Standard PDF - Wiley Online Library
advertisement

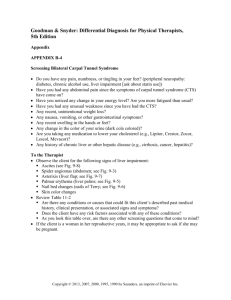
Fate of Extrahepatic Human Stem and Precursor Cells After Transplantation into Mouse Livers Marc Brulport,1,2 Wiebke Schormann,1,2 Alexander Bauer,1,2 Matthias Hermes,1,2 Carolin Elsner,1,2 Friedrich Jakob Hammersen,1,2 Walter Beerheide,3 Dimitry Spitkovsky,4 Wolfgang Härtig,5 Andreas Nussler,6 Lars Christian Horn,7 Jeanett Edelmann,8 Oliver Pelz-Ackermann,9 Jörg Petersen,10 Manja Kamprad,11 Marc von Mach,12 Amelie Lupp,13 Henryk Zulewski,14* and Jan G. Hengstler1,2* In recent years, a large number of groups studied the fate of human stem cells in livers of immunodeficient animals. However, the interpretation of the results is quite controversial. We transplanted 4 different types of human extrahepatic precursor cells (derived from cord blood, monocytes, bone marrow, and pancreas) into livers of nonobese diabetic/severe combined immunodeficiency mice. Human hepatocytes were used as positive controls. Tracking of the transplanted human cells could be achieved by in situ hybridization with alu probes. Cells with alu-positive nuclei stained positive for human albumin and glycogen. Both markers were negative before transplantation. However, cells with alu-positive nuclei did not show a hepatocyte-like morphology and did not express cytochrome P450 3A4, and this suggests that these cells represent a mixed cell type possibly resulting from partial transdifferentiation. Using antibodies specific for human albumin, we also observed a second human albumin–positive cell type that could be clearly distinguished from the previously described cells by its hepatocyte-like morphology. Surprisingly, these cells had a mouse and not a human nucleus which is explained by transdifferentiation of human cells. Although it has not yet been formally proven, we suggest horizontal gene transfer as a likely mechanism, especially because we observed small fragments of human nuclei in mouse cells that originated from deteriorating transplanted cells. Qualitatively similar results were obtained with all 4 human precursor cell types through different routes of administration with and without the induction of liver damage. Conclusion: We observed evidence not for transdifferentiation but instead for a complex situation including partial differentiation and possibly horizontal gene transfer. (HEPATOLOGY 2007;46:861-870.) Abbreviations: CYP3A4, cytochrome P450 3A4; DAB, 3,3⬘-diaminobenzidine; NOD, nonobese diabetic; PAS, periodic acid Schiff; RAG-2, recombination activation gene-2; SCID, severe combined immunodeficiency; uPA, urokinase plasminogen activator. From the 1Leibniz Research Centre for Working Environment and Human Factors, Dortmund, Germany, and 2Center for Toxicology, Institute of Legal Medicine and Rudolf-Boehm Institute of Pharmacology and Toxicology, University of Leipzig, Leipzig, Germany; 3Siam Life Science, Limited, Suriyawong Bangrak, Bangkok, Thailand; 4Institute for Vegetative Physiology, University of Cologne, Cologne, Germany; 5Department of Neurochemistry, Paul Flechsig Institute for Brain Research, University of Leipzig, Leipzig, Germany; 6Fresenius Biotech GmbH, Bad Homburg, Germany; 7Institute of Pathology, Division of Gynaecopathology, University of Leipzig, Leipzig, Germany; 8Institute of Legal Medicine, 9Laboratory of Molecular Medicine, Interdisciplinary Centre for Clinical Research, University of Leipzig, Leipzig, Germany; 10Heinrich Pette Institute for Experimental Virology, University of Hamburg, Eppendorf, Hamburg, Germany; 11Institute of Clinical Immunology, University of Leipzig, Leipzig, Germany; 12II Medical Department, University of Mainz, Mainz, Germany; 13Institute of Pharmacology and Toxicology, Friedrich Schiller University, Jena, Germany; 14Division for Endocrinology, Diabetes and Clinical Nutrition, Department of Research, University Hospital Basel, Basel, Switzerland. Received December 13, 2006; accepted March 26, 2007. Supported by the Federal Ministry of Education and Research funding priority HepatoSys (31P3131) and by the Interdisciplinary Centre for Clinical Research at the University of Leipzig (01KS9504, project Z10). *Jan G. Hengstler and Henryk Zulewski share senior authorship. Address reprint requests to: Marc Brulport, Leibniz Research Centre for Working Environment and Human Factors, Ardeystraße 67, D-44139 Dortmund, Germany. E-mail: brulport@ifado.de; or Henryk Zulewski, Division for Endocrinology, Diabetes and Clinical Nutrition, Department of Research, University Hospital Basel, Hebelstraße 22, CH-4031 Basel, Switzerland. E-mail: zulewskih@uhbs.ch. Copyright © 2007 by the American Association for the Study of Liver Diseases. Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/hep.21745 Potential conflict of interest: Nothing to report. Supplementary material for this article can be found on the HEPATOLOGY Web site (http://interscience.wiley.com/jpages/0270-9139/suppmat/index.html). 861 862 I BRULPORT ET AL. n recent years, numerous reports described the generation of hepatocytes or “hepatocyte-like” cells from various types of extrahepatic stem or precursor cells.1,2 At first glance, this appears to provide exciting new opportunities for cell therapy, as some types of stem cells proliferate efficiently in vitro and therefore may help to generate a larger supply of human hepatocytes or precursor cells for transplantation. On the other hand, some studies presenting far-reaching conclusions with respect to the capacity of stem cell therapy have not yet been reproduced or may have been interpreted in an overly optimistic manner. The first evidence that hematopoietic stem cells might be capable of differentiating into hepatocytes in rodents came from Petersen et al.3 Similar results were obtained in further studies using different animal models and purified cell types for transplantation (for a review, see Hengstler et al.1). Later, it was recognized that cell fusion and not transdifferentiation was responsible in the FAH⫺/⫺ mouse model.4-6 However, other authors using different mouse models with less severe selection pressure did not observe evidence for cell fusion.7-9 Therefore, this matter is still discussed controversially. The intriguing results obtained in rodents stimulated many groups to study the fate of human stem and precursor cells in livers of experimental animals (Supplemental Table 1; for a review, see Hengstler et al.1). Recipients were mostly immunodeficient severe combined immunodeficiency (SCID) or nonobese diabetic (NOD)/SCID mice. Although different cell types and routes of injection have been tested, qualitatively similar results have been reported (Supplemental Fig. 1). All 18 published studies observed either human albumin–positive or HepPar1 (a human hepatocyte antigen) -positive hepatocyte-like cells. Most of these studies confirmed their results by reverse transcriptase (RT)-PCR. Here we analyzed in detail the human albumin–positive cells observed in mouse livers after human precursor cell transplantation. A new aspect of our study is the combination of cell tracking techniques and marker analysis in the same cells. Using this technique, we consistently observed 2 different types of human albumin–positive cells after the transplantation of human cord blood cells. The first cell type, named type 1, has a human nucleus. However, its morphology is not hepatocyte-like. Some but not all of the analyzed hepatocyte markers were positive. Type 2 has a perfect hepatocyte-like morphology similar to that of the cells shown in Supplemental Fig. 1. Surprisingly, however, type 2 cells had a mouse nucleus and not a human nucleus. Qualitatively similar results were obtained when the experiments were reproduced with dif- HEPATOLOGY, September 2007 ferent types of human precursor cells, namely bone marrow stem cells, monocyte-derived cells, and hepatopancreatic precursor cells. Therefore, no clear transdifferentiation of human precursor cells to hepatocytes was observed, but instead a complex situation was observed that may include partial transdifferentiation and horizontal gene transfer. Materials and Methods Cells and Culture Conditions. The isolation of human adherently proliferating cord blood cells,10 human monocyte– derived NeoHep cells,11 nestin-positive hepatopancreatic precursor cells,12,13 mesenchymal bone marrow cells,14 and primary human hepatocytes15 was performed as described (for a detailed description, see the supplementary material). Marking with CM-DiI was performed with a commercially available kit (Invitrogen, Karlsruhe, Germany). Transplantation into NOD/SCID and Urokinase Plasminogen Activator (uPA)/Recombination Activation Gene-2 (RAG-2) Mice. Male NOD/SCID or uPA/ RAG-2 mice, 8-12 weeks old,16 were used. Cells (750,000) suspended in 100 L of a culture medium were transplanted directly either into the left liver lobe11 or into the spleen. A detailed description of the transplantation procedure and preparation of the liver is given in the supplementary material. Immunostaining, In Situ Hybridization, and Histological Standard Staining Techniques. For immunohistochemical detection of human albumin antihuman albumin rabbit antiserum (Abcam; diluted 1:1000 in a solution of 0.3% bovine serum albumin in a tris-buffered saline) and the commercially available ABC kit (Vector Laboratories, Burlingame, CA) were used. For in situ hybridization, fluorescein-labeled alu probes (BioGenex, San Ramon, CA) and digoxigenin-labeled major mouse satellite DNA (a gift from Dr. O. Brüstle) were used. Prussian blue staining, periodic acid Schiff (PAS) staining, and Solanum tuberosum lectin staining standard protocols were used to detect iron deposition, glycogen, and endothelial cells, respectively. Combined in situ hybridization (using alu probes) and immunostaining and standard histological staining techniques were performed on the same slices to analyze hepatocyte marker expression in alu-positive cells. Detailed descriptions of all techniques are given in the supplementary material. Duplex PCR for the Detection of Human DNA in a Mouse Background. A recently published protocol for the quantification of small amounts of human DNA in mouse tissues was applied.17 The technique is based on primers specific for the ␣-satellite repeat of human chro- HEPATOLOGY, Vol. 46, No. 3, 2007 mosome 7 and primers amplifying fragments from the mouse chromosome 8 gene repeat sequence. Product ratios are determined by the standard electrophoresis of end-stage PCR reactions. Microsatellite Analysis for Human Identification. DNA was extracted from the cord blood cell lines before transplantation and from formalin-fixed and paraffin-embedded tissue of mouse livers 3 weeks after transplantation as described.18 For PCR amplification, we used the PowerPlex16 Kit (Promega, Madison, WI), which contained the following short tandem repeat loci: D3S1358, TH01, D21S11, D18S51, PentaE, D5S818, D13S317, D7S820, D16S539, CSFPO, PentaD, VWA, D8S1179, TPOX, FGA, and amelogenin. All resulting PCR products were resolved and detected by capillary electrophoresis (for details, see the supplementary material). Results Characterization of Human Stem and Precursor Cells. Most of our transplantation experiments were performed with adherently proliferating cord blood cells.10 Therefore, we characterized our cells by surface marker analysis (Supplemental Fig. 2A). The pattern of surface marker expression was very similar to that obtained in a previous study using adherently proliferating cord blood cells.7 For instance, CD10, CD13, CD29, CD90w, CD105, and CD144 were positive, whereas CD31 and CD34 did not differ from isotype controls (Supplemental Fig. 2A). All other cell types were handled according to published procedures