Trends in dementia-free life expectancy among elderly
advertisement

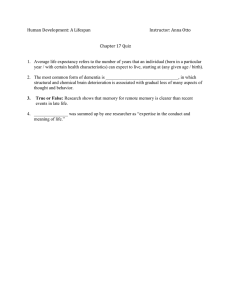
© International Epidemiological Association 1999 International Journal of Epidemiology 1999;28:1110–1118 Printed in Great Britain Trends in dementia-free life expectancy among elderly members of a large health maintenance organization Catherine Sauvaget,a Ichiro Tsuji,a Mary N Haanb and Shigeru Hisamichia Background This study examined the secular trends of life expectancy without dementia among elderly American members of a health maintenance organization, and observed if an increased life expectancy is accompanied by an increase in the duration of life with dementia. Methods The data derived from two chronological 9-year prospective cohort studies of members of the Kaiser Permanente Medical Care Program of Northern California. The first and second cohorts included 2702 and 2926 people aged >65 years free from dementia at baseline. Life expectancy without dementia or dementia-free life expectancy (DemFLE) is defined as the average number of years a person is expected to live without dementia. Total life expectancy is equal to the sum of DemFLE and life expectancy with dementia. Estimations of DemFLE were based on mortality data and incidence of dementia, using double-decrement life tables. Results Between the first and second cohorts, all-cause mortality rates declined, while the incidence of dementia remained constant in both men and women. Among the males, total life expectancy increased at a higher rate than DemFLE. Consequently, the duration of life with dementia was extended in the second cohort. Conversely, among the females DemFLE increased at a higher rate than total life expectancy, thus the duration of life with dementia decreased in the second cohort. The median age of dementia onset was postponed by 2–3 years in the second cohort for females, and did not show any specific difference between the two cohorts in males. Conclusion The trends of health expectancies suggest an extension of the duration of life with dementia for males and a compression of dementia for females. A decreased incidence of risk factors for dementia among females in the second cohort such as stroke may explain these trends. Keywords Health expectancy, dementia, incidence, compression and extension of morbidity Accepted 29 April 1999 In recent decades, a decline in the mortality rate in the US has led to an increase in life expectancy. With a rapid extension of life expectancy, the number of elderly people suffering from dementing illnesses is escalating. Cognitive impairment and mental diseases are among the most common morbid conditions in later life. The prevalence of dementia among elderly Americans aged >65 years is estimated to be between 5% and a Department of Public Health, Tohoku University School of Medicine, Sendai, Japan. b Department of Epidemiology and Preventive Medicine, University of California School of Medicine, Davis, CA, USA. Reprint requests to: Catherine Sauvaget, Department of Public Health, Tohoku University School of Medicine, Sendai 980–8575, Japan. E-mail: sauvaget@mail.cc.tohoku.ac.jp 10%.1–8 The number of elderly people suffering from dementia and living in the US was estimated at 3.1 million people in 1990; this number is projected to increase 2.5- to 4-fold by the year 2040.9 The question that arises is whether longevity is a reward. Nobody would appreciate the added years of life if they were accompanied by disability or dementia. In order to answer this question, a new health indicator that takes both morbidity and mortality into consideration has emerged.10 Healthy life expectancy is defined as the duration an individual at a given age is expected to live without any specific morbid condition. A comparison of healthy life expectancies between different times allows us to appraise the quality of increased years of life. Three scenarios are possible. The first argues that life expectancy increases faster than healthy life expectancy, thus the duration to 1110 TRENDS IN DEMENTIA-FREE LIFE EXPECTANCY be spent with poor health increases. At an extreme limit, life expectancy increases while healthy expectancy remains the same; this figure leads to ‘the pandemic of mental disorders and chronic diseases’.11 Second, a more optimistic concept implies a stagnation in life expectancy concomitant with an increase of healthy expectancy; this theory is known as ‘the compression of morbidity’.12,13 The third pattern, called ‘dynamic equilibrium’, describes a stability of morbidity and health status levels, thus life expectancy and healthy expectancy increase at the same rate.14 Dementia-free life expectancy (DemFLE) is