Ultrasound diagnosis and management of fetal intestinal obstruction
advertisement

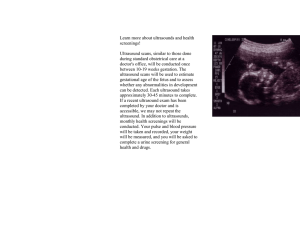
Samuel et al., Diagnosis of intestinal obstruction by ultrasound 333 Short communications J.Perinat.Med. 12(1984) 333 Ultrasound diagnosis and management of fetal intestinal obstruction and volvulus in utero N. Samuel, D. Dicker, D. Feldberg, J. A. Goldman Department of Obstetrics-Gynecology, Golda Meir Medical Center, Petah-Tikva, and Tel-Aviv University Medical School, Israel 1 Introduction Curriculum vitae For many centuries no means were available to evaluate the human fetus in utero. While amniocentesis, amniography and fetoscopy are all invasive techniques, fetal anatomy as well as major congenital malformations currently can be accurately determined at an early stage with the aid of non-invasive ultrasonography [8]. Modern ultrasonographic examination of the fetus allows in utero evaluation of congenital anomalies. Recently a group of fetal malformations has been added, namely those amenable to correctable surgery after birth. We present a case of severe intestinal obstruction in utero diagnosed by ultrasonography and corrected by surgery immediately following premature planned delivery by Ceasarean section. NURITH SAMUEL was born in 1952, and was graiuated from Tel-Aviv University Medical School in 1978. Subsequently she has been in training in the Department of Obstetrics and Gynecology at the Golda Meir Medical Center (Chief: Prof. J. Goldman), Petah-Tikva, Israel. She is at the present Senior Resident with a special interest in ultrasound. stomach, kidneys and bladder appeared normal. The mass remained static over the next week, yet a significant dilatation of the small bowel loops was obvious (Figs. 3, 4), and peristalsis was markedly increased. One dilated loop of bowel was observed 2 Case report to enter the mass (Fig. 5). H. S., a 31 years old woman was seen in the ultra- The biophysical score of the fetus was normal. sound clinic of the Golda Meir Medical center in Amniocentesis revealed fetal lung immaturity as the 33rd week of her second pregnancy because tested by lung profile. Bile acids and alpha-fetoof suspected polyhydramnios. The first pregnancy proteins were within normal range [3, 14]. In view and delivery were normal. In the 18th week of her of the fetal abdominal mass which most probably present gestation the ultrasound scan was perfectly represented meconium originating in the small normal. Sonography at this time revealed mild poly- bowel and the presence of acute progressing hydramnios and an abdominal mass of 5 χ 7 cms. intestinal dilatation, five days later, with proven located under the fetal liver (Fig. 1). Slightly fetal lung maturity, a Caesarean section was perdilated intestinal loops were observed (Fig. 2). The formed in order to prevent spontaneous perfora© by Walter de Gruyter & Co. Berlin · New York 334 Samuel et al., Diagnosis of intestinal obstruction by ultrasound Fig. 1. Ultrasound scan: intraabdominal mass in the fetus Fig. 3. Progressively enlarged intestinal loops after 48 (M: mass; K: kidney; P: placenta; A: amniotic fluid) "hours. Fig. 2. Slightly enlarged loops of small bowel: 33rd week of pregnancy (L: intestinal loops). Fig. 4. Same after 72 hours J.Perinat. Med. 12 (1984) Samuel et al., Diagnosis of intestinal obstruction by ultrasound 335 3 Comment The improving technique and range of diagnostic ultrasonography and ultrasound equipment has made it possible to detect fetal congenital anomalies early in pregnancy; however, even more important is the early detection of potentially, surgically correctable malformations of the fetus. Indeed, several reports of sporadic cases have been published recently [1, 2 , 4 , 6 , 7 , 9 , 10, 11, 12, 13, 15, 16, 17,18]. The case described here is one involving an anomaly of the termina ileum. Only few cases of this localization have been described. In fact, JASSANI etal. [10] published the largest series of gastrointestinal tract anomalies of the fetus recognized prenatally; of nine, one was a case of small bowel obstruction due to jejuno-ileal atresia and volvulus, with perforation of the distal ileum. Fig. S. Enlarged intestinal loops penetrating into mass (arrow). tion or irreversible ischemia of a wide portion of small bowel. The abdomen of the newborn was found to be distended, and