and have already been extensively characterized in the indicated references: human monocyte– derived NeoHep cells,11,19 human hepatopancreatic precursor cells,12,13 and mesenchymal bone marrow stem cells.14 Cord blood, hepatopancreatic, and mesenchymal stem cells had a fibroblast-like morphology (Supplemental Fig. 2B,C). In contrast, NeoHep cells (Supplemental Fig. 1D) appeared to be large, round cells interspersed with a smaller number of spindle-shaped cells, as described by Ruhnke et al.11,19 Cord blood, hepatopancreatic, and mesenchymal cells were negative for albumin and cytochrome P450 3A4 (CYP3A4) immunostaining; iron storage was evidenced by Prussian blue staining, glycogen storage by PAS staining. Endothelial cells were detected using S. tuberosum lectin staining (Supplemental Fig. 3). For all transplantation experiments, freshly isolated primary human hepatocytes were used as positive controls. Tracking of the Transplanted Cells in Mouse Livers. The cell types described in the previous paragraph were transplanted into NOD/SCID mice: 750,000 cells were injected directly into the left liver lobe. A first milestone ana- BRULPORT ET AL. 863 lyzing the fate of the human cells in the mouse livers was the tracking of the transplanted cells. As positive controls, primary human hepatocytes were transplanted. Using probes for alu sequences, we could clearly identify human hepatocytes by in situ hybridization in a mouse liver microenvironment (Fig. 1). Human nuclei were visualized by green fluorescence and showed a morphology and size characteristic of human hepatocytes. For the staining of mouse nuclei, a mouse major satellite probe was applied that led to characteristic pink spots within the nuclei of mouse hepatocytes (Fig. 1). Combined in situ hybridization using alu probes and mouse major satellite probes also allowed the identification of cell fusion by the presence of green and pink nuclei in the same cell. As expected, no evidence for cell fusion was observed after the transplantation of human hepatocytes. In situ hybridization with alu probes was combined with immunostaining using antibodies specific for human albumin. This technique identified human cells (by the green fluorescence of the nuclei) that additionally showed a positive albumin staining [visualized by 3,3⬘-diaminobenzidine (DAB) staining], a scenario that should be expected after the transplantation of human hepatocytes (Supplemental Fig. 4). Having obtained plausible results for our positive controls, the primary human hepatocytes, we next studied adherently proliferating human cord blood cells, using similar techniques. We also observed alu-positive cells 1 day to 3 weeks after the transplantation of cord blood cells (shown later in Figs. 2 and 4). However, the alu-positive nuclei were much smaller than those of human hepatocytes (Fig. 1 and Supplemental Fig. 4) and showed an angular shape. Small clusters of alu-positive cells were often found in vessels. Because of the morphological differences from human hepatocytes, we performed additional controls to analyze whether the alu-positive cells were derived from the transplanted cord blood cells: 1. Before transplantation, cord blood cells were marked with the red fluorescent dye CM-DiI. After transplantation, red fluorescent structures were observed (Fig. 2A) that colocalized with the alu-positive nuclei (Fig. 2B). 2. Using a panel of 16 short tandem repeats for the forensic identification of individuals, we analyzed 1 of our cord blood cell lines before transplantation (Supplemental Fig. 5A) and mouse livers 3 weeks after transplantation with this cell line (Supplemental Fig. 5B and Supplemental Table 3). For all markers, we typed identical alleles. With the application of forensic standards, human DNA in the mouse liver could be shown to derive from the same individual whose cord blood cells had been established. The probability of compliance was more than 99.9%. Next, we performed a semiquantitative analysis of alupositive nuclei in the left liver lobe 4 hours, 12 hours, 24 864 BRULPORT ET AL. HEPATOLOGY, September 2007 Fig. 1. Identification of human and mouse nuclei by in situ hybridization. Slides were incubated with both alu probes (green fluorescence, human nuclei) and mouse major satellite probes (pink spots, mouse nuclei). (A) NOD/SCID mouse liver, (B) human liver, and (C) NOD/SCID mouse liver after the transplantation of 750,000 human hepatocytes into the left liver lobe. Part C shows the section of the left liver lobe with the highest density of human cells. The scale bar is 50 m. hours, 5 days, and 21 days after transplantation. For this purpose, we counted alu-positive structures; for instance, the 2 cell clusters in Fig. 2B were counted as 1 alu-positive structure (Table 1). We observed an increase between 4 and 12 hours after transplantation, which could be explained by the redistribution of cell pools. Later, a decrease was observed, and only a relatively small fraction of alu-positive cell clusters remained 3 weeks after transplan- Fig. 2. Tracking of human cord blood cells 1 day after transplantation into the left liver lobe of NOD/SCID mice. The cord blood cells were labeled by the red fluorescent dye CM-DiI before transplantation and were additionally visualized by in situ hybridization using an alu probe (green fluorescence). The red fluorescence visualizes CM-DiI (A). Human nuclei were identified with a human-specific alu probe and visualized with a Cy2-labeled antibody (green fluorescence). Overlay of red and green fluorescence together with 4⬘,6-diamidino-2-phenylindole nuclear staining (blue) to verify the colocalization of nuclei with alu probe– positive structures (B). The scale bar is 50 m. tation. To confirm these results by an independent method, we applied a recently established duplex PCR technique that allows the quantification of human DNA in a