Starting penetration rate Years between penetration start and peak Peak penetration Duration of peak penetration in years Retention rate in decline years Stage of development 2018 1% Incidence 9 15% Phase 2 GRIFFIN SECURITIES EQUITIES RESEARCH 38% Market growth rate Price per patient 4 90% 458,054 Percent addressable 2.5% $60,000 Treatment price growth 3% Royalty rate 30% Probability of commercialization 25% 12 Ziopharm Oncology October 16, 2013 Glioblastoma – More Developed Countries Year penetration starts Starting penetration rate Years between penetration start and peak Peak penetration Duration of peak penetration in years Retention rate in decline years Stage of development 2019 3% Incidence 8 20% Preclinical 70% Market growth rate Price per patient 5 90% 63,597 Percent addressable 1% $75,000 Treatment price growth 3% Royalty rate 30% Probability of commercialization 25% A Discussion of our Assumptions: Launch dates: We are looking for Ad-RTS-IL12 to launch first for melanoma in 2017, followed by breast cancer in 2018 and glioblastoma in 2019. Population estimates: The sizes of the melanoma and breast cancer patient populations reflect GLOBOCAN 2008 estimates, adjusted for population growth, while we have applied an incidence rate of 5.1 patients per 100,000 individuals to arrive at the glioblastoma population in more developed countries where the incidence rate is higher than in less developed regions.18 In addition, the percent of the population that is considered addressable reflects the proportion of patients who are diagnosed with advanced/metastatic disease in the cases of melanoma and breast cancer. For glioblastoma, we have assumed that 70% of the patients would be eligible to receive the gene therapy given the rapidity with which the disease normally progresses. Market penetration rates: We have assumed very low initial acceptance rates for melanoma and breast cancer, reflecting the novelty of the therapy, the availability of alternative treatment options, and the need to gain insurance coverage. Peak penetration rates were made after taking into consideration alternative therapies currently in existence and under development. Pricing: The prices of Ad-RTS-IL12 treatment for different cancers are unknown. Accordingly, we have calculated our estimates using the price of a full course of Herceptin ($70,000 in the United States in 2012) and adding a 20% premium to arrive at our U.S. price. Overseas prices vary, but to set a single value, we selected $60,000, or about 30% less than the domestic cost. The estimate for glioblastoma, $75,000, is a blended fee, based on a 60:40 split between U.S. and foreign patients. Royalty rate: This figure (30%), which is the amount that Ziopharm will receive based on a marketer’s sales, is consistent with historical licensing fees paid for innovative drugs. Probability of commercialization: Based on the completion of the Phase 1 clinical trial of Ad-RTS-IL12 for melanoma, we have set this probability at 25% after taking into consideration historical success rates for drugs at a similar stage of development. 18 Central Brain Tumor Registry of the United States, Fact Sheet. GRIFFIN SECURITIES EQUITIES RESEARCH 13 Ziopharm Oncology October 16, 2013 ANNUAL INCOME STATEMENTS҂ ҂ st (Fiscal year ends December 31 .) Data are in thousands, except for per-share figures. Estimates are in italics. Total Revenue Operating expenses R&D expense Licensing fee G&A expense Total operating costs Operating profit/(loss) Other income (expense) net Warrant valuation adj Pretax profit/(loss) Income taxes Net profit/(loss) Earnings/(loss) per share Shares outstanding 2012 2013 2014 2015 2016 2017 2018 $ 800 $ 800 $ 6,800 $ 13,300 $ 16,500 $ 52,357 $ 245,028 $ 83,446 ‐ 19,523 102,969 $ (102,169) (13) 6,050 $ (96,132) ‐ $ (96,132) $ 50,900 ‐ 15,500 66,400 $ (65,600) 11 10,385 $ (55,204) ‐ $ (55,204) 47,000 ‐ 14,000 61,000 $ (54,200) ‐ ‐ $ (54,200) ‐ $ (54,200) $ 45,000 ‐ 14,000 59,000 $ (45,700) ‐ ‐ $ (45,700) ‐ $ (45,700) $ 35,000 ‐ 14,000 49,000 $ (32,500) ‐ ‐ $ (32,500) ‐ $ (32,500) $ 36,000 ‐ 16,000 52,000 $ 357 ‐ ‐ $ 357 136 $ 221 $ 44,105 10,729 17,152 71,986 $ 173,042 ‐ ‐ $ 173,042 65,756 $ 107,286 $ (1.22) $ (0.66) $ (0.58) $ (0.47) $ (0.33) $ 0.00 $ 0.89 78,546 83,335 93,188 98000 100,000 120,000 120,250 Assumptions: