Full Guidance on Using QOF to Improve Palliative / End of Life Care
advertisement

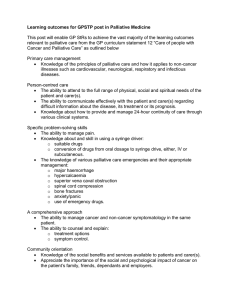
V25 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care Guidelines for practices on the revised Quality Outcome Framework (QOF) points for Palliative Care and the Gold Standard Framework (GSF) This Guidance may be of particular use to practice managers, enabling their practices to institute changes to claim QOF points in the GMS contract for April 06. Drs Amanda Free, Keri Thomas, Wendy-Jane Walton and Teresa Griffin of The Gold Standards Framework National Central Team Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 1 of 26 Contents 1 Page Introduction 3 Why bother? - the three trajectories of illnesses, summary of new QOF palliative care points and predicted numbers 2 Getting going - the new recommendations for palliative care in QOF: a) setting up the supportive / palliative care register b) holding the MDT Meetings 6 3 Further steps 8 3.1 3.2 3.3 3.4 GSF 7 C’s and levels of adoption Read Codes Out of hours palliative care and handover forms Assessment tools Appendix 1 IDENTIFY 8 9 9 9 10 Prognostic Indicators for patients in the last 6-12 months of life 15 Appendix 2 ASSESS a b c SCR 1 SCR 2 MDT 16 18 Appendix 3 Significant Event Analysis 19 Appendix 4 Palliative Care Read Codes – GSF Template 20 Appendix 5 Levels of Adoption of GSF 21 Appendix 6 Suggested QOF Assessment for Palliative Care Points 22 Glossary of terms in PIG 23 “The college is pleased to support the Gold Standards Framework, which is having a huge impact on the quality of care at the end of patients' lives. The values expressed in this framework are central to the College ethos of Knowledge with Compassion.” Dr Graham Archard Vice Chairman Royal College of General Practitioners, March '05 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 2 of 26 1 Introduction – Why bother? The challenge:Each GP will have about 20 patient deaths/year. About 1% of the population will die each year - e.g. with a list size of 10,000 patients, an average practice will have about 100 patient deaths/ year Most of our patients now die from cancer (about a quarter) organ failure - heart failure, COPD etc (about a third) or frailty/dementia/multiple co-morbidities (about a third) With the predicted demographic changes over the coming years, more people are living longer with serious illness, and more will die from non cancer illnesses, often related to their long term conditions. How can we predict which will be the patients in the last year of life? How can we ensure that these patients are given the best care in this their final stage of life? – in particular the final year of life? Improving care for patients nearing the end of their lives is one of the most important and highly valued aspects of our work in general practice. Yet until now, we have often failed to target care towards this group of patients, mainly because of difficulty in identifying them and responding to their needs. Using the Gold Standards Framework in Community Palliative Care, already used by about a third of the practices in England, Scotland and Northern Ireland, many have found that they can provide better quality and more focused care for these patients. They also feel that the service provided feels better organised and managed. The result is a greater consistency in the standard of care, with fewer patients ‘slipping through the net’ and more reliable community care provided by the Primary Health Care Team. As from April 06, there are now some QOF points specifically targeted for palliative care patients - 3 points for having a register for all patients predicted to be in the last 6- 12 months of life with any diagnosis, and 3 points for holding a multidisciplinary meeting at least 3 monthly (plus other general points included in end of life care – see later e.g. dementia) For GSF Practices For those already using the GSF in their practice, this is an opportunity to be rewarded for some of the work you are already doing. But as the register is for ALL patients in the last 6-12 months of life, it is an opportunity to maybe extend your registers to move beyond cancer patients to include more non cancer patients also. We know that far fewer non-cancer patients are currently receiving supportive care than may be eligible to do so, (just compare the lung cancer patient with the COPD patient with the same prognosis) - some guidance for this is given in the following pages and in the separate prognostic indicators paper. For those practices that are not using GSF currently, this may be an opportunity to focus on this important group of patients, to identify and collate their information using a register and to discuss their management plans as a team. This is the first step in improving palliative care organisation within your practice team. You might like then to develop this care further with the suggestions made in other key task areas of GSF. Although you may well be doing much of it in an ad hoc way already, by pulling it together into a practice framework or protocol, with an agreed plan of care for people in the last year of life, you are likely to find, as others have, that care can in fact become easier, more fulfilling and lead to more people dying a good death, in the place and in the manner of their choosing. So by undertaking and claiming these QOF points, this may be the first step to focusing more on your patients nearing the end of life. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 3 of 26 Fig 1: The three main illness trajectories and deaths / GP / year and end stage illness (Assuming GP list size of 2000 patients) After Lynn et al in WHO Guidance Palliative Care The Solid Facts Ed Higginson High Illness Trajectories GP's workload - 20 deaths / GP / yr “Cancer” Trajectory, Diagnosis to Death Cancer Function 1 Possible hospice enrolment Death Low Sud d en D eat h Onset of incurable cancer High Organ System Failure Trajectory Function Cancer Time ~ Often a few years, but decline usually seems < 2 months (mostly heart and lung failure) 2 Frailty / Dem entia Death Low Begin to use hospital often, self-care becomes difficult Time ~ 2-5 years, but death usually seems “sudden” High Organ Failure Function Frailty / Dementia Trajectory Death 3 Low Onset could be deficits in ADL, speech, ambulation Time ~ quite variable up to 6-8 years Fig 1 The three main illness trajectories and deaths/GP/year and three trajectories of end stage illness Every GP will average about 20 deaths/ 2000 patients/ year. These will be from broadly three groups of patients (See Fig 1). Rapid Decline 1) Cancer patients – about 5 deaths/GP/year, with a roughly predictable disease trajectory of slow decline, varying in timescale with each cancer group, then steady deterioration. This picture epitomizes the standard patient in need of palliative care, and the predicted hospice/ specialist palliative care input at certain stages - most palliative care services are currently directed mainly to cancer patients with this trajectory of illness. 