for Qualified Grantee(s)")
Minnesota Department of Human Services
Health Care Administration
Request for Proposals for Qualified
Grantee(s) to Provide Health Care Services
to Medical Assistance and MinnesotaCare
Enrollees Under Alternative Payment
Arrangements Through the Integrated
Health Partnerships (IHP) Demonstration
Date of Publication: April 25th, 2016
Americans with Disabilities Act (ADA) Statement: This information is available in
accessible formats for people with disabilities by calling 651-431-2202 or by using
your preferred relay service. For other information on disability rights and
protections, contact your agency’s Americans with Disabilities Act (ADA)
coordinator.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 1 OF 33
Table of Contents
I. Introduction....................................................................................................................................4
A. Purpose of Request .................................................................................................................................... 4
B. Objective of this RFP .................................................................................................................................. 4
C. Background................................................................................................................................................. 4
1.
General ............................................................................................................................................... 4
2.
Eligible Populations ............................................................................................................................ 5
3.
Excluded Populations ......................................................................................................................... 5
4.
Other Information .............................................................................................................................. 6
II. Scope of Work................................................................................................................................6
A. Overview .................................................................................................................................................... 6
1.
System Requirements ........................................................................................................................ 7
2.
Overview of Payment Models and Risk ............................................................................................. 8
3.
Definitions of Total Cost of Care ...................................................................................................... 11
4.
Attribution Methodology ................................................................................................................. 11
5.
Quality Measures ............................................................................................................................. 12
6.
Interaction with Medicaid Managed Care Organizations (MCOs) ................................................... 13
7.
IHP Access to Data ........................................................................................................................... 13
8.
Learning Opportunities .................................................................................................................... 14
B. Tasks/Deliverables.................................................................................................................................... 14
III. Proposal Format..........................................................................................................................14
A. Required Proposal Contents .................................................................................................................... 15
B. Proposal Requirements ............................................................................................................................ 16
1.
Executive Summary:......................................................................................................................... 16
2.
Description of the Applicant Delivery System: ................................................................................ 16
3.
Description of MHCP Population Served by the Delivery System: .................................................. 17
4.
Proposed Payment Arrangement: ................................................................................................... 17
5.
Quality Measures: ............................................................................................................................ 19
6. Minnesota Accountable Communities for Health Continuum of Accountability Matrix Assessment
Tool: ......................................................................................................................................................... 20
D. Required Statements ............................................................................................................................... 20
IV. RFP Process.................................................................................................................................25
A. Timeline .................................................................................................................................................... 25
2017 IHP RFP – APRIL 25TH, 2016
PAGE 2 OF 33
B. Optional Individual Question and Answer Sessions ................................................................................. 25
C. Responders’ Questions............................................................................................................................. 26
D. Proposal Submission ................................................................................................................................ 26
V. Proposal Evaluation and Selection ................................................................................................27
A. Overview of Evaluation Methodology ..................................................................................................... 27
B. Evaluation Team ....................................................................................................................................... 27
C. Evaluation Phases ..................................................................................................................................... 27
1.
Phase I – Required Statements Review ........................................................................................... 28
2.
Phase II - Evaluation of Technical Requirements of Proposals. ....................................................... 28
3.
Phase III - Selection of the Successful Responder(s) ........................................................................ 28
D. Contract Negotiations and Unsuccessful Responder Notice ................................................................... 28
VI. Required Contract Terms and Conditions .....................................................................................29
VII. State’s Rights Reserved ..............................................................................................................32
Appendices ......................................................................................................................................33
2017 IHP RFP – APRIL 25TH, 2016
PAGE 3 OF 33
I. Introduction
The goal of the Integrated Health Partnerships (IHP) demonstration is to improve the quality and value of
the care provided to the citizens served by public health care programs. This Request for Proposal (RFP)
solicits a response from organizations interested in participating in the Integrated Health Partnership
program. The demonstration creates an “Integrated Health Partnership” structure for provider
organizations to voluntarily contract with the Minnesota Department of Humans Services (DHS) to care for
Minnesota Health Care Programs (MHCP) recipients in both fee-for-service (FFS) and managed care under a
payment model that holds these organizations accountable for the total cost of care and quality of services
provided to this population. Within this structure, DHS seeks to expand demonstration projects in different
geographic regions of the state and across different models of care delivery that will integrate health care
with chemical and mental health services, safety net providers, and social service agencies. The projects will
include clear incentives for quality of care and targeted savings, and will result in increased competition in
the marketplace through direct contracting with providers.
A. Purpose of Request
The Minnesota Department of Human Services, through its Health Care Administration (State), is seeking
Proposals from qualified Responders to test alternative and innovative health care delivery systems serving
MHCP recipients.
Minnesota Statutes § 256B.0755 directs the State to solicit proposals to test alternative and innovative
health care delivery systems that provide services to a specified patient population for an agreed-upon
total cost of care or risk/gain sharing payment arrangement. It also states that the request for proposals
should be developed in consultation with hospitals, primary care providers, health plans, and other key
stakeholders.
B. Objective of this RFP
The objective of this RFP is to contract with qualified Responders to perform the tasks and services set forth
in this RFP. It is anticipated that any contract awarded under this RFP will have a start date of January 1,
2017, and an initial term of one year. Thereafter, the Commissioner of Human Services may choose to
renew any contract awarded under this RFP annually.
Proposals must be submitted by 4:00 p.m. Central Time on August 19, 2016. This RFP does not obligate
the State to award a contract or complete the project, and the State reserves the right to cancel the
solicitation if it is considered to be in its best interest. All costs incurred in responding to this RFP will be
borne by the Responder.
C. Background
1.
General Under the authority of Minnesota Statutes § 256B.0755, the State is soliciting proposals
for Responders to participate in alternative payment arrangements for health care services on a
statewide basis as an IHP. The proposed IHP will serve the population of non-dually eligible adults
and children in Medical Assistance and MinnesotaCare enrolled under both fee-for-service and
managed care programs.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 4 OF 33
2.
3.
Eligible Populations The following persons who are recipients of Medical Assistance and
MinnesotaCare are eligible for attribution to the IHP:
a.
Medical Assistance Enrollees – Including pregnant women, children under 21, and adults
without children.
b.
MinnesotaCare Enrollees – Including pregnant women, children under 21, and adults
without children. Individuals must belong to an eligible group under Minnesota Statutes,
Chapter 256L, and meet income criteria, satisfy all other eligibility requirements, and pay a
premium to the State.
c.
Recipients receiving Medical Assistance due to blindness or disability, as determined by the
U.S. Social Security Administration or the State Medical Review Team, who are not dually
eligible for Medicare.
Excluded Populations The following persons are excluded from attribution to the IHP:
1.
Recipients receiving Medical Assistance who are dually eligible for Medicare.
2.
Recipients receiving Medical Assistance under the Refugee Assistance Program pursuant
to 8 U.S.C. 1522(e).
3.
Individuals who are Qualified Medicare Beneficiaries (QMB), as defined in Section 1905(p)
of the Social Security Act, 42 U.S.C. 1396d (p), who are not otherwise receiving Medical
Assistance.
4.
Individuals who are Service Limited Medicare Beneficiaries (SLMB), as defined in Section
1905(p) of the Social Security Act, 42 U.S.C. 1396a(a)(10)(E)(iii) and 1396d(p), and who are
not otherwise receiving Medical Assistance.
5.
Non-citizen recipients who only receive emergency Medical Assistance under Minnesota
Statutes, section 256B.06, subd. 4.
6.
Recipients receiving Medical Assistance on a medical spend down basis.
7.
Medical Assistance recipients with cost-effective employer-sponsored private health care
coverage, or who are enrolled in a non-Medicare individual health plan determined to be
cost-effective according to Minnesota Statutes, section 256B.69, subd. 4, (b)(9).
8.
Medical Assistance recipients with private health care coverage through a Health
Maintenance Organization (HMO) licensed under Minnesota Statutes, Chapter 62D.
9.
MinnesotaCare recipients who are enrolled in the Healthy Minnesota Contribution
Program.
10.
The commissioner may exclude recipients enrolled in Minnesota Senior Care Plus (MSC+),
other than those in section 1 above.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 5 OF 33
(b) Excluded Populations from Total Cost of Care. The following persons are excluded from the
Total Cost of Care (TCOC) Performance Assessment Process.
1.
4.
Recipients for whom DHS receives incomplete claims data due to third-party liability
coverage.
Other Information
•
Minnesota Health Care Programs Fact Sheet
https://edocs.dhs.state.mn.us/lfserver/Public/DHS-4932-ENG
•
Center for Medicare and Medicaid Innovation Models
http://innovations.cms.gov
•
IHP website and RFI Responses
http://www.dhs.state.mn.us/provider/HCDeliveryDemo
•
Minnesota Health Reform Initiative
http://www.health.state.mn.us/healthreform
Attachments Included:
A. 2017 Integrated Health Partnerships (IHP) Model Base Contract and Attachments (Appendix A
of this document)
B. DHS IHP Provider Portal (Appendix B of this document)
C. Sample Provider Roster and Roster Reference Guide (Appendix C of this document)
D. SIM Minnesota Accountable Communities for Health Continuum of Accountability Matrix
Assessment Tool (Appendix D of this document)
II. Scope of Work
A. Overview
This RFP provides background information and describes the services desired by the State. It delineates the
requirements for this procurement and specifies the contractual conditions required by the State. Although
this RFP establishes the basis for Responder Proposals, the detailed obligations and measures of
performance will be defined in the final negotiated contract.
The purpose of the IHP demonstration is to provide opportunities for providers and other organizations to
develop innovative forms of care delivery under shared savings and loss payment arrangements that reduce
the cost of care, improve health outcomes, and improve patient experience. The demonstration will be
conducted over three-year contract cycles with annual performance periods. The demonstration will be
conducted statewide and is not limited to providers or MHCP participants in a specified geographic area.
MHCP participants included in the demonstration are non-dually eligible Medical Assistance and
MinnesotaCare enrollees attributed to the IHP for the performance period.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 6 OF 33
1.
System Requirements
To be considered eligible to participate as an IHP for the purposes of responding to this RFP, a successful
Responder must meet the following criteria:
a.
Provide the full scope of primary care, and adopt methods of care delivery so that the full
scope of primary care is provided and care is coordinated across the spectrum of services
provided.
b.
All providers included in the IHP demonstration payment model must be enrolled MHCP
providers.
c.
Demonstrate, through the care delivery model, how the IHP will affect the total cost of care
of its MHCP participants regardless of whether the services are delivered by the IHP.
d.
Demonstrate how formal and informal partnerships with community-based organizations,
social service agencies, counties, public health resources, etc. are included in the care
delivery model. Responders are encouraged to propose mechanisms to incorporate these
organizations directly into the payment model.
e.
Demonstrate how the IHP will engage and coordinate with other providers, counties, and
organizations, including county-based purchasing plans that provide services to the IHP’s
patients on issues related to local population health, including applicable local needs,
priorities, and public health goals. Responders should describe how local providers,
counties, organizations, county-based purchasing plans, and other relevant purchasers
were consulted in developing the application to participate in the demonstration project.
f.
Demonstrate how the IHP will meaningfully engage patients and families as partners in the
care they receive, as well as in organizational quality improvement activities and leadership
roles.
g.
Demonstrate established processes to monitor and ensure the quality of care provided.
Participate in quality measurement activities as required by the State and engage in quality
improvement activities.
h.
Demonstrate the capacity to receive data from the State via secure electronic processes
and use it to identify opportunities for patient engagement and to stratify its population to
determine the care model strategies needed to improve outcomes.
i.
Nothing in the contract agreement will obviate all providers included in the IHP from
meeting all MHCP fee-for-service and/or managed care organization (MCO) requirements
including, but not limited to enrollment, reporting, claims submission, and quality
measures.
IHPs will not administer the MHCP benefit set or pay claims under the demonstration or be required to
contract for additional services outside of the services delivered by the IHP.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 7 OF 33
An IHP may include an organizing entity and agreement of shared governance. This may include but is not
limited to a non-profit or a county or group of counties; however any IHP payments must be provided to
and/or received from an MHCP enrolled provider identified in section III.B.4.c of this RFP by the IHP.
2.
Overview of Payment Models and Risk
Organizations that meet the system requirements described above are eligible to participate in either a
Virtual or Integrated payment mode as described below. Eligibility for each payment model will be
determined by the integration and scope of services provided by the IHP as described below.
The payment models outlined are based on IHP performance against a risk-adjusted total cost of care target
for all qualifying MHCP participants attributed to the IHP for the performance period. The total cost of care
target will be calculated using risk-adjusted MHCP fee-for-service claims and encounter claims submitted by
managed care organizations (MCOs) under contract with the State. IHP financial incentives under the
demonstration related to reducing total costs will be contingent on performance on quality and patient
experience outcomes. All shared savings and losses payments under the models described below will be
calculated and disbursed annually via a reconciliation payment. Providers will continue to receive the
current MHCP fee-for-service or MCO contracted payment during the performance period. Responders are
encouraged to involve community organizations, local public health, behavioral health or long term care
service providers in the distribution of shared savings and losses payments as defined in Sections III and IV,
and bonus points are available for such arrangements.
DHS is committed to a credible and fair risk-sharing and performance measurement process. In developing
the initial IHP model analytics, DHS compiled a significant amount of stakeholder and expert feedback and
performed a variety of analyses to develop the initial proposed payment model. During previous IHP
negotiation and contract development processes, the payment model was refined based on additional
research, actuarial analyses and feedback, and is described below and in the supplementary
documentation.
To assure the credibility of the process during the three year contract cycles of the project, the payment
models and process as described below may be subject to mutually agreed-upon modifications based on
additional DHS research, emerging findings or feedback from the participating IHPs. In April 2016, DHS
released a Request for Information (RFI) to solicit feedback on certain aspects of the IHP demonstration.
Response to this RFP does not preclude IHPs from being able to respond to the RFI or from participation in
future demonstrations or alternative models that arise as a result of the RFI process in the future.
a. Type of Models
Model 1: Virtual IHP
i.
Provider organizations eligible for the Virtual IHP payment model include primary care
providers and/or multi-specialty provider groups that are not formally integrated with a
hospital or integrated system via aligned financial arrangements and common clinical and
information systems. Provider organizations with an MHCP population between 1,0001,999 attributed participants are eligible only for the Virtual IHP model, regardless of their
level of formal integration.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 8 OF 33
ii.
The payment model is a shared savings model that will distribute the difference between
annual expected and actual realized total cost of care if savings are achieved, a portion of
which is contingent on quality and patient experience outcomes.
Model 2: Integrated IHP
i.
Provider organizations eligible for the Integrated IHP include an integrated delivery system
that provides a broad spectrum of outpatient and inpatient care as a common financial and
organizational entity. Provider organizations must serve an MHCP population of 2,000
attributed participants or greater in order to be eligible for the integrated model.
ii.
The payment model incorporates shared risk over time and builds toward a two-way risk
sharing model that distributes the difference between the annual expected and actual
realized total cost of care whether savings are achieved or not, a portion of which is
contingent on quality and patient experience measures.
iii.
Responders are required to propose the amount of risk for the MHCP population attributed
to the IHP for the purposes of this RFP. The basic terms of the risk sharing agreement are
outlined below. In responding to this RFP, IHPs will be required to propose their risk sharing
arrangement within these parameters.
b. Total Cost of Care (TCOC) Performance Assessment Process
IHP performance assessment is based on a comparison of the observed TCOC for each performance period
(Calendar Year (CY) 2017, CY2018, and CY2019) to a “TCOC Target.” The TCOC Target is based on a base
period TCOC (CY2016) after adjusting for expected trend and changes in attributed population size and
relative risk from the base period to the performance periods. The target is expressed as a “per member
per month” (PMPM) value.
The Base Period Attributed Population will be developed for each IHP using 2016 claims, MCO encounter
data, and the attribution process as described in this RFP. Using this attributed population, the Base Period
Total Cost of Care (Base TCOC) will be developed using the services as outlined in Section II.A.3 in this RFP.
Claims for an individual member that fall outside of pre-determined thresholds will be capped to adjust the
PMPM results to exclude “catastrophic cases” and better reflect the IHP’s target population. In addition,
the Base Period Risk Score will be assessed for the assigned members, using the Johns Hopkins ACG® risk
adjustment tool to determine the relative risk of the base population. In addition to developing weights
based exclusively on the services included in the Base TCOC, the weights used to assess the risk of the
population will be calculated using the pre-determined claim caps to adjust the weights and reduce the
impact of catastrophic cases.
Early in each performance period, DHS will develop an Expected Trend rate for the total cost of care based
on the trend rates used to develop the annual expected cost increases for the aggregate MHCP population,
with appropriate adjustments for services excluded from the Base TCOC or other factors that are applicable
to the total cost of care and goals of the program. An initial TCOC Target for the upcoming performance
period can be established using the Base TCOC and Expected Trend. The target will ultimately be adjusted
for the relative risk of the actual population attributed to the IHP in the performance period.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 9 OF 33
At the end of each performance period, DHS will determine the Performance Period Attributed Population
using retrospective claims data and the attribution process as described in this RFP. In addition, the
Performance Period Total Cost of Care (Performance TCOC) will be developed, adjusting for any claims for
an individual member that fall outside of pre-determined catastrophic case thresholds. The risk score for
the measurement period’s attributed population will be used to calculate the change in relative risk from
the base period to the performance period. Using the change in relative risk, the Target TCOC will be
adjusted based on the increase or decrease in the risk of the attributed populations. The Adjusted Target
TCOC will be compared to the Performance TCOC for purposes of determining the performance results and
the basis for the calculation of shared savings and losses.
c. Total Cost of Care Performance Measurement Specifications and Requirements
To assure that a participating IHP does not have the measurement of their performance inappropriately
impacted by changes in the risk status of the membership, DHS will perform risk adjustment on the
attributed populations in the base period and performance period and adjust the Target TCOC (the “Adj.
Target TCOC”) to reflect the changes in risk. To further refine the measurement process and reduce the
potential variability inherent in any risk score methodology, DHS has developed the following specifications
and requirements:
1. Population sizes: Successful Responders must meet a minimum attributed MHCP population size of
1,000 members. For purposes of developing the risk arrangements, DHS is defining the following
MHCP sizes:
a. Small Population – 1,000 to 1,999 attributed patients (Eligible for Virtual model only)
b. Medium Population – 2,000 to 4,999 attributed patients
c. Large Population – more than 5,000 attributed patients
2. Claim cap levels: To reduce the potential variability of the risk assessment process and the financial
results, DHS will develop the risk scores and total cost of care PMPM by removing the claim costs
for individual members that fall above specific thresholds. Because of the greater impact of large
claimants on the results for smaller populations, DHS developed the following general guidelines
for managing catastrophic risk:
a. Small Population – $50,000 maximum annual claims per patient
b. Medium Population – $100,000 maximum annual claims per patient
c. Large Population – $200,000 maximum annual claims per patient
3. Minimum Performance Thresholds: DHS has established a two percent (2%) minimum performance
threshold that must be met prior to the distribution of any shared savings or losses payments
between the State (including its contracted MCOs, as applicable) and the IHP. Specifically, the
Performance TCOC must be above 102% or below 98% of the Adj. Target TCOC in the Integrated
IHP for shared savings and losses payments to occur. A Virtual IHP will not receive any shared
savings unless their Performance TCOC is below 98% of the Adj. Target TCOC. Once the
performance target is met, shared savings or shared losses payments are calculated back to the
first dollar, i.e., any amount above or below the TCOC target.
4. Shared Savings and Shared Losses Payment Distributions: DHS is requiring Integrated IHP
Responders to propose their preferred performance thresholds for shared savings or shared losses
between DHS and the IHP, within some specified parameters. The performance threshold
2017 IHP RFP – APRIL 25TH, 2016
PAGE 10 OF 33
parameters gradually incorporate two-way risk sharing and increased flexibility for IHPs over the
three years of the demonstration. The parameters for each year are as follows:
a. Performance Period 1: IHP shares any savings equally (50/50) with the State/MCOs provided
the 2% minimum performance threshold has been achieved. The maximum threshold for
shared savings in Performance Period 1 must be the same in Performance Period 3 and is
limited to a maximum of 85% of the TCOC Target.
b. Performance Period 2: IHP assumes some downside risk, but it need not be symmetrical to the
proposed shared savings threshold. The IHP has some discretion around the amount of risk it is
willing to bear, but the ratio of shared savings thresholds to shared loss thresholds must be 2:1.
For example, if the IHP wishes to avoid risk for claims above 106% of the TCOC Target, the
maximum threshold for shared savings is 88% (6 percentage points x 2 = 12) below the TCOC
Target. All shared savings and shared losses are distributed equally (50/50) with the
State/MCOs.
c. Performance Period 3: IHP assumes two-way risk with symmetrical risk sharing thresholds. For
example, if an IHP wishes to avoid risk at 115% of the TCOC Target, the maximum threshold for
shared savings must be 85%. An IHP may elect different distributions of shared savings and
shared losses within the proposed thresholds. The maximum threshold for shared savings in
Performance Period 3 must be the same as in Performance Period 1 and is limited to a
maximum of 85% of the TCOC Target (see section 2.3 of Attachment B-1 of the model contract
in Appendix A of this document, for specific requirements and additional detail).
d. Virtual IHPs: Note that a Virtual IHP does not have the option of proposing a schedule and will
be required to share any savings (once the 2% minimum performance threshold is met) equally
(50/50) with the State for all three years of the demonstration.
3.
Definitions of Total Cost of Care
The two payment models will use the same methodology and categories of service to calculate the riskadjusted Total Cost of Care (TCOC) target. TCOC will be calculated by the State for all MHCP recipients in
both fee-for-service and managed care attributed to the IHP for the performance period. Further detail on
the categories of service included and the specific procedure codes included in each category is provided in
Attachment E: Core Services of the IHP model contract included as an attachment to this RFP. The State
reserves the right to modify the services included in the total cost of care calculation under this RFP. The
Responder may propose additional Medicaid covered services for inclusion in the TCOC target. The
Responder should detail in their proposal any additional services beyond the core set by major category of
service and procedure code.
4.
Attribution Methodology
MHCP participants will be attributed by the State to an IHP using retrospective claims data for the purposes
of determining the TCOC Target and actual Performance TCOC. Participants will be attributed to one IHP at
a time. All of the attributed participants’ care as provided in the total cost of care definition will be
attributed to the IHP, regardless of whether the IHP delivered the services.
An interim attributed population will be determined early in the performance period and shared with the
IHP. The final attributed population for the performance period will be re-calculated following 12 months of
2017 IHP RFP – APRIL 25TH, 2016
PAGE 11 OF 33
claims run-out for purposes of accountability under the payment models. Attribution will be done using a
hierarchical process that incents active outreach and retention of patients by the IHP under the following
general methodology:
E. 1st – Participants actively enrolled in care coordination through a certified Health Care Home (HCH)
submitting a monthly care coordination claim.
F. 2nd – Participants that cannot be attributed based on HCH enrollment may be attributed to the IHP
based on the number of Evaluation and Management (E&M) visits (i.e., encounters) with provider
who specializes in primary care.
G. 3rd – Participants that cannot be attributed through primary care visits may be attributed to the IHP
based on their E&M visits with non-primary care (specialty) providers.
If a Participant was not enrolled with a HCH and did not have any E&M claims within the relevant twelve
(12) month period and therefore were not attributed to an IHP, then the attribution process described
above will be repeated using claims occurring within an additional twelve (12) month period, for a total of
twenty-four (24) months.
Because the results of the attribution method will impact the size of the population included in each IHP’s
demonstration payment model, the State and Responder will define contract terms based on subsequent
analysis of which participants are actually attributable.
5.
Quality Measures
1. Shared savings under the payment models for IHPs will be contingent in part on clinical quality and
patient experience measure results. The State will align quality measures across demonstrations
and with existing measures and data collection under the Statewide Quality Reporting and
Measurement System (Minnesota Statutes § 62U.02), and Health Care Home Outcomes (Minnesota
Statutes § 256B.0751, subd. 6). The core set of quality measures, reporting specifications, and the
benchmarking and scoring methodology are provided in detail in Attachment F: Quality and Patient
Experience Measures of the IHP model contract included as Appendix A to this RFP. Performance
on quality measures will impact the amount of shared savings (if any) achieved by each IHP and is
phased in over the three year demonstration as follows:
a. Performance Period 1: 25% of IHP portion of shared savings based on reporting measures.
b. Performance Period 2: 25% of IHP portion of shared savings based on performance.
c. Performance Period 3: 50% of IHP portion of shared savings based on performance.
2. The State will determine preliminary minimum and maximum attainment thresholds for each
measure for all IHPs under the demonstration before the beginning of Performance Periods 2 and 3
and will post them on the DHS website. The State will notify the IHP of final thresholds upon final
calculation using the data based on the most recent quality measurement periods.
3. In addition to the core set of measures defined by the State, successful Responders are encouraged
to propose additional measures and to demonstrate how the additional measures apply to the
specific communities and/or population served by the IHP. These measures can include specific
health outcomes measures, patient experience measures, or measures of overall population health.
Proposed additional measures are subject to approval by the State. Guidelines for additional
measures include:
2017 IHP RFP – APRIL 25TH, 2016
PAGE 12 OF 33
a. The measure must utilize a state or nationally recognized quality measure specification.
b. The data must be able to be collected by a third party using an existing data collection
mechanism.
c. The data must be validated and audited by a third party.
d. The measure must not be impacted by high variability due to coding changes.
e. The measure must assess healthcare processes and/or outcomes desirable for the IHP
population.
6.
Interaction with Medicaid Managed Care Organizations (MCOs)
The IHP demonstration will be implemented consistently at the delivery system level and for MHCP
participants currently enrolled in either fee-for-service and managed care. The State will implement and
execute the IHP payment model, quality measures and methodology, patient attribution for both MHCP
enrollees in fee-for-service and in MCOs under contract with the State to provide services to non-dually
eligible Medical Assistance and MinnesotaCare enrollees. The MCOs will participate as a payer in the IHP
payment process via their contract requirement with the State.
MHCP participants will be attributed to an IHP regardless of whether they are enrolled in fee-for-service or
in an MCO. All attributed participants will be calculated together at the IHP level for the purposes of the
Total Cost of Care and the payment model. The State will calculate the total cost of care targets and the
shared savings or losses payment across both fee-for-service and managed care using retrospective claims
and encounter data. The State will also calculate the quality measures and overall score using data
applicable to each measure. The State and its contracted MCOs, as applicable, will each pay its portion of
the shared savings payments to the IHP (or the State and its contracted MCOs will receive shared losses
payments from the IHP).
MCOs (licensed health plans or County-Based Purchasing Organizations) may not participate as principal
Respondents in the IHP demonstration.
7.
IHP Access to Data
DHS will make utilization and risk information for its attributed population available to IHP providers via
DHS’ IHP and MN-ITS data portals. The data will be populated by a monthly set of risk adjustment (Johns
Hopkins Adjusted Clinical Groups [ACG®]) output in the DHS data warehouse, and will include both fee-forservice and MCO encounter claim data. Data will be as timely as possible given standard claims lag, and will
be available via risk adjustment software output or standardized reports.
Key variables available to delivery systems will be primarily from ACG® output, and will include populationlevel data (such as the total cost of care and rates of inpatient and emergency department utilization) and
participant-level data (such as medical and pharmacy utilization histories, predictive risk information, and
indices of care coordination).
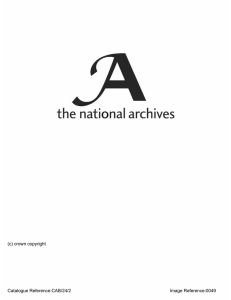
The data in the portals will be provided in raw exportable form for IHP use, but will also be provided in
easily digestible reports and visual graphics. Examples can be found in Appendix B, DHS IHP Provider Portal.
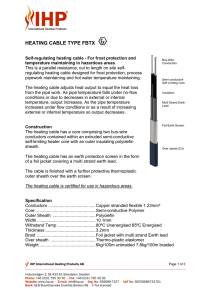
A few examples of the features and reports provided through the DHS IHP Provider Portal are:
2017 IHP RFP – APRIL 25TH, 2016
PAGE 13 OF 33
• Performance Dashboard (see Figure 1)
• Total Cost of Care Summary (Breakdowns by Category
of Service, inside system vs. outside system, included
versus excluded services, by member program, etc)
• Care Coordination Reports (Care Management
Reports, Chronic Condition Profile, Provider Roster
Gaps, and Attribution Change Analysis)
• Utilization Reports (Inpatient & ED Trends by Clinic,
Pharmacy Utilization and Spend)
• Quality Reports (HEDIS Measures, Summary of Quality
and Patient Experience Measures)
8.
Figure 1: Performance Dashboard
Learning Opportunities
IHPs are invited to participate in Quarterly Data Users Group Meetings with DHS. DHS may present on data
related topics, answer questions, and facilitate data-related discussions amongst IHPs. Data Users Group
meetings are an opportunity for IHPs to communicate and collaborate with the state and one another.
IHPs are also invited to participate in the annual IHP Learning Day. The IHP Learning Day is a forum to
discuss key issues, potential strategies, and future opportunities for IHPs.
B. Tasks/Deliverables
Successful Responders will:
1. Demonstrate innovative care models and community coordination, integration or linkages.
2. Describe the care model, programs and strategies and demonstrate how they will impact the total
cost of care, clinical quality, and patient experience outcomes.
3. Agree to the requirements and structure defined in the RFP and the Model Contract in Appendix A
of this document.
4. Agree to enter into a three-year demonstration with DHS, with at least annual opportunities to renegotiate key contract provisions.
5. Propose the nature of the shared savings and/or losses arrangement, including the amount and
distribution of shared savings and losses, within the guidelines laid out in the RFP.
6. Provide an estimated population size included in IHP to verify minimum population participation
requirements.
III. Proposal Format
Proposals must conform to all instructions, conditions, and requirements included in the RFP. Responders
are expected to examine all documentation and other requirements. Failure to observe the terms and
conditions in completion of the Proposal are at the Responder’s risk and may, at the discretion of the State,
result in disqualification of the Proposal for non-responsiveness. Acceptable Proposals must offer all
services identified in Section II - Scope of Work and agree to the contract conditions specified throughout
the RFP.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 14 OF 33
A. Required Proposal Contents
Within the guidelines laid out in the Scope of Work above, Responders must describe their care model
capabilities and propose specific elements of the demonstration payment model. Proposals should adhere
to the following format:
1. Table of Contents
2. Proposal Requirements
a.
b.
c.
d.
e.
f.
g.
Executive Summary
Description of the Applicant Delivery System
Description of Care Models
Description of Community Partnerships
Description of Patient and Family Engagement
Description of MHCP Population Served by Delivery System
Proposed Payment Arrangement
i. Selected Payment Model and Justification
ii. Defined Provider Population and Accountable Fiscal Entity
iii. Additional Service Categories Included in Total Cost of Care (if applicable)
iv. MHCP Population Size
v. Proposed Amount of Assumed Risk
vi. Mechanism for Distributing Shared Savings and Losses Payments
vii. Quality Measures
h. Additional Proposed Measures (if applicable)
i. Description and data of Applicability of Measures to the Population Served
j. SIM Minnesota Accountable Health Model: Continuum of Accountability Matrix Assessment
Tool 1
3. Required Statements
a.
b.
c.
d.
e.
Responder Information and Declarations
Exceptions to Terms and Conditions
Affidavit of Non-collusion
Trade Secret/Confidential Data Notification
Submission of Certified Financial Audit, IRS Form 990, or Most Recent Board-Reviewed
Financial Statements
f. Disclosure of Funding Form
g. Human Rights Compliance
i. Affirmative Action Data Page
ii. Equal Pay Certificate
h. Certification and Restriction on Lobbying
4. Appendix (If Applicable)
1Available
as Appendix D. A Word format version is available at the following website: http://www.dhs.state.mn.us/SIM_Docs_Reps_Pres
2017 IHP RFP – APRIL 25TH, 2016
PAGE 15 OF 33
Any additional information thought to be relevant, but not applicable to the prescribed format, may be
included in an Appendix of the Responder’s Proposal. Please use letter “K” for this Appendix and attach it at
the end of the Responder’s Proposal.
B. Proposal Requirements
The following will be considered minimum requirements of the proposal. Emphasis should be on
completeness and clarity of content.
1.
Executive Summary: This component of the proposal should demonstrate the Responder's
understanding of the requirements in this RFP and any problems anticipated in accomplishing the
work. The Executive Summary should also show the Responder’s overall design of the project in
response to achieving the deliverables as defined in this RFP. Specifically, the proposal should
demonstrate the Responder's familiarity with the project elements, its solutions to the problems
presented and knowledge of the requested services.
2.
Description of the Applicant Delivery System: This section must include information on the
programs and activities of the delivery system, the number of people served, geographic area
served, staff experience, and/or programmatic accomplishments. Include reasons why the
Responder organization is capable to effectively complete the services outlined in the RFP. Include
a brief history of the organization and all strengths that the Responder considers are an asset to the
program. The Responder should demonstrate the length, depth, and applicability of all prior
experience in providing the requested services. The Responder should also verify that the delivery
system provides the full scope of primary care services (defined as overall and ongoing medical
responsibility for comprehensive care for preventive care and a full range of acute and chronic
conditions). The Responder should also demonstrate the skill and experience of lead staff and
designate a project manager with experience in planning and providing the proposed services.
a. Description of Care Models: This section should detail how the IHP expects to lower the total
cost of care and maintain or improve clinical quality and patient experience through innovative
care delivery models, such as health care home certification or other national certifications,
community-based or collaborative initiatives (e.g., DIAMOND, RARE, etc.). Include information
on approaches and methods to coordinate care across the spectrum of services included in the
payment model; encourage prevention and health promotion to create healthier communities;
and use of data to target care interventions, stratify patients by complexity and conduct quality
improvement activities.
The Responder should provide examples and summaries of experience with similar performance or
risk-sharing arrangements including percentages of total patient population and primary payer
break out included in these arrangements between the Responder and Medicare or other payers, if
applicable.
b. Description of Community Partnerships: This section should describe any existing or
planned partnerships between the IHP and community-based organizations and public health
resources, such as disability and aging services, social services, transportation services, and
school-based services. Describe the expected impact of these partnerships on key outcomes of
interest.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 16 OF 33
The Responder should describe how the IHP will engage and coordinate with other providers,
counties, and organizations, including county-based purchasing plans, that provide services to the
IHP’s patients on issues related to local population health, including applicable local needs,
priorities, and public health goals. Describe how the IHP consulted with local providers, counties,
organizations, county-based purchasing plans, and other relevant purchasers in developing the
application to participate in the demonstration project.
c. Description of Patient and Family Partnerships: This section should demonstrate the ways
in which patients (and their families where appropriate) are meaningfully engaged as partners
in the care they receive, as well as in organizational quality improvement activities and
leadership roles.
3.
Description of MHCP Population Served by the Delivery System: This section must describe
the entire MHCP population currently served by the IHP, including the total number of MHCP
enrollees served, the overall proportion of the payer mix represented by MHCP enrollees, and key
descriptive information such as age, gender, race/ethnicity, and the diagnoses/conditions of
highest prevalence. As described above, the population served must include all MHCP enrollees not
specifically excluded from the demonstration payment model.
