Position and Orientation of Hyoid Bone in Class II Division 1
advertisement

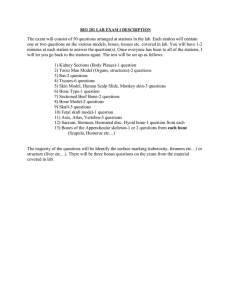
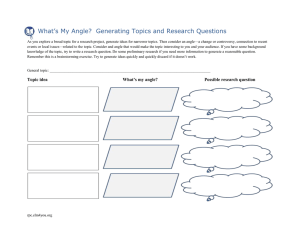
10.5005/jp-journals-10021-1039 ORIGINAL ARTICLE Rohit Khanna et al Position and Orientation of Hyoid Bone in Class II Division 1 Subjects: A Cephalometric Study 1 Rohit Khanna, 2Tripti Tikku, 3VP Sharma ABSTRACT Objective: The present study was undertaken to compare the pharyngeal dimensions in Angle’s Class I normal and Angle’s Class II division 1 samples, and to correlate it with the dentoskeletal parameters in both the groups. Materials and methods: The sample consists of 92 pretreatment lateral cephalogram, which were categorized into two groups, Group A and Group B, that they should present Angle’s Class I and Angle’s Class II molar relationship. Each group consists of 25 males and 21 females. Descriptive statistics for 14 variables were calculated. Results obtained from this study imply that Angle’s Class II Division 1 samples with retrognathic mandible showed an inferoposterior displacement of hyoid bone. Results: The positional alteration of hyoid was prevalent in skeletal malrelationship rather than dentoalveolar malocclusion. The anteroposterior dimension of pharynx at hyoid level was more in males than in females, and it was relatively less in Angle’s Class II Division 1 samples to Class I samples. No significant sexual dimorphism exists in angular measurements of hyoid positioning. Keywords: Hyoid bone, Dentofacial Pattern, Facial morphology, Pharyngeal dimension. How to cite this article: Khanna R, Tikku T, Sharma VP. Position and Orientation of Hyoid Bone in Class II Division 1 Subjects: A Cephalometric Study. J Ind Orthod Soc 2011;45(4):212-218. INTRODUCTION Attempts have been made to visualize the position of hyoid bone in various dentofacial patterns.1-5 In almost all previous studies, hyoid bone was related to the cranium, due to which a great variability was observed in its position even on slight movement of the head. To minimize the variability in its position, Bibby1 in 1981, related the hyoid bone to mandibular symphysis and third cervical vertebra in individuals with Class I malocclusions. Precise measurement of hyoid bone position by cephalometric means is considered difficult. Graber2 stated that slight variations in head position in the cephalostat, the postural position of the spine, and the state of function all affect the position of the hyoid bone. Stepovich3 reported that when roentgenograms of the same person were taken at different time intervals, the hyoid bone was found to be positioned differently in each film. Ingervall and associates4 believe that Stepovich exaggerated the lack of precision in recording the hyoid bone 1 Professor, 2Professor and Head, 3Former Head and Ex-Dean 1,2 Department of Orthodontics and Dentofacial Orthopedics Uttar Pradesh Dental College and Research Centre, Lucknow Uttar Pradesh, India 3 Department of Orthodontics, Faculty of Dental Sciences, Chhatrapati Shahuji Maharaj Medical University, Erstwhile King George’s Medical College, Lucknow, Uttar Pradesh, India Corresponding Author: Rohit Khanna, Professor, Department of Orthodontics and Dentofacial Orthopedics, Uttar Pradesh Dental College and Research Centre, Lucknow, Uttar Pradesh, India e-mail: rohitkhanna@doctor.com, rohitkhanna.dr@gmail.com Received on: 5/11/11 Accepted after Revision: 10/11/11 212 position, although they admit that the hyoid position will vary even under standard conditions. King5 noted that changes in head position lead to changes in the position of the hyoid bone in the same person. If the head is extended back, then the hyoid bone moves back; if the head is tipped forward, then the hyoid bone moves forward. This confirmed the postulate of Negus6 who found that the hyoid bone to elevate when the head was in dorsiflexion and to move down when the head was in ventriflexion. Ingervall7 found a positive correlation (although not always significant) between the anteroposterior distance between retruded contact and intercuspal positions of the mandible and the vertical movement of the hyoid bone between these positions. In another study, Ingervall7 compared the hyoid bone positions when the mandible is in intercuspal position and when it is in postural position. He found that the hyoid bone was higher in postural position than in intercuspal position. Brodie8 brought