1000
STROKE
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
8. Manuck SB, Kaplan JR, Clarkson TB: Behaviorally induced heart
rate reactivity and atherosclerosis in cynomolgus monkeys. Psychosom Med 45: 95-108, 1983
9. Kaplan JR, Manuck SB, Clarkson TB, et al. Social stress and
atherosclerosis in normocholesterolemic monkeys. Science 220:
733-735, 1983
10. Lipid Research Clinics Program. Manual of Laboratory Operations: Lipid and lipoprotein analysis. DHEW publication no.
(NIH) 76-628. Bethesda, Maryland: National Institutes of Health,
1974
11. Williams RB: Psychophysical differences between Type A and B
individuals that may lead to coronary heart disease. In: Dembroski
TM (ed). Proceedings of the Fonim on Coronary Prone Behavior.
DHEW publication no. (NIH) 78-1451:185-191, 1977
12. Siegel J: Nonparametric statistics. New York, McGraw Hill, 1956
13. Castelli WP: High density lipoproteins: An overview. In Gotto AM
Jr, Smith LC, Allen B (eds.), Atherosclerosis V. New York,
Springer-Verlag, 478-483, 1980
14. Kirk RE: Experimental design (2nd Edition), Belmont, CA,
Brooks/Cole, 1982
15. Solberg LA, McGarry PA, Moossy J, et al: Distribution of cerebral
atherosclerosis by geographic location, race and sex. Lab Invest
18: 604-612, 1968
VOL
15, N o
6, NOVEMBER-DECEMBER 1984
16. Kuller L, Reisler DM: An explanation for variations in distribution
of stroke and arteriosclerotic heart disease among populations and
racial groups. Am J Epidemiol 93: 1-9, 1971
17. Kuller LH: Epidemiology of stroke. In: Schoenberg BS (ed), Advances in Neurology, Vol. 19. New York, Raven Press, 281-311,
1978
18. Lavy S: Medical risk factors for stroke. In: Goldstein M et al (eds),
Advances in Neurology, Vol. 25. New York, Raven Press, 127—
133, 1979
19. Wolf PA, Kannel WB, Dawber TR: Prospective investigations:
The Framingham study and the epidemiology of stroke. In:
Schoenberg BS (ed), Advances in Neurology, Vol 19. New York,
Raven Press, 107-120, 1978
20. Corbett WT, Schey HM, Lehner NDM, et al: Standardized method
for recording blood pressure in anesthetized Macaca fascicularis.
Lab Anim 15: 37-40, 1981
21. Hollander W, Geer JC, Garcia JH: Aggravation of cerebral atherosclerosis by hypertension. Arteriosclerosis 3: 479a, 1983
22. Glagov S: Low heart rate retards coronary atherosclerosis. Arteriosclerosis 3: 466a, 1983
23. Hamm TE, Kaplan JR, Clarkson TB, et al: Gender and social
factors in the atherosclerosis of cynomolgus monkeys. Atherosclerosis 48: 221-233, 1983
CT-CBF Correlations of Cognitive Deficits in
Multi-Infarct Dementia
Y A S U H I S A K I T A G A W A , M . D . , P H . D . , JOHN S. MEYER, M . D . , HISAO TACHIBANA, M . D . , P H . D .
K A R L F. MORTEL, P H . D . , AND ROBERT L. ROGERS, M . A .
SUMMARY Fifteen right-handed patients with Multi-Infarct Dementia underwent cognitive testing by
the Jacobs Mini-Mental Scale (MMQ), and xenon contrast CT scanning. Local cerebral blood flow (LCBF)
and local partition coefficient (LX) values were measured by stable xenon contrast CT scanning and
potential methodological errors were discussed. Reduced values were graded: 0 = normal, 1 = mild, 2 =
moderate, 3 = severe. Graded values were pooled and plotted on composite brain maps to display locations
of abnormal LX and LCBF values. Topographic brain maps, showing most frequent locations of reduced L>.
values, confirmed the common anatomical locations of multiple cerebral infarcts to be distributed in both
thalami, temporal lobes, basal ganglia, left internal capsule and right cingulate cortex. Gray matter flow
values were reduced in similar cortical and subcortical regions. There were no correlations between MMQ
scores and reduced LCBF values for caudate and lenticular nuclei. Direct and statistically significant
correlations were found between reduced MMQ scores and mean LCBF values for left or right frontal
cortex, left or right temporal cortex and left or right thalamus. Subgrouping MMQ tests according to
functions assessed, indicated that left mid-temporal ischemia correlated with dyscalculia and memory
disturbances while ischemia of both frontal lobes correlated with disorientation to time and place.
Stroke Vol 15, No 6, 1984
DEMENTIA is becoming a serious public health problem in our aging population. Epidemiological studies
have shown that dementia is present in 4.4-8% of
populations over age 65 years.'^ Pathological investigations have revealed that of the commonest forms of
dementia, about 50% of elderly demented patients sufFrom the Cerebrovascular Research Laboratories, VA Medical Center, Department of Neurology, Baylor College of Medicine; and Department of Psychology, University of Houston, Houston, Texas. This
work was supported, in part, by the Veterans Administration Medical
Center and by a Grant provided by Mr. Harry K. Smith and Mr. Albert
K. Smith, Houston, Texas.
Address correspondence to: John S. Meyer, M.D., Director, Cerebrovascular Research Laboratories, VA Medical Center, 2002 Holcombe Boulevard, Houston, Texas 77211.
Received October 17, 1983; revision #2 accepted May 11, 1984.
fer from senile dementia of Alzheimer's type (SDAT),
20% from multi-infarct dementia (MID) and 10% have
both diseases (MIX).1
Differentiation between SDAT and MID is a commonly encountered diagnostic problem in the clinic.
Hachinski's ischemic score5 has proven clinically useful in distinguishing between these most common
types of dementia and the validity of this scoring system has been neuropathologically established in a series of autopsied cases by Rosen, et al.6
The present communication will attempt to correlate
cognitive deficits measured in patients with MID with
quantitative measurements of local cerebral blood flow
measured by xenon contrast CT scanning.
In the majority of cases, MID appears to be a cere-
1001
STABLE XENON, CTCBF IN MID/Kitagawa et al
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
bral manifestation of long-standing hypertension. At
autopsy hyperplastic cerebral arteriosclerosis is evident with bilateral multiple small lacunar infarcts.7 The
severity of the dementia is not only proportional to the
cumulative severity of the lacunar state, but also to the
locations of the lacunes. 8 From a cognitive point of
view, patients with MID may be considered as a useful
model. They offer an opportunity for studying those
regions of the brain, which if damaged by multiple
small infarcts, may give rise to dementia.
