The American Osteopathic
Association
presents
The
Building Blocks of Medicine
Webinar Series
Building Blocks of Medicine
Part I, Session One
An Introduction to Health Insurance
Jennifer Searfoss, J.D., C.M.P.E
Objectives
• What is health insurance?
– Understanding the lingo
• Medicare program overview
• What is a contract?
– Scope of an agreement
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Setting the Foundation
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
What is Health Insurance?
• An agreement between a beneficiary and an
insurance company to protect against paying
the “full cost” of medical services.
–
–
–
–
Beneficiary agrees to pay a premium each moth
Beneficiary agrees to a deductible
Beneficiary agrees to copayments for services
Beneficiary may agree to stay in a certain network
for services to be covered
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
“Health” is Broad
• Insurance usually falls into three categories
– Medical
– Dental
– Vision
• Other policies available to cover long-term
health needs for unskilled nursing, home
health and/or hospice care.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Understanding the Lingo
PREMIUM: Amount paid by the beneficiary as a
lump sum or periodic installments to compensate the
insurer for bearing the risk of a payout.
DEDUCTIBLE: A specified amount that the
beneficiary must pay before the insurer will pay a claim.
COPAYMENT: A payment made by the beneficiary
in addition to that made by an insurer.
COINSURANCE: The deductible and copayment
amounts combined that are the financial responsibility
of the beneficiary.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Understanding the Lingo
BENEFICIARY: The insured person. For most
insurance, this includes the policy holder and all
dependents (spouse, children) on the policy. For
Medicaid, each individual is the policy-holder.
INSURER: States license health insurance carriers.
Administrative Services Only: This is employer-based
coverage where the employer bears the risk. Insurance
companies only administer the network and process claims.
This falls under federal jurisdiction. State law does not apply.
Fully Insured: This is self-insured and small business policies
where the insurance company bears the risk. State law applies.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
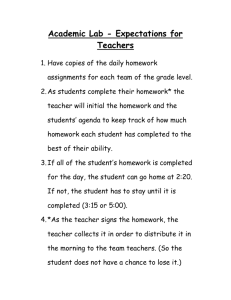
An Example:
Exchange Products
Plan Type
Monthly Premium Range
Typical
Deductible
Coinsurance
Max outof-pocket
Age 20
Age 64
Bronze
$68-150
$320-707
$5,000
70%
$6,350
Silver
$106-171
$499-806
$2,000
80%
$6,350
Gold
$121-205
$571-967
$0
80%
$6,350
Platinum
$171-181
$806-853
$0
90%
$6,350
Catastrophic
$93-135
$6,350
100%
$6,350
(up to age 30)
All sample figures are for single coverage. Amounts for families would be double.
Sample premium rates from Montgomery County, Maryland for non-smokers.
All plans have to cover a wide range of benefits.
Lower-income enrollees in exchanges are eligible for reduced cost-sharing.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Medicare Overview
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Parts of Medicare
• Part A (hospital insurance)
– Medicare Part A helps cover inpatient care.
– Most people do not pay for Medicare Part A coverage.
• Part B (medical insurance)
– Medicare Part B helps cover doctors’ services and outpatient
hospital care.
– Most people pay a monthly premium for Medicare Part B.
• Part C (managed care; “Medicare Advantage”)
– HMO contracts offered in 1982. 1.6 million benes enrolled by 1992.
– Part C established by Congress in 1997 (BBA). First offered as HMO in
1998 and revised in 2003 (MMA) as insurers exited market.
– Today, over 20 percent Medicare benes enrolled in MA plans.
– If entitled to Part A and enrolled in Part B, beneficiaries eligible to
switch to a MA plan, if in service area.
– Some plans have a monthly premium; may include Part D benefit.
• Part D (prescription drug coverage)
– Created in 2003 as part of the MMA. Coverage began Jan. 1, 2006.
– Monthly premium or included in Part C benefit.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
2014 Medicare Coinsurance
• Part A: Most people don’t pay a premium.
– If a person didn’t quality and wishes to purchase
Part A coverage, the monthly premium is up to
$426 each month.
• $1,216 deductible for each benefit period
– Days 61-90: $304 coinsurance per day of each
benefit period
– Days 91 and beyond: $608 coinsurance per each
"lifetime reserve day" after day 90 for each benefit
period (up to 60 days over your lifetime).