attention to the suprahyoid muscles which suspend the hyoid bone, the larynx, the pharynx, and the tongue, since these muscles are attached at or near the symphysis of the mandible, it follows that, should the hyoid bone passively follow the course of the chin, all of the above structures would fall back and thus tend to shut off the airway. This is prevented by shortening of the suprahyoid muscles. Grant9 studied the position of the hyoid bone in Class I, II and III malocclusions. He concludes that the hyoid bone position is constant in all three classes and that the position of the hyoid bone is determined by the musculature and not by the occlusion of the teeth. Durzo and Brodie10 showed that the relationship between the hyoid bone and the mandible is maintained from the age of 3 years. According to them the hyoid bone is positioned at a level opposite to the lower portion of the third cervical vertebrae and the upper portion of the fourth cervical vertebrae. Its anteroposterior position, it is dependent on the relative lengths JAYPEE JIOS Position and Orientation of Hyoid Bone in Class II Division 1 Subjects: A Cephalometric Study of the muscles running to it and also on gravity acting on the larynx. Bench11 found that the hyoid bone gradually descends from a position opposite the lower half of the third and the upper half of the fourth cervical vertebrae at the age of 3 years to a position opposite the fourth cervical vertebrae in adulthood. King5 found that the distance between the hyoid bone and the cervical vertebrae is constant until puberty, when the hyoid bone moves slightly forward. Bibby1 postulated that since hyoid is not related to cranial reference plane (as in all previous studies) the incorrectness stem from changes in head postures is minimized. Apart from establishing norms for the hyoid triangle, he found that bony pharynx at the level of PNS and hyoidale to have the same anteroposterior dimension with 0.98 coefficient of correlation. He did not find any sexual dimorphism in hyoid position. Bibby RE12 found that hyoid bone has a stable position and is independent of any posture alterations due to tonguethrusting or mouth breathing. Haralabakis et al13 strongly suggest that hyoid bone moves in close conjunction with the pharynx, cervical spine, and mandibular plane in patients with entirely different skeletal patterns. Erdinc et al 14 found that hyoid bone location in the hypodivergent group was not changed vertically, however, it had more of a posterior placement with the increase of Pg-H distance. Bucchieri15 investigated that the altered hyoid bone position may influence tongue position and upper airway patency of OSA patients. Ferraz16 concluded that the hyoid bone keeps a stable position, probably in order to secure correct ratios in the airways, and it does not depend on the respiratory pattern. Pae17 investigated that changes in hyoid position over time were significant in dolichofacial subjects but not in brachyfacial subjects. Ritu Duggal et al18 concluded that the anteroposterior position of the hyoid bone was more forward in subjects with short face syndrome and the vertical position of the hyoid bone was comparable among subjects with different vertical jaw dysplasias and axial inclination of the hyoid bone closely followed the axial inclination of the mandible. The present study was undertaken to compare the pharyngeal dimensions in Angle’s Class I normal and Angle’s Class II division 1 samples, and to correlate it with the dentoskeletal parameters in anteroposterior dimension irrespective of facial divergence and to find the role of sagittal mandibular positioning in hyoid bone position. 1. Group A: Subjects having Angle’s Class I molar relationship with ideal occlusion, and no significant abnormalities in the vertical dimension of facial form. This group comprised of 25 male and 21 female subjects from the records of control group of previous conducted studies. 2. Group B: Subjects having Angle’s Class II division 1 malocclusion. This group comprised of 25 male and 21 female subjects from the patients reporting at the Department of Orthodontics, King George’s Medical College, Lucknow. The subjects of entire sample mentioned above fell in the age group of 16 to 24 years, with the mean age of 18 years for females and 20 years for males. METHODS The following osteometric landmarks were used in the present study (Fig. 1). 