Effect of radiographic techniques „kVp and mAs… on image quality
advertisement

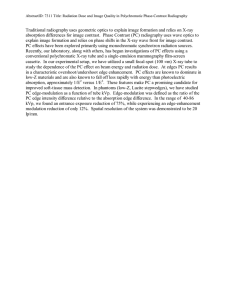
Effect of radiographic techniques „kVp and mAs… on image quality and patient doses in digital subtraction angiography Nikolaos A. Gkanatsiosa) Department of Radiology, University of Florida, P.O. Box 100374, Gainesville, Florida 32610 Walter Huda Department of Radiology, SUNY Upstate Medical University, Syracuse, New York 13210 Keith R. Peters Department of Radiology, University of Florida, P.O. Box 100374, Gainesville, Florida 32610 共Received 10 January 2002; accepted for publication 17 May 2002; published 16 July 2002兲 We investigated how varying the x-ray tube voltage and image receptor input exposure affected image quality and patient radiation doses in interventional neuroradiologic imaging. Digital subtraction angiography 共DSA兲 images were obtained of a phantom with 1 mm diameter vessels containing iodine at concentrations between 4.5 and 50 mg/cc. The detection threshold concentration of iodine was determined by inspecting DSA images obtained at a range of x-ray tube voltages and input exposure levels. Surface doses were obtained from measured x-ray tube output data, and corresponding values of energy imparted were determined using the exposure-area product incident on the phantom. In one series of experiments, the air kerma at the image intensifier (X) was varied between 0.44 Gy per frame and 8.8 Gy per frame at a constant x-ray tube voltage of 70 kVp. In a second series of experiments, the tube voltage was varied between 50 and 100 kVp, and the mAs adjusted to maintain a constant exposure level at the input of the image intensifier. At a constant x-ray tube voltage, the surface dose and energy imparted were directly proportional to the input exposure per frame used to acquire the DSA images. On our DSA system operated below 2.2 Gy per frame, the threshold iodine concentration was found to be proportional to X ⫺0.57, which is in reasonable agreement with the theoretical prediction for a quantum noise limited imaging system. Above 2.2 Gy per frame, however, the threshold iodine concentration was proportional to X ⫺0.26, indicating that increasing the input exposure above this value will only achieve modest improvements in image quality. At a constant image intensifier input exposure level, increasing the x-ray tube voltage from 50 kVp to 100 kVp reduced the surface dose by a factor of 6.1, and the energy imparted by a factor of 3.5. The detection threshold iodine concentration was found to be proportional to kV p n , where n was 2.1 at 1.1 Gy per frame, and 1.6 at 3.9 Gy per frame. For clinical situations that can be modeled by a uniform phantom, reducing the x-ray tube voltage rather than increasing the exposure level would best achieve improvements on our DSA imaging system performance. © 2002 American Association of Physicists in Medicine. 关DOI: 10.1118/1.1493213兴 Key words: image quality, dosimetry, digital subtraction angiography, tube voltage, x-ray techniques INTRODUCTION Interventional neuroradiology involves studies of the vasculature and blood kinetics of the brain by means of catherization performed with the transfemoral artery technique.1,2 In these interventional neuroradiologic procedures, image quality is critical with neuro-vascular instruments being as small as 90 m, and even smaller vessel sizes.3 The continuous branching of the cerebral vessels leads to a reduction of the vessel diameter being imaged and thus the amount of iodine present in the vessel. A higher iodine concentration may sometimes be required to image distant vessels, especially during the capillary phase. Iodine concentration, however, is generally limited by direct toxicity at higher concentrations.4 An alternative to increasing the iodine concentration would be to improve the acquired signal-to-noise ratio. Practical ways to improve detection of small vessels during interven1643 Med. Phys. 29 „8…, August 2002 tional neuroradiologic procedures include the variation of x-ray tube voltage5,6 and x-ray beam intensity used to produce the radiographic image.7,8 Interventional neuroradiologic procedures often require long fluoroscopic exposure times as well as the acquisition of a large number of radiographic images.9,10 As a result, the amount of radiation received by the patient is a matter of major concern. The surface 共skin兲 dose predicts the possibility of inducing deterministic injuries, and is the key dose parameter whenever the threshold dose for the indication of such injuries is exceeded.11,12 It is desirable to keep surface doses below threshold doses for the induction of deterministic effects, which is often taken to be ⬃2 Gy. 13,14 For radiation doses below the deterministic