- Wiley Online Library
advertisement

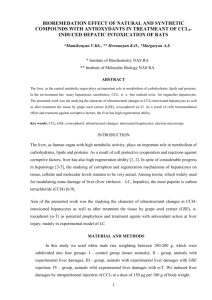
Epithelial Cell Adhesion Molecule (EpCAM) Marks Hepatocytes Newly Derived from Stem/Progenitor Cells in Humans So-Mi Yoon,1* Domniki Gerasimidou,2* Reiichiro Kuwahara,3 Prodromos Hytiroglou,2 Jeong Eun Yoo,1 Young Nyun Park,1,4 and Neil D. Theise5 Epithelial cell adhesion molecule (EpCAM) is a surface marker on human hepatic stem/ progenitor cells that is reported as absent on mature hepatocytes. However, it has also been noted that in cirrhotic livers of diverse causes, many hepatocytes have EpCAM surface expression; this may represent aberrant EpCAM expression in injured hepatocytes or, as we now hypothesize, persistence of EpCAM in hepatocytes that have recently derived from hepatobiliary progenitors. To evaluate this concept, we investigated patterns of EpCAM expression in hepatobiliary cell compartments of liver biopsy specimens from patients with all stages of chronic hepatitis B and C, studying proliferation, senescence and telomere lengths. We found that EpCAM(1) hepatocytes were rare in early stages of disease, became increasingly prominent in later stages in parallel with the emergence of ductular reactions, and were consistently arrayed around the periphery of cords of keratin 19(1) hepatobiliary cells of the ductular reaction, with which they shared EpCAM expression. Proliferating cell nuclear antigen (proliferation marker) and p21 (senescence marker) were both higher in hepatocytes in cirrhosis than in normal livers, but ductular reaction hepatobiliary cells had the highest proliferation rate, in keeping with being stem/progenitor cell–derived transit amplifying cells. Telomere lengths in EpCAM(1) hepatocytes in cirrhosis were higher than EpCAM(2) hepatocytes (P < 0.046), and relatively shorter than those in the corresponding ductular reaction hepatobiliary cells (P 5 0.057). Conclusion: These morphologic, topographic, immunophenotypic, and molecular data support the concept that EpCAM(1) hepatocytes in chronic viral hepatitis are recent progeny of the hepatobiliary stem/progenitor cell compartment through intermediates of the transit amplifying, ductular reaction hepatobiliary cells. (HEPATOLOGY 2011;53:964-973) T here is a growing consensus that some contribution to hepatocyte mass derives from intrahepatic, hepatobiliary stem cells and that the contribution depends on presence of injury, its form, and its degree.1-8 Support for this concept is found in animal models, often employing a two-hit experimental method in which there is poisoning of hepatocytes to inhibit their replication (e.g., 2-acetylaminofluorene) Abbreviations: CHB, chronic hepatitis B; CHC, chronic hepatitis C; EpCAM, epithelial cell adhesion molecule; K, keratin; PCNA, proliferating cell nuclear antigen. From the 1Department of Pathology, Brain Korea 21 Project for Medical Science, Center for Chronic Metabolic Disease, Yonsei University Health System, Seoul, South Korea; the 2Department of Pathology, Aristotle University Medical School, Thessaloniki, Greece; the 3Division of Gastroenterology, Department of Medicine, Kurume University School of Medicine, Kurume, Japan; the 4Institute of Gastroenterology, Yonsei University Health System, Seoul, South Korea; and the 5Department of Pathology and Medicine, Beth Israel Medical Center, New York, NY. Received July 20, 2010; accepted December 2, 2010. Supported by a Korea Science and Engineering Foundation grant from the Korean Ministry of Science and Technology (R13-2002-054-03004-0 and 20100008075) and by a grant from the National R&D Program for Cancer Control, Ministry for Health, Welfare, and Family Affairs, Republic of Korea (0920300) (to Y. N. P.). *These authors contributed equally to this work. Address reprint requests to: Young Nyun Park, M.D., Ph.D., Department of Pathology, Yonsei University Health System 250 Seongsanno, Seodaemun-gu, Seoul, 120-752, South Korea. E-mail: young0608@yuhs.ac; fax: (82)-2-362-0860; or Neil Theise, M.D., Division of Digestive Diseases, Beth Israel Medical Center, First Avenue at 16th Street, New York, NY 10003. E-mail: ntheise@chpnet.org; fax: 212-420-4373. C 2010 by the American Association for the Study of Liver Diseases. Copyright V View this article online at wileyonlinelibrary.com. DOI 10.1002/hep.24122 Potential conflict of interest: Nothing to report. Additional Supporting Information may be found in the online version of this article. 