1. Nasion (N) 2. Sella (S) 3. Articulare (Ar) 4. Gonion (Go) 5. Menton (Me) 6. Capitulare (C): Center of the head of the condyle 7. Xi: Geometrically determined centroid of the ramus 8. Pt. D: Located by inspection as the center of body of the mandibular symphysis seen on lateral cephalogram. MATERIALS AND METHODS The present study was based on lateral cephalograms of 92 individuals selected on the conviction that they should present Angle’s Class I and Angle’s Class II molar relationship. The cephalograms for the purpose were obtained from records maintained in the Department of Orthodontics, Faculty of Dental Sciences, King George’s Medical College, Lucknow, India. The cephalograms of the subjects were categorized into the following two groups: Fig. 1: Osteometric landmarks The Journal of Indian Orthodontic Society, October-December 2011;45(4):212-218 213 Rohit Khanna et al 9. C3: The point at the most inferior anterior position on the third cervical vertebra.1 10. Hyoidale (Hy): The most superior, anterior point on the body of the hyoid bone.1 11. AA’: The most anterior point on the body of the atlas vertebra, seen on the lateral cephalogram.1 12. PNS 13. Subspinale (Point ‘A’). For the location of point ‘C’, a ‘template’ with concentric circles on a graph was designed on the basis of geometric visualization. The circle which most nearly coincided with the perimeter of condylar head was superimposed and the geometric center of condyle was located. Similarly, for the location of ‘point D’, the inner cortical plate was traced and the center of this circumscribed area was located with the help of the ‘template’. For the linear and angular measurements, a scale and protractor were used and readings were recorded to the nearest of 0.5 mm and half degree respectively. Tracings of the cephalograms of each group were repeated after an interval of 2 weeks and both sets of measurements were subjected to t-test. p-value was found to be 0.1, i.e. significant for all the measurements, signifying that the location of the points and lines were correct. MEASUREMENTS Following five linear and seven angular measurements were analyzed: Linear Measurements (in mm) 1. Sella-Nasion (S-N)—it is drawn from selected point Sella to Nasion. It represents the anterior-posterior latent of the anterior cranial base. 2. Capitulare-Xi (C-Xi)—line connecting center of condyle, i.e. capitulare to the geometric center of the ramus of mandible, i.e. Xi. This line will be named as Capitulare axis in this study. 3. C3-Hy(C3-Hy)—formed by joining most inferior-anterior point on the third cervical vertebrae to most superior, anterior point on the hyoid bone.1 4. Hyoidale-Pt. D (Hy-D)—line connecting most superior anterior point on the hyoid bone to center of mandibular symphysis. 5. AA’-PNS—line adjoining the most anterior point on body of atlas vertebrae and posterior nasal spine designating upper bony nasopharynx.1 Angular Measurements (in degree) 1. Saddle angle (NSAr)—the angle formed by joining Nasion, Sella and Articulare is an assessment of the relationship of anterior and posteriolateral cranial base. 2. Articulare angle (SArGo)—the angle is constructed by joining sella, articulare and gonion. 3. Gonial angle (ArGoMe)—the angle formed by tangents of body of the mandible and posterior border or ramus. 214 4. SNA—the angle formed with sella nasion plane and the line joining nasion and point A. 5. SND—the angle formed between sella-nasion plane and nasion-point D plane. 6. Hyoidale angle (C3HyD)—the angle formed by C3 to Hyoidale plane and Hyoidale Pt. D. The angle formed superiorly by two planes is read as hyoidale angle. 7. Hyoid plane angle—formed by intersection of long axis of greater horn of hyoid with C3-Pt. D line. RESULTS The data obtained by the linear and angular measurements from tracings of lateral cephalograms was subjected to statistical analysis. The arithmetic means and standard deviations of the linear and angular measurements are given in Table 1. The Hy-D dimensions does not reveal any statistically significant changes between the Groups A and B both in male and female samples. In Table 2, the significance of difference (t-value) of angular and linear measurements in Group A and Group B has been depicted. Referring to Table 1, the differences in means show the C3-D is lesser in Group B. In Table 3, the anteroposterior measurements of pharynx (C3-Hy) showed highly significant