4.
Proposed Payment Arrangement:
a. Selected Payment Model and Justification: This section will indicate whether the delivery
system qualifies for the Virtual IHP or the Integrated IHP payment model described in Section II
above. If the Responder identifies the Virtual IHP model, it must describe the organizational
structure of the delivery system and demonstrate that it either does not operate within a
formally integrated care system, or serves an MHCP population of 1,000 – 1,999 participants, or
both. Features of such integration include, but are not limited to, common clinical and
information systems, shared financial structure and a common parent organization. This
section will also indicate the catastrophic claim cap level to be used in the payment model
based on the number of qualifying MHCP participants served, as illustrated in Section II.
b. Defined Provider Population: This section identifies the providers who will be participating
in the IHP. This must be done in a way that allows DHS to link claims data to a defined fiscal
entity or group of providers, as it determines the IHP’s attributable population.
o The Responder must specify the Group National Provider Identifiers (NPI) (type 2) for the
entities participating in the IHP, and
o A complete list of individual provider NPIs participating in the IHP, which must be in the
form of an Microsoft Excel spreadsheet in the sample format provided in Appendix C:
Provider Roster.
c. Accountable Financial Entity: The Respondent must specify the MHCP enrolled billing
provider NPI or Tax Identification Number (TIN) that it wishes to be the locus of accountability
for the delivery system and contracting partner with the State. This will be the identified entity
for the shared savings and loss payments to be transmitted to and from DHS.
d. Additional Service Categories Included in Total Cost of Care (if applicable): Attachment
A: Patient Attribution Method, Provider Taxonomy, and Core Services of the IHP model contract
included as an attachment to this RFP lists the minimum services included in the Total Cost of
Care (TCOC) for all demonstration payment models. Responders are encouraged to include
2017 IHP RFP – APRIL 25TH, 2016
PAGE 17 OF 33
additional services in the TCOC in their proposal. This section should identify any additional
service categories that the IHP proposes to be accountable for through their inclusion in the
TCOC calculation. Responders need not complete this section if they do not wish to add
services to the defined TCOC model.
e. MHCP Population Size: This section should provide an estimate of the population size that
the IHP expects to serve under the demonstration project, and a confirmation of the
corresponding catastrophic claim cap laid out in Section II. In addition to the estimate, the
methodology, assumptions and information (e.g. plan provided data, payment analysis) used by
the IHP to estimate the population size should be briefly described in the response.
f.
Proposed Amount of Assumed Risk: This section must contain a proposal for the amount
and distribution of the shared savings and/or losses payments in the model in each of the three
years of the demonstration. (The Virtual Model contains a standard 50/50 split of shared
savings.) Within the guidelines described in Section II above, the Respondent must propose the
amount of shared savings and losses. In the Integrated IHP model, the amount of shared
savings and shared loss must adhere to the following guidelines:
•
•
•
Performance Period 1: IHP shares any savings equally (50/50) with the State/MCOs
provided the 2% minimum performance threshold has been achieved. The maximum
threshold for shared savings in Performance Period 1 must be the same in Performance
Period 3 and is limited to a maximum of 85% of the TCOC Target.
Performance Period 2 (Integrated only): IHP assumes some downside risk, but it need
not be symmetrical to the proposed shared savings threshold. The IHP has some
discretion around the amount of risk it is willing to bear, but the ratio of shared savings
thresholds to shared loss thresholds must be 2:1. For example, if the IHP wishes to
avoid risk for claims above 106% of the TCOC Target, the maximum threshold for
shared savings is 88% (6 percentage points x 2 = 12) below the TCOC Target. All shared
savings and losses are distributed equally (50/50) with the State/MCOs.
Performance Period 3 (Integrated only): IHP assumes two-way risk with symmetrical
risk sharing thresholds. For example, if an IHP wishes to avoid risk at 115% of the TCOC
Target, the maximum threshold for shared savings must be 85%. An IHP may elect
different distributions of shared savings and losses within the proposed thresholds. The
maximum threshold for shared savings in Performance Period 3 must be the same as
the maximum threshold in Performance Period 1 and is limited to a maximum of 85%
of the TCOC Target. (See section 1.3 of Attachment D of the model contract in Appendix
A of this document, for additional detail on the settlement process).
The table below provides a hypothetical example of a permissible 3-year risk sharing agreement under the
integrated model, along with a suggested format for developing your response.
Performance Period 1
Shared Savings Only
% of Adj. Target
IHP/DHS
Threshold
TCOC
Distribution
1
112% - 115%
None
2
110% - 112%
None
3
106% - 110%
None
4
102% - 106%
None
5
100% - 102%
None
6
98% - 100%
50% / 50%
7
94% - 98%
50% / 50%
8
90% - 94%
50% / 50%
Performance Period 2
Example
Responder to Complete
% of Adj.
IHP/DHS
% of Adj.
IHP/DHS
Target TCOC
Distribution
Target TCOC
Distribution
110% - 115%
None
110% - 112%
None
106% - 110%
None
102% - 106%
50% / 50%
100% - 102%
50% / 50%
98% - 100%
50% / 50%
94% - 98%
50% / 50%
90% - 94%
50% / 50%
2017 IHP RFP – APRIL 25TH, 2016
Performance Period 3
Example
Responder to Complete
% of Adj.
IHP/DHS
% of Adj.
IHP/DHS
Target TCOC
Distribution
Target TCOC
Distribution
112% - 115%
40% / 60%
110% - 112%
50% / 50%
106% - 110%
60% / 40%
102% - 106%
70% / 30%
100% - 102%
70% / 30%
98% - 100%
70% / 30%
94% - 98%
70% / 30%
90% - 94%
60% / 40%
PAGE 18 OF 33
9
10
88% - 90%
85% - 88%
50% / 50%
50% / 50%
88% - 90%
85% - 88%
50% / 50%
None
88% - 90%
85% - 88%
50% / 50%
40% / 60%
•
The % thresholds for the second and third year of the Demonstration can be modified based on the
preferences of the bidding IHP. The selected shared savings/losses distributions must follow the
guidelines described below.
•
For Performance Period 2, the IHP is expected to accept downside risk, which can be capped at a
threshold specified by the IHP. However, if the IHP chooses to cap the loss threshold, the amount of
shared savings must be capped at a 2:1 percentage of the loss cap.
•
For Performance Period 3, the thresholds and distribution percentages may differ from the
example and can vary by year. However, the IHP/State distribution must be the same for savings
and losses at the symmetric thresholds (e.g., 90 to 94% gain share distribution must equal the 106
to 110% loss share distribution). Additionally, the shared savings thresholds in Performance Period
3 must be the same as Performance Period 1.
•
The State may consider deviations from the threshold and distribution percentage requirements
described above for Responders that include community providers or organizations or additional
service beyond the core set for TCOC in the IHP payment model. The Responder should follow the
requirements above for completing the financial template but include details of how they propose
to include community providers or organizations and/or additional services in their proposal.
Deviations from the current requirements may need further federal approval.
g. Mechanism for Distributing Shared Savings and Losses Payments: This section must
describe the manner in which the IHP will distribute potential shared savings payments among
its component parts or entities, as well as the nature of shared responsibility for potential
shared losses payments penalties in the Integrated Model. If applicable, the IHP should
highlight the direct inclusion of community organizations in the payment model structure.
5.
Quality Measures: As described in Section II above, a portion of shared savings that accrue to the
IHP are contingent on clinical quality and patient experience measure reporting in Performance
Period 1 and performance in Performance Periods 2 and 3. The “core set” of quality measures for
all IHPs in the demonstration are measures included in the Statewide Quality Reporting and
Measurement System pursuant to Minnesota Statutes § 62U.02. An IHP may propose measures in
addition to the core set in accordance with the guidelines described below.
a. Additional Proposed Measures (if applicable): If desired, the Responder may identify
additional quality and patient experience measures to incorporate into the payment model.
These additional measures do not replace the core measure set identified above. Describe how
the measures are defined and collected, how they have been validated and endorsed by state
and/or national organizations, and otherwise meet the guidelines described is section II.A.5. of
this RFP.
b. Description of Applicability of Measures to the Population Served: This section must
describe how the clinical quality and patient experience measures (both the core set and any
additional measures proposed) apply to the specific populations and communities served by
the Respondent, as well as how the care models, community partnerships, and patient and
family partnerships are expected to improve quality of provided care.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 19 OF 33
6.
Minnesota Accountable Communities for Health Continuum of Accountability Matrix
Assessment Tool: The Minnesota Accountable Health Model: Continuum of Accountability
Matrix Assessment Tool (Appendix D; also at the link:
http://www.dhs.state.mn.us/SIM_Docs_Reps_Pres) is an interactive tool that allows organizations
to answer questions to determine their location on the accountability continuum. The STATE will
use this tool to better understand IHP participants and status in achieving the goals of the
Minnesota Accountable Health Model, what supports are needed to achieve the goals, and how we
may be able to provide additional tools or resources. This tool will be used to help DHS assess
progress throughout the course of the demonstration.
D. Required Statements
Complete the correlating forms found in eDocs by right clicking on the links below (in blue), select “Copy
Hyperlink” and paste into your web browser and click Enter. These forms must be submitted as the
“Required Statements” section of your proposal. You must use the current forms found in eDocs. Failure to
use the most current forms found in eDocs in completion of the proposal are at the responder’s risk and
may, at the discretion of the State, result in disqualification of the proposal for “nonresponsiveness.”
1. Responder Information and Declarations (Responder Information/Declarations Form DHS-7020-ENG):
Complete and submit the attached “Responder Information and Declarations” form. If you are required to
submit additional information as a result of the declarations, include the additional information as part of
this form. The Responder may fail the Required Statements Review in the event that the Responder does
not affirmatively warrant to any of the warranties in the Responder Information and
Declarations. Additionally, the State reserves the right to fail a Responder in the event the Responder does
not make a necessary disclosure in the Responder Information and Declarations, or makes a disclosure
which evidences a conflict of interest.
2. Exceptions to RFP Terms (Exceptions to Terms and Conditions Form- DHS-7019-ENG): The contents of
this RFP and the proposal(s) of the successful responder(s) may become part of the final contract if a
contract is awarded. Each responder's proposal must include a statement of acceptance of all terms and
conditions stated within this RFP or provide a detailed statement of exception for each item excepted by
the responder. Responders who object to any condition of this RFP or model contract must note the
objection on the attached “Exceptions to RFP Terms” form. If a responder has no objections to any terms
or conditions, the responder should write “None” on the form.
Responder should be aware of the State’s standard contract terms and conditions in preparing its response.
A sample State of Minnesota, Department of Human Services Contract is attached in the Appendix for your
reference. Much of the language reflected in the contract is required by statute. If you take exception to
any of the terms, conditions or language in the contract, you must indicate those exceptions in your
response to the RFP. Only those exceptions indicated in your response to the RFP will be available for
discussion or negotiation.
Responders are cautioned that any exceptions to the terms of the model contract which give the responder
a material advantage over other responders may result in the responder’s proposal being declared
nonresponsive. Proposals being declared nonresponsive will receive no further consideration for award of
the Contract. Also, proposals that take blanket exception to all or substantially all boilerplate contract
provisions will be considered nonresponsive proposals and rejected from further consideration for contract
award.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 20 OF 33
3. Affidavit of Noncollusion (Affidavit of Noncollusion Form- DHS-7021): Each responder must complete
and submit the attached “Affidavit of Noncollusion” form. A proposal will fail this component if an Affidavit
of Noncollusion is not submitted.
4. Trade Secret/Confidential Data Notification (Trade Secret/Confidential Data Notice Form- DHS-7015ENG): All materials submitted in response to this RFP will become property of the State and will become
public record in accordance with Minnesota Statutes, section 13.591, after the evaluation process is
completed. Pursuant to the statute, completion of the evaluation process occurs when the government
entity has completed negotiating the contract with the successful responder. If a contract is awarded to
the Responder, the State must have the right to use or disclose the trade secret data to the extent
otherwise provided in the grant contract or by law.
If the responder submits information in response to this RFP that it believes to be trade secret/confidential
materials, as defined by the Minnesota Government Data Practices Act, Minnesota Statutes, section 13.37,
and the responder does not want such data used or disclosed for any purpose other than the evaluation of
this proposal, the responder must:
a. Clearly mark every page of trade secret materials in its proposal at the time the proposal is submitted
with the words “TRADE SECRET” or “CONFIDENTIAL” in capitalized, underlined and bolded type that is at
least 20 pt.; the State does not assume liability for the use or disclosure of unmarked or unclearly marked
trade secret/confidential data;
b. Fill out and submit the attached “Trade Secret/Confidential Information Notification Form,” specifying
the pages of the proposal which are to be restricted and justifying the trade secret designation for each
item. If no material is being designated as protected, a statement of “None” should be listed on the form;
c. Satisfy the burden to justify any claim of trade secret/confidential information. In order for a trade secret
claim to be considered by the State, detailed justification that satisfies the statutory elements of Minnesota
Statutes, section and the factors discussed in Prairie Island Indian Community v. Minnesota Dept. of Public
Safety, 658 N.W.2d 876, 884-89 (Minn.App.2003) must be provided. Use of generic trade secret language
encompassing substantial portions of the proposal or simple assertions of trade secret interest without
substantive explanation of the basis therefore will be regarded as nonresponsive requests for trade secret
exception and will not be considered by the State in the event of a data request is received for proposal
information; and
d. Defend any action seeking release of the materials it believes to be trade secret and/or confidential, and
indemnify and hold harmless the State, its agents and employees, from any judgments awarded against the
State in favor of the party requesting the materials, and any and all costs connected with that defense. This
indemnification survives the State’s award of a contract. In submitting a response to this RFP, the
responder agrees that this indemnification survives as long as the trade secret materials are in the
possession of the State. The State is required to keep all the basic documents related to its contracts,
including selected responses to RFPs, for a minimum of six years after the end of the contract. Non-selected
RFP proposals will be kept by the State for a minimum of one year after the award of a contract, and could
potentially be kept for much longer.
The State reserves the right to reject a claim if it determines responder has not met the burden of
establishing that the information constitutes a trade secret or is confidential. The State will not consider
2017 IHP RFP – APRIL 25TH, 2016
PAGE 21 OF 33
prices or costs submitted by the responder to be trade secret materials. Any decision by the State to
disclose information designated by the responder as trade secret/confidential will be made consistent with
the Minnesota Government Data Practices Act and other relevant laws and regulations. If certain
information is found to constitute a trade secret/confidential, the remainder of the Proposal will become
public; only the trade secret/confidential information will be removed and remain nonpublic.
The State also retains the right to use any or all system ideas presented in any proposal received in
response to this RFP unless the responder presents a positive statement of objection in the proposal.
Exceptions to such responder objections include: (1) public data, (2) ideas which were known to the State
before submission of such proposal, or (3) ideas which properly became known to the State thereafter
through other sources or through acceptance of the responder's proposal. A proposal may fail if a Trade
Secret/Confidential Data form is not completed and submitted with the proposal.
5. Documentation to Establish Fiscal Responsibility: The successful responder must be fiscally
responsible. Therefore, responders must include in their proposals sufficient financial
documentation to establish their financial stability.
IRS Form 990s. If a responder is a not-for-profit organization that completed an IRS Form 990 in
2015, responder must submit its Form 990.
If responder is concerned that its 2015 IRS Form 990 does not demonstrate its fiscal responsibility,
it may supplement its application with any of the additional material described below. An IRS Form
990 is a federal tax return for nonprofit organizations. Nonprofit organizations that are recognized
as exempt from federal income tax must file a Form 990 or Form 990 EZ if it has averaged more
than $25,000 in annual gross receipts over the past three tax years. Please do submit any
information about any pending major accusations that could affect your financial stability.
Organizations without 2015 IRS Form 990s.
(1) Organizations that have not completed and IRS Form 990 should submit a certified financial
audit if they have one. A certified financial audit is a review of an organization’s financial
statements, fiscal policies and control procedures by an independent third party to
determine if the statements fairly represent the organization’s financial position and if
organizational procedures are in accordance with Generally Accepted Accounting Principles
(GAAP). Any organization with an annual revenue greater than $750,000 is required to
have a certified financial audit completed for any fiscal year in which they have total
revenue of more than $750,000.
(2) If the organization does not have a certified financial audit, the organization must submit
its most recent board-reviewed financial statements if it has a board.
(3) If the organization does not have a certified financial audit or board-reviewed financial
statements because it does not have a board, the organization should submit a certified
statement of assets and debts (balance sheet) and evidence of cash flow including amounts
in a checking account.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 22 OF 33
Responders may also include documentations of cash reserves to carry you through
shortages or delays in receipt of revenue, and/or any other documents sufficient to
substantiate responsible fiscal management.
State may request additional information from these responders as necessary to determine
financial stability.
All responders must submit any information about any pending major accusations that could
affect your financial stability.
In the event a responder is either substantially or wholly owned by another corporate entity, the
proposal must also include the most recent detailed financial report of the parent organization,
and a written guarantee by the parent organization that it will unconditionally guarantee
performance by the responder in each and every term, covenant, and condition of such contract
as may be executed by the parties.
If the responder is a county government or a multi-county human services agency that has 1.) had
an audit in the last year by the State Auditor or an outside auditing firm or 2) meets the
requirements of the Single Audit Act, the responder is not required to submit financial statements.
However, the State reserves the right to request any financial information to assure itself of a
county’s financial status.
The information collected from these inquiries will be used in the State’s determination of the
award of the contract. It may be shared with other persons within the Minnesota Department of
Human Services who may be involved in the decision-making process, and/or with other persons
as authorized by law. If you choose not to provide the requested information, your organization’s
proposal will found nonresponsive and given no further consideration. The State reserves the right
to request any additional information to assure itself of a responder's financial reliability. If a
responder’s submission in response to this component does not demonstrate its financial stability,
the responder may fail this requirement and be disqualified from further consideration.
6. Disclosure of Funding Form (Disclosure of Funding Form- DHS-7018-ENG)
Per the Federal Funding Accountability and Transparency Act of 2006 “Transparency Act” or “FFATA”
(Public Law 109-282), all entities and organizations receiving federal funds are required to report full
disclosure of funding (United States Code, title 31, chapter 61, section 6101). The purpose of FFATA is to
provide every American with the ability to hold the government accountable for each spending decision.
The end result is to reduce wasteful spending in the government. The FFATA legislation requires
information on federal awards to be made available to the public through a single, searchable website.
Federal awards include grants, sub-grants, loans, awards, and delivery orders.
In order to comply with the federal statute, the Minnesota Department of Human Services is required to
obtain and report by the grantee’s Data Universal Numbering System (DUNS) number and determine if the
grantee meets specific requirement which would require additional reporting items and to collect
2017 IHP RFP – APRIL 25TH, 2016
PAGE 23 OF 33
additional information on executive compensation if required. In order to comply with federal law and to
collect this information, responders are required to fill out the Disclosure of Funding Form and submit it
with their response. The form requires responders to provide their Data Universal Numbering System
(DUNS) number. The Data Universal Numbering System (DUNS) number is the nine-digit number
established and assigned by Dun and Bradstreet, Inc. (D&B) to uniquely identify business entities. If a
responder does not already have a DUNS number, a number may be obtained from the D&B by telephone
(currently 866-705-5711) or the Internet (currently at http://fedgov.dnb.com/webform). The responder
must have a DUNS number before their response is submitted.
7. Human Rights Compliance:
a. Affirmative Action Certification (Affirmative Action Data Page- DHS-7016-ENG).For all
contracts estimated to be in excess of $100,000, Responders are required to complete and
submit the attached “Affirmative Action Data” page. As required by Minnesota Rules, part
5000.3600, “It is hereby agreed between the parties that Minnesota Statutes, section
363A.36 and Minnesota Rules, parts 5000.3400 - 5000.3600 are incorporated into any
contract between these parties based upon this specification or any modification of it. A
copy of Minnesota Statutes, section 363A.36 and Minnesota Rules, parts 5000.3400 5000.3600 are available upon request from the contracting agency.”
b. Equal Pay Certificate. (Equal Pay Certificate Compliance – DHS -7075-ENG) 2
i. Scope. Pursuant to Minnesota Statutes, section 363A.44, the State shall not
execute a contract for goods or services or an agreement for goods or services in
excess of $500,000 with a business that has 40 or more full-time employees in the
State of Minnesota or a state where the business has its primary place of business
on a single day during the prior 12 months, unless the business has an equal pay
certificate or it has certified in writing that it is exempt.
ii. This section does not apply to a business, with respect to a specific contract, if the
commissioner of administration determines that the requirements of this section
would cause undue hardship on the business. This section does not apply to a
contract to provide goods or services to individuals under Minnesota Statutes,
chapters 43A, 62A, 62C, 62D, 62E, 256B, 256I, 256L, and 268A, with a business that
has a license, certification, registration, provider agreement, or provider
enrollment contract that is a prerequisite to providing those good or services.
c. Application. If your response to this RFP is or could be within the scope of Minnesota
Statutes, section 363A.44, you must apply for an equal pay certificate by paying a $150
filing fee and submitting an equal pay compliance statement to the Minnesota Department
of Human Rights (“MDHR”). MDHR’s Equal Pay Certificate Application Form can be
obtained at http://mn.gov/mdhr/compliance/forms.html. It is your sole responsibility to
submit this statement to MDHR and – if required – apply for an equal pay certification
before the due date of this proposal and obtain the certification prior to the execution of
any resulting contract.
d. Revocation of Contract. If a contract is awarded to a business that does not have an equal
pay certificate as required by Minnesota Statutes, section 363A.44, or is not in compliance
2
https://edocs.dhs.state.mn.us/lfserver/Public/DHS-7075-ENG
2017 IHP RFP – APRIL 25TH, 2016
PAGE 24 OF 33
with the laws identified within section 363A.44, MDHR may void the contract on behalf of
the state, and the contract may be abridged or terminated by DHS upon notice that the
MDHR has suspended or revoked the certificate of the business.
e. Equal Pay Certificate Compliance Form. You must complete the Equal Pay Certificate of
Compliance Form and submit it with your proposal. The Equal Pay Certificate of
Compliance Form can be obtained at https://edocs.dhs.state.mn.us/lfserver/Public/DHS7075-ENG.
8. Certification Regarding Lobbying (Certificate Regarding Lobbying Form- DHS-7017-ENG): Federal money
will be used or may potentially be used to pay for all or part of the work under the contract, therefore the
responder must complete and submit the attached “Certification Regarding Lobbying” form.
IV. RFP Process
A. Timeline
This timeline outlines the RFP process during 2016 for the 2017 contract.
ACTIVITY
DATE
RFP Publication
April 25th, 2016
All RFP Questions Received
July 25th, 2016
Optional Individual Q&A Sessions with Potential Responders
May 16th - July 25th, 2016
All RFP Questions Answered and Posted on DHS Website
Anticipated August 1st, 2016
Proposal Responses Due
August 19th, 2016
RFP Review Completed
Anticipated September 2nd, 2016
Notice of Intent to Contract
Anticipated September 9th, 2016
IHP Model and Contract Overview Plenary Meetings (Two 3Anticipated September 19th – 30th
hour meetings)
Individual Potential IHP Contract Negotiations Begin
Anticipated September 19th
Performance period begins
January 1, 2017
B. Optional Individual Question and Answer Sessions
DHS staff is making available to all potential provider responders one optional 60-minute Question and
Answer (Q&A) session May 16th through July 25th, 2016 in person or via conference call. The optional Q&A
sessions will serve as an opportunity for Responders to ask specific questions of State staff concerning the
project. A Q&A session is not mandatory. DHS staff will record all questions and answers provided in the
individual sessions and post them to the DHS website. To schedule a Q&A session for your provider
organization, please contact Mathew Spaan at Mathew.Spaan@state.mn.us before or by July 18, 2016.
Responders may attend via conference call (contact the State contact for this RFP for more information
about attending by conference call) or in person. Oral answers given at the conference will be non-binding.
Written responses to questions asked at the conference will be sent to all identified prospective
Responders after the conference.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 25 OF 33
C. Responders’ Questions
Responders’ questions regarding this RFP must be submitted in writing prior by 4:00 p.m. Central Time on
July 25th, 2016. All questions must be addressed to:
Request for Proposal Response
Attention: Mathew Spaan
Health Care Administration
Department of Human Services
PO Box 64983
St. Paul, MN 55164-0983
Questions may also be e-mailed to Mathew.Spaan@state.mn.us.
Other personnel are NOT authorized to discuss this RFP with Responders before the proposal submission
deadline. Contact regarding this RFP with any State personnel not listed above could result in
disqualification. The State will not be held responsible for oral responses to Responders.
Questions will be addressed in writing and distributed to all identified prospective Responders. Every
attempt will be made to provide timely answers, with the intent that they are sent no later than August 1st,
2016.
D. Proposal Submission
One (1) original and six (6) copies of the proposal must be submitted. Additionally, Responder shall include
an electronic copy of the proposal and all required documents on a USB storage device or other electronic
storage with the Proposal submission. Proposals must be physically received (not postmarked) by 4:00
p.m. Central Time on August 19th, 2016 to be considered. Late proposals will not be considered and will be
returned unopened to the submitting party. Faxed or e-mailed proposals will not be accepted.
Clearly label the original "Proposal – Original" and each copy “Proposal – Copy”. All proposals, including
required copies, must be submitted in a single sealed package or container. Proposals should be submitted
in three-ring binders or spiral bound binders with each section indexed with label tabs. The main body of
the proposal pages must be numbered and submitted in 12-point font on 8 ½ X 11 inch paper, single
spaced. The size and/or style of graphics, tabs, attachments, margin notes/highlights, etc. are not restricted
by this RFP and their use and style are at the responder’s discretion.
The above-referenced packages and all correspondence related to this RFP must be delivered to:
Attention: Mathew Spaan
Health Care Administration
Department of Human Services
444 Lafayette Road N.
St. Paul, MN 55155
It is solely the responsibility of each responder to assure that their proposal is delivered at the specific
place, in the specific format, and prior to the deadline for submission. Failure to abide by these
2017 IHP RFP – APRIL 25TH, 2016
PAGE 26 OF 33
instructions for submitting proposals may result in the disqualification of any non-complying proposal.
V. Proposal Evaluation and Selection
A. Overview of Evaluation Methodology
1. All responsive proposals received by the deadline will be evaluated by the State. Proposals will be
evaluated on “best value” as specified below, using a 100 point scale. The evaluation will be conducted in
three phases:
a. Phase I
b. Phase II
c. Phase III
Required Statements Review
Evaluation of Proposal Requirements
Selection of the Successful Responder(s)
2. During the evaluation process, all information concerning the proposals submitted, except identity and
address of the responder, will remain non-public and will not be disclosed to anyone whose official duties
do not require such knowledge.
3. Nonselection of any proposals will mean that either another proposal(s) was determined to be more
advantageous to the State or that the State exercised the right to reject any or all Proposals. At its
discretion, the State may perform an appropriate cost and pricing analysis of a responder's proposal,
including an audit of the reasonableness of any proposal.
B. Evaluation Team
1. An evaluation team will be selected to evaluate Responder Proposals.
2. State and professional staff, other than the evaluation team, may also assist in the evaluation
process. This assistance could include, but is not limited to, the initial mandatory requirements
review, contacting of references, or answering technical questions from evaluators.
3. The State reserves the right to alter the composition of the evaluation team and their specific
responsibilities.
C. Evaluation Phases
At any time during the evaluation phases, the State may, at the State’s discretion, contact a responder to
(1) provide further or missing information or clarification of their proposal, (2) provide an oral presentation
of their proposal, or (3) obtain the opportunity to interview the proposed key personnel. Reference checks
may also be made at this time. However, there is no guarantee that the State will look for information or
clarification outside of the submitted written proposal. Therefore, it is important that the responder
ensure that all sections of the proposal have been completed to avoid the possibility of failing an evaluation
phase or having their score reduced for lack of information.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 27 OF 33
1. Phase I – Required Statements Review
The Required Statements will be evaluated on a pass or fail basis. Responders must "pass" each of the
requirements identified in these sections to move to Phase II.
2. Phase II - Evaluation of Technical Requirements of Proposals.
A total of 100 points have been assigned to these component areas. Of the 100 possible points, there are
15 bonus points that represent elements that are not required proposal elements. The total possible points
for these component areas are as follows:
Component
Total Possible Points
a. Executive Summary
5
b. Description of the Applicant Delivery System
40
c. Description of MHCP Population Served by Delivery System
5
d. Proposed Payment Arrangement
30
(Including 5 possible bonus points for Direct Inclusion of Community
Partners in Payment Model and 5 possible bonus points for Inclusion of
Additional Service Categories in “Total Cost of Care”)
e. Quality Measures
20
(Including 5 possible bonus points for Additional Measures Proposed
Beyond the Core Set)
Total:
100
The evaluation team will review the components of each responsive Proposal submitted. Each component
will be evaluated on the Responder's understanding and the quality and completeness of the Responder's
approach and solution to the problems or issues presented.
3. Phase III - Selection of the Successful Responder(s)
a. Only the Proposals found to be responsive under Phases I and II will be considered in Phase III.
b. The evaluation team will review the scoring in making its recommendations of the Successful
Responder(s).
c. The State may submit a list of detailed comments, questions, and concerns to one or more
Responders after the initial evaluation. The State may require said response to be written, oral, or
both. The State will only use written responses for evaluation purposes. The total scores for those
Responders selected to submit additional information may be revised as a result of the new
information.
d. The evaluation team will make its recommendation based on the above-described evaluation
process. The Successful Responder(s), if any, will be selected less than three weeks after the
Proposal submission due date.
The final award decision will be made by the Commissioner or authorized designee. The Commissioner or
authorized designee may accept or reject the recommendation of the evaluation team.
D. Contract Negotiations and Unsuccessful Responder Notice
2017 IHP RFP – APRIL 25TH, 2016
PAGE 28 OF 33
If a Responder(s) is selected, the State will notify the Successful Responder(s) in writing of their selection
and the State’s desire to enter into contract negotiations. Until the State successfully completes
negotiations with the selected Responder(s), all submitted Proposals remain eligible for selection by the
State.
In the event contract negotiations are unsuccessful with the selected Responder(s), the evaluation team
may recommend another Responder(s). The final award decision will be made by the Commissioner or
authorized designee. The Commissioner or authorized designee may accept or reject any subsequent
recommendation of the evaluation team.
After the State and chosen Responder(s) have successfully negotiated a contract, the State will notify the
unsuccessful Responders in writing that their Proposals have not been accepted. All public information
within Proposals will then be available for Responders to review, upon request.
VI. Required Contract Terms and Conditions
A. Requirements. All responders must be willing to comply with all state and federal legal requirements
regarding the performance of the grant contract. The requirements are set forth throughout this RFP
and are contained in the attached grant contract in the Appendix.
B. Governing Law/Venue. This RFP and any subsequent contract must be governed by the laws of the
State of Minnesota. Any and all legal proceedings arising from this RFP or any resulting contract in
which the State is made a party must be brought in the State of Minnesota, District Court of Ramsey
County. The venue of any federal action or proceeding arising here from in which the State is a party
must be the United States District Court for the State of Minnesota.
C. Travel. Reimbursement for travel and subsistence expenses actually and necessarily incurred by the
grantee as a result of the grant contract will be in no greater amount than provided in the current
"Commissioner’s Plan” promulgated by the commissioner of Minnesota Management and Budget.
Reimbursements will not be made for travel and subsistence expenses incurred outside Minnesota
unless it has received the State’s prior written approval for out of state travel. Minnesota will be
considered the home state for determining whether travel is out-of-state.
D. Preparation Costs. The State is not liable for any cost incurred by Responders in the preparation and
production of a proposal. Any work performed prior to the issuance of a fully executed grant contact
will be done only to the extent the responder voluntarily assumes risk of non-payment.
E. Contingency Fees Prohibited. Pursuant to Minnesota Statutes, section 10A.06, no person may act as or
employ a lobbyist for compensation that is dependent upon the result or outcome of any legislation or
administrative action.
F. Certification Regarding Debarment, Suspension, Ineligibility, and Voluntary Exclusion. Federal money
will be used or may potentially be used to pay for all or part of the work under the contract, therefore
the responder must certify the following, as required by the regulations implementing Executive Order
12549.
Certification Regarding Debarment, Suspension, Ineligibility and Voluntary Exclusion -- Lower Tier
Covered Transactions
2017 IHP RFP – APRIL 25TH, 2016
PAGE 29 OF 33
Instructions for Certification
1.
By signing and submitting this proposal, the prospective lower tier participant is providing the
certification set out below.
2.
The certification in this clause is a material representation of fact upon which reliance was placed
when this transaction was entered into. If it is later determined that the prospective lower tier
participant knowingly rendered an erroneous certification, in addition to other remedies available
to the federal government, the department or agency with which this transaction originated may
pursue available remedies, including suspension and/or debarment.
3.
The prospective lower tier participant shall provide immediate written notice to the person to
which this proposal is submitted if at any time the prospective lower tier participant learns that its
certification was erroneous when submitted or had become erroneous by reason of changed
circumstances.
4.
The terms covered transaction, debarred, suspended, ineligible, lower tier covered transaction,
participant, person, primary covered transaction, principal, proposal, and voluntarily excluded, as
used in this clause, have the meaning set out in the Definitions and Coverages sections of rules
implementing Executive Order 12549. You may contact the person to which this proposal is
submitted for assistance in obtaining a copy of those regulations.
5.
The prospective lower tier participant agrees by submitting this response that, should the proposed
covered transaction be entered into, it shall not knowingly enter into any lower tier covered
transaction with a person who is proposed for debarment under 48 C.F.R. part 9, subpart 9.4,
debarred, suspended, declared ineligible, or voluntarily excluded from participation in this covered
transaction, unless authorized by the department or agency with which this transaction originated.
6.
The prospective lower tier participant further agrees by submitting this proposal that it will include
this clause titled “Certification Regarding Debarment, Suspension, Ineligibility and Voluntary
Exclusion--Lower Tier Covered Transaction,” without modification, in all lower tier covered
transactions and in all solicitations for lower tier covered transactions.
7.
A participant in a covered transaction may rely upon a certification of a prospective participant in a
lower tier covered transaction that it is not proposed for debarment under 48 C.F.R. part 9, subpart
9.4, debarred, suspended, ineligible, or voluntarily excluded from covered transactions, unless it
knows that the certification is erroneous. A participant may decide the method and frequency by
which it determines the eligibility of its principals. Each participant may, but is not required to,
check the List of Parties Excluded from Federal Procurement and Nonprocurement Programs
8.
Nothing contained in the foregoing shall be construed to require establishment of a system of
records in order to render in good faith the certification required by this clause. The knowledge
and information of a participant is not required to exceed that which is normally possessed by a
prudent person in the ordinary course of business dealings.
9.
Except for transactions authorized under paragraph 5 of these instructions, if a participant in a
covered transaction knowingly enters into a lower tier covered transaction with a person who is
proposed for debarment under 48 C.F.R. 9, subpart 9.4, suspended, debarred, ineligible, or
2017 IHP RFP – APRIL 25TH, 2016
PAGE 30 OF 33
voluntarily excluded from participation in this transaction, in addition to other remedies available
to the federal government, the department or agency with which this transaction originated may
pursue available remedies, including suspension and/or debarment.
