Temperature Change in Human Muscle During and After Pulsed
advertisement

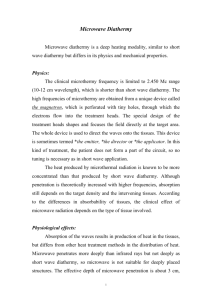
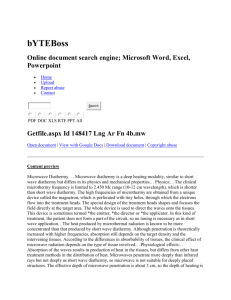
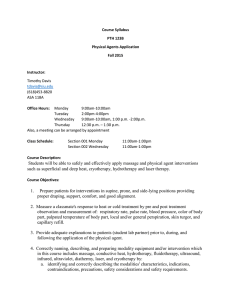
Journal of Orthopaedic & Sports Physical Therapy 1999;29(1):13-22 Temperature Change in Human Muscle During and After Pulsed Short-Wave Diathermy David 0.Draper, EdD, ATC1 Kenneth Knight, PhD, ATC2 1 Fujiwara, MD, PhD, PT3 ). Chris Caste14 Study Design: A time series design was used, with the dependent variable being gastrocnemius muscle temperature at a depth of 3 cm. Objectives: To determine the rate of temperature rise and the rate of post-treatment temperature decline in skeletal muscle following the application of pulsed short-wave diathermy (PSWD). Background: Data on PSWD rate and longevity of heating are 20 years old and outdated. With the recent introduction of advanced diathermy equipment, results of our study would provide clinicians with much needed information regarding treatment duration. Methods and Measures: A 23-gauge thermistor was inserted into the center of the medial head of the anesthetized gastrocnemius muscle, 3 cm below the skin's surface of 20 subjects. The PSWD (27.12 MHz frequency) was applied using the following parameters: 800 bursts per second; 400 psecond burst duration; 850 pecond interbunt interval; with a peak root mean square (RMS) amplitude of 150 W per burst and an average RMS output of 48 W. Temperature changes were documented every 5 minutes during the treatment and additionally at 5 and 10 minutes following treatment. Results: The average baseline and peak temperatures were 35.84 2 0.93OC and 39.80 + 0.83"C, respectively. Mean temperature increases were: 1.36 0.90°C (5 min); 2.87 2 1.44"C (10 min); 3.78 2 1.lg°C (15 min); 3.49 1.13"C (20 min). After the treatment terminated, intramuscular temperature dropped 0.97 0.68"C in 5 minutes and 1.78 0.69" in 10 minutes. Conclusions: PSWD is an effective modality if temperature elevation of deep tissue over a large area is the clinical objective. ) Orthop Sports Phys 7her 1999;29:13-22. + + + + Key Words: diathermy, heat, ultrasound Professor and Director of Graduate Athletic Trainingand Sports Medicine, Brigham Young Universify Provo, Utah Professor of Athletic Training at Brigham Young Universify Provo, Utah Professor of O~hopaedicsand Physical Therapy, Shinshu Universify Matsumoto, japan Vice President ofAccelerated Care Plus-LLC, Topeka, Kan hrtially funded by Accelerated Care Plus-LLC, 6700 S.W. Topeka Blvd, Topeka, KS 66619 Send correspondence to Dr. David 0.Draper, Brigham Young Universify RB 122, Provo, UT 84602. lthough rarely used in clinical practice, pulsed short-wave diathermy (PSWD)3.22.23 produces an increase in tissue temperature, which in turn results in desirable therapeutic effects such as pain relief,34 muscle relaxation,4JVncreased blood f l o ~ , ' . ' extensibility ~.~~ of collagen tissue,' decreased joint stiffness:.21 and enhanced recovery from hematomas and ligamentous i n j ~ r y .In ~ ,part, ~ the lack of use of pulsed short-wave diathermy exists because of a shortage of controlled studies, which have quantified the dosage and the resulting effects; inadequate device design, which causes radio interference with medical devices, computers, and communications equipment; and unquantified electromagnetic radiation exposure to the operator and patient.I5J7Information on diathermy heating is outdated17 because of engineering improvements in recently developed units. For instance, improved shielding from electromagnetic waves not only protects the patient, but may also heat the target tissues more effectively.17 During the past 8 years, we have studied the rate of tissue tempera- A ture increase and decay following ultrasound applicat i o n ~ . ~This . ~ .information ~ provides dose-response and heating time frames for therapists to use when treating patients with ultrasound. These standards were established in human muscle and tendon. They are limited to an area 2 times the effective radiating area of the transducer (approximately twice the size of the soundhead) because we have discovered that ultrasound can only heat this small an area.5.MR In contrast to ultrasound, PSWD is capable of heating large areas of the body.Iw0 Guidelines, however, regarding the rate of heating during, and the rate of tissue temperature decay following the application of PSWD with updated and improved diathermy devices