threshold dose, the patient risk consists of the stochastic risk of carcinogenesis and the induction of genetic effects.15 For a given type of radiologic examination such as interventional neuroradiologic proce- 0094-2405Õ2002Õ29„8…Õ1643Õ8Õ$19.00 © 2002 Am. Assoc. Phys. Med. 1643 1644 Gkanatsios, Huda, and Peters: Effect of radiographic techniques 1644 TABLE I. Scoring scheme used to assess the visibility of vessel with varying concentrations of iodine contrast material. FIG. 1. Schematic diagram of the acrylic phantom with the vessel and blank inserts used to simulate small vessels for the purpose of evaluating image quality in neuroradiology. dures, the stochastic risk may be taken to be directly proportional to the total energy imparted to the patient.16 Reducing the total energy imparted to the patient will minimize the stochastic risk, and help to ensure that the patient dose is as low as reasonably achievable 共ALARA兲.17 DSA image quality needs to be adequate for the specified imaging task, and to ensure that there are no adverse clinical consequences as a result of inadequate visualization of catheters or vasculature. Changing radiographic technique factors for DSA procedures will impact both the surface dose and energy imparted.18,19 Any attempt to improve image quality by modification of radiographic technique factors should also require that the corresponding patient radiation dose be minimized. A quantitative understanding of the relationship between image quality and patient dose is therefore an important step towards the development of imaging protocols that FIG. 2. Digitally subtracted angiographic image of the DSA acrylic phantom with the 1.0 mm vessel insert. Medical Physics, Vol. 29, No. 8, August 2002 Score Description 1 2 3 4 5 Vessel not seen Vessel poorly seen (⬍50%) 50% of vessel delineated Most of vessel visible (⬎50%) Vessel perfectly visible maintain adequate diagnostic imaging performance whilst ensuring that patient radiation dose is kept ALARA. In this study, we investigated how changing x-ray tube voltage and input exposure to the image receptor affects radiation dose and image quality in DSA phantom studies that simulate interventional neuroradiologic procedures. METHOD Image quality phantom The phantom used to assess image quality consisted of thirteen stacked acrylic blocks with dimensions of 30 cm ⫻30 cm⫻1.3 cm. 20 The acrylic vessel insert measured 30 cm⫻9.0 cm⫻1.3 cm and had 30 cylindrical vessels 1.0 mm in diameter and 35 mm in length drilled along its midplane at intervals of 8.0 mm apart. The vessels were filled with iodinated contrast prepared from Ultravist 共Berlex Laboratories, Wayne, NJ兲 300 iopromide solution diluted in heparin solution to accurately prepare very low concentrations of iodine. Heparin was selected as the dilution medium because this is what is used clinically to deliver iodine contrast into the blood stream. The contrast medium was mixed thoroughly before injected into the 1.0 mm vessels of the DSA phantom. To avoid settling of the iodine contrast at the bottom of the vessel walls, the vessel insert was positioned with the vessels oriented horizontally and exposures were taken shortly after the mixing was done with the vessel insert shaken in between exposures. The iodine concentrations of the contrast medium used to fill each vessel ranged from 4.5 mg/cc of iodine to 50 mg/cc, with the ratio of iodine concentration in any two adjacent vessels being 0.92. The acrylic phantom with a vessel insert appropriate for DSA is shown in Fig. 1. In this study, an image quality index was defined as the lowest concentration of iodine in a 1.0 mm diameter vessel that may be visually detected in a DSA image. An example of DSA images obtained for this study is shown in Fig. 2. The five-point scale used to evaluate the DSA images is summarized in Table I. An observer was trained to score images of different iodine concentration using a representative series of ten DSA images of the phantom obtained during preliminary experimental work. The observer was asked to maintain a consistent criterion in using the ranking scheme listed in Table I. After training, images were presented in a random order. The concentration in the vessel that corresponded to a score of three 共see Table I兲 was taken as the iodine detection 1645 Gkanatsios, Huda, and Peters: Effect of radiographic techniques threshold in this study, with linear interpolation used where necessary. TABLE II. Imaging techniques during tube voltage experiments. 