Certification Regarding Debarment, Suspension, Ineligibility and Voluntary Exclusion - Lower Tier Covered
Transactions
1.
The prospective lower tier participant certifies, by submission of this proposal, that neither it nor its
principals is presently debarred, suspended, proposed for debarment, declared ineligible, or
voluntarily excluded from participation in this transaction by any Federal department or agency.
2.
Where the prospective lower tier participant is unable to certify to any of the statements in this
certification, such prospective participant shall attach an explanation to this proposal.
G. Insurance Requirements
1. Responder shall not commence work under the grant contract until they have obtained all the insurance
described in Appendix A, section 2.9 and the State of Minnesota has approved such insurance. All policies
and certificates shall provide that the policies shall remain in force and effect throughout the term of the
grant contract.
2. Additional Insurance Conditions:
• Responder’s policy(ies) shall be primary insurance to any other valid and collectible insurance
available to the State of Minnesota with respect to any claim arising out of Responder’s
performance under this grant contract;
• If Responder receives a cancellation notice from an insurance carrier affording coverage herein,
responder agrees to notify the State of Minnesota within five (5) business days with a copy of the
cancellation notice, unless responder’s policy(ies) contain a provision that coverage afforded under
the policy(ies) will not be cancelled without at least thirty (30) days advance written notice to the
State of Minnesota;
• Responder is responsible for payment of grant contract related insurance premiums and
deductibles;
• If Responder is self-insured, a Certificate of Self-Insurance must be attached;
• Include legal defense fees in addition to its liability policy limits; and
• Obtain insurance policies from an insurance company having an “AM BEST” rating of A- (minus);
Financial Size Category (FSC) VII or better and must be authorized to do business in the State of
Minnesota; and
• An Umbrella or Excess Liability insurance policy may be used to supplement the responder’s
policy limits to satisfy the full policy limits required by the grant contract.
4. The State reserves the right to immediately terminate the grant contract if the responder is not in
compliance with the insurance requirements and retains all rights to pursue any legal remedies against the
2017 IHP RFP – APRIL 25TH, 2016
PAGE 31 OF 33
responder. All insurance policies must be open to inspection by the State, and copies of policies must be
submitted to the State’s authorized representative upon written request.
5. The successful responder is required to submit Certificates of Insurance acceptable to the State of
Minnesota as evidence of insurance coverage requirements prior to commencing work under the grant
contract.
VII. State’s Authority
Notwithstanding anything to the contrary, the State reserves the right to:
A. Reject any and all proposals received in response to this RFP;
B. Disqualify any responder whose conduct or proposal fails to conform to the requirements of this RFP;
C. Have unlimited rights to duplicate all materials submitted for purposes of RFP evaluation, and duplicate
all public information in response to data requests regarding the proposal;
D. Select for contract or for negotiations a proposal other than that with the lowest cost or the highest
evaluation score;
E. Consider a late modification of a proposal if the proposal itself was submitted on time and if the
modifications were requested by the State and the modifications make the terms of the proposal more
favorable to the State, and accept such proposal as modified;
F. At its sole discretion, reserve the right to waive any non-material deviations from the requirements and
procedures of this RFP;
G. Negotiate as to any aspect of the proposal with any responder and negotiate with more than one
responder at the same time, including asking for responders’ “Best and Final” offers;
H. Extend the grant contract, in increments determined by the State, not to exceed a total contract term of
five years; and
I. Cancel the RFP at any time and for any reason with no cost or penalty to the State.
J. Correct or amend the RFP at any time with no cost or penalty to the State. The State will not be liable for
any errors in the RFP or other responses related to the RFP.
2017 IHP RFP – APRIL 25TH, 2016
PAGE 32 OF 33
Appendices
Appendix A: Sample State of Minnesota, Department of Human Services IHP Contract and
Contract Attachments
Appendix B: IHP Provider Portal
Appendix C: IHP Provider Roster & Roster Instructions
Appendix D: Minnesota Accountable Communities for Health Continuum of Accountability Matrix
Assessment Tool
2017 IHP RFP – APRIL 25TH, 2016
PAGE 33 OF 33
Appendix A: Sample State of Minnesota, Department of Human Services IHP Contract and Contract Attachments
[2017 RFP VERSION]
MINNESOTA
DEPARTMENT OF HUMAN SERVICES
INTEGRATED HEALTH PARTNERSHIPS CONTRACT
with
[NAME OF IHP]
January 1, 2017
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 1 OF 28
STATE OF MINNESOTA
DEPARTMENT OF HUMAN SERVICES
INTEGRATED HEALTH PARTNERSHIPS CONTRACT
TABLE OF CONTENTS
SECTION
PAGE
Article. 1 ACRONYMS, ABBREVIATIONS AND DEFINITIONS. ........................................... 5
Article. 2 IHP REQUIREMENTS. ................................................................................................. 8
2.1 Legal Entity. .......................................................................................................................... 8
2.2 Governance. .......................................................................................................................... 8
2.3 Legal Authority. .................................................................................................................... 9
2.4 Documentation of Legal Entity and Fiscal Soundness. ........................................................ 9
2.5 Assurance of Ability to Make Final Payments. .................................................................... 9
2.6 Taxpayer Identification Number. .......................................................................................... 9
2.7 Provider Rosters. ................................................................................................................... 9
2.8 Statutory Eligibility. ............................................................................................................ 10
2.9 Insurance and Insurance Risk Management. ...................................................................... 10
Article. 3 DUTIES. ....................................................................................................................... 11
3.1 Participation in Demonstration. .......................................................................................... 11
3.2 Provider Enrollment. ........................................................................................................... 11
3.3 Shared Savings or Losses.................................................................................................... 11
3.4 Provision of Data. ............................................................................................................... 11
3.4.1 Data from IHP. ............................................................................................................. 11
3.4.2 Data from STATE. ....................................................................................................... 11
3.4.3 Data. ............................................................................................................................. 13
3.5 Data Analysis. ..................................................................................................................... 13
3.6 Required Reports and Notices. ........................................................................................... 13
3.7 Patient Protection and Patient-Centeredness. ..................................................................... 14
Article. 4 PAYMENT. .................................................................................................................. 14
4.1 Claims Payments and Demonstration Payments................................................................. 14
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 2 OF 28
4.2 Terms of Payment. .............................................................................................................. 15
4.3 Payment Errors.................................................................................................................... 16
Article. 5 TERM AND TERMINATION; DISPUTE RESOLUTION. ....................................... 16
5.1 Effective Dates. ................................................................................................................... 16
5.2 Automatic Renewal. ............................................................................................................ 17
5.3 Termination. ........................................................................................................................ 17
5.3.1 Termination By STATE............................................................................................... 17
5.3.2 Pre-termination Action by STATE. ............................................................................. 18
5.3.3 Termination by IHP. .................................................................................................... 18
5.3.4 Termination Procedures. .............................................................................................. 19
5.3.5 Dispute Resolution. ...................................................................................................... 19
Article. 6 AUTHORIZED REPRESENTATIVE AND RESPONSIBLE AUTHORITY. ........... 19
6.1 STATE. ............................................................................................................................... 19
6.2 IHP. ..................................................................................................................................... 19
Article. 7 QUALITY AND PATIENT EXPERIENCE MEASURES.......................................... 19
7.1 Source of Measure Specifications and Reporting Requirements. ....................................... 19
7.2 Changes in Measures. ......................................................................................................... 20
7.3 Changes in Calculation Methods. ....................................................................................... 20
7.4 Quality and Patient Experience Data Appeals. ................................................................... 20
Article. 8 INFORMATION PRIVACY AND SECURITY. ......................................................... 20
8.1 Part of the Welfare System. ................................................................................................ 20
8.2 Information Privacy and Security. ...................................................................................... 20
8.4.............................................................................................................................................. 21
8.5.............................................................................................................................................. 21
8.6.............................................................................................................................................. 21
8.7.............................................................................................................................................. 21
Article. 9 Intellectual Property Rights. ......................................................................................... 21
9.1 Definitions........................................................................................................................... 21
9.2 Use of Works and Documents. ........................................................................................... 21
Article. 10 COMPLIANCE WITH STATE AND FEDERAL LAWS......................................... 22
10.1 Compliance with Federal Laws. ....................................................................................... 22
10.2 Affirmative Action And Non-Discrimination................................................................... 22
10.2.1 Affirmative Action requirements for IHPs with more than 40 full-time employees
and a contract in excess of $100,000. ................................................................................... 22
10.2.2 Affirmative Action and Non-Discrimination requirements for all IHPs. .................. 22
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 3 OF 28
10.2.3 Compliance with Department of Human Rights Statutes. ......................................... 23
10.3 Workers' Compensation. ................................................................................................... 23
10.4 Voter Registration Requirement. ...................................................................................... 23
10.5 Federal Audit Requirements. ............................................................................................ 24
10.6 Debarment Information..................................................................................................... 24
10.7 Ownership and Control; Exclusions of Individuals and Entities. ..................................... 24
Article. 11 OTHER PROVISIONS. ............................................................................................. 24
11.1 Governing Law, Jurisdiction and Venue. ......................................................................... 24
11.2 Waiver. .............................................................................................................................. 25
11.3 Contract Complete. ........................................................................................................... 25
11.4 Assignment. ...................................................................................................................... 25
11.5 Amendments. .................................................................................................................... 25
11.6 Indemnification. ................................................................................................................ 25
11.7 STATE Audits. ................................................................................................................. 25
11.8 Right to Review before Publication. ................................................................................. 25
11.9 Religious-Based Counseling. ............................................................................................ 26
11.10 Payment to Subcontractors. ............................................................................................ 26
11.11 Severability. .................................................................................................................... 26
11.12 Execution in Counterparts............................................................................................... 26
11.13 Survival. .......................................................................................................................... 26
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 4 OF 28
STATE OF MINNESOTA
DEPARTMENT OF HUMAN SERVICES
INTEGRATED HEALTH PARTNERSHIPS CONTRACT
For (IHP
Name)
THIS CONTRACT, and amendments and supplements thereto, is between the State of
Minnesota, acting through its Department of Human Services (DHS) Health Care Administration
(hereinafter STATE) and [NAME OF IHP] (hereinafter IHP), witnesseth that:
WHEREAS, the STATE, pursuant to Minnesota Statutes, §§ 256.01, subd. 2 (a)(6)
and 256B.0755, is empowered to enter into contracts for an Integrated Health Partnerships
payment model that will represent a wide variety of geographic locations, patient populations,
providers, and care coordination models, and will encourage formal and informal partnerships
among health care delivery systems, counties, and non-profit agencies that provide services such
as social services, public health, mental health, community-based projects, and continuing care;
and
WHEREAS, the STATE has received approval from the Centers for Medicare and Medicaid for
an “Integrated Care Models for Health Care Delivery Systems” State Plan Amendment; and
WHEREAS, the STATE is in need of contractors for the delivery of health care services under
the demonstration described in Minnesota Statutes, § 256B.0755, and
WHEREAS, the STATE is permitted to share information with the IHP in accordance with
Minnesota Statutes, § 13.46, and
WHEREAS, IHP has established a mechanism of shared governance as described in Minnesota
Statutes, § 256B.0755, subd. 1 (d), and is a [PLACEHOLDER for type of corporation] in good
standing under the relevant laws of the State of Minnesota [cite to 317A, 322B, etc.]; and
WHEREAS, the IHP represents that it is duly qualified and willing to perform the services set
forth herein,
NOW, THEREFORE, it is agreed:
Article. 1 ACRONYMS, ABBREVIATIONS AND DEFINITIONS. The following terms as
used in this Contract and its Attachments shall be construed and interpreted as follows:
(1) “ACG” means the data obtained from claims and encounters as derived from the
Johns Hopkins Adjusted Clinical Groups (ACG®).
(2) “Attributed Population” means the Patients included in the Total Cost of Care
calculations for which the IHP is accountable.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 5 OF 28
(3) “Attribution” means the process described in Attachment A, Patient Attribution
Method, Provider Taxonomy, and Services Provided of determining which Patients
are assigned to a particular IHP.
(4) “Claims Run-out” means the period of time between the date a service is
rendered and the date the claims or encounter data record is considered complete.
(5) “Contract” means this Contract, its terms and conditions, attachments, documents
incorporated by reference under the terms of this Contract, and any future modifying
agreements made pursuant to sections 8.4 or 11.5 of this Contract.
(6) “Day” means calendar day unless otherwise specified (for example, business
day).
(7) “Fee For Service” (FFS) means the Minnesota Health Care Programs payment
method whereby a health care provider is paid directly by DHS for each service
rendered.
(8) “Final Payment” means an adjustment to the Interim Payment that occurs after
the conclusion of a Performance Period based on complete data. A percentage of the
Final Payment shall be affected by IHP performance on quality and patient
experience measures.
(9) “IHP Entity” means an Integrated Health Partnership that is able to deliver the
full scope of primary care services and directly deliver or demonstrate the ability to
coordinate with additional non-primary care providers. The IHP Entity may be a
separate legal entity able to bind providers to the terms of this Contract to deliver
services. The IHP Entity that is a Party to this Contract is further described in
Attachment B-1, IHP-Specific Governance and Financial Settlement Information
(10) “IHP Participant” means a constituent part of an IHP as a health care delivery
system, and includes but is not limited to clinic location(s), hospitals, physician and
other provider group(s) or outpatient service locations. Each IHP Participant shall be
included in the Shared Governance mechanism required by Minnesota Statutes,
§ 256B.0755, subd. 1(d). A list of the IHP Participants and a description of the
shared governance system is included in Attachment B-1, IHP-Specific Governance
and Financial Settlement Information
(11) “IHP Fiscal Agent” means the agent or entity acting as the fiscal agent for the
IHP Entity that makes, distributes or receives Interim Payments and Final Payments.
(12) “Integrated Health Partnership (IHP)” means a health care delivery system
described in Minnesota Statutes, § 256B.0755, subd. 1(d).
(13) “Health Home” means a provider organization certified by the Minnesota
Department of Health (MDH) as a Health Care Home pursuant to Minnesota
Statutes, § 256B.0751, or a Behavioral Health Home certified by the Minnesota
Department of Human Services (DHS) pursuant to Minnesota Statutes, § 256B.0757.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 6 OF 28
(14) “Interim Payment” means the payment of the Shared Savings amount that
occurs after the conclusion of a demonstration Performance Period based on the most
complete data available at that time. The Interim Payments shall not be affected by
IHP performance on quality and patient experience measures.
(15) “Managed Care Organization” (MCO) means an entity that has, or is seeking to
qualify for, a comprehensive risk contract with the STATE pursuant to the
Minnesota PMAP program in Minnesota Statutes, § 256B.69 and the MinnesotaCare
program in Minnesota Statutes, Chapter 256L.
(16) “MinnesotaCare” means the program authorized in Minnesota Statutes, Chapter
256L.
(17) “Minnesota Health Care Programs” (MHCP) means Minnesota’s Medical
Assistance and MinnesotaCare programs including FFS and managed care programs.
(18) “Minnesota Health Care Programs Provider Agreement” means the form “DHS4138” agreement, as amended, between the STATE and a provider allowing the
provider to serve MHCP recipients.
(19) “Party” means the STATE or IHP and “Parties” means both the STATE and
IHP.
(20) “Patient” or “Attributed Patient” means, for purposes of this Contract, either a
recipient in the MHCP FFS program or an MCO enrollee who is included in the
IHP’s Attributed Population.
(21) “Performance Period” means a period of time for the purposes of calculating the
Total Cost of Care for services provided to the IHP Attributed Patients.
(22) “Prepaid Medical Assistance Program (PMAP)” means the Medicaid program
authorized under Minnesota Statutes, § 256B.69 and Minnesota Rules, Parts
9500.1450 through 9500.1464.
(23) “Primary Care Provider” means a health care provider whose principal specialty
is among those listed as “primary care” or “PCP” in Attachment A, Patient
Attribution Method, Provider Taxonomy, and Services Provided, Section 3.1.
(24) “Quality Measurement Period” means a specific reporting period based upon
dates of service, discharge dates, or visit dates for which a particular quality or
patient experience measure is calculated to determine scoring and impact on Shared
Savings.
(25) “Roster” means a list of the IHP Participants and Primary Care and Specialty
Providers the IHP provides to the STATE on or before the last business day of each
quarter according to specifications provided by the STATE.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 7 OF 28
(26) “Shared Governance” means a mechanism of IHP governance pursuant to
Minnesota Statutes, § 256B.0755, subd. 1(d).
(27) “Shared Losses” means the amount by which the observed Performance Period
Total Cost of Care is in excess of the adjusted Total Cost of Care target for the
Performance Period after the IHP Entity exceeds the performance threshold as
described in Attachment B-1, IHP-Specific Governance and Financial Settlement
Information
(28) “Shared Savings” means the amount by which the observed Performance Period
Total Cost of Care is below the adjusted Total Cost of Care target for the
Performance Period after the IHP Entity exceeds the performance threshold as
described in Attachment B-1, IHP-Specific Governance and Financial Settlement
Information
(29) “Specialty Provider” means a provider whose principal specialty is other than
those listed as “primary care” in Attachment A, Patient Attribution Method, Provider
Taxonomy, and Services Provided, Section 3.1.
(30) “Total Cost of Care” means, in the context of this Contract, the cost of services
as specified in Attachment A, Patient Attribution Method, Provider Taxonomy, and
Services Provided, using the list of core services in Section 4.1 (Core Services).
Article. 2 IHP REQUIREMENTS. IHP represents and warrants that it meets the requirements
of Minnesota law, in that:
2.1 Legal Entity. IHP warrants it is a recognized legal entity formed under applicable state,
federal, or tribal law and authorized to conduct business in the State of Minnesota. Its charter,
articles, and/or bylaws allow it to:
(A) Receive and distribute or make Interim and Final Payments;
(B) Make Final Payments determined to be owed to the STATE or an MCO under
this Contract;
(C) Establish reporting, and ensure IHP Participants’ compliance with reporting of
health care quality measures in Attachment B-2, Quality and Patient Experience
Measures as applicable; and
(D) Fulfill other IHP functions as defined herein.
2.2 Governance. IHP warrants that IHP and its Participants have a mechanism of Shared
Governance in accordance with Minnesota Statutes, § 256B.0755, subd. 1(d), which is
described in Attachment B-2, Quality and Patient Experience Measures. In addition:
(A) The IHP must make available a copy of this Contract to each IHP Participant, and
other individuals and entities involved in IHP governance.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 8 OF 28
(B) The IHP governing body must have a conflict of interest policy that applies to
members of the governing body, IHP management and their agents who exercise
operational or managerial control over the IHP. The conflict of interest policy must:
(1) Require the disclosure of relevant financial interests;
(2) Provide a procedure to determine whether a conflict of interest exists and set
forth a process to address conflict; and
(3) Address remedial action for any person or entity that fails to comply with the
policy.
2.3 Legal Authority. IHP warrants that it possesses the legal authority to enter into this
Contract and that it has taken all actions required by its articles, by-laws, resolutions,
operating agreements and/or applicable laws to exercise that authority, and to authorize its
undersigned signatories to execute this Contract, or any part thereof, and to bind IHP and IHP
Participants to its terms.
2.4 Documentation of Legal Entity and Fiscal Soundness.
(A) Upon request, IHP must provide copies to the STATE of all relevant documents
effectuating the IHP’s formation and operation relevant to the IHP demonstration,
including but not limited to its articles, by-laws, resolutions, operating agreements,
partnership agreements, joint venture agreements, management and consulting
agreements, asset purchase agreements, financial statements and records, and resumes
and other documentation for leaders of the IHP.
(B) Annually and ongoing, the IHP must submit to the STATE its most recent
certified financial audit, IRS Form 990, or most recent board-reviewed financial
statements of its IHP Participants by the end of the second quarter following each
Performance Period.
2.5 Assurance of Ability to Make Final Payments. IHP must have the ability to make a
Final Payment of Shared Losses for which it may be liable. The STATE may request
documentation that the IHP is capable of making a Final Payment of Shared Losses, if it is
expected that a Shared Losses payment may exceed the amount that DHS FFS program would
pay the IHP Fiscal Agent for 120 days’ services. Documentation of a repayment mechanism
may include reinsurance, escrowed funds, surety bonds, a line of credit the STATE can draw
upon, or another payment mechanism that will ensure its ability to repay the STATE.
2.6 Taxpayer Identification Number. IHP will designate a single Taxpayer Identification
Number (TIN) of the IHP Fiscal Agent to receive any Interim or Final Payments.
2.7 Provider Rosters. IHP agrees that its IHP Participants and providers will remain as listed
on the Roster reported to the STATE each quarter, except that:
(A) IHP may add IHP Participant locations, clinics, groups of providers, or individual
Primary Care Providers or Specialty Providers to its Roster by the last day of each
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 9 OF 28
quarter. IHP may add non-Participant locations, clinics, regional health systems, or
groups of providers only by amending Attachment B-1 pursuant to section 11.5.
(B) Any changes to processes for maintaining provider Rosters and corresponding
impacts to Attribution will be discussed with the IHP, and at least ninety (90) days’
notice will be provided to the IHP.
2.8 Statutory Eligibility. IHP warrants that it is eligible to participate in the demonstration
consistent with Minnesota Statutes, § 256B.0755, in that it and/or its Participants has or will:
(A) Establish processes to monitor and ensure the quality of care provided;
(B) Provide the full scope of primary care, and adopt methods of care delivery so that
the full scope of primary care is provided and care is coordinated across the spectrum
of services provided;
(C) Contract and/or coordinate with necessary providers and clinics for the delivery
of care; and contract or form partnerships with community-based organizations and
public health resources;
(D) Develop and use processes to engage Patients and their families meaningfully in
the care they receive;
(E) Have the capability to use data provided by the STATE to identify opportunities
for Patient engagement and to stratify its population to determine the care model
strategies needed to improve outcomes; and
(F) Provide consistent implementation of its care delivery model regardless of
whether a Patient is enrolled in FFS or managed care in accordance with Minnesota
Statutes, § 256B.0755, subd. 1(c).
2.9 Insurance and Insurance Risk Management. IHP agrees that it will:
(A) At all times during the term of the Contract keep in force a commercial general
liability insurance policy or a program of self-insurance with the following minimum
amounts: $2,000,000 per occurrence and $2,000,000 annual aggregate, protecting it
from claims for damages for bodily injury, including sickness or disease, death, and
for care and loss of services as well as from claims for property damage, including
loss of use which may arise from operations under the Contract whether the
operations are by the IHP or by a subcontractor or by anyone directly or indirectly
employed by the IHP under the Contract.
(B) Upon request of the STATE, purchase stop loss insurance or another form of
insurance risk management pursuant to Minnesota Statutes, § 256B.0755, subd. 1 (e).
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 10 OF 28
Article. 3 DUTIES.
3.1 Participation in Demonstration. IHP and the STATE agree to participate in the
demonstration described in Minnesota Statutes, § 256B.0755.
3.2 Provider Enrollment. All IHP Participants and their providers must be enrolled in
MHCP and comply with the provisions of the MHCP Provider Agreement, as amended.
3.3 Shared Savings or Losses. IHP understands and agrees that the demonstration requires
calculation of Shared Savings or Shared Losses based upon the Attribution of Patients to the
IHP. The Attribution model is described in Attachment A, Patient Attribution Method,
Provider Taxonomy, and Services Provided, appended and made a part of this Contract. The
Shared Savings and Shared Losses calculation is described in Attachment B-1, IHP-Specific
Governance and Financial Settlement Information appended and made a part of this Contract.
3.4 Provision of Data. The Parties agree to provide data as follows:
3.4.1 Data from IHP. IHP and/or its Participants agrees to provide necessary data in the
form of claims and/or encounters, as required by its MHCP Provider Agreement with DHS
or its contract with any MCO that participates in the Minnesota Health Care Programs,
using standard data formats as required by state and federal law and/or the relevant
contract.
(A) Claims and/or encounters must be submitted within the timeframes required by
the relevant provider agreement or contract.
(B) Quality and patient experience data must be submitted consistent with the data
collection and submission requirements of the Minnesota Statewide Quality
Reporting and Measurement System (Minnesota Rules, Chapter 4654) for measures
in Attachment B-2, Quality and Patient Experience Measures.
(C) In the event the STATE identifies trends or patterns suggesting improper claim
submission, discriminatory marketing activities, selective recruitment, or avoidance
of at-risk patients, IHP agrees to submit additional documentation as required by the
STATE for further investigation.
(D) Upon request, the IHP shall provide status updates, data, or reports to the STATE
associated with this demonstration to assist the STATE in meeting CMS monitoring
and reporting obligations related to the status and progress of the IHP’s care delivery
transformation. This includes: participation in IHP learning collaboratives, tracking
the progress of the IHP’s analysis of utilization and ACG output data provided by the
STATE as well as the IHP’s clinical data, and updates on the progress of expansion
and formation of relationships and coordination with community partners.
3.4.2 Data from STATE. STATE agrees to provide the following data in a secure format:
(A) Clinical Data. The STATE will provide clinical data, ACG risk adjustment
output and claims-level data outlined in (1) or (2) below for the IHP’s Attributed
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 11 OF 28
Population monthly throughout the term of this Contract, unless otherwise mutually
agreed by the Parties in writing. Data will be derived from the STATE data
warehouse, and will include both FFS claim data and MCO encounter data in a form
and format determined by the STATE. The STATE will provide IHP with at least
ninety (90) days’ notice of changes in the data format, unless otherwise mutually
agreed by the Parties.
(1) Data for a rolling twelve (12) month period will be provided on a monthly basis
no later than the final business day of each month, unless otherwise mutually agreed
in writing by the Parties. The ACG risk adjustment output will have a three (3)
month lag for Claims Run-out; claims-level data will not have a lag for Claims Runout.
(2) Data will include patient claim-level data (which must be protected according to
Article. 8) including name and date of birth; procedure codes and diagnosis codes,
inpatient and emergency department utilization; medical and pharmacy utilization;
predictive risk information including an individual risk score; and indices of care
coordination for the defined Attributed Population. All lines of claims for chemical
and alcohol dependency treatment programs as governed by 42 USC § 290dd-2 and
42 CFR § 2.1 to § 2.67 will be excluded.
(B) Quarterly Total Cost of Care Data Package. The STATE will provide lists of
Patients with name and date of birth who are attributed to the IHP, their Total Cost of
Care, and risk score by forty-five (45) days after the end of each quarter, according to
the methodology described in Attachment A, Patient Attribution Method, Provider
Taxonomy, and Services Provided, applied to the eligible populations described in
Section 1, Eligible and Excluded Populations, and based on the Settlement
Information Sets described in Attachment B-1, IHP-Specific Governance and
Financial Settlement Information.
(C) Annual payment-to-charge ratio or equivalent cost factor as determined by the
STATE. The STATE will provide a payment-to-charge ratio or equivalent cost factor
annually to the IHP and no later than forty-five (45) days after the beginning of the
Performance Period.
(D) IHP may reconcile its patients to its Attributed Population list.
(1) In the event that IHP believes an Attributed Population list contains errors, IHP
must provide notice and supporting data to the STATE, according to error report
specifications provided by the STATE, no later than sixty (60) days after the
receiving the Attributed Population list associated with the settlement calculation.
(2) The STATE will review the possible error(s) and at least thirty (30) days before
the Final Payment calculation will provide a written response of whether it will make
changes based upon this review. The determination that results from the STATE’s
review shall be final. Any adjustment to the IHP Attributed Population based on the
STATE’s review will be included in the IHP’s Final Payment calculation.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 12 OF 28
(E) The STATE shall not provide provider- or episode-specific cost of care for any
code or encounter, pursuant to Minnesota Statutes, § 256B.69, subd. (9)(c).
3.4.3 Data. The Parties will work together to anticipate and mitigate problems that may
affect the data in Article 3.
3.5 Data Analysis. The STATE shall perform necessary data analysis to calculate the
Attribution and settlement methods described in Attachment A, Patient Attribution Method,
Provider Taxonomy, and Services Provided, and Attachment B-1, IHP-Specific Governance
and Financial Settlement Information, respectively.
3.6 Required Reports and Notices.
(A) IHP shall provide the initial Roster of its Participants and Primary Care and
Specialty Providers to the STATE forty-five (45) days prior to the beginning of the
Performance Period.
(B) IHP shall notify the STATE of a change in its Authorized Representative,
pursuant to the timeframes in section 6.2.
(C) IHP shall notify the STATE within ten (10) days of the following events:
(1) Material change in fiscal soundness that may impair the ability of IHP to perform
its obligations under this Contract.
(2) Upon being served with any legal action filed with a court or administrative
agency, related to this Contract or which may materially affect the IHP’s ability to
perform its obligations hereunder.
(D) IHP shall notify the STATE of errors in its Attributed Population list consistent
with the timeframes in 3.4.2 above.
(E) Report Certification. As a condition for receiving payment and upon request, IHP
shall certify its data and reports that are utilized by the STATE for purposes
including, but not limited to Total Cost of Care calculations and provider Rosters.
(1) Data or reports which must be certified are:
(a) Provider Rosters pursuant to section 3.6(A);
(b) Alternative quality reporting (only for IHPs who have alternative quality
reporting in Attachment B-2, Quality and Patient Experience Measures
(c) Other data or reports requested by the STATE with notice that a certification
is required; and
(d) Errors in its Attributed Population list pursuant to section 3.4.2(D).
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 13 OF 28
(2) The certification must be signed by an officer of the IHP or an individual who
has been delegated the authority to sign for the IHP chief executive officer or chief
financial officer. The certification shall accompany the data or report, or IHP may
submit a separate written certification due by the 5th day of the following month for
any submissions in the previous month. The certification must identify each
submission, the date it was submitted, and attest, based on best knowledge,
information, and belief, to the accuracy, completeness and truthfulness of the data or
report.
3.7 Patient Protection and Patient-Centeredness.
(A) IHP shall comply with Medicaid marketing requirements:
(1) The IHP, its agents and marketing representatives, may not offer or grant any
reward, favor or compensation as an inducement to a MHCP recipient to receive
services from the IHP or an IHP Participant.
(2) The IHP, acting indirectly through publications and other marketing activity, or
through mass media advertising (including the Internet), may inform MHCP
recipients of the availability of IHP-related services through the IHP, the location
and hours of service and other IHP characteristics, subject to all restrictions in this
section. IHP shall provide the STATE with a timely advance copy of such materials.
(B) Patients attributed to the IHP are free to choose any qualified provider.
(C) IHP and its Participants must not discriminate among Patients on the basis of
health status and must not engage in activities designed to result in selective
recruitment and attribution of Patients with more favorable health status.
(D) IHP and its Participants shall have processes in place to accomplish the
following:
(1) Promote patient engagement;
(2) Develop infrastructure for IHP Participants to internally report on quality and
cost metrics that enables the IHP to monitor performance and use these results to
improve care over time; and
(3) Coordinate care across and among providers.
Article. 4 PAYMENT.
4.1 Claims Payments and Demonstration Payments. Services shall be paid as follows:
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 14 OF 28
(A) IHP Participants will receive reimbursement for health care services according to
and under its contract(s) with the Department of Human Services FFS program, or the
relevant MCO in which the Patient is enrolled; and
(B) Shared Savings or Shared Losses will be calculated by the STATE pursuant to the
method in Attachment B-1, IHP-Specific Governance and Financial Settlement
Information, and distributed based on the method described in Section 2, Settlement
Process. Final Payment of Shared Savings is reducible by the score calculated for
quality and patient experience determined by Attachment B-2, Quality and Patient
Experience Measures.
4.2 Terms of Payment. Shared Savings and Shared Losses will be calculated, and paid
according the timeframes in this section.
(A) Interim Payments.
(B) Shared Savings and Shared Losses interim settlements will be calculated by the
STATE and reported to the IHP and applicable MCOs no later than the last business
day of the fifth month following the close of the Performance Period, as described in
2.4 (B) of Attachment B-1, IHP-Specific Governance and Financial Settlement
Information.
(1) Shared Savings Interim Payments owed by the STATE to the IHP based upon
FFS shall be paid by the STATE to the IHP on the next available FFS payment
warrant after the notice in 4.2(A)(1) above.
(2) The STATE will direct applicable MCOs to make Shared Savings Interim
Payments to the IHP within thirty (30) days of the date that the STATE informs the
MCOs of the amount owed.
(C) Final Payment. Final Payments of Shared Savings and Shared Losses will be
calculated by the STATE and reported to the IHP and applicable MCOs no later than
the last business day of the seventeenth (17th) month following the close of the
Performance Period, as described in 2.4 (C) of Attachment B-1, IHP-Specific
Governance and Financial Settlement Information. The receipt of data necessary to
complete the Final Payment calculation is a condition precedent to the Final Payment.
(1) Final Payment of Shared Savings owed by the STATE to the IHP based upon
FFS shall be paid by the STATE to the IHP on the next available DHS FFS payment
after the notice in 4.2(B)(1) above.
(2) The STATE will direct applicable MCOs to make Final Payments of Shared
Savings to the IHP within thirty (30) days of the date that the STATE informs the
MCOs of the amount owed.
(3) Final Shared Losses, as calculated by the STATE, shall be paid by the IHP to the
STATE or applicable MCO no later than one hundred and twenty (120) days after
the calculation in section 4.2(B)(1) above is completed and the IHP is notified. The
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 15 OF 28
STATE may, at its option, offset any Shared Losses obligation by withholding
payment from current payment warrants on a schedule to be agreed upon between
the Parties.
(D) Certain Laws not Applicable to Payments. The Parties agree that Interim and
Final payments are not claims payments subject to the prompt pay laws in Minnesota
Statutes, § 62Q.75. The vendor payment timelines in Minnesota Statutes, § 16A.124
apply to these payments only after final calculation pursuant to this Article.
(E) All services provided by IHP pursuant to this Contract shall be performed to the
satisfaction of the STATE, as determined at its sole discretion, and in accord with all
applicable federal, state, and local laws, ordinances, rules and regulations including
business registration requirements of the Office of the Secretary of State.
(F) Neither Party shall pay interest on any amounts due hereunder.
4.3 Payment Errors. In the event of a payment error identified by either Party:
(A) From DHS FFS system: If either Party determines that there has been a material
error in its payment to or from the other Party that resulted in overpayment or
underpayment due to reasons that do not include the agreed-upon methodology in the
Attachments, or Fraud or Abuse by the IHP, its Participating Entities or an Attributed
Patient; then the STATE or IHP may make a claim under this section within sixty
(60) days from the discovery of the error.
(B) From an MCO payment error: If either Party determines that there has been a
material error in payment that resulted in overpayment or underpayment, which error
is due to changes in or errors in claims or encounters processing by an MCO, the
procedure in section 4.3(A) shall be followed except that the timeframe for initial
notice shall be extended to ninety (90) days.
(C) The IHP must have filed a timely and Patient-Specific appeal of Attribution under
section 3.4.2(D) in order to assert any claims regarding Attribution.
(D) The Party receiving the claim in (A) or (B) above shall acknowledge in writing or
e-mail the receipt of the claim.