have not yet been established. The purpose of this study was to measure the rate of temperature rise and decay in human muscle during PSWD treatments and use these data to establish treatment guidelines. METHODS We used a time series design with intramuscular (IM) temperature as the dependent variable. In each subject, IM temperature measurements were taken before the application of and at 5, 10, 15, and 20 minutes during the application of the PSWD. In a similar fashion IM temperature measurements were taken at 5 and 10 minutes after the treatment was finished. FIGURE 1. A 23-gauge thermistor was inserted into the center of the medial head of the gastrocnemius muscle, 3 cm below the skin's surface at the muscle's greatest girth. Physitemp Instruments, Clifton, NJ) interfaced with a Bailey Instruments BAT-10 monitor (Physitemp Instruments) that displayed the temperature in degrees Celsius. The accuracy of temperature recordings of the probe is within O.l°C, and the monitor is accurate to within O.l°C (manufacturer's data); therefore, the worst case error would be 2 0.2"C. Procedures While the subject was lying prone on a table, one of the investigators (DD) used a caliper to plot the depth for the insertion of the thermistor." A 1-mL injection of 1% lidocaine (Xylocaine) was administered subcutaneously to anesthetize the area. The thermis tor was inserted into the center of the medial head Twenty college students (12 men, 8 women) with a of the gastrocnemius muscle, 3 cm below the skin's surface at the muscle's greatest girth (Figure 1). mean age of 22.4 2 2.0 years volunteered to particiThe diathermy drum was 200 cm2 and had a 2.5 pate in this investigation. Inclusion criteria were that cm space plate to protect the tissue from direct conthe left triceps surae muscle mass was free from ecchymosis, swelling, or injury for at least 3 months be- tact with the electrode, so toweling was not necessary during operation. We placed the diathermy drum fore participation in the study. The study was a p onto the posterior aspect of the muscle belly with proved by the Institutional Human Subjects Review the space plate in contact with the subject's skin. We Board at Brigham Young University. All participants positioned the drum so that the tip of the thermistor signed a consent form after they were informed of was in direct line with the center of the drum (Figthe risks involved in the experiment. ure 2). Before turning on the diathermy unit, we recordInstruments ed baseline temperature, then pulled out the probe to avoid electromagnetic interference and local heatThe diathermy unit used to gather our data was ing effects on the metal probe. Diathermy was a p the Megapulse (Accelerated Care Plus-LLC, Topeka, plied for 20 minutes at the following settings: 800 Kan) with an operating frequency of 27.12 MHz and a pulsed mode yielding 800 bursts per second. An in- bursts per second; 400-psecond burst duration; 850psecond interburst interval with a peak root mean duction drum coil electrode was used to deliver the square amplitude of 150 W per burst and an average electromagnetic energy. The unit was new and was root mean square output of 48 W. We briefly (10 seccalibrated by the manufacturer before the start of onds) interrupted the treatment at 5-minute intervals the study. Muscle and room temperature were measured with to reinsert the probe and record temperature. At the completion of the 20-minute treatment the unit was a 23gauge thermistor needle (Phystek MT-23/5, J Orthop Sports Phys Ther.Volurne 29.Number 1 .Januar). 1999 34 + -5 FIGURE 2. Position of the diathermy drum and its relationship to the thermistor. turned off, and we recorded temperature decay at 5 and 10 minutes following treatment. At the end of the recording, we removed the thermistors, cleaned the area with 70% isopropyl alcohol, and applied a bandage to the area. Statistical Analysis Differences in baseline tissue temperatures and the temperatures recorded at specific intervals (5 min, 10 min, 15 min, and 20 min) were calculated and averaged. A 1-way ANOVA with repeated measures was computed ( P = .01). Differences between individual pairs of means was established with Tukey post hoc tests ( P = .05). I Heating - 0 7 1 5 10 15 Decay - 20 1 25 30 Time (minutes) FIGURE 3. Intramuscular (gastrocnemius; 3 cm deep) temperatures during heating and 10 minutes of decay resulting from 20 minutes of pulsed shortwave diathermy (PSWD). the tissue, which