1.1 Gy/frame DSA images All DSA acquisitions were performed using a biplane Toshiba 共Toshiba America Medical Systems, Tustin, CA兲 KXO-80 high voltage diagnostic x-ray generator and the Toshiba DFP-2000A/A3 digital fluorography system configured for interventional neuroradiologic procedures. The TV camera used on the Toshiba imaging system was a MTV500A, high definition (1024⫻1024), low noise CCD camera. The x-ray source-to-image receptor distance 共SID兲 was set to the maximum value of 105 cm, with the acrylic phantom positioned so that the geometric magnification of the vessel insert was 1.2. DSA acquisitions were obtained using the 0.6 mm focal spot size and a 23 cm diameter image intensifier mode. The x-ray tube filtration in the frontal and lateral imaging planes was equivalent to 3.0 mm of aluminum 共tube inherent filtration兲. An additional 3.0 mm aluminum equivalent filtration was added in the frontal plane by the x-ray table. The generator was set to manual techniques allowing fine adjustments of the tube voltage 共kVp兲, tube current 共mA兲, exposure time 共ms兲 and optical gain 共TV iris兲. The x-ray tube voltage was monitored using a Machlett Dynalyser III 共Greenwich Instrument CO., Inc., Greenwich, CT兲. A 10⫻5-60 共the 10⫻5-60 ionization chamber has a gain of ⫻10 for better resolution兲 ionization chamber of a MDH 1015C exposure meter was positioned behind the grid of the image intensifier to record the input exposure to the image receptor. An exposure of 2.58⫻10⫺4 C/kg 共1 Roentgen兲 was taken to correspond to an air kerma of 8.73 mGy.21 During digital subtraction acquisitions, a mask frame was acquired of the blank phantom insert. The blank insert was replaced by the vessel insert and twenty additional frames were acquired 共3 frames/s兲, with the tenth frame of each DSA image acquisition used for the observer study. The window and level of the displayed images were adjusted to optimize signal detection during each DSA image acquisition. The optical gain was controlled by electronic adjustments of the iris diameter to produce a constant pixel value between 2000 and 2100, which corresponds to the target values used by the biplane imaging system for routine patient examinations. In the first experiment, a series of measurements were performed where the air kerma at the input of the image intensifier was maintained at either 1.1 Gy/frame or 3.9 Gy/frame, and with the x-ray tube voltage varied between 50 and 100 kVp. As the x-ray tube voltage was increased, the corresponding mAs value was reduced to maintain a constant air kerma level at the image intensifier input, which was monitored with an ionization chamber. Table II summarizes the technique factors used in these experiments 共i.e., kVp and mAs兲 together with corresponding measured pixel values. The data in Table II demonstrate the pixel value was kept relatively constant in these experiments, with average values (⫾standard deviation) of 2068⫾34 at 1.1 Gy/frame and 2039⫾56 at 3.9 Gy/frame. In the second experiment, Medical Physics, Vol. 29, No. 8, August 2002 1645 a 3.9 Gy/frame kVp mAs Video level mAs Video level 50 56 60 66 70a 80 90 100 28.0 14.4 9.28 5.40 4.00 2.24 1.50 0.960 2075 2018 2104 2028 2068 2054 2117 2079 80.0 47.5 33.0 20.5 17.0 7.50 4.60 3.20 1914 2052 2031 2085 2018 2056 2080 2075 Baseline techniques. another series of measurements were obtained at a constant tube voltage of 70 kVp, and with the input air kerma to the image intensifier varied from 0.44 Gy/frame to 8.8 Gy/ frame in thirteen steps. The optical gain was adjusted to maintain constant pixel value as the input air kerma was modified, with an average pixel value for the thirteen measurements of 2051⫾28. Radiation dosimetry The entrance exposure to the acrylic phantom was recorded by a 10⫻5-6 ionization chamber of an MDH 1015C exposure meter attached to the beam entrance surface of the phantom during each DSA acquisition. The ionization chamber was positioned to avoid any overlap with the iodinated vessels of the vessel insert, and the measured exposure included backscatter radiation coming from the acrylic phantom. Frame entrance exposures were obtained from the integral exposure measured for each image acquisition sequence divided by the number of acquired frames. A conversion factor of 2.58⫻10⫺4 C/kg 共1R兲 corresponding to an absorbed dose of 9.3 mGy for muscle tissue was used to convert the beam entrance exposure to surface dose.21 The energy imparted was computed using the method described in detail elsewhere.22,23 The total phantom thickness was 16.9 cm of acrylic, which was taken to be equivalent to 20 cm of water for computing values of energy imparted, given that the density of acrylic is 1.19 g/cm3 . 