964 HEPATOLOGY, Vol. 53, No. 3, 2011 followed by injury to eliminate significant amounts of hepatocyte mass, either by application of a second toxin (e.g., retrosine, monocrotaline) or partial hepatectomy.9 In such procedures, there is stem cell activation leading to expansion of a progenitor pool referred to as oval cells. In these experiments, whether hepatocytes are derived from other, preexisting hepatocytes or from stem/progenitor cell activation and differentiation can be partly evaluated through tracking experiments where populations of cells from an animal with a distinctive marker are transplanted into animals without the marker (e.g., wild-type, dipeptidyl peptidase-4 positive cells into dipeptidyl peptidase-4–positive knockout recipients, or male, Y chromosome–positive cells into female recipients).9,10 These models have provided a working hypothesis for human liver disease. In acute acetaminophen toxicity, the most severe (lethal) injury leads to activation of a stem/progenitor cell compartment, predominantly located in the proximal branches of the biliary tree, including the bile ductules and the canals of Hering.11 This proliferative response, the human equivalent of the oval cell response in rodents, is referred to as a ductular reaction.12 In chronic liver diseases, such as viral or autoimmune hepatitis and alcoholic or nonalcoholic fatty liver disease, ductular reactions are also prominent, but generally only in the late stages of disease, leading to the hypothesis that it is only after several years, often decades of chronic injury that the hepatocytes lose their replicative potential necessitating activation of the stem/progenitor cell response.13-15 In both of these settings, the stem/progenitor cell response arises because hepatocytes have been largely eliminated (acute injury) or have lost their replicative potential (chronic injury), paralleling the animal data. These human correlates to the animal models have depended on data gathered predominantly on the basis of morphology/architecture (e.g., three dimensional reconstructions of ductular reactions indicating their link to regenerating hepatocytes)6,7,11 or immunohistochemical markers of proliferation and/or senescence (Ki-67, p21 respectively, in most studies).13-15 These data show that in the early stages of chronic liver disease, hepatocytes can easily accomplish hepatocyte restitution through cell division; ductular reactions are largely absent. However, as disease progresses over many years to decades, hepatocytes show faltering proliferation (by Ki-67 expression) and increasing senescence (p21 expression). With these changes there arise parallel, highly proliferative ductular reactions. More precise cell tracking experiments of the type performed in animals are, of course, not easily possible YOON ET AL. 965 in humans, although the recently published data of Lin et al.16 exploiting mutational analysis in mitochondrial DNA encoded cytochrome c oxidase enzyme goes a long way to accomplishing this, convincingly showing the descent of hepatocytes from stem/progenitor cells of associated ductular reactions. Nonetheless, in humans, the specific distinction between hepatocytederived hepatocytes and stem/progenitor cell-derived hepatocytes has to date not been accomplished. Recently, however, epithelial cell adhesion molecule (EpCAM) has been identified as a surface marker on human hepatic stem/progenitor cells that is absent on mature hepatocytes.2,17,18 Yet, it has also been noted that in cirrhotic livers of diverse causes, many hepatocytes have EpCAM surface expression2; this may represent aberrant EpCAM expression in injured hepatocytes versus persistence of EpCAM in hepatocytes that have recently been derived from hepatobiliary progenitors. We have hypothesized that EpCAM positive [EpCAM(þ)] hepatocytes are indeed newly derived hepatocytes, originating from differentiation of EpCAM(þ) stem/progenitor cells in ductular reactions. To evaluate this concept, we investigated the patterns of EpCAM expression in hepatocytes and ductular reactions of liver biopsy specimens from patients with chronic hepatitis B and C in all stages of disease, performed immunohistochemical studies of proliferation and senescence, and evaluated telomere lengths of all hepatobiliary cells in the sections studied. Materials and Methods Liver Samples. Archival, formalin-fixed, paraffinembedded sections of liver specimens were obtained from the Departments of Pathology at Beth Israel Medical Center, New York, United States, Kurume University School of Medicine, Kurume, Japan, Aristotle University Medical School, Thessaloniki, Greece, and from the Liver Cancer Specimen Bank, part of the National Research Resource Bank Program, which is administered by the Korea Science and Engineering Foundation under the Ministry of Science and Technology. Approvals from the respective institutional review boards or the equivalent were obtained prior to beginning all investigations. The liver biopsy specimens consisted of 33 cases of chronic hepatitis B (CHB) and 69 cases of chronic hepatitis C (CHC). Histologically normal (control) liver specimens were obtained from wedge-biopsied livers of donors for liver transplantation, autopsy, or normal tissue distant from tumor in hepatic resections. 