a hard mass was palpated in the right upper abdomen. Barium enema performed immediately after delivery revealed a rather narrow large bowel leading to a "dead-end" a few centimeters beyond the ileocecal valve. Markedly dilated intestinal loops were seen with a minute amount of contrast material under the diaphragm which represented a picture which could correspond to microperforation of the bowel. .Laparotomy of the baby was performed one hour after delivery. The operative findings included mild peritonitis with atresia of the terminal ileum, and above the atresia, there was a mass of convoluted intestinal loops resulting in volvulus. One of the loops was adherent to the abdominal wall, and was filled with thick meconium. This loop was obviously the mass seen on ultrasonographic scan. The volvulus was resected, and ileostomy and colostomy were done. The baby recovered rapidly; repair of the colostomy and ileostomy was performed 2 months after surgery. The baby is at present in good general condition. J. Perinat. Med. 12(1984) Elective Caesarean section rather than a trial at vaginal delivery was indicated in our case since immediate surgical correction was considered necessary. Moreover, this mode of delivery was considered less traumatic for a premature, handicapped neonate, and cervical and uterine conditions for spontaneous delivery were unfavourable. Furthermore, the compromised small bowel was obviously fluid-filled and progressively dilating to an extent that intestinal ischemic necrosis and meconium ileus was threatening to lead to gangrene, intestinal perforation and meconium peritonitis. In fact, we believe that it has not hitherto been mentioned and should be emphasized that although prenatal obstruction may well be a gradual .process, progress to complete obstruction has a rather dynamic course. Consequently, regular ultrasound scans may detect the true course of the process, and improve the prognosis of the fetus. It is interesting to note that the biophysical score, (fetal movements, breathing, tonus, non-stress test, etc*) during the observation period, and up to the delivery by Caesarean section, was entirely normal. In view of the fact that the number of treatable congenital defects in the fetus is steadily growing, the ethical issues of the fetus as a patient must certainly be given consideration [5J. Samuel et al., Diagnosis of intestinal obstruction by ultrasound 336 4 Conclusions The prenatal detection of such birth defects permits planning for the optimal time, site and mode r u The number and types of cases is growing m whom ' ofde jj v prenatal diagnosis of correctable fetal anomalies ^' are made by ultrasonography. Summary A case has been described in which the diagnosis of acute intestinal obstruction of the fetal small bowel was made antenatally with the aid of ultrasonography. Ceasarean section was done in the 34th week of pregnancy. One hour after birth ileostomy and colostomy were performed Keywords: after resection of a volvulus in the terminal ileum. Two months later the ileostomy and colostomy were closed, and the baby is doing well. The importance of precise diagnosis of the anomaly in utero is emphasized to avoid unjustified termination of pregnancy. Antenatal volvulus in fetus, antenatal ultrasound, correctable fetal anomaly. Zusammenfassung Ultraschalldiagnose und Vorgehen bei einem Darmverschluß und Volvulus in utero Wir haben einen Fall beschrieben, in dem antenatal mit Hilfe des Ultraschalls ein aktuer Dünndarmverschluß diagnostiziert wurde. In der 34. Schwangerschaftswoche erfolgte die Sectio; eine Stunde post partum wurden nach Resektion eines Volvulus im terminalen Ileum eine Ileo- stomie und eine Kolostomie angelegt. Nach zwei Monaten wurde das Kolostoma verschlossen; das Kind gedeiht gut. Wir möchten nachdrücklich auf die Bedeutung einer präzisen Diagnose fetaler Anomalien in utero hinweisen. So können nämlich ungerechtfertigte Schwangerschaftsabbrüche vermieden werden. Schlüsselwörter: Antenataler Volvulus beim Feten, antenataler Ultraschall, korrigierbare fetale Anomalien. Resume Diagnostic echographique et conduite a tenir devant une occlusion intestinale par volvulus in utero Les auteurs decrivent une observation au cours de laquelle le diagnostic chez le foetus d'occlusion intestinale aique du grele a ete porte pendant la grossesse a l'aide de