Cerebral blood flow studies have provided some
insights concerning the pathogenesis and differences
between MID and SDAT.9"21 It has been known for 30
years that organic dementia is consistently accompanied by bilateral hemispheric reductions of cerebral
blood flow and oxygen uptake. 9
The development of regional methods for measuring
cerebral blood flow, such as I33Xe clearance methods,
made some regional quantitation possible between
cognitive deficits and the severity and nature of dementia.10"21 However, these two-dimensional radioisotopic methods ignore or underestimate many zones of
zero or reduced flow because clearance of l33Xe from
bordering zones obscures them (so-called "look
through" phenomenon). There are other problems
which impair the resolving powers of the 133Xe method
including Compton scatter and lack of knowledge of
brain-tissue solubility coefficients (IA).
With the advent of computerized reconstruction
techniques for transmission and emission tomography
it is now possible to image the brain in three dimensions with high resolution. Positron emission tomography provides considerable advantages of measuring
both blood flow and metabolism but has the disadvantages of enormous cost, prolonged time consumption
for patients and investigators and relatively poor resolution compared to computerized x-ray transmission
tomography.22-23
TABLE 1 Case Series
Age
Case
numbers
The excellent resolving powers of x-ray transmission tomography, utilizing the CT scanner for measuring both LA. and LCBF during inhalation of stable
xenon gas (CTCBF method), overcomes the limitations of the 133Xe clearance method and provides the
best resolution of any method presently available for
measuring cerebral blood flow (circa 80 cu mm).24"32
The purpose of the present communication is to
report regional patterns of reduced LA. and LCBF values measured by the CTCBF method in 15 patients
with well-established MID and to correlate anatomical
zones of regional ischemia with cognitive deficits
measured within a few days of the LCBF and LA.
determinations.
Case Series
Fifteen right-handed and cooperative patients with
well-defined MID were selected from a larger series
with this disease being followed in this laboratory. The
diagnosis in all patients was well-established. It was
confirmed by history of sudden onset and fluctuating
course, the presence of risk factors for cerebrovascular
disease and by medical and neurological examinations
showing hypertension, cerebral arteriosclerosis by
neurovascular examination (bruits, hypertensive retinal changes, etc.) and focal neurological signs. The
cognitive deficits were confirmed by the Mini-Mental
Status examination (MMQ) of Jacobs, et al33 modified
after that described by Folstein, et al.34 Scores in normal age-matched volunteers are between 29-31 but the
patient's scores were between 11-20 (table 1).
The patient's ages ranged from 57 to 85 years with a
mean age of 71.5 ± 10.1. All patients had a history of
chronic but not malignant or accelerated hypertension,
recurrent attacks of cerebral ischemia including transient ischemic attacks, reversible ischemic neurological deficits and small strokes. Patients with large or
aphasic strokes were excluded. All showed evidence
MABP
(mmHg)
(in years)
Gender
1
84
F
110
2
72
F
104
3
54
M
129
4
65
M
97
5
81
M
98
6
72
M
123
7
79
M
110
8
75
M
97
9
85
F
100
10
60
F
109
11
57
M
99
12
74
F
93
13
79
F
97
14
77
F
93
15
59
F
89
71.5±10.1
7M.8F
Mean values
103.2± 11.2
PECOj
(mmHg)
34.6
38.5
34.2
35.6
37.1
34.2
35.7
35.9
28.7
35.9
35.7
33.0
40.2
34.2
35.7
35.3±2.6
Ischemic
score
MMQ
11
15
7
13
value
9
17
9
11
8
18
11
20
7
19
12
13
7
16
10
18
9
19
10
14
9
19
7
14
7
8.9±1.7
16
16.1 ±2.7
1002
STROKE
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
of arteriosclerosis elsewhere in the body such as arteriosclerotic heart disease, arteriosclerotic retinopathy
and/or bruits over the carotid and vertebral arteries.
There were focal neurological signs on examination, a
history of focal neurologic symptoms, the presence of
at least one or more risk factors for atherothrombotic
stroke, step-wise neurologic deterioration, and multisegmental cerebral atherosclerosis revealed in the majority of cases by aorto-cranial arteriogTaphy. CT scanning in all cases showed evidence of multiple cerebral
infarcts (low density lesions, asymmetrical or focal
cortical atrophy, ventricular asymmetry). Cases with
recent stroke (within 30 days of the last stroke) were
excluded to avoid any influences ofreactivehyperemia
upon CBF. The ischemic index criteria of MayerGross, as described by Hachinski, et al,14 were part of
the evaluation used for differentiating MID from
SDAT. Patients with an ischemic index of 7 or more
were considered qualified to meet the rigid criteria
required for establishing an unequivocal clinical diagnosis of MID. Patients with Bingwanger's subcortical
leukoencephalopathy were excluded by the criteria
listed above, plus the characteristic CT findings of a
diffuse rather than multifocal low density lesions by
CT examination.35
Table 1 displays the mean age, gender, mean arterial
blood pressure, PECO2, Hachinski's Ischemic Score,
and MMQ at the time of measurement of LCBF and LX
values.
Methods
Measurements of LCBF and LX were carried out
utilizing the stable xenon CTCBF method for each
region of interest by means of a single compartmental
analysis program. Details of the method have been
reported in previous publications.24 2J28-31 After explaining the procedure to each patient and family, including a simple explanation of the exposure to x-rays
and the discomfort of lying in the scanner for 20 minutes, informed consent* was signed by both patient
and the legal guardian.
Patients were asked to fast for 6 hours before the CT
scanning to avoid the possibility of vomiting during the
procedure. Each patient was then placed in the EMI
1010 CT scanner to obtain two back-to-back 8 mm
brain slices, 8 mm apart 4.0 cm and 4.8 cm above the
orbito-meatal line and in that horizontal plane. The two
slices selected provided optimal information about
gray and white matter of frontal, temporal, parietal and
occipital lobes, internal capsule, thalamus and basal
ganglia. To avoid excessive radiation exposure only
two slices were measured for LCBF and LX values.
The brain stem, cerebellum and upper hemispheric
levels were not measured. Body nitrogen was displaced by inhalation of 100% oxygen for 10 minutes
piror to the CBF measurements. During denitrogenation, 3-4 serial non-contrast scans were made. Three
*The informed consent form used and the protocol for measuring
CBF by the CT xenon contrast method were approved by the Institutional Review Board, Veterans Administration Medical Center, Houston.
VOL 15, No 6, NOVEMBER-DECEMBER
1984
to four xenon contrast scans were obtained between the
2nd and 9th minute of inhalation of 35-37.5% stable
xenon gas mixed with 62.5-65% oxygen. Oxygen in
these concentrations is a mild vasoconstrictor, reducing LCBF values for gray matter by at most 5% and
white matter by considerably less.23 These minimal
vasoconstrictive effects are within the experimental
error of the method which is ± 5%. The xenon mixture was administered through a semi-closed partial
rebreathing system. The rate of increase in alveolar
concentration of xenon gas was carefully controlled so
that gradual increases in alveolar xenon concentration
resulted.