24 Since the exposure was obtained from direct exposure measurements during each image acquisition sequence, it included backscatter. The backscatter radiation fraction was measured for the corresponding phantom at each applied tube voltage and was subtracted from the measured exposures to obtain the free-in-air exposure.20 The exposure area at the beam entrance plane of the phantom was computed from geometry assuming a circular beam area of 23 cm diameter at the image intensifier plane. Values of energy imparted for head x-ray examinations were converted into the corresponding adult effective doses using E/ 共mSv/J兲 conversion factors averaged for the posteroanterior and lateral views and ranged between 4.1 and 5.9 mSv/J depending on the selected x-ray tube voltage.25 1646 Gkanatsios, Huda, and Peters: Effect of radiographic techniques 1646 FIG. 3. Threshold iodine concentration as a function of tube voltage. The asterisks correspond to the 3.9 Gy/frame, and the triangles correspond the 1.1 Gy/frame. RESULTS Measurement precision Five digital subtraction acquisition sequences, obtained at 70 kVp, were generated at different times over a one-day period. These five sequences were used to determine the radiation dosimetry precision and reader performance precision. The average entrance exposure measured was 0.852 ⫾0.006 mGy/frame. The average of five observer readings for the threshold contrast concentration at 70 kVp and 2.6 Gy/frame was 8.0⫾0.96 mg/cc. As expected, the precision of radiation exposure measurements (⬍1%) is much lower than the reproducibility of the detection threshold value 共12%兲, given that the latter is based on the subjective assessment of a human observer.26 X-ray tube voltage Figure 3 shows the threshold iodine concentration as a function of tube voltage. The solid and dashed lines shown in Fig. 3 are least squares fits to the experimental data. At 1.1 Gy/frame, the threshold iodine concentration was proportional to the kVp 2.1, where the coefficient of determination of the least squares fit (r 2 ) was 0.92. At this input exposure, a 10 kVp increase of the tube voltage from the baseline 共70 kVp兲 increased the threshold iodine concentration by 32%. Reducing the x-ray tube voltage from 70 kVp to 60 kVp reduced the detection threshold concentration by 27%. At 3.9 Gy/frame, the threshold concentration was proportional to kVp 1.6, where the coefficient of determination of the least squares fit (r 2 ) was 0.97. At an exposure level of 3.9 Gy/ frame, increasing the tube voltage from 70 kVp to 80 kVp increased the threshold concentration by 23%, whereas reducing the x-ray tube voltage from 70 kVp to 60 kVp reduced the detection threshold concentration by 21%. Over the x-ray tube voltage range investigated in this study 共50– 100 kVp兲, the average increase in detection threshold as a result of reducing the exposure level from 3.9 to 1.1 Gy/ frame was 1.7⫾0.3. Figure 4 shows the relative behavior of surface dose and energy imparted as a function of tube voltage. The data of Medical Physics, Vol. 29, No. 8, August 2002 FIG. 4. Relative behavior of surface dose and energy imparted as a function of tube voltage. Solid diamonds and lines correspond to 1.1 Gy/frame; triangles and broken lines correspond to 3.9 Gy/frame. Data has been normalized so that values at 70 kVp were equal to 1. Fig. 4 have been fitted to power functions with resulting coefficient of determination (r 2 ) between 0.95 and 0.98. Table III provides a summary of the key dosimetry parameters 共i.e., surface dose, energy imparted and effective dose兲 obtained at the two exposure levels investigated. As expected, relative changes of both surface dose and energy imparted as a function of x-ray tube voltage were similar at TABLE III. DSA dosimetry summary. a kVp Surface dose 共mGy/frame兲 Energy imparted 共mJ/frame兲 Effective dose 共Sv/frame兲 50 60 70 80 90 100 1.2a关3.9兴b 0.62关2.4兴 0.38关1.3兴 0.28关0.96兴 0.24关0.65兴 0.20关0.66兴 1.6关5.0兴 0.95关3.7兴 0.66关2.3兴 0.54关1.9兴 0.50关1.4兴 0.44关1.5兴 6.5 关20兴 4.4 关17兴 3.3 关11兴 2.9 关10兴 2.8关7.9兴 2.6关8.8兴 1.1 Gy/frame input air kerma. 3.9 Gy/frame input air kerma. b 1647 Gkanatsios, Huda, and Peters: Effect of radiographic techniques 1647 FIG. 5. Threshold iodine concentration as a function of image intensifier input air kerma at 70 kVp and a constant pixel intensity. exposure levels of 1.1 Gy/frame and 3.9 Gy/frame. Increasing the x-ray tube voltage from 50 kVp to 100 kVp reduced the surface dose by a factor of 6.1, and reduced the energy imparted by a factor of 3.5. Input air kerma Figure 5 shows the threshold iodine concentration as a function of image intensifier input air kerma at a constant x-ray tube voltage of 70 kVp where both the ordinate and abscissa are plotted using a logarithmic scale. Data below and above 2.2 Gy/frame were fitted separately to a least squares fit to a line. Below 2.2 Gy/frame, the detection threshold concentration was found to be proportional to X ⫺0.57 where the coefficient of determination (r 2 ) was 0.98. Above 2.2 Gy/frame, the detection threshold