2) The Organ Failure patients – about 6 patient deaths/GP/Year. This represents an increasing number of patients dying not of cancer but of predominantly single organ failure, such as heart, lung, nerve, kidney, liver or other organ failure. Their picture is much more of steady decline over years with intermittent exacerbations, often requiring hospitalisation, with often an unclear terminal phase leading to death. There is difficulty predicting which exacerbation will be their last, so in the end, death may come as a shock, with little preparation beforehand by the patient, family and staff. These patients often miss out on the benefits given to many cancer patients. However, by estimating which patients fall into this rough category of being in the final year of life using the predictive indicators suggested, and by raising awareness of their needs, more can be done to enable good palliative symptom control, service provision, carer support and respite and life closure discussions for these patients. Also some hospital admissions might be averted, especially in the terminal stages, and more patients would be enabled to live out the end of their lives where they would choose to. As their picture is that of a slower decline, supportive care for example using GSF at an early stage is important to enable them to live well until they die. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 4 of 26 Gradual Decline 3) Frailty / dementia patients – with multiple co-morbidities and organ failures. About 7-8 patient deaths/GP/Year. This group of patients consists mainly of elderly patients with multiple organ failures, with cumulative co-morbidities and frailty. With increasing age also, the prevalence of dementia increases, and this contributes to or can dominate their overall condition. This number is increasing and is likely to be the predominant group over the next few years. Their needs are different from those of the traditional cancer patient, with more long term community support needed, better support for carers; and more are within institutionalised care. However, their end of life stories may be equally needy though less well voiced, and greater support is needed. As many frail elderly live in care homes, where one in five deaths occur , and there are particular issues sometimes with primary palliative care provision in care homes, particular attention is required for those living in care homes (see GSF in care homes programme on GSF website). Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 5 of 26 2 Getting going - New recommendations for palliative care in QOF In summary in the new GP contract’s Quality and Outcome Framework (QOF) from April 06:- New points specifically now available relating to palliative care for all patients 3 points for assembling a palliative/supportive care register for all patients estimated to be in the last 6-12 months of life, with cancer and non- cancer illnesses. 3 points for holding regular (at least 3 monthly) multi-disciplinary case review meetings where all patients on the palliative care register are discussed. The aim of these meetings is to – ensure that each patient has a management plan as defined by the practice team and are acted upon by the most appropriate member of the team. – Ensure that the management plan includes preferences for place of care. – Ensure that the support needs of carers are discussed and addressed wherever reasonably possible. Total 6 points Current and related points available for cancer and other long term conditions relevant to palliative care 5 points for producing a register of all cancer patients excluding non-melanotic skin cancers. 6 points for recording a cancer care review within 6 months of diagnosis on patients diagnosed with cancer within the last 18 months. 5 points for producing a register of patients with dementia. 15 points for reviewing the care of patients diagnosed with dementia in the previous 15 months. 6 points for undertaking a minimum of 3 significant event reviews in the past year. 4 points for having undertaken a minimum of 12 significant event reviews in the last 3 years which include (amongst other things) new cancer diagnoses and deaths where terminal care has taken place at home. 2 points for having a system to alert the out of hours service to patients dying at home. 3 points for having a protocol for the identification of carers and a mechanism for the referral of carers for a social services assessment. Total 52 points Total number of points in the QOF 2 available for those using GSF in their practice Further information and guidance on QOF is available at www.nhsemployers.org Palliative care Points a) Setting up the Palliative/ Supportive care register b) Holding the MDT meetings level 1/C1 of GSF Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 6 of 26 a) A total of three points will be awarded for setting up and maintaining a palliative care register. All patients in the last 6-12 months of life should be included on this register. For those already using GSF this register is already in place in the form of the supportive care register (SCR), but to claim the points the patients must be entered on the computer with one of the recommended Read codes. As the points awarded are not many it is important to maximise the prevalence figures to maximise income generated. It is intended that the palliative care register, in order to provide equity for all our patients, should include all patients with palliative care needs, not just our cancer patients. If we look at an average GP list of 2000 patients, there will be an average of 20 deaths per year. Between one and three of these will be sudden deaths. It can therefore be argued that it should have been possible to identify the other 17 to 19 patients as having end stage illness, and therefore they should all have been on the palliative care register. Within the new guide and in the non cancer section of the GSF website, there are papers on the prognostic indicators and ideas on how to identify these patients, but it has to be accepted that this can never be entirely accurate In summary, to identify these patients we can use any of the following methods: 1. The surprise question, “Would you be surprised if this patient were to die in the next 6-12 months”. 2. The patient prefers comfort care only rather than increasingly misnamed ‘curative’ treatment. 