(E) Neither Party shall assert any claim for or seek the payment of or make any
adjustment for any erroneous payment made pursuant to this Contract more than one
year after the date such payment was actually received by the receiving Party.
Article. 5 TERM AND TERMINATION; DISPUTE RESOLUTION.
5.1 Effective Dates. This Contract shall be effective on January 1, 2017, or upon the date
that the final required signature is obtained by the STATE, pursuant to Minnesota Statutes,
§ 16C.05, subd. 2, whichever occurs later, and shall remain in effect through December 31,
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 16 OF 28
2017, or until all obligations set forth in this Contract have been satisfactorily fulfilled,
whichever occurs first.
5.2 Automatic Renewal. Notwithstanding the termination date in section 5.1 above, this
Contract shall automatically renew at the end of the current term for a successive one-year
term, not to exceed a total of three years, unless the STATE or IHP gives written notice of its
intention not to renew (consistent with 5.3.4 below), at least sixty (60) days before expiration
of the then-current term.
5.3 Termination.
5.3.1 Termination By STATE.
(A) Without Cause. This Contract may be terminated by the STATE at any time,
with or without cause, upon ninety (90) days written notice to IHP. In the event of
such a termination, IHP shall be entitled to payment, determined on a pro rata basis,
of Shared Savings through the effective date of termination for work or services
satisfactorily performed, but IHP will not be required to make payment for Shared
Losses, if any, through the effective date of termination.
(B) For Cause. The STATE has the right to suspend or terminate this Contract in
writing immediately when the STATE deems:
(1) The health or welfare of its Patients is endangered;
(2) When the STATE has reasonable cause to believe that the IHP has breached a
material term of the Contract; or
(3) When IHP non-compliance with the terms of the Contract may jeopardize federal
financial participation in the STATE’s Medicaid program.
(C) Insufficient Funds. The STATE may immediately terminate this Contract if it
does not obtain funding from the Minnesota Legislature, or other funding source; or if
funding cannot be continued at a level sufficient to allow for payment. Termination
will be by written notice to the IHP. The IHP will be entitled to or obligated to pro
rata payment of Shared Savings or Shared Losses up to the date of termination for
services satisfactorily performed to the extent that funds are available. The STATE
will not be assessed any penalty if the contract is terminated because of the decision
of the Minnesota Legislature, or other funding source, not to appropriate funds. The
STATE must provide the IHP notice of the lack of funding within a reasonable time
of the STATE’s receiving that notice.
(D) Breach. Notwithstanding any other provision of this Contract, upon STATE’s
knowledge of a curable material breach of the Contract by IHP, STATE shall provide
IHP written notice of the breach and thirty (30) days to cure the breach from the date
it receives the notice of breach, unless a longer period is mutually agreed upon if the
breach can be cured. In urgent situations, as determined by the STATE, the STATE
may establish a shorter time period to cure the breach. If IHP does not cure the
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 17 OF 28
breach within the time allowed, IHP will be in default of this Contract and STATE
may terminate the Contract immediately. If IHP has breached a material term of this
Contract and cure is not possible, STATE may immediately terminate this Contract.
(E) The STATE may terminate this Contract in the event the IHP:
(1) Becomes insolvent, is dissolved or liquidated;
(2) Files or has filed against it a petition in bankruptcy and, in the case of an
involuntary petition, such petition is not dismissed within thirty (30) days;
(3) Makes a general assignment for the benefit of its creditors;
(4) IHP or any of its Participants, Primary Care Providers, Specialty Providers or
principals is in violation of section 10.6 below, unless the IHP has promptly provided
termination notice to and taken steps to disaffiliate itself from any such Participant,
Primary Care Provider, Specialty Provider or principal; or
(5) Ceases conducting business in the ordinary course.
5.3.2 Pre-termination Action by STATE. The STATE may, but is not required to, take
one or more of the following actions if the STATE concludes termination of the Contract is
warranted:
(A) Provide a warning notice to the IHP regarding noncompliance;
(B) Request a Corrective Action Plan for the IHP; or
(C) Place the IHP on a special monitoring plan.
5.3.3 Termination by IHP. IHP may terminate this Contract under the following
circumstances:
(A) With Cause; Loss of an IHP Participant. IHP must notify the STATE under
section 3.6 above in the event that one or more of its constituent IHP Participants will
no longer be available to treat Patients under this Contract. In the event that this
departing IHP Participant provides care for more than fifty percent (50%) of the
IHP’s most recent quarter Attributed Population, the IHP may provide written notice
of termination and follow the termination procedures outlined in section 5.3.4. The
IHP will be entitled to pro rata payment of Shared Savings up to the effective date of
the termination.
(B) Without Cause. Upon ninety (90) days’ written notice to the STATE. The IHP
will be entitled or obligated to pro rata payment of Shared Savings or Shared Losses
up to the effective date of the termination in the second and third years of the
demonstration only.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 18 OF 28
5.3.4 Termination Procedures. Upon termination of this Contract and continuing until
Final Payment is complete, the IHP shall, upon request of the STATE, provide information
to the STATE that may be necessary to end data collection and determine payments owed.
IHP shall cooperate with a mutually agreed-upon termination plan.
5.3.5 Dispute Resolution. In the event of a dispute between the STATE and IHP, the
Parties will work together in good faith to resolve any disputes about their business
relationship.
(A) If the Parties are unable to resolve the dispute within thirty (30) days following
the date one party sent written notice of the dispute to the other party, the Parties may
submit the dispute to non-binding mediation before a single mediator prior to
commencing any other forms of dispute resolution. The mediator shall accept both
written and oral argument as requested, and make its recommendation within fifteen
(15) days of receiving the request for recommendation unless the Parties mutually
agree to a longer time period. The Commissioner of Human Services shall resolve all
disputes after taking into account the recommendations of the mediator and within
three (3) business days after receiving the recommendation of the mediator. The cost
of mediation shall be shared equally between the Parties, and each party shall be
responsible for its own expenses, including attorney’s fees. Whether or not the
Parties elect to submit the dispute to non-binding mediation, nothing in this paragraph
shall bar either party from enforcing its rights under this Contract in any legal forum.
(B) IHP may not dispute the methodologies in the Attachments.
Article. 6 AUTHORIZED REPRESENTATIVE AND RESPONSIBLE AUTHORITY.
6.1 STATE. The STATE's authorized representative for the purposes of administration of
this Contract is Heather Petermann, or her successor. If the STATE’s authorized
representative changes at any time during this Contract, the STATE will provide notice to the
IHP.
6.2 IHP. The IHP’s authorized representative is listed in Attachment B-1, IHP-Specific
Governance and Financial Settlement Information. If IHP’s authorized representative
changes at any time during this Contract, IHP must notify the STATE within three (3)
business days.
Article. 7 QUALITY AND PATIENT EXPERIENCE MEASURES. The STATE and IHP
agree that the following standardized set of quality measures will be used as described in
Attachment B-2, Quality and Patient Experience Measures to affect the amount of Shared
Savings, subject to any modifications described in said Attachment.
7.1 Source of Measure Specifications and Reporting Requirements. The STATE will use
the Minnesota Statewide Quality Reporting and Measurement System measure specifications
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 19 OF 28
and reporting requirements, including all updates and modifications, as published by the
Minnesota Department of Health (MDH) in Minnesota Rules, Chapter 4654, for each
respective measure described in Attachment B-2 and standardized measure specifications and
reporting requirements for each measure described in said attachments.
7.2 Changes in Measures. The STATE may change the measures both in response to
changes promulgated by MDH and Minnesota Community Measurement (MNCM) or any
other measurement organization identified in Attachment B-2, Quality and Patient Experience
Measures as applicable, and as the IHP demonstration evolves.
(A) The STATE will not notify IHP regarding updates and modifications that
originate from MDH, MNCM, or other organization used as a source of measures
when the organization publishes its measure specifications.
(B) The STATE will only add to or delete from the list of measures listed in
Attachment B-2, Quality and Patient Experience Measures as applicable prior to a
Performance Period, and will provide notice to IHP of the proposed new measure at
least ninety (90) days in advance.
7.3 Changes in Calculation Methods. The STATE will notify the IHP of the thresholds
described in Attachment B-2, Quality and Patient Experience Measures as applicable, before
the beginning of the Performance Period by publishing preliminary thresholds on the DHS
public website. The STATE will notify the IHP of final thresholds upon calculation using the
data based on the most recent Quality Measurement Period. The STATE will work with the
IHP on any modifications to the calculation methods, quality measure thresholds, or other
modifications resulting from changes to a measure or measures pursuant to section 7.1 or 7.2
to achieve the goals of the demonstration. The STATE will notify the IHP of the change.
7.4 Quality and Patient Experience Data Appeals. Appeal processes that the IHP may use
for quality and patient experience data are limited to those provided by the relevant
organizations receiving the data (for example, MDH and MNCM) pursuant to Minnesota
Rules, Part 4654.
Article. 8 INFORMATION PRIVACY AND SECURITY.
8.1 Part of the Welfare System. For purposes of executing its responsibilities and to the
extent set forth in this Contract, the IHP will be considered part of the “welfare system,” as
defined in Minnesota Statutes, § 13.46, subd. (1).
8.2 Information Privacy and Security. IHP and the STATE must comply with the
Minnesota Government Data Practices Act, Minnesota Statutes, Chapter 13, and the Health
Insurance Portability Accountability Act (HIPAA), 45 CFR Parts 160 and 164, as it applies to
all data provided by STATE under this Contract, and as it applies to all data created,
collected, received, stored, used, maintained, or disseminated by IHP under this Contract.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 20 OF 28
(A) The data privacy and security of data provided by the STATE to the IHP in
section 3.4.2 will be governed by the business associate agreement attached as
Attachment B-3, Business Associate, and incorporated by reference herein..
(B) The civil remedies of Minnesota Statutes § 13.08 apply to data governed by the
Minnesota Government Data Practices Act. The remedies of HIPAA apply to the
release of data governed by HIPAA.
8.4. It is expressly agreed that, with the exception of the data in section 3.4.2, STATE will not
be disclosing or providing information protected under the Minnesota Government Data
Practices Act, Minnesota Statutes Chapter 13, (the “Data Practices Act”) as “not public data”
on individuals to IHP under this Contract, as that term is defined under the Data Practices Act.
8.5. Notwithstanding paragraph 8.4, in its capacity as IHP under this Contract, IHP must
comply with the provisions of the Data Practices Act as though it were a governmental entity
as defined by the Data Practices Act. IHP will be performing functions of a government entity
under Minn. Stat. § 13.05, subd. 11, and thus any data created, collected, received, stored,
used, maintained or disseminated by IHP in performing its duties under this contract is subject
to the protections of the Data Practices Act. The civil remedies of Minnesota Statutes, section
13.08 apply to the release of the data governed by the Data Practices Act, Minnesota Statutes,
ch. 13, by either the IHP or the STATE.
8.6. IHP’s obligations while performing the functions of a government entity include, but are
not limited to, complying with Minn. Stat. § 13.05, subd. 5 to establish appropriate security
safeguards for all records containing data on individuals.
8.7. IHP must comply with Minn. Stat. § 13.055 to investigate and appropriately report or
notify regarding any potential unauthorized acquisition of data created, collected, received,
stored, used, maintained, or disseminated by GRANTEE in performing its duties under this
Contract.
Article. 9 Intellectual Property Rights.
9.1 Definitions. Works means all inventions, improvements, discoveries (whether or not
patentable or copyrightable), databases, computer programs, reports, notes, studies,
photographs, negatives, designs, drawings, specifications, materials, tapes, and disks
conceived, reduced to practice, created or originated by IHP, its employees, agents, and
subcontractors, either individually or jointly with others in the performance of this Contract.
Works includes “Documents.” Documents are the originals of any databases, computer
programs, reports, notes, studies, photographs, negatives, designs, drawings, specifications,
materials, tapes, disks, or other materials, whether in tangible or electronic forms, prepared by
IHP, its employees, agents, or subcontractors, in the performance of this Contract.
9.2 Use of Works and Documents. IHP owns any Works or Documents developed by the
IHP in the performance of this Agreement. The STATE and the U.S. Department of Health
and Human Services will have royalty free, non-exclusive, perpetual and irrevocable right to
reproduce, publish, or otherwise use, and to authorize others to use, the Works or Documents
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 21 OF 28
for government purposes. If using STATE data for publication, IHP must cite the data, or
make clear by referencing that STATE is the source.
Article. 10 COMPLIANCE WITH STATE AND FEDERAL LAWS. IHP, its Participants
and other individuals or entities performing functions related to IHP’s activities shall comply
with all applicable state and federal laws and regulations in the performance of its obligations
under this Contract. Any revisions to applicable provisions of federal or state law and
implementing regulations, and policy issuances and instructions, except as otherwise specified in
this Contract, apply as of their effective date. If any terms of this Contract are determined to be
inconsistent with rule or law, the applicable rule or law provision shall govern.
10.1 Compliance with Federal Laws. Notwithstanding any applicable waivers of fraud and
abuse laws, the IHP shall comply with all applicable federal laws in the performance of its
obligations under this Contract including, but not limited to:
(A) Federal Criminal Law;
(B) The False Claims Act (31 USC 3729 et seq.);
(C) The anti-kickback statute (42 USC 1320a-7b(b);
(D) The civil monetary penalties law (42 USC 1320a-7a); and
(E) The physician self-referral law (42 USC 1395nn).
10.2 Affirmative Action And Non-Discrimination.
10.2.1 Affirmative Action requirements for IHPs with more than 40 full-time
employees and a contract in excess of $100,000. If IHP has had more than 40 full-time
employees within the State of Minnesota on a single working day during the previous
twelve months preceding the date IHP submitted its request for proposal response to the
STATE, it must have an affirmative action plan, approved by the Commissioner of Human
Rights of the State of Minnesota, for the employment of qualified minority persons,
women and persons with disabilities. See Minnesota Statutes § 363A.36. If IHP has had
more than 40 full-time employees on a single working day during the previous twelve
months in the state in which it has its primary place of business, then IHP must either: 1)
have a current Minnesota certificate of compliance issued by the Minnesota Commissioner
of Human Rights; or 2) certify that it is in compliance with federal Affirmative Action
requirements.
10.2.2 Affirmative Action and Non-Discrimination requirements for all IHPs. The
IHP agrees not to discriminate against any employee or applicant for employment because
of race, color, creed, religion, national origin, sex, marital status, status in regard to public
assistance, membership or activity in a local commission, disability, sexual orientation, or
age in regard to any position for which the employee or applicant for employment is
qualified. Minnesota Statutes, § 363A.02. IHP agrees to take affirmative steps to employ,
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 22 OF 28
advance in employment, upgrade, train, and recruit minority persons, women, and persons
with disabilities.
(A) The IHP must not discriminate against any employee or applicant for
employment because of physical or mental disability in regard to any position for
which the employee or applicant for employment is qualified. The IHP agrees to take
affirmative action to employ, advance in employment, and otherwise treat qualified
disabled persons without discrimination based upon their physical or mental disability
in all employment practices such as the following: employment, upgrading, demotion
or transfer, recruitment, advertising, layoff or termination, rates of pay or other forms
of compensation, and selection for training, including apprenticeship, consistent with.
Minn. Rule 5000.3550.
(B) IHP agrees to comply with the rules and relevant orders of the Minnesota
Department of Human Rights issued pursuant to the Minnesota Human Rights Act.
(C) Notification to employees and other affected parties. The IHP agrees to post in
conspicuous places, available to employees and applicants for employment, notices in
a form to be prescribed by the commissioner of the Minnesota Department of Human
Rights. Such notices will state the rights of applicants and employees, and IHP’s
obligation under the law to take affirmative action to employ and advance in
employment qualified minority persons, women, and persons with disabilities.
(D) The IHP will notify each labor union or representative of workers with which it
has a collective bargaining agreement or other contract understanding, that the IHP is
bound by the terms of Minnesota Statutes, § 363A.36 of the Minnesota Human Rights
Act and is committed to take affirmative action to employ and advance in
employment minority persons, women, and persons with physical and mental
disabilities.
10.2.3 Compliance with Department of Human Rights Statutes. In the event of IHP’s
noncompliance with the provisions of this clause, actions for noncompliance may be taken
in accordance with Minnesota Statutes § 363A.36, and the rules and relevant orders issued
pursuant to the Minnesota Human Rights Act.
10.3 Workers' Compensation. The IHP certifies that it is in compliance with Minnesota
Statutes, § 176.181, subdivision 2, pertaining to workers’ compensation insurance coverage.
The IHP’s employees and agents will not be considered employees of the STATE. Any
claims that may arise under the Minnesota Workers’ Compensation Act on behalf of these
employees or agents and any claims made by any third party as a consequence of any act or
omission on the part of these employees or agents are in no way the STATE’S obligation or
responsibility.
10.4 Voter Registration Requirement. (If applicable) IHP certifies that it will comply with
Minnesota Statutes, § 201.162 by providing voter registration services for its employees and
for the public served by the IHP.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 23 OF 28
10.5 Federal Audit Requirements. IHP certifies it will comply with the Single Audit Act,
and federal procurement regulations at 2 CFR Part 200, as applicable. All sub-recipients
receiving $500,000 or more of federal assistance in a fiscal year will obtain a financial and
compliance audit made in accordance with the Single Audit Act, or federal procurement
regulations at 2 CFR Part 200 as applicable. Failure to comply with these requirements could
result in forfeiture of federal funds.
10.6 Debarment Information.
(A) Debarment By State, its Departments, Commissions, Agencies or Political
Subdivisions. By signing this Contract, IHP certifies that neither it nor its IHP
Participants, Primary Care Providers or principals is presently debarred or suspended
by the STATE, any of its departments, commissions, agencies, or political
subdivisions. This certification is a material representation upon which this Contract
award was based. IHP shall provide immediate written notice to the STATE’S
authorized representative if at any time it learns that this certification was erroneous
when submitted or becomes erroneous by reason of changed circumstances.
(B) Certification Regarding Debarment, Suspension, Ineligibility, and Voluntary
Exclusion. Federal money will be used or may potentially be used to pay for all or
part of the work under the contract, therefore IHP certifies that it is in compliance
with federal requirements on debarment, suspension, ineligibility and voluntary
exclusion specified in the solicitation document implementing Executive Order
12549. IHP’s certification is a material representation upon which this Contract
award was based.
10.7 Ownership and Control; Exclusions of Individuals and Entities. To the extent the
IHP is not otherwise providing the following information to the STATE, the IHP as applicable
shall:
(A) Make full disclosure of ownership and control information as required by 42 CFR
§§ 455.100 through 455.106, and upon request, full disclosure of business
transactions, as is required by 42 CFR § 455.105;
(B) Make full disclosure of persons convicted of program crimes as required by 42
CFR § 455.106; and
(C) Ensure that IHP, all of its owners, managers, employees and subcontractors are
not excluded from participation in Medicare, Medicaid or other federal health care
programs. IHP must immediately report any exclusion information discovered to the
STATE.
Article. 11 OTHER PROVISIONS.
11.1 Governing Law, Jurisdiction and Venue. This Contract, and amendments and
supplements thereto, shall be governed by the laws of the State of Minnesota. Venue for all
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 24 OF 28
legal proceedings arising out of this Contract, or breach thereof, shall be in the state or federal
court with competent jurisdiction in Ramsey County, Minnesota.
11.2 Waiver. If either Party fails to enforce any provision of this Contract, that failure does
not waive the provision or the Party’s right to enforce it.
11.3 Contract Complete. This Contract contains all negotiations and agreements between
the STATE and IHP. No other understanding regarding this Contract, whether written or oral
may be used to bind either party.
11.4 Assignment. IHP shall neither assign nor transfer any rights or obligations under this
Contract without the prior written consent of the STATE.
11.5 Amendments. Any amendments to this Contract shall be in writing, and shall be
executed by the same Parties who executed the original contract, or their successors in office.
11.6 Indemnification. In the performance of this Contract by IHP, or IHP’s agents or
employees, the IHP must indemnify, save, and hold harmless the STATE, its agents, and
employees, from any claims or causes of action, including attorney’s fees incurred by the
STATE, to the extent caused by IHP’s:
(A) Intentional, willful, or negligent acts or omissions;
(B) Actions that give rise to strict liability; or
(C) Breach of contract or warranty.
The indemnification obligations of this clause do not apply in the event the claim or cause of
action is the result of the STATE’S sole negligence. This clause will not be construed to bar any
legal remedies the IHP may have for the STATE’S failure to fulfill its obligation under this
Contract.
11.7 STATE Audits. Under Minnesota Statutes, § 16C.05, subd. 5, the books, records,
documents, and accounting procedures and practices of the IHP and its employees, agents, or
subcontractors relevant to this Contract shall be made available and subject to examination by
the STATE, including the contracting Agency/Division, Legislative Auditor, and State
Auditor for a minimum of six years from the end of this Contract.
11.8 Right to Review before Publication. Each Party agrees to provide to the other Party a
prepublication copy of materials listed below that identifiably mention the IHP and the
demonstration project. Each Party agrees to provide comments, if any, within ten (10) days of
receipt of the materials. IHP shall not state or imply that the STATE endorses the IHP’s
products or services.
Each Party shall provide to the other Party copies of any formal presentation by the Party or
its subcontractors, including reports, statistical or analytical materials, papers, articles, or
professional publications, based on information obtained through the administration of this
IHP Contract.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 25 OF 28
11.9 Religious-Based Counseling. IHP agrees that no religious-based counseling shall take
place under the auspices of this Contract.
11.10 Payment to Subcontractors. As required by Minnesota Statutes, §16A.1245, the IHP
must pay all subcontractors, less any retainage, within ten (10) days of the IHP’s receipt of
payment from the STATE for undisputed services provided by the subcontractor(s) and must
pay interest at the rate of one and one-half percent per month or any part of a month to the
subcontractor(s) on any undisputed amount not paid on time to the subcontractor(s). For the
purposes of this clause, subcontractor does not include IHP Participants or providers.
11.11 Severability. If any provision or paragraph of this Contract is found by a court of
competent jurisdiction to be legally invalid or unenforceable, such provision or paragraph
shall be deemed to have been stricken from this Contract and the remainder of this Contract
shall be deemed to be in full force and effect.
11.12 Execution in Counterparts. Each party agrees that this Contract may be executed in
two or more counterparts, all of which shall be considered one and the same agreement, and
which shall become effective if and when both counterparts have been signed and dated by
each of the parties. It is understood that both parties need not sign the same counterpart.
11.13 Survival. All provisions of this Contract that, by their nature and content, should
survive the termination of this Contract in order to achieve the fundamental purposes of this
Contract shall survive and continue to bind the Parties. IHP’s continuing obligations, after
said period, include but are not limited to the following provisions: Article. 8 Information
Privacy and Security; 11.1 Jurisdiction and Venue, 11.6 Indemnification, and 11.7 State
Audits.
Signature page follows.
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 26 OF 28
IN WITNESS WHEREOF, the Parties hereto have executed this Contract. This Contract is
hereby accepted and considered binding in accordance with the terms outlined in the preceding
statements.
STATE OF MINNESOTA
[NAME OF IHP]
DEPARTMENT OF HUMAN SERVICES
(Two corporate officers must execute)
By:
By:
Name:
Print Name:
Title: Assistant Commissioner
Title:
Date:
Date
And
By:
Print Name:
Title:
Date
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 27 OF 28
List of Attachments
Attachment A, Patient Attribution Method, Provider Taxonomy, and Services Provided
Attachment B-1, IHP-Specific Governance and Financial Settlement Information
Attachment B-2, Quality and Patient Experience Measures
Attachment B-3, Business Associate
2017_RFPVersion_IHP_Contract_Model_20160415
[NAME OF IHP]
INTEGRATED HEALTH PARTNERSHIPS CONTRACT – PAGE 28 OF 28
ATTACHMENT A: Patient Attribution Method, Provider
Taxonomy, and Services Provided
Eligible and Excluded Populations: This document further describes the populations
who are included or excluded from Attribution and Total Cost of Care.
Eligible Populations. The following persons who are recipients of Medical Assistance
and MinnesotaCare are eligible for Attribution to the IHP:
(1) Medical Assistance Enrollees: Including pregnant women, children under 21,
adults without children, and state-funded Medical Assistance.
(2) MinnesotaCare Enrollees: Including children under 21, and adults without
children. Individuals must belong to an eligible group under Minnesota Statutes,
Chapter 256L, meet income criteria, satisfy all other eligibility requirements, and pay
a premium to the State.
(3) Recipients receiving Medical Assistance due to blindness or disability as
determined by the U.S. Social Security Administration or the State Medical Review
Team who are not dually eligible for Medicare.
Excluded Populations from Attribution. The following persons are excluded from
Attribution to the IHP:
(1) Recipients receiving Medical Assistance who are dually eligible for Medicare.
(2) Recipients receiving Medical Assistance under the Refugee Assistance Program
pursuant to 8 U.S.C. 1522(e).
(3) Individuals who are Qualified Medicare Beneficiaries (QMB), as defined in
Section 1905(p) of the Social Security Act, 42 U.S.C. 1396d (p), who are not
otherwise receiving Medical Assistance.
(4) Individuals who are Service Limited Medicare Beneficiaries (SLMB), as defined
in Section 1905(p) of the Social Security Act, 42 U.S.C. 1396a(a)(10)(E)(iii) and
1396d(p), and who are not otherwise receiving Medical Assistance.
(5) Non-citizen recipients who only receive emergency Medical Assistance under
Minnesota Statutes, section 256B.06, subd. 4.
(6) Recipients receiving Medical Assistance on a medical spend down basis.
(7) Medical Assistance recipients with cost-effective employer-sponsored private
health care coverage, or who are enrolled in a non-Medicare individual health plan
determined to be cost-effective according to Minnesota Statutes, section 256B.69,
subd. 4, (b)(9).
ATTACHMENT A – PAGE 1 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
(8) Medical Assistance recipients with private health care coverage through a Health
Maintenance Organization (HMO) licensed under Minnesota Statutes, Chapter 62D.
(9) MinnesotaCare recipients who are enrolled in the Healthy Minnesota
Contribution Program.
(10) The commissioner may exclude recipients enrolled in Minnesota Senior Care
Plus (MSC+), other than those in section 1.3(1) above.
Excluded Populations from Total Cost of Care. The following persons are excluded
from the Total Cost of Care (TCOC) Performance Assessment Process as described in
Attachment D, section 1.3, Total Cost of Care (TCOC) Performance Assessment Process:
a) Recipients for whom DHS receives incomplete claims data due to third-party
liability coverage.
Patient Attribution Method. This section describes the STATE’s method of how a
recipient in the MHCP FFS program or a managed care organization enrollee is assigned to the
IHP’s Attributed Population as an Attributed Patient. This section also details the provider
taxonomy that should be utilized by the IHP when providing the STATE with a provider roster
for the purposes of determining attribution.
2.1.1 Definitions. For the purposes of this Attachment:
a) Capitalized terms in this Attachment take the same meanings as in the Contract.
b) “E&M” refers to Evaluation and Management coding.
c) “HCPCS” refers to the HCFA Common Procedural Coding System.
d) “Non-IHP provider” means a provider not listed on a Roster submitted by an IHP.
Patients. Patients must have had at least one visit or encounter with a Roster provider
during the Performance Period and such visit must have been paid to a billing entity on the
Roster to be eligible for Attribution. Certain populations are categorically excluded from the
IHP model (for example, persons with dual eligibility), and are removed from the pool of
MHCP Recipients who can be attributed (see 1.1 “Eligible and Excluded Populations”).
Patients who have less than six (6) months of continuous enrollment in qualifying programs
or less than nine (9) total months of enrollment in qualifying programs during the
Performance Period are excluded from Attribution. Throughout the course of the
Performance Period, a Patient’s attribution status (either among IHPs or to no IHP) may
change as the Patient’s utilization pattern changes.
Attribution Steps. Once the exclusion process is completed to determine the base
population eligible for Attribution, the Attribution process counts qualifying visits for each
MHCP Recipient across providers on all the IHP Rosters and compares the total claim counts
at each IHP to those at non-IHP providers. In performing the comparisons, there are four
steps evaluated in the following order:
ATTACHMENT A – PAGE 2 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
1)
Health Home (Health Care Home or Behavioral Health Home) claims;
2)
E&M procedures by a Primary Care Provider; and
3)
E&M procedures by a Specialty Provider; and
4)
Tie Breaking Step.
As the algorithm progresses, a MHCP recipient is either definitively assigned to an IHP and not
evaluated in subsequent steps, determined to be not attributable to any IHP for the period, or
passed to the next step in the Attribution decision process.
STEP 1. If Health Home Claim Code(s) are Present:
Patients with Health Home (HCH or BHH) care coordination claims (HCPCS Code S0280
and/or S0281) are attributed to the IHP using the treating and billing provider as follows:
1)
Patients with care coordination codes at only one IHP are attributed to the IHP.
2)
Patients with care coordination codes at more than one IHP or at non-IHP
provider(s) are attributed to the IHP or non-IHP provider(s) that submitted the greater
number of care coordination claims.
3)
Patients with an equal number of care coordination codes are attributed to the IHP
or the non-IHP provider having the most recent date of service care coordination claim..
4)
Patients with no HCH codes are assessed by the decision criteria in Step 2.
STEP 2. If Attribution From Health Home Claims Has Not Occurred, but
Qualifying Visit(s) to a Primary Care Provider are Present:
Patients with the following E&M codes paid to an IHP billing provider and performed by an IHP
Roster provider with a primary care specialty (as defined in Section 3.1 “Provider Taxonomy”)
99201 through 99215, 99304 through 99350, 99381 through 99387, 99391 through 99397,
G0402, G0438, and G0439 are attributed to the IHP as follows:
1) Patients with Primary Care Provider E&M codes at only one IHP are attributed to the
IHP.
2) Patients with more Primary Care Provider E&M codes than at any other IHP or nonIHP provider(s) are attributed to the IHP that submitted the greater number of E&M
codes by that IHP’S Primary Care Providers.
3) Patients with an equal number of Primary Care Provider E&M codes at more than one
IHP or non-IHP provider are assessed by the decision criteria as described in Step 4.
4) Patients with a greater number of E&M codes at an individual non-IHP provider(s)
than at any IHP are not attributed to any IHP.
ATTACHMENT A – PAGE 3 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
5) Patients with no Primary Care Provider E&M codes at any IHP are assessed by the
decision criteria in Step 3.
STEP 3. If Attribution From HCH Claims or Qualifying Visits to Primary Care
Providers Has Not Occurred, but Qualifying Visits to Other Specialty Providers are
Present:
Patients with the following E&M codes performed by a Specialty Provider and paid to a billing
provider from the IHP roster: 99201 through 99215, 99304 through 99350, 99381 through
99387, 99391 through 99397, G0402, G0438, and G0439 are attributed to the IHP as follows:
1)
Patients with Specialty Provider E&M codes at only one IHP are attributed to the
IHP.
2)
Patients with Specialty Provider E&M codes at more than one IHP are attributed
to the IHP that submitted the greater number of E&M codes by that IHP’S Specialty
providers.
3)
Patients with an equal number of Specialty Provider E&M codes at more than one
IHP are not attributed to any IHP.
4)
Patients with a greater number of E&M codes at an individual non-IHP
provider(s) than at any IHP Specialty Providers are not attributed to any IHP.
STEP 4. Tie Breaking:
1)
Patients with an equal number of E&M codes at more than one IHP Primary Care
Providers, and having no E&M codes at IHP Specialty Providers are attributed to the
IHP with the most recent date of service E&M claim.
2)
Patients with an equal number of E&M codes at more than one IHP Primary Care
Provider and having a greater number of E&M codes at one of those IHP Specialty
Providers are attributed to the IHP with the greater number of E&M codes at Specialty
Providers.
3)
Patients with an equal number of E&M codes at more than one IHP Primary Care
Provider, and having an equal number of E&M codes at those IHP Specialty Providers
are attributed to the IHP with the most recent Primary Care Provider date of service
E&M claim.
4)
Patients with an equal number of E&M codes at an IHP Primary Care Provider
and a non-IHP provider are attributed to the IHP if the IHP had the most recent date of
service E&M claim.
Attribution Time Periods. The Attribution Steps described above in section 1.4 will be
based on claims in a twelve (12) month period of a Patient’s claim history. If attribution does
not occur and Patient did not have any claims within the twelve (12) month period, then the
ATTACHMENT A – PAGE 4 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Attribution Steps described in sections 1.4.1 – 1.4.4 will be repeated using claims occurring
within an additional twelve (12) month period for a total of twenty-four (24) months.