l'echographie. Une cesarienne a ete effectuee a la 34e semaine Mots-cles: de gestation; apres resection de la zone volvulee sur l'ileon terminal, une heure apres la naissance, on a realise une ileostomie et une colostomie. Deux mois plus tard la colostomie a ete fermee et le bebe se porte bien. L'importance du diagnostic precis de l'anomalie in utero est soulignee afin d'eviter une interruption injustifiee de la grossesse. Anomalie foetale curable, echographie ant6natale, volvulus antenatal chez le foetus. Acknowlegments: Thanks are due to Dr. ABRAMOWITZ and Dr. R. KATZ for their assistance in the interpretation of ultrasound scans. Bibliography [1] ANDRASSY, R. J., G. H. MAHOUR: Gastrointestinal anomalies associated with oesophageal atresia or tracheoesophageal fistula. Arch. Surg. 114 (1979) 1125 [2] BEAN, W. J., M. A. CALONJE, C. N. APRILL et al.: Anal atresia; a prenatal ultrasound diagnosis. J.Clin. Ultrasound 6 (1978) 111 [3] DELEZE, G., D. SIDIROPOULOS, G. BAUMGARTNER: Determination of bile acid concentration in human amniotic fluid for prenatal diagnosis of intestinal obstruction. Pediatrics 59 (1977) 647 [4] DUENHOELTER, J. H., R. SANTOS-RAMOS, C. R. ROSEN FELD et al.: Prenatal diagnosis of gastrointestinal tract obstruction. Obstet. Gynecol. 47 (1976)618 [5] FLETCHER, J. C.: Editorial; the fetus as patient. JAMA 246 (1981) 772 [6] GEE,H.,U.ABDULLA: Antenatal ultrasonic demonstration of fetal bowel. Radiology 124 (1977) 471 [7] HARRISON, M. R., M. S. GOLBUS, R. A. FILLY; Management of the fetus with a correctable congenital defect. JAMA 246 (1981) 774 J. Perinat. Med. 12 (1984) 337 Samuel et al., Diagnosis of intestinal obstruction by ultrasound [8] BOBBINS, J. C., P. GRANNUM, R. L. BERKOWITZ etal.: Ultrasound in the diagnosis of congenital anomalies. Am. J. Obstet. Gynecol. 134 (1979) 331 [9] HOULTON, M. C., M. SUTTON, J. AITKEN: Antenatal diagnosis of duodenal atresia. J. Obstet. Gynecol. 81 (1974) 818 [10] JASSANI, M. N., M. W. L. GAUDERER, A. A. FAN AROFF et al.: A perinatal approach to the diagnosis and management of gastrointestinal malformations. Obstet. Gynecol. 59 (1980) 33 [11] LEES, R. F., B. A. ALFORD, H.NORMAN etal.: Sonographic appearance of duodenal atresia in utero. Am. J. Roentgenol. 131 (1978) 701 [12] LOVEDAY, B. J., J. A.BARR, J. AILKEN: The intrauterine demonstration of duodenal atresia by ultrasound. Br. J. Radiol. 48 (1975) 1031 [13] QUEEN AN, J. T., E. C. GADOW: Amniography for detection of congenital malformations. Obstet. Gynecol. 35 (1970) 648 [14] SEPPALA, M.: Increased alpha fetoprotein in amniotic fluid associated with congenital atresia of the fetus. Obstet. Gynecol. 42 (1973) 613 J. Perinat. Med. 12(1984) [15] TOULOUKIAN, R. J.: Clinics in Perinatology: Intestinal atresia. Philad. Saunders. Vol. 5 (1978) 3 [16] WROBLESKI,D., C.WESSELHAFT: Ultrasonic diagnosis of prenatal intestinal obstruction. J. Ped. Surg. 14 (1979) 598 [17] ZIMMERMAN, H. B.: Prenatal demonstration of gastric and duodenal obstruction by ultrasound. J. Can. Assoc. Radiol. 29 (1978) 138 [18] BAXI, L. V., MING-NENG YEH, W. A. BLANC et al.: Antepartum diagnosis and management of in utero intestinal volvulus with perforation. N. Engl. J. Med. 308 (1983) 1519 Received December 1, 1983. Revised April 12,1984. Accepted April 24, 1984. Nurith Samuel, M.D. Tel-Aviv University Medical School Dept. Obstetrics-Gynecology Golda Meir Medical Center Petah-Tikva, Israel ·f edited by D. Voth and P. Glees 17 χ 24 cm. XII, 515 pages. With 207 illustrations and 81 tables. 1984. Clothbound DM 148,- ISBN 3110100290 Clinicians treating vasospasm and cerebral haemorrhage and experts in the field of cerebral blood flow have contributed to the present volume. This comprehensive survey deals with the anatomy of cerebral vessels and the physiology and pharmacology of smooth vascular muscle. The application of advances in these fields to the pathophysiology of cerebral blood flow and the severe consequences of cerebral arterial spasm are discussed at length. The diagnostic and clinical aspects of angiospasm and the timing of operating a ruptured aneurysm are treated in depth based on data from a large number of cases. Special attention is paid to the problem of pharmacotherapy which makes possible for the first time an effective therapeutical intervention through the application of the so-called calcium antagonists. W DE G