We have assumed that Ziopharm receives a $50 million upfront licensing fees in the second half of 2014 for its Ad-RTS-IL12 therapy and legacy small molecule drugs. This amount is spread evenly over 48 months, which is an approximate time to commercial launch. R&D expenses should decline in the second half of 2013 since the ongoing clinical trials are nearly completed. In 2014, investments in new product development should ramp up as more clinical studies begin. Thereafter, we’ve allowed R&D expenditures to ease as some costs are borne by licensees. In 2018, we’ve assumed that R&D costs approximate 18% of revenues. General & administrative costs will likely be decline modestly in the near term and then hold fairly constant until the Company’s revenues permit an expansion of the infrastructure to accommodate more drug and business development activities. In 2018, the first full year in which we figure operations will be profitable, we have included a licensing fee due Intrexon for its contribution to Ziopharm’s drugs that are on the market. We have included provisions for tax liabilities at a 38% rate for financial reporting purposes, although the cash outlay will be limited by net operating loss carryforwards of $111.5 million and R&D tax credits of $20 million as of December 31, 2012. The number of shares outstanding reflects anticipated equity financings in 2014 and 2016, as well as allowances for stock-based compensation. Our per-share figures are based on basic shares outstanding in years in which the Company books a loss, and on fully diluted during periods of profitability. QUARTERLY INCOME STATEMENTS҂ ҂ st (Fiscal year ends December 31 .) Data are in thousands, except for per-share figures. Estimates are in italics. 2012 Research Contract Revenue Operating expenses R&D expense G&A expense Total operating costs Operating profit/(loss) Other income (expense) net Warrant valuation adj Pretax profit/(loss) Income taxes Net profit/(loss) 2013 2014 Q1 $ 200 Q2 $ 200 Q3 $ 200 Q4 $ 200 Q1 $ 200 Q2 $ 200 Q3 $ 200 Q4 $ 200 Q1 $ 200 Q2 $ 200 Q3 $ 3,200 Q4 $ 3,200 $ 13,985 4,848 18,833 $ (18,633) (26) (5,811) $ (24,470) ‐ $ (24,470) $ 18,264 4,902 23,166 $ (22,966) 3 (650) $ (23,613) ‐ $ (23,613) $ 16,215 5,712 21,927 $ (21,727) (42) 3,945 $ (17,824) ‐ $ (17,824) $ 34,982 4,061 39,043 $ (38,843) 52 8,566 $ (30,225) ‐ $ (30,225) $ 19,112 4,671 23,783 $ (23,583) (4) 10,788 $ (12,799) ‐ $ (12,799) $ 14,775 3,721 18,496 $ (18,296) 7 (403) $ (18,692) ‐ $ (18,692) $ 9,013 3,608 12,621 $ (12,421) 4 ‐ $ (12,417) ‐ $ (12,417) $ 8,000 3,500 11,500 $ (11,300) 4 ‐ $ (11,296) ‐ $ (11,296) $ 9,000 3,500 12,500 $ (12,300) ‐ ‐ $ (12,300) ‐ $ (12,300) $ 11,500 3,500 15,000 $ (14,800) ‐ ‐ $ (14,800) ‐ $ (14,800) $ 13,000 3,500 16,500 $ (13,300) ‐ ‐ $ (13,300) ‐ $ (13,300) $ 13,500 3,500 17,000 $ (13,800) ‐ ‐ $ (13,800) ‐ $ (13,800) Earnings/(loss) per share $ (0.32) $ (0.30) $ (0.23) $ (0.37) Shares outstanding 75,620 78,515 78,670 81,379 GRIFFIN SECURITIES EQUITIES RESEARCH $ (0.15) $ (0.22) $ (0.15) $ (0.13) 82,906 83,083 83,600 83,750 $ (0.13) $ (0.16) $ (0.14) $ (0.15) 92,500 93,000 93,500 93,750 14 Ziopharm Oncology BALANCE SHEET҂ ҂ October 16, 2013 st (Fiscal year ends December 31 .) Data are in thousands. ASSETS 6/30/2013 12/31/2012 Current Assets Cash & equivalents 38,932 Accounts Receivable Prepaid expenses & other Total Current Assets Property & equipment 73,306 31 58 4,067 6,912 $ 43,030 $ $ 1,713 $ Other 860 $ otal Assets 80,276 1,994 1,134 45,603 $ 83,404 1,165 $ 1,509 18,969 $ 16,516 20,997 $ 18,864 - $ LIABILITIES & STOCKHOLDERS' EQUITY Current Liabilities Accounts payable $ Accrued expenses Other 863 Total Current Liabilities Long-term debt $ $ Deferred revenue 839 2,333 Deferred rent $ Warrant liabilities 365 $ 2,576 Total Liabilities $ 2,733 400 12,962 26,271 $ 84 $ 34,959 Shareholders Equity Common Stock, par value $ Additional Paid-In Capital 334,463 Accumulated Deficit Total Shareholders Equity Total Liabilities & Equity 83 332,086 (315,215) (283,724) $ 19,332 $ 48,445 $ 45,603 $ 83,404 VALUATION ANALYSIS Our valuation analysis was conducted via a discounted future price method. We applied a price-earnings multiple of 40x to the Company’s projected earnings of $0.89 in 2018, resulting in a future price of $35.60. That figure was discounted back four