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
2014 Medicare Coinsurance
• Part B: Beneficiaries may have Medigap plans
to help pay for these costs (separate premium).
– $104.90 monthly premium
– $147.00 deductible
– 20% copayment
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Medicare Payment Systems
• Medicare Part A
–
–
–
–
Hospital (prospective payment system)
Nursing Home (prospective payment system)
Home Health (prospective payment system)
Hospice (prospective payment system)
• Medicare Part B
– Hospital outpatient (prospective payment system)
– Physician services (RBRVS)
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Other Payment Systems
• Ambulatory surgical centers
• Specialty facilities not included in the payment
system for other acute care hospitals
•
•
•
•
– Psychiatric facilities, cancer hospitals, children’s
hospitals, long-term care hospitals, inpatient
rehabilitation facilities
Clinical laboratories
Ambulance services
Dialysis for patients with end-stage renal disease
Special payments for rural hospitals
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Outpatient Hospital Payment
• The hospital outpatient payment system is also a PPS whereby
hospitals receive a fixed payment called an ambulatory payment
classification (APC) for a specific procedure.
• Unlike the inpatient system, if multiple procedures are
performed, the hospital may be eligible to receive more than one
APC payment per outpatient admission.
– OPPS runs on a calendar year basis (Jan. 1 – Dec. 31).
• Services include ED visits, diagnostic procedures (needle
biopsies, mammograms) and surgeries (knee repair).
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
What Are APCs?
• OPPS payments are based on the APC system, which
divides outpatient services into approximately 750
groups.
• The services within each APC group are clinically
similar and require comparable services.
• CMS bundles services and items (drugs, supplies)
associated with primary procedure.
• Each APC is assigned a relative weight based on the
median cost of the services within the APC.
• Exception: Some services are temporarily assigned to
“new technology” APCs. These services are too new to
be represented elsewhere in the outpatient PPS.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Payments under the OPPS
Payment = APC weight x Conversion factor x
Wage index + Add-on payments
Conversion
factor
Coverts weight into dollar amounts
Wage index Accounts for geographic variation in hospitals’ labor
costs (applied only to labor portion of rate)
Add-ons
Pass through payments for new drugs and devices for
2 to 3 years, outlier payments for high-cost services,
outlier payments for high-cost services, hold harmless
payments for certain hospitals, transitional payments
to limit loss under the PPS.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
The Resource Based Relative
Value Scale (RBRVS)
• Congress adopted the current update formula for
physician payments in the Balanced Budget Act
(BBA) of 1997.
• Anesthesia services are based on values from a
uniform relative value guide developed and
maintained by the American Society of
Anesthesiology (ASA) and use a separate
payment system which we will not cover today.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Medicare Reimbursement
Formula
Resource Based Relative Value Scale
Payment =
{(RVU work x GPCI work) +
(RVU practice expense x GPCI
practice expense) + (RVU
malpractice x GPCI malpractice)}
X
conversion
factor
RVU = Relative Value Unit
GPCI = Geographic Practice Cost Indices
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Relative Value Units (RVUs)
• Modifications to the RVU values must, by statute,
be conducted in a manner that does not increase
aggregate costs to the Medicare system by more
than $20 million per year.
• To prevent Medicare expenditures from exceeding
this cap, CMS must lower the conversion factor,
thereby reducing physician compensation for all
services.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Geographic Practice Cost
Indices (GPCIs) - gyp·sies
• GPCIs consider variations in the cost of providing
medical products and services across the country.
• Each area is attributed its own GPCI for each of the
work, practice expense and malpractice factors.
– 90 different GPCI localities
• CMS is required to update GPCIs at least every three
years.
– Data often from the census (thus a 10 year update).
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
The Conversion Factor
•
•
•
The “conversion factor” is a multiplier, converting the
geographically adjusted inputs to full Medicare allowable.
Annual adjustments are based on the Medicare Economic
Index, a measure of medical inflation, which is modified by
the figure resulting from the Sustainable Growth Rate
(SGR) formula.
The SGR is essentially a cost control mechanism and is the
result of four estimates:
•
•
•
•
Change in national gross domestic product
Increase in beneficiary enrollment in Medicare
Increase in physician fees
Cost of complying with new law/regulation
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Other Payment Models
• Durable Medical Equipment, Prosthetics, Orthotics,
and Supplies (DEMPOS): Uses a competitive bidding
process for area venders of items and supplies
• AWP/ASP: Published rates for physician injectible
drugs (chemo).