in turn is converted into an electric field that heats tissue through resistive heating.3' The heat generated is proportional to the absorption of the electric current flow through the tissue.31 Pulsed short-wave diathermy is an appropriate modality for heating deep muscle tissue. Besides micre wave diathermy and ultrasound, it is the only modality able to increase temperatures in tissues that lie more than 2 cm below the epidermis. Before this investigation, little was known regarding the heating rate of PSWD, its peak heating, and the rate of temperature decay after treatment. Rate of Heating RESULTS The rate of temperature increase during applications of PSWD was linear for 15 minutes, after which it decreased (Figure 3). Average temperature increases above baseline were 1.36 2 0.90°C at 5 minutes; 2.87 2 1.44"C at 10 minutes; 3.78 ? 1.19"C at 15 minutes; and 3.49 2 1.13"C at 20 minutes. The average baseline temperature was 35.84 ? 0.93"C and the mean peak temperature was 39.80 2 0.83"C. All temperatures were significantly greater than baseline (F [6, 1721 = 42.9, P = .001, Tukey < .O5). The highest average temperature recorded was at 15 minutes and it remained at this level at the 20-minute measurement. The temperature dropped an average of 0.97 ? 0.6S°C during the first 5 minutes, and 0.81°C at the 10-minute mark, for a total temperature decay of 1.78 2 0.69"C in 10 minutes. This was a significant drop from the peak temperature ( P < .05). DISCUSSION Pulsed short-wave diathermy applied through an inductive field applicator induces a magnetic field in J Orthop Sports Phys Ther.Volume 29.Number 1 .January 1999 Suggested treatment times for this modality range from 10 to 60 minutes." The optimum treatment duration for PSWD is important to determine. Because peak heating occurred at 15 minutes and leveled off by the 20-minute mark in 8 (40%) of our subjects, we feel that 1 5 to 20-minute applications of PSWD at the parameters studied will provide clinically meaningful heating (4°C) in muscle to a depth of 3 cm. Peak Heating Our average peak temperature of 39.80°C, or a 4°C increase over baseline, fits the definition of therapeutic heating range proposed by several researchers. Lehmannl* stated that temperature increases of 1°C can reduce mild inflammation and increase metabolism and that moderate heating, an increase of 2 to 3"C, will decrease pain and muscle spasm. Increasing tissue temperatures more than 3 to 4°C above baseline will increase tissue extensibility, enabling the clinician to treat chronic connective tissue p r o b lems.lHAccording to Behrens and M i c h l o v i t ~opti~~~ mal heating occurs when the tissue temperature rises 15 above 38 to 45°C. The peak heating obtained in our experiment fell within Lehrhann's standards for vigorous heating and reached the lower end of the therapeutic temperature range suggested by Behrens and Michl~vitz.~;~~ Rate of Temperature Decay usually stiff and unyielding until heated.11J9Therefore, greater and more permanent elongation results when a stress is placed on heated tissue.27This also diminishes the risks associated with applying stress on a tissue that is not adequately heated.32.33In our study, peak heating occurred 15 to 20 minutes into the treatment. We suggest a follow-up study to see what effect heating muscle for 15 to 20 minutes via PSWD would have on joint range of motion. The more heat a tissue absorbs, the greater the chance that collagen elongation can occur. Although obtaining therapeutic temperature increases in tissue Indirect Comparisons with Ultrasound is important, the time the tissue will remain heated By far the most popular deep heating modality is at the desired level is equally important. To stretch ultrasound, and it is used much more frequently collagen, Michlovitz suggested that the temperature than PSWD. In surveys of physical therapists in Almust reach and remain between 40 to 45°C for 5 berta, Canada,= and Australia2!' only 0.6% and 8% of rnin~tes.'