966 YOON ET AL. HEPATOLOGY, March 2011 Table 1. Immunohistochemistry Systems Used in the Present Study Antibody Source Miltenyi Biotec (BIMC) Novocastra (AUMS) Calbiochem (KUSM, KOSEF) Clone Dilution Antigen Retrieval Antigen Detection HEA-125 VU-1D9 VU-1D9 1:200 1:100 1:3000 Target Retrieval Solution (Dako) at 99 C (30 minutes) Bond Vision Biosystems 100 mM sodium citrate (pH 6.0) boiled in microwave (15 minutes) Dako EnVision kit Bond Vision Biosystems Dako EnVision kit AUMS, Aristotle University Medical School; BIMC, Beth Israel Medical Center; KOSEF, Korea Science and Engineering Foundation; KUSM, Kurume University School of Medicine. The liver biopsy specimens with chronic hepatitis were staged for fibrosis according to a modified Ishak staging system19 (1, portal fibrosis; 2, fibrous septa; 3, transition to cirrhosis; 4, established cirrhosis) and for grade of necroinflammatory activity (1, mild; 2, moderate; 3, severe [i.e., with confluent necrosis]). Immunohistochemistry. Four-micron thick tissue sections were deparaffinized with xylene and rehydrated with graded alcohols. After washing in distilled water, sections were immersed in 3% hydrogen peroxide to block endogenous peroxidase. Details of EpCAM staining methods used at the three institutions are given in Table 1. Other antibodies used for immunohistochemical stains included: keratin (K) 19 (clone RCK108, Dako, Glostrup, Denmark; dilution 1:20), p21WAF1/Cip1 (clone SX118, Dako; dilution 1:50), and proliferating cell nuclear antigen (PCNA) (clone PC10, Dako; dilution 1:75). These stains were either performed in sequential cuts of the tissue block (EpCAM/K19) or in the same slide (double staining of EpCAM with K19, p21WAF1/Cip1, or PCNA). We used the DAKO Envision Kit (Dako) for immunohistochemistry with a single primary antibody, using 3,3-diaminobenzidine (Dako) as the chromagen. All slides were counterstained with hematoxylin. For double immunohistochemical staining, the EnVision AP system (Dako) and Vector Blue Alkaline Phosphatase Substrate Kit III (SK-5300, Vector Laboratories, Burlingame, CA) were used to detect the first primary antibody, and then the EnVision DuoFLEX Doublestain System (SK110) (Dako) and Vector NovaRED Substrate Kit (SK-4800, Vector Laboratories) were used to detect the second primary antibody. The extent of EpCAM(þ) hepatocytes was assessed both in relationship to K19(þ) cells of ductular reactions, as well as semiquantitatively by evaluating the entirety of the tissue on each stained slide (0, no positive hepatocytes; 1þ, <5% of hepatocytes positive for EpCAM; 2þ, 5%-10% of hepatocytes positive for EpCAM; 3þ, 11%-50% of hepatocytes positive for EpCAM; 4þ, >50% of hepatocytes positive for EpCAM). Telomere Evaluation by Way of Quantitative Fluorescence In Situ Hybridization. Six of the CHB cirrhosis cases and nine normal liver cases were eval- uated for telomere lengths by way of quantitative fluorescence in situ hybridization. The peptide nucleic acid probes included Cy3 telomere probe (50 -Cy3-OOCCC-TAA-CCC-TAA-CCC-TAA-30 ) and FAM centromere [P2] probe (50 -FAM-OO-ATTCGTTG GAAACGGGA-30 ), both obtained from Panagene, Daejon, South Korea. In brief, tissue sections were deparaffinized in xylene and rehydrated in graded alcohols. Antigen retrieval was performed in citrate buffer (pH 6.0) in a 700-W microwave oven for 10 minutes, and the sections were fixed in 10% buffered formalin. The sections were then treated with protease I solution (1 mg/mL, Vysis, Downers Grove, IL) at 37 C for 10 minutes, dehydrated in graded alcohols, and air-dried. The telomere/centromere probe mix (telomere: 2.5 lL 10 lg/mL PNA Cy3-telomere probe, 2.5 lL 25 lg/ mL FAM centromere probe) was then applied, followed by denaturation at 80 C for 3 minutes and hybridization at 37 C for 2 hours using Vysis HYBrite. The sections were washed in posthybridization buffer (NP40/20x saline sodium citrate, Vysis) at room temperature for 30 minutes and then in Trisbuffered saline with Tween 20 for 15 minutes. To detect EpCAM, incubation with monoclonal antibody (EpCAM clone VU-1D9; Calbiochem, Darmstadt, Germany; dilution 1:3000) was performed for 1 hour at room temperature, after which the secondary antibody (goat anti-rabbit-Alexa flour 633; Invitrogen, Eugene, OR) was applied. The