concentration was found to be proportional to X ⫺0.26 where the coefficient of determination (r 2 ) was 0.96. For our DSA imaging system, increasing the image intensifier input air kerma from 1.1 Gy/frame to 2.2 Gy/frame reduced the detection threshold concentration by 34%, whereas increasing the input air kerma from 3.9 Gy/frame to 7.8 Gy/frame reduced the detection threshold concentration by only 16%. The empirical data presented in Fig. 5 indicate that above an input air kerma of about 2.2 Gy/ frame, there is only modest improvement in the detection threshold concentration of 1.0 mm diameter vessels with increasing input air kerma. These results are only applicable to the imaging system investigated in this study, and could be different for other types of DSA imaging system. air kerma by 63%. At 3.9 Gy/frame, a 25% reduction in detection threshold concentration may be achieved by either lowering the tube voltage to 59 kVp, or by increasing the input air kerma by a factor of 200%. The increased surface dose and energy imparted required to achieve this 25% reduction on the iodine threshold concentration are summarized in Table IV. Improvements in image quality by reducing the x-ray tube voltage always resulted in lower doses than could be achieved by increasing the x-ray intensity level to the image receptor at a constant x-ray tube voltage. Radiation dose versus image quality DISCUSSION Figures 6 and 7 show the relative increases in surface dose and energy imparted as the iodine detection thresholdconcentration is reduced by changing either the image intensifier input air kerma or the x-ray tube voltage. The data generated in Figs. 6 and 7 are based on the least squares curves fitted to the empirical data in Figs. 3–5. At 70 kVp and 1.1 Gy/frame, a 25% reduction in detection threshold concentration may be achieved by either lowering the tube voltage to 61 kVp, or by increasing the input For a film-screen imaging system, the exposure level is effectively fixed by the need to produce an optimum optical density. Any variations in the exposure level in screen-film radiography will produce over 共or under兲 exposed films, with a concomitant drop in image contrast. In digital imaging systems, however, the range of receptor input exposure can vary by over an order of magnitude 共e.g., Fig. 5兲, yet still produce diagnostic quality images. The advent of relatively sophisticated digital imaging equipment thus offers considerable Medical Physics, Vol. 29, No. 8, August 2002 FIG. 6. Increased surface dose resulting from reducing the x-ray tube potential or increasing the exposure level to achieve the specified improvement in threshold detection concentration of iodine. 1648 Gkanatsios, Huda, and Peters: Effect of radiographic techniques 1648 TABLE V. Computed mean x-ray energies of x-ray spectra, half-value layers 共mm Al兲, and iodine attenuation coefficients as a function of x-ray tube voltage. kVp Incident mean energy and HVL Exit mean energy and HVL Mass attenuation coefficient of I (cm2 /g) c 50 60 70 80 90 100 32.6a关1.8兴b 36.3关2.2兴 39.7关2.5兴 43.1关2.8兴 46.2关3.2兴 49.0关3.6兴 39.1关2.2兴 44.6关3.9兴 49.4关5.2兴 54.0关6.26兴 58.1关7.2兴 61.7关7.9兴 23.4 16.6 12.7 10.0 8.26 7.03 a Incident mean energy in keV. Half-value layer in mm Al. c Mass attenuation coefficient is determined at the mean x-ray energy. b FIG. 7. Increased energy imparted resulting from reducing the x-ray tube potential or increasing the exposure level to achieve the specified improvement in threshold detection concentration of iodine. flexibility in acquiring x-ray image data.27 The wide range of input radiation exposures, as well as variations in the selected x-ray tube voltage, could play a significant role in helping to optimize patient dose and image quality. A quantitative understanding of the relationship between dose and image quality is therefore important to help operators make the best use of digital imaging equipment. Improvements in imaging performance should require the modification of those radiographic technique factors that minimize the patient radiation risk. Conversely, if it is possible to reduce TABLE IV. Changes in surface dose and energy imparted required to reduce the iodine threshold concentration by 25% by reducing the x-ray tube potential, or by increasing the input air kerma to the image intensifier. 