Dupont Tedlar gas sampling bags (Model 130a,
AeroVironment Inc., Pasadena, California 91107)
were used to deliver the gas mixtures. These are made
of Tedlar plastic which is impermeable to xenon gas.
This has proved to be cost-effective, since the unused
portion of the gas remains in the bag and can be used
for later patients.
A gradual build-up of alveolar xenon concentrations
provides optimal curve fitting and minimizes any
subanesthetic effects of xenon gas. Local CT enhancements of the brain during build-up by xenon were
measured in selected regions of interest from small
volumes (80-250 cu mm3) located in homogeneous
gray or white matter. End-tidal xenon gas concentrations were monitored with a Gow-Mac thermoconductivity analyzer. Inspiratory and expiratory gas concentrations were recorded on a polygraph. Since end-tidal
and arterial gas concentration are in equilibrium, these
values were converted to A H changes for blood using
a proportionality constant derived from Kelcz's formula36 and corrected for the patient's hematocrit. The
time consumed while making these measurements is
15-20 minutes at cost of $50 per patient.
LCBF and LX values were calculated by means of a
computer program utilizing least squarefittingof saturation curves for both end-tidal and brain tissue A H
values fitted to infinity. Blood pressure, PECO2,
PEO2, EKG and EEG were concurrently recorded on
the polygraph. Local CT enhancements of the brain by
stable xenon, during inhalation of the gas, were measured as changes in Hounsfield units plotted from a
baseline of 3-4 non-contrast CT scans and the 3 or
more data points measured by the CT scanner during
saturation with the contrast agent. Saturation curves
were then plotted prior to computer analysis. These
were considered satisfactory if they appeared curvilinear and showed deviations of ± 0.5 Hounsfield units or
less derived for 3 or more points. If these criteria were
not met that particular curve was rejected as unsatisfactory and was not analyzed by the computer. Such
rejections occurred in about 20% of all measurements
and were evenly distributed among controls and
patients.
The smoothing of the curves, necessary because of
the low signal to noise ratio is a potential source of
error of the method which could influence LX values in
particular and therefore LCBF values to a lesser degree. Such errors could result in misclassifications of
STABLE XENON, CTCBF IN MID/Kitagawa et al
TABLE 2 Methods Used on Brain Maps for Classifying Reduced
Local Blood Flow and Lambda Values
White matter
Gray matter
LCBF values
60.1->60.1
60-58
57.9-55
54.9-<54.9
LX values
O.8O1->O.8O1
0.80-0.78
0.779-0.75
0.749-<0.749
Points
assigned
0
1
2
3
0
1
2
3
LCBF values
20.1->20.1
20-18
17.9-15
14.9-<14.9
LX values
1.301->1.301
1.30-1.28
1.279-1.25
1.249-< 1.249
Points
assigned
0
1
2
3
0
1
2
3
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
the data by the methods to be described later when
discussing tables 2 and 3.
The volumes or voxels of interest selected for each
measurement measured between 80-250 cu mm derived from what appeared by their appearance on plain
CT scanning, to be composed of homogeneous gray or
white matter. If when sampling gray matter, some
white matter was included by error due to partial volume effects, this became apparent from calculated LX
values, which showed values higher than for normal
gray matter (0.86 ± 0.04). If LA's for gray matter
were excessive this sample was rejected as inhomogeneous, and another voxel was sampled. In practice,
this was rarely a problem, particularly when selecting
homogeneous volumes of white matter, since white
matter of the human brain is usually thicker than corti-
cal gray matter. In other words, for anatomical reasons
partial volume effects were rare when sampling white
matter and could be corrected when sampling gray.
The possibility of errors associated with CTCBF measurements has been reviewed in detail elsewhere.28' "• 38
In order to plot the most common tomographic localizations for severe reductions of LCBF and LX. values measured among the entire series of patients, reduced LCBF and LX values were classified into grades
of severity between 0, 1, 2, and 3 (table 2). Regions
with flow values below 10 ml/100 g brain/min were
seldom encountered and were not included in order to
avoid diffusion errors when measuring LX, values. Total scores for reduced flows and X values for representative regions of the brain were then plotted on composite brain maps as pooled data for all 15 cases. For
example, 3 points were assigned to regions showing
severe reductions of LCBF and LX values, 2 points
were assigned for moderate reductions and 1 point for
mild and zero points for regions having normal LCBF
and LX values. In this age group, normal values for
gray matter LCBF were considered to be 60 ml/lOOg
brain/min or above, as judged from similar measurements in age-matched normal volunteers.28 Values
below 55 ml/lOOg brain/min were considered to be
severely reduced. Normal values for white matter
LCBF were considered to be values above 20 ml/lOOg
brain/min, while those between 10-15 ml/lOOg brain/
min were considered to be severely reduced. Regarding LX values, gray matter values below 0.80 were
considered to be reduced and those below 0.75 were
considered severely reduced. White matter LX values
were considered abnormal if below 1.30 and severely
TABLE 3 Correlation of LCBF Values with MMQ Scores. Correlation Coefficients were Significant between MMQ
Scores and Mean LCBF Values for Left or Right Frontal Cortex, Left or Right Temporal Cortex and Left or Right
Thalamus
Regression
Correlation
Statistical
line
coefficient (r)
significance
N*
y = 0.80x + 46.9
15
0.79
P < 0.01
0.52
y = 0.87x + 46.9
15
P < 0.05
y = 1.06x x 42.5
0.59
15
P < 0.05
N.S.
N.S.
0.10
7
0.32
12
N.S.
N.S.
0.74
y = O.78x + 47.6
12
P < 0.01
y = 1.61x + 32.7
0.58
15
P < 0.05
0.21
N.S.
N.S.
6
11
N.S.
N.S.
0.06
N.S.
0.36
15
N.S.
N.S.
0.50
13
N.S.
0.62
11
y = 0.87x + 45.4
<
P 0.05
N.S.
0.44
9
N.S.
12
N.S.
0.19
N.S.
11
y = 0.80x + 44.9
0.61
<
P 0.05
7
N.S.
0.01
N.S.
15
N.S.
N.S.
0.09
•Number ofregionsof interest examined. Someregionswere excluded for technical reasons, due to head movement or
poor head positioniong.