3. Clinical indicators (see Prognostic Indicators in Guide and on website) We are hoping to develop further this guidance, which includes clinical indicators, validated and agreed by some of the UK specialist bodies, to make it easier for PHCT’s to identify those patients in the last 612 months of life. Currently though we are using indicators validated by some UK Specialist bodies with some other guidance taken from the USA. b) Three points will be awarded for discussing those patients on the register at three monthly (at least) MDT meetings. As before, GSF practices will already be doing this, and will probably be meeting monthly. Practices not using GSF will first need to identify those it would be useful to meet with - a core group would be GP’s, District nurse, Community specialist palliative care nurse, Practice nurses and administrative staff in many teams, Social services It is then useful to appoint a coordinator to organise the meetings and keep the project “on track”, and a lead GP. At the meeting the Register’s first summary sheet, SCR1 (see templates on website) acts as a good template upon which to base discussion about the patients, ensuring for example that their wishes re place of care have been shared, management plans have been agreed, and that someone in the team has sent information to the out of hours service. It also provides a written summary for audit and a written record that the meetings have taken place. Once the non-cancer patients are included on the register the number of different professionals involved will increase. For example, the respiratory nurse and the heart failure nurse should now be consulted and included in the meetings. This will become logistically more complicated and teams will have to find local solutions dependant upon such things as list size and geography. We envisage that some teams will choose to split the register into cancer and non-cancer and could, for example, discuss the non-cancer patients 3 monthly and the cancer patients at the meetings on the other 2 months. This may make better use of the specialist teams’ time. Examples of ways of holding MDT meetings are in the Guide below. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 7 of 26 3 Further steps 3.1 GSF 7 C’s and levels of adoption Once teams have the register and meetings in place we hope that they will want to take it further, to further improve the care that they offer to their dying patients. In the Gold Standards Framework programme there are seven key tasks, also known as the Seven C’s. C1 – Communication set up the register and meet regularly as a team. ensure that the patients have the information they need e.g. in home packs ensure that the patient’s wishes are taken into account e.g. re place of care C2 – Co-ordination appoint a co-ordinator and a lead GP and DN. C3 – Control of symptoms pool knowledge and expertise to address physical, psychological, social and spiritual needs use symptom assessment tools C4 – Continuity of care inform the out of hours service about the patients work together with the secondary care teams C5 – Continued learning use audit (e.g. place of death) and significant event or after death analysis identify and address knowledge gaps develop practice protocols C6 – Carer support identify and address their emotional, practical and financial needs extend care into the bereavement phase C7 – Care in the dying phase use a protocol for the last 48hrs of life such as the Liverpool Care Pathway, for more information www.endoflifecare.nhs.uk ensure that drugs are prescribed in anticipation of need After completing C1 (register and meetings) teams will find that it is very easy and very natural to progress through the other C’s, but it can be done at their own pace. For help and advice, e.g. on After Death Analysis, teams should register with the central GSF team and contact their local facilitator (details from SHA End of Life Care lead). Other information is available on the GSF web site. In order to track progress locally and nationally we have divided the Framework into 4 levels, roughly equating to the 7 C’s, so that we can measure not only how many teams have adopted GSF, but how deeply it is being adopted and used, in order to improve the care that we deliver to our patients in their last year of life. See appendix 5 for more details. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 8 of 26 3.2 Read Codes In order to qualify for the QOF points it is important to use the qualifying diagnostic codes for Palliative Care: ZV57C 8H7g. 8BAP. 8BAT. 8H6A. 8CM1. 8HH7. 8BJ1. 8BA2. 8H7L. 8BAS. 9EB5. 1Z01. (V)Palliative care Referral to Palliative care service Specialist palliative care Specialist palliative care treatment – outpatient Refer to terminal care consult On gold standards palliative care framework Referred to community specialist palliative care team Palliative treatment Terminal care Refer for terminal care Specialist palliative care treatment – daycare DS1500 Disability living allowance completed Terminal illness – late stage Other useful Read codes for palliative care are in appendix 4, including for example Read codes for preferences on place of death. 3.3 Out of hours palliative care and handover forms Few GP’s now work weekends or nights, so it is important that we work together with the out of hours service to provide as much continuity of care for our patients as possible. All the good work done in hours can rapidly be undone out of hours if for example the patient is advised inappropriately to call an ambulance, resulting in a distressing A&E attendance and wait. We must inform the out of hours service of our patients condition, preferences and plans. Most out of hours services have developed their own forms to be faxed over to them, ensuring that these patients are treated as a priority and that their wishes are taken into account, and the PHCT needs to develop a system to ensure that these forms are used. Alternatively the SCR2, or Supportive Care Register Front Sheet can be used, see appendix 2. We must also ensure that drugs are left in the home in anticipation of need. This is particularly important for those patients choosing to die at home as they enter the terminal phase of their illness. A supply of diamorphine, glycopyrronium, midazolam and cyclizine, for example, may well save the carer driving miles to get the drugs, and again may save inappropriate hospital admissions, as well as meaning that symptoms can be treated promptly. 3.4 Assessment tools Better symptom control for patients must be one of our most important goals. We must address their physical, psychological, social and spiritual symptoms. But there is some evidence, for example, that doctors are only aware of a proportion of patients’ symptoms, and symptom assessment tools may help us with this. There are many choices of these tools, and their use should be agreed as a team. Some examples are included on the website. Tools can also help with audit, enabling us to build a case for improved local resourcing. But it is important that we remain patient focussed, addressing our patients’ priorities rather than simply pen-pushing. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 9 of 26 Appendix 1: Prognostic Indicators for patients who are “sick enough to die” and who are reasonably likely to be “in the last 6-12 months of life Although inherently a difficult area to predict we know that currently we are not recognising the actual likely prognostic trajectory for many patients, especially for non-cancer patients with advanced disease, and therefore we are under-estimating the number of people in need of palliative/ supportive care. These clinical prognostic indicators are an attempt to estimate when patients are in the last year or so of life. They have been drawn and referenced from a number of sources including from specialist centres in this country and abroad- they will be updated as more information is obtained. Although these are intrinsically only a very approximate guide to prognosis, these clinical indicators can therefore act as a rough guide to indicate to those in specialist secondary services and primary care that patients may be in need of palliative / supportive care and could be included on the register. In summary, to identify these patients we can use any of the following methods: 1. The surprise question, “Would you be surprised if this patient were to die in the next 6-12 months”. 2. The patient prefers comfort care only, not increasing misnamed ‘curative’ treatment. 3. Clinical indicators - general or disease specific (see Prognostic Indicators below) Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 10 of 26 Prognostic Indicator Guidance Revised Vs 5. Sept 08 “Earlier recognition of people nearing the end of their life leads to earlier planning and better care” Guidance to enable better identification of patients who may need supportive/palliative care About 1% of the population die each year, yet it is intrinsically difficult to predict or identify which patients may be in their last year of life. If predicted earlier, some supportive care measures could be introduced that would enable earlier discussion of their wishes, improve care aligned to their preferences and fewer crises. In short, if we could better identify these patients, we might be more able to provide better care for them as they approach the end of their lives. This guidance paper suggests which adult patients with any condition predicted to be in the final 6-12 months of life might be in need of supportive/palliative care. It was developed originally to support primary care teams using the Gold Standards Framework (GSF) and Quality Outcome Framework (QOF) to include more appropriate patients on their Palliative/Supportive Care Registers, and thereby to encourage better prediction of possible need and provision of care. The focus is more on improving prediction of need for support, rather than pure prognostication of time remaining. Though all prognostication is inherently inexact, and as people live longer with more co-morbid conditions, there can be disparity between levels of care provided to patients with different diagnoses. This guidance aims to help clinicians to support more patients nearing the end of life, whatever their underlying illness. It contributes to the development of accepted indicators for patients in the last months/year of life, which will aid identification of such patients and promote excellence in end of life care. Three triggers for Supportive/ Palliative Care are suggested - to identify these patients we can use any combination of the following methods: 1. The surprise question ‘Would you be surprised if this patient were to die in the next 6-12months’ an intuitive question integrating co-morbidity, social and other factors. If you would not be surprised, then what measures might be taken to improve their quality of life now and in preparation for the dying stage. The surprise question can be applied to years/months/weeks/days and trigger the appropriate actions at each stage ie “the right think to happen at the right time” 2. Choice/ Need - The patient with advanced disease makes a choice for comfort care only, not ‘curative’ treatment, or is in special need of supportive / palliative care eg refusing renal transplant 3. Clinical indicators - Specific indicators of advanced disease for each of the three main end of life patient groups - cancer, organ failure, elderly frail/ dementia (see over) High Rapid “Cancer” Trajectory, Diagnosis to Death Typical Case Histories GP's workload - Average 20 deaths/GP/yr (approximate proportions) 1-2 Function Cancer 1) Mrs A - A 54 year old woman with cancer of colon with liver secondaries and requiring a stent for jaundice who is feeling increasingly weak and tired. Likely rapid decline Death Low Sudden Death 5 Cancer High Function Frailty / Dem entia Onset of incurable cancer Time – Often a few years, but decline usually seems <2 months 2) Mr B - A 76 year old man with heart failure with increasing breathlessness on walking who finds it difficult to leave Organ System Failure Trajectory his home has had 2 hospital admissions in the last year and is worried about the prospect of any more emergencies and coping in the future (mostly heart and lung failure) Death Organ Failure 6 Begin to use hospital often, self-care becomes difficult Time ~ 2-5 years, but death usually seems “sudden” High Frailty / Dementia Trajectory Function 7-8 Low Death Low Onset could be deficits in ADL, speech, ambulation Time ~ quite variable up to 6-8 years 3) Mrs C - An 81 year old lady with COPD, heart failure, osteoarthritis and increasing forgetfulness, who lives alone. She fractured her hip after a fall, eats a poor diet and finds mobility difficult. She wishes to stay at home but is increasingly unable to cope alone and appears to be ‘skating on thin ice’. Likely slow decline, difficult to predict dying phase. Common picture in care homes The Department of Health’s new End of Life Care Strategy July 08 suggests development of a care pathway begins with the” identification of people approaching the end of life and initiating discussions about preferences for end of life care” (Exec.Summary 9 p.11). It also suggests use of this guidance to support such early identification “For many people suffering from a chronic illness a point is reached where it is clear that the person will die from their condition. Despite this, for many conditions it may be difficult, if not impossible and potentially unhelpful, to estimate prognosis accurately. The Prognostic Indicator Guidance developed as part of the Gold Standards Framework (GSF) provides useful prompts or triggers to a healthcare professional that discussions about the end of life should be initiated, if this has not already happened”. (3.22) Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 11 of 26 Trigger 3 – Specific clinical indicators of advanced disease These clinical prognostic indicators are an attempt to estimate when patients have advanced disease or are in the last year or so of life. These are only indicators and must be interpreted with clinical judgement for each individual patient, but they can help to alert clinicians to the need for extra supportive are. They have been drawn from a number of expert sources from the UK and abroad, and are updated regularly. Some use such indicators routinely, to assess patients’ need for palliative/supportive/hospice care. Although these are intrinsically only a very approximate guide to prognosis, these clinical indicators can therefore act as a rough guide to indicate to those in primary care and in secondary services that patients may be in need of palliative / supportive care. Primary care teams may include these patients on their Supportive/palliative care registers and hospital staff may suggest to GPs in discharge letters that such patients are included on the registers, if helpful. Co-morbidities or other General Predictors of End Stage illness1 / 2 Co-morbidity is increasingly the biggest predictive indicator of mortality and morbidity. Also▪ Weight loss - Greater than 10% weight loss over 6 months ▪ General physical decline ▪ Serum Albumin < 25 g/l ▪ Reducing performance status / ECOG/Karnofsky score (KPS) < 50%. Dependence in most activities of daily living(ADLs) 1. Cancer Patients Cancer3 Any patient whose cancer is metastatic or not amenable to treatment, with some exceptions – this may include some cancer patients from diagnosis e.g. lung cancer. ‘The single most important predictive factor in cancer is performance status and functional ability’ – if patients are spending more than 50% of their time in bed/lying down, prognosis is estimated to be about 3 months or less. More exact predictors for cancer patients are available elsewhere on the GSF website. 