defined as the average number of years an individual at a given age is expected to live without dementia. This estimation is based on mortality data and on the prevalence or incidence of dementia. To date, DemFLE has been estimated for European countries, Australia and Japan.15–20 In no previous studies has DemFLE been measured on similar populations at different periods. Thus, it is still unknown whether an increased life expectancy is associated with an extension or a compression of the duration to be lived with dementia. In the study reported here, data were derived from two chronological cohorts of subjects aged >65 years. These subjects were all members of the Kaiser Permanente Medical Care Program of Northern California (KPMCP-NC), one of the largest prepaid health maintenance organizations in the US.21 The KPMCP-NC provides comprehensive medical services to more than two million members of all ages. In order to analyse trends in life expectancies free of dementia, two cohorts of approximately 3000 elderly subjects each were followed for 9 years. For both cohorts in 1971 and 1980, all-cause mortality and onset of dementia were recorded. Identical study designs and methods were applied to each cohort. Estimations of DemFLE were based on mortality and the incidence of dementia during the followup period. The objective of the study is to examine the changes over time of DemFLE among two populations of elderly Americans members of the KPMCP-NC, and to observe whether an increase in longevity is accompanied by an increase in the duration to be spent with dementia, i.e. a ‘longer life associated with worsening health’.22 Method Data collection The study design has been published elsewhere.23 In brief, the data were derived from medical records of two cohorts of elderly Americans who were members of the KPMCP-NC between 1971 and 1979, and between 1980 and 1988. Members of the first cohort were >65 years in 1971, and those of the second cohort were >65 years in 1980. The 1971 cohort included 2877 people, while the 1980 cohort included 3113 people. The sample selection was stratified to attain equal numbers of observations (1000 in each) in three sex-age cells for each cohort: 65–69, 70–79, >80 years. Outpatient records of the study subjects were abstracted for 9 years from the baseline year (January 1971 and January 1980). A mortality search was performed using the California Automated Mortality Linkage (CAMLIS). The CAMLIS uses vital statistics tapes obtained from the California Department of Health Services to produce a weighted value that reflects the level of probability that a subject’s death and vital statistics match. 1111 All borderline values were reviewed individually to determine whether the match was correct. During the follow-up period, onset of dementia, death, or withdrawal were recorded. In the 1971 and 1980 cohorts, 7.1% and 8.6% of the subjects withdrew from the membership of KPMCP-NC before the end of the follow-up period. Comparison of the withdrawal populations in the two cohorts did not show any significant differences in terms of sex, age, race, and education level. Calculation of incidence of dementia and mortality Incident cases of dementia were identified by chart review. The KPMCP-NC did not perform a screening programme to detect dementia. In order to be diagnosed as having dementia, patients had to visit clinics. Under these circumstances, less severe cases of dementia or cases referred directly to a nursing home could have been missed, and thus the number of cases could be underestimated. Diagnosis was made by a primary care physician when the person visited the KPMCP-NC and, in most cases, was confirmed by a neurologist. Dementia was diagnosed according to the International Classification of Diseases-9th revision (ICD-9) criteria. Incident cases of dementia were defined as those diagnosed after the baseline date. Severity of dementia was not considered in this study since such information was not available for some cases. Cases of dementia present at or before baseline were considered as prevalent cases. Prevalent dementia was identified by reviewing the medical charts for 4 years before the beginning of the follow-up period. In the first cohort, on 1 January 1971, 175 prevalent cases of dementia were identified and excluded from the analyses; for the second cohort, on 1 January 1980, 187 prevalent cases were excluded. The 1971 cohort included 2702 subjects (males: 1320, females: 1382) who were free of dementia at baseline, and the 1980 cohort included 2926 such subjects (males: 1459, females: 1467). The age- and sex-specific incidence rates of dementia and the age- and sex-specific mortality rates during