Region
of interest
Cortical gray matter
Lt. frontal matter
Lt. temporal cortex
Lt. parietal cortex
Lt. occipital cortex
Rt. frontal cortex
Rt. temporal cortex
Rt. parietal cortex
Rt. occipital cortex
Subcortical gray matter
Lt. caudate nucleus
Lt. thalamus
Lt. putamen
Rt. caudate nucleus
Rt. thalamus
Rt. putamen
White matter
1003
1004
STROKE
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
reduced if below 1.25. By pooling the scores for regional reductions, two maps were constructed, one for
reduced LA topography and another for reductions of
LCBF.
Cognitive deficits were quantitatively assessed by
the modification described by Jacobs et al of the Folstein "mini-mental state (MMQ)." This was administered immediately before the CBF test in the majority
of cases and within one week in the remainder. The
validity of this rapid assessment of cognitive mental
deficits has been established in a large series of patients. 3334 They correlate well with Wechsler Adult
Intelligence Scale (WAIS). A score between 11-20
indicates moderate to moderately severe cognitive impairment but with sufficient insight to understand the
test procedure and sign informed consent. They have
considerable advantages over the longer psychological
test batteries. The latter are time-consuming and patients with dementia tend to tire or refuse to cooperate.
The MMQ is designed specifically for organic mental
syndromes and takes only 30 minutes or less to complete. As evaluated in this laboratory the weighting of
the MMQ scale is as follows: Orientation 5 questions,
Attention and Calculation 11 questions, Opposites and
Similarities 5 questions, Memory Registration 6 questions and Memory Consolidation 4 questions. Normal
age-matched volunteers in this laboratory score 29-31
out of a possible 31.
Methods For Data Analysis
Bivariate correlation coefficients were calculated
between MMQ scores and quantitative LCBF values
for each region using the Pearson Product-Moment
analysis. The slope and intercept of the bivariate regression line were also calculated in order to compare
magnitude of effect. Subsequently, a set of correlation
coefficients were also determined between LCBF values and subtests of the MMQ. These included orientation, digit repeating and reversing, calculation,
similarities and tests of memory. Significance of correlations were tested against the t-distribution and statistical significance was set at p < .05.
Regarding the statistical methods used for analyzing
data obtained utilizing the available EMI 1010 scanner
in this hospital, the mean standard deviation for human
VOL 15, No
6, NOVEMBER-DECEMBER
1984
brain slices measured as Hounsfield units during 4
serial control scans measured in gray or white matter
prior to the xenon gas inhalation was ±0.7 Hounsfield
units for regions of interest 80 cu mm or larger. During
xenon inhalation of mixtures of 35-37.5% xenon the
measured A H increases were between 5.5 to 8.5
H.U., provided there was no movement of the head.
LA and LCBF values were calculated by the use of a
single compartment double-integration program and a
DEC 10 computer. This was carried out for each one of
multiple regions of interest selected from two adjacent
brain sections. Two or more representative LCBF and
LA values were pooled to provide the data for each of
the anatomical regions of interest for patients and normal volunteers listed in tables 2 and 3.
This laboratory has accumulated CTCBF measurements among 245 patients and normal volunteers over
the past 6 years. These data have been analyzed blindly
and at different times. The data were computed and
analyzed first among the normal volunteers without
knowledge of results in MID, Alzheimer's disease,
cases with both (MIX) and dementia of other types
such as normal pressure hydrocephalus, etc. Later data
from MID patients were computed and analyzed without knowledge of values for age-matched controls.
Later data from the two groups were compared.
Regions most affected by minor head movements
were usually located in frontal and occipital cortex. If
such minor head movement occurred, these data points
were discarded as already described. However, the
same technical problems were found to exist for both
patients and normal controls, so that the numbers of
discarded data points were similar in both groups and
observer bias is considered unlikely.
Results
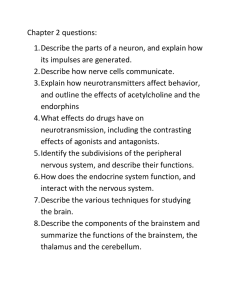
Confirmation Of Regional Anatomical Patterns Of
Infarction In MID
Figure 1 illustrates a composite brain map displaying the topography for pooled local A values among the
group of 15 right-handed patients with MID. Moderately to severely reduced LA values are seen in the
thalamus bilaterally, both caudate nuclei, both putamenal nuclei, the left, mid- and inferior temporal corti-
C O M P O t m MAIN MAP Or POOLID LOCAL LAMBDA VALUU M 1t PUOXT HAHOfD
PATHNT* WITH MM.TMWAHCT DCHZHTU TO SHOW UOIONAL AHATOWC MTTDWS
OF IMFAUCTION*
FIGURE 1. Multiple infarcts as evidenced by
decreased Lk values were most commonly distributed in the thalamus bilaterally, both basal
ganglia, both temporal cortices plus the left
internal capsule and the right cingulate cortex.
STABLE XENON, CTCBF IN MID/Kitagawa et al
1005
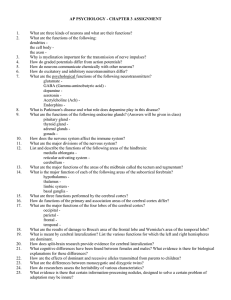
COMPOSITE MAIN HAP OF POOLED LOCAL C«F VALUES IW 11 RK3HT HANDED PATIENTS
WITH HULT1—MFAftCT DEMENTIA TO SHOW MOIONAL ANATOMIC PATTERNS OF
FUHCT1OMAL ISCHEMIA
UwlMlon
FIGURE 2. Reduced LCBF patterns were
measured in the thalamus bilaterally, both basal ganglia, both temporal cortices, the left inferior frontal cortex and the left parietal
cortex.
Severely
Reduced
Moderately
Reduced
'• •---I Reduced
•
Borderline
Reduced
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
ces, the right superior and mid-temporal cortex, the
right cingulate cortex, the left internal capsule and left
frontal white matter. Mildly reduced LX values are also
present in the right fronto-temporal white matter.
These regions of reduced X values are distributed bilaterally and in a patchy manner typical of lacunar
infarcts.31 They confirm the anatomical sites of multiple cerebral infarctions or zones of reversible ischemia
which were sometimes (but not always) apparent as
low density lesions by plain CT scanning.31
Regional Anatomic Patterns Of Functional Ischemic
Impairment
Figure 2 displays a composite brain map illustrating
the most common sites of reduced LCBF values derived from pooled data for the entire series of 15 patients with MID. Moderately or severely reduced flow
patterns are seen in the,fhalamus bilaterally, both caudate nuclei, both lenticular nuclei, the left superior
temporoparietal cortex, the left inferior temporal cortex, plus the right superior and right mid-temporal
cortex and the left inferior frontal cortex. Reductions
of LCBF are patchy, bilateral in every case and, in
general, follow the territorial distribution of both middle cerebral arteries.