Provider Taxonomy. An IHP may designate on its Roster whether a provider serves as a
Primary Care Provider (“PCP”) or Specialty Provider (“SPE”) in its organization. In absence
of this designation, the provider’s primary taxonomy code will be used to categorize the
provider according to the table below. If neither a PCP / SPE designation nor a primary
taxonomy code is included on the Roster, the primary taxonomy code for that provider from
the National Plan and Provider Enumeration System (NPPES) file will be used to categorize
the provider according to the table below. A provider taxonomy not listed in this attachment
will be considered a Specialty Provider, unless the IHP has otherwise designated the provider
as a “PCP” on their Roster.
a) Mapping Definitions from NUCC Database Download (Version 12.0, 1/1/12)
Taxonomy
PCP/SPE
Type
Classification
Specialization
207K00000X
SPE
Allopathic & Osteopathic Physicians
Allergy & Immunology
207L00000X
SPE
Allopathic & Osteopathic Physicians
Anesthesiology
207LP2900X
SPE
Allopathic & Osteopathic Physicians
Anesthesiology
Pain Medicine
207LC0200X
SPE
Allopathic & Osteopathic Physicians
Anesthesiology
Critical Care Medicine
208U00000X
SPE
Allopathic & Osteopathic Physicians
Clinical Pharmacology
208C00000X
SPE
Allopathic & Osteopathic Physicians
Colon & Rectal Surgery
207N00000X
SPE
Allopathic & Osteopathic Physicians
Dermatology
207P00000X
SPE
Allopathic & Osteopathic Physicians
Emergency Medicine
207PE0004X
SPE
Allopathic & Osteopathic Physicians
Emergency Medicine
207PT0002X
SPE
Allopathic & Osteopathic Physicians
Emergency Medicine
207Q00000X
PCP
Allopathic & Osteopathic Physicians
Family Medicine
207QS0010X
SPE
Allopathic & Osteopathic Physicians
Family Medicine
Sports Medicine
207QA0000X
PCP
Allopathic & Osteopathic Physicians
Family Medicine
Adolescent Medicine
207QA0505X
PCP
Allopathic & Osteopathic Physicians
Family Medicine
Adult Medicine
208D00000X
PCP
Allopathic & Osteopathic Physicians
Family Medicine
General Practice
208M00000X
SPE
Allopathic & Osteopathic Physicians
Hospitalist
207R00000X
PCP
Allopathic & Osteopathic Physicians
Internal Medicine
207RR0500X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Rheumatology
207RC0000X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
207RX0202X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Cardiovascular
Disease
Medical Oncology
207RG0100X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Gastroenterology
207RE0101X
PCP
Allopathic & Osteopathic Physicians
Internal Medicine
Endocrinology
207RH0003X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
207RI0200X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Hematology &
Oncology
Infectious Disease
207RH0000X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Hematology
ATTACHMENT A – PAGE 5 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Emergency Medical
Services
Medical Toxicology
Taxonomy
PCP/SPE
Type
Classification
Specialization
207RP1001X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Pulmonary Disease
207RN0300X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Nephrology
207RI0011X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
207RC0200X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
Interventional
Cardiology
Critical Care Medicine
207RC0001X
SPE
Allopathic & Osteopathic Physicians
Internal Medicine
207RG0300X
PCP
Allopathic & Osteopathic Physicians
Internal Medicine
207RH0002X
PCP
Allopathic & Osteopathic Physicians
Internal Medicine
207SG0201X
SPE
Allopathic & Osteopathic Physicians
Medical Genetics
207T00000X
SPE
Allopathic & Osteopathic Physicians
Neurological Surgery
207V00000X
PCP
Allopathic & Osteopathic Physicians
207VM0101X
SPE
Allopathic & Osteopathic Physicians
207VX0201X
SPE
Allopathic & Osteopathic Physicians
207W00000X
SPE
Allopathic & Osteopathic Physicians
Obstetrics &
Gynecology
Obstetrics &
Gynecology
Obstetrics &
Gynecology
Ophthalmology
207X00000X
SPE
Allopathic & Osteopathic Physicians
Orthopedic Surgery
207XS0106X
SPE
Allopathic & Osteopathic Physicians
Orthopedic Surgery
Hand Surgery
207XX0005X
SPE
Allopathic & Osteopathic Physicians
Orthopedic Surgery
Sports Medicine
207Y00000X
SPE
Allopathic & Osteopathic Physicians
Otolaryngology
207ZP0105X
SPE
Allopathic & Osteopathic Physicians
Pathology
207ZP0102X
SPE
Allopathic & Osteopathic Physicians
Pathology
207ZN0500X
SPE
Allopathic & Osteopathic Physicians
Pathology
Clinical
Pathology/Laboratory
Medicine
Anatomic Pathology &
Clinical Pathology
Neuropathology
207ZH0000X
SPE
Allopathic & Osteopathic Physicians
Pathology
Hematology
207ZB0001X
SPE
Allopathic & Osteopathic Physicians
Pathology
208000000X
PCP
Blood Banking &
Transfusion Medicine
Allopathic & Osteopathic Physicians
Pediatrics
2080P0205X
PCP
Allopathic & Osteopathic Physicians
Pediatrics
2080P0207X
SPE
Allopathic & Osteopathic Physicians
Pediatrics
2080P0006X
SPE
Allopathic & Osteopathic Physicians
Pediatrics
2080P0202X
SPE
Allopathic & Osteopathic Physicians
Pediatrics
2080N0001X
SPE
Allopathic & Osteopathic Physicians
Pediatrics
2080P0203X
SPE
Allopathic & Osteopathic Physicians
Pediatrics
208100000X
SPE
Allopathic & Osteopathic Physicians
Physical Medicine &
Rehabilitation
ATTACHMENT A – PAGE 6 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Clinical Cardiac
Electrophysiology
Geriatric Medicine
Hospice and Palliative
Medicine
Clinical Genetics
(M.D.)
Maternal & Fetal
Medicine
Gynecologic Oncology
Pediatric
Endocrinology
Pediatric HematologyOncology
Developmental –
Behavioral Pediatrics
Pediatric Cardiology
Neonatal-Perinatal
Medicine
Pediatric Critical Care
Medicine
Taxonomy
PCP/SPE
Type
Classification
Physical Medicine &
Rehabilitation
Physical Medicine &
Rehabilitation
Specialization
2081P0004X
SPE
Allopathic & Osteopathic Physicians
Spinal Cord Injury
Medicine
Pediatric
Rehabilitation
Medicine
Pain Medicine
2081P0010X
SPE
Allopathic & Osteopathic Physicians
2081P2900X
SPE
Allopathic & Osteopathic Physicians
2083X0100X
SPE
Allopathic & Osteopathic Physicians
Physical Medicine &
Rehabilitation
Preventive Medicine
2083P0901X
SPE
Allopathic & Osteopathic Physicians
Preventive Medicine
2083P0500X
SPE
Allopathic & Osteopathic Physicians
Preventive Medicine
2084N0400X
SPE
Allopathic & Osteopathic Physicians
Psychiatry & Neurology
Occupational
Medicine
Public Health &
General Preventive
Medicine
Preventive Medicine/
Occupational
Environmental
Medicine
Neurology
2084P0800X
SPE
Allopathic & Osteopathic Physicians
Psychiatry & Neurology
Psychiatry
2084A0401X
SPE
Allopathic & Osteopathic Physicians
Psychiatry & Neurology
Addiction Medicine
2085R0001X
SPE
Allopathic & Osteopathic Physicians
Radiology
Radiation Oncology
2085R0202X
SPE
Allopathic & Osteopathic Physicians
Radiology
Diagnostic Radiology
2085R0203X
SPE
Allopathic & Osteopathic Physicians
Radiology
Therapeutic Radiology
2085R0204X
SPE
Allopathic & Osteopathic Physicians
Radiology
Vascular &
Interventional
Radiology
208600000X
SPE
Allopathic & Osteopathic Physicians
Surgery
2086S0122X
SPE
Allopathic & Osteopathic Physicians
Surgery
2086S0129X
SPE
Allopathic & Osteopathic Physicians
Surgery
Plastic and
Reconstructive
Surgery
Vascular Surgery
2086S0127X
SPE
Allopathic & Osteopathic Physicians
Surgery
Trauma Surgery
208G00000X
SPE
Allopathic & Osteopathic Physicians
208800000X
SPE
Allopathic & Osteopathic Physicians
Thoracic Surgery
(Cardiothoracic
Vascular Surgery)
Urology
261Q00000X
PCP
Ambulatory Health Care Facilities
Clinic/Center
101YM0800X
SPE
Counselor
103T00000X
SPE
1041C0700X
SPE
104100000X
SPE
111N00000X
SPE
Behavioral Health & Social Service
Providers
Behavioral Health & Social Service
Providers
Behavioral Health & Social Service
Providers
Behavioral Health & Social Service
Providers
Chiropractic Providers
111NI0013X
SPE
Chiropractic Providers
Chiropractor
Mental Health
Psychologist
Social Worker
Clinical
Social Worker
Chiropractor
ATTACHMENT A – PAGE 7 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Independent Medical
Examiner
Taxonomy
PCP/SPE
Type
Classification
Specialization
133V00000X
SPE
Dietary and Nutritional Service Providers
Dietitian, Registered
152W00000X
SPE
Eye and Vision Services Providers
Optometrist
291U00000X
SPE
Laboratories
176B00000X
PCP
Other Service Providers
Clinical Medical
Laboratory
Midwife
174400000X
SPE
Other Service Providers
Specialist
367A00000X
PCP
367H00000X
SPE
364SM0705X
PCP
Advanced Practice
Midwife
Anesthesiologist
Assistant
Clinical Nurse Specialist
Medical-Surgical
364SP0809X
SPE
Clinical Nurse Specialist
Psych/Mental Health
364S00000X
PCP
364SA2200X
PCP
364SP0807X
SPE
364SP0808X
SPE
364SN0000X
SPE
367500000X
SPE
363LF0000X
PCP
363LP0200X
PCP
363L00000X
PCP
363LA2200X
PCP
363LW0102X
PCP
363LG0600X
PCP
363LP0808X
SPE
363LX0001X
PCP
363LN0005X
SPE
363LN0000X
SPE
363A00000X
PCP
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Clinical Nurse Specialist
Clinical Nurse Specialist
Adult Health
Clinical Nurse Specialist
Clinical Nurse Specialist
Psych/Mental Health,
Child & Adolescent
Psych/Mental Health
Clinical Nurse Specialist
Neonatal
Nurse Anesthetist
Certified Registered
Nurse Practitioner
Family
Nurse Practitioner
Pediatrics
Nurse Practitioner
Nurse Practitioner
Adult Health
Nurse Practitioner
Women's Health
Nurse Practitioner
Gerontology
Nurse Practitioner
Psych/Mental Health
Nurse Practitioner
Nurse Practitioner
Obstetrics &
Gynecology
Neonatal Critical Care
Nurse Practitioner
Neonatal
Physician Assistant
ATTACHMENT A – PAGE 8 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Taxonomy
PCP/SPE
363AM0700X
PCP
363AS0400X
SPE
363LP0222X
SPE
363LP2300X
PCP
213E00000X
SPE
213ES0103X
SPE
213ES0131X
SPE
225100000X
SPE
390200000X
PCP
333600000X
SPE
Type
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Physician Assistants & Advanced Practice
Nursing Providers
Podiatric Medicine & Surgery Service
Providers
Podiatric Medicine & Surgery Service
Providers
Podiatric Medicine & Surgery Service
Providers
Rehabilitative & Restorative Service
Providers
Student in an Organized Health Care
Training Program
Suppliers
Classification
Specialization
Physician Assistant
Medical
Physician Assistant
Surgical
Nurse Practitioner
Pediatrics, Critical
Care
Primary Care
Nurse Practitioner
Podiatrist
Podiatrist
Foot & Ankle Surgery
Podiatrist
Foot Surgery
Developmental
Physical Therapist
Pharmacy
Services included in the Total Cost of Care: This document further describes the
STATE’s method of measuring Total Cost of Care.
Core Services. Categories of service included in Total Cost of Care are:
(1) Physician services;
(2) Nurse midwife;
(3) Nurse practitioner;
(4) Child & Teen Check-up (EPSDT);
(5) Public health nurse;
(6) Rural health clinic;
(7) Federally qualified health center;
(8) Laboratory;
(9) Radiology;
(10) Chiropractic;
(11) Pharmacy;
(12) Vision;
(13) Podiatry;
(14) Physical therapy;
(15) Speech therapy;
(16) Occupational therapy;
(17) Audiology;
(18) Mental health;
(19) Chemical dependency;
(20) Outpatient hospital;
(21) Ambulatory surgical center;
(22) Inpatient hospital;
(23) Anesthesia;
(24) Hospice;
(25) Home health (excluding personal
care assistant services); and
(26) Private duty nursing.
ATTACHMENT A – PAGE 9 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Procedure/Revenue Codes. Procedure/revenue codes used by the STATE in calculating
Total Cost of Care include (see next pages):
Category of Service
Procedure/Revenue Codes
0001T, 0002T, 0003T, 0005T, 0006T, 0007T, 0008T, 0009T, 0012T, 0013T, 0014T,
0016T, 0017T, 0018T, 0019T, 0020T, 0021T, 0024T, 0025T,0054T, 0055T, 0056T,
056
0057T, 0060T, 0061T, 0092T 0095T, 0098T, 0099T, 0123T, 0124T, 0137T, 0155TAmbulatory Surgery 0158T, 0160T-0173T, 0176T-0177T, 0190T –0192T, 01968-01969, 10000-69999,
90870, 91010, 91033, 92018-92019, 93510, 93526, 93542-93545, 93555-93556,
93600, 93602, 93603, 93610,93612, 93615, 93616, 93618, 93631, 93650-93652,
95900, 95903, 95904, 95992, 96530, 96570-96571, C9716, C9724-C9728, D0120,
D0140, D0150, D0160, D0180, D0210-D0350, D0416-D0418, D0421, D0431,
D0460, D0470-D0471, D0475-D0479, D0481-D0485, D1110, D1120, D1201,
D1203- D1205, D1351, D2110, D2120, D2130-D2131, D2140, D2150, D2160D2161, D2210, D2330-D2332, D2335-D2337, D2380-D2382, D2385-D2388,
D2390-D2394, D2710, D2712, D2750-D2752, D2780-D2783, D2790, D2794,
D2910, D2915, D2920, D2930-D2934, D2940, D2950-D2952, D2954- D2955,
D2960, D2970-D2971, D2975, D2980, D2999, D3211, D3220, D3222, D3230,
D3240, D3310, D3320, D3330, D3346-D3348, D3351-D3353, D3410, D3421,
D3425-D3426, D3430, D3470, D3920, D3950, D3999, D4210-D4211, D4220,
D4240-D4241, D4245, D4260-D4261, D4265, D4271, D4273, D4275-D4276,
D4321, D4341-D4342, D4355, D4381, D4910, D4999, D5850-D5851, D5955,
D5982, D5986, D5991, D6053-D6054, D6094, D6190, D6194, D6205, D6214,
D6240-D6242, D6253, D6624, D6634, D6710, D6750-D6752, D6794, D6930,
D6972-D6973, D6975, D6980, D6999, D7110-D7111, D7120, D7130, D7140,
D7210, D7220, D7230, D7240-D7241, D7250, D7260-D7261, D7270, D7280D7283, D7285-D7286, D7288, D7310-D7311, D7321, D7411-D7415, D7472D7473, D7485, D7510-D7511, D7520-D7521, D7671, D7771, D7880, D7953,
D7963, D7972, D7999, D9110, D9420, D9910, G0104, G0105, G0121, G0127,
G0186, G0242-G0243, G0247, G0259, G0260, G0268, G0269, G0289, G0338G0340, G0364, G0392-G0393, M0050-M0054, Q1001-Q1005, Q3014, S0390,
S0630, S0800, S0810, S0812, S2050-S2055, S2060-S2061, S2065, S2070, S2080,
S2102-S2103, S2109, S2112, S2115, S2120, S2130, S2140, S2142, S2150, S2180,
S2190, S2202, S2204-S2211, S2213, S2220, S2230, S2235, S2250, S2255, S2260,
S2300, S2340-S2342, S2344, S2350-S2351, S2360-S2361, S2370-S2371, S2400S2405, S2409, S2411, S3902, S3904, S3906, S4011, S4013-S4018, S4020-S4023,
S4025-S4028, S4030-S4031, S4035, S4037, S4981, S5022, S8001, S8030, S9015,
S9025, S9034, S9088, S9527-S9528, X5301, V2630-V2632, V2790
ATTACHMENT A – PAGE 10 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Other Criteria
Bill Type is 83X
Category of Service
Procedure/Revenue Codes
041 Anesthesia:
Other Criteria
Proc Code Modifiers:
47, AA, AB, AC, AD, AE
(ends 12/31/2004), QK,
QO, QS, QX, QZ, Z2, Z3,
Z4
or
Proc Code Modifier: QH
or QI, (effective from
01/01/91 thru
02/28/1991)
or
Proc Code Modifier: QJ
(ends 12/31/2002)
or
Proc Code Modifier: QL
(ends 12/31/1998)
or
Proc Code Modifier: QQ
(begins 12/31/2000)
or
Proc Code Modifier: QY
(ends 12/31/1997)
058
Audiology
0208T – 0212T, 92550-92596, 92597 (ends 04/30/2004), 92598-92599, 9262092621, 92625, 92633, 92700 (w/o modifier GN, begins 05/01/2004), S0618,
S9476, X4611-X4612, X6000-X6001
470-0472, 479
044
T1016, T1017 (with no modifier or modifier NOT EQUAL TO HE, U3), T2022,
T2023 (w/modifier NOT HE or U3), T2041 (Begins 10/01/2004), X5401, X5424Case Management - X5425, X5455-X5456, X5476-X5477, X5491, X5566-X5567
Other
ATTACHMENT A – PAGE 11 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Category of Service
Procedure/Revenue Codes
Other Criteria
(99344 OR 97602 OR 98967 OR T1016 AND Pay To Provider Number =
017195000)
062
H0005, H0020, H2035, H2036, H0049, H0050, X0690, X5627
Chemical
Dependency
H0001, H0003, H0005-H0016, H0021-H0022, H0026-H0029, H2034, H2036,
H0043-H0044, H0047-H0050, H2001, S9475, T1006-T1012, X0690, X5627
040
Primary Diag: : 303305.03, 305.2-305.92
Submitter ID: 650015300
(CCDTF) and Claim Type
"O"
Outpatient/Rehabilitatio
n
X5324, X5622
Child and Teen
Checkup
039
X5340, X5623
Child and Teen
Checkup Outreach
057
Not Applicable
Chiropractic
118
S9129 (w/modifier UC), X5429
Extended
Occupational
Therapy
121
S9131 (w/modifier UC), X5426, X5453, X5468, X5579-X5580
Extended Physical
Therapy
122
Extended Private
S9124, T1002 (w/modifier UC), T1003 (w/modifier UC), X5266-X5267, X5433X5441, X5465-X5466, X5577-X5578
ATTACHMENT A – PAGE 12 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Prov Type is 37
(Chiropractor)
Category of Service
Procedure/Revenue Codes
Other Criteria
Duty Nursing
124
S5181 (w/modifier UC), X5430
Extended
Respiratory Therapy
125
S9128 (w/modifier UC), X5427
Extended Speech
Therapy
082
00510, 00512, 00521, 00522, 00524, 00525, 00527, 00528, 00780, 00900
Bill Type 731 or 737
Fed Qualified Health Ended 07/15/2009
Cntr Svc
020
Home Health
Services
9503-99512, 99539, 99551-99569, 99600-99602, G0151-G0153, G0154 (IF Maj
Prog NOT AC), G0155, G0156 (IF Wvr Type NOT F, G, H, I, J, K, L, M, P, Q, R, or S)
G0157- G0164, S0270 – S0274, S5180-S5181, S9035, S9061, S9097-S9098,
S9122, S9126-S9129, S9131, S9200, S9208-S9214, S9220, S9225, S9230, S9300,
S9308, S9310, S9335, S9339-S9343, S9370, S9372, S9395, S9420, S9423, S9425,
S9524, S9526, S9529, S9533, S9535, S9537-S9539, S9542-S9543, S9545-S9546,
S9550, S9555, S9558-S9560, S9562, S9590, S9800, S9802-S9803, S9810, T1004
(IF Wvr Type NOT F, G, H, I, J, K, L, M, P, Q, R, or S), T1021-T1022, T1030-T1031,
X4015, X5208-X5285, X5327, X5660-X5661
Not Applicable
072
Bill Type 32X-34X
Q5001-Q5010, X5210-X5228
Hospice
001
Not Applicable
Bill Type 81X or 82X
Not Applicable
Bill Type is 11X and Prov
COS is Inpatient Hospital,
Inpatient Hospital
ATTACHMENT A – PAGE 13 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Category of Service
Procedure/Revenue Codes
General
073
Other Criteria
General
Not Applicable
Inpatient Hosp Neonatal ICU
Bill Type is 11X
and
Prov COS is Inpatient,
Neonatal, ICU
and
Source of admission is "4
or “A”
and
Type of Admission is not
"4"
and
DRG equals 386 – 390 or
482 or 541 or 542
and
Recipient age < 1
OR
Effective 01/01/07
Bill Type is 11X
and
Prov COS is Inpatient,
Neonatal, ICU
And
Recip date of birth= date
of admission
And
One of the diagnosis
codes = V30.1 or V31.1
or V32.1 or V33.1 or
ATTACHMENT A – PAGE 14 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Category of Service
Procedure/Revenue Codes
Other Criteria
V34.1 or V35.1 or V36.1
or V37.1
And
One of the revenue
codes = 0174
OR
Effective 11/01/08
Bill Type is 11X
and
Prov COS is Inpatient,
Neonatal, ICU
and
Source of admission is
"6"
and
Type of Admission is "4"
and
DRG equals 386 – 390 or
482 or 541 or 542
and
Principal diagnosis code
= V30.1 or V31.1 or
V32.1 or V33.1 or V34.1
or V35.1 or V36.1 or
V37.1 or V39.1
and
Recipient age < 1
006
Not Applicable
Inpatient Hosp
ATTACHMENT A – PAGE 15 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Bill Type is 11X
And
Category of Service
Procedure/Revenue Codes
Rehabilitation
080
Laboratory
Other Criteria
Prov COS is Inpatient
Rehabilitation
0010T, 0023T, 0026T, 0030T, 0043T, 0058T, 0059T, 0085T, 0087T, 36415-36416,
80000-89999, 99000-99001, 99195, A9220, C1010-C1018, C1020- C1022, G0001,
G0026-G0027, G0050-G0060, G0103 (begins 07/01/2001), G0107 (begins
07/01/2001), G0123-G0124, G0141, G0143-G0145, G0147,
G0148, G0265-G0266, G0306-G0307, G0328, G0416 – G0419, G0430 –G0435,
G9143, P2031, P3000-P3001, P7001, P7020, P9010-P9024, P9031P9040, P9044, P9051-P9060, P9600, P9603-P9615, Q0048, Q0060-Q0061,
Q0063, Q0091, Q0095-Q0102, Q0111-Q0116, Q0126, Q2022, S3600- S3601,
S3618, S3620, S3625 – S3626, S3628, S3630, S3645, S3650, S3652, S3655,
S3700-S3701, S3708, S3711, S3717, S3800, S3818-S3820, S3822-S3823, S3828S3831, S3833-S3835, S3837, S3840-S3853, S3855, S3860 – S3862, S3865 –
S3866, S3870, S3890, S4036, S4040, X5328, Y8000, Y8020-Y9001
046
Mental Health
090
90785, 90791, 90792, 90801 – 90815, 90875-90876, 90816 – 90829, 90832 90847, 90862 - 90865, M0064, 90885 - 90889, S9484, , 90846 - 90847,
99354,90849, 90853, 90857, S9484 UA, S9484 UA HN
Not Applicable
ProvType is 66 (Nurse
Midwife)
Not Applicable
ProvType is 65 (Nurse
Practitioner)
Nurse Midwife
Services
091
Nurse Practitioner
Services
054
Occupational
Therapy
29065 (w/modifier GO, begins 05/01/2004), 29075 (w/modifier GO, begins
05/01/2004), 29085-29086 (w/modifier GO, begins 05/01/2004), 29105
(w/modifier GO, begins 05/01/2004), 29125-29126 (w/modifier GO, begins
05/01/2004), 29130-29131 (w/modifier GO, begins 05/01/2004), 29200
(w/modifier GO, begins 05/01/2004), 29220 (w/modifier GO, begins
05/01/2004), 29240 (w/modifier GO, begins 05/01/2004), 29060 (w/modifier
ATTACHMENT A – PAGE 16 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Category of Service
Procedure/Revenue Codes
GO, begins 05/01/2004), 29080 (w/modifier GO, begins 05/01/2004), 29345
(w/modifier GO, begins 05/01/2004), 29355 (w/modifier GO, begins
05/01/2004), 29365 (w/modifier GO, begins 05/01/2004), 29405 (w/modifier
GO, begins 05/01/2004), 29425 (w/modifier GO, begins 05/01/2004), 29445
(w/modifier GO, begins 05/01/2004), 29505 (w/modifier GO, begins
05/01/2004), 29515 (w/modifier GO, begins 05/01/2004), 29520 (w/modifier
GO, begins 05/01/2004), 29530 (w/modifier GO, begins 05/01/2004), 29540
(w/modifier GO, begins 05/01/2004), 29550 (w/modifier GO, begins
05/01/2004), 29580 (w/modifier GO, begins 05/01/2004), 29581 (w/modifier
GO), 29590 (w/modifier GO, begins 05/01/2004), 90901(ends 04/30/2004),
90901 (w/modifier GO, begins 05/01/2004), 90911 (w/modifier GO), 92526
(w/modifier GO), 92610 (w/modifier GO, begins 05/01/2004), 92611
(w/modifier GO, begins 05/01/2004), 92626 – 92627 (w/modifier ‘GO’), 92630
(w/modifier ‘GO’) 92633 (w/modifier ‘GO’), 95831 (w/modifier GO, begins
05/01/2004), 95832 (w/modifier GO, begins 05/01/2004), 95833 (w/modifier
GO, begins 05/01/2004), 95834 (w/modifier GO, begins 05/01/2004), 95851
(w/modifier GO, begins 05/01/2004), 95852 (w/modifier GO, begins
05/01/2004), 96110 (with modifier GO, begins 01/01/2010), 96111 (with
modifier GO, begins 01/01/2010), 96125, 97003-97004, 97010 (ends
04/30/2004), 97010 (w/modifier GO, begins 05/01/2004), 97012-97013 (ends
04/30/2004), 97012-97013 (w/modifier GO, begins 05/01/2004), 97016 (ends
04/30/2004), 97016 (w/modifier GO, begins 05/01/2004), 97018 (ends
04/30/2004), 97018 (w/modifier GO, begins 05/01/2004), 97020 (ends
04/30/2004), 97020 (w/modifier GO, begins 05/01/2004), 97022 (ends
04/30/2004), 97022 (w/modifier GO, begins 05/01/2004), 97024 (ends
04/30/2004), 97024 (w/modifier GO, begins 05/01/2004), 97026 (ends
04/30/2004), 97026 (w/modifier GO, begins 05/01/2004), 97028 (ends
04/30/2004), 97028 (w/modifier GO, begins 05/01/2004), 97032 (ends
04/30/2004), 97032 (w/modifier GO, begins 05/01/2004), 97033 (ends
04/30/2004), 97033 (w/modifier GO, begins 05/01/2004), 97034 (ends
04/30/2004), 97034 (w/modifier GO, begins 05/01/2004), 97035 (ends
04/30/2004), 97035 (w/modifier GO, begins 05/01/2004), 97036 (ends
04/30/2004), 97036 (w/modifier GO, begins 05/01/2004), 97039 (w/modifier
GO, begins 05/01/2004), 97110 (ends 04/30/2004), 97110 (w/modifier GO,
begins 05/01/2004), 97112-97113 (ends 04/30/2004), 97112-97113 (w/modifier
GO, begins 05/01/2004), 97116 (ends 04/30/2004), 97116 (w/modifier GO,
begins 05/01/2004), 97124 (ends 04/30/2004), 97124 (w/modifier GO, begins
05/01/2004), 97139 (w/modifier GO, begins 05/01/2004), 97140(ends
04/30/2004), 97140 (w/modifier GO, begins 05/01/2004), 97150 (w/modifier
GO, begins 05/01/2004), 97504 (ends 04/30/2004), 97504 (w/modifier GO,
begins 05/01/2004), 97520 (ends 04/30/2004), 97520 (w/modifier GO, begins
05/01/2004), 97530 (ends 04/30/2004), 97530 (w/modifier GO, begins
05/01/2004), 97532-97533, 97535, 97537, 97540-97541, 97542 (ends
04/30/2004), 97542 (w/modifier GO, begins 05/01/2004), 97545-97546
ATTACHMENT A – PAGE 17 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Other Criteria
Category of Service
Procedure/Revenue Codes
Other Criteria
(w/modifier GO, begins 05/01/2004), 97597-97598 (w/modifier GO) 9760597606 (w/modifer GO) 97703(ends 04/30/2004), 97703 (w/modifier GO, begins
05/01/2004), 97755 (modifier EQUAL TO ‘GO’), 97760 (w/modifier ‘GO’), 97761
(w/modifier ‘GO’), 97762 (w/modifier ‘GO’97750 (w/modifier GO, begins
05/01/2004), 97770, 97799 (w/modifier GO, begins 05/01/2004), G0129, G0281
(modifier = ‘GO’), G0282 (modifier =‘GO’), G0283 (modifier = ‘GO’), H5300,
H5510, H5511, Q0082, Q0109-Q0110, Q4017-Q4024 (w/modifier GO, begins
05/01/2004), Q4041-Q4049 (w/modifier GO, begins 05/01/2004), Q4051
(w/modifier GO, begins 05/01/2004), X4510-X4513, X4515-X4520, X4522-X4526,
X5510-X5511, X6004- X6005
Procedure codes associated with CMS-1500 claim form
or 430-434, 439
007
Not Applicable
Bill Type is 13X or 14X
Outpatient Hospital Or
Services
762
Not Applicable
X5350
Bill Type is 730, 732-739
Bill Type is 731
Or 519
030
Not Applicable
Pharmacy Services
051
29065 (w/modifier GP, begins 05/01/2004), 29075 (w/modifier GP, begins
05/01/2004), 29085-29086 (w/modifier GP, begins 05/01/2004), 29105
Physical Therapy (w/modifier GP, begins 05/01/2004), 29125-29126 (w/modifier GP, begins
05/01/2004), 29130-29131 (w/modifier GP, begins 05/01/2004), 29200
(w/modifier GP, begins 05/01/2004), 29220 (w/modifier GP, begins
05/01/2004), 29240 (w/modifier GP, begins 05/01/2004), 29060 (w/modifier
GP, begins 05/01/2004), 29080 (w/modifier GP, begins 05/01/2004), 29345
(w/modifier GP, begins 05/01/2004), 29355 (w/modifier GP, begins
05/01/2004), 29365 (w/modifier GP, begins 05/01/2004), 29405 (w/modifier
GP, begins 05/01/2004), 29425 (w/modifier GP, begins 05/01/2004), 29445
(w/modifier GP, begins 05/01/2004), 29505 (w/modifier GP, begins
ATTACHMENT A – PAGE 18 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Claim Type P
Category of Service
Procedure/Revenue Codes
05/01/2004), 29515 (w/modifier GP, begins 05/01/2004), 29520 (w/modifier
GP, begins 05/01/2004), 29530 (w/modifier GP, begins 05/01/2004), 29540
(w/modifier GP, begins 05/01/2004), 29550 (w/modifier GP, begins
05/01/2004), 29580 (w/modifier GP, begins 05/01/2004),29581 (w/modifier
GP), 29590 (w/modifier GP, begins 05/01/2004), 90900, 90901(ends
04/30/2004), 90901 (w/o modifier GO, begins 05/01/2004), 90911 (w/modifier
GP), 95831 (ends 04/30/2004), 95831 (w/o modifier GO, begins 05/01/2004),
95832 (ends 04/30/2004), 95832 (w/o modifier GO, begins 05/01/2004), 95833
(ends 04/30/2004), 95833 (w/o modifier GO, begins 05/01/2004), 95834 (ends
04/30/2004), 95834 (w/o modifier GO, begins 05/01/2004), 95835-95850,
95851 (ends 04/30/2004), 95851 (w/o modifier GO, begins 05/01/2004), 95852
(ends 04/30/2004), 95852 (w/o modifier GO, begins 05/01/2004), 96110 (with
modifier GP, begins 01/01/2010), 96111 (with modifier GP, begins 01/01/2010),
1097000-97002, 97005-97006, 97010 (ends 04/30/2004), 97010 (w/o modifier
GO, begins 05/01/2004), 97011, 97012-97013 (ends 04/30/2004), 97012-97013
(w/o modifier GO, begins 05/01/2004), 97014-97015, 97016 (ends 04/30/2004),
97016 (w/o modifier GO, begins 05/01/2004), 97017,97018 (ends 04/30/2004),
97018 (w/o modifier GO, begins 05/01/2004), 97019, 97020 (ends 04/30/2004),
97020 (w/o modifier GO, begins 05/01/2004),97021, 97022 (ends 04/30/2004),
97022 (w/o modifier GO, begins 05/01/2004), 97023, 97024 (ends 04/30/2004),
97024 (w/o modifier GO, begins05/01/2004), 97025, 97026 (ends 04/30/2004),
97026 (w/o modifier GO, begins 05/01/2004), 97027, 97028 (ends 04/30/2004),
97028 (w/o modifier GO, begins 05/01/2004), 97029-97031, 97032 (ends
04/30/2004), 97032 (w/o modifier GO, begins 05/01/2004), 97033 (ends
04/30/2004), 97033 (w/o modifier GO, begins 05/01/2004), 97034 (ends
04/30/2004), 97034 (w/o modifier GO, begins 05/01/2004), 97035 (ends
04/30/2004), 97035 (w/o modifier GO, begins 05/01/2004), 97036 (ends
04/30/2004), 97036 (w/o modifier GO, begins 05/01/2004), 97037-97038,
97039 (ends 04/30/2004),97039 (w/o modifier GO, begins 05/01/2004), 97110
(ends 04/30/2004), 97110 (w/o modifier GO, begins 05/01/2004), 97111, 9711297113 (ends 04/30/2004), 97112-97113 (w/o modifier GO, begins 05/01/2004),
97114-97115, 97116 (ends 04/30/2004), 97116 (w/o modifier GO, begins
05/01/2004), 97117-97123, 97124 (ends 04/30/2004), 97124 (w/o modifier GO,
begins 05/01/2004), 97125-97138, 97139 (ends 04/30/2004), 97139 (w/o
modifier GO, begins 05/01/2004), 97140(ends 04/30/2004), 97140 (w/o
modifier GO, begins 05/01/2004), 97141-97145, 97150 (ends 04/30/2004),
97150 (w/o modifier GO, begins 05/01/2004), 97200-97241, 97250, 9726097261, 97265, 97500-97503, 97504 (ends 04/30/2004), 97504 (w/o modifier
GO, begins 05/01/2004), 97505-97519, 97520 (ends 04/30/2004), 97520 (w/o
modifier GO, begins 05/01/2004), 97521-97529, 97530 (ends 04/30/2004),
97530 (w/o modifier GO, begins 05/01/2004), 97531, 97542 (ends 04/30/2004),
97542 (w/o modifier GO, begins 05/01/2004), 97545-97546 (ends 04/30/2004),
97545-97546 (w/o modifier GO, begins 05/01/2004), 97597-97598 (w/o
modifier GO) 97605-97606 (w/o modifier GO), 97700-97701, 97703(ends
ATTACHMENT A – PAGE 19 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Other Criteria
Category of Service
Procedure/Revenue Codes
04/30/2004), 97703 (w/o modifier GO, begins 05/01/2004), 97720-97721,
97750 (ends 04/30/2004), 97750 (w/o modifier GO, begins 05/01/2004), 97752,
97755 (modifier NOT EQUAL TO ‘GO’), 97760 (w/o modifier OR modifier NOT
EQUAL TO ‘GO’), 97761 (w/o modifier OR modifier NOT EQUAL TO ‘GO’), 97762
(w/o modifier OR modifier NOT EQUAL TO ‘GO’), 97799 (ends 04/30/2004),
97799 (w/o modifier GO, begins 05/01/2004), G0281 (modifier = ‘GP’), G0282
(modifier = ‘GP’), G0283 (modifier = ‘GP’), H5220-H5299, M0005-M0008, Q0086,
Q0103-Q0104, Q4017-Q4024 (w/modifier GP, begins 05/01/2004), Q4041Q4049 (w/modifier GP, begins 05/01/2004), Q4051 (w/modifier GP, begins
05/01/2004), S8940, S8945, S8948, S8990, S9033, X0715, X4521, X4600-X4601,
X5515-X5516, X6006-X6008
Procedure codes listed above
or 420-424, 429
043
Physician Services
0001F, 0001T, 0002F, 0002T, 0003F, 0003T, 0004F, 0005F, 0005T, 0006F, 0006T,
0007F, 0007T, 0008F, 0008T, 0009F, 0009T, 0010F, 0011F, 0012F,
0012T, 0013T, 0014F, 0014T, 0015F, 0016T, 0017T, 0018T, 0019T, 0020T, 0021T,
0024T, 0025T, 0027T, 0028T, 0029T, 0031T, 0032T, 0033T, 0034T, 0035T, 0036T,
0037T, 0038T, 0039T, 0040T, 0041T, 0042T, 0044T, 0045T, 0046T, 0047T, 0048T,
0049T, 0050T, 0051T, 0052T, 0053T, 0054T, 0055T, 0056T, 0057T, 0060T, 0061T,
0062T, 0063T, 0064T, 0065T, 0068T, 0069T, 0070T, 0073T, 0074T-0084T, 0086T,
0088T, 0115T-0117T, 0120T, 0123T - 0124T, 0126T, 0130T, 0133T, 0135T, 0137T,
0140T – 0143T, 0153T – 0154T, 0155T-0158T, 0160T-0173T, 0176T-0181T,
0184T-0186T, 0188T – 0192T – 0207T, 0213T – 0238T, 0243T – 0275T, 0500F0503F, 0509F, 0513F, 0514F, 0516F-0521F, 0525F, 0526F, 0528F–0529F, 0535F,
0540F, 0545F, 0575F, 1000F-1002F, 2000F, 4000F-4002F, 4006F, 4009F, 4011F,
7010F, 01967-01969, 01995-01996, 10000-29064, 29065 (ends 04/30/2004),
29065 (w/o modifier GO or GP, begins 05/01/2004), 29066-29074, 29075 (ends
04/30/2004), 29075 (w/o modifier GO or GP, begins 05/01/2004), 29076-29084,
29085-29086 (ends 04/30/2004), 29085-29086 (w/o modifier GO or GP, begins
05/01/2004), 29087-29104, 29105 (ends 04/30/2004), 29105 (w/o modifier GO
or GP, begins 05/01/2004), 29106-29124, 29125-29126 (ends 04/30/2004),
29125-29126 (w/o modifier GO or GP, begins 05/01/2004), 29127-29129,
29130-29131 (ends 04/30/2004), 29130-29131 (w/o modifier GO or GP, begins
05/01/2004), 29132-29199, 29200 (ends 04/30/2004), 29200 (w/o modifier GO
