request for examination
advertisement

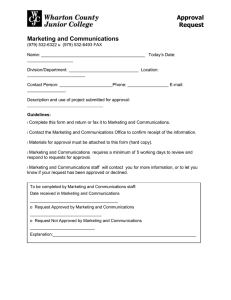
REQUEST FOR EXAMINATION r STAT Patient Information Physician Information First Name Last Name Name Address Home Phone Other Phone Phone Fax M OHIP Version Code |F MM / DD Sex Date of Birth Appointment Date/Time MM / DD / YYYY / YYYY Date Doctor’s Signature Copy To / YYYY Appointment Date Appointment Time Name X-Ray (No Appointment) SPINE & PELVIC UPPER EXTREMITIES r Single/KUB r Acute (includes PA chest) r Cervical Spine r Thoracic Spine r Lumbar (L/S) Spine* r L/S Spine Pelvis & R L HEAD & NECK r Neck for soft tissues r Skull r Sinuses r Facial Bones r Nose r Mandible r Orbits r Temporomandibular joint -TMJ CHEST r Chest PA & LAT r Ribs: r R r L r B (includes PA chest) r Sterno – Clavicular Jts. r Sternum Fax # Ultrasound (By Appointment) ABDOMEN MM / DD S.I. Joints* r Sacrum/Coccyx r S. I. Joints r Pelvis LOWER EXTREMITIES R L r r Hip r r Femur r r Knee r r Tib. & Fib. r r Ankle r r Foot r r Heel r r Toe: 1 2 3 r r Elbow r r Forearm r r Shoulder r r Humerus r r Clavicle r r A. C. Joints r r Scapula r r Wrist r r Scaphoid r r Hand r r Finger: 1 2 2 3 4 1 4 5 5 3 4 5 r Abdomen r Abdomen & Pelvis r Pelvis - Transvaginal unless contraindicated r PVR -Post Void Residual r Bladder r Transrectal Prostate r Renal r Abdominal Wall r Nuchal Translucency- IPS (11-13 weeks) r OB — Under 16 weeks MM / DD / YYYY LMP: r OB — Over 16 weeks r Thyroid and/or Neck r Aorta r Carotid r Scrotum r Inguinal canal: r Right r Left r Upper Extremity Venous: r Right r Left r Upper Extremity Arterial: r Right r Left r Lower Extremity Venous: r Right r Left r Lower Extremity Arterial: r Right r Left r MSK r Other r Other: r Echocardiogram: Clinical History Requested BMD r WSIB Gastrics (By Appointment) r Baseline r 3yr- First follow-up Low Risk: High Risk: r 5 year r 1 year r r r r r UGI Barium Swallow Small Bowel UGI/SBFT Barium Enema Breast Imaging (By Appointment) r Mammogram r Ultrasound r Left r Right r Bilateral r Implants r OBSP Right Left www.cmlhealthcare.com 24-hour notice required to cancel appointment or $75 charge will be billed to patient. * As per Ministry of Health Guidelines IMG-ON-GTA-04 * Please bring your health card and this paper with you to your appointment. (X) X-Ray (U) Ultrasound (M) Mammography Brampton North York 164 Queen Street E. Phone: 905-450-6717 Fax: 905-450-6719 (X/U/M/B/V) 1 hour Validated Prkng 4949 Bathurst St.,Unit #100 Phone: 416-223-5460 Fax: 416-223-8335 (X/U/M) Bathurst & Finch Free Parking Mississauga 10 Kingsbridge Garden, #100 Phone: 905-568-3768 Fax: 905-568-9652 (U/CT/MRI) Free Parking Hurontario & 403 71 King Street W., Unit #102 Phone: 905-897-1144 Fax: 905-897-1146 (X/U/B/M/V) Oakville 1525 Cornwall Rd. , Suite 18 Phone: 905-815-0999 Fax: 905-815-0997 (V) 581 Argus Rd. , Lower Level Phone: 905-338-6644 Fax: 905-338-6656 (X/U/B-Lab Services) 4800 Leslie Street, Unit #LL Phone: 416-493-1011 Fax: 416-493-1019 (X/U/M/B/F/E/V) Leslie & Sheppard Free Parking 4430 Bathurst St., Unit #206 Phone: 416-226-6941 Fax: 416-226-4270 (X/U/B/V - Lab) Free Parking 5801 Yonge Street, Unit #5 Phone: 416-222-6989 Fax: 416-222-4278 (X/U/M/B/V) Free Parking Food Basics plaza 491 Lawrence Ave. W., Bsmnt Phone: 416-781-9375 Fax: 416-781-7175 (X/U/M/B) Bathurst & Lawrence 5 Fairview Mall Dr., Unit #100 Phone: 416-499-3559 Fax: 416-499-4631 (X/U/M/B/E/V) Close to Fairview Mall (D) Doppler (F) Fluoroscopy 1017 Wilson Ave., Unit #100 Phone: 416-631-7581 Fax: 416-631-9759 (X/U - Lab Services) Downtown Toronto 1881 Yonge St., Unit #402 Phone: 416-966-3886 Fax: 416-487-8746 (V) Yonge & Davisville 1881 Yonge St., Unit #612 