Correlation of LCBF Values With Different Cognitive
Functions As Judged By MMQ Subtests
Significant correlation coefficients between LCBF
values and MMQ subtests categorized according to the
different cognitive performances tested are presented
in table 4. Left mid-temporal flow reductions correlated with both dyscalculia and memory disturbances.
Reduced flow values of both frontal lobes correlated
with disorientation to time and place and with attention
as tested by repeating and reversing digits and days of
the week. The functional contribution of the thalamus
to cognitive performance seems to be a broad one as
judged by correlation of reduced thalamic LCBF values correlated with MMQ testing. Correlations of
thalamic LCBF reductions were significant for impaired calculating ability, problems with attention in
repeating and reversing digits, reversing days of the
week plus inability to judge and name similarities and
opposites.
Correlation Between MMQ Scores And
Left And Right Temporal Cortex LCBF Values (N=3O)
70
Correlation Of LCBF Reductions With The Severity Of
Dementia
Table 3 correlates mean LCBF values for different
regions with the pooled mean MMQ scores. The severity of dementia correlated directly with reductions of
LCBF values for cortical gray matter (r = 0.79, p <
0.01) but not for hemispheric white matter. There were
no correlations between MMQ scores and reductions
of LCBF values in the caudate and lenticular nuclei.
Direct correlations were found between reduced MMQ
scores and reduced gray matter flow values measured
bilaterally for thalamus and fronto-temporal cortical
regions. Correlation coefficients were significant between mean MMQ scores and mean LCBF values for
left (r = 0.52, p< 0.05) or right (r = 0 . 7 4 , p < 0 . 0 1 )
frontal cortex, left (r = 0.59, p < 0.05) or right (r =
0.58, p < 0.05) temporal cortex and left (r = 0.62, p
< 0.05) or right (r = 0.61, p < 0.05) thalamus (figure
3 and 4).
so
o •••-L«M r-0.59. P< 0.05
• — n g M r-Q58.p<0.05
40
T
w
15
20
MMO Scor.
FIGURE 3. Significant correlations were observed between
mean MMQ scores and LCBF values for both left and right
temporal cortex.
STROKE
1006
Correlation Between MMQ Scores And
Left And Right Thatamus LCBF Values (N=22)
70
s
60
E
o
•
50
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
10
IS
L«« r-(l62.p<0.05
Right r - a e i , p < 0 . 0 5
20
MMO Score
FIGURE 4. Significant correlations were seen between MMQ
scores and left and right thalamus.
Discussion
It is now generally agreed that CBF is reduced in
patients with organic dementia. Regarding average
CBF values, O'Brien and Mallet12 and Hachinski, et
al14 reported significantly lower CBF values in patients
with MID compared to patients with SDAT whereas
Ingvar and Gustafson" reported CBF reductions to be
about equal in both forms of dementia. Others have
obtained results showing that CBF reductions in both
MID and SDAT correlate well with the degree of dementia. 1020 Regarding regional flow patterns, Obrist,
et al'° and Ingvar, et al18 using the intra-arterial carotid
bolus 133Xe method reported local CBF reductions in
fronto-temporal regions in SDAT. Yamaguchi, et al20
reported patchy bilateral reductions of CBF in patients
with MID utilizing the l33Xe inhalation method.
VOL 15, No
6, NOVEMBER-DECEMBER
1984
Computerized reconstruction techniques now make
it possible to render images of the brain in three dimensions. Benson, et al39 using PET scanning reported
little or no decrease in CMR glucose in patients with
MID compared to normal subjects, possibly due to
enhanced anaerobic glycolysis. However, studies by
Frackowiak, et al40 with oxygen-15 showed that rCBF
and rCMR0 2 were markedly depressed in both parietal
regions in patients with vascular dementia. Kuhl41 reported scattered asymmetric defects in glucose metabolism in MID. These minor discrepancies reported
from PET scanning may be attributed to the relatively
poor resolution (circa 1 cu cm) of the method, a disadvantage common to all isotope methods, plus a paucity
of cases studied. Current measurements of both LA. and
LCBF in patients with MID made by the CTCBF method provide better resolution with more accurate estimates of zones of low flow. Present observations are
consistent with earlier reports from this laboratory.
Meyer, et al31-42 and Tachibana, et al43 reported multifocal reductions of LCBF in MID with abnormally
large coefficients of variation compared to similar
measurements in SDAT or in age-matched normals.
In considering flow values below which functional
disorder may be expected, values below 55 ml/lOOg
brain/min for gray matter and below 15 ml for white
matter were noted to be associated with cognitive disorders in the present study. These values at which
symptoms appear are about 20% below those for agematched normal values.43 Methodological and temporal differences in the measurements of LCBF explain
why flow values reported here are higher than critical
values associated with neurological deficits in acute
experimental studies utilizing implanted hydrogen
electrodes.44-45 The present series of patients with MID
were allowed to recover from the acute stage of the
most recent infarct before LCBF measurements were
made, which permits some restoration of CBF to the
ischemic areas. Some neurologic and cognitive recovery did occur in some patients, so that some vascular
lesions in MID are reversible. Present resolution of
TABLE 4 Correlation of LCBF Values with MMQ Subtests which Assess Different Cognitive Performances. Reduced
LCBF Values in the Left Mid-temporal Cortex Correlated with Both Dyscalculia and Memory Disturbances. Low Values
in Both Frontal Lobes Correlated with Disorientation to Time and Place
Cognitive performance tested
Orientation
Repeating and reversing digits
and days of the week
Calculation
Similarities and opposites
Memory
Anatomical significant
variables
(ROI's)
Rt.
Rt.
Lt.
Rt.
Rt.
Lt.
Lt.
Lt.
Rt.
Rt.
Rt.
Rt.
Rt.
Lt.
cingulate cortex
frontal cortex
frontal cortex
cingulate cortex
frontal cortex
frontal cortex
thalamus
mid-temporal cortex
thalamus
frontal cortex
sup. temporal cortex
thalamus
temporal cortex
mid-temporal cortex
Correlation
coefficients
0.76
0.73
0.56
0.83
0.77
0.76
0.62
0.65
0.63
0.62
0.81
0.70
0.56
0.63
Statistical
significance
p < 0.05
p < 0.05
p < 0.05
p < 0.01
p < 0.01
p < 0.01
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p < 0 05
p < 0.05
p < 0.05
STABLE XENON, CTCBF IN MID/Kitagawa et al
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
CTCBF method utilizing the 8 mm collimator is 80 cu
mm, whereas implanted hydrogen electrodes can detect flow changes in regions of 1 cu mm.45 Patients
with MID reported here had suffered from their ischemic episodes over a relatively long time interval (over
a mean interval of approximately seven years). Chronic lesions may be expected to develop some collateral
circulation so that despite persistent functional impairment the flow values are higher than when measured in
the acute stages of cerebral infarction.31 In longitudinal
follow-up some of our MID cases have shown regions
of reversible ischemia with improvement of both
MMQ and CBF values which again confirms that some
ischemic lesions in MID are reversible.