1.1 Gy/frame 3.9 Gy/frame Parameter X-ray tube potential Exposure level X-ray tube potential Exposure level Surface dose Energy imparted 44% 29% 63% 63% 70% 46% 200% 200% Medical Physics, Vol. 29, No. 8, August 2002 image quality without adversely affecting diagnostic performance, technique factors should be modified to maximize patient dose savings. In screen-film radiography, it is well established that increasing x-ray tube voltage or x-ray beam quality degrades image quality.18,28 –30 The data presented in Fig. 3 shows that tube voltage has a significant effect on the iodine detection threshold concentration in DSA, as well. Changing the x-ray tube voltage will predominantly affect the contrast of the signal detected by the imaging system if the absolute x-ray intensity level remains constant. Reducing the x-ray tube voltage lowers the average photon energy and increases x-ray absorption because of the rapid rise in photoelectric absorption as the average photon energy approaches the iodine 33 keV K edge. An additional factor affecting image quality at different x-ray tube voltages is the presence of scatter radiation. Scatter radiation generally increases with increased x-ray tube voltage, and will thereby reduce image contrast.31 The data in Fig. 3 may be compared with theoretical changes in x-ray spectral energies and x-ray absorption coefficients for iodine. For the theoretical calculation, average incident photon energies and half-value layers 共HVL兲 were computed for a 3 mm Al filtered x-ray tube running at constant voltage.32 The exit mean energy and HVL were obtained by filtering the x-ray spectra with 20 cm of water. The absorption coefficient of iodine was determined using the exit mean photon energies.21,33 Table V shows the computed values of incident photon energy and exit photon energy, together with the corresponding iodine mass attenuation coefficient. Reducing the x-ray tube voltage from 100 kVp to 50 kVp would be expected to improve the image contrast by about a factor of 3. The relationship between selected kVp and mass attenuation coefficient in Table V was fitted to a power law 共i.e., inversely proportional to kVp n 兲, with the theoretical value of n determined to be 1.7. This theoretical prediction may be compared to the experimental data obtained at doses where quantum mottle is dominant—this corresponds to a slope of 2.1 obtained at an exposure rate of 1.1 Gy/frame 共see Fig. 3兲. The differences between the measured and theoretical values may be due to uncertainties in 1649 Gkanatsios, Huda, and Peters: Effect of radiographic techniques the x-ray spectra as well as changes in quantum noise as a function of kVp which were neglected in our computations. The primary source of noise in 共digital兲 x-ray imaging is usually quantum mottle, which corresponds to random spatial fluctuations of the distribution of x-ray quanta absorbed by the detector.8,34 Since the production and attenuation of x rays are governed by Poisson statistics, quantum mottle is inversely proportional to the square root of the radiation exposure level used to generate an image. The results shown in Fig. 5 demonstrate that for input air kerma smaller than 2.2 Gy/frame, this specific DSA imaging system is quantum noise limited, since the observed performance shows proportionality close to the value of to X ⫺0.5 expected for a quantum noise limited system. A significant performance gain can be achieved by increasing the input air kerma at these lower exposure levels. At exposure levels greater than 2.2 Gy/frame, the measured iodine detection threshold concentration is proportional to X ⫺0.26, demonstrating that imaging performance is no longer limited by quantum mottle alone. At these higher exposure levels, additional noise factors become significant and would need to be included in any analysis of system imaging performance. These noise sources include factors such as electronic noise, time jitter and structure noise.8,34 –37 The relative importance of these additional noise sources is also the reason for the differences in the slopes observed in Fig. 3. For a quantum noise limited system, the slope of the curve plotting threshold concentration and kVp would be independent of the radiation exposure level. System noise will set an upper limit to the x-ray flux, which may be taken to occur when the quantum and electrical noise components are equal.38 One limitation of our study is that the phantom used had a constant thickness which is rarely achieved in clinical practice. For a non-uniform patient, the highest exposure level occurs in the thinest body region and this should be mapped to the maximum signal level of the video camera.38 The resultant signal to noise ratio of the vessel containing the iodine will depend on the transmitted x-ray intensity in the region of interest. This limitation is of much greater importance in nonuniform areas such as the lung or extremities, than for abdominal or head imaging. Bright spots in DSA imaging should be minimized by appropriate bolusing to attempt to ensure that all regions of the image are obtained at maximum signal levels.31 The data presented in Figs. 6 and 7 indicate how