the follow-up period were calculated with the person-years method. In the first and second cohorts, the person-years at risk was the time from either 1 January 1971 or 1 January 1980 to the earliest date for incidence of dementia, death, withdrawal from KPMCP-NC, or either to 31 December 1979 or 31 December 1988. In the 1971 cohort, 17 454 person-years were observed for the incidence of dementia (males: 8090 person-years, females: 9364 personyears), and in the 1980 cohort, this figure was 19 387 personyears (males: 9306 person-years, female: 10 081 person-years). Calculation of DemFLE and total life expectancy For estimation of DemFLE, we performed a double-decrement life table analysis, as proposed by Katz et al.24 The probability of living free from dementia in the DemFLE calculations was based on the following formula: d dm 1px = 1 – 1px – 1px where: 1px = probability of living free from dementia during the interval between age x and age x + 1 d 1px = probability of dying during the interval between age x and age x + 1 dm = probability of becoming demented during the 1px interval between age x and age x + 1 1112 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY The estimations of the total life expectancy (TLE) were based on the probability of dying, according to the following formula: d 1px = 1 – 1px where: 1px = probability of living during the interval between age x and age x + 1 d 1px = probability of dying during the interval between age x and age x + 1 d dm were obtained by the person-years method as 1px and 1px described above. The probabilities were estimated for each year of age and each sex. Because the observed probabilities were somewhat unsteady due to a smaller sample size at higher ages, a smoothing method with logistic regression was used. In this method, the observed age-specific probabilities were fit to the exponential function: Mx = e(α + β ln x) where Mx represents the predicted probability at age x, α and β the regression coefficients, and ln x the natural logarithm of age x. In the data presented here, all regression coefficients were significant (P , 0.001) and R2 of each model was between 0.84 and 0.91. The DemFLE corresponds to the number of years a person can expect to live without dementia. Dementia life expectancy (DemLE) is defined as the time to be spent with dementia. The TLE is the sum of these two durations. A survival analysis was applied to the data. The association between dementia onset and potential risk factors of dementia was examined using the Cox proportional hazards regression model. The dependent variable was the number of years from baseline of each cohort (1971 and 1980) to the point of the development of dementia. Independent variables included age, sex, education level, smoking status, and prevalence of specific medical conditions, respectively. Results Table 1 presents the characteristics of the study subjects according to the cohort. Sex, age distribution, and education level were similarly distributed in the two study populations. The frequency of outpatient visits did not differ by cohorts. However, Whites were significantly less represented in the second cohort while Blacks were more numerous (χ2, P , 0.001). Prevalence and incidence of dementia in the 1980 cohort did not show any significant difference between the two races (prevalence of dementia in Whites: 6.5%, Blacks: 4%, χ2 P = 0.077; incidence of dementia in Whites: 1.8%, Blacks: 1.6%, χ2 P = 0.469). Table 1 Frequency distribution of socio-demographic variables according to the cohort 1971 cohort Variables 1980 cohort No. % No. % Men 1320 48.9 1459 49.9 Women 1382 51.1 1467 50.1 65–69 606 22.5 664 22.7 70–74 366 13.6 381 13.0 75–79 938 34.8 933 31.9 80–84 672 24.9 699 23.9 85+ 116 4.3 249 8.5 White 2351 92.4 2410 84.2 Black 103 4.1 312 10.9 Asian 35 1.4 68 2.4 Hispanic 16 0.6 41 1.4 Other 40 1.5 33 1.1 2380 88.1 2553 87.3 322 11.9 373 12.8 >1 visit 2662 98.5 2894 98.9 No visit 40 1.5 32 1.1 P-value Sex 0.449 Age (years) 0.406 Racea 0.001 Educational level Low-Middleb Highc 0.344 Outpatient visitsd 0.197 a Unspecified race was deleted. b Elementary and grade, high school, Trade, 1–2 years college. c 3–4 years college, graduate college. d Outpatient visits in Medicine, Surgery, Home Health, and Nursing Home. subtypes was prevented since all types of dementia were included in the analyses. The crude incidence rate of dementia in the 1971 cohort was 2.21 per 100 person-years (2.35 for males, 2.09 for females); in the 1980 cohort, the crude rate was 2.36 (2.33 for males, 2.39 for females). The standardized incidence ratio (SIR) of the 1980 cohort relative to the 1971 cohort was 1.00 for males and 1.09 for females. There was no significant difference in the incidence rate of dementia between the two cohorts (P . 