In MID, LCBF values were consistently reduced
bilaterally in fronto-temporal cortex and subcortical
gray matter and the severity of these reductions correlated with cognitive impairments. Reduced LX values
indicate the anatomical site of infarctional or ischemic
damage. They are not as useful for making functional
correlations as reductions of LCBF values. LCBF values are known to be reduced when there are clinical
signs of neurological impairment in the absence of
permanent changes of LX values. The functional neurological disorders correlated with reduced LCBF values whether the flow reductions were due to primary
ischemia, infarctions or secondary to diaschisis.23-31
The patchy distribution of bilateral ischemic lesions
as judged by the map of decreased LA. values is consistent with the topography of hypertensive and lacunar
infarcts in the distribution of the middle cerebral artery
as reported at autopsy.'"7 Reduction in LA. values in
recent ischemia are due to local edema and in old
infarcts are due to gliosis which are also associated
with low density lesions on plain CT scanning.46 Studies in animal models by CT xenon enhancement have
shown that in acute, subacute and chronic infarction,
in regions where X values were redued by 10-30 percent, edema followed later by tissue necrosis and gliosis with cystic degeneration was evident. In chronic
lesions there were necrotic nerve cells, lipid-laden
macrophages, gliosis, and revascularization.46 Reduction of X values in acute ischemia was due to dilution of
lipids by water, and in chronic cerebral ischemia was
attributed to replacement of normal brain lipids by
neutral fats and gliotic tissue that show less solubility
for xenon. Xenon is reported to have a Bunsen coefficient of 1.7 in oil at 37° C and 0.085 in water at 37° C
with an oil-water ratio of 20. 4? Xenon solubility in
water or spinal fluid is low, with near zero values.
Short inhalation intervals of'Xe may be insufficient to
evaluate true X's especially in diseased areas with low
perfusion. However, the computer program described
here estimates LA. values extrapolated to saturation at
infinity provided LCBF is not below 10 ml/lOOg brain/
min.46
Ladurner, et al8 also reported composite topographic
maps of sites of cerebral infarction noted by plain CT
scanning in patients with vascular dementia. These
maps of low density CT lesions observed in MID are
similar to the present topography of reduced LX val-
1007
ues. The main areas affected in both studies were the
basal ganglia, thalamus and sylvian cortex bilaterally.
The common involvement of the thalamus in MID
patients appeared to be an important determinant of
dementia in both these studies.
The effect of one or more strokes on intelligence
varies as a function of location and extent of the infarction. Present results are in agreement with Tomlinson,
et al1 who correlated their clinical and neuropathological observations in MID. They concluded that occasionally when the total quantity of destroyed brain
tissue was not large, dementia might still be manifested during life if important parts of the brain were
destroyed. These authors did not specify which parts of
the brain were important in terms of cognitive function
other than to mention that they appeared to be in the
distribution of the middle cerebral artery.
The present study confirms that apart from the anatomical correlates of infarction in patients with MID
discussed above, impairment of function in the thalamus bilaterally together with functional disturbance in
the cortical distribution of both middle cerebral arteries
are important determinants of dementia. While bilateral lesions are necessary, functional impairments within
the left temporal cortex appear to play an important
role in right handed subjects. Correlation with MMQ
subtests suggests that low LCBF values for the left
mid-temporal cortex, correlate both with dyscalculia
and memory disturbance and that bilateral frontal impairments contribute to disorientation to time and place
and to impaired attention. Thalamic ischemia appears
to result in overall cognitive blunting.
Baer, et al15 also working in this laboratory, utilized
a large battery of psychometric tests, including the
Wechsler-Adult Intelligence Scale and reported significant correlations between the severity of dementia
and mean LCBF values for frontal, temporal and parietal cortex measured by the l33Xe method. This method
does not measure flow values in deep brain structures
nor permit detailed functional and anatomic cognitive correlations. The CTCBF methods appear to
make possible detailed and quantitative correlations
between brain topography and function with statistical
reproducibility.
Within the limitations and constraints imposed by
measurements of limited horizontal sections of the
brain, present results suggesting that the thalamus is
important to cognitive function is not new. Two patterns of dementia have been proposed, a cortical type
and a subcortical type.48-49 Cortical dementia is characterized by dysphasia, amnesia and global intellectual
deficits but without motor, sensory or affective symptoms which are frequently present in SDAT patients.
The concept of subcortical dementia has been based on
behavioral syndromes reported in patients with prominent pathological changes in subcortical gray matter.
These behavioral syndromes include emotionality and
personality change, memory disorders, defective ability to manipulate newly acquired knowledge, and slowing of information processing. Such syndromes were
frequently present in our MID patients and presumably
STROKE
1008
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
would be acceptable as examples of subcortical dementia. Emotional incontinence is described as one of
the common features included as one criterion in the
Hachinski index and aphasic disturbances are also
common, although they were excluded in the present
study, if severe.
Subcortical dementia has been reported in degenerative,50 vascular and neoplas'tic lesions of the thalamus
and basal ganglia. Guberman et al51 reported bilateral
paramedian thalamic lacunar infarctions associated
with subcortical dementia, with characteristic clinical
and CT features.
Bilateral lesions of the ventrolateral nucleus of the
thalamus are associated with modest reductions in
scores on the Wechsler Adult Intelligence Scale.49
In general, observations from clinico-pathologic
and stereotaxic studies support the hypothesis that
thalamo-corticolimbic projection systems participate
in cognitive functioning.52'" While the present results
support the view that MID constitutes an additional
etiology of subcortical "dementia," overt multi-infarct dementia requires additional lesions of frontal and
temporal cortex. This is consistent with the view that
both cortical and subcortical systems are involved in
dementia either directly or by disconnection of projection systems.54
Acknowledgment
We wish to acknowledge the assistance of Dr. John Thornby, biostatlstician, VA Medical Center and Baylor College of Medicine in data
analysis and Richard E. Dowell, Jr., M.A. for technical assistance.
Mrs. Julie E. Link processed the manuscript.