2. Organ Failure Patients 2.1 Heart Disease - CHF 4 At least two of the indicators below :▪ CHF NYHA stage III or IV – shortness of breath at rest or minimal exertion ▪ Patient thought to be in the last year of life by the care team - the ‘surprise’ question ▪ Repeated hospital admissions with symptoms of heart failure ▪ Difficult physical or psychological symptoms despite optimal tolerated therapy 2.2 Chronic Obstructive Pulmonary Disease – COPD 5 ▪ Disease assessed to be severe e.g. (FEV1 <30%predicted – with caveats about quality of testing) ▪ Recurrent hospital admission (>3 admissions in 12 months for COPD exacerbations) ▪ Fulfils Long Term Oxygen Therapy Criteria ▪ MRC grade 4/5 – shortness of breath after 100 meters on the level or confined to house through breathlessness ▪ Signs and symptoms of right heart failure ▪ Combination of other factors e.g. anorexia, previous ITU/NIV/resistant organism, depression ▪ >6 weeks of systemic steriods for COPD in the preceding 12 months 2.3 Renal Disease 6 ▪ Patients with stage 5 kidney disease who are not seeking or are discontinuing renal replacement therapy. This may be from choice or because they are too frail or have too many co-morbid conditions. ▪ Patients with stage 5 chronic kidney disease whose condition is deteriorating and for whom the one year ‘surprise question’ is applicable ie overall you would not be surprised if they were to die in the next year? ▪ Clinical indicators: ▪ CKD stage 5 (eGFR <15 ml/min) ▪ Symptomatic renal failure -Nausea and vomiting, anorexia, pruritus, reduced functional status, intractable fluid overload) ▪ Increasingly severe symptoms from comorbid conditions requiring more complex management or difficult to treat NB. many people with Stage 5 CKD have stable impaired renal function and do not progress or need RRT. 2.4 Neurological Disease - a) Motor Neurone Disease7 MND patients should be included from diagnosis, as it is a rapidly progressing condition Indicators of rapid deterioration include: ▪ Evidence of disturbed sleep related to respiratory muscle weakness in addition to signs of dyspnoea at rest ▪ Barely intelligible speech ▪ Difficulty swallowing ▪ Poor nutritional status ▪ Needing assistance with ADL’s ▪ Medical complications eg pneumonia, sepsis ▪ A short interval between onset of symptoms and diagnosis ▪ A low vital capacity (below 70% of predicted using standard spirometry) Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 12 of 26 b) Parkinson's Disease 8 The presence of 2 or more of the criteria in Parkinson disease should trigger inclusion on the Register ▪ Drug treatment is no longer as effective / an increasingly complex regime of drug treatments ▪ Reduced independence, need for help with daily living ▪ Recognition that the condition has become less controlled and less predictable with “off” periods ▪ Dyskinesias, mobility problems and falls ▪ Swallowing problems ▪ Psychiatric signs (depression, anxiety, hallucinations, psychosis) c) Multiple Sclerosis 9 Indications of deterioration and inclusion on register are:▪ Significant complex symptoms and medical complications ▪ Dysphagia (swallowing difficulties) is a key symptom, leading to recurrent aspiration pneumonias and recurrent admissions with sepsis and poor nutritional status ▪ Communication difficulties e.g. Dysarthria + fatigue ▪ Cognitive impairment notably the onset of dementia ▪ Breathlessness may be in the terminal phase 3. Patients with Frailty and Dementia Frailty 10 ▪ Multiple comorbidities with signs of impairments in day to day functioning ▪ Deteriorating functional score eg EPOC/ Karnofsky ▪ Combination of at least 3 symptoms of: weakness, slow walking speed, low physical activity, weight loss, reduced weight loss, self reported exhaustion Dementia11 ▪ Unable to walk without assistance, and ▪ Urinary and fecal incontinence, and ▪ No consistently meaningful verbal communication, and ▪ Unable to dress without assistance ▪ Barthel score < 3 ▪ Reduced ability to perform activities of daily living Plus any one of the following: 10% weight loss in previous six months without other causes, Pyelonephritis or UTI, Serum albumin 25 g/l, Severe pressure scores eg stage III / IV, Recurrent fevers, Reduced oral intake / weight loss, Aspiration pneumonia Stroke 12 ▪ Persistent vegetative or minimal conscious state / dense paralysis / incontinence ▪ Medical complications ▪ Lack of improvement within 3 months of onset ▪ Cognitive impairment / Post-stroke dementia Functional scores- 1) Karnofsky Performance Status Score The Karnofsky score, measures patient performance of activities of daily living. Score Function 100 Normal, no evidence of disease 50 Requires considerable assistance 90 Able to perform normal activity with only minor symptoms 40 Disabled, requires special assistance 80 Normal activity with effort, some symptoms 30 Severely disabled 70 Able to care for self but unable to do normal activities 20 Very sick, requires active supportive treatment 60 Requires occasional assistance, cares for most needs 10 Moribund 2) WHO/ ECOG Performance Status1 0 1 2 3 4 5 Fully active, able to carry on all pre-disease performance without restriction Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g. light housework, office work Ambulatory and capable of self care but unable to carry out work activities: upright more than 50% of waking hours Capable of only limited self care, confined to bed or chair more than 50% of waking hours Completely disabled, cannot carry on any self care, totally confined to bed or chair Dead Prognostication or Prediction of need. Prognostication is inherently difficult and inaccurate, even when informed by objective clinical indicators, and the trend is usually to over-estimate prognosis and to under-estimate planning for possible need, especially for those with non-cancer illnesses. The aim of this paper is to enable better identification of patients who may need supportive/ palliative care. It focuses more on pragmatically and instinctively improving prediction of decline, leading to better anticipation of need for support, and less on pure prognostication of time remaining, for which there is much more accurate guidance available (see GSF website). In anticipating this possible deterioration, earlier discussions about preferences and needs can be initiated; some practical measures could be introduced leading to prevention of crises and referral sought for extra help or advice. The aim of such Advance Care Planning discussions , is to seek out their particular unmet needs and preferences, sometimes previously unvoiced, enabling more people to live out the final stage of life as they wish. We suggest a change towards instinctive, anticipatory and ‘insurance-type’ thinking, rather than pure prediction of likely timescale, so that appropriate support and care can be mobilised. We know that some attempt to improve this prediction, however inaccurate, is key to beginning the process that leads to better end of life care for all. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 13 of 26 How to use this Guidance This Guidance document aims to clarify triggers for consideration of patients in need of supportive/palliative care. This is not attempting to answer the question ‘how long have I got?’ but more in answer to the question ‘what can we do?’, and is in response to the common way of thinking ‘Hope for the best but prepare for the worst’. The main processes used in GSF are to identify, assess, plan, and at all times communicate about patient care and preferences. Use of this guidance might enable better identification of patients nearing the end of their lives i.e. in the last 6-12 months of life, to trigger better assessment and pre-planning e.g. holistic needs assessment, Advance Care Plans, and the appropriate management care plan and provision of supportive care related to their needs. For primary care teams, this is the first step towards developing a Supportive/ Palliative Care Register, now part of QOF palliative care points in the GMS contract. For more details of suggestions for claiming the QOF points, templates etc see the www.goldstandardsframework.nhs.uk/gp_contract.php. For those using the Gold Standards Framework (GSF), this might trigger inclusion of more non-cancer patients in the current Supportive Care Register. Of course, not all of these tests are performed in primary care, but GPs/DNs collate information from hospitals and, together with their own holistic assessment, form an overall view of a patient’s likely prognosis. N.B: It can be much harder to predict whether patients in the third category of frail elderly patients are nearing end of their lives, as they are intrinsically more complex and vulnerable, with a more chronic variable illness trajectory. We do not suggest necessarily that all patients in this third category are included on the GSF Supportive Care Register, unless they fulfil the other criteria of co-morbidity, need or predicted decline, but we are suggesting that more non-cancer organ failure patients be included i.e. with Heart Failure and COPD, to the expected prevalence or to represent at least half the patients in the Supportive Care registers For hospital teams, in addition to accessing supportive/palliative care services and consideration of supportive measures, it would also be helpful to notify the GP/Primary care team that this patient has advanced disease and could be included on their Supportive/Palliative Care Register. For specialist palliative care/ hospice teams - Although traditionally focussed mainly on cancer patients, specialist palliative care now extends to patients with non-cancer illnesses. There is greater collaboration with other teams e.g. heart failure nurses, to provide best patient care, and these indicators may help clarify referrals. For PCTs /Commissioners/managers etc - This could be used as part of an End of Life care strategic plan for the area, with improved provision of services for all patients nearing the end of life. NB Long Term Conditions. There is a strong overlap with care for patients with Long Term Conditions and prediction of unplanned admissions to hospital and that of patients with advanced disease in the last year of life. This is especially true for patients with heart failure or COPD. Close collaboration with Case Managers to support good end of life care is very important. For Care Homes - Use of some broad prognostic indicators has been found to help identify patients most in need in some care homes, and help focus care and trigger key actions (see below and GSF Care Homes on website) Examples of prognostic indicators used as part of patient needs assessment Patients have differing requirements at varying stages of their illness. Some GPs categorise their patients on the Supportive Care Register according to estimated prognosis and need, and colour code them accordingly. Care Homes using the GSF for Care Homes Programmes have also found the intuitive grouping of their residents to be very helpful. Although only a rough guide, this helps teams ’awareness of patients’ varying needs, focuses care to ensure that the right care is directed at the right time, ensures regular review, and triggers key actions at each stage. A needs/support plan is therefore developed. Suggested prognostic coding could be: C - ‘Continuing Care’ D - ‘Days’ Unstable / frequent exacerbations Deteriorating Dying / terminal phase Months prognosis Weeks prognosis Days prognosis A - ‘All’ B - ‘Benefits’ eg DS1500 Stable Years + prognosis The use of means of estimating approximate prognosis and need i.e. the intuitive ‘surprise’ question, needs/choice based care, and these clinical indicators, may help to ensure that patients with advanced illness receive higher quality proactive care and support as they near the end of their lives. Development of this guidance paper. This paper was developed and later fully revised following wide consultation with a large number of specialist clinical bodies, special interest groups, national disease associations, Royal College of General Practitioners and major palliative care texts. We were helped also by considering prognostic indicators from other countries eg USA, used to trigger referral of non-cancer patients to hospice/palliative care. Since its first development in June 06, this ‘PIG’ paper has been widely used by clinicians nationally and internationally, by GPs in the UK (90% of whom now have supportive/palliative care registers), by care homes’ staff, researchers and many others. We undertake regular reviews and would be pleased to receive any comments or ideas for improvements or example of usage. The accompanying Needs Support Matrixes are also in development for most conditions. Further information and other prognostic guidance is available from www.goldstandardsframework.nhs.uk Prof Keri Thomas, Dr Amanda Free and members of the National GSF Centre info@goldstandardsframework.nhs.uk References The ‘Surprise question’ was first developed and expounded by Prof Joanne Lynn, RAND Lecturer USA and senior advisor on end of life care. 1 Others from Community Hospices: www.communityhospices.org/_assets/TWH_indicator_crds6.pdf 