– Average Wholesale Price (AWP) is a varying technique of
calculating drug sales rate.
– Average Sales Price (ASP) is a published Medicare rate
based on manufacturer reporting of sales prices.
– Medicare competitive bidding project failed.
– Some payers now reimbursing based on cost with invoice.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Medicare Advantage
• Balance Budget Act of 1997 established Medicare Part
C, effective Jan. 1, 1999.
– Mandated coverage but great flexibility.
• Major benefit – drug coverage but optional
• Other benefits – preventative services often covered but
Congressional testimony illustrated payer difficulty in
showing “new” services that were covered.
• Only available in certain areas.
• Payment rates and coverage policies set by payer.
– Must include national coverage policies and certain other
conventions.
– Generally more like private insurance rather than Medicare.
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
What is a contract?
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Statue of Frauds &
the Four Corners
• An act of the English Parliament back in 1677 established
the common law considerations for contracts
– States adopted some form of the Statute of Frauds that is also
consistent with the Uniform Commercial Code (sale of goods)
– The “four corners” of the contract reference the page(s) of the
contract to evidence the agreement rather than additional evidence
from oral agreements or how the parties acted (parol evidence)
• Thus, contracts today in the United States generally must:
–
–
–
–
Be in writing
Last longer than one year
Signed by the party paying for the goods or services
Specify the prices for goods and services
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Medical Contracts Are
Different
• Participation agreements in health plan
networks often do not include an exhaustive
list of goods and services covered by the
contract
– Rates for top codes for “specialty”
– No disclosure of how proprietary claims
processing edits will affect rates
• Administrative guides and other notices are
part of the agreement by reference
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Types of Contracts
• Bilateral agreements: signatures from both
parties (clinician and health plan) required
• Unilateral agreements: agreement signed by
initiating party (health plan) and unless the
other party (clinician) disagrees within a
specified timeframe, the agreement is effective
– Most changes to contracts are done unilaterally
– Notice of changes may not need to be mailed
– Timeframe must be “reasonable”
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
The Agreement
• Establishes the responsibilities of each party
• Threshold for credentialing and privileges
• Covers “medically necessary” services
– Medical services considered reasonable,
necessary, and/or appropriate, based on evidencebased clinical standards of care
• Clarifies timely filing requirements
– How quickly claims must be submitted to be paid
and how quickly they will pay you
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Things To Check
• Term period
– Generally an initial term, then evergreen
– Termination requires a notice period prior to
anniversary. Ex: 120 days notice prior to 6/1
anniversary means formal written notice was due
to plan by 2/1
• Notice requirements for changes to practice
• Document retention requirements
• Office availability; appointment availability
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Part II: Enrollment &
Credentialing
To receive a contract, each physician must be
enrolled or credentialed.
– What are these requirements?
•
Who do they apply to?
– How does Medicare differ from private
insurance?
– What is revalidation or re-credentialing and why
is it required?
– Online systems: PECOS and CAQH’s Universal
Provider Datasource
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
The
Building Blocks of Medicine
Webinar Series
www.osteopathic.org/buildingblocks
May 22:
Medicare Enrollment and Health Plan
Credentialing
All rights reserved. © 2013-14 Searfoss Consulting Group, LLC. To distribute or copy, please contact jen@SCGhealth.com.
Questions
Jennifer Searfoss, J.D., C.M.P.E
o 888-886-8054
e jen@SCGhealth.com
Practice Management Communications
• Free, timely and relevant practice management email communications from the AOA.
• Physicians, practice staff, consultants and other health
care partners are invited to sign up.
Sign up by sending a subscribe message to
practicemanagement@osteopathic.org
Practice Management Webinars
www.osteopathic.org/pmwebinars
Movie
•
•
•
•
HIPAA
Meaningful Use
ERISA
ICD-10
•
•
•
•
Coding
Value Based Modifiers
Healthcare Literacy
Building Blocks of Medicine
Please support our work through
your AOA membership.
Join today.
To become a member call the AOA toll free at (800) 621-1773, press 1
or join online
www.osteopathic.org/membership