0.05 in both sexes). Table 2 presents the age-specific incidence rates of dementia by sex in the two cohorts. Similar rates were observed for both sexes in the 1971 and 1980 cohorts, except for men in the age group 70–74 years (threefold higher in the 1980 cohort) and for women aged >85 years (1.5 times higher in the 1980 cohort). Mortality Incidence of dementia Among the first cohort (n = 2702), 386 subjects were newly diagnosed as having dementia. In the second cohort (n = 2926), 457 incident cases were detected during the follow-up period. In the 1971 cohort, most of the cases were coded as non-specific dementia (non-specific dementia: 97%, Alzheimer’s dementia: 2%), while in the 1980 cohort, the percentage of Alzheimer cases increased tenfold (non-specific dementia: 75%, Alzheimer’s dementia: 20%). Bias due to the misclassification of dementia In the 1971 cohort, 1057 people died during the follow-up period; and in the 1980 cohort, 1071 deaths were recorded. Table 3 shows the age-specific mortality rates by sex in the two cohorts. Within a decade, men have presented a decline in mortality rates at all ages, except after the age of 85 years in the 1980 cohort. Women also showed lower mortality rates before the age of 85 years in the second cohort. The standardized mortality ratio (SMR) in the second cohort relative to the first cohort, TRENDS IN DEMENTIA-FREE LIFE EXPECTANCY 1113 Table 2 Incidence rates for dementia per 100 person-years according to sex, age group, and cohort Males Females 1971–1979 Rate (95% CI) 1980–1988 Rate (95% CI) 1971–1979 Rate (95% CI) 65–69 0.22 (0.19–0.25) 0.30 (0.27–0.33) 0.48 (0.45–0.51) 0.00 70–74 0.32 (0.30–0.34) 0.89 (0.88–0.90) 0.67 (0.65–0.69) 0.68 (0.66–0.70) 75–79 1.66 (1.61–1.71) 1.76 (1.71–1.81) 1.65 (1.61–1.69) 1.39 (1.36–1.42) 80–84 3.01 (2.91–3.11) 2.84 (2.75–2.93) 2.97 (2.88–3.06) 2.68 (2.60–2.76) 85+ 6.10 (5.80–6.40) 5.52 (5.28–5.76) 3.82 (3.65–3.99) 5.68 (5.45–5.91) Age group (years) 1980–1988 Rate (95% CI) Table 3 Mortality rates per 100 person-years according to sex, age group, and cohort Males Females 1971–1979 Rate (95% CI) 1980–1988 Rate (95% CI) 1971–1979 Rate (95% CI) 1980–1988 Rate (95% CI) 65–69 1.95 (1.86–2.04) 1.48 (1.43–1.53) 1.43 (1.38–1.48) 1.47 (1.42–1.52) 70–74 4.04 (3.87–4.21) 2.97 (2.86–3.08) 1.92 (1.86–1.98) 2.00 (1.94–2.06) 75–79 6.30 (6.05–6.55) 4.57 (4.41–4.73) 2.89 (2.98–3.07) 2.80 (2.71–2.89) 80–84 8.79 (8.47–9.11) 7.57 (7.30–7.84) 5.46 (5.28–5.64) 3.92 (3.80–4.04) 11.95 (11.35–12.53) 12.36 (11.83–12.89) 8.98 (8.58–9.38) 9.08 (8.73–9.43) Age group (years) 85+ Table 4 Total life expectancy (TLE), dementia-free life expectancy (DemFLE), dementia life expectancy (DemLE) and per cent of life without dementia of the total life expectancy (%DemFLE) for selected ages according to sex and cohort 1971 cohort Age (years) 1980 cohort TLE DemFLE DemLE %DemFLE TLE DemFLE DemLE %DemFLE 65 16.71 15.92 0.79 95.27 18.11 16.93 1.18 93.48 70 13.30 12.58 0.72 94.59 14.47 13.38 1.09 92.47 75 10.38 9.72 0.66 93.64 11.29 10.31 0.98 91.32 80 7.95 7.35 0.60 92.45 8.61 7.75 0.86 90.01 85 5.97 5.46 0.51 91.46 6.43 5.69 0.74 88.49 90 4.41 3.97 0.44 90.02 4.69 4.08 0.61 86.99 95 3.20 2.84 0.36 88.75 3.36 2.86 0.50 85.12 65 21.12 18.82 2.30 89.11 21.48 19.63 1.85 91.39 70 17.33 15.19 2.14 87.65 17.47 15.74 1.73 90.10 75 13.98 12.00 1.98 85.84 13.87 12.30 1.57 88.68 80 11.05 9.29 1.76 84.07 10.73 9.36 1.37 87.23 85 8.59 7.04 1.55 81.96 8.11 6.94 1.17 85.57 90 6.56 5.24 1.32 79.88 5.97 5.01 0.96 83.92 95 4.94 3.84 1.10 77.73 4.30 3.53 0.77 82.09 Males Females was 0.87 for men (P , 0.01), and 0.91 for women (P , 0.05). In other words, mortality rates were significantly lower in the second cohort for both males and females. Health expectancies Table 4 shows the duration of TLE, DemFLE, DemLE and the percentage of life without dementia within the TLE on every 5-year age interval for each gender in both cohorts, and Figure 1 shows the trends of the three expectancies in both genders. Over the decade between the 1971 and 1980 cohorts, TLE has increased among males, especially at younger ages. In males aged 65 years old, TLE was 16.7 years in the 1971 cohort, and 18.1 years in the 1980 cohort. After the age of 85 years, TLE in both cohorts tended to be similar. The TLE for females younger than 80 years did not change. For females aged 65 years, TLE was 21.1 years in the first cohort and 21.5 in the second cohort. After the age of 75 years, TLE in the second cohort tended to be lower than in the first cohort. As compared with the 1971 cohort, DemFLE in the 1980 cohort increased in both males and females at