This was indeed a little tricky question and only 6% of our
advertisement

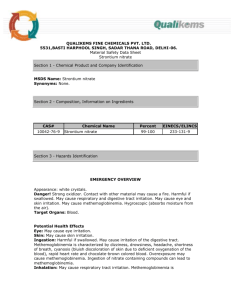
C. Administer methylene blue. This was indeed a little tricky question and only 6% of our respondents got it correct. The explanation that follows will leave us all better informed and educated. The abrupt fall in oxygen saturation confirmed the physical finding of cyanosis and indicated an acute change in the ability of hemoglobin to bind oxygen. The most likely explanation for these findings in this patient is an acute episode of methemoglobinemia. An arterial blood gas analysis would have supported the diagnosis of methemoglobinemia by showing an adequate PO with a reduced saturation. Co-oximetry would confirm the diagnosis by directly measuring methemoglobin levels. Methemoglobinemia is caused by exposure of blood to chemicals that oxidize the iron in hemoglobin from the ferrous state (Fe2+) to the ferric state (Fe3+). Because methemoglobin cannot bind oxygen, an acute increase in methemoglobin levels will cause a fall in oxygen saturation. Local anesthetics, such as lidocaine, are known oxidizing agents. Lidocaine is well absorbed systemically through the tracheobronchial mucosa and has been rarely associated with methemoglobinemia during endoscopic procedures. 2 Methemoglobinemia can usually be successfully managed by withdrawing the offending agent (ie, no further administration of lidocaine). In this case, however, administration of methylene blue to acutely correct the methemoglobinemia would be the most appropriate next step for several reasons. Evaluating symptoms related to methemoglobinemia in this patient would have been difficult because the patient had been sedated with midazolam for the procedure. Patients with a genetic deficiency in NADH-methemoglobin reductase tolerate chronic methemoglobinemia well, but an abrupt increase in methemoglobin levels, as in this case, leaves less time for compensation. Pulse oximetry has been reported to poorly reflect the degree of desaturation in methemoglobinemia. Earlier studies suggested that pulse oximetry might plateau at 85% despite markedly elevated levels of methemoglobin. Newer pulse oximeter models, however, deal with methemoglobin interference in various ways and may be more accurate in reflecting the degree of desaturation in methemoglobinemia. This patient had marked desaturation by pulse oximetry that was confirmed by co-oximetry. Methylene blue is administered in a dose of 1 to 2 mg/kg body weight intravenously over 5 minutes. The dose may be repeated in an hour. Although methemoglobinemia is a rare complication of lidocaine administration, stocking a code cart with methylene blue might be considered in areas in which lidocaine is frequently used. A concern about administering methylene blue is the potential for causing hemolysis. Oxidant stress can cause both methemoglobinemia and hemolysis. Enzymes in erythrocytes that both reduce methemoglobin and protect from oxidant-induced hemolysis depend in part on NADPH. Methylene blue augments the ability of NADPH-methemoglobin reductase to reduce methemoglobin. It has been speculated that methylene blue might deplete NADPH-methemoglobin reductase through correction of methemoglobinemia and predispose to hemolysis. This might especially be the case in patients with glucose-6-phosphate dehydrogenase deficiency who have an impaired ability to produce NADPH. This patient, who was a woman, would be much less likely to have such a deficiency. Most case reports describe methylene blue as being well tolerated. Large series have shown that the incidence of bronchospasm and laryngospasm related to bronchoscopy are extremely low. The absence of respiratory distress, wheezing, and stridor on physical examination makes these possibilities unlikely in this case. Consequently, bronchodilators would not be of value. Neither intubation nor administration of corticosteroids would be needed with the prompt administration of methylene blue. Thanks for your participation..