mouse background.17 These results confirmed the decrease already seen with in situ hybridization. Nevertheless, human DNA still was detectable 21 days after transplantation (Supplemental Table 4). Two Different Types of Human Albumin–Positive Cells. We applied an immunostaining technique with antibodies specific for human albumin (Fig. 3A-D). Much care was taken to establish conditions that minimized false positive results in mock-transplanted mice (Supplemental Table 5 and Supplemental Fig. 6). Using this technique, we consistently observed human albumin–positive cells after the transplantation of cord blood cells (Fig. 3A). However, 2 types of human albumin– positive cells could be differentiated. One cell type (named type 1 cell) does not resemble human hepatocytes (Fig. 3A1,A2). Nuclei of type 1 cells appear smaller than those of hepatocytes and have an angular shape. Type 1 cells usually occur as cell clusters, are often located in small vessels, and do not form columnar structures that are typical for hepatocytes. A second cell type (named type Table 1. Numbers of alu-Positive Structures 4 Hours, 12 Hours, 24 Hours, 5 Days, and 21 Days After the Transplantation of 750,000 Human Cord Blood Cells into the Left Liver Lobe of NOD/SCID Mice Removal of Transplanted Liver After After After After After 4 hours 12 hours 24 hours 5 days 21 days Number of Analyzed Slices Mice per Group alu-Positive Nuclei (Mean) Standard Error 8 8 10 7 8 3 3 3 3 4 78.4 118.1 233.1 37.4 2.6 19.6 22.1 63.3 12.0 1.2 HEPATOLOGY, Vol. 46, No. 3, 2007 BRULPORT ET AL. 865 Fig. 3. Two morphologically different types of human albumin–positive cells were observed 3 weeks after the transplantation of cord blood cells, monocyte-derived cells, hepatopancreatic precursor cells, or bone marrow– derived stem cells into the left liver lobe of NOD/SCID mice. Immunostaining was performed with antibodies specific for human albumin. Sections from human liver served as positive controls, and sham-transplanted NOD/ SCID mouse livers were used as negative controls. Twenty-one days after transplantation, type 2 cells showed a morphology similar to that of genuine hepatocytes. In contrast, type 1 cells did not have a hepatocyte-like morphology. The scale bar in A1, A2, B1, B3, B4, C1, C4, D1, and D3 is 20 m; in B2, it is 50 m; and in E and F, it is 100 m. 2 cell) has an hepatocyte-like morphology (Fig. 3A3,A4). Type 2 cells often show 2 nuclei and are well integrated into the liver tissue. However, they usually occur as single cells and, therefore, never form liver tissue. Results similar to those for cord blood cells were obtained after the transplantation of monocyte-derived cells (NeoHep cells), hepatopancreatic precursor cells, and bone marrow– derived mesenchymal stem cells (Fig. 3B-D). Combined Cell Tracking and Marker Analysis Reveals Type 1 Cells as Partially Differentiated Stem Cells. In the next step, we combined the tracking techniques with CM-DiI and alu-probe in situ hybridization with an analysis of hepatocyte markers in the same cells. For this purpose, mouse livers 3 weeks after the transplantation of CM-DiI–marked cord blood cells were immunostained with human albumin–specific antibodies followed by in situ hybridization with alu probes of the same slices. A representative result of human albumin– positive type 1 cells is shown in Fig. 4C. The CM-DiI cell tracker (Fig. 4E,F) and in situ hybridization (Fig 4D,F) demonstrate that the human albumin–positive cluster of type 1 cells consists indeed of the transplanted human cells. Therefore, the hepatocyte marker albumin that is negative in cord blood cells before transplantation (Supplemental Fig. 3A) becomes expressed after transplantation into the liver microenvironment. A similar procedure was applied for PAS staining to analyze whether type 1 cells stored glycogen (Supplemental Fig. 7). Indeed, type 1 cells were characterized by a colocalization of PAS-positive staining (Supplemental Fig. 7D) in cells with alu- positive nuclei (Supplemental Fig. 7E). Therefore, glycogen is another marker newly expressed after transplantation. However, not all analyzed hepatocyte markers were positive in type 1 cells. For instance, alu-positive type 1 cells stained negative for CYP3A4, the major cytochrome P450 in human liver (Supplemental Fig. 8). In our negative controls for immunostaining, we observed cell clusters with a cauliflower-like, brownish cytoplasmatic stain (Supplemental Fig. 9). These brownish structures occurred independently of the first and secondary antibodies and were absent in mock-transplanted mice. They are relevant from a technical point of view because an inexperienced operator might misinterpret them as positive DAB staining. To elucidate the nature of the brownish inclusions, we performed several histological routine staining techniques and finally identified some type 1 cells as Prussian blue–positive; this suggested that these cells store iron. Supplemental Fig. 10 demonstrates the colocalization of Prussian blue (Supplemental Fig. 10D) with CM-DiI–positive and alu-positive nuclei (Supplemental Fig. 10E). However, only those type 1 cells located between hepatocytes stained positive with Prussian blue (Supplemental Fig. 10D,E). We also observed alu-positive CM-DiI cells in the endothelium of vessels (Supplemental Fig. 10G,H). These endothelial type 1 cells stained negative for Prussian blue (Supplemental Fig. 10F), in contrast to some type 1 cells located between hepatocytes (Supplemental Fig. 10D,E). To further characterize endothelial type 1 cells, we used a costaining technique with in situ hybridization plus S. tuberosum lectin; the latter reliably identified endothelial cells of veins (green arrows in 866 BRULPORT ET AL. Supplemental Fig. 11A,B) and sinusoidal lining cells (white arrows in Supplemental Fig. 11A,B). Supplemental Fig. 11C1,C2 shows an alu-positive endothelial