difference between males and females in both the groups. The highly significant change was observed in hyoidale angle due to the inferiorly positioned hyoid bone in Group B to Group A (Table 2). Thus, it was decided to correlate the hyoidale angle to certain angular measurements contributing to Class II, division 1 tendencies (Tables 4 and 5). The angle SND-relating mandible to the cranium showed a very highly significant coefficient of correlation to hyoidale angle both in males and females in Group A (Table 4), and a high level of significance in Group B (Table 5), confirming that distally positioned mandible contributes mainly to the inferior drop of hyoid bone. The angle SNA shows significant correlation in Group A (Table 4) in both males and females, while no significant correlation was observed in Group B (Table 5). This showed that the Class II, division 1 relationships in the given sample were due to a retruded mandible rather than the procumbency of the maxilla (Fig. 2). The saddle angle (NS Ar) and articulare angle (S Ar Go) showed low level negative correlation to hyoidale angle in Group A (Table 4) and Group B (Table 5). The negative correlation indicates that with increase in saddle angle and articulare angle there is simultaneous decrease in hyoidale angle in Groups A and B (Table 5). The gonial angle showed no significant correlation in Groups A and B (Tables 4 and 5) for both males and females (Fig. 2). The hyoid plane angle (posterior superior angle between long axis of greater horn of hyoid and C3-D line) when correlated to hyoidale angle (C3HyD) showed a negatively high level of significance, i.e. with the decrease in the hyoidale angle (C3HyD) there was simultaneous increase in hyoid plane angle. JAYPEE JIOS Position and Orientation of Hyoid Bone in Class II Division 1 Subjects: A Cephalometric Study Table 1: Arithmetic means and standard deviations of angular and linear measurements Sl. No. Variables Group A Males (n = 25) Mean SD Group B Females (n = 21) Mean SD Males (n = 25) Mean SD Females (n = 21) Mean SD Angular measurements (in degree) C3HyD SNA SND NSAr S-Ar-Go Ar-Go-Me Hyoid plane angle 1. 2. 3. 4. 5. 6. 7. 178.36 81.28 76.70 125.88 141.00 120.32 16.90 8.38 2.86 2.61 3.37 5.19 5.55 8.38 180.80 78.81 75.76 128.48 139.05 124.62 22.00 9.38 3.36 2.33 5.95 6.94 5.44 9.25 158.50 81.40 73.40 128.12 139.84 119.70 21.72 16.30 3.45 3.67 4.43 6.42 5.23 9.82 155.57 78.50 70.85 127.47 142.33 127.10 28.12 12.07 3.87 3.40 6.69 5.76 5.79 12.45 Linear measurements (in mm) 1. 2. 3. 4. 5. 6. 7. C3Hy AA’-PNS S-N C-Xi C3Hy:HyD HyD C3D 37.48 35.06 71.84 38.12 0.858 44.06 81.98 4.19 4.35 3.95 2.85 0.11 6.42 9.21 32.02 33.40 69.57 34.05 0.78 41.05 75.17 2.78 3.03 3.44 3.49 0.12 5.05 6.16 36.30 35.12 72.46 38.18 0.82 44.16 76.89 3.83 3.91 3.54 2.76 0.136 6.01 9.30 32.88 33.95 69.67 33.62 0.818 40.20 68.12 3.66 3.17 3.65 2.61 0.21 7.68 8.92 Table 2: Mean difference of measurements in Groups A and B and their level of significance Sl. No. 1. 2. 3. 4. 5. 6. 7. 8. Measurements Males (n = 25) Females (n = 21) Mean difference t-value p-value Mean difference t-value p-value 19.86 1.18 0.06 0.036 0.1 5.09 0.62 0.06 5.43 1.41 0.055 1.028 0.057 1.95 0.58 0.07 *** NS NS NS NS * NS NS 25.24 0.86 0.55 0.038 0.85 7.05 0.1 0.38 7.56 0.84 0.57 0.72 0.32 2.98 0.08 0.41 *** NS NS NS NS C3HyD (in degree) C3-Hy (in mm) AA’-PNS (in mm) C3Hy:HyD (in mm) Hy-D (in mm) C3D (in mm) S-N (in mm) CXi (in mm) NS NS *p < 0.05: Significant; ***p < 0.001: Very highly significant; NS: Not significant Table 3: Mean difference of measurements in Groups A and B and their level of significance Measurements Males (n = 25) C3Hy (in mm) AA’-PNS (in mm) C3HyD (in degrees) Hyoid plane angle (in degrees) Mean difference t-value 5.48 1.66 2.44 5.10 4.76 1.51 0.97 1.92 Females (n = 21) p-value ** NS NS NS Mean difference t-value 3.92 1.17 2.94 6.50 3.54 1.07 0.70 1.92 p-value ** NS NS NS **p < 0.01: Highly significant; NS: Not significant Table 4: Coefficient of correlation ‘r’ of angle C3-HyD with following angular measurements in Group A and their level of significance Sl. No. Angular measurements Sex ‘r’ p-value 1. SND Male (n = 25) Female (n = 21) 0.798 0.703 *** *** 2. SNA Male Female 0.445 0.573 * ** 3. N-S-Ar Male Female –0.034 –0.116 NS NS 4. S-Ar-Go Male Female –0.172 –0.164 NS NS 5. Ar-Go-Me Male Female 0.04 0.19 NS NS 6. Hyoid plane angle Male Female –0.687 –0.59 ** ** *p < 0.05: Significant; **p < 0.01: Highly significant; ***p < 0.001: Very highly significant; NS: Not significant The Journal of Indian Orthodontic Society, October-December 2011;45(4):212-218 215 Rohit Khanna et al Table 5: Coefficient of correlation ‘r’ of C3-Hy (in mm) with following linear measurements in Group A and their level of significance Sl. No. Linear measurements 1. AA’-PNS 2. S-N 3. C-Xi Sex ‘r’ p-value Male Female Male Female Male Female 0.85 0.71 0.41 0.51 0.35 0.23 *** *** * * NS NS *p < 0.05: Significant; ***p < 0.001: Very highly significant; NS: Not significant Table 6: Coefficient of correlation ‘r’ of C3Hy (in mm) with following linear measurements in Group B and their level of significance Sl. No. Linear measurements 1. AA’-PNS 2. S-N 3. C-Xi Sex ‘r’ p-value Male Female Male Female Male Female 0.55 0.49 0.25 0.35 0.175 0.22 ** * NS NS NS NS *p < 0.05: Significant; **p < 0.01: Highly significant; NS: Not significant Fig. 2: Difference in facial morphology in normal and Class II div 1 malocclusion This value of hyoid plane angle was found in bxoth males and females (Tables 4 and 5) (Fig. 2). The anteroposterior dimension of pharynx (C3-Hy) was further correlated with linear measurements (Table 6). When correlated with AA’-PNS it revealed a very highly significant level in Group A both in males and females, indicating that the hyoid bone represents the anterior bony boundary of the pharynx at a lower level. While the drop in level of coefficient of correlation was observed in Group B, which was probably due 216 to change in dimension of either C3-Hy or AA’-PNS, but on visualizing the significance of difference in means of AA’-PNS (Tables 1 and 2) it was observed to be statistically not significant between Groups A and B, i.e. change was probably due to decrease in anteroposterior dimension of C3-Hy in Group B. Similarly, when C3-Hy was correlated to S-N plane and C-Xi, it was found that level of correlation changes from Group A to Group B. The mean difference of S-N and C-Xi amongst the groups was negligibly small (Table 1), indicating the probable changes in C3-Hy dimension. Referring to Table 2, the low level of significance in the mean difference of C3-Hy in Group A and B was observed. Although the t-value was statistically nonsignificant but the difference in values establishes that change exists in anteroposterior dimension of C3-Hy in Group A to Group B. DISCUSSION Whenever vital functions of respiration and deglutition are imposed upon by morphological alteration, the compensations in morphology and physiological activities are integrated upon modification in neurological pathway. This discussion will deal mainly with the variations in mandibular morphology and concurrent changes in associated structures in Class I subjects and subjects with Angle’s Class II division 1 malocclusion. Hoffman and Hoffman19 believed that the hyoid bone was important for tongue position, since most of the extrinsic muscles of the tongue are attached to it and it also maintains the pharyngeal airway, which is essential to life. It was found that the positioning of hyoid was variable in Class I and Angle’s Class II division 1 malocclusion. To evaluate the shift of hyoid and its effect on the patency of airway, the anteroposterior dimension of pharynx (C3-Hy) was compared with upper bony airway (AA’-PNS). It was observed that coefficient of correlation was lesser in Class II division 1 samples than in normal subjects (Fig. 2). The slight decrease (statistically nonsignificant) in anteroposterior dimension of pharynx at level of hyoid. The probable reason for this decrease was the posterior movement of hyoid bone as mandible attains distal position in Class II division 1 sample. The patency of the airway is to be maintained for the survival, hence the further posterior displacement of hyoid was resisted. To compare the relative change in distance of hyoid to cervical vertebrae (C3-Hy) and hyoid to center of mandibular symphysis (Hy-D) in Class I and Class II division 1 samples. The ratio (C3Hy: HyD) was calculated for each sample and subjected to statistical analysis, which showed no significant difference in means (Table 2) was observed. While the distance between cervical vertebrae and mandibular symphysis (C3-D) was significantly decreased in samples with Class II division 1 malocclusion (Tables 1 and 2). The position of hyoid was altered in order to accommodate the muscles