~ In our study, the mean peak temperature respondents, respectively, used PSWD daily, yet 94% was 0.2OC less than 40°C, but the rate of decay was and 93%, respectively, used ultrasound daily. Pulsed quite slow. Following PSWD, our subject's muscle short-wave diathermy, however, may be a better motemperature decayed only 0.97 2 0.68"C in 5 mindality than ultrasound in some situations. Its rate of utes (from 39.8"C to 38.8"C) and 1.78 -+ 0.69"C (to heating compares favorably to ultrasound and the 38.1°C) in 10 minutes. The rate of temperature delower rate of temperature decay and clinician freecay is slow, especially when compared to previous dom are distinct advantages of this modality over ulstudies of ~ l t r a s o u n d This . ~ ~ ~is probably caused in trasound. On the basis of our research, we believe part by the larger mass of tissue that is affected with that in some situations PSWD might be preferred PSWD, allowing these tissues to retain heat longer. As mentioned earlier, an interesting observation in over ultrasound. The rate of heating with continuous PSWD a p our study was that peak heating occurred at 15 minpears similar to 1 MHz ultrasound when insonating utes and then leveled off for the last 5 minutes of an area 2 times the size of the effective radiating the application. It is possible that the amount of area (ERA) of the crystal. In an earlier study6we reelectromagnetic energy emitted by the device was not sufficient to raise the muscle temperature higher. ported that 1 MHz ultrasound delivered at 1.5 W/cm2 for 10 minutes raised human gastrocnemius Another possibility for this phenomenon has to do muscle temperature 3OC, similar to the present with the "set point" concept postulated by Guyton and Hall.'!' According to their theory, central and lo- 2.87% increase after 10 minutes of PSWD. It a p pears, therefore, that the amount of heating of these cal mechanisms and reflex arcs continually attempt 2 modalities is similar. to maintain the core temperature at a set point esIt has become an all too frequent practice to use tablished by the hypothalamus. Although local temultrasound when attempting to heat large areas such perature is allowed to vary more than core temperaas the entire lumbar region. Ultrasound is ineffective ture, it still has limits, so excessive heat exchange We base this on previfrom locally heated or cooled portions of the body is at heating large areas.5.10.25.28 ous investigations and on the fact that in our experiprevented. Several researchers support this idea and have shown that as temperature increases, blood flow ments we used a template to limit the application increases to help maintain a set t e m p e r a t ~ r e . * J ? J ~ J area ~ . ~ ~to 2 ERA. For example, in a recent study5we heated two different sizes of muscle area (2 ERA and Thus, as PSWD heats tissues near maximum, the in6 ERA) with 1 MHz ultrasound at 1.5 W/cm2 for 10 crease in temperature and blood flow engages the body's natural cooling mechanism in an effort to de- minutes. The smaller area yielded a 3.6OC increase crease tissue damage. During the past decade our re- (moderate to vigorous heating) whereas the larger area only raised l.l°C (mild heating). Thus, treating search team has tested various heat modalities in a large area will dilute the dose and minimize the over 200 subjects in vivo, and we have yet to raise thermal effects. Ultrasound is thus an effective thermuscle temperature higher than 43°C,".7.Wwith avermal modality only when the target area does not exage peak temperatures of 41°C. ceed twice the size of the ERA of the ~ r y s t a l . ~ ~ . ~ ~ Although we did not study whether or not preCompared to our ultrasound head that measured heating muscle with PSWD has any effect on in5 cm2, our diathermy drum had a large surface area creased range of motion via stretching, our data of(200 cm2). There is a possibility, therefore, that diafer a suggested time to stretch the tissues. Gerstenl1 and Lehmann et all9 have reported that the ultimate thermy would heat a larger body area. We recently completed a study to test for the heating area of time to elongate collagenous tissue is at the peak of PSWD.1° We used methods identical to this study, exheating. This occurs because collagenous tissue is 16 J Orthop Sports P h y TheroVolume 290Number 1 *January 1999 cept 3 thermistors were implanted in the triceps surae o f 10 subjects. One thermistor was directly under the center o f the applicator drum, while the other two were implanted at opposite ends, 5 c m f r o m the center probe. A l l three probes measured mean increases in temperature o f 3 t o 4.5"C above baseline. O n the basis o f these results, PSWD heats tissue areas nearly as large as the diameter o f the applicator drum. T h e advent o f managed care has required the clinician t o perform quality work in a short time. Heating with ultrasound requires constant attendance by a therapist o r assistant. Application o f PSWD requires only general supervision o f the patient, and the clinician can work concurrently with another client. This may enable the therapist t o b e more efficient. 