type 1 cell, which at first glance seems to resemble the host’s endothelial cells. However, a closer examination by confocal microscopy reveals a lectin-negative cytoplasm (the yellow arrow in Supplemental Fig. 11C4), in contrast to the lectin-positive genuine endothelial cells of the host (the white arrows in Supplemental Fig. 11C4). Therefore, endothelial type 1 cells do not perfectly match the staining pattern of real endothelial cells. In conclusion, our combined tracking/marker analysis technique leads to a preliminary classification of type 1 cells (Table 2) that is in agreement with a partial but not complete differentiation of cord blood cells into endothelial cells and hepatocytes. In particular, the difference between albumin-positive type 1 cells and real hepatocytes is obvious because of differences in the morphology and marker expression. To analyze whether type 1 cells are apoptotic or proliferate, we performed double stainings of the same slices with alu-probe in situ hybridization plus either ki67 immunostaining or TUNEL staining. The results show that both apoptosis (Supplemental Fig. 12) and proliferation (Supplemental Fig. 13) are very rare in type 1 cells. Human Albumin–Positive Type 2 Cells Have a Mouse Nucleus but Not a Human Nucleus. At first glance, type 2 cells (examples are shown in Fig. 3A3,A4) seem to be promising because of their hepatocyte-like morphology and clear-cut positive human albumin staining. On the other hand, we feel that these cells should be interpreted with caution because our in situ hybridization experiments with alu probes (Fig. 2B) did not show alupositive nuclei that would match the nuclei of type 2 cells. Therefore, we decided to study human albumin–positive type 2 cells in detail and performed consecutive in situ hybridization with alu probes and mouse major satellite probes followed by albumin immunostaining. A representative result (Fig. 5) shows a typical type 2 cell staining positive with antibodies specific for human albumin. The DAB (human albumin) -positive cell in Fig. 5C appears darker than that in Fig. 5D in comparison with the surrounding DAB negative cells. This is due to the fact that DAB quenches fluorescence. Nevertheless, the DAB-positive cell could be shown as mouse major satellite–positive (Fig. 5D). In contrast, in situ hybridization with alu probes was negative (Fig. 5E). Therefore, the cell shown in Fig. 5 has a mouse nucleus but not a human nucleus, despite positive staining for human albumin. A positive control with human liver that underwent exactly the same procedure showed clear-cut alu-positive nuclei (Supplemental Fig. 4). We carefully evaluated several type 2 cells (further examples are shown in Supplemental Fig. 14) but never could demonstrate intact human nuclei. In a mi- HEPATOLOGY, September 2007 nority of type 2 cells, small alu-positive fragments (Supplemental Fig. 15) were visible. In addition, dye transfer from transplanted CM-DiI–marked cord blood cells into mouse hepatocytes was observed (Supplemental Fig. 16). A possible relevance of alu-positive fragments and dye transfer is addressed in the Discussion section. Selection Pressure and Different Routes of Administration: Qualitatively Similar Results. All experiments shown so far were obtained in NOD/SCID mice without the induction of a selection advantage for the transplanted cells. In these experiments, human cells were injected directly into the left liver lobe. It should be considered that this procedure causes substantial local liver damage (Supplemental Fig. 17) but no specific selection advantage. To study a possible influence of selection pressure, we used uPA/RAG-2 mice20-22 that suffered from permanent deterioration of hepatocytes. Human cord blood cells (750,000 per mouse) were transplanted into uPA/RAG-2 mice. Transplantations were performed intrasplenically or by direct injections into the left liver lobes using three mice per group. Qualitatively, similar observations were made as already described for NOD/ SCID mice (Supplemental Fig. 18) for both routes of administration. There seemed to be quantitative differences. However, the latter were not systematically addressed in this study. Discussion The limited availability of hepatocytes has been recognized as the major hurdle of liver cell therapy.2 A wider use of liver cell therapy will not be possible until adequate numbers of functional cells for transplantation become more readily available. Although the most relevant cytokines for liver regeneration are known, human hepatocytes cannot yet be stimulated to proliferate efficiently in vitro.23,24 Also, the generation of functional hepatocytes from human oval cells is not yet possible. Therefore, several groups have tried to differentiate specific types of extrahepatic stem and precursor cells into hepatocytes (for a review, see Hengstler et al.1). A strategy for the evaluation of the differentiation capacity of human stem cells is transplantation into the livers of immunodeficient animals and analysis of whether previously silent human hepatocyte markers become expressed. This approach offers the advantage of a real liver microenvironment. A disadvantage may be the human-in-mouse situation with possible interspecies incompatibilities. However, human and monkey hepatocytes have been shown to survive and remain functional in livers of immunodeficient mice.20-22 Therefore, the fate of human stem cells in mouse livers may give some evidence of their hepatocellular differentiation capacity. HEPATOLOGY, Vol. 46, No. 3, 2007 BRULPORT ET AL. 867 Fig. 4. Combined analysis of human albumin expression, CM-DiI cell tracker, and in situ hybridization with alu probes of the same slice. The left liver lobe of a NOD/SCID mouse was analyzed 3 weeks after the transplantation of human cord blood cells. Consecutive immunostaining with antibodies specific for human