References
1. Tomlinson BE, Blessed G, Roth M: Observations of the brains of
demented old people. J Neural Sci 11: 205-242, 1970
2. Kay DWK, Foster EM, McKennie AA, Roth M: Mental illness and
hospital usage in the elderly. Compr Psychiatry 11: 26-35, 1970
3. BroeGA, AkhtarGR: Neurologic disorders in the elderly at home.
J Neurol 39: 362-366, 1976
4. Tower DB: Alzheimer disease — senile dementia and related disorders. Neurological Status. In: Katzman R, Terry RO, Bick KL
(eds.) Alzheimer's disease: senile dementia and related disorders
(Aging, Vol. 7) Raven Press, New York, 1-4, 1978
5. Hachinski VC, LassenNA, Marshall J: Multi-infarct dementia — a
cause of mental deterioration in the elderly. Lancet 2: 207-209,
1974
6. Rosen WG, Terry RD, Fuld PA, Katzman R, Peck A: Pathological
verification of ischemic score in differentiation of dementia. Ann
Neurol 7: 486-488, 1980
7. Fisher CM: Lacunar strokes and infarcts: A review. Neurology 32:
871-876, 1982
8. Ladumer G, Iliff LD, Sager WD, Lechner H: A clinical approach
to vascular (multi-infarct) dementia. In: Meyer JS, Lechner H,
Reivich M (eds): Cerebral Vascular Disease: Eleventh International Salzburg Conference, 1982, Amsterdam. Excerpta Medica,
236-243, 1983
9. Lassen NA, Munck O, Tottery ER: Mental function and cerebral
oxygen consumption in organic dementia. Arch Neurol Psychiatry
77: 126-133, 1957
10. Obrist WD, Chivian E, Cronqvist S, IngvarDH: Regional cerebral
blood flow in senile and presenile dementia. Neurology 20: 315322, 1970
11. Ingvar DH, Gustafson L: Regional cerebral blood flow in organic
dementia with early onset. Acta Neurol Scand 46 (Suppl 43): 4273, 1970
12. O'Brien MD, Mallett BL: Cerebral cortex perfusion rates in dementia. J Neurol Neurosurg Psychiatry 33: 497-500, 1970
VOL 15, No 6, NOVEMBER-DECEMBER 1984
13. Simard D, Olesen J, Paulson OB, Lassen NA, Skinhoj E: Regional
cerebral blood flow and its regulation in dementia. Brain 94: 273288, 1971
14. Hachinski VC, Iliff LP, Zilhka E, et al: Cerebral blood flow in
dementia. Arch Neurol 32: 632-637, 1975
15. Baer PE, Faibish GM, Meyer JS, Mathew NT, Rivera VM: Neuropsychological correlates of hemispheric and regional cerebral
blood flow in dementia. In: Meyer JS, Lechner H, Reivich M
(eds.): Cerebral Vascular Disease. Seventh International Conference Salzburg. Georg Thieme Publishers, Stuttgart, 100-106,
1976
16. Perez FL, Mattew NT, Stump DA, Meyer JS: Regional cerebral
blood flow statistical patterns and psychological performance in
multi-infarct dementia and Alzheimer's disease Canad J Neurol
Sci 4: 53-62, 1977
17. Meyer JS: Improved method for nomnvasive measurement of regional cerebral blood flow by l33Xe inhalation: Part II. Measurements in health and disease. Stroke 9: 205-210, 1978
18. Ingvar DH, Brun A, Hagberg B, Gustafson L: Regional cerebral
blood flow in the dominant hemisphere in confirmed cases of
Alzheimer's disease, Pick's disease, and multi-infarct dementia:
Relationship to clinical symptomatology and neuropathological
findings. In: Katzman R, Terry RD, Bick KL (eds.). Alzheimer's
disease: senile dementia and related disorders (Aging, Vol 7),
Raven Press, New York, 203-211, 1978
19. Obrist WD: Cerebral circulatory changes in normal aging and dementia. In: Hoffmeister F, Muller C (eds.): Brain Function in Old
Age: Bayer Symposium VII, Springer Verlag, 278-287, 1979
20. Yamaguchi F, Meyer JS, Yamamoto M, Sakai F, ShawT Nomnvasive regional cerebral blood measurements in dementia. Arch
Neurol 37: 410-418, 1980
21. Butler RW, Dickinson WA, Katholi C, Halsey JH: The comparative effects of organic brain disease on cerebral blood flow and
measured intelligence. Ann Neurol 13: 155-159, 1983
22. Lenzi GL, Jones T, Frackowiak RSJ: Positron emission tomography: State of the art in neurology. Prog Nucl Med 7: 118-137,
1981
23. Phelps ME, Mazziotta JC, Huang S: Study of cerebral function
with positron computed tomography. J Cereb Blood Flow Metabol
2: 113-162, 1982
24. Meyer JS, HaymanLA, Yamamoto M, Sakai F, NakajimaS: Local
cerebral blood flow measured by CT scan after stable xenon inhalation. Am J Neuroradiol 1: 213-225, 1980
25. Meyer JS, Hayman LA, AmanoT, et al' Mapping local blood flow
of human brain by CT scanning during stable xenon inhalation.
Stroke 12: 426-436, 1981
26. Sakai F, Gotoh F, Ebihara S, Kitagawa Y, Hata T, Takagi Y,
Komagamine M: Xenon enhanced CT method for the measurement
of local cerebral blood flow in man. J Cereb Blood Flow Metabol 1:
29-30, 1981
27. Ono H, Ono K, Mori K: Mapping of CBF distribution by dynamic
Xe-enhanced CT scan method. J Cereb Blood Flow Metabol 1: 5051, 1981
28. Amano T, Meyer JS, Okabe T, Shaw T, Mortel KF: Stable xenon
CT cerebral blood flow measurements computed by a single compartment — double integration model in normal aging and dementia. J Comput Assist Tomogr 6: 923-932, 1982
29. Gur D, Wolfson SK, Yonas H, et al: Progress in cerebrovascular
disease: local cerebral blood flow by xenon enhanced CT. Stroke
13: 750-758, 1982
30. Segawa H, Wakai S, Tamura A, Yoshimasu N, Nakamura O, Ohta
M: Computed tomographic measurement of local cerebral blood
flow by xenon enhancement. Stroke 14: 356-362, 1983
31. Meyer JS, Okayasu H, Tachibana H, Okabe T: Stable xenon CT
CBF measurements in prevalent cerebrovascular disorders
(Stroke). Stroke IS: 80-90, 1984
32. Ackerman RH: Of cerebral blood flow, stroke and SPET. Stroke
15: 1-4, 1984
33. Jacobs JW, Bernhard MR, Delgado A, Strain JJ: Screening for
organic mental syndromes in the medically ill. Ann Intern Med 86:
40-46, 1977
34. Folstein MF, Folstein SE, McHugh PR: "Mini-mental state" A
practical method for grading the cognitive state of patients for the
clinician. J Psychiat Res 12: 189-198, 1975
35. Rosenberg GA, Komfeld M, Stoning J, Bicknell JM: Subcortical
STABLE XENON, CTCBF IN MID/Kitagawa et al
36
37.
38.
39.
40.
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
41.
42.