younger ages. At 65 years old, men in the first cohort presented a DemFLE of 15.9 years, while in the second cohort at the same age, DemFLE 1114 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY Figure 1 Trends of total life expectancy (TLE), dementia-free life expectancy (DemFLE), and dementia life expectancy (DemLE) according to sex and cohort TLE 80–88 DemFLE 80–88 DemLE 80–88 TLE 71–79 DemFLE 71–79 DemLE 71–79 was 16.9 years. The DemFLE for 65-year-old men in the second cohort was longer than TLE itself for the same age in the first cohort. Women aged of 65 years in the first cohort had a DemFLE of 18.8 years, and in the second cohort a DemFLE of 19.6 years. After 80 years old, in both sexes, DemFLE in the 1971 and 1980 cohorts did not change. As shown in Figure 1 for males, trends of DemFLE in the second cohort and TLE in the first cohort overlapped. Within a decade, the DemFLE of the 1980 cohort reached the duration of TLE of the 1971 cohort. The percentage of life free from dementia within the total life (% DemFLE) decreased between the two cohorts among males, TRENDS IN DEMENTIA-FREE LIFE EXPECTANCY 1115 Figure 2 Median age of dementia onset according to sex, year of follow-up, and cohort —–■—– – –▲– – 1971 Cohort 1980 Cohort and increased among females. For males 65 years old in the 1971 cohort, DemFLE represented 95% of the TLE, and 93% in the 1980 cohort. For females at the same age in the first cohort, DemFLE represented 89% of the TLE, and in the second cohort 91%. Between the 1971 and 1980 cohorts, the duration of life with dementia presented an opposite trend between both genders: increasing in men and decreasing in women. For men aged 65 years in the first cohort, DemLE was 0.8 years, and in the second cohort DemLE reached 1.2 years. For women at 65 years old in the 1971 cohort, DemLE was 2.3 years, this duration decreased to 1.8 years in the 1980 cohort. Age of dementia onset The median age of dementia onset for each year of follow-up according to sex and cohort is presented in Figure 2. Because the age composition of the cohorts varied every year, a comparison of the onset age for each year of follow-up is more accurate than a comparison of the summarized onset age of the whole cohort. If TLE remains constant with time, a delay of the onset age observed in the second cohort is an indirect indicator of a compression of morbidity. Among males, no specific trend was noticed: a constant or delayed age of onset was observed for some years of follow-up, as well as an earlier age of onset in the second cohort for some other years. For 1116 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY Table 5 Relation between the number of years free from dementia and potential predictors of development of dementia determined by Cox proportional hazards model 1971–1979 cohort Variables No. 1980–1988 cohort RR (95% CI)a RR (95% CI)b No. RR (95% CI)a RR (95% CI)b Sex Female 1382 Male 1320 1467 1.00 (0.92–1.08) 1459 1.18 (1.09–1.29) 1276 1.01 (0.93–1.09) Age (years) >75 1467 ,75 1235 1650 1.18 (1.09–1.28) Education level Low 2380 High 322 2553 0.99 (0.87–1.13) 373 1.04 (0.93–1.17) Smoking status Current or past Never 753 1949 1924 0.98 (0.90–1.08) 1002 0.99 (0.91–1.07) Stroke history Yes 163 No 2539 209 1.30 (1.07–1.57) 1.27 (1.04–1.54) 1.06 (0.97–1.16) 1.03 (0.95–1.13) 2717 1.21 (1.02–1.42) 1.18 (1.00–1.40) 1.09 (1.00–1.18) 1.06 (0.98–1.16) CVDc history Yes 831 No 1871 1055 1871 Hypertension Yes 835 No 1867 1209 1.00 (0.91–1.09) 1717 1.02 (0.89–1.17) 2676 1.26 (0.89–1.80) 2885 1.04 (0.88–1.21) 2715 1.05 (0.97–1.13) Diabetes mellitus Yes 288 No 2414 250 1.06 (0.92–1.23) Parkinson’s disease Yes 46 No 2656 41 1.20 (0.83–1.72) Depression Yes 201 No 2501 211 1.08 (0.92–1.26) a (95%CI): crude relative hazard and 95% CI. b (95%CI): Relative hazard adjusted by sex and age and 95% CI. c Cardiovascular disease. females, the median age of dementia onset was postponed by 2–3 years. When examining the relation between potential predictors of dementia and dementia onset with the Cox proportional hazards model using older age group, low education level, and presence of specific medical conditions as the reference category (Table 5), we found that the absence of medical history of stroke increased significantly the number of years free from dementia (relative hazard [RH] = 1.30, P = 0.0083 in the 1971 cohort; RH = 1.21, P = 0.0269 in the 1980 cohort). A significant relation was also observed between dementia onset and the absence of cardiovascular disease in the second cohort (RH = 1.09, P = 0.0478). However, when adjusting for sex and age, the significance with cardiovascular disease disappeared (RH = 1.06, P = 0.1529). The other variables