Phone: 416-487-2425 Fax: 416-487-0746 (U) Yonge & Davisville 11 King Street W., Suite C-100 Phone: 416-864-1814 Fax: 416-864-1499 (X/U/F) Yonge & King 790 Bay St., Unit #418 Phone: 416-260-9382 Fax: 416-260-2274 (X/U) Corner of Bay & College Women’s Imaging Centre 790 Bay St., Unit # 520 Phone: 416-260-1974 Fax: 416-260-1687 (U) Corner of Bay & College (B) Bone Mineral Density 280 Spadina Ave., Unit #306 Phone: 416-603-1197 Fax: 416-603-1199 (X/U/M/B/F) At Spadina & Dundas In Dragon City Mall 39 Pleasant Blvd., 2nd Flr Phone: 416-928-3467 Fax: 416-928-3502 (U/B/N) One block south of St Clair East off of Yonge 586 Eglinton Ave.E., #104 Phone: 416-485-9471 Fax: 416-485-9309 (U/X/M/B) Eglinton, one block west of Bayview Thornhill 7131 Bathurst St., #LL03 Phone: 905-889-2400 Fax: 905-889-2455 (X/U/B - Lab Services) Bathurst & Steeles Free Parking Newmarket 17215 Leslie St Phone: 905-836-2626 Fax: 905-836-5043 (X/U/M - Lab Services) No Frills Plaza Free Parking For additional locations across Ontario, visit www.cmlhealthcare.com Preparation & Instructions (G) Gastric Ultrasound Preparation and Instructions No eating or drinking (smoking or chewing gum) 8 hours prior to appointment. Obstetrical/Pelvis (V) Vascular (N) Nuclear Scarborough Ajax 1371 Neilson Rd., Unit #309 Phone: 416-287-1818 Fax: 416-287-2126 (X/U/B) White Medical Bldg. 300 Harwood Ave. S. Phone: 905-426-8976 Fax: 905-426-7843 (CT/MRI) Free Parking 4190 Finch Ave. E., #LL04 Phone: 416-293-5940 Fax: 416-293-6036 (X/U/M/B/E - Lab ) Finch & Midland Free Parking 2901 Lawrence Ave. E., Unit #103 Phone: 416-266-7535 Fax: 416-266-9631 (X/U/B - Lab Services) 4 story tan medical building Pickering 1105 Kingston Road, #D202 Phone: 905-420-3068 Fax: 905-420-6057 (X/U/M/B - Lab-Services ) Above Shoppers Free Parking Markham 10 Unionville Gate, Unit #204 Phone: 905-479-3945 Fax: 905-479-5538 (X/U/M/B) Unionville Med Centre Free Parking 6633 Hwy 7, Unit #5 Phone: 905-294-4880 Fax: 905-472-6629 (X/U) Free Parking Connect with us These instructions are IMPORTANT. Please follow them. Abdomen (E) Echo @cmlhealthcare * CML is a scent free environment Gastric Preparation and Instructions Stomach, UGI, Barium Swallow Nothing to eat or drink after midnight, which includes chewing gum, candies and smoking. 34oz or 1Litre of water 1 hour prior to appointment. Do not go to the washroom. Small Bowel Preparation (Allow 2-5 hours for appointment) Abdomen/Pelvis Nothing to eat or drink after midnight, which includes chewing gum, candies and smoking. No eating or drinking 8 hours prior to appointment. 34oz or 1Litre of water 1 hour prior to appointment. Do not go to the washroom. Colon Examination (Barium Enema) Prostate (Transrectal) Clear fluids for the two (2) days prior to this examination. (fruit juice, bouillon, clear beef or Fleet enema 2 hours before the examination (kit may be purchased at your pharmacy.) Drink 34oz or 1Litre of water 1 hour prior to appointment. Do not go to the washroom. Bone Mineral Densitometry Do not take calcium supplements for 24 hours prior to examination. Patients are asked to wear clothing without zippers or metal attachments. Mammogram Remove deodorant, powder and perfume prior to appointment. chicken broth, consomme, gelatin, popsicles and coffee or tea with sugar. Two days before the exam: Clear fluids The day before the exam: Clear fluids Take: 10 ozs. (chilled) Magnesium Citrate at 4:00 p.m., 3 Dulcolax tablets at 6:00 p.m. (Do not crush or chew tablets), At least 5 large glasses of water during the afternoon and evening prior to examination. Day of the examination: May have clear fluids only until examination is completed.