sections were counterstained with 4’-6-diamidine-2-phenylindole and mounted with Prolong anti-fade mounting medium (Molecular Probes, Eugene, OR) for observation. Then the sections were examined under fluorescent microscope. The telomere fluorescence intensity and the centromere fluorescence intensity were analyzed using Image Pro Plus 5.0 software (MediaCybernetics, Silver Spring, MD), and the telomere fluorescence intensity/ centromere fluorescence intensity ratio was calculated in each telomere dot. To facilitate day-to-day comparison, a fluorescence bead (Molecular Probe) was photographed and analyzed. Statistical Analysis. Statistical analysis was performed using SPSS software (SPSS, Chicago, IL) and assessed using a Student t test and Mann-Whitney U HEPATOLOGY, Vol. 53, No. 3, 2011 YOON ET AL. Table 2. Patient Demographics and Chronic Hepatitis Stage Fibrosis Stage Chronic hepatitis C Chronic hepatitis B Controls Median Age (Range) Male:Female n 1 2 3 4 54 years (22-73) 39:30 69 21 10 20 18 47 years (15-69) 19:14 33 8 7 5 13 48 years (42-61) 5:7 12 — — — — test as deemed appropriate. P < 0.05 was considered statistically significant; P < 0.1 was considered marginally significant. Results The number of cases in each disease, including the successive stages, age, and sex of patients, are summarized in Table 2. All cases showed necroinflammatory activity graded as mild or moderate without any showing confluent necrosis sufficient to grade it as severe activity. Fig. 1. EpCAM staining in early and late stage chronic viral hepatitis. (A) EpCAM stain in chronic hepatitis C with portal fibrosis highlights bile ducts and ductules (cytoplasmic staining) and a cluster of periportal hepatocytes (membranous staining). (B) On K19 stain of a sequential section, there is no positivity in hepatocytes. (C) EpCAM stain of hepatitis B cirrhosis shows cytoplasmic staining of biliary structures. Ductular reactions, inclusive of intermediate cells show some cytoplasmic staining, but also membranous staining. The hepatocytes surrounding the ductular reactions show extensive membranous staining. (D) K19 stain of a sequential section lacks intermediate cell and hepatocyte staining. (E, F) On double staining for EpCAM and K19, all cells of the ductular reaction and surrounding hepatocytes with K19 expression (blue) are also EpCAM(þ) (brown). Original magnifications: 200 (A, B, E), 40 (C, D, F). 967 Immunohistochemistry. Examples of EpCAM and K19 stains are shown in Fig. 1. In all livers, normal and diseased, EpCAM expression was seen in the cytoplasm of cholangiocytes of all branches of the biliary tree, including canals of Hering, ductules, and small and large bile ducts (Fig. 1A,C). In normal liver, hepatocytes were rarely if ever positive for EpCAM (2 of 12 samples) and showed only membranous staining (data not shown). In diseased liver specimens, hepatocellular staining was also membranous, whereas staining of the intermediate cells of the ductular reactions ranged from cytoplasmic to membranous, depending on the degree of hepatocellular differentiation. We compared staining using all three immunohistochemistry methods, by circulating sequential slides from all three institutions to each institution. Circulated slides included normal controls, early stage CHC, and CHB cirrhosis. Neither the institutional staining investigators (R. K., P. H., Y. N. P.) nor the central coordinating pathologist (N. D. T.) noted any differences in staining intensity or pattern of 968 YOON ET AL. HEPATOLOGY, March 2011 Table 3. Expression of EpCAM in Hepatocytes of Livers with Chronic Hepatitis, Semiquantitatively Assessed by Way of Immunohistochemistry Extent of EpCAM Hepatocyte Staining Stage of Disease Control livers Portal fibrosis (stage 1) Fibrous septa (stage 2) Transition to cirrhosis (stage 3) Established cirrhosis (stage 4) 0 11 21 31 41 10 12 4 1 0 2 14 6 2 5 0 3 5 10 8 0 0 2 12 8 0 0 0 0 10 localization, emphasizing the ease and reliability of staining for this antigen with diverse clones, methods of antigen retrieval, and detection procedures (data not shown). When sequential slides were stained for EpCAM and K19, in all stages of chronic hepatitis, EpCAM(þ) hepatocytes were always located in contiguity with K19(þ) ductular cells, with the EpCAM(þ) cells arrayed around the periphery of ductular reactions (Fig. 1A-D). In 12 cases in which double staining for EpCAM and K19 was accomplished (stages 1-4), all cells of the ductular reaction and surrounding hepatocytes with K19 expression were also EpCAM(þ) (Fig. 1E,F), and EpCAM(þ)/K19() cells, particularly hepatocytes, increased with increasing stage of disease (data not shown). Table 3 