or GP, begins 05/01/2004), 29201-29219, 29220 (ends 04/30/2004), 29220 (w/o
modifier GO or GP, begins 05/01/2004), 29221-29239, 29240 (ends
04/30/2004), 29240 (w/o modifier GO or GP, begins 05/01/2004), 29241-29259,
29060 (ends 04/30/2004), 29060 (w/o modifier GO or GP, begins 05/01/2004),
29061-29079, 29080 (ends 04/30/2004), 29080 (w/o modifier GO or GP, begins
05/01/2004), 29081-29344, 29345 (ends 04/30/2004), 29345 (w/o modifier GO
or GP, begins 05/01/2004), 29346-29354, 29355 (ends 04/30/2004), 29355 (w/o
ATTACHMENT A – PAGE 20 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Other Criteria
Category of Service
Procedure/Revenue Codes
modifier GO or GP, begins 05/01/2004), 29356-29364, 29365 (ends
04/30/2004), 29365 (w/o modifier GO or GP, begins 05/01/2004), 29366-29404,
29405 (ends 04/30/2004), 29405 (w/o modifier GO or GP, begins 05/01/2004),
29406-29424, 29425 (ends 04/30/2004), 29425 (w/o modifier GO or GP, begins
05/01/2004), 29426-29444, 29445 (ends 04/30/2004), 29445 (w/o modifier GO
or GP, begins 05/01/2004), 29446-29504, 29505 (ends 04/30/2004), 29505 (w/o
modifier GO or GP, begins 05/01/2004), 29506-29514, 29515 (ends
04/30/2004), 29515 (w/o modifier GO or GP, begins 05/01/2004), 29516-29519,
29520 (ends 04/30/2004), 29520 (w/o modifier GO or GP, begins 05/01/2004),
29521-29529, 29530 (ends 04/30/2004), 29530 (w/o modifier GO or GP, begins
05/01/2004), 29531-29539, 29540 (ends 04/30/2004), 29540 (w/o modifier GO
or GP, begins 05/01/2004), 29541-29549, 29550 (ends 04/30/2004), 29550 (w/o
modifier GO or GP, begins 05/01/2004), 29551-29579, 29580 (ends
04/30/2004), 29580 (w/o modifier GO or GP, begins 05/01/2004), 29581
(without modifier GO or GP), 29582-29589, 29590 (ends 04/30/2004), 29590
(w/o modifier GO or GP, begins 05/01/2004), 29591-36410, 36420-69999,
90000-90699, 90700--90799, 90902-90910, 90911 (ends 04/30/2004), 90911
(w/o modifier GO or GP, begins 05/01/2004), 90918-90925, 90935-90950,
90971- 91299, 92500-92504, 92511-92520, 92531-92548, 92601-92604, 92611
(ends 04/30/2004), 92611 (w/o modifier GO or GN, begins 05/01/2004), 92612
(ends 04/30/2004), 92612 (w/o modifier GN, begins 05/01/2004), 92613, 92614
(ends 04/30/2004), 92614 (w/o modifier GN, begins 05/01/2004), 92615, 92616
(ends 04/30/2004), 92616 (w/o modifier GN, begins 05/01/2004), 92617, 92640,
92700 (ends 04/30/2004), 92950-93982, 93990, 94002-94005, 94010-94799,
94800-94899, 95000-95300, 95411,95800 – 95801, 95803, 95805-95830, 9585795882, 95900-95999, 96000-96004, 96020, 96040, 96110 (modifier NOT EQUAL
GN, GO, GP) 96111 (modifier NOT EQUAL GN GO GP), 96115, 96150-96155,
96360 – 96361, 96365 – 96376, 96379, 96400-96549, 96567, 96570-96571,
96900-96999, 97601-97602 (ends 04/30/2004), 97601-97602 (w/o modifier GO
or GP, begins 05/01/2004), 97780-97781, 97802-97804, 97810-97811, 9781397814, 98900-98929, 98960-98962, 98966-98969, 99002-99065, 99075-99091,
99100-99145, 99148-99192, 99199-99429, 99431-99444, 99450-99455, 99471 –
99472, 99475 - 99480, 99499, 99605-99607, 99990, A4260, A9150, A9152A9153, A9200, A9535, C8921-C8930, C8950-C8955, C8957 , C9019-C9020,
C9104-C9116, C9119-C9121, C9124-C9129, C9202-C9204, C9207- C9220, C9223C9230, C9232-C9235, C9237-C9240, C9245 – C9248, C9251 – C9267, C9270 –
C9284, C9399, C9410-C9433, C9435-C9440, C9704, C9712-C9721, C9724 –
C9731, C9800 – C9802, G0002-G0010, G0015-G0016, G0030-G0047, G0051G0053, G0062-G0066, G0101-G102, G0103 (ends 06/30/2001), GO104-G0106,
G0107 (ends 06/30/2001), G0108-G0116, G0121, G0125-G0128, G0159-G0161,
G0163-G0171, G0173-G0175, G0178-G0187, G0190-G0194, G0237-G0243,
G0245-G0251, G0255-G0261, G0263-G0264, G0267-G0275, G0278-G0280,
G0281 (modifier NOT EQUAL ‘GO’, ‘GP’), G0282 (modifier NOT EQUAL ‘GO’,
‘GP’), G0283 (modifier NOT EQUAL ‘GO’, ‘GP’), G0288-G0295, G0297-G0300,
ATTACHMENT A – PAGE 21 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Other Criteria
Category of Service
Procedure/Revenue Codes
G0302-G0305, G0308-G0327, G0329, G0332-G0333, G0337-G0351, G0353G0368, G0372, G0375 - G0377, G0392-G0393, G0396-G0400, G0402 – G0415,
G0420 – G0429, G0436 – G0441, G3001, G8006-G801, G8051-G8062, G8075G8080, G8093-G8094, G8099-G8100, G8103-G8104, G8106-G8117, G8126G8131, G8152-G8167, G8170-G8172, G8182-G8186, G8191-G8243, G8245G8347, G8351, G8354, G8357, G8360, G8362, G8365, G8367, G8370-G8386,
G8389-G8391, G8385-G8410, G8415-G8443, G8445-G8544, G8545 – G8553,
G8556 – G8693, G9001-G9012, G9016 -G9036, G9050-G9142, G9147, H0033,
H1000-H1005, H1010, J0100-J7020, J7040-J7042, J7050, J7052-J7130, J7140J7170, J7184-J7199, J7300, J7302-J7304, J7306 – J7312, J7315-J7317, J7319 J7325, J7330, J7335, J7340 - J7350, J7500-J7511, J7513, J7515-J7518, J7520,
J7525, J7599, J7602 – J7606-J7609, J7610-J7799, J8498-J8499, J8501, J8510,
J8515, J8520-J8521, J8530-J9999, K0119-K0125, K0140-K0146, K0166-K0167,
K0415-K0416, K0418, K0453, K0503-K0528, K0548, M0070, M0075, M0100M0101, M0300-M0585, M0592, M0702-M0799, M0910, M0945, M0974M0982, P9001, P9041-P9043, P9045-P9048, P9050, Q0019-Q0032, Q0034Q0035, Q0044, Q0059, Q0062, Q0066, Q0068, Q0081, Q0083-Q0085, Q0093Q0094, Q0108, Q0124-Q0132, Q0134, Q0136-Q0141, Q0144, Q0156-Q0185,
Q0187, Q0510-Q0515, Q1003, Q2001-Q2021, Q2023 - Q2027, Q2035- Q2044,
Q3013-Q3014, Q3021-Q3026, Q3030, Q4052-Q4055, Q4075-Q4077, Q4079,
Q4081-Q4092, Q4095 – Q4098, Q9920-Q9944, Q9955-Q9957, Q9968, S0009S0040, S0071-S0098, S0104, S0106-S0109, S0112, S0114- S0118, S0122, S0124,
S0126, S0128, S0130, S0132-S0133, S0135-S0141, S0145-S0148, S0156-S0167,
S0169 - S0183, S0187, S0189-S0191, S0193-S0199, S0206, S0220-S0221, S0250,
S0255, S0257, S0260, S2068, S0270-S0274, S0280 , S0281, S0302, S0310, S0315S0317, S0320, S0340-S0342, S0345-S0347, S0390, S0592, S0601-S0622, S0625,
S0630, S0800, S0810, S0812, S1025, S2050-S2055, S2060-S2061, S2065–S2067,
S2070, S2075-S2077- S2080, S2082-S2083, S2085, S2090-S2091, S2095, S2102S2103, S2107, S2109, S2112- S2115, S2117 – S2118, S2120, S2130-S2131, S2135,
S2140, S2142, S2150, S2152, S2180, S2190, S2202, S2204-S2211, S2213, S2215,
S2220, S2225, S2230, S2235, S2250, S2255, S2260, S2262, S2265-S2267, S2270,
S2300, S2325, S2340-S2342, S2344, S2348, S2350-S2351, S2360-S2363, S2370S2371, S2400-S2405, S2409, S2411, S2900, S3854, S3900, S3902, S3904 - S3906,
S4011, S4013-S4018, S4020-S4023, S4025-S4028, S4030-S4031, S4035, S4037,
S4042, S4981, S4989, S4993, S5000-S5001, S5022, S5550-S5553, S5565-S5566,
S5570-S5571, S8001, S8004, S8030, S9034, S8040, S8048-S8049, S8075, S8110
(begins 07/01/2001), S8301, S8950, S9015, S9023, S9025, S9055-S9056, S9075,
S9083, S9085, S9088, S9090, S9092, S9105, S9117, S9140-S9141, S9145, S9150,
S9381, S9401, S9430, S9436-S9439, S9441-S9445, S9447, S9449, S9451-S9455,
S9460, S9465, S9472-S9474, S9527-S9528, S9806, S9900, S9970, S9981-S9982,
S9986, S9988-S9991, T1013-T1014, T1016 (IF Maj Prog NOT AC AND Primary
Diag = 010-018.99, 795.5, or V01.1, V12.01, V74.1,), T1023-T1029, T1502, T1503,
T2042-T2047, T2050-T4520, T4544-T5000, T5002-T5998, T6000-T6515, V2630V2632, V2785, V2790, W0100-W9999, X0995, X1000-X1018, X1030-X1031,
ATTACHMENT A – PAGE 22 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Other Criteria
Category of Service
Procedure/Revenue Codes
Other Criteria
X1050-X1395, X1410, X1420, X1520, X1672, X2300, X2390-X2393, X2395-X2396,
X3100-X3102, X3120-X3121, X5355-X5356, X5493-X5501, X5509, X5659, X5698X5699, X9001, Y0069, Y9300- Y9324
J0001-J9999, 90281-90799, 95115-95180 (begins 08/01/2000)
055
Not Applicable
Podiatry
089
Private Duty Nursing
088
G0154 (IF Maj Prog = AC), S9216-S9218, T1000, T1002-T1003, X4020-X4021,
X4029, X4031, X4033, X4035, X5641-X5642, X5646-X5649, X5662-X5663
99500-99502, S5190, S9123, S9446, T1015, X4010, X5286-X5288, X5546-X5549
Public Health
Nursing
079
0066T, 0067T, 0071T, 0072T, 0082T, 0144T – 0152T, 0159T, 0174T-0175T, 0182T
– 0183T, 0187T, 0239T – 0242T, 70000-79999 (EXCEPT 7010F, which was moved
Radiology, Technical to Physician, ‘043’), C8900-C8914, C8918-C8920, C8931 – C8936, C9722-C9723,
Component
G0120, G0122, G0130-G0133, G0188, G0202-G0207, G0210-G0236, G0252G0254, G0262, G0296, G0330 – G0331, G0336, G0389, M0080, Q0064-Q0065,
Q0067, Q0069-Q0072, Q0076, Q0092, R0065, R0070-R0076, R6129, S0820,
S0830, S8035, S8037, S8042, S8055, S8080, S8085, S8092-S8093, S9022, S9024,
Y1000, Y7000-Y7603
ATTACHMENT A – PAGE 23 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Prov Tpe is 36
(Podiatrist)
Category of Service
083
Procedure/Revenue Codes
00521, 00522, 00524, 00525, 00527, 00528, 00529, 00780, 00900
Other Criteria
Bill Type is 71X
Rural Health Clinic or
Services
X5325-X5326
Ended 07/15/2009
053
Speech Therapy
078
92506-92508, 92510, 92525, 92526 (if modifier NOT EQUAL to ‘GO’), 92597
(begins 05/01/2004), 92605-92609, 92610 (ends 04/30/2004), 92610 (w/o
modifier GO, begins 05/01/2004), 92611 (w/modifier GN, begins 05/01/2004),
92612 (w/modifier GN, begins 05/01/2004), 92614 (w/modifier GN, begins
05/01/2004), 92616 (w/modifier GN, begins 05/01/2004), 92626 – 92627 (if
modifier NOT EQUAL to ‘GO’, 92630 (if modifier NOT EQUAL to ‘GO’), 92633 (if
modifier NOT EQUAL to ‘GO’), 96105, 96110 (with modifier GN, begins
01/01/2010), 96111 (with modifier GN, begins 01/01/2010), 92700 (w/modifier
GN, begins 05/01/2004), G0195-G0201, S9152, V5301-V5364, X4610, X4613X4614, X5517, X6002-X6003
0065T, 90000-90080, 99056, 99172, 99201-99205, 99211-99215, S0592, S0625
Vision
92000-92065, 92081-92287, 92499, G0117-G0118, G9041 – G9044, S3000
Att_A_Patient Attribution and Financial Settlement Information _ 031716
ATTACHMENT A – PAGE 24 OF 24
PATIENT ATTRIBUTION METHOD, PROVIDER TAXONOMY, AND SERVICES PROVIDED
Prov Type 35
Optometrist of 75
Optician
ATTACHMENT B-1: IHP-Specific Description, Governance, and
Financial Arrangement
1.1 Summary. This document further defines the IHP Entity, [name of IHP]’s Participants,
and certain other details about the IHP as referenced in the IHP Contract. It also details the
IHP’S amount of risk and the distribution of Shared Savings and Shared Losses between the
STATE (or MCO) and [IHP NAME] (IHP) during the demonstration, referenced in Section 2,
IHP Specific Settlement Information.
1.2 As defined in Article 1 (9) of the Contract, the IHP Entity is:
☐ Provider health system(s) whose clinics and/or hospitals are owned by or under
contract for the purposes of this demonstration.
☐ A separate legal entity.
[Insert description of the IHP from the RFP response here. IHP should edit for any changes
since the RFP response.]
1.3 As defined in Article 1 (10), the list of IHP Participants includes (as of DATE):
Name
Address
Specialty
MN Community Measurement ID
Number*
*If IHP Participant is a clinic.
1.4 As defined in Article 1 (11) of the Contract, the IHP Fiscal Agent is:
1.5 Description of the IHP’S Shared Governance System as required under section 2.2
of the Contract:
(A) The IHP’S Shared Governance System includes the following groups of providers
and suppliers as listed in Minnesota Statutes, 256B.0755, subd. 1 (d).
☐ Professionals in group practice arrangements;
ATTACHMENT B-1: PAGE 1
IHP-SPECIFIC GOVERNANCE
1 of 7
☐ Networks of individual practices of professionals;
☐ Partnerships or joint venture arrangements between hospitals and health care
professionals;
☐ Hospitals employing professionals; or
☐ Other groups of providers of services and suppliers.
(B) IHP contracts with a managed care plan or a county-based purchasing plan to
provide administrative services:
☐ Yes
☐ No
(C) List of Members of the IHP’S Governing Body
Name:
Title:
Expertise
Patient
Representative?
Y/N
Consumer
Advocate?
Y/N
Guaranteeing entity for this Contract to make a Final Payment of Shared Losses is:
1.6 Taxpayer Identification Number (TIN) of the IHP Fiscal Agent to receive any
Interim or Final Payments as required in section 2.6 of the Contract:
1.7 Insurance as required in section 2.9 of the Contract:
☐ The IHP has in force a commercial general liability policy with a minimum
amount of $2,000,000 per occurrence and $2,000,000 annual aggregate; or
☐ The IHP maintains a program of self-insurance.
1.8 The IHP’S authorized representative as required in section 6.2 of the Contract:
ATTACHMENT B-1: PAGE 2
IHP-SPECIFIC GOVERNANCE
2 of 7
2.1 IHP Financial Settlement Information. IHP performance will be measured against a
Total Cost of Care target, derived from the IHP’s historical performance and adjusted for
changes in population risk and expected trend. If the performance threshold in section 2.5 is
met, all Shared Savings or Shared Losses will be shared (i.e., first dollar) based upon the
agreed-upon distribution between DHS and IHP described in Section 3.1, subject to
reductions determined by Attachment B-2, Quality.
2.2 Definitions.
(A) Capitalized terms in this Attachment take the same meanings as in the Contract.
(B) “Base Period” means the period covering dates of service beginning January 1,
2016 and ending December 31, 2016.
(C) “Performance Period 1” means the period covering dates of service beginning
January 1, 2017 and ending December 31, 2017.
(D) “Performance Period 2” means the period covering dates of service beginning
January 1, 2018 and ending December 31, 2018.
(E) “Performance Period 3” means the period covering dates of service beginning
January 1, 2019 and ending December 31, 2019.
(F) “Caps” or “Cap” means thresholds to adjust the PMPM results for “catastrophic
cases” as follows:
(1) 1,000 to 1,999 Attributed Patients in the IHP = $50,000 maximum annual claims
per Patient; or
(2) 2,000 to 4,999 Attributed Patients in the IHP = $200,000 maximum annual
claims per Patient; or
(3) 5,000 or more Attributed Patients in the IHP = $200,000 maximum annual claims
per Patient.
2.3 Total Cost of Care (TCOC) Performance Assessment Process. Because the Attributed
Population will change from the Base Period to the Performance Period(s), the STATE will
adjust the Total Cost of Care target for changes in the Attributed Population and illness
burden (i.e., population risk score).
2.3.1 Base Period.
(A) Base Period Attributed Population: DHS will attribute patients to an IHP using
retrospective claims and MCO encounter data available to DHS consistent with
Attachment A, Patient Attribution Method, Provider Taxonomy, and Services Provided.
(B) Base Period Total Cost of Care (Base TCOC):
ATTACHMENT B-1: PAGE 3
IHP-SPECIFIC GOVERNANCE
3 of 7
(1) DHS will calculate the retrospective per patient per month (PMPM) TCOC for
the Base Period Attributed Population.
(2) The Base TCOC will be based on the core services outlined in Attachment A,
Section 4, Core Services. The services included in the TCOC may not change except
under a contract amendment.
(3) Claim costs for an Attributed Patient that fall outside of Caps in 2.2(F) above will
be capped to adjust the PMPM results for catastrophic cases.
(C) Base Period Risk Score:
(1) Based on the services included in the Base TCOC, a risk score will be developed
for the Attributed Population to reflect the relative risk of the population.
(2) DHS will use the ACG® risk adjustment tool and develop category-specific risk
weights based on the aggregate claims experience of the MHCP population who are
eligible for attribution. In addition to developing weights based exclusively on the
services included in the Base TCOC, the weights will be developed using the claim
Caps to adjust the weights and reduce the impact of catastrophic cases.
(D) Expected Trend:
(1) DHS will develop an expected trend rate for the Total Cost of Care based on the
same unit cost and utilization trend rates used to develop the annual expected cost
increases for the aggregate MHCP population.
(2) Appropriate adjustments will be made for services excluded from the Base
TCOC or other factors that are applicable to the Total Cost of Care and goals of the
program.
(E) Total Cost of Care Target (TCOC Target): The TCOC Target PMPM for the
Performance Period will be developed based on the Base TCOC and the expected trend.
2.3.2 Performance Period.
(A) Performance Period Total Cost of Care (Performance TCOC):
(1) At the end of a Performance Period, DHS will calculate the Performance Period
TCOC PMPM for the Performance Period Attributed Population.
(2) Claim costs for an Attributed Patient that fall outside of Caps in 2.2(F) above will
be capped to adjust the PMPM results for catastrophic cases.
(B) Performance Period Risk Score: Based on the services included in the Total Cost of
Care, a risk score will be developed for the Performance Period Attributed Population to
reflect their relative risk. The risk weights will be based on the aggregate MHCP
population’s claims experience, based exclusively on the services included in the Total
ATTACHMENT B-1: PAGE 4
IHP-SPECIFIC GOVERNANCE
4 of 7
Cost of Care, and developed using the claim Caps in 2.2(F) above to adjust the weights
for catastrophic cases.
(C) Adjusted Total Cost of Care Target (Adj. TCOC Target):
(1) The Target TCOC will be adjusted based on the increase or decrease in the risk
of the Attributed Populations (i.e., the change in the population risk from the Base
Period to the Performance Period).
(2) The Adjusted TCOC Target will be compared to the Performance Period TCOC
for purposes of determining the performance results and the basis for any financial
settlement.
2.4 Settlement Timing and Information.
(A) Each performance period will result in the calculation of Interim Payment and
Final Payment by the STATE for purposes of integrating sufficient Claims Runout
information into the final Shared Savings and Shared Losses calculation. The Interim
Payment will be calculated within five (5) months from the end of the Performance
Period using up to three (3) months of Claims Run-out. The Final Payment will be
calculated within seventeen (17) months of the end of the Performance Period using a
minimum of twelve (12) months of Claims Run-out.
(B) The Interim Payment will be calculated no later than five (5) months following the
end of the Performance Period based on:
(1) The final Base Period TCOC based on the claims incurred during the Base
Period by the Attributed Population in the final Base Period Attributed Population.
(2) The interim Performance Period TCOC based on the claims incurred during the
Performance Period by the Attributed Population in the interim Performance Period
Attributed Population.
(3) The change in risk between the final Base Period Risk Score for the Attributed
Population in the final Base Period Attributed Population and the interim
Performance Period Risk Score for the Attributed Population in the interim
Performance Period Attributed Population.
(4) The Base Period TCOC will be adjusted for trend and the change in the Base
Period Risk Score and the Performance Period Risk Score to develop the interim
Adjusted Target. The interim Adjusted Target will be compared to the interim
Performance Period TCOC for purposes of calculating the settlement amount.
(C) The Final Payment will be calculated no later than seventeen (17) months following
the end of the performance period based on:
(1) The final Base Period TCOC based on the claims incurred during the Base Period
by the Attributed Population in the final Base Period Attributed Population.
ATTACHMENT B-1: PAGE 5
IHP-SPECIFIC GOVERNANCE
5 of 7
(2) The final Performance Period TCOC based on the claims incurred during the
Performance Period by the Attributed Population in the final Performance Period
Attributed Population.
(3) The change in risk between the final Base Period Risk Score for the Attributed
Population in the final Base Period Attributed Population and the final Performance
Period Risk Score for the Attributed Population in the final Performance Period
Attributed Population.
(4) The Base Period TCOC will be adjusted for trend and the change in the Base
Period Risk Score and the Performance Period Risk Score to develop the Final
Adjusted Target. The Final Adjusted Target will be compared to the final
Performance Period TCOC for purposes of calculating the Final Payment.
2.5 Performance Thresholds. A two percent (2%) minimum performance threshold must
be met prior to any Shared Savings or Shared Losses.
(A) For an integrated IHP, the Performance TCOC must be above 102% or below 98%
of the Adjusted TCOC Target for Shared Losses or Shared Savings payments to occur.
(B) For a virtual IHP, the Performance TCOC must be below 98% of the Adjusted
TCOC Target for Shared Savings payments to occur.
3.1 Amount and Distribution of Assumed Risk. This section includes the amount and
distribution of the Shared Savings and Shared Losses in each of the three years of the
demonstration.
3.3 IHP Shared Savings and Losses. The IHP may counter-propose the amount of Shared
Savings and Shared Losses (i.e. savings achieved, meeting the two percent (2%) minimum
performance threshold).. IHP must provide such counter-proposal, if any, to the STATE at
least one hundred and twenty (120) days before renewal of the Contract according to section
5.2 Automatic Renewal. In the absence of a counter-proposal, the table in 3.2.1(B) below
shall govern for the subsequent Performance Period.
3.3.1 The Parties agree that the amount of Shared Savings and Shared Losses will be as
follows:
[IF INTEGRATED IHP]
(A) Actual Performance Period 1 and Proposed Performance Periods 2 and 3: IHP
must meet the two percent (2%) minimum performance threshold in order to receive
any Shared Savings or incur payments for Shared Losses. IHP assumes two-way risk
with symmetrical risk sharing thresholds and percentages. The maximum threshold for
Shared Savings in Performance Period 3 must be the same in Performance Period 1 and
is limited to a maximum of 85% of the Target TCOC.
[IF VIRTUAL IHP]
ATTACHMENT B-1: PAGE 6
IHP-SPECIFIC GOVERNANCE
6 of 7
As a virtual IHP, IHP shall have no Shared Losses. Shared Savings shall be shared
equally (50/50) in each year of the demonstration when a Total Cost Of Care (TCOC)
savings of 2% or greater is achieved (see 2.5(B) Performance Thresholds).
(B) Summary Table. The table below includes the actual and proposed three-year risk
sharing agreement for IHP.
Threshold
Performance Period 1
% of Adj. Target
IHP/DHS
TCOC
Distribution
Performance Period 2
% of Adj. Target IHP/DHS
TCOC
Distribution
Performance Period 3
% of Adj.
IHP/DHS
Target TCOC
Distribution
1
2
3
4
5
6
7
3.4 Claims Cap. The IHP has elected a claims Cap of $50,000/$100,000/$200,000 maximum
annual claims per Patient under section 2.2 (F).
Att_B-1_IHP-Specific_Governance_Financial Settlement _031716
ATTACHMENT B-1: PAGE 7
IHP-SPECIFIC GOVERNANCE
7 of 7
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
[IHP NAME]
2015 Base Period (To Be Updated for 2016 Base Period)
1.1 Summary: This document further describes the STATE’s method of measuring quality and patient experience among
Attributed Patients.
1.2 Definitions.
(A) Capitalized terms in this Attachment take the same meanings as in the Contract.
(B) “Absolute Improvement” is defined as the change in performance from Baseline to follow-up.
(C) “Baseline” means the Quality Measurement Period for the prior Performance Period (e.g., the Quality Measurement
Periods for Performance Period 1 are the Baseline for the Quality Measurement Periods for Performance Period 2).
(D) “MNCM” means Minnesota Community Measurement.
(E) “Relative Improvement” is defined as Absolute Improvement divided by the Baseline measurement.
(F) “Total Population” and “Sample” refer to use by MDH or the respective measure specification organization.
(Rest of page intentionally left blank.)
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
1 of 11
1.3 Measures: For the demonstration Performance Periods, the following measures will be used:
1.3.1. Physician Clinic Measures. Measures must be submitted using the data collection mechanism identified in the following
table.
Measure
Category
C01
Clinical
Measure Name
Optimal Diabetes
Care (ODC)
Composite:
HbA1c Control
Measure
Specification
Organization
Method of Data
Collection
Rate Used in
Calculations
Population
Data
Required
MNCM
MDH (via
MNCM portal
using DDS*
process); DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
MNCM
MDH (via
MNCM portal
using DDS*
process) ; DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
Statin use unless allowed
contraindications or exceptions
are present **
Blood Pressure
Tobacco Cessation
Aspirin use for selected patients
C02
Clinical
Optimal Vascular
Care Composite:
Statin use unless allowed
contraindications or exceptions
are present **
Blood Pressure Control
Tobacco Cessation
Aspirin Use
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
2 of 11
Measure
Category
Measure Name
Measure
Specification
Organization
Method of Data
Collection
Rate Used in
Calculations
Population
Data
Required
C03
Clinical
Depression
Depression Remission at Six
Months
MNCM
MDH (via
MNCM portal
using DDS*
process); DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
C04
Clinical
Optimal Asthma
Control
Composite:
Child/Adolescent
Asthma
Well-Controlled
MNCM
MDH (via
MNCM portal
using DDS*
process); DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
Not at Risk of Exacerbations
C05
Clinical
Asthma Care:
Child/Adolescent
Asthma Education and SelfManagement
MNCM
MDH (via
MNCM portal
using DDS*
process); DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
C06
Clinical
Optimal Asthma
Control
Composite: Adult
Asthma
Well-Controlled
MNCM
MDH (via
MNCM portal
using DDS*
process); DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
Not at Risk of Exacerbations
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
3 of 11
Measure
Category
Measure Name
Measure
Specification
Organization
Method of Data
Collection
Rate Used in
Calculations
Population
Data
Required
C07
Clinical
Asthma Care:
Adults
Asthma Education and SelfManagement
MNCM
MDH (via
MNCM portal
using DDS*
process); DHS
shall obtain the
measure results
Medicaidspecific
Total
Population
C08
Patient
Experience
Consumer
Assessment of
Healthcare
Providers and
Systems
Clinician &
Group Survey
(CG-CAHPS): 6
Months
Reference Period
Timely Appointments, Care and
Information
MNCM
MDH; DHS
shall obtain the
measure results
Total
Population
“Top Box”
Rate
Sample or
Total
Population
C09
C10
C11
C12
How Well Providers
Communicate with Patients
Helpful Respectful and
Courteous Office Staff
Patient Rating of Provider as 9
or 10.
Measuring Care Coordination**
* All IHP Participant clinics must submit total population data via the direct data submission (DDS) process for these measures,
except for those without an electronic medical record who may submit data based on a sample as mutually agreed upon in writing by
the Parties. For those clinics that submit data based on a sample, the sample-based results will be reweighted to reflect the clinic total
population.
** This measure will be included if it is required for reporting in the final administrative rule for the Minnesota Statewide Quality
Reporting and Measurement System (Minnesota Administrative Rules, Chapter 4654) adopted during calendar year 2015 by the
Minnesota Department of Health.
(Remainder of page intentionally left blank)
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
4 of 11
1.3.2. Hospital Measures:
Measure
Category
H03
Patient
Experience
H04
H05
Measure Name
Consumer
Assessment of
Healthcare
Providers and
Systems Hospital
Survey (Hospital
CAHPS):
Communication with Nurses
H07
Communication about
Medications
H08
Cleanliness of Hospital
Environment
H09
Quietness of Hospital
Environment
H10
Discharge Information
H11
Overall Hospital Rating
H12
Recommend the Hospital as 9
or 10
H13
Care Transitions
H15
Clinical
AHRQ Patient
Safety For
Selected
Pressure Ulcer Rate (PSI 03)
Rate Used in
Calculations
Population
Data
Required
MDH (via
CMS Hospital
Compare):
DHS shall
obtain the
measure
results
Total
Population
“Top Box”
Rate
Sample or
Total
Population
AHRQ
MDH (via
CMS
Hospital
Total
Population
Rate
Sample or
Total
Population
Responsiveness of Hospital
Staff
Pain Management
Method of Data
Collection
CMS
Communication with Doctors
H06
H14
Measure
Specification
Organization
Iatrogenic Pneumothorax Rate
(PSI 06)
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
5 of 11
Measure
Category
H16
Measure Name
Indicators
composite (PSI
90)
Measure
Specification
Organization
Central Venous CatheterRelated Blood Stream
Infections Rate (PSI 07)
H17
Postoperative Hip Fracture Rate
(PSI 08)
H18
Postoperative Hemorrhage or
Hematoma Rate (PSI 09)
H19
Postoperative Physiologic and
Metabolic Derangement Rate
(PSI 10)
H20
Postoperative Respiratory
Failure Rate (PSI 11)
H21
Postoperative Pulmonary
Embolism or Deep Vein
Thrombosis Rate (PSI 12)
H22
Postoperative Sepsis Rate (PSI
13)
H23
Postoperative Wound
Dehiscence Rate (PSI 14)
H24
Accidental Puncture or
Laceration Rate (PSI 15)
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
Method of Data
Collection
Rate Used in
Calculations
Population
Data
Required
Compare):
DHS shall
obtain the
measure
results
6 of 11
1.3.3. Graduated Effect on Shared Savings Payments in Demonstration Performance Periods. Quality and patient
experience measures will affect the IHP’s portion of the Shared Savings. The amount of the Final Payment that would otherwise
be available pursuant to section 4.2 (B) of the Contract shall be modified:
(A) Performance Period 1. Reporting of the measures will have a twenty-five percent (25%) effect on the payment (if any) of
Shared Savings; that is, 25% of the dollar amount saved in the Total Cost of Care calculation in Attachment B-1 “IHP
Specific Governance and Financial Settlement,” shall be multiplied by the overall quality score calculated in section 1.5
below. The remainder of the available Shared Savings Final Payments shall not be reduced by the effect of the quality and
patient experience scores.
(B) Performance Period 2. The measure results will have a twenty-five percent (25%) effect on the payment (if any) of
Shared Savings; that is, 25% of the dollar amount saved in the Total Cost of Care calculation in Attachment B-1 “IHP
Specific Governance and Financial Settlement,” shall be multiplied by the overall quality score calculated in section 1.5
below. The remainder of the available Shared Savings Final Payments shall not be reduced by the effect of the quality and
patient experience scores.
(C) Performance Period 3. The measure results will have a fifty percent (50%) effect on the payment (if any) of Shared
Savings; that is, 50% of the dollar amount saved in the Total Cost of Care calculation in Attachment B-1 “IHP Specific
Governance and Financial Settlement,” shall be multiplied by the overall quality score calculated in section 1.5 below. The
remainder of the available Shared Savings Final Payments shall not be reduced by the effect of the quality and patient
experience scores.