years, to 2014, using an annual rate of 35%, which we believe adequately represents the risks inherent in the drug development program. The result was a share price of $10.72. Accordingly, we have raised our 12-month price target to $10.75. GRIFFIN SECURITIES EQUITIES RESEARCH 15 Ziopharm Oncology October 16, 2013 DISCLOSURES ANALYST(s) CERTIFICATION: The analyst(s) responsible for covering the securities in this report certify that the views expressed in this research report accurately reflect their personal views about Ziopharm, Inc. (the “Company”) and its securities. The analyst(s) responsible for covering the securities in this report certify that no part of their compensation was, is, or will be directly or indirectly related to the specific recommendation or view contained in this research report. RATINGS: Griffin Securities, Inc. currently has BUY ratings on shares of Intrexon Corp. (NYSE: XON) and ZIOPHARM Oncology, Inc. (NasdaqCM: ZIOP). Griffin Securities, Inc. has no investment ratings on any of the other companies mentioned in this report. MEANINGS OF RATINGS: Our rating system is based upon 12 to 36 month price targets. BUY describes stocks that we expect to appreciate by more than 20%. HOLD/NEUTRAL describes stocks that we expect to change plus or minus 20%. SELL describes stocks that we expect to decline by more than 20%. SC describes stocks that Griffin Securities has Suspended Coverage of this Company and price target, if any, for this stock, because it does not currently have a sufficient basis for determining a rating or target and/or Griffin Securities is redirecting its research resources. The previous investment rating and price target, if any, are no longer in effect for this stock and should not be relied upon. NR describes stocks that are Not Rated, indicating that Griffin Securities does not cover or rate this Company. DISTRIBUTION OF RATINGS: Currently Griffin Securities has assigned BUY ratings on 82% of companies it covers, HOLD/NEUTRAL ratings on 18%, and SELL ratings on 0%. Griffin Securities has provided investment banking services for 12% of companies in which it has had BUY ratings in the past 12 months and 0% for companies in which it has had HOLD/NEUTRAL, NR, or no coverage in the past 12 months or has suspended coverage (SC) in the past 12 months. COMPENSATION OR SECURITIES OWNERSHIP: The analyst(s) responsible for covering the securities in this report receive compensation based upon, among other factors, the overall profitability of Griffin Securities, including profits derived from investment banking revenue. The analyst(s) that prepared the research report did not receive any compensation from the Company or any other companies mentioned in this report in connection with the preparation of this report. The analyst responsible for covering the securities in this report currently does not own common stock in the Company, but in the future may from time to time engage in transactions with respect to the Company or other companies mentioned in the report. Griffin Securities from time to time in the future may request expenses to be paid for copying, printing, mailing and distribution of the report by the Company and other companies mentioned in this report. Griffin Securities expects to receive, or intends to seek, compensation for investment banking and noninvestment banking services from the Company in the next three months. Griffin Securities has managed or co-managed a public offering for Intrexon Corp. in the past 12 months. Griffin Securities has received compensation from Intrexon Corp. in the past 12 months for investment banking services and non-investment banking services. FORWARD-LOOKING STATEMENTS: This Report contains forward-looking statements, which involve risks and uncertainties. Actual results may differ significantly from such forward-looking statements. Factors that might cause such a difference include, but are not limited to, those discussed in the “Risk Factors” section in the SEC filings available in electronic format through SEC Edgar filings at www.SEC.gov on the Internet. GENERAL: Griffin Securities, Inc. (“Griffin Securities”) a FINRA (formerly known as the NASD) member firm with its principal office in New York, New York, USA is an investment banking firm providing corporate