geniohyoid and anterior belly of diagastric, which could be the probable reason for posterior displacement of hyoid and slight decrease in C3-Hy dimension. The decrease in C3-Hy was not sufficient to JAYPEE JIOS Position and Orientation of Hyoid Bone in Class II Division 1 Subjects: A Cephalometric Study accommodate the hyoid and hence the change was expected in either superior or inferior direction. It was further noticed that the angle formed by C3-Hy line and Hy-D (C3HyD-Hyoidale angle) superiorly at the hyoid decreases in Class II division 1 subjects indicating the inferior positioning of the hyoid bone. The very highly statistically significant difference in hyoidale angle (C3HyD) was noticed among Class I normal and Angle’s Class II division 1 samples (Table 2). Grant9 also reported the difference in hyoid bone position, and found hyoid bone was higher in Class III than in Class II subjects in relation to cervical vertebrae. It was observed that retrognathic mandible leads to inferioposterior displacement of hyoid bone. This inferior-posterior displacement of hyoid might affect the tongue posture in oral cavity and stretching of the pharyngeal wall, because hyoglossus muscles and middle constrictor muscles of pharynx take their attachments on greater horn of hyoid bone. The hyoidale angle was also correlated to angle SNA showed a significant correlation in Class I normal subjects, while in Class II division 1 samples it was statistically not significant (Tables 4 and 5). The above findings showed that Class II division 1 tendency of samples in the present study was due to mandibular retrusion rather than maxillary procumbency. Two of the samples revealed the higher positioning of hyoid similar to that found in Class I normal subjects. On further investigation, the Class II division 1 tendency in those samples was due to maxillary procumbency rather than distal mandibular positioning. It was thus interpreted that for change in position of hyoid it was necessary that the subjects should possess retrognathic mandible. Increase in saddle angle (NSAr) and articulare angle (SArGo) leads to retrognathic mandibular pattern. On correlating these angular measurements to hyoidale angle, they showed statistically insignificant negative correlation in Class I normal subjects and Class II division 1 samples (Tables 4 and 5). The gonial angle (ArGoMe) showed no significant correlation with hyoidale angle in both the Classes (Tables 4 and 5). These findings strengthens the fact that the skeletal malrelationship causes the change in hyoid position, i.e. sagittal malformation has highly significant role in inferoposterior positioning of hyoid bone. The possible explanation for the low level correlation of saddle angle to hyoidale angle is that, large saddle angle is compensated with a change in articulare angle and length of ramus. While the articulare angle apart from affecting the anteroposterior positioning of mandible, also changes in closing and opening of bite. In Class II division 1 malocclusion, the distal mandibular position increases the articulare angle, while the deep overbite compensate this increase resulting in a relatively less change in articulare angle. The hyoid plane angle (long axis of greater horn of hyoid to C3-D line). When correlated with hyoidale angle (C3HyD) revealed a highly significant negative coefficient of correlation (Tables 4 and 5). The increase in hyoid plane angle with an inferior drop of body of hyoid in Class II division 1 malocclusion was noticed, thereby maintaining the relative length of middle constrictor muscle of pharynx and hyoglossus muscle, which takes its attachments on greater horn of the hyoid bone. However, the decrease in hyoidale angle was to accommodate geniohyoid, anterior belly of diagastric and mylohyoid muscles. The slight posterior displacement is justifiable due to stylohyoid muscle and ligaments attached to the body of hyoid, which pulls the hyoid bone posteriorly when it is displaced inferiorly, encroaching upon pharyngeal space in Class II division 1 subjects, resulting the decrease in anteroposterior dimension of pharyngeal space. The anteroposterior linear dimension of pharynx (C3-Hy) showed a marked sexual dimorphism. The highly significant values of difference in means in both Class I and Class II subjects were observed (Table 3). The anteroposterior dimension was found more in males than in females (Table 1) as also observed by King, EW.5 His roentgenographic study of pharyngeal growth, revealed an increase of 7.8 mm in males and 2.3 mm in females between three months and sixteen years of life. While AA’-PNS showed statistically no significant changes in males and females. Though small difference in means was observed in AA’-PNS both in normal and Angle’s Class II division 1 malocclusion. The hyoid plane angle and hyoidale angle revealed no statistically significant difference in means amongst males and females both in Class I normal subjects and Class II division 1 malocclusion (Table 3). Bibby1,12 also observed the lack of sexual dimorphism, in hyoid plane angle. Hence, it could well be concluded that slight change in linear dimension of pharyngeal space at the level of hyoid occurs in skeletal Class II division 1 malocclusion. The change was due to the inferior-posterior displacement of hyoid, the position of which is governed by certain skeletal parameters of dentofacial complex. Furthermore, sexual dimorphism exist in C3-Hy linear measurement, but the angular measurement hyoidale angle and hyoid plane angle did not reveal marked difference in male and female samples. CONCLUSION The following conclusions were drawn: 1. Angle’s Class II division 1 samples with retrognathic mandible showed an inferoposterior displacement of hyoid bone. 2. The positional alteration of hyoid was prevalent in skeletal malrelationship rather than dentoalveolar malocclusion. 3. The anteroposterior dimension of pharynx at hyoid level was more in males than in females, and it was relatively less in Angle’s Class II division 1 samples to Class I samples. 4. No significant sexual dimorphism exists in angular measurements of hyoid positioning. The Journal of Indian Orthodontic Society, October-December 2011;45(4):212-218 217 Rohit Khanna et al REFERENCES 1. Bibby RE, Preston CB. The hyoid triangle. Am J Orthod 1981;80(1):92-97. 2. Graber LW. Hyoid changes following orthopedic treatment of mandibular prognathism. Angle Orthod 1978;48(1):33-38. 3. Stepovich ML. A cephalometric positional study of the hyoid bone. Am J Orthod 1965;51(12):882-900. 4. Ingervall B, Carlsson GE, Helkimo M. Change in location of hyoid bone with mandibular positions. Acta Odontol Scand 1970;28(3):337-61. 5. King EW. A roentgenographic study of pharyngeal growth. Angle Orthod 1952;22:33-37. 6. Negus VE. The mechanism of larynx. St Louis 1940. 7. Ingervall B. Positional changes of mandible and hyoid bone relative to facial and dental arch morphology. A biometric investigation in children with postnormal occlusion (Angle Class II, Div. I). Acta Odontol Scand 1970;28(6):867-94. 8. Brodie AG. Consideration of musculature on diagnosis, treatment and retention. Am J Orthod 1952;38:823-35. 9. Grant LE. A radiographic study of the hyoid bone position in Angle Class I, II and III. Unpublished Master Thesis, Univ. of Uanas City. 10. Durzo CA, Brodie AG. Growth behavior of hyoid bone. Angle Orthod 1962;32:193-203. 218 11. Ruel W, Bench BS. Growth of the cervical vertebrae as related to tongue, face, and denture behavior. Am J Orthod 1963;49: 183-214. 12. Bibby RE. The hyoid bone position in mouth breathers and tongue-thrusters. Am J Orthod 1984;85(5):431-33. 13. Haralabakis NB, Toutountzakis NM, Yiagtzis SC. The hyoid bone position in adult individuals with open bite and normal occlusion. Eur J Orthod 1993;15(4):265-71. 14. Erdinc AM, Dincer B, Sabah ME. Evaluation of the position of the hyoid bone in relation to vertical facial development. J Clin Pediatr Dent 2003;27(4):347-52. 15. Bucchieri A, Mastrangelo C, Stella R, Poladas EG. Cephalometric evaluation of hyoid bone position in patients with obstructive sleep apnea. Minerva Stomatol 2004;53(1-2):33-39. 16. Ferraz MJ, Nouer DF, Teixeira JR, Bérzin F. Cephalometric assessment of the hyoid bone position in oral breathing children. Braz J Otorhinolaryngol 2007;73(1):45-50. 17. Pae EK, Quas C, Quas J, Garrett N. Can facial type be used to predict changes in hyoid bone position with age? A perspective based on longitudinal data. Am J Orthod Dentofacial Orthop 2008;134(6):792-97. 18. Duggal R, Jena AK. Hyoid bone position in subjects with different vertical jaw dysplasias. Angle Orthod 2011;81:81-85. 19. Hoffman JA, Hoffman RL. Tongue-thrust and deglutition: Some anatomical, physiological, and neurological considerations. J Speech Hear Disord 1965;30:105-20. JAYPEE