such as younger age, being male, having a high education level, being free from hypertension, or diabetes mellitus, or Parkinson’s disease, or depression, respectively, did not show any significant relation with the age of dementia onset in one or both cohorts. Discussion This paper presents chronological series of life expectancies without dementia among elderly Americans. Estimates of TLE and DemFLE were based on the longitudinal observation of two cohorts of elderly members of the same health maintenance organization. Trends in life expectancy and health expectancy over a 9-year period were examined. The results indicated that trends of increase in TLE and in DemFLE were quite different between the genders. The DemFLE increased at a slower rate than life expectancy among males. Consequently, DemLE increased in the second cohort and the %DemFLE decreased in the TRENDS IN DEMENTIA-FREE LIFE EXPECTANCY 1980 cohort. Conversely, for females, with a faster progression rate of DemFLE compared to TLE, the %DemFLE improved and the duration with dementia decreased in the second cohort. Before interpreting the findings, we should point out the three major limitations of this study. First, while the two cohorts were similar in terms of sex and age distribution, education level and frequency of outpatient visits, they differed in terms of race. The second cohort included less White subjects but more Black elderly. Differences in the dementia prevalence due to race are controversial. One study has reported a higher prevalence of dementia among Blacks,25 while two others showed no difference.26,27 Studies on race and incidence of dementia are scarce. The present report is consistent with a recent survey which found no significant difference in the incidence of dementia between the two races.27 Consequently, we may assume that the difference in the race distribution between the 1971 and the 1980 cohorts has not biased the comparison over time of the DemFLE. Second, in the KPMCP-NC, the mental status of the members was not routinely screened. The members had to visit the clinics in order to receive a dementia diagnosis. Some patients would be unable or reluctant to visit when their mental status declined; also, some cases would have been referred directly to nursing homes or kept at home without a diagnostic evaluation. Under these circumstances, some of the dementia cases would have been missed and, therefore, the incidence rate may have been underestimated. As we will describe later, however, the incidence of dementia in the populations we studied was consistent with those of two previous population-based studies among elderly Americans.28,29 Third, the attitude of both physicians and patients to dementia has changed over the decades; consequently, these changes may have affected the estimate of the rate of incidence of dementia. Diagnostic practices have varied between the 1970s and the 1980s. During the 1980s, the diagnostic criteria of dementia were established internationally and the definition of senile dementia appeared in DSM-III and ICD-9.30 Moreover, the development of standardized diagnostic interviews and mental examinations has improved the detection of dementing illnesses. The use of computer tomography scans and other imaging tools has increased dramatically between the two cohorts.23 Improvements in the detection of Alzheimer’s dementia are reflected in the dementia distribution among each cohort.31 Moreover, physicians have become more inclined to tell the patient and his/her family the true diagnosis. In addition, families of demented elderly patients are more aware of dementing illnesses, and seek greater medical and social support. These changes in physicians’ and patients’ attitudes may have resulted in increased number of diagnosis of dementia. However, the present data showed that the incidence of dementia did not change throughout the study period 1971–1988. The strength of the present study lies in the utilization of the same method among comparable populations. The calculation methods used in the 1971 and 1980 cohorts were identical, taking into consideration the incidence of dementia and mortality at the same time. The incidence of dementia in these two cohorts was consistent with the results of two previous reports of population-based studies in the US. Both studies showed higher incidence rate with older age. In the Rochester study, incidence rates increased from 1117 0.13 per 100 person-years for the age group 60–69 years to 2.18 for the elderly aged >80 years.29 In the Framingham study, the rates were lower than in the present report because the severity of dementia was restricted to moderate and severe cases.28 