43.
arteriosclerotic encephalopathy (Bingwanger): Computerized tomography. Neurology 29: 1102-1106, 1979
Kelcz F, Hilal SK, Hartwell P, Joseph PM: Computed tomographic
measurement of the xenon brain-blood partition coefficient and
implications for regional cerebral blood flow: A preliminary report.
Radiol 127: 385-392, 1978
Rottenberg DA, LuHC, Kearfott KJ: The in vivo autoradiographic
measurement of regional cerebral blood flow using stable xenon
and computerized tomography: The effects of tissue heterogeneity
and computerized tomography noise. J Cereb Blood Flow Metabol
2: 173-178, 1982
Gur D, Shabason L, Wolfson SK, Yonas H, Good WF: Measurement of local cerebral blood flow by xenon-enhanced computerized
tomography imaging: A critique of an error assessment. J Cereb
Blood How Metabol 3: 133-135, 1983
Benson D, Kuhl D, Phelps M, Cummings JL, Tsia SY: Positron
emission computed tomography in the diagnosis of dementia. Ann
Neurol 10: 76, 1981
FrackowiakRSJ.PozzilliC, Legg NJ, DuBoulayGH, Marshall J,
Lenzi GL, Jones T: Regional cerebral oxygen supply and utilization in dementia. A clinical and physiological study with oxygen15 and positron tomography. Brain 104: 753-778, 1981
Kuhl DE: The effects of aging and stroke on patterns of local
cerebral glucose utilization. In: Reivich M (ed.): Cerebrovascular
Disease. Thirteenth Princeton Conference. Raven Press, New
York, pp 19-27, 1983
Meyer JS, Shaw T, Okayasu H, Tachibana H: Multi-infarct and
Alzheimer dementias differentiated from normal aging by xenon
contrast CT-CBF measurements. J Cereb Blood Flow Metabol 3
(Suppl 1): S506-S507, 1983
Tachibana H, Meyer JS, Okayasu H, Shaw T, Kandula P, Rogers
RL: Xenon contrast CT-CBF scanning of the brain differentiates
44.
45
46
47
48
49
50.
51
52.
53.
54
1009
normal age related changes from multi-infarct dementia (MID) and
senile dementia of Alzheimer type (SDAT). J Gerontol 1984, (in
press)
Jones TH, Morawetz RB, Crowell RM, et al: Thresholds of focal
cerebral ischemia in awake monkeys. J Neurosurg 54: 773-782,
1981
Heiss WD: Progress in cerebrovascular disease. Flow thresholds of
functional and morphological damage of brain tissue. Stroke 14:
329-331, 1983
Meyer JS, Yamamoto M, Hayman LA, Sakai F, Nakajima S,
Armstrong D: Cerebral embolism. Local CBF and edema measured
by CT scanning and Xe> inhalation. Neurol Res 2: 101-126, 1980
Cullen SC, Gross EG: The anesthetic properties of xenon in animals and human beings with additional observations on krypton.
Science 133: 580-582, 1951
Albert ML. Subcortical dementia. In: Katzraan R, Terry RD, Bick
KL (eds.): Alzheimer's disease: senile dementia and related disorders (Aging, Vol 7) Raven Press, New York, 173-180, 1978
Riklan M, Levita E: Subcortical correlates of human behavior.
Williams & Wilkins, Baltimore, 1969
Albert ML, Feldman RG, Willis AL: The subcortical dementia of
progressive supranuclear palsy. J Neurol Neurosurg Psychiatry 37:
121-130, 1974
Guberman A, Stuss D: The syndrome of bilateral paramedian thalamic infarction. Neurology 33: 540-546, 1983
Fedis P, Van Buren JM: Memory and perceptual deficits during
electrical stimulation in the left and right thalamus and parietal
subcortex. Brain Lang 2: 78-100, 1975
Brown JW. Language, cognition and the thalamus. Confin Neurol
36: 33-60, 1974
MayeuxR, Stern Y, Rosen J, Benson F. Is "subcortical dementia"
a recognizable clinical entity? Ann Neurol 14: 278-283, 1983
Headache in Cerebrovascular Disease
RUSSELL K. PORTENOY, M . D . , * t CHRISTOPHER J. ABISSI, M . D . , t RICHARD B. LIPTON, M . D . , * t
ALAN R. BERGER, M . D . , * t MARK F. MEBLER, M . D . , t JENNY BAGLIVO, P H . D . , 1
AND SEYMOUR SOLOMON, M . D . * t
SUMMARY Two hundred fifteen consecutive patients with cerebrovascular events were evaluated prospectively for the incidence and characteristics of headache. Of 163 patients able to communicate, headache
occurred in 29% with bland infarcts, 57% with parenchymal hemorrhage, 36% with transient Lschemic
attacks and 17% with lacunar infarcts. Patients with a history of recurrent throbbing headache were
significantly more likely to have headache, usually throbbing in quality, during the present illness. Women
developed headache significantly more often than men. Headache began prior to the vascular event in 60%
of patients and at its onset in 25%. The quality, onset and duration of the headache varied widely among
patients.
Headache in cerebrovascular disease is common, though neither its occurrence nor characteristics
predict lesion type or location. Though the pathogenesis of the headache is unknown, its association with
prior throbbing headache suggests that similar factors may operate in both.
Stroke Vol 15, No 6, 1984
HEADACHE occurs commonly in cerebrovascular
disease. Numerous reports have evaluated headache in
patients with ischemic stroke,1"7 cerebral embolism, 2 ' x*• *-'' intracerebral hemorrhage2-3- '• 12~14 and
transient ischemic attacks.' 12 ' " • l 6 Headache incidence
From the Department of Neurology,* the Headache Unit.t and the
Department of Biostatistics,:t Montefiore Medical Center and Albert
Einstein College of Medicine. Address correspondence to: Dr. Seymour
Solomon, Department of Neurology, Montefiore Medical Center, 111
East 210th Street, Bronx, New York 10467.
Received March 15, 1984; revision # 1 accepted May 29, 1984.
has varied widely in these series, in part due to differences in patient sampling. Most studies are limited by
the problems inherent in the evaluation of transitory
symptoms with a retrospective chart review. No prospective study has determined the incidence and characteristics of headache in a single population with such
diverse lesions as lacunar and hemispheric infarcts,
transient ischemic attacks and parenchymal hemorrhages. In addition, very few surveys have attempted
to relate a history of headache to complaints of pain
during the acute event.
CT-CBF correlations of cognitive deficits in multi-infarct dementia.
Y Kitagawa, J S Meyer, H Tachibana, K F Mortel and R L Rogers
Stroke. 1984;15:1000-1009
doi: 10.1161/01.STR.15.6.1000
Downloaded from http://stroke.ahajournals.org/ by guest on October 1, 2016
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1984 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/15/6/1000
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click Request
Permissions in the middle column of the Web page under Services. Further information about this process is
available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/