2 Hospice Referral Guidelines adapted from AMJ of Hospice and Palliative Care; Sept/Oct 1997, NHO guidelines 3 Weissman, MD. Determining prognosis in advanced cancer. Fast Fact and Concept #13; 2nd Edition, July 2005. End-of-Life Palliative Education resource Center 4 NHS Modernisation Agency- Coronary Heart Disease Collaborative (December 2004) Palliative and Supportive Care in Heart Failure: www.heart.nhs.uk/serviceimprovement/1338/4668/Palliative%20Care%20Framework.pdf www.heart.nhs.uk 5 Chronic obstructive pulmonary disease: Management of chronic obstructive pulmonary disease in adults in primary and secondary care. National Institute for Clinical Excellence. London. (February 2004) British Thoracic Society Long term Oxygen Therapy Criteria www.brit-thoracic.org.uk/cgi-bin/showpage.fcgi 6 Communication from the broad renal multi professional team and nominated by the renal association, renal advisory group of the NSF, British Renal Society, and British Transplant Society. www.britishrenal.org 7 Communication from Tricia Holmes, Director of Care Development at Motor Neurone Disease Association: www.mndassociation.org 8 Communication from The Just Invisible Report on Parkinsons Disease Society; 2005 9 MS and Palliative Care A guide for health and Social Care Professionals Chapter 2 pg 12 (2006) 10 Gaub, Mary Gunter, Prost, Evan, Bomar, Marilee, Farid, Reza, Et al., 2004. Efficacy of Balance and Flexibility Intervention in a Frail Female Centenarian, Journal of Geriatric Physical Therapy, Availab from: www.findarticles.com/p/articles/mi_qa4055/is_200301/ai_n9465425 Full Barthel Guidance on Using to Improve / End of Life Care in Primary Care v25 July 06 Page 14 of 26 11 Score: Barthel's indexQOF of activities of daily livingPalliative (BAI), http://www.patient.co.uk/showdoc/40001654/ 12 Watson M, Lucas C, Hoy A, Back I (2005) Oxford Handbook of Palliative Care: Oxford University Press 13 Am. J. Clin. Oncol.:Oken, M.M., Creech, R.H., Tormey, D.C., Horton, J., Davis, T.E., McFadden, E.T., Carbone, P.P.: Toxicity And Response Criteria Of The Eastern Cooperative Oncology Group. Am J Clin Oncol 5:649-655, 1982. Appendix 2 – SCR1, SCR2, MDT C SCR1 Summary of Palliative Care Patients Name of patient Name of Carer Diagnosis( +code) G P D N Problems/ Concerns Anticipated needs Information given/ Carer issues DS 1500 date Macmillan Nurse/ CNS Hospic e/ SPC SCR1 Summary sheet - Gold Standards Framework © Keri Thomas and Department of Health England 2005 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 15 of 26 OOH Handover Form Date sent Preferred place of Care stated + date Actual place death + date Berea vement Care Crisis Events/ Notes B SCR2 Supportive Care Register Front sheet Name Diagnosis ........................................... Comp No Secondaries DOB DS 1500 date/Ca registered.....….. Date of diagnosis Hosp No Address Family/carer contacts Tel No Personnel involved Key GP Key DN Oncologist ........................................ .................. .................. Other specialists ............................... .................. .................. Macmillan/Nurse/SPC Hospice .................. .................. Others eg SS..................................... Other conditions Treatment Surgery Radiotherapy Chemotherapy Current Medication Priorities (Problems and concerns- physical, psychological, social, spiritual) Other issues (incl. care plan, out of hours care, drugs left at home, before considering admission try etc) Preferred place of care: Comments: Date: Supportive Care Register front-sheet / Out of hours handover form - Gold Standards Framework © Keri Thomas and Department of Health England 2005 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 16 of 26 SCR2 Supportive Care Register Front sheet contd./…. Date Initials Notes/important events /cont over …. Supportive Care Register front-sheet / Out of hours handover form - Gold Standards Framework © Keri Thomas and Department of Health England 2005 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 17 of 26 C Example of holding a Meeting for palliative care using GSF Combine with your usual MDT meeting Meet with GPs, District Nurses, admin staff eg practice manager Invite specialist palliative care nurses / Macmillan / hospice nurses Sometimes representatives from other groups eg practice nurses, receptionists, social services etc Preferably monthly meetings or more regular - minimum 3 monthly Suggested plan of meeting 1. Discuss new patients for inclusion on the register according to your inclusion criteria eg cancer patients, those eligible for DS1500, those suspected to be in last year of life with the surprise question etc 2. Discuss existing patients on register- use the SCR1 and 2 to act as checklist and reminders- keep in mind current plans, patient preferences, communication with others, anticipating future needs and proactive planning. 3. Review patient deaths - use Significant Event Analysis, After Death Analysis etc Staff support and debriefing. Bereavement follow up for family and carers. 4. Action points - learning needs, commissioning issues, practice protocols/ procedures, audit etc AOB Next meeting date. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 18 of 26 Appendix 3 – Significant Event Analysis SIGNIFICANT EVENT ANALYSIS SCR 6 WHAT WENT WELL? WHAT DIDN’T GO SO WELL? WHAT COULD HAVE BEEN DONE BETTER? Traffic lights SEA -© Gold Standards Framework 2005 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 19 of 26 Appendix 4 - Palliative Care Read Codes – GSF Template Supportive Care Register 8CM1 9EB5 8H7g On Gold Standards Palliative Care Framework DS1500 issued to patient Palliative Care Referral QOF Points QOF Points QOF Points Preferred Place of Care 8CN1 94Z1 94Z2 94Z3 94Z4 94Z5 Preferred Place of care /death (Chosen / Discussed) - PPD PPD - home PPD - Hospice PPD - Community hospital PPD - hospital PPD - nursing home Suggested as Suggested as Suggested as Suggested as Suggested as Suggested as useful useful useful useful useful useful Suggested as Suggested as Suggested as Suggested as Suggested as Suggested as useful useful useful useful useful useful Advance Care Planning 1R1 13VH 9X0 9X1 9X2 9X20 Not for resuscitation Living Will Advance directive discussed with patient Advance directive discussed with relative Advance directive signed Advance directive signed, copy in notes Treatment plan / care plan 8BC1 8BAD 8BC4 Treatment plan given Pain and symptom management On a syringe driver Suggested as useful Suggested as useful Suggested as useful GP OOH service notified Suggested as useful Out of Hours 9e0 Specialist Palliative Care 8HH7 8HY 8BAR 8BAS 8BAT 8BAP 8H6A 8H7L 8BJ1 Referred to Community Specialist Palliative Care Team Referral to hospice Referral to Specialist Palliative Care In-patient Referral to Specialist Palliative Care Day-care Referral to Specialist Palliative Care Out-patient Specialist Palliative Care Refer to terminal care consult Refer for terminal care Palliative treatment QOF Points Suggested as useful Suggested as useful QOF Points QOF