Between the first and the second cohorts, mortality decreased, especially among the males, while the incidence of dementia remained constant among both genders. Trends of increase in TLE and DemFLE were quite different between the two sexes. For males, although both TLE and DemFLE increased, the degree of increase was more remarkable in the former than in the latter. As a result, the duration to be spent with dementia or DemLE was prolonged and an extension of morbidity took place among the males. For females at younger ages, DemFLE increased by about one year under the relatively constant TLE. Thus, compression of morbidity was observed among females under 80 years of age. Women in their eighties presented a plateau in DemFLE; while women aged 85 years and over showed a decrease in both TLE and DemFLE, supporting an equilibrium. However, estimations for the oldest ages should be considered with the utmost caution since the probabilities of death and dementia in the life table were predicted by a logistic regression model according to the relationship between these events and age. The discrepancy between the actual value and the predicted value increases with age, thus the estimate becomes less reliable at older ages. The results of the present study indicate that, especially among females, DemFLE has grown in spite of a constant incidence rate of dementia. This fact could be explained by a postponement of dementia onset. In order to corroborate this trend, we have calculated the median age of dementia onset for each year of follow-up and have compared the results between both cohorts. Males did not show any specific trend but the median age of dementia onset was postponed by 2–3 years among females in the second cohort. The compression of morbidity among females was confirmed by the postponement of the median age of dementia onset in the 1980 cohort. A previous report on the same population has shown decreased incidence rates of stroke for females in the second cohort; while males up to 75 years of age presented increased rates.23 A decreased incidence rate of stroke, one of the risk factors for vascular dementia, may account for a later onset of dementia and partly explain the sex difference observed. The gender difference in the trends of DemFLE suggests to us that sex-related factors may account for the risk and prevention of dementia. According to previous studies, oestrogen use by post-menopausal women may postpone and decrease the risk of Alzheimer’s dementia.32,33 However, the use of oestrogen in these two age/time cohorts is low. Moreover, the effect of oestrogen replacement therapy on the risk of Alzheimer’s disease needs to be fully explored, since the results are still controversial.34,35 In line with previous studies on active life expectancy which reported a pandemic of disabilities,36,37 the present report shows, despite a stable incidence of dementia within a decade, a similar trend for dementia among men (i.e. an extension of the duration of life spent with dementia). A less pessimistic trend is observed among women, supporting a compression of dementia associated with a constant dementia incidence. The results suggest that in women of the present cohorts, the onset of dementia is delayed, although it is not fully prevented. 1118 INTERNATIONAL JOURNAL OF EPIDEMIOLOGY Acknowledgements The authors are grateful to Dr Gary Friedman, Director of the Kaiser Permanente Medical Care Program of Northern California Division of Research, for his support in this study. 18 Ritchie K, Mathers C, Jorm A. Dementia-free life expectancy in Australia. Aust J Public Health 1994;18:149–52. 19 Roelands M, van Oyen H, Baro F. Dementia-free life expectancy in Belgium. Eur J Public Health 1994;4:33–37. 20 Sauvaget C, Tsuji I, Minami Y et al. Dementia-free life expectancy among elderly Japanese. Gerontology 1997;43:168–75. References 1 Bachman DL, Wolf PA, Linn R et al. Prevalence of dementia and probable senile dementia of the Alzheimer type in the Framingham Study. Neurology 1992;42:115–19. 2 Canadian Study of Health and Aging Working Group. Canadian Study of Health and Aging: study methods and prevalence of dementia. Can Med Assoc J 1994;150:899–913. 3 Eastwood MR, Rifat SL, Roberts D. The epidemiology of dementia in North America. Eur Arch Psy Clin N 1991;240:207–11. 4 Evans DA, Funkenstein HH, Albert MS, Scherr PA, Cook NR, Chown 21 Haan MN, Selby JV, Quesenberry CP, Schmittdiel JA, Fireman BH, Rice DP. The impact of aging and chronic disease on use of hospital and outpatient services in a large HMO: 1971–1991. J Am Geriatr Soc 1997;45:667–74. 22 Verbrugge LM. Longer life but worsening health? Trends in health and mortality of middle-aged and older persons. Milbank Mem Fund Qly/Health Soc 1984;62:475–519. 