albumin (C) and in situ hybridization with alu probes (D). Red fluorescence visualizes the position of the cell tracker CM-DiI because cord blood cells have been CM-DiI–marked before transplantation (E). The merged picture (F) demonstrates that the cluster of human albumin–positive type 1 cells (C) colocalizes with CM-DiI–positive cells and with alu-positive nuclei. A human liver slice was used as a positive control for in situ hybridization (A) and in immunohistochemistry (B1), whereas sham-transplanted NOD/SCID mouse liver served as a negative control (B2). The scale bar is 100 m in A and B and 50 m in C-F. A large number of groups have transplanted human extrahepatic stem and precursor cells into immunodeficient animals (for an overview, see Supplemental Table 1). Interestingly, very similar results have been obtained after transplantation, that is, hepatocyte-like cells expressing human albumin or the human hepatocyte antigen HepPar1. The impressive consistency between the results of different groups is illustrated in Supplemental Fig. 1, in which we collected representative published images of mouse livers after the transplantation of human stem and precursor cells. However, the interpretation of these observations is quite controversial (for a review, see Hengstler et al.1). Several authors tend to give an optimistic Table 2. Classification of Cell Types Observed in Livers of NOD/SCID Mice After the Transplantation of Extrahepatic Human Precursor Cells Type 1 Cells ● Alu-positive (human) nuclei, mouse major satellite staining negative ● No hepatocyte-like morphology (small angular nuclei) ● Expression of human albumin, positive PAS (glycogen) staining ● No expression of CYP3A4 ● Accumulation of iron in some type 1 cells 3 Probably result of partial transdifferentiation Type 2 Cells ● Mouse major satellite–positive (mouse) nuclei, no alu-positive (human) nuclei ● Perfect hepatocyte-like morphology ● Expression of human albumin ● No accumulation of iron Fig. 5. Representative example of a human albumin–positive type 2 cell that has a mouse nucleus but no human nucleus. Consecutive albumin immunostaining and in situ hybridization with alu probes and mouse major satellite probes were performed with slices of the left liver lobe of a NOD/SCID mouse 3 weeks after the transplantation of human cord blood cells. The immunostaining visualized a human albumin–positive type 2 cell (C). The same cell proved negative for in situ hybridization with an alu probe (E) but was positive with a mouse major satellite probe (D), as indicated by the yellow arrow. Human (A) and sham-transplanted (B) NOD/SCID mouse liver tissue slices were used as positive controls. The scale bar is 50 m. 868 BRULPORT ET AL. view. For instance, Kogler et al.7 transplanted adherently proliferating cells isolated from human cord blood into livers of fetal sheep. The authors observed the expression of albumin and human hepatocyte–specific antigen after transplantation and concluded that the human cord blood cells differentiated into human parenchymal hepatic cells. Newsome et al.25 demonstrated the expression of the HepPar1 human hepatocyte–specific antigen and concluded that cells from human cord blood “become mature hepatocytes” in livers of NOD/SCID mice. Ishikawa et al.26 detected human albumin and the HepPar1 antigen in livers of immunodeficient mice, postulating that the engrafted cells from human cord blood “functioned as hepatocytes.” However, other scientists10,13,27,28 (for a review, see Hengstler et al.1), including our group, remained skeptical because we observed the expression of some but not all hepatocyte markers that should be expressed by a real human hepatocyte. Because of its high relevance, we decided to study more closely the fate of human stem cells in mouse livers. For this purpose, we established cell tracking techniques that reliably allow the identification of the transplanted cells and additionally hepatocyte marker analysis in the same cells. In our study, efficient tracking of transplanted human cells could be achieved by a combination of in situ hybridization with alu probes and marking of the cells with CM-DiI before transplantation. The results obtained with this technique correlated well with data obtained from a duplex PCR technique quantifying human DNA in a mouse background. In comparison with the data 4 and 24 hours after transplantation, a strong decrease in the number of surviving human cells from cord blood was obtained after 21 days (Table 1). Nevertheless, a sufficient number of the transplanted cord blood cells survived (median: 2.6 alupositive structures per slice) to allow a combined analysis of alu-probe in situ hybridization and hepatocyte markers. Indeed, alu-positive cells were also positive for human albumin and for PAS staining, indicating glycogen storage. Importantly, both markers were negative in cord blood cells before transplantation. Therefore, exposure to the liver microenvironment caused expression of at least 2 previously silent hepatocyte markers. However, the alupositive cells did not show a hepatocyte-like morphology. Their nuclei are much smaller than the large, round nuclei of hepatocytes. Moreover, they stained negative for CYP3A4, the major cytochrome P450 in human hepatocytes. This scenario suggests that the transplanted cells have a mixed phenotype that might be explained by partial differentiation. The resulting mixed cell type is not implausible if we consider the molecular mechanisms controlling gene expression. The somatic stem and precursor cells, torn out from their physiological surround- HEPATOLOGY, September 2007 ings and introduced into a new microenvironment, are likely to be stimulated to express some previously silent genes. However, because the transplanted cell types represent somatic and not embryonic stem cells, the local accessibility of genes to the