1.4 Calculation of Measures for the Overall Quality Score.
1.4.1. Weights. The patient experience measures described in sections 1.3.1 and 1.3.2 above shall account for twenty-five
percent (25%) of the overall quality score, as specified in Section 1.5.2. The remaining measures in sections 1.3.1 and 1.3.2
above shall account for seventy-five (75%) of the overall quality score, as specified in Section 1.5.2, regardless of the number of
measures agreed upon by the Parties.
1.4.2. Quality Measurement Periods. Applicable dates of service, visit dates, or discharge dates for the three Performance
Periods of the demonstration are described below for each quality measure.
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
7 of 11
Applicable Dates of Service (DOS), Visit Dates, or Discharge Dates
Measure
Performance Period 1 (2016)
Quality Measurement Periods
Performance Period 2 (2017)
Optimal Diabetes Care Composite
Optimal Vascular Care Composite
Depression Remission at 6 Months
January – December 2016 DOS
January – December 2016 DOS
January – December 2015 Days
of Index with a follow-up
period of July 2015 – June 2016
July 2015 – June 2016 DOS
January – December 2017 DOS
January – December 2017 DOS
January – December 2016 Days
of Index with a follow-up
period of July 2016 – June 2017
July 2016 – June 2017 DOS
January – December 2018 DOS
January – December 2018 DOS
January – December 2017 Days
of Index with a follow-up
period of July 2017 – June 2018
July 2017 – June 2018 DOS
July 2015 – June 2016 DOS
July 2016 – June 2017 DOS
July 2017 – June 2018 DOS
July 2015 – June 2016 DOS
July 2016 – June 2017 DOS
July 2017 – June 2018 DOS
July 2015 – June 2016 DOS
July 2016 – June 2017 DOS
July 2017 – June 2018 DOS
September – November 2014
DOS
October 2015 – September
2016
January – December 2016 DOS
September – November 2016
DOS
October 2016 – September
2017
January – December 2017 DOS
September – November 2016
DOS
October 2017- September 2018
Optimal Asthma Control Composite
– Adults
Asthma Care – Adults: Asthma
Education and Self-Management
Optimal Asthma Control Composite
– Children / Adolescents
Asthma Care – Children /
Adolescents: Asthma Education and
Self-Management
Patient Experience (CG-CAHPS)
Patient Experience (HCAHPS) **
AHRQ Patient Safety For Selected
Indicators composite (PSI 90)
Performance Period 3 (2018)
January – December 2018 DOS
** Discharge dates within these time periods. If more recent data (i.e., full calendar year that would allow alignment with Performance
Period dates) is available at the time of the calculation of the final settlement calculation, it will be used in place of the discharge dates listed.
1.5 Cumulative Calculation Methods.
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
8 of 11
1.5.1. Awarding of Points
(A) Reporting. For Performance Period 1, the IHP shall be awarded two (2) points for each measure listed in section 1.3. For
each measure, the two (2) points shall be reducible by the percent of IHP Participants not reporting the quality measure in the
manner specified in section 1.3.
(B) Aggregating clinic-level results and hospital-level results. An IHP quality measure result will be determined for each
quality measure by summing the numerators and denominators of multiple clinic-level results or hospital-level results, as
applicable.
(C) Performance. For Performance Periods 2 and 3, the IHP rate for each measure listed in section 1.3 shall be assessed for
both achievement and improvement and the score for each measure will be the greater of the achievement or improvement
score as defined below. For each measure, the points awarded shall be reducible by the percent of IHP Participants not
reporting the quality measure in the manner specified in section 1.3.
(1) Achievement. Each measure shall be assessed against a defined minimum attainment threshold and an upper
threshold. For each measure that meets or exceeds the upper threshold, two (2) points shall be awarded. For each
measure that is below the minimum attainment threshold, zero (0) points shall be awarded. For each measure that meets
or exceeds the minimum attainment threshold and is below the upper threshold, between one (1) and two (2) points shall
be awarded, according to the following ranges:
Percentile
th
th
30 -< 40
40th - < 50th
50th - < 60th
60th - < 70th
70th - < 80th
Points Awarded
1.0
1.2
1.4
1.6
1.8
The STATE will notify IHP, before the beginning of the Performance Period, by publishing on the DHS public website
the minimum attainment and upper preliminary thresholds. The STATE will notify the IHP of final thresholds upon
calculation using the data based on the most recent Quality Measurement Period.
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
9 of 11
(2) Improvement.
(a) Each measure shall be assessed against a Baseline rate. For each measure that has a ten percent (10%) or more
Relative Improvement compared to the Baseline rate, the IHP shall be awarded two (2) points. For each measure that
has less than a five percent (5%) Relative Improvement compared to the Baseline rate, the IHP shall be awarded zero
(0) points. For each measure that has five percent (5%) or more and less than ten percent (10%) Relative Improvement
compared to the Baseline rate, between one (1) and two (2) points shall be awarded according to the following ranges:
Percent (%) Relative Improvement
5% - < 6%
6% - < 7%
7% - < 8%
8% - < 9%
9% - < 10%
Example calculation:
Points Awarded
1.0
1.2
1.4
1.6
1.8
Performance Period 1 (Baseline) rate = 25%
Performance Period 2 rate achieved = 28%
(28% - 25% = 3% Absolute Improvement; 3% ÷ 25% = 12% Relative Improvement)
Improvement points earned for measure = 2 points
(b) If a measure specification changes in a way that would make a year-to-year comparison statistically invalid, such as
a change in the clinical target value (for example, most recent HbA1c value changes from <8.0 to <7.0 for the Optimal
Diabetes Care Measure from one measurement period to the next) awarding points based on improvement will not be
available for that measure.
(D) For all Performance Periods, the total points earned by IHP in each measure category shall be summed and divided by
the total points available for that category to produce a category score of the percentage of points earned versus points
available for the Performance Period. The points score shall be converted to an overall quality score, considering the weights
listed below and in section 1.4.1 above.
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
10 of 11
1.5.2. Table of measures, points and weights.
Measure Category
Integrated Model Weights
Virtual Model Weights
Clinical, clinic
45%
60%
Clinical, hospital
30%
15%
Total Clinical
75%
75%
Patient Experience, clinic
15%
20%
Patient Experience, hospital
10%
5%
Total Patient Experience
25%
ATTACHMENT B-2: IHP-SPECIFIC QUALITY AND PATIENT EXPERIENCE MEASURES.
Base Period 2015
25%
11 of 11
ATTACHMENT B-3: BUSINESS ASSOCIATE
1.1 Summary. This Attachment sets forth the terms and conditions in which STATE will share
data with and permit IHP to use or disclose Protected Information that the parties are legally
required to safeguard pursuant to the Minnesota Data Practices Act under Minnesota Statutes,
chapter 13, the Health Insurance Portability and Accountability Act rules and regulations codified at
45 CFR Parts 160, 162, and 164 (HIPAA) and other applicable laws.
The parties agree to comply with all applicable provisions of the Minnesota Data Practices Act,
HIPAA, and any other state and federal statutes that apply to the Protected Information.
It is expressly agreed that IHP is a “business associate” of STATE, as defined by HIPAA under
45 CFR § 160.103. The disclosure of protected health information to IHP that is subject to the
HIPAA is permitted by 45 CFR § 164.502(e)(1)(i).
1.2 Definitions
(A) Agent means IHP's employees, contractors, subcontractors, and other non-employees
and agents.
(B) Applicable Safeguards means the state and federal provisions listed in section 1.4.1
below.
(C) Breach means the acquisition, access, use, or disclosure of unsecured protected
health information in a manner not permitted by HIPAA, which compromises the
security or privacy of protected health information.
(D) Business associate means the same as “business associate” at 45 CFR § 160.103, and
in reference to the party in the Contract and this Attachment, shall mean IHP.
(E) Contract means the Integrated Health Partnership contract between STATE and IHP.
(F) Disclosure means the release, transfer, provision of access to, or divulging in any
manner of information by the entity in possession of the Protected Information.
(G) HIPAA means the rules and regulations codified at 45 CFR Parts 160, 162, and 164.
(H) Individual means the person who is the subject of protected information.
(I) Privacy incident means a violation of an information privacy provision of any
applicable state and federal law, statute, regulation, rule, or standard, including those
listed in the Contract and this Attachment.
(J) Protected information means any information that is or will be used by STATE or
IHP, and is protected by federal or state laws, statutes, regulations or standards,
including those listed in this Attachment. This includes, but is not limited to,
individually identifiable information about a State, county or tribal human services
ATTACHMENT B-3 – PAGE 1 OF 10
BUSINESS ASSOCIATE
agency client or a client’s family member. Protected information also includes, but is not
limited to, protected health information, as defined below, and protected information
maintained within or accessed via a State information management system, including a
State “legacy system” and other State application.
(K) Protected health information (PHI) or “the PHI data” is a subset of individually
identifiable health information in accordance with 45 CFR § 160.103, but for purposes
of this Attachment refers only to specific information that is received, created,
maintained, or transmitted by IHP as a business associate on behalf of DHS, as listed in
section 3.4.2 of the Contract.
(L) Security incident means the attempted or successful unauthorized use or the
interference with system operations in an information system. Security incident does not
include pings and other broadcast attacks on a system’s firewall, port scans, unsuccessful
log-on attempts, denials of service, and any combination of the above, provided that
such activities do not result in the unauthorized use of Protected Information.
(M)
Use means any activity by the parties involving protected information
including its creation, collection, access, use, modification, employment, application,
utilization, examination, analysis, manipulation, maintenance, dissemination, sharing,
disclosure, transmission, or destruction. Use includes any of these activities whether
conducted manually or by electronic or computerized means.
(N) User means an agent of either party, who has been authorized to use protected
information.
1.3 Information Exchanged
(A) This Attachment governs the PHI data that will be exchanged pursuant to IHP
performing the services described in the Contract. For the purposes of this Attachment,
data exchanged include only the data described in section 3.4.2 of the Contract.
(B) The PHI data exchanged under the Contract is provided to IHP in order for IHP to
perform program analysis in order to improve its performance under the Contract.
(C) STATE is permitted to share the PHI data with IHP pursuant to Minnesota Statutes,
§ 13.46 and the laws listed in section 1.4.1 below.
1.4 Information Privacy and Security
1.4.1 Compliance with Applicable Safeguards.
(A) State and Federal Safeguards. The parties acknowledge that the Protected
Information to be shared under the terms of the Contract may be subject to one of the
following laws, statutes, regulations, rules, and standards, as applicable (“Applicable
Safeguards”). The parties agree to comply with all rules, regulations and laws, including
ATTACHMENT B-3 – PAGE 2 OF 10
BUSINESS ASSOCIATE
as amended or revised, applicable to the exchange, use and disclosure of data under the
Contract.
(1) Health Insurance Portability and Accountability Act rules and regulations
codified at 45 CFR Parts 160, 162, and 164 (HIPAA);
(2) Minnesota Government Data Practices Act (Minn. Stat. Chapter 13);
(3) Minnesota Health Records Act (Minn. Stat. §144.291 - 144.298);
(4) Confidentiality of Alcohol and Drug Abuse Patient Records (42 USC § 290dd-2
and 42 CFR § 2.1 to §2.67);
(5) Tax Information Security Guidelines for Federal, State and Local Agencies (26
USC 6103 and Publication 1075);
(6) U.S. Privacy Act of 1974;
(7) Computer Matching Requirements (5 USC 552a);
(8) Social Security Data Disclosure (section 1106 of the Social Security Act);
(9) Disclosure of Information to Federal, State and Local Agencies (“DIFSLA
Handbook” Publication 3373);
(10) Final Exchange Privacy Rule of the Affordable Care Act (45 CFR § 155.260);
and
(11) NIST Special Publication 800-53, Revision 4 (NIST.SP.800-53r4).
(B) Statutory Amendments and Other Changes to Applicable Safeguards. The Parties
agree to take such action as is necessary to amend the Contract and this Attachment from
time to time as is necessary to ensure, current, ongoing compliance with the
requirements of the laws listed in this section or in any other applicable law.
1.4.2 IHP Data Responsibilities
(A) Use Limitation.
(1) Restrictions on Use and Disclosure of the PHI data. Except as otherwise
authorized in the Contract or this Attachment, IHP may only use or disclose the PHI
data as necessary to provide the services to STATE as described herein, or as
otherwise permitted or required by law, provided that such use or disclosure of the
PHI data, if performed by STATE, would not violate the Contract, this Attachment,
HIPAA, or other state and federal statutes or regulations that apply to the PHI data.
(2) Federal tax information. To the extent that Protected Information used under the
Contract constitutes “federal tax information” (FTI), IHP shall ensure that this data
ATTACHMENT B-3 – PAGE 3 OF 10
BUSINESS ASSOCIATE
only be used as authorized under the Patient Protection and Affordable Care Act, the
Internal Revenue Code, 26 USC § 6103(C), and IRS Publication I 075.
(B) Individual Privacy Rights. IHP shall ensure individuals are able to exercise their
privacy rights regarding the PHI data, including but not limited to the following:
(1) Complaints. IHP shall work cooperatively with STATE to resolve complaints
received from an individual; from an authorized representative; or from a state,
federal, or other health oversight agency.
(2) Amendments to the PHI data Requested by Data Subject Generally. Within ten
(10) business days, IHP must forward to STATE any request to make any
amendment(s) to the PHI data in order for STATE to satisfy its obligations under
Minn. Stat. § 13.04, subd. 4. IHP must also make any amendment(s) to the PHI data
as directed or agreed to by STATE pursuant to 45 CFR § 164.526 or otherwise act as
necessary to satisfy STATE or IHP’s obligations under 45 CFR § 164.526
(including, as applicable, the PHI data in a designated record set).
(C) Background Review and Reasonable Assurances Required of Agents.
(1) Reasonable Assurances. IHP represents that, before its Agents are allowed to use
or disclose the PHI data, IHP has conducted and documented a background review of
such Agents sufficient to provide IHP with reasonable assurances that the Agent will
comply with the terms of the Contract, this Attachment and Applicable Safeguards.
(2) Documentation. IHP shall make available documentation required by this section
upon request by STATE.
(D) Ongoing Responsibilities to Safeguard Protected Information.
(1) Privacy and Security Policies. IHP shall develop, maintain, and enforce policies,
procedures, and administrative, technical, and physical safeguards to ensure the
privacy and security of Protected Information obtained from the STATE.
(2) Electronic Protected Information. IHP shall implement and maintain appropriate
safeguards, and comply with Subpart C of 45 CFR Part 164 (HIPAA Security Rule)
with respect to electronic PHI data to prevent the use or disclosure other than as
provided for by the Contract or this Attachment.
(3) Monitoring Agents. IHP shall ensure that any contractor, subcontractor, or other
agent to whom IHP discloses Protected Information on behalf of STATE, or whom
IHP employs or retains to create, receive, use, store, disclose, or transmit Protected
Information on behalf of STATE, agrees to the same restrictions and conditions that
apply to IHP under the Contract and this Attachment with respect to such Protected
Information, and in accordance with 45 CFR §§ 164.502(e)(1)(ii) and 164.308(b)(2).
ATTACHMENT B-3 – PAGE 4 OF 10
BUSINESS ASSOCIATE
(4) Minimum Necessary Access to Protected Information. IHP shall ensure that its
Agents use only the minimum necessary Protected Information needed to complete
an authorized and legally permitted activity.
(5) Training. IHP shall ensure that Agents are properly trained and comply with all
Applicable Safeguards and the terms of the Contract and this Attachment.
(E) Responding to Privacy Incidents, Security Incidents, and Breaches. HP will comply
with this section for all protected information shared under the Contract.
(1) Mitigation of harmful effects. Upon discovery of any actual or suspected privacy
incident, security incident, or breach, IHP will mitigate, to the extent practicable, any
harmful effect of the privacy incident, security incident, or breach. Mitigation may
include, but is not limited to, notifying and providing credit monitoring to affected
individuals.
(2) Investigation. Upon discovery of any actual or suspected privacy incident,
security incident, or breach, IHP will investigate to (1) determine the root cause of
the incident, (2) identify individuals affected, (3) determine the specific protected
information impacted, and (4) comply with notification and reporting provisions of
the Contract, this Attachment and applicable law.
(3) Corrective action. Upon identifying the root cause of any privacy incident,
security incident, or breach, IHP will take corrective action to prevent, or reduce to
the extent practicable, any possibility of recurrence. Corrective action may include,
but is not limited to, patching information system security vulnerabilities, employee
sanctions, or revising policies and procedures.
(4) Notification to individuals and others; costs incurred. IHP will determine whether
notice to data subjects and/or any other external parties regarding any privacy
incident or security incident is required by law. If such notice is required, IHP will
comply with STATE and IHP’s obligations under any applicable law requiring
notification, including, but not limited to, Minn. Stat. § 13.05 and 13.055. If a
privacy incident or security incident results in a breach of the PHI data, as this term
is defined in this Attachment, then IHP will provide notice to individual data subjects
under any applicable law requiring notification, including but not limited to
providing notice as outlined in 45 CFR § 164.404. If IHP fails to notify individual
data subjects or other external parties as required by law, then IHP will reimburse
STATE for any costs incurred as a result of IHP’s failure to provide notification.
(5) Obligation to report to STATE. Upon discovery of a privacy incident, security
incident, or breach involving the PHI data, IHP will report to STATE in writing as
specified in section 2.2(F).
(6) Communication with authorized representative. IHP will send any written reports
to, and communicate and coordinate as necessary with, STATE’s authorized
representative.
ATTACHMENT B-3 – PAGE 5 OF 10
BUSINESS ASSOCIATE
(7) Cooperation of response. IHP will cooperate with requests and instructions
received from STATE regarding activities related to investigation, containment,
mitigation, and eradication of conditions that led to, or resulted from, the security
incident, privacy incident, or breach.
(8) Information to respond to inquiries about an investigation. IHP will, as soon as
possible, but not later than forty-eight (48) hours after a request from STATE,
provide STATE with any reports or information requested by STATE related to an
investigation of a security incident, privacy incident, or breach.
(9) Documentation. IHP will document actions taken under 1.4.2(E)(1) through
1.4.2(E)(4) of this section, and provide such documentation to STATE upon request.
(F) Reporting Privacy Incidents, Security Incidents, and Breaches. IHP will comply
with the reporting obligations of this section as they apply to the kind of protected
information involved. IHP will also comply with section 1.4.2(E) in responding to any
privacy incident, security incident, or breach.
(1) IHP will report breaches and security incidents involving the PHI data to STATE
and other external parties. IHP will notify STATE, in writing, of (1) any breach or
suspected breach of PHI; (2) any security incident; or (3) any violation of an
individual's privacy rights as they involve the PHI data created, received, maintained,
or transmitted by IHP or its Agents on behalf of STATE.
(a) Breach reporting. IHP will report, in writing, any breach of the PHI data to
STATE within five (5) business days of discovery, in accordance with 45 C.F.R
§ 164.410.
(b) Content of report to STATE. Reports to the authorized representative
regarding breaches of the PHI data will include:
(i) Identities of the individuals whose unsecured PHI has been breached.
(ii) Date of the breach and date of its discovery.
(iii) Description of the steps taken to investigate the breach, mitigate its
effects, and prevent future breaches.
(iv) Sanctions imposed on members of IHP’s workforce involved in the
breach.
(v) Other available information that is required to be included in notification
to the individual under 45 CFR § 164.404(c).
(vi) Statement that IHP has notified, or will notify, affected data subjects in
accordance with 45 CFR § 164.404.
ATTACHMENT B-3 – PAGE 6 OF 10
BUSINESS ASSOCIATE
(2) Security incidents resulting in a breach. IHP will report, in writing, any security
incident that results in a breach, or suspected breach, of the PHI data to STATE
within five (5) business days of discovery, in accordance with 45 C.F.R § 164.314
and 45 C.F.R § 164.410.
(3) Security incidents that do not result in a breach. IHP will report all security
incidents that do not result in a breach, but involve systems maintaining the PHI data
to STATE on a monthly basis, in accordance with 45 C.F.R § 164.314.
(4) Other violations. IHP will report any other violation of an individual’s privacy
rights as it pertains to the PHI data to STATE within five (5) business days of
discovery. This includes, but is not limited to, violations of HIPAA data access or
complaint provisions.
(5) Reporting to other external parties. IHP will report all breaches of the PHI data to
the federal Department of Health and Human Services, as specified under 45 CFR
§ 164.408. If a breach of the PHI data involves 500 or more individuals, IHP will
immediately notify STATE. STATE and IHP will coordinate any report to the news
media and federal Department of Health and Human Services in accordance with 45
CFR §§ 164.406-408.
(6) Other Protected Information. IHP will report other privacy incidents and security
incidents involving the PHI data to STATE.
(a) Initial report. IHP will report all other privacy and security incidents
involving the PHI data to STATE, in writing, within five (5) days of discovery. If
IHP is unable to complete its investigation of, and response to, a privacy incident
or security incident within five (5) days of discovery, then IHP will provide
STATE with all information regarding the PHI data under 1.4.2(E) that is
available to IHP at the time of the initial report.
(b) Final report. IHP will, upon completion of its investigation of and response to
a privacy incident or security incident, or upon STATE’s request, submit in
writing a report to STATE documenting all actions taken under section 1.4.2(E).
(G) Designated Record Set; PHI. If, on behalf of STATE the IHP maintains a complete
or partial designated record set, as defined in 45 CFR § 164.501 , IHP shall provide the
means for an individual to access, inspect, or receive copies of the individual’s PHI;
provide the means for an individual to make an amendment to the individual’s PHI; and
provide the means for access and amendment in the time and manner that complies with
HIPAA or as otherwise directed by STATE.
(H) Access to Books and Records, Security Audits, and Remediation. IHP shall conduct
and submit to audits and necessary remediation as required by this section to ensure
compliance with all Applicable Safeguards and the terms of the Contract and this
Attachment.
ATTACHMENT B-3 – PAGE 7 OF 10
BUSINESS ASSOCIATE
(1) IHP represents that it has audited and will continue to regularly audit the security
of the systems and processes used to provide services under the Contract and this
Attachment, including, as applicable, all data centers and cloud computing or hosting
services under contract with IHP. IHP will conduct such audits in a manner
sufficient to ensure compliance with the security standards referenced in this
Attachment.
(2) This security audit required above will be documented in a written audit report
which will, to the extent permitted by applicable law, be deemed confidential
security information and not public data under the Minnesota Government Data
Practices Act.
(3) IHP agrees to make its internal practices, books, and records related to its
obligations under the Contract and this Attachment available to STATE or a STATE
designee upon STATE’s request for purposes of conducting a financial or security
audit, investigation, or assessment, or to determine IHP’s or STATE’s compliance
with Applicable Safeguards, the terms of this Attachment and accounting standards.
For purposes of this provision, other authorized government officials includes, but is
not limited to, the Secretary of the United States Department of Health and Human
Services.
(4) IHP will make and document best efforts to remediate any control deficiencies
identified during the course of its own audit(s), or upon request by STATE or other
authorized government official(s), in a commercially reasonable timeframe.
(I) Documentation Required. Any documentation required by this Attachment, or by
applicable laws, standards, or policies, of activities including the fulfillment of
requirements by IHP, or of other matters pertinent to the execution of the Contract, must
be securely maintained and retained by IHP for a period of six years from the date of
expiration or termination of the Contract, or longer if required by applicable law, after
which the documentation must be disposed of consistent with section 2.6 of this
Attachment.
(J) IHP shall document disclosures of the PHI data made by IHP that are subject to the
accounting of disclosure requirement described in 45 CFR § 164.528, and shall provide
to STATE such documentation in a time and manner designated by STATE at the time
of the request.
(K) Requests for Disclosure of Protected Information. Pursuant to Minnesota Statutes,
§ 13.05, subd. 11, all of the data created, collected, received, stored, used, maintained, or
disseminated by the IHP in performing under this Contract is subject to the requirements
of Chapter 13, and IHP must comply with those requirements as if it were a government
entity. Unless provided for otherwise in this Contract, if IHP receives a request to
release the PHI data referred to in section 3.4.2 of the IHP Contract, IHP must
immediately notify and consult with the STATE. The STATE will give IHP instructions
concerning the release of the data to the requesting party before the data are released. If
ATTACHMENT B-3 – PAGE 8 OF 10
BUSINESS ASSOCIATE
IHP discloses Protected Information after coordination of a response with STATE, it
shall document the authority used to authorize the disclosure, the information disclosed,
the name of the receiving party, and the date of disclosure. All such documentation shall
be maintained for the term of the Contract and shall be produced upon demand by
STATE.
(L) Conflicting Provisions. IHP shall comply with all applicable provisions of HIPAA
and with the Contract and this Attachment. To extent that the parties determine,
following consultation, that the terms of this Attachment are less stringent than the
Applicable Safeguards, IHP must comply with the Applicable Safeguards. In the event
of any conflict in the requirements of the Applicable Safeguards, IHP must comply with
the most stringent Applicable Safeguard.
(M)
Data Availability. IHP, or any entity with legal control of any assets of IHP,
shall make any and all protected information under the Contract and this Attachment
available to STATE upon request within a reasonable time as is necessary for STATE to
comply with applicable law.
1.5 Data Security.
(A) STATE Information Management System Access. If STATE grants IHP access to
Protected Information maintained in a STATE information management system
(including a STATE “legacy” system) or in any other STATE application, computer, or
storage device of any kind, then IHP agrees to comply with any additional system- or
application-specific requirements as directed by STATE.
(B) Electronic Transmission. The parties agree to encrypt electronically transmitted
Protected Information in a manner that complies with NIST Special Publications 800-52,
Guidelines for the Selection and Use of Transport Layer Security Implementations; 80077, Guide to IPsec VPNs; 800-113, Guide to SSL VPNs, or others methods validated
under Federal Information Processing Standards 140-2.
(C) Portable Media and Devices. The parties agree to encrypt Protected Information
written to or stored on portable electronic media or computing devices in a manner that
complies with NIST SP 800-111, Guide to Storage Encryption Technologies for End
User Devices.
1.6 IHP Permitted Uses and Responsibilities.
(A) Management and Administration. Except as otherwise limited in the Contract or this
Attachment, IHP may:
(1) Use PHI for the proper management and administration of IHP or to carry out the
legal responsibilities of IHP.
(2) Disclose PHI for the proper management and administration of IHP, provided
that the disclosure is required by law; or the disclosure is required to perform the
ATTACHMENT B-3 – PAGE 9 OF 10
BUSINESS ASSOCIATE
services provided to or on behalf of STATE or the disclosure is otherwise authorized
by STATE, and IHP:
(3) Obtains reasonable assurances, in the form of a data sharing agreement, from the
entity to whom the PHI will be disclosed that the PHI will remain confidential, and
will not be used or disclosed other than for the contracted services or the authorized
purposes; and
(4) IHP requires the entity to whom PHI is disclosed to notify IHP of any
compromise to the confidentiality of PHI of which it becomes aware.
(5) De-identify PHI. IHP may use PHI to create de-identified PHI provided that IHP
complies with the de-identification methods specified in 45 CFR § 164.514.
(6) Aggregate PHI. IHP may use PHI to perform data aggregation services for
STATE. The use of PHI by IHP to perform data analysis or aggregation for parties
other than STATE must be expressly approved by STATE.
1.7 STATE Data Responsibilities
(A) STATE shall disclose Protected Information, including the PHI data, only as
authorized by law to IHP for its use or disclosure.
(B) STATE shall obtain any consents or authorizations that may be necessary for it to
disclose Protected Information with IHP.
(C) STATE shall notify IHP of any limitations that apply to STATE’s use and disclosure
of Protected Information that would also limit the use or disclosure of Protected
Information by IHP.
(D) STATE shall refrain from requesting IHP to use or disclose Protected Information in
a manner that would violate applicable law or would be impermissible if the use or
disclosure were performed by STATE.
ATTACHMENT B-3 – PAGE 10 OF 10
BUSINESS ASSOCIATE
Appendix B: DHS IHP Provider Portal
1. Example of Performance Dashboard in the IHP Portal
2. Example of IHP Care Management Report within the IHP Portal
3. Example of IHP Summary of Quality and Patient Experience Measures in IHP Portal
Appendix C: IHP Provider Roster & Roster Instructions
MN DEPARTMENT OF HUMAN SERVICES (DHS)
INTEGRATED HEALTH PARTNERSHIPS (IHP) PROVIDER ROSTERS
Description
Each Integrated Health Partnership (IHP) must submit a roster of their participating primary care and specialty providers to be used
in the attribution methodology. An IHP may submit an updated roster by the last business day of each quarter. The most recently
submitted roster remains in effect for an IHP if no updated roster is received.
Provider Rosters can be submitted in delimited text files or .xls formats. The minimum necessary fields are bolded below. It is
helpful to include the applicable data elements below (provider name, credentials, etc.) in the event it is necessary to address
corrections or clarifications when matching to DHS data.
If a provider practices at multiple locations within the IHP, it is only necessary to list the provider once. The provider’s E&M services
for any location participating in the IHP will be included for attribution.
If all the clinics (“organizational”) NPI’s which make up the participating IHP locations are not represented at least once on the
roster, the IHP should include the provider location as a separate provider record (line) on the roster. IHPs should include providers
who are part of participating locations as defined on Attachment B of the IHP’s contract. If an IHP wishes to expand the list of
participating partners or locations, please first contact your DHS IHP Lead.
IHP Rosters should include all providers who were active during the prior year. Each submission is used to update a provider record
(based on individual NPI) or add providers to an IHP’s roster. Unless inclusion of a provider was a submission error or other special
circumstance, providers are not removed from an IHP’s roster. Providers who become inactive or leave a participating IHP location
are handled through use of the individual + pay-to provider NPI combinations.
Column Definitions
Column Name
Definition
IHP Organization
The IHP submitting the roster (for example A123456789)
Provider NPI
The NPI of the provider who renders the service for the IHP. Format the NPI as text.
Last Name
The last name of the treating provider.
First Name
The first name of the treating provider.
Middle Name
The middle name or initial of the treating provider.
Credentials or Title
Treating Provider’s credentials (MD, PA, CNS, etc.) if available.
Taxonomy Code
This field can only be empty if the IHP has entered a valid value in the “Specialty” field. Otherwise, it
must contain the taxonomy code for the provider’s specialty (for example, 207R00000X). The taxonomy
code will be used to designate the provider as a primary care provider or a specialty care provider.
Location
The name of the primary location or clinic for the provider.
Address 1
Address 2
The address of the primary clinic location.
City
State
Employer Legal Name
The Group Practice or Legal DBA name for the participating IHP entity through which the provider is
employed. This may be the same as the clinic location, or may be a larger provider group. Attribution is not
done at this level, but the employer name may be helpful for future aggregated reporting back to the IHP.
EIN (TIN)
The tax identification number for the employer group or clinic receiving payment. Format the tax id as text.
Clinic NPI
The organizational NPI used for billing at the provider’s primary location. Format the Clinic NPI as text.
v.2012Dec
1
Although listed with a specific provider, all clinic NPI’s on the IHP roster are used in aggregate to ensure
that only E&M services occurring at participating IHP entities are included in attribution.
Specialty
An IHP can designate whether the treating provider functions as a primary care provider (“PCP”) or
specialty care provider (“SPE”) for this IHP. If a “PCP” or “SPE” is entered in this column, its value will
override the mapping based on the provider’s registered or listed taxonomy code. This column can be
empty only if the IHP has included the provider’s taxonomy code.
The submission of a Provider Roster must be certified by a delegate of the IHP. The certification can be in the form of an email
which identifies the submission date, file or submission name, and an attestation that the data is believed to be accurate and
complete based on the best knowledge. The attestation can accompany the roster submission (for example in the email used to
submit the roster), or may be submitted separately according to section 3.6.E of the IHP contract.
v.2012Dec
2
IHP_organization
A555778421
A555778421
A555778421
A555778421
NPI
123456
7890
234567
8910
321478
9054
155839
2852
Last_N
ame
Lastna
me
Namel
ast
First_ Middle_
Taxonomy_
Name Name Title
Code
207Q00000
First L
MD
X
363A00000
Name
PA-C X
Provid
Sample er
DO
Smith
Joe
NP
Location
Primary Clinic
Location
Address_1
Address
Address_2
City
City
State
State
Location
Provider_Employer_
Name
EIN
Clinic_NPI
Specialty
SystemName1
11-2222222
9876541320 PCP
SystemName 2
22-3333333
7654321071 PCP
Location
Address
City
State
SystemName 2
22-3333333
7654321071 SPE
ClinicName
Address
City
State
SystemName1
11-2222222
5432102101 PCP
Appendix D: Minnesota Accountable Communities for Health Continuum of Accountability Matrix Assessment Tool
Minnesota Accountable Health Model: Continuum of Accountability Assessment Tool
The Minnesota Accountable Health Model is working to support organization’s participation in accountable care models in order to achieve the vision of
the Triple Aim: improved consumer experience of care, improved population health, and lower per capita health care costs. This tool is designed to help
organizations assess where they are now in achieving the basic capabilities, relationships, and functions they need to have in place in order to achieve
these goals, and to provide guideposts that will allow them to track their progress as they continue to evolve in their work.
At the State level, the Minnesota Department of Health (MDH) and Department of Human Services (DHS) will use this tool to better understand SIMMinnesota participants (grantees, TA recipients, Accountable Communities for Health, and others) status in achieving the goals of the Minnesota
Accountable Health Model, what supports are needed from SIM-Minnesota to achieve the goals, and how we may be able to provide additional tools or
resources. An organization's self-assessment will NOT be used to make funding decisions; rather, this tool will be used to help us develop targets and
goals for participating organizations, and to assess their progress.
In this document, the terms ‘organization’ and ‘provider’ are meant to include a broad range of health and health care providers and support services
providers that may or may not formally be part of an existing ACO, but that are moving towards greater accountability for quality, cost of care and
health of the populations they serve. Many types of organizations, including not only providers of medical care but also organizations that operate in
the behavioral health, social services, local public health, long term care/post-acute care settings, community organizations, and other public/private
sector partners that provide supportive services to individuals and families, can all have a role in convening, leading or participating in these models.
While there are multiple examples of how an organization may achieve the goals of the Minnesota Accountable Health Model, this assessment tool
describes the components necessary to demonstrate movement toward this long-term vision. As you work through this assessment, remember that:
•
Organizations or partnerships may be at different levels of development on different issues.
•
It is not necessary for an organization to have achieved capabilities in all areas in order to be eligible for support or technical assistance under
the Minnesota Accountable Health Model. The goal is to help organizations or providers move onto this grid, or move further to the right, in as
many areas as possible.
•
Organizations may move along this continuum at different rates and use different approaches.
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
1
Directions:
This assessment is designed to help organizations understand where they are on the continuum of Minnesota’s Accountable Health Model. The results
will help identify areas for improvement, and track changes over time.
Instructions:
1. Each facility or physical site should complete an assessment (e.g., a practice, clinic, hospital, organization, or provider).
2. Fill out the organization’s name, date it is being completed, name of individual(s) completing the assessment tool and their title(s).
3. For each question, select the level that best represents your organization, and within that level choose the appropriate response by checking the
box: Beginning, In-Progress, Mostly Done. In some cases you may be in more than one level and therefore can select responses for each level.