finance, merger and acquisitions, brokerage, and investment opportunities for institutional, corporate, and private clients. The analyst(s) are employed by Griffin Securities. Our research professionals provide important input into our investment banking and other business selection processes. Our salespeople, traders, and other professionals may provide oral or written market commentary or trading strategies to our clients that reflect opinions that are contrary to the opinions expressed herein, and our proprietary trading and investing businesses may make investment decisions that are inconsistent with the recommendations expressed herein. Griffin Securities may from time to time perform corporate finance or other services for some companies described herein and may occasionally possess material, nonpublic information regarding such companies. This information is not used in preparation of the opinions and estimates herein. While the information contained in this report and the opinions contained herein are based on sources believed to be reliable, Griffin Securities has not independently verified the facts, assumptions and estimates contained in this report. Accordingly, no representation or warranty, express or implied, is made as to, and no reliance should be placed on, the fairness, accuracy, completeness or correctness of the information and opinions contained in this report. GRIFFIN SECURITIES EQUITIES RESEARCH 16 Ziopharm Oncology October 16, 2013 The information contained herein is not a complete analysis of every material fact in respect to any company, industry or security. This material should not be construed as an offer to sell or the solicitation of an offer to buy any security in any jurisdiction where such an offer or solicitation would be illegal. We are not soliciting any action based on this material. It is for the general information of clients of Griffin Securities. It does not take into account the particular investment objectives, financial situations, or needs of individual clients. Before acting on any advice or recommendation in this material, clients should consider whether it is suitable for their particular circumstances and, if necessary, seek professional advice. Certain transactions - including those involving futures, options, and other derivatives as well as non-investment-grade securities - give rise to substantial risk and are not suitable for all investors. The material is based on information that we consider reliable, but we do not represent that it is accurate or complete, and it should not be relied on as such. The information contained in this report is subject to change without notice and Griffin Securities assumes no responsibility to update the report. In addition, regulatory, compliance, or other reasons may prevent us from providing updates. ZIOP PRICE CHART – 2 Year BUY BUY BUY Source: BigCharts.com 6/26/2006 – Initiating Coverage: share price: $5.05; rating: BUY; 12-month price target: $18.00. Updating coverage: 12/07/2006: share price $6.36; rating: BUY; 12-month price target: $20; 5/03/2007: share price $5.80; rating: BUY; 12-month price target: $20.00; 3/13/2008: share price: $2.52; rating: BUY; 12-month price target: $15.00; 7/02/2008: share price: $1.87; rating: BUY; 12-month price target: $15.00; 5/18/2009: share price: $0.77; rating: BUY; 12-month price target: $3.00; 6/09/2009: share price: $1.87; rating: BUY; 12-month price target: $3.00; 3/4/2010: share price: $3.53; rating: BUY; 12-month price target: $8.00; 1/20/2011: share price: $5.60; rating: BUY; 12-month price target: $11.00; 4/25/2011: share price: $6.36; rating: BUY; 12-month price target: $11.00; 5/18/2011: share price: $6.85; rating: BUY; 12-month price target: $11.00; 9/21/2011: share price: $4.57; rating: BUY; 12-month price target: $11.00; 3/30/2012: share price: $5.40; rating: BUY; 12-month price target: $12.00; 12/12/2012: share price: $4.44; rating: BUY; 12-month price target: $12.00; 10/16/2013: share price, $4.09; rating, BUY; 12-month price target, $10.75. XON 3-Month Price Chart BUY BUY Source: BigCharts.com 9/30/13 – Initiating Coverage: share price, $23.01; rating, BUY; 12-month price target, $36.00; 10/4/2013 Update: share price, $25.10; rating, BUY, 12-month price target, $36.00. GRIFFIN SECURITIES EQUITIES RESEARCH 17