Points QOF Points QOF Points QOF Points QOF Points Terminal care End of Life pathway QOF Points Suggested as useful Care of the Dying 8BA2 8BAQ Read Codes for Carers 918F 971E 13Hc 8O81 Has a carer Discussed with carer Bereavement Bereavement support Suggested as Suggested as Suggested as Suggested as useful useful useful useful Suggested as Suggested as Suggested as Suggested as Suggested as Suggested as Suggested as Suggested as useful useful useful useful useful useful useful useful Read Codes following death 949 9491 9493 9495 949A 949B 949C 94B Patient died to record Place of death Died at home Died in nursing home Died in hospital Died in hospice Died in community hospital Died in surgery Cause of death Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 20 of 26 Appendix 5 – Levels of Adoption of GSF Level 1 – C 1, 2 First Gear Set up SC Register, Primary Care Team Meeting and Coordinator Level 2 – C 3, 4, 5 Second Gear Assessment Tools, Out of Hours Handover, Education Audit and Reflective Practice Level 3 – C 6, 7 Third Gear Carer/family support, bereavement plan and care in the final days Level 4 – Sustain embed extend Fourth Gear Sustain and build on all developments as standard practice Embed – develop a practice protocol, PCT LES etc Extend to other settings e.g. care homes, non cancer, Advance Care Planning, pathway for the last days (LCP) and other areas Then cruise on in fifth gear! Level 4 Level 3 Level 2 Level 1 C6, 7 C3, 4, 5 Practice protocol Sustained Extend eg care homes C1, 2 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 21 of 26 Appendix 6 – Suggested QOF Assessment for Palliative Care Points 1 Palliative/Supportive Care Register in place for patients in last year of life 2 Evidence of inclusion of non-cancer patients 3 Dates of multidisciplinary team meetings 4 Meetings are multidisciplinary case review meetings to discuss those patients on the register 5 Evidence that a management plan/advance care plan, which includes preference for place of care, is used 6 Evidence that carers’ needs are addressed Y N Y N Further related areas to look at see page 6, please note that 52 points can be covered using GSF Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 22 of 26 Glossary to terms in PIG ADL: Activities of daily living Barthel’s index: Assessment of ability to perform activities of daily living, using 10 different areas of activity and a score of 0-20. A higher score denotes greater functional independence. CHF: Congestive heart failure. A condition where the heart is unable to meet the body’s needs. This results in a build up of fluid, or congestion, in the tissues. CKD: Chronic kidney disease, measured in stages 1 to 5, with stage 5 being established renal failure. COPD: Chronic obstructive pulmonary disease. A chronic, progressive disorder characterised by airways obstruction and little or no reversibility. DS1500: form that should be completed in order to claim the Disability Living Allowance. All patients in the last 6 months of life are entitled to this. eGFR: Estimated glomerular filtration rate. A formula-based estimation of glomerular filtration rate, calculated and reported automatically by clinical biochemistry laboratories using serum creatinine, age, sex and ethnicity. GFR>60: stages 1+2 CKD GFR 30-59: stage 3 CKD GFR<30: stages 4+5 CKD FEV1: Forced expiratory volume in 1 second, is the volume of air expelled in the first second of a forced expiration using spirometry, measured in litres. Forced Vital Capacity (FVC): The volume expired during a full forced expiration into a spirometer. The FEV1/FVC ratio gives an estimate of severity of airflow obstruction. ITU: Intensive therapy unit, formerly known as Intensive care unit. Karnofsky Performance Status (KPS): A scoring system to assess the well-being of palliative care patients and their ability to perform ordinary tasks, from 0% (dead) to 100% (fully active) and used in prognostication. Further details are in the Prognostic Indicators Guidance paper. MDT: Multi-disciplinary team; involving nurses, doctors, social worker, occupational therapist, etc. as appropriate, working together. MRC grade: The Medical Research Council dyspnoea scale for grading the degree of a patient’s breathlessness. 1. Not troubled by breathlessness except on strenuous exercise. 2. Short of breath when hurrying or walking up a slight hill. 3. Walks slower than contemporaries on the level because of breathlessness, or has to stop for breath when walking at own pace. 4. Stops for breath after about 100m or after a few minutes on the level. 5. Too breathless to leave the house, or breathless when dressing or undressing. NIV: Non-invasive ventilation, as opposed to ventilation via tracheostomy or intubation; often known as NIPPV or non-invasive positive pressure ventilation. Ventilatory assistance to aid respiration at night time, and as disease progresses it can also be used during the day. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 23 of 26 NYHA class: The New York Heart Association classification of functional severity in heart failure. Class I: heart disease present but no undue dyspnoea. Class II: comfortable at rest; dyspnoea on ordinary activities. Class III: less than ordinary activity causes dyspnoea, which is limiting. Class IV: dyspnoea present at rest; all activity causes discomfort. OOH form: form to be faxed to the Out of Hours service informing them of the patient’s needs and preferences. Pressure Sore grades: Classification of pressure sores improves patient assessment and subsequent intervention. Grade I: The precursor phase. Redness which blanches with light pressure. Grade II: Redness which remains when light pressure applied. Grade III: Full thickness loss of skin not including the subcutaneous tissue. Grade IV: The sore extends into subcutaneous tissue and deep fascia. PHCT: Primary health care team, a community based, multidisciplinary team, working from or with the GP practice. Read codes: A standard set of clinical terms produced and maintained by the NHS Information Authority, used for inputting data into clinical IT systems. SCR: Supportive care register. A register of all patients with supportive or palliative care needs. QOF: Quality and outcomes framework of the new GMS contract for GPs. The framework, by awarding points for achievement of certain targets, is an attempt to reward GPs for good practice. Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 24 of 26 General References Doyle D, Hanks G, McDonald N (Eds) (1995) Oxford Textbook of Palliative Medicine: Oxford University Press : Oxford Hospice of Baltimore: www.gbmc.org/hospice University of Pennsylvania / Genesis Eldercare: Identification of a Palliative Care Customer: www.mywhatever.com/cifwriter/library/41/pe6010.html End Stage Disease Indicators, Community Hospices Leaders in End of Life Care Since 1888, Maryland, Northern Virginia and Washington DC Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 25 of 26 Full Guidance on Using QOF to Improve Palliative / End of Life Care in Primary Care v25 July 06 Page 26 of 26