modification of radiographic technique factors affect imaging performance and patient dose, given a detection task of identifying a circular vessel 共1.0 mm diameter兲 containing iodine contrast media. It is evident that achieving improved imaging performance by reduction in x-ray tube voltage is the preferred option, since the patient doses are significantly lower than when the same level of imaging performance is achieved by increasing the input radiation exposure level to the image receptor. Our results also show that increasing the image intensifier input air kerma beyond 2.2 Gy/frame on our specific DSA system provided relatively little improvement in measured imaging performance. Use of such higher Medical Physics, Vol. 29, No. 8, August 2002 1649 radiation exposure levels would require explicit justification in terms of the anticipated benefit to the patients to offset risk of deterministic effects and the higher stochastic risks. At our institution, the typical interventional neuroradiologic DSA x-ray tube voltages are currently 76 to 80 kVp for the frontal plane and 66 to 70 kVp for the lateral plane, and with corresponding air kerma values at the input of the image intensifier set at 4.4 and 6.1 Gy/frame. A typical diagnostic examination can result in 400 DSA images in each of the two imaging projection planes. As a result, patient surface doses from DSA imaging could easily be of the order of 0.65 Gy, which would need to be added to any dose associated with fluoroscopic imaging, typically 0.25 Gy. Such data clearly demonstrate the potential for inducing deterministic effects in DSA studies, particularly in studies that require an increased number of radiographic images. Typical value of energy imparted to a patient undergoing an interventional neuroradiologic procedure is 6 J, and the corresponding patient effective dose would therefore be of the order of 30 mSv.20 These effective doses are much higher than is normally encountered in conventional radiography.39 DSA patient effective doses are at the upper end of the range of patient doses in radiology, and emphasize the need to pay careful attention to minimizing patient doses. CONCLUSION The results obtained in this study demonstrate that for improving low contrast detection on our DSA imaging system, reducing x-ray tube voltage 共i.e., kVp兲 was a superior strategy to that of increasing the x-ray beam intensity level 共i.e., mAs兲. For a given x-ray DSA imaging system, there is an exposure level at which quantum mottle will cease to be the dominant source of image noise. For the DSA system investigated in this work, this exposure level was found to be about 2.2 Gy per frame at the input to the image intensifier. For this specific DSA system, increasing the image intensifier input exposure level beyond 2.2 Gy per frame would be of limited benefit given that the improvement in low contrast detection performance is relatively modest. ACKNOWLEDGMENTS We would like to thank Lynn Rill for reading the images, and Dennis Pinner 共Toshiba兲 for technical support in using the biplane imaging system. a兲 Current address: LORAD, A Hologic Company, 36 Apple Ridge Road, Danbury, CT 06810. 1 F. Vinuela, Interventional Neuroradiology 共Raven, New York, 1992兲. 2 A. G. Osborn, Diagnostic Cerebral Angiography, 2nd ed. 共Lippincott, Philadelphia, PA, 1999兲. 3 R. I. Grossman and D. M. Yousem, Neuroradiology: The Requisites 共Mosby-Year Book, St. Louis, MO, 1994兲. 4 J. J. Caro, E. Trindade, and M. McGregor, ‘‘The risks of death and of severe nonfatal reactions with high- vs low-osmolality contrast media: a metaanalysis,’’ J. Radiol. 156, 825– 832 共1991兲. 5 W. M. Thompson, R. A. Halvorsen, R. K. Gedgaudas, F. M. Kelvin, R. P. Rice, S. Woodfield, G. A. Johnson, L. W. Hedlung, and D. B. Jorgensen, ‘‘High kVp vs. low kVp for T-tube operative cholangiography,’’ Radiology 146, 635– 642 共1983兲. 1650 Gkanatsios, Huda, and Peters: Effect of radiographic techniques 6 M. J. Tapiovaara and M. Sandborg, ‘‘Evaluation of image quality in fluoroscopy by measurements and Monte Carlo calculations,’’ Phys. Med. Biol. 40, 589– 607 共1995兲. 7 H. Fujita, K. Doi, M. L. Giger, and H.-P. Chang, ‘‘Investigation of basic imaging properties in digital radiography. 5. Characteristic curves of II-TV digital systems,’’ Med. Phys. 13, 13–18 共1986兲. 8 M. L. Giger, K. Doi, and H. Fujita, ‘‘Investigation of basic imaging properties in digital radiography. 7. Noise Wiener spectra of II-TV digital imaging systems,’’ Med. Phys. 13, 131–138 共1986兲. 9 B. Berthelsen and Å. Cederblad, ‘‘Radiation doses to patients and personnel involved in embolization of intracerebral arteriovenous malformations,’’ Acta Radiol. 