4. A glossary of terms and resources can be found at the end of the document. Not all terms may apply to all providers or organizations.
5. If you determine that you have not yet met Level A requirements for a particular row (i.e. you are at the ‘pre-level’ for that capability), check the
pre-level box.
6. If you determine that you have fully met the expectations for a certain level within a row, move to the next level.
7. Use comment fields at the end of each section to provide additional information or context as needed.
8. Save and print a copy of this assessment for your records when you are finished.
Within each level you should choose where your organization is in implementing:
Beginning – your organization is at the initial stages of implementing this process or activity
In Progress – your organization is moving forward and making steady advances toward the goal of full implementation
Mostly done – your organization is generally complete in implementing this process or activity
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
2
Name of Organization: Click here to enter text.
Date: Click here to enter text.
Name of person completing form: Click here to enter text.
Title of person completing form: Click here to enter text.
If more than one person, add info here: Click here to enter text.
Model Spread and Multi-Payer Participation Section
1. What type of payment arrangements do you participate in?
Pre-Level
We only receive
payment for delivered
services in the form of
fee-for-service or
capitation payments
without any incentives.
☐
Level A
We have alternative
types of payment
arrangements with at
least one payer that
represents less than
20% of our total
consumer base, OR
participation in at least
one performance-based
or value-based
incentive system
representing less than
5% of our total
revenue.
Level B
We have alternative
types of payment
arrangements with at
least one payer that
represents 20% to 50%
of our total consumer
base, OR participation
in at least one
performance-based or
value-based incentive
system representing 5%
to 15% of our total
revenue.
Level C
We have alternative
types of payment
arrangements with at
least one payer that
represents 50% to 75%
of our total consumer
base, OR participation
in a performance-based
or value-based
incentive system
representing 15% to
30% of our total
revenue.
Level D
We have alternative
types of payment
arrangements with at
least one payer that
represents greater than
75% of our total
consumer base, OR
participation in a
performance-based or
value-based incentive
system representing
greater than 30% of our
total revenue.
☐
☐
☐
☐
Briefly describe any alternative payment arrangements you participate in.
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
3
Payment Transformation Section
2. What types of alternatives to fee-for-service (FFS) payment arrangement(s) do you participate in? Select the level that best represents your
organization, and within that level choose the appropriate response by checking the box.
Pre-Level
We only receive
payment for delivered
services in the form of
fee-for-service without
any incentives.
☐Beginning
☐In progress
☐Mostly done
Level A
We have little or no
readiness to manage
global costs, but may
be willing to assume
fixed payment for some
ancillary services.
Examples include:
Health care home or
similar coordination
fees, quality
improvement/incentive
payments.
Level B
We are ready to
manage global costs
with upside risk. We
participate in shared
savings or similar
arrangement with both
cost and quality
performance with some
payers; may have some
financial risk (e.g.
episode-based
payments).
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level C
We are ready to
manage global cost
with upside and
downside risk. We
participate in shared
savings and some
arrangements moving
toward risk sharing
through Total Cost of
Care or partial to full
capitation for certain
activities; may include
savings reinvestments
and/or payments to
community partners
not directly employed
by the contracting
organization.
Level D
We are ready to accept
global capitation
payments. Community
partners are sharing in
accountability for cost,
quality and population
health are included in
the financial model in
some form.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Enter any comments you have about Payment Transformation:
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
4
Delivery and Community Integration and Partnership Section
3. Population Management: To what extent does your practice have a process to identify appropriate patients/clients for care coordination? Select
the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐None
Level A
We do not currently
have a process in place
but are planning or
beginning to implement
this.
☐Beginning
☐In progress
☐Mostly done
Level B
We have an informal
process where care
team members and
providers identify
patients/clients for care
coordination.
☐Beginning
☐In progress
☐Mostly done
Level C
We routinely assess
patients’/clients’ needs
for care coordination
using methods such as
pre-visit planning, use
of registries and team /
provider input.
☐Beginning
☐In progress
☐Mostly done
Level D
We systematically
assess the
patient/client
population for care
coordination needs
with use of data or
screening tools, such as
population based
registry and community
or payer data on a
regular basis.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
5
4. Care Coordination: To what extent are external care coordinators or care managers identified and collaborative integrated relationships
developed? Select the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ None
Level A
We have internal care
coordination or
management (within
clinics, services or colocated) where
patients/clients and
families have direct
involvement in
establishing patient
centered goals.
☐Beginning
☐In progress
☐Mostly done
Level B
We regularly ask our
patients/clients if they
have external care
coordinators or
managers by service
provider. Names of
external care
coordinators or
managers and other
service providers such
as specialists, or schools
are included on the
patients’/clients’ care
plan and staff members
communicate across
locations with
patient/client and
family as partners.
☐Beginning
☐In progress
☐Mostly done
Level C
We have developed
collaborative
relationships with
external care
coordinators or
managers, and
appropriate
components of external
care plans are
incorporated into the
patients’/clients’ care
plan and families
understand who is
involved in their care
and participate as
partners.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
External care managers
(including health plan
case managers), care
coordinators, and
patients/clients and
families are working
together in partnership
in a patient centered,
coordinated care
environment. Roles are
defined,
communication
systems are in place
and information is
shared and updated in
a shared care plan.
There is integration on
all levels of care
coordination.
☐Beginning
☐In progress
☐Mostly done
6
5. Team Based Work: To what extent has your organization addressed how team members implement work functions as a team? Select the level
that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐None
Level A
Our organization
defines who is on the
team, identifies roles
and functions of team
members.
☐Beginning
☐In progress
☐Mostly done
Level B
Our organization has
actively worked to
define and reorganize
roles and
responsibilities in teambuilding based services
including the
patient/client and
family (clients) as an
active partner on the
team.
☐Beginning
☐In progress
☐Mostly done
Level C
Our organization has
redesigned roles and
responsibilities and
established trusting
relationships among
team members that
allow team members to
function at the top of
their license, education
or scope of work.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
Our organization is
actively working to
integrate teams with
defined roles and
responsibilities broadly
with a range of services
beyond a single
provider organization.
☐Beginning
☐In progress
☐Mostly done
7
6. Referral Processes: To what extent are referrals documented, tracked for participation and does the referring provider know the results of the
referral? Select the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ We do not make
referrals to providers or
community resources.
Level A
Our referral system is
informal and staff
generally has limited
knowledge of referral
resources.
☐Beginning
☐In progress
☐Mostly done
Level B
Our referral system is
somewhat formal and
involves providing
patients/clients with
contact information for
referral resources
however this does not
include follow up.
☐Beginning
☐In progress
☐Mostly done
Level C
Our referral processes
are established.
Referrals are made to
providers or to
community resources
and there is a record
maintained of the
referral, whether and
when the patient/client
was seen, and the
result of the referral.
☐Beginning
☐In progress
☐Mostly done
Level D
Our referral process is
formal, well
established, referrals
are completed in
partnership with the
patient/client, and
includes follow up with
the patient/client and
referred entity. Data is
systematically collected
on referrals and used
for data analytics such
as quality
improvement. There is
ongoing problem
solving with referral
resources.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
8
7. Transitions Planning: To what extent is there a formal process for transitioning patients/clients to or from another provider or organization?
Select the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ None
Level A
We have an informal
process and it is not
done systematically.
☐Beginning
☐In progress
☐Mostly done
Level B
Our process is wellestablished for some
but not all transitions in
care provider(s).
Assistance is provided
on an as-needed basis
in response to requests
from patient/client
and/or family.
☐Beginning
☐In progress
☐Mostly done
Level C
Our process is wellestablished for most
care provider
transitions, and
includes post-transition
follow-up with
patients/clients and
caregivers.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
Our process is wellestablished for
transitions between all
usual care providers,
and care givers. The
EHR provides prompts
and templates for
health care transition
activities.
☐Beginning
☐In progress
☐Mostly done
9
8. Transitions Communication: Is there care transitions communication? Select the level that best represents your organization, and within that level
choose the appropriate response by checking the box.
Pre-Level
☐ It is not done
systematically.
Level A
Our communication on
care transitions and
expectations are
variable and dependent
on each individual
provider’s interest and
usual practice.
☐Beginning
☐In progress
☐Mostly done
Level B
We inform
patient/client or care
giver to call the
provider with
questions. Team
communicates with
patients/clients or care
givers when there are
requests for
information, but there
is not deliberate followup.
☐Beginning
☐In progress
☐Mostly done
Level C
We have implemented
standardized methods
to assess patient’s
transition. There is
monitoring of
communication
between providers,
scheduling follow up
appointments by
protocol. There may be
some difficulty
transferring and / or
obtaining service
records for continued
care.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We have ongoing
communication by
skilled team members
that includes written
goal setting and care
planning with the
patient/client and care
giver regarding the
transition with
information and
resources. There is
minimal difficulty
transferring and / or
obtaining service
records for continued
care.
☐Beginning
☐In progress
☐Mostly done
10
9. Quality Improvement: To what extent does your practice have quality improvement (QI) processes in place? Select the level that best represents
your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ None
Level A
We have established a
quality improvement
team that can measure
data, and has a
structured quality
improvement process
in place.
☐Beginning
☐In progress
☐Mostly done
Level B
Our quality
improvement team
meets regularly and
includes operations
staff. It has a welldeveloped quality
improvement plan that
includes the triple aim
(clinical, patient/client
experience and cost).
There is a mechanism in
place for input and
feedback on quality
metrics.
Level C
We are transparent in
how quality data is
shared with providers
and team members,
and an environment of
team collaboration in
addressing quality
results, including direct
input from consumers
and partners.
Level D
Our administrative
team and providers are
held accountable for
quality improvement,
through regular
performance
assessments linked to
QI goals or targets, and
possibly individual
compensation.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
11
10. Training: To what extent does your organization provide access to trainings and other resources on, effective, sustainable communication for care
integration? Select the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ None
Level A
We have limited
training for our staff.
☐Beginning
☐In progress
☐Mostly done
Level B
We have training
available to our staff
and it is formally
promoted by our
leadership.
☐Beginning
☐In progress
☐Mostly done
Level C
We have training widely
available to our staff. It
is utilized/modeled by
our leadership, and is
required by our
policies.
☐Beginning
☐In progress
☐Mostly done
Level D
Our training is widely
used in an interprofessional team or
integrated work team.
☐Beginning
☐In progress
☐Mostly done
11. Community Resources: To what extent do you have knowledge of community agencies and resources within the area you serve or have
developed partnerships? Select the level that best represents your organization, and within that level choose the appropriate response by checking
the box.
Pre-Level
☐ None
Level A
We have limited
knowledge or working
relationships with
community resources
or agencies.
Level B
We make referrals to
community resources
but have limited
knowledge of how they
operate.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level C
We have established
mutually beneficial
community
partnerships for
referrals and we work
actively with partners in
problem solving and
communications.
Level D
We have formalized
partnerships supported
by an infrastructure
where partners plan
together, measure
outcomes together and
share information
together.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
12
12. Culturally Appropriate Care Delivery: To what extent is the care delivered sensitive to values, customs and cultures of individuals? Select the level
that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ Not at all
Level A
We have a basic
understanding of the
cultural needs of
people receiving care or
services.
☐Beginning
☐In progress
☐Mostly done
Level B
We address the needs
of individuals receiving
services or care by
providing interpreter
services, culturally
specific educational
materials, and staff
training on providing
culturally appropriate
services.
☐Beginning
☐In progress
☐Mostly done
Level C
We collect cultural
background, racial
heritage and primary
language information in
a systematic way and
use this information in
providing care delivery
or services.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We use demographic
data such as race,
language and ethnicity
for our patient/client
population to address
disparities.
☐Beginning
☐In progress
☐Mostly done
13
13. Emerging Workforce Roles: Does your organization employ emerging professionals (including but not limited to, community health workers,
community paramedics, dental therapists)? Select the level that best represents your organization, and within that level choose the appropriate
response by checking the box.
Pre-Level
☐ We have never
considered, or may be
non-applicable to
service.
Level A
We are interested in,
have done initial
research and have
begun the planning
process to integrate
one or more of these
roles into our service
delivery model.
☐Beginning
☐In progress
☐Mostly done
Level B
We’ve considered and
we are redesigning
current team member
work roles at this time
to implement or we’re
considering bringing on
a new role.
☐Beginning
☐In progress
☐Mostly done
Level C
We’ve been
implementing but are
still unsure if new skills
and time are being
utilized effectively.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We have employed
“emerging
professionals” for some
time and we
understand how to
ensure that new skills
and time are utilized
efficiently.
☐Beginning
☐In progress
☐Mostly done
14
14. Patient and Family Centered Care: To what extent has your practice implemented principles of patient and family centered care (that includes
family values and preferences)? Select the level that best represents your organization, and within that level choose the appropriate response by
checking the box.
Pre-Level
☐ None
Level A
We have included these
principles as part of our
organization’s vision
and mission statement.
☐Beginning
☐In progress
☐Mostly done
Level B
These principles are a
key priority for our
organization and are
included in training and
orientation.
☐Beginning
☐In progress
☐Mostly done
Level C
We include these
principles in job
descriptions and
performance metrics
for all staff and
providers and
incorporate into
planning and
organization of care.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We consistently and
systematically use
these principles to
guide organization
changes, plan care
delivery and measure
system performance. It
is consistently
demonstrated in care
or services interactions
at the person and
organization level.
☐Beginning
☐In progress
☐Mostly done
15
15. Patient Centered Care: To what extent is input solicited from patients/clients for organizational improvement activities? Select the level that best
represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ None
Level A
We have an informal
process in place
collecting patient/client
input.
☐Beginning
☐In progress
☐Mostly done
Level B
We regularly solicit
patient/client input
through patient/client
experience surveys and
results are shared with
clinic teams and acted
on.
☐Beginning
☐In progress
☐Mostly done
Level C
We receive frequent
input from
patients/clients and
families using survey
methods, point of care
information, focus
groups or participation
on patient/client
advisory groups; results
are shared with clinic
teams and acted on.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We receive frequent
and actionable input
from patients/clients
and families who
participate on
interdisciplinary clinic
level quality
improvement teams to
provide input into
quality improvement.
☐Beginning
☐In progress
☐Mostly done
16
16. Self-Management Support: To what extent are patients/clients provided support in self-management and decision making? Select the level that
best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ None
Level A
We provide limited selfmanagement by
distributing educational
materials (e.g.,
pamphlets, booklets,
web pages);
information is usually
suggested to
patients/clients and
families without
discussions.
☐Beginning
☐In progress
☐Mostly done
Level B
Providers and/or staff
members, such as a
health educator or peer
coach, provide
patients/clients with
education information.
We often make
referrals to selfmanagement classes or
educators with limited
instruction, referral, or
follow up.
☐Beginning
☐In progress
☐Mostly done
Level C
We provide selfmanagement support
by goal setting and
action planning with
members of our service
team. Evidence based
documents for shared
decision making are
used by team members
or we make referrals to
an established partner.
☐Beginning
☐In progress
☐Mostly done
Level D
We provide selfmanagement support
systematically
supported and provided
by members of our
trained service team in
patient empowerment,
motivational
interviewing
techniques, problem
solving methods and
decision making
techniques. Shared
decision making with
decision aids activities
are tracked and
evaluated through QI
processes.
☐Beginning
☐In progress
☐Mostly done
Enter any comments you have about delivery and Community Integration and Partnership:
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
17
Infrastructure to Support Shared Accountability Organizations Section
17. Infrastructure: To what extent has your organization participated in establishing governance for managing business, legal and financial
arrangements with partnering organization? Select the level that best represents your organization, and within that level choose the appropriate
response by checking the box.
Pre-Level
☐ We do not have any
partnerships or
relationships at this
time.
Level A
We have identified
partners and have
begun the planning
process for establishing
formal business
relationships.
☐Beginning
☐In progress
☐Mostly done
Level B
We and our partners
have established an
oversight body (a group
of individuals
representing the
partners) to set a
vision, strategic and
business plans, and
data sharing
agreements that meet
regularly.
☐Beginning
☐In progress
☐Mostly done
Level C
Our governing body has
established a formal
legal structure that
includes the strategic
and business plans and
is overseeing the
implementation of the
plans, approving annual
budgets, monitoring
financial and
operational
performance, sharing
some aspects of
financial gain/risk and
related activities.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
Our governing body
actively responds to
changes in the
marketplace,
reimbursement rates
and policy to ensure
sustainability of the
partnerships. Key
aspects of our
governance assure that
our communities are
represented.
☐Beginning
☐In progress
☐Mostly done
18
18. Governing Body: To what extent does your governing body represent the composition of your community? Select the level that best represents
your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ No formal governing
body exists
Level A
No formal governing
body exists, but
stakeholder groups are
convened based on
input from the
community.
☐Beginning
☐In progress
☐Mostly done
Level B
A standing membership
list based on role is
created to advise the
organization.
☐Beginning
☐In progress
☐Mostly done
Level C
Governing body
composition is
representative of the
community served,
patient family
representatives,
providers, payers,
behavioral health social
services, local public
health, and education.
Formal composition is
proposed.
Level D
Governing body
composition is
representative of the
community served,
patient family
representatives,
providers, payers,
behavioral health social
services, local public
health, and education.
Composition is formally
defined.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Enter any comments you have about Infrastructure to Support Shared Accountability:
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
19
Health Information Technology Capabilities Section
19. Indicate your practice’s implementation of an electronic health record (EHR) system or similar interoperable information system (not including
stand-alone practice management systems). Select the level that best represents your organization, and within that level choose the appropriate
response by checking the box.
Pre-Level
☐ We are not yet
using or planning for
an HER.
(Skip to question 31)
Level A
We do not use an EHR
but are in the planning
and/or implementation
process.
Level B
We have an EHR in use
for 1%-50% of staff and
providers at our
practice.
Level C
We have an EHR in use
for 51%-80% of staff
and providers at our
practice.
Level D
We have an EHR in use
for more than 80% of
staff and providers at
our practice.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
20. What is the name of the EHR software you use or plan to use? Click here to enter text.
21. To what extent does your practice use your EHR for Computerized Provider Order Entry (CPOE)? Select the level that best represents your
organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ Our practice does
not enter orders.
Level A
We do not use our EHR
for CPOE but are in the
planning and/or
implementation
process.
Level B
The CPOE function is
enabled and in use as
part of workflow for
1%-50% of provider
orders.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level C
We use CPOE for 51%80% of provider orders.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We use CPOE for more
than 80% of provider
orders.
☐Beginning
☐In progress
☐Mostly done
20
22. To what extent does your practice use your EHR for clinical decision support tools, such as: reminders; care plans and flow sheets; guidelines
based on conditions specific to the patient/ client or condition? Select the level that best represents your organization, and within that level choose
the appropriate response by checking the box.
Pre-Level
☐ Our practice is not
yet using or planning to
use clinical decision
support tools.
Level A
We do not use clinical
decision support tools
in our EHR but are in
the planning and/or
implementation
process.
☐Beginning
☐In progress
☐Mostly done
Level B
We use the clinical
decision support tools
in our EHR for 1%-50%
of our patients/clients
who need it.
Level C
We use the clinical
decision support tools
in our EHR for 51%-80%
of our patients/clients
who need it.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level D
We use the clinical
decision support tools
in our EHR for more
than 80% of our
patients/clients who
need it.
☐Beginning
☐In progress
☐Mostly done
23. To what extent does your practice use your EHR for summary care records? Select the level that best represents your organization, and within that
level choose the appropriate response by checking the box.
Pre-Level
☐ Our practice is not
yet using or planning to
use summary care
records.
Level A
We do not use the EHR
to create summary care
records but are in the
planning and/or
implementing process.
☐Beginning
☐In progress
☐Mostly done
Level B
We use the EHR to
create summary care
records for 1%-50% of
our patients/clients.
Level C
We use EHR to create
summary care records
51%-80% of our
patients/clients.
Level D
We use the EHR to
create summary care
records more than 80%
of our patients/clients.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
21
24. To what extent does your practice electronically track patient/client consent to release health information using your EHR? Select the level that
best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ Our practice is not
yet using or planning to
use the EHR or a Health
Information Exchange
Service Provider (HIESP)
to electronically
manage patient/client
consent.
Level A
We do not currently
use the EHR or a HIESP
to electronically
manage patient/client
consent but are in the
planning and/or
implementation
process.
Level B
We use our EHR or a
HIESP to manage
consent for 1%-50% of
our patients/clients.
Level C
We use the EHR or a
HIESP to manage
consent for 51%-80% of
our patients/clients
Level D
We use the EHR or a
HIESP for more than
80% of our
patients/clients.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
25. How does your practice use your EHR to monitor immunization information for your patients/ clients?(For example, accessing the Minnesota
Immunization Information Connection to review patients’ past vaccination to ensure proper administration for next does or getting alerts or
reminders for vaccines). Select the level that best represents your organization, and within that level choose the appropriate response by checking
the box.
Pre-Level
☐ Our practice is not
yet using or planning to
monitor immunization
information for our
patients/ clients using
the EHR.
Level A
We do not monitor
immunization
information.
☐Beginning
☐In progress
☐Mostly done
Level B
We do not use the EHR
to monitor
immunizations but are
in the planning and/or
implementing process.
☐Beginning
☐In progress
☐Mostly done
Level C
We use the EHR to
monitor immunizations
for 1%-50% of
patients/clients.
Level D
We use the EHR to
monitor immunizations
for 51%-80% of
patients/clients.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
22
26. How does your practice use data from your EHR for quality improvement? E.g. reporting to the State of Minnesota and/or payers, not including
billing? Select the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ Our practice is not
yet using or planning to
use data from the EHR
system for quality
improvement.
Level A
We do not currently
use data from the EHR
for quality
improvement but are in
the planning and/or
implementing process.
Level B
We use data from the
EHR to measure
internal quality
improvement, such as
to create benchmarks,
goals or priorities.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level C
We use data from the
EHR to support
improving the quality of
our care delivery.
Level D
We use data from the
EHR to improve health
outcomes for our
patients/clients.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Enter any comments you have about Health Information Technology:
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
23
Health Information Exchange Capabilities Section
27. How does your practice electronically exchange clinical information with other organizations (e.g., lab or test results, care plans)? This does not
include using fax or unsecure e-mail. Select the level that best represents your organization, and within that level choose the appropriate response
by checking the box.
Pre-Level
☐ Our practice is not
yet using or planning to
exchange health
information
electronically.
Level A
We do not currently
exchange health
information
electronically but are in
the planning and/or
implementing process
(e.g., identifying use
cases).
Level B
We electronically push
(send) information (i.e.,
test results, care plan)
to affiliated
organizations (e.g.,
practicing within the
same health system).
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level C
Level C
We electronically push
(send) information (i.e.,
test results, care plan)
to unaffiliated
organizations (e.g., not
practicing within the
same health system).
Level D
We electronically pull
(query) information
from organizations.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
28. To what extent does your practice electronically exchange a patient’s summary of care record, or similar documentation such as a discharge
summary or transfer form that has information for continuity of care to other settings or providers? This does not include using fax or unsecure
email. Select the level that best represents your organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ Our practice is not
yet exchanging or
planning to exchange
the summary care
record.
Level A
We are not
electronically
exchanging the
summary care records
but are in the planning
and/or implementing
process.
☐Beginning
☐In progress
☐Mostly done
Level B
We electronically
exchange the summary
care records for 1%50% of patients/ clients
who require transition,
referral or sharing with
another provider.
Level C
We electronically
exchange the summary
care records for 51%80% of patients/ clients
who require transition,
referral or sharing with
another provider.
☐Beginning
☐Beginning
☐In progress
☐In progress
☐Mostly done
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Level D
We electronically
exchange the summary
care records for more
than 80% of patients/
clients who require
transition, referral or
sharing with another
provider.
☐Beginning
☐In progress
☐Mostly done
24
29. To what extent does your practice electronically prescribe non-controlled substances? Select the level that best represents your organization, and
within that level choose the appropriate response by checking the box.
Pre-Level
☐ We do not prescribe
medications.
Level A
We do not e-prescribe
but are beginning the
planning and/or
implementation
process.
☐Beginning
☐In progress
☐Mostly done
Level B
Use for 1%-50% of
prescriptions for noncontrolled substances.
Level C
Use for 51%-80% of
prescriptions for noncontrolled substances.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level D
Use for more than 80%
of prescriptions for
non-controlled
substances.
☐Beginning
☐In progress
☐Mostly done
30. To what extent does your practice electronically prescribe controlled substances? Select the level that best represents your organization, and
within that level choose the appropriate response by checking the box.
Pre-Level
☐ We do not prescribe
medications.
Level A
We do not e-prescribe
but are beginning the
planning and/or
implementation
process.
☐Beginning
☐In progress
☐Mostly done
Level B
Use for 1%-50% of
prescriptions for
controlled substances
Level C
Use for 51%-80% of
prescriptions for
controlled substances
Level D
Use for more than 80%
of prescriptions for
controlled substances
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
31. Are you currently using an electronic system such as a practice management system or computerized database to manage patient/client
☐ Yes
☐ No
information? These do not include billing systems.
32. Describe your practice’s plans for implementing an EHR, including expected timeframes for planning to actively use the EHR, needs, and expected
barriers. Click here to enter text.
Enter any comments you have about Health Information Exchange:
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
25
Data Analytics Capabilities Section
33. How does your practice approach the topic of data analysis and organization of information? Select the level that best represents your
organization, and within that level choose the appropriate response by checking the box.
Pre-Level
☐ Our practice does
not have a strategy for
managing information.
Level A
We are beginning to
organize information
about patients when
specific needs or
questions arise using
tools such as
spreadsheets or simple
databases.
Level B
We are establishing
common and reliable
source(s) of
information to
understand our
patients/clients and
inform practice
decisions.
☐Beginning
☐In progress
☐Mostly done
☐Beginning
☐In progress
☐Mostly done
Level C
We have begun to
coordinate or integrate
data from multiple
sources including
clinical and financial.
☐Beginning
☐In progress
☐Mostly done
Level D
We have a robust data
strategy and reliable
data sources to inform
practice decisions. Our
practice has established
data warehouse(s) and
analysis software that
can aggregate
information from
multiple sources,
including external data
sources.
☐Beginning
☐In progress
☐Mostly done
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
26
34. How is information used by your practice? Select the level that best represents your organization, and within that level choose the appropriate
response by checking the box.
Pre-Level
☐ Our practice is
primarily paper based.
Level A
We can view and easily
use information about
an individual
patient’s/client’s
history to identify risk
factors.
☐Beginning
☐In progress
☐Mostly done
Level B
We use information
across patient/client
populations to prepare
descriptive reports
about our common
conditions, services or
costs.
☐Beginning
☐In progress
☐Mostly done
Level C
Our practice uses data
to inform strategies or
establish clinical or
financial targets. We
can analyze information
from ancillary providers
and major partners to
allow patient risk
profiling, provider
assessment, and
analysis of defined
subpopulations
(patients by chronic
status, race/ethnicity,
compliance level, etc.).
We have dedicated
staff whose primary
responsibilities include
interpreting and
understanding our
data.
☐Beginning
☐In progress
☐Mostly done
Level D
We use data to
understand our
population and how it
compares to similar or
related practices. We
regularly update
information to
understand how our
population and costs
are changing. Data is
used for predictive or
prescriptive analysis.
We are beginning to
work with community
partners to identify
opportunities to engage
community resources
to manage
subpopulations with
specific needs
(engagement of
behavioral health/social
service, emerging
public health threat,
etc.).
☐Beginning
☐In progress
☐Mostly done
Enter any comments you have about Data Analytics Capabilities:
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
27
Conclusion
For e-Health collaboratives or ACHs: If you are submitting an assessment for a collaborative or partnership (in addition to individual assessments for
participating organizations), please describe the process you used to collectively complete the form and which organizations contributed.
Please provide any general comments or additional feedback.
Glossary
Care Coordination is a function that supports information-sharing across providers, patients, types and levels of service, sites and time frames. The goal
of coordination is to ensure that patients’ needs and preferences are achieved and that care is efficient and of high quality. Care coordination is most
needed by persons who have multiple needs that cannot be met by a single clinician or by a single clinical organization, and which are ongoing, with
their mix and intensity subject to change over time. Source: US. Department of Health and Human Services, Meaningful Measures of Care Coordination,
NCVHS, http://www.ncvhs.hhs.gov/091013p9.pdf
Care Coordinator is a person who has primary responsibility to organize and coordinate care and services for clients/patients served in a variety of
settings, e.gl health care homes, behavioral health clinics, acute care settings and so on.
Care Manager is a person who has primary responsibility to organize and coordinate care based on a set of evidence-based, integrated clinical care
activities that are tailored to the individual patient, and that ensure each patient has his or her own coordinated plan of care and services.
Care Plan is the structure used to define the management actions for the various conditions, problems, or issues. A care plan must include at a minimum
the following components: problem (the focus of the care plan), goal (the target outcome) and any instructions that the provider has given to the
patient. A goal is a defined target or measure to be achieved in the process of patient care (an expected outcome).
Clinical Decision Support (CDS) refers broadly to providing clinicians or patients with clinical knowledge and patient-related information, intelligently
filtered or presented at appropriate times, to enhance patient care.
Computerized Provider Order Entry (CPOE) is a computer application that allows a physician's orders for diagnostic and treatment services (such as
medications, laboratory, and other tests) to be entered electronically instead of being recorded on order sheets or prescription pads. The computer
compares the order against standards for dosing, checks for allergies or interactions with other medications, and warns the physician about potential
problems.
Data Analytics-is the systematic use of data and related business insights to drive fact-based decision making for planning, management, measurement
and learning. Analytics may be descriptive, predictive or
prescriptive. http://www.ibm.com/smarterplanet/global/files/the_value_of_analytics_in_healthcare.pdf
28
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
Electronic Health Record (EHR) is a real-time patient health record with access to evidence-based decision support tools that can be used to aid
clinicians in decision-making. The EHR can automate and streamline a clinician's workflow, ensuring that all clinical information is communicated. It can
also prevent delays in response that result in gaps in care. An EHR requires the capacity that information be interoperable, or able to send information
electronically to other providers within and outside of the treatment setting. The EHR can also support the collection of data for uses other than clinical
care, such as billing, quality management, outcome reporting, and public health disease surveillance and reporting. EHR is considered more
comprehensive than the concept of an Electronic Medical Record (EMR) or Practice Management System (PMS).
Emerging professionals- include Community Health Workers, Community Paramedics, Dental Therapists and Advanced Dental Therapists, with possible
future inclusion of other practitioners such as Doulas and Certified Peer Support Specialists
e-prescribing means secure bidirectional electronic information exchange between prescribers (providers), dispensers (pharmacies), Pharmacy Benefits
Managers, or health plans, directly or through an intermediary network. E-prescribing encompasses exchanging prescriptions, checking the prescribed
drug against the patient’s health plan formulary of eligible drugs, checking for any patient allergy to drug or drug-drug interactions, access to patient
medication history, and sending or receiving an acknowledgement that the prescription was filled.
Health information exchange or HIE means the electronic transmission of health related information between organizations according to nationally
recognized standards. Health information exchange does not include paper, mail, phone, fax, or standard/regular email exchange of information.
Integrated care covers a complex and comprehensive field and there are many different approaches to and definitions of the concept. One overarching
definition (Grone, O. and Garcia-Barbero, M. 2002)is integrated care is a concept bringing together inputs, delivery, management and organization of
services related to diagnosis, treatment, care, rehabilitation and health promotion. Integration is a means to improve services in relation to access,
quality, user satisfaction and efficiency.
Interoperabililty: The ability of two or more information systems or components to exchange information and to use the information that has been
exchanged accurately, securely, and verifiably, when and where needed. Reference: ehealth Initiative, http://www.ehealthinitiative.org/
Interprofessional Team: As defined in the Institute of Medicine’s (IOM) Report, Health Professions Education: A Bridge to Quality, (2003) an
interdisciplinary (Interprofessional) team is “composed of members from different professions and occupations with varied and specialized knowledge,
skills, and methods.” (p. 54) Members of an Interprofessional team communicate and work together, as colleagues, to provide quality, individualized
care for patients. Texas Tech University, Interprofessional Teamwork, http://www.ttuhsc.edu/qep/teamwork.aspx
Patient and Family Centered Care means planning, delivering, and evaluating health care through patient-driven, shared decision-making that is based
on participation, cooperation, trust, and respect of participant perspectives and choices. It also incorporates the participant's knowledge, values, beliefs,
and cultural background into care planning and delivery. Patient and family-centered care applies to patients of all ages.
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
29
Push: This is a secure sending of information between two known entities with an established business relationship, such as a primary care provider and
a specialist. These types of transactions typically relate to routine workflow and processes. A non-health care example of a push transaction would be
sending an email.
Pull: This is a secure accessing of information that involves a query and a response. The query is the request for information about a patient, and the
response is the retrieval of clinical information on the patient or information on where the clinical data can be found. For example, conducting a Google
web search is a non-health care example of a pull transaction.
Summary of Care Record– a summary of care record may include the following elements:
• Patient name
• Care team including the primary care provider of record and any
additional known care team members beyond the referring or
• Referring or transitioning provider's name and office contact
transitioning provider and the receiving provider
information
•
Current problem list (a list of current, active and historical
• Vital signs (height, weight, blood pressure, BMI)
diagnoses)
• Smoking status
•
Current medication list (a list of medications that a given patient
• Functional status, including activities of daily living, cognitive and
is currently taking), and
disability status
• Current medication allergy list (a list of medications to which a
• Care plan field, including goals and instructions
given patient has known allergies)
• Procedures
•
Diagnosis lists
• Encounter diagnosis
• Advance directives
• Immunizations
• Contact information; guardianship information
• Laboratory test results
• Critical incident information relating to physical and/or
• Demographic information (preferred language, sex, race,
mental/behavioral health
ethnicity, date of birth)
• Reason for referral
Teamwork is defined as the interaction and relationships between two or more health professionals who work interdependently to provide safe, quality
patient care. Teamwork includes the interrelated set of specific knowledge (cognitive competencies), skills (affective competencies), and attitudes
(behavioral competencies) required for an interprofessional team to function as a unit (Salas, DiazGranados, Weaver, and King, 2008).
Resources:
Transitions of Care: The movement of a patient from one setting of care (hospital, ambulatory primary care practice, ambulatory specialty care practice,
long-term care, home health, rehabilitation facility) to another. CMS, EHR incentive program, Meaningful Use Menu, http://www.cms.gov/Regulationsand-Guidance/Legislation/EHRIncentivePrograms/downloads/8_Transition_of_Care_Summary.pdf
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
30
Care Integration: Evidence shows that this is the most effective component for providing team based/ integrated care. (SAMSHA-HRSA, 2013; Thielke, et
al, 2007) Standard Framework for Levels of Integrated Healthcare, SAMHSA, http://www.integration.samhsa.gov/integrated-caremodels/A_Standard_Framework_for_Levels_of_Integrated_Healthcare.pdf
ACO-Governance: How-to Manual for Physicians, AMA, http://www.ama-assn.org/resources/doc/psa/physician-how-to-manual.pdf
Minnesota Accountable Health Model – SIM Minnesota
Formatting updates: February 2016
31
 for Qualified Grantee(s)")