summarizes the semiquantitative assessment of the extent of EpCAM(þ) hepatocyte staining in biopsy specimens according to the stage of chronic hepatitis. Normal livers had no EpCAM hepatocyte staining, or only slight staining (<5%). The extent of EpCAM(þ) hepatocytes, overall, increased in parallel with the stage of disease. Only cirrhotic livers had 4þ (>50%) of parenchyma displaying membranous EpCAM staining. There was no association between hepatocyte EpCAM expression and grade of necroinflammation, nor were there significant differences between livers of comparable stage between those with CHC versus CHB. As expected, p21WAF1/Cip1 and PCNA were expressed in cell nuclei. Labeling indices were calculated for various cell types of normal livers (bile duct lining cells, canal of Hering cells, hepatocytes) and of CHB cirrhotic livers (bile duct lining cells, hepatobiliary cells of ductular reactions, hepatocytes) (Fig. 2; Supporting Tables 1 and 2), including EpCAM(þ) versus EpCAM() hepatocytes (Fig. 3). For both antigens, there were statistically significant labeling index differences between CHB cirrhosis and normal controls, concerning all epithelial cell types. In particular, hepatocytes in cirrhosis showed significantly increased p21 expression compared with hepatocytes in normal livers, whereas reactive ductular cells had even more marked difference from the normal canal of Hering cells (Fig. 2A). In addition, the cells of ductular reactions showed markedly elevated proliferation rates (measured by PCNA expression) compared with all other cell types of normal or diseased liver (Fig. 2B). Whereas hepatocytes in cirrhosis had a wider rate of proliferation than those in normal liver, the difference did not reach statistical significance in this study. Fig. 2. Labeling indices for (A) p21 and (B) PCNA in normal liver versus hepatitis B cirrhosis. CoH, canals of Hering. HEPATOLOGY, Vol. 53, No. 3, 2011 YOON ET AL. 969 shortening from ductular reaction to EpCAM(þ) hepatocytes and to EpCAM() hepatocytes (Fig. 5B). Discussion Fig. 3. Labeling indices for (A) p21 and (B) PCNA in EpCAM(þ) versus EpCAM() hepatocytes in hepatitis B cirrhosis. CoH, canals of Hering. p21 and PCNA labeling indices showed no significant difference between EpCAM(þ) hepatocytes and EpCAM() hepatocytes (Fig. 3). Telomere Length Evaluation. The telomere lengths were measured by studying from 50 to 214 telomere dots (telomere length signal detected by quantitative fluorescence in situ hybridization) according to cell type in nine cases of normal liver (Fig. 4G; Supporting Table 3). In normal liver, there was no significant difference in telomere lengths among normal hepatocytes, canal of Hering cells and bile duct cells (Fig. 5A), nor did they differ according to age or sex. In cirrhotic livers, the telomere lengths were measured by studying from 33 to 189 telomere dots according to cell type in six cases (Fig. 4G; Supporting Table 4). When comparing the telomere lengths between EpCAM(þ) hepatocytes and EpCAM() hepatocytes in cirrhosis, the telomere lengths of EpCAM() hepatocytes were significantly shorter than those of EpCAM(þ) hepatocytes (P ¼ 0.046). In addition, EpCAM(þ) hepatocytes showed relatively shorter telomere length than ductular reactions (P ¼ 0.057), whereas EpCAM() hepatocytes showed significantly shorter telomere length than ductular reactions (P ¼ 0.016) (Figs. 4 and 5A). There was no significant difference in telomere length according to patient age in both cirrhotic and normal livers. When the telomere lengths of ductular reactions, EpCAM(þ) hepatocytes, and EpCAM() hepatocytes were traced in each patient, there was gradual telomere A growing body of work in the last few decades has identified cells of the ductular reactions in human livers in diverse but usually severe acute and chronic liver diseases as being the equivalent of the oval cells seen in rodent models of injury.1,2,5,11-16,18 As such, the ductular reactions are thought to be the transit amplifying cells deriving from activation of the stem cell compartments of the liver.1,7 Like oval cells, the cells are thus thought to have at least two possible differentiation pathways, toward hepatocytes and toward cholangiocytes, the dominant direction being determined by the presence of injury and the nature and severity of that injury. In diseases with a predominance of hepatocyte injury, the ductular reaction is triggered by acute destruction of large amounts of parenchyma11 or by senescence of hepatocytes by chronic low level injury, and presumably results in hepatocyte replenishment from the stem/progenitor cell compartments.13- 15 In acute liver failure from acetaminophen