23 Haan MN, Selby JV, Rice DP et al. Trends in cardiovascular disease incidence and survival in the elderly. Ann Epidemiol 1996;6:348–56. 24 Katz S, Branch LG, Branson MH, Papsidero JA, Beck JC, Greer DS. Active life expectancy. N Engl J Med 1983;309:1218–24. MJ. Prevalence of Alzheimer’s Disease in a community population of older persons. Higher than previously reported. JAMA 1989;262: 2551–56. 25 Heyman A, Fillenbaum G, Prosnitz B, Raiford K, Burchett B, Clark C. 5 Gauthier S, McDowell I, Hill G. Canadian Study of Health and Aging 26 Schoenberg BS, Anderson DW, Haerer AF. Severe dementia. Preval- (CaSHA). Psychiatr J Univ Ottawa 1990;15:227–29. 6 Kramer M, German PS, Anthony JC, Von Korff M, Skinner EA. Patterns of mental disorders among the elderly residents of Eastern Baltimore. J Am Geriatr Soc 1985;33:236–45. 7 Robertson D, Rockwood K, Stolee P. The prevalence of cognitive impairment in an elderly Canadian population. Acta Psychiat Scand 1989;80:303–09. 8 Weissman MM, Myers JK, Tischler GL et al. Psychiatric disorders (DSM-III) and cognitive impairment among the elderly in a US urban community. Acta Psychiatr Scand 1985;71:366–79. 9 Lilienfeld DE, Perl DP. Projected neurodegenerative disease mortality in the United States, 1990–2040. Neuroepidemiology 1993;12:219–28. 10 Robine J-M, Ritchie K. Healthy life expectancy: evaluation of global indicator of change in population health. Br Med J 1991;302: 457–60. 11 Kramer M. The rising pandemic of mental disorders and associated chronic diseases and disabilities. Acta Psychiatr Scand 1980;62: 382–97. 12 Fries JF. Aging, natural death, and the compression of morbidity. N Engl J Med 1980;303:130–35. 13 Fries JF. The compression of morbidity: near or far? Milbank Q 1989; 67:208–32. 14 Manton KG. Changing concepts of morbidity and mortality in the elderly population. Milbank Q 1982;60:183–244. 15 Perenboom RJM, Boshuizen HC, Breteler MMB, Ott A, van de Water HPA. Dementia-free life expectancy (DemFLE) in The Netherlands. Soc Sci Med 1996;43:1703–07. 16 Ritchie K, Jagger C, Brayne C, Letenneur L. Dementia-free life Estimated prevalence of dementia among elderly black and white community residents. Arch Neurol 1991;48:594–98. ence and clinical features in a biracial US Population. Arch Neurol 1985;42:740–43. 27 Fillenbaum GG, Heyman A, Huber MS et al. The prevalence and 3-year incidence of dementia in older black and white community residents. J Clin Epidemiol 1998;51:587–95. 28 Bachman DL, Wolf PA, Linn RT et al. Incidence of dementia and prob- able Alzheimer’s Disease in a general population: the Framingham Study. Neurology 1993;43:515–19. 29 Schoenberg BS, Kokmen E, Okasaki H. Alzheimer’s Disease and other dementing illnesses in a defined United States population: incidence rates and clinical features. Ann Neurology 1987;22:724–29. 30 Ritchie K. International comparisons of dementia-free life expectancy: a critical review of the results obtained. In: Mathers C, McCallum J, Robine J-M (eds). Advances in Health Expectancies: Proceedings of the 7th Meeting of the International Network on Health Expectancy (REVES), Canberra, February 1994. Australian Institute of Health and Welfare: AGPS, Canberra, 1994, pp.271–79. 31 Fox P. From senility to Alzheimer’s Disease: the rise of the Alzheimer’s Disease movement. Milbank Q 1989;67:58–102. 32 Tang M-X, Jacobs D, Stern Y et al. Effect of oestrogen during meno- pause on risk and age of onset of Alzheimer’s Disease. Lancet 1996; 348:429–32. 33 Paganini-Hill A, Henderson VW. Estrogen deficiency and risk of Alzheimer’s Disease. Am J Epidemiol 1994;140:256–61. 34 Haskell SG, Richardson ED, Horwitz RI. The effect of estrogen replacement on cognitive function in women: a critical review of the literature. J Clin Epidemiol 1997;50:1249–64. 35 Yaffe K, Sawaya G, Lieberburg I, Grady D. Estrogen therapy in postmenopausal women: effects on cognitive function and dementia. JAMA 1998;279:688–95. expectancy: preliminary calculations for France and the United Kingdom. In: Robine J-M, Mathers C, Bone M, Romieu I (eds). Calculation of Health Expectancy: Harmonization, Consensus Achieved and Future Perspectives. Colloques INSERM/John Libbey Eurotext Ltd 1993;226:233–44. 36 Crimmins EM, Saito Y, Ingegneri D. Changes in life expectancy 17 Ritchie K, Robine J-M, Letenneur L, Dartigues J-F. Dementia-free life 37 van de Water HPA, Boshuizen HC, Perenboom RJM. Health expect- expectancy in France. Am J Public Health 1994;84:232–36. and disability-free life expectancy in the United States. Population and Development Review 1989;15:235–67. ancy in the Netherlands 1983–1990. Eur J Public Health 1996;6:21–28.