32, 492– 497 共1991兲. 10 N. A. Gkanatsios, W. Huda, K. R. Peters, and J. A. Freeman, ‘‘Evaluation of an on-line patient exposure meter in neuroradiology,’’ Radiology 203, 837– 842 共1997兲. 11 W. Huda and K. R. Peters, ‘‘Radiation-induced temporary epilation after a neuroradiologically guided catheterization procedure,’’ Radiology 193, 642– 644 共1994兲. 12 E. Vano, L. Arranz, J. M. Sastre, C. Moro, A. Ledo, M. T. Garate, and I. Minguez, ‘‘Dosimetric and radiation protection considerations based on some cases of patient skin injuries in interventional cardiology,’’ Br. J. Radiol. 71, 510–516 共1998兲. 13 L. K. Wagner, P. J. Eifel, and R. A. Geise, ‘‘Potential biological effects following high x-ray dose interventional procedures,’’ J. Vasc. Interv Radiol. 5, 71– 84 共1994兲. 14 International Commission on Radiological Protection 共ICRP兲, Publication 47: Annals of the ICRP 14(3). Non-Stochastic Effects of Ionizing Radiation 共Pergamon, Oxford, 1984兲. 15 International Commission on Radiological Protection 共ICRP兲, Publication 60: Annals of the ICRP 21(1–3). 1990 Recommendations of the International Commission on Radiological Protection 共Pergamon, Oxford, 1991兲. 16 B. Wall, R. Harrison, and F. Spiers, ISPM Report #53: Patient Dosimetry Techniques in Diagnostic Radiology 共The Institute of Physical Science in Medicine, York, England, 1988兲. 17 International Commission on Radiological Protection 共ICRP兲, Publication 34: Protection of the patient in diagnostic radiology 共Pergamon, Oxford, 1982兲. 18 P. C. Shrimpton, D. J. Jones, and B. F. Wall, ‘‘The influence of tube filtration and potential on patient dose during x-ray examinations,’’ Phys. Med. Biol. 33, 1205–1212 共1988兲. 19 A. M. Norbash, D. Busick, and M. P. Marks, ‘‘Techniques for reducing interventional neuroradiologic skin dose: tube position rotation and supplemental beam filtration,’’ Am. J. Neuroradiol. 17, 41– 49 共1996兲. 20 N. A. Gkanatsios, Doctoral thesis: Patient doses and image quality in interventional neuroradiology 共University of Florida, Gainesville, FL, 1998兲. Medical Physics, Vol. 29, No. 8, August 2002 21 1650 H. E. Johns and J. R. Cunningham, The Physics of Radiology, 4th ed. 共Charles C. Thomas, Springfield, IL, 1983兲. 22 N. A. Gkanatsios, Master thesis: Computation of energy imparted in diagnostic radiology 共University of Florida, Gainesville, FL, 1995兲. 23 N. A. Gkanatsios and W. Huda, ‘‘Computation of energy imparted in diagnostic radiology,’’ Med. Phys. 24, 571–579 共1997兲. 24 The Health Physics and Radiological Health Handbook, edited by B. Shleien 共Scinta, Inc., Silver Springs, MD, 1992兲. 25 W. Huda and N. A. Gkanatsios, ‘‘Effective doses and energy imparted in diagnostic radiology,’’ Med. Phys. 24, 1311–1316 共1997兲. 26 W. R. Hendee and P. N. T. Wells, The Perception of Visual Information, 2nd ed. 共1997兲. 27 W. R. Hendee and J. H. Trueblood, Medical Physics Monograph No. 22: Digital Imaging 共Medical Physics Publishing, Madison, WI, 1993兲. 28 E. D. Trout, J. P. Kelley, and G. A. Cathey, ‘‘The use of filters to control radiation exposure to the patient in diagnostic roentgenology,’’ Am. J. Roentgenol., Radium Ther. Nucl. Med. 57, 946 –963 共1952兲. 29 K. Koedooder and H. W. Venema, ‘‘Filter materials for dose reduction in screen-film radiography,’’ Phys. Med. Biol. 31, 585– 600 共1986兲. 30 H. D. Nagel, ‘‘Comparison of performance characteristics of conventional and K-edge filters in general diagnostic radiology,’’ Phys. Med. Biol. 34, 1269–1287 共1989兲. 31 B. H. Hasegawa, The Physics of Medical X-Ray Imaging, 2nd ed. 共Medical Physics Publishing, Madison, WI, 1991兲. 32 M. Tucker, G. Barnes, and D. Chakraborty, ‘‘Semiempirical model for generating tungsten target x-ray spectra,’’ Med. Phys. 18, 211–218 共1991兲. 33 J. Hubbell, ‘‘Photon mass attenuation and energy-absorption coefficients from 1 keV to 20 MeV,’’ Int. J. Appl. Radiat. Isot. 33, 1269–1290 共1982兲. 34 H. Fujita, K. Ueda, J. Morishita, T. Fujikawa, A. Ohtsuka, and T. Sai, ‘‘Basic imaging properties of a computed radiographic system with photostimulable phosphors,’’ Med. Phys. 16, 52–59 共1989兲. 35 B. A. Arnold and P. O. Scheibe, ‘‘Noise analysis of a digital radiography system,’’ Am. J. Roentgenol. 142, 609– 613 共1984兲. 36 M. K. Giger, Ph.D. dissertation: Investigation of basic imaging properties in digital radiography 共University of Chicago, Chicago, IL, 1985兲. 37 J. Esthappan, H. Harauchi, and K. R. Hoffmann, ‘‘Evaluation of imaging geometries calculated from biplane images,’’ Med. Phys. 25, 965–975 共1998兲. 38 R. A. Kruger, C. A. Mistretta, and S. J. Riederer, ‘‘Physical and technical considerations of computerized fluoroscopy difference imaging,’’ IEEE Trans. Nucl. Sci. NS 28, 205–212 共1981兲. 39 United Nations Scientific Committee on the Effects of Atomic Radiation 共UNSCEAR兲, 1993 Report to the General Assembly: Medical Radiation Exposures 共United Nations, New York, 1993兲.