toxicity, three-dimensional reconstruction of K19(þ) ductular reactions suggested that many hepatocytes appeared to be deriving from the proximal, smallest branches of the biliary tree (i.e., the canals of Hering and ductules), which comprise a stem cell niche of mammalian livers.11 In chronic liver disease, similar three-dimensional reconstruction showed that ductular reactions in chronic viral hepatitis (CHB and CHC), autoimmune hepatitis, and fatty liver diseases likewise gave rise to hepatocyte buds indicating hepatocyte repopulation.13- 15 Studies of proliferation in these settings, with PCNA or Ki-67 as proliferation markers, supported this hypothesis by confirming that ductular reactions are highly proliferative, as one would expect in transit amplifying cells involved in stem cell–derived repopulation.13,20 That this process is likely triggered by increasing inability of hepatocytes themselves to replicate after years or decades of injury in chronic disease was then confirmed by immunohistochemical evaluation of p21 as a marker of senescence.14,15 As hepatocytes become increasingly senescent in later stages of diseases, indicated by increasing p21 expression with advancing stage, only then does the ductular reaction emerge, suggesting that stem cells have taken over the burden of hepatic restitution. 970 YOON ET AL. HEPATOLOGY, March 2011 Fig. 4. Quantitative fluorescence in situ hybridization for telomere length assessment combined with immunohistochemical stain for EpCAM. The red and green signals in the nuclei correspond to telomere and centromere signals, respectively. Red EpCAM(þ) immunostaining can be seen on the cell membranes of bile ducts, ductular reactions, canals of Hering, and some hepatocytes. (A-D) Representative features of bile duct (A), ductular reaction (B), EpCAM(þ) hepatocytes (C), and EpCAM() hepatocytes (D) in hepatitis B viral cirrhosis. (E, F) Representative features of hepatocytes (E), canals of Hering (arrows) (E), and bile ducts (F) in normal liver. (G) Number of telomere dots according to telomere length in various cell types in cirrhosis (above) and in normal liver (below). Telomere length was measured by the ratio of telomere fluorescence intensity and centromere fluorescence intensity in each telomere dot. HEPATOLOGY, Vol. 53, No. 3, 2011 Fig. 5. Telomere lengths in various cell types. (A) Telomere lengths in epithelial cell types of hepatitis B viral cirrhosis and normal human liver. (B) Telomere lengths in various cell types of 6 patients with hepatitis B viral cirrhosis. Only two studies in humans, however, have actually provided cell tracking data to support the idea that cells of the ductular reaction become hepatocytes. In the first, a male patient with hepatitis C cirrhosis underwent liver transplantation and received an organ from a female donor, but then developed severe acute injury in the form of fibrosing cholestatic recurrent hepatitis C.21 Using colocalization of Y chromosome (by way of fluorescence in situ hybridization) and K8/ 18 (by way of immunohistochemistry), 40% of the hepatocytes in the afflicted liver bore Y chromosomes, indicating derivation from the recipient (probably of YOON ET AL. 971 bone marrow origin). However, not only were cells of the ductular reaction frequently Y chromosome–bearing, but hepatocytes adjacent to the ductular reaction were more likely to be Y-positive than those in the perivenular regions (64% versus 16%, respectively). These data imply that ductular reaction cells become new hepatocytes, though in this disease setting the full lineage pathway appeared to be from bone marrow to ductular reaction to hepatocyte. The second study, by Lin et al,.16 concerns cirrhosis that developed in several chronic liver diseases, and used analysis of mutations in mitochrondrial DNA encoding cytochrome c oxidase enzyme. This study unambiguously demonstrated the derivation of hepatocytes containing distinct mutations as deriving from adjacent ductular reactions with the identical mutation (a majority of cirrhotic nodules, furthermore, being clonal, suggesting derivation from a single stem/progenitor cell within a preexisting canal of Hering). In related, but separate lines of investigation, marker studies of these hepatobiliary lineages have revealed a variety of important molecules that indicate varying shades of hepatocyte and biliary commitment. Of particular importance have been studies showing that EpCAM is a marker of the hepatobiliary stem cell niche and that when such cells develop into hepatocytes in culture, the new hepatocytes as well as the cells with intermediate features between stem/progenitor cells and hepatocytes also display membranous EpCAM. 