transcriptional machinery may be limited. For instance, histone modifications determine the accessibility of chromatin and control gene expression patterns29 (for a review, see Gan et al.30). Our results suggest that the mere exposure of somatic stem cells to a liver microenvironment is not sufficient to induce the complex mechanisms (i.e., activation of transcription factors plus establishment of accessible and responsive chromatin) that finally lead to the expression of the several hundreds of genes that make up a hepatocyte. Multistep protocols starting with dedifferentiation steps for the establishment of responsive chromatin by altering the acetylation and methylation patterns possibly may be more successful.11,19,31 Also, promising results have been obtained by multistep protocols for the differentiation of embryonic stem cells into the hepatic lineage.32 Immunostaining for human albumin after the transplantation of human cells into mouse livers showed 2 different types of albumin-positive cells. Type 1 cells have a human nucleus and correspond to the previously described mixed cell types with a non-hepatocyte–like morphology. In contrast, type 2 cells stain positive for human albumin and are characterized by a hepatocyte-like morphology with its characteristic polygonal shape and large, round nuclei. These 2 human albumin–positive cell types were observed consistently after the transplantation of 4 different extracellular precursor cell types used in this study, namely, adherently proliferating cord blood cells, monocyte-derived NeoHep cells, hepatopancreatic precursors, and mesenchymal stem cells from bone marrow. Our type 2 cells correspond perfectly to the human albumin–positive or HepPar1-positive cells in mouse livers observed by several other groups after human stem cell transplantation (Supplemental Fig. 1). At first glance, these cells seem to be promising candidates resulting from a transdifferentiation process. However, by combined in situ hybridization and albumin immunostaining, we have clearly demonstrated that type 2 cells have a mouse nucleus and not a human nucleus (Fig. 5 and Supplemental Fig. 14). Therefore, type 2 cells cannot result from transdifferentiation of the transplanted human stem cells. Cell fusion is improbable because we never observed both a human nucleus and a mouse nucleus in type 2 cells. Although it has not yet been formally proven, we suggest horizontal gene transfer as the most likely mechanism that could explain human albumin–positive type 2 cells. We have shown that the majority of the transplanted human cells deteriorate within 3 weeks. On the other hand, hepatocytes HEPATOLOGY, Vol. 46, No. 3, 2007 are able to recognize and internalize apoptotic cells by means of specific receptors (galactose-specific and mannose-specific receptor, receptor for phosphatidylserine, and asialoglycoprotein receptor) and by cytoskeletal reorganization that allows the engulfment of apoptotic bodies.33,34 The identification of apoptotic cells by hepatocytes is achieved by sugar residues and phosphatidylserine exposed on the surface of apoptotic bodies. In fact, we have observed small fragments of human (alu-positive) nuclear fragments in mouse cells and also have identified dye transfer from the transplanted cells into hepatocytes of the host. This suggests that chromosomal fragments from deteriorating transplanted cells may use apoptotic bodies as a Trojan horse to enter hepatocytes, leading to the expression of some human genes in mouse cells. However, further experiments are needed to prove this hypothesis, such as the transplantation of human stem cells carrying reporter constructs. An unexpected result was the detection of alu-positive cells with an endothelial morphology integrated into the endothelial layer of vessels. S. tuberosum lectin staining, a technique that reliably identifies endothelial cells,35 revealed differences in the staining pattern between alu-positive endothelial-like cells and real endothelial cells of the host, suggesting that an interpretation of transdifferentiation should still be treated with caution. Nevertheless, further studies concerning a possible role of cord blood cells as endothelial cell precursors are indicated. In conclusion, we did not observe transdifferentiation of human extrahepatic stem cells to hepatocytes after transplantation into mouse livers. Instead, we have seen a complex situation including partial transdifferentiation and possibly horizontal gene transfer. Presently, we cannot rule out that the reported limitations might be due to the human-in-mouse situation. Nevertheless, it should be considered that cells capable of horizontal gene transfer may be used as vehicles for gene delivery, for instance, in inherited metabolic liver disease. Acknowledgment: The authors thank Dr. J. Grosche for expert technical assistance with the operation of the confocal microscope. References 1. Hengstler JG, Brulport M, Schormann W, Bauer A, Hermes M, Nussler AK, et al. Generation of human hepatocytes by stem cell technology: definition of the hepatocyte. Expert Opin Drug Metab Toxicol 2005;1:61-74. 2. Nussler A, Konig S, Ott M, Sokal E, Christ B, Thasler W, et al. Present status and perspectives of cell-based therapies for liver diseases. J Hepatol 2006;45:144-159. 3. Petersen BE, Bowen WC, Patrene KD, Mars WM, Sullivan AK, Murase N, et al. Bone marrow as a potential source of hepatic oval cells. Science 1999;284:1168-1170. BRULPORT ET AL. 869 4. Willenbring H, Bailey AS, Foster M, Akkari Y, Dorrell C, Olson S, et al. Myelomonocytic cells are sufficient for therapeutic cell fusion in liver. Nat Med 2004;10:744-748. 5. Vassilopoulos G, Wang PR, Russell DW. Transplanted bone marrow regenerates liver by cell fusion. Nature 2003;422:901-904. 6. Wang X, Montini E, Al-Dhalimy M, Lagasse E, Finegold M, Grompe M. Kinetics of liver repopulation after bone marrow transplantation. Am J Pathol 2002;161:565-574. 