2,16 These findings led us to hypothesize that EpCAM(þ) hepatocytes are derived relatively recently from the stem cell niche rather than from other, preexisting hepatocytes. The goal of the present study was to investigate this possibility within intact tissue specimens from livers of patients with hepatitis B and C through several means. The first is by determining whether EpCAM(þ) hepatocytes develop only in the context of ductular reactions, stage by stage, and exploring the topological relationships of these cells (Fig. 1 and Table 3). Four important points support our primary hypothesis: (1) EpCAM(þ) hepatocytes, like ductular reactions, increase in frequency and extent with increasing stage of disease; (2) although ductular reactions sometimes do not have associated EpCAM(þ) hepatocytes, EpCAM(þ) hepatocytes, when present, are always associated with ductular reactions; (3) EpCAM(þ) hepatocytes always appear as aggregates surrounding a core of ductular reaction cells; and (4) cells of intermediate morphology between the smallest progenitor cells of the ductular reaction and mature appearing, EpCAM(þ) hepatocytes are always also EpCAM(þ). 972 YOON ET AL. Thus, morphologically, topographically, and immunophenotypically, EpCAM(þ) hepatocytes appear to derive from cells of the ductular reaction. Such data, although compelling, are incomplete. We thus hypothesized that if EpCAM(þ) hepatocytes were stem cell–derived, they would have telomere lengths that were longer than those of the EpCAM() hepatocytes. This hypothesis is based on prior data indicating that ductular reactions have increased telomerase activation22-25 and that senescent hepatocytes, after years of increased cell turnover, would have shortened telomeres.26-29 We would also expect that EpCAM() hepatocytes in cirrhosis would have telomeres that would be shorter than those in EpCAM(þ) hepatocytes, and that telomere length of EpCAM(þ) hepatocytes would be shorter than that in ductular reactions. These predictions were confirmed in a statistically meaningful way for hepatocytes in CHB cirrhosis. We also sought to explore issues of proliferation and senescence as previous studies had done,13-15,20 but discriminating between hepatocytes that were EpCAM(þ) and those that were EpCAM(). However, there was no significant difference of PCNA and p21 labeling indices between EpCAM(þ) hepatocytes and EpCAM() hepatocytes. We have no clear explanation for these findings, though we suspect that the variable nature of staining for both p21 and PCNA in regard to fixation and staining conditions plays an important role; study of freshly prepared EpCAM(þ) versus EpCAM() hepatocytes may be required to more fully evaluate their relative senescence and cell cycle status. In summary, we hypothesize that EpCAM(þ) hepatocytes in chronic liver disease represent hepatocytes that have derived from activation of a stem cell compartment of the liver in the setting of chronic hepatitis, whereas EpCAM() hepatocytes in such livers have derived from preexisting hepatocytes. In support of this hypothesis, we present morphologic, topographic, immunophenotypic, and molecular data. Our most compelling data, which are indicative of current functional behavior as well as cell behavior over time, are represented in the finding that EpCAM(þ) hepatocytes have telomere lengths that are longer than those of EpCAM() hepatocytes and shorter than the ones of ductular reactions. This finding is in accord with our hypothesis and with prior published data regarding telomerase activity in hepatic stem cell and transit amplifying cell populations. Because EpCAM is a surface membrane antigen, we can expect that isolation and immunosorting of hepatocytes from fresh liver specimens may yield quite HEPATOLOGY, March 2011 interesting data regarding the nature of liver regeneration in both acute and chronic liver diseases, with stronger statistical significance than found in this archival tissue study. Moreover, these data may have practical implications regarding selection of hepatocytes for use in therapeutic cell transplantation or in populating of artificial liver assist devices. References 1. Theise ND. Gastrointestinal stem cells. III. Emergent themes of liver stem cell biology: niche, quiescence, self-renewal, and plasticity. Am J Physiol Gastrointest Liver Physiol 2006;290:G189-G1893. 2. Zhang L, Theise N, Chua M, Reid LM. The stem cell niche of human livers: symmetry between development and regeneration. HEPATOLOGY 2008;48:1598-1607. 3. Kung JW, Forbes SJ. Stem cells and liver repair. Curr Opin Biotechnol 2009;20:568-574. 