7. Kogler G, Sensken S, Airey JA, Trapp T, Muschen M, Feldhahn N, et al. A new human somatic stem cell from placental cord blood with intrinsic pluripotent differentiation potential. J Exp Med 2004;200:123135. 8. Harris RG, Herzog EL, Bruscia EM, Grove JE, Van Arnam JS, Krause DS. Lack of a fusion requirement for development of bone marrow-derived epithelia. Science 2004;305:90-93. 9. Schwartz RE, Reyes M, Koodie L, Jiang Y, Blackstad M, Lund T, et al. Multipotent adult progenitor cells from bone marrow differentiate into functional hepatocyte-like cells. J Clin Invest 2002;109:12911302. 10. Beerheide W, von Mach MA, Ringel M, Fleckenstein C, Schumann S, Renzing N, et al. Downregulation of beta2-microglobulin in human cord blood somatic stem cells after transplantation into livers of SCID-mice: an escape mechanism of stem cells? Biochem Biophys Res Commun 2002; 294:1052-1063. 11. Ruhnke M, Ungefroren H, Nussler A, Martin F, Brulport M, Schormann W, et al. Differentiation of in vitro-modified human peripheral blood monocytes into hepatocyte-like and pancreatic islet-like cells. Gastroenterology 2005;128:1774-1786. 12. Eberhardt M, Salmon P, von Mach MA, Hengstler JG, Brulport M, Linscheid P, et al. Multipotential nestin and Isl-1 positive mesenchymal stem cells isolated from human pancreatic islets. Biochem Biophys Res Commun 2006;345:1167-1176. 13. von Mach MA, Hengstler JG, Brulport M, Eberhardt M, Schormann W, Hermes M, et al. In vitro cultured islet-derived progenitor cells of human origin express human albumin in severe combined immunodeficiency mouse liver in vivo. Stem Cells 2004;22:1134-1141. 14. Pittenger MF, Martin BJ. Mesenchymal stem cells and their potential as cardiac therapeutics. Circ Res 2004;95:9-20. 15. Hengstler JG, Utesch D, Steinberg P, Platt KL, Diener B, Ringel M, et al. Cryopreserved primary hepatocytes as a constantly available in vitro model for the evaluation of human and animal drug metabolism and enzyme induction. Drug Metab Rev 2000;32:81-118. 16. Petersen J, Dandri M, Gupta S, Rogler CE. Liver repopulation with xenogenic hepatocytes in B and T cell-deficient mice leads to chronic hepadnavirus infection and clonal growth of hepatocellular carcinoma. Proc Natl Acad Sci U S A 1998;95:310-315. 17. Pelz O, Wu M, Nikolova T, Kamprad M, Ackermann M, Egger D, et al. Duplex polymerase chain reaction quantification of human cells in a murine background. Stem Cells 2005;23:828-833. 18. Legrand B, Mazancourt P, Durigon M, Khalifat V, Crainic K. DNA genotyping of unbuffered formalin fixed paraffin embedded tissues. Forensic Sci Int 2002;125:205-211. 19. Ruhnke M, Nussler AK, Ungefroren H, Hengstler JG, Kremer B, Hoeckh W, et al. Human monocyte-derived neohepatocytes: a promising alternative to primary human hepatocytes for autologous cell therapy. Transplantation 2005;79:1097-1103. 20. Dandri M, Lutgehetmann M, Volz T, Petersen J. Small animal model systems for studying hepatitis B virus replication and pathogenesis. Semin Liver Dis 2006;26:181-191. 21. Dandri M, Burda MR, Zuckerman DM, Wursthorn K, Matschl U, Pollok JM, et al. Chronic infection with hepatitis B viruses and antiviral drug evaluation in uPA mice after liver repopulation with tupaia hepatocytes. J Hepatol 2005;42:54-60. 22. Petersen J, Burda MR, Dandri M, Rogler CE. Transplantation of human hepatocytes in immunodeficient UPA mice: a model for the study of hepatitis B virus. Methods Mol Med 2004;96:253-260. 870 BRULPORT ET AL. 23. Michalopoulos GK, DeFrances M. Liver regeneration. Adv Biochem Eng Biotechnol 2005;93:101-134. 24. Michalopoulos GK, DeFrances MC. Liver regeneration. Science 1997; 276:60-66. 25. Newsome PN, Johannessen I, Boyle S, Dalakas E, McAulay KA, Samuel K, et al. Human cord blood-derived cells can differentiate into hepatocytes in the mouse liver with no evidence of cellular fusion. Gastroenterology 2003; 124:1891-1900. 26. Ishikawa F, Drake CJ, Yang S, Fleming P, Minamiguchi H, Visconti RP, et al. Transplanted human cord blood cells give rise to hepatocytes in engrafted mice. Ann N Y Acad Sci 2003;996:174-185. 27. Sharma AD, Cantz T, Richter R, Eckert K, Henschler R, Wilkens L, et al. Human cord blood stem cells generate human cytokeratin 18-negative hepatocyte-like cells in injured mouse liver. Am J Pathol 2005;167:555-564. 28. Aurich I, Mueller LP, Aurich H, Luetzkendorf J, Tisljar K, Dollinger MM, et al. Functional integration of hepatocytes derived from human mesenchymal stem cells into mouse livers. Gut 2007;56:405– 415. 29. Mateescu B, England P, Halgand F, Yaniv M, Muchardt C. Tethering of HP1 proteins to chromatin is relieved by phosphoacetylation of histone H3. EMBO Rep 2004;5:490-496. HEPATOLOGY, September 2007 30. Gan Q, Yoshida T, McDonald OG, Owens GK. Concise review: epigenetic mechanisms contribute to pluripotency and cell lineage determination of embryonic stem cells. Stem Cells 2007;25:2-9. 31. Schmittwolf C, Kirchhof N, Jauch A, Durr M, Harder F, Zenke M, et al. In vivo haematopoietic activity is induced in neurosphere cells by chromatin-modifying agents. EMBO J 2005;24:554-566. 32. Kania G, Blyszczuk P, Jochheim A, Ott M, Wobus AM. Generation of glycogen- and albumin-producing hepatocyte-like cells from embryonic stem cells. Biol Chem 2004;385:943-953. 33. Dini L, Pagliara P, Carla EC. Phagocytosis of apoptotic cells by liver: a morphological study. Microsc Res Tech 2002;57:530-540. 34. McVicker BL, Tuma DJ, Kubik JA, Hindemith AM, Baldwin CR, Casey CA. The effect of ethanol on asialoglycoprotein receptor-mediated phagocytosis of apoptotic cells by rat hepatocytes. HEPATOLOGY 2002;36:1478-1487. 35. Betz T, Teipel J, Koch D, Hartig W, Guck J, Kas J, et al. Excitation beyond the monochromatic laser limit: simultaneous 3-D confocal and multiphoton microscopy with a tapered fiber as white-light laser source. J Biomed Opt 2005;10:054009.