4. Mishra L, Banker T, Murray J, Byers S, Thenappan A, He AR, et al. Liver stem cells and hepatocellular carcinoma. HEPATOLOGY 2009;49: 318-329. 5. Alison MR, Islam S, Lim S. Stem cells in liver regeneration, fibrosis and cancer: the good, the bad and the ugly. J Pathol 2009;217: 282-298. 6. Kofman AV, Morgan G, Kirschenbaum A, Osbeck J, Hussain M, Swenson S, et al. Dose- and time-dependent oval cell reaction in acetaminopheninduced murine liver injury. HEPATOLOGY 2005;41:1252-1261. 7. Kuwahara R, Kofman AV, Landis CS, Swenson ES, Barendswaard E, Theise ND. The hepatic stem cell niche: identification by label-retaining cell assay. HEPATOLOGY 2008;47:1994-2002. 8. Petersen B, Shupe T. Location is everything: the liver stem cell niche. HEPATOLOGY 2008;47:1810-1812. 9. Oh SH, Witek RP, Bae SH, Zheng D, Jung Y, Piscaglia AC, et al. Bone marrow-derived hepatic oval cells differentiate into hepatocytes in 2-acetylaminofluorene/partial hepatectomy-induced liver regeneration. Gastroenterology 2007; 132:1077-1087. 10. Theise ND, Badve S, Saxena R, Henegariu O, Sell S, Crawford JM, et al. Derivation of hepatocytes from bone marrow cells in mice after radiation-induced myeloablation. HEPATOLOGY 2000;31:235-240. 11. Theise ND, Saxena R, Portmann BC, Thung SN, Yee H, Chiriboga L, et al. The canals of Hering and hepatic stem cells in humans. HEPATOLOGY 1999;30:1425-1433. 12. Roskams TA, Theise ND, Balabaud C, Bhagat G, Bhathal PS, BioulacSage P, et al. Nomenclature of the finer branches of the biliary tree: canals, ductules, and ductular reactions in human livers. HEPATOLOGY 2004;39:1739-1745. 13. Falkowski O, An HJ, Ianus IA, Chiriboga L, Yee H, West AB, et al. Regeneration of hepatocyte ‘buds’ in cirrhosis from intrabiliary stem cells. J Hepatol 2003;39:357-364. 14. Richardson MM, Jonsson JR, Powell EE, Brunt EM, NeuschwanderTetri BA, Bhathal PS, et al. Progressive fibrosis in nonalcoholic steatohepatitis: association with altered regeneration and a ductular reaction. Gastroenterology 2007;133:80-90. 15. Clouston AD, Powell EE, Walsh MJ, Richardson MM, Demetris AJ, Jonsson JR. Fibrosis correlates with a ductular reaction in hepatitis C: roles of impaired replication, progenitor cells and steatosis. HEPATOLOGY 2005;41:809-818. 16. Lin WR, Lim SN, McDonald SA, Graham T, Wright VL, Peplow CL, et al. The histogenesis of regenerative nodules in human liver cirrhosis. HEPATOLOGY 2010;51:1017-1026. 17. de Boer CJ, van Krieken JH, Janssen-van Rhijn CM, Litvinov SV. Expression of Ep-CAM in normal, regenerating, metaplastic, and neoplastic liver. J Pathol 1999;188:201-206. 18. Schmelzer E, Wauthier E, Reid LM. The phenotypes of pluripotent human hepatic progenitors. Stem Cells 2006;24:1852-1858. HEPATOLOGY, Vol. 53, No. 3, 2011 19. Theise ND. Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach. Mod Pathol 2007;20(Suppl. 1):S3-S14. 20. Koukoulis G, Rayner A, Tan KC, Williams R, Portmann B. Immunolocalization of regenerating cells after submassive liver necrosis using PCNA staining. J Pathol 1992;166:359-368. 21. Theise ND, Nimmakayalu M, Gardner R, Illei PB, Morgan G, Teperman L, et al. Liver from bone marrow in humans. HEPATOLOGY 2000; 32:11-16. 22. Kotoula V, Hytiroglou P, Pyrpasopoulou A, Saxena R, Thung SN, Papadimitriou CS. Expression of human telomerase reverse transcriptase in regenerative and precancerous lesions of cirrhotic livers. Liver 2002;22:57-69. 23. Youssef N, Paradis V, Ferlicot S, Bedossa P. In situ detection of telomerase enzymatic activity in human hepatocellular carcinogenesis. J Pathol 2001;194:459-465. 24. Harada K, Yasoshima M, Ozaki S, Sanzen T, Nakanuma Y. PCR and in situ hybridization studies of telomerase subunits in human non-neoplastic livers. J Pathol 2001;193:210-217. YOON ET AL. 973 25. Hytiroglou P, Kotoula V, Thung SN, Tsokos M, Fiel MI, Papadimitriou CS. Telomerase activity in precancerous hepatic nodules. Cancer 1998;82:1831-1838. 26. Lee YH, Oh BK, Yoo JE, Yoon SM, Choi J, Kim KS, et al. Chromosomal instability, telomere shortening, and inactivation of p21(WAF1/ CIP1) in dysplastic nodules of hepatitis B virus-associated multistep hepatocarcinogenesis. Mod Pathol 2009;22:1121-1131. 27. Oh BK, Kim YJ, Park C, Park YN. Up-regulation of telomere-binding proteins, TRF1, TRF2, and TIN2 is related to telomere shortening during human multistep hepatocarcinogenesis. Am J Pathol 2005;166: 73-80. 28. Plentz RR, Park YN, Lechel A, Kim H, Nellessen F, Langkopf BH, et al. Telomere shortening and inactivation of cell cycle checkpoints characterize human hepatocarcinogenesis. HEPATOLOGY 2007;45: 968-976. 29. Kim H, Oh BK, Roncalli M, Park C, Yoon SM, Yoo JE, et al. Large liver cell change in hepatitis B virus-related liver cirrhosis. HEPATOLOGY 2009;50:752-762.