9. 10. 11. 12. 13. 14. CONCLUSION 15. Our data demonstrate the rate o f heating during PSWD and the rate o f temperature decay after application. This appears t o b e similar t o previously reported heating with 1-MHz ultrasound. This, coupled with the ability t o operate the unit without constant monitoring by the therapist, makes i t a useful modality for heating tissue before stretching and exercise. Pulsed short-wave diathermy hasn't been used much as a therapeutic modality in the past 20 year^.^.^^ Many recent graduates have n o t been exposed t o this technology and use ultrasound as the only modality t o heat deep tissue.= Our data justify the use o f PSWD as a modality capable o f heating large, deep muscle tissue. 16. 17. 18. 19. 20. REFERENCES Abramson Dl, Burnett C, Bell Y, Tuck S. Changes in blood flow, oxygen uptake and tissue temperatures produced by therapeutic physical agents. Am] Phys Med. 1960;47:5162. Akyurekli D, Gerig LH, Raaphorst GP. Changes in muscle blood flow distribution during hyperthermia. Int 1 Hyperthermia. 1997;13:481-496. Behrens BJ, Michlovitz SL. Physical Agents: Theory and Practice for the Physical Therapist Assistant. Philadelphia: F.A. Davis Company; 1996. Brown M, Baker RD. Effect of pulsed short wave diathermy on skeletal muscle injury in rabbits. Phys Ther. 1987;67:208-213. Chudleigh DW, Schulthies SS, Draper DO, Myrer JW. Muscle Temperature Change during Ultrasound Treatments of 2 and 6 ERA [master's thesis]. Brigham Young University, Provo, Utah; 1997. Draper DO, Castel JC, Caste1 D. Rate of temperature increase in human muscle during 1 MHz and 3 MHz continuous ultrasound. ] Orthop Sports Phys Ther. 1995;22: 142-1 50. Draper DO, Ricard MD. Rate of temperature decay in human muscle following 3 MHz ultrasound: The stretching window revealed. ] Athl Train. 1995;30:304-307. Emami B, Song CW. Physiological mechanisms in hyperJ Orthop Sports Phys Ther .Volume 29. Number 1 .January 1999 21. 22. 23. 24. 25. 26. 27. 28. 29. thermia: A review. Int] Radiat Oncol Biol Phys. 1984;lO: 289-295. Fenn JE. Effect of pulsed electromagnetic energy (Diapulse) on experimental haematomas. Can Med Assoc l . 1969;100:251-253. Garrett C, Draper DO, Knight K. The Differences in Heating Obtained During a 1 M H z Ultrasound Treatment and a Diathermy Treatment in the Human Calf Muscle [master's thesis]. Provo, Utah: Brigham Young University; 1998. Gersten JW. Effect of ultrasound on tendon extensibility. Am I Phys Med. 1955;34:362-369. Guerquin-Kern JL, Palas L, Samsel M, Gautherie M. Microwave hyperthermia: Influence of blood flow and thermoregulation processes. Bull Cancer. 1981;68:273-280. Guyton AC, Hall JE. Textbook of Medical Physiology. 9th ed. Philadelphia: W.B. Saunders; 1996:918-919. Hansen TI, Kristensen JH. Effect of massage, shortwave diathermy and ultrasound upon 133Xedisappearance rate from muscle and subcutaneous tissue in the human calf. Scand ] Rehabil Med. 1973;5:179-182. Hellstrom RO, Stewart WF. Miscarriages among female physical therapists who report using radio- and microwave-frequency electromagnetic radiation. Am ] Epidemiol. 1993;138:775-785. Hume SP, Robinson JE, Hand JW. The influence of blood flow on temperature distribution in the exteriorized mouse intestine during treatment by hyperthermia. Br I Radiol. 1979;52:219-222. Kitchen S, Partridge C. Review of shortwave diathermy continuous and pulsed patterns. Physiotherapy. 1992;78: 243-252. Lehmann JF. Therapeutic Heat and Cold. 4th ed. Baltimore: Williams & Wilkins; 1990. Lehmann JF, Masock AJ, Warren CG, Koblanski JN. Effect of therapeutic temperatures on tendon extensibility. Arch Phys Med Rehabil. 1970;51:481-487. Lehmann JF, McDougall JA, Guy AW, Warren CG, Esselman PC. Heating patterns produced by shortwave diathermy applicators in tissue substitute models. Arch Phys Med Rehabil. 1983:64:575-577. Lehrnann JF, warren CG, Scham SM. Therapeutic heat and cold. Clin Orthop. 1974;99:207-245. Lindsay DM, Dearness J, McGinley CC. Electrotherapy usage trends in private physiotherapy practice in Alberta. Physiother Can. 1995;47:30-34. Lindsay DM, Dearness J, Richardson C, Chapman A, Cuskelly G. A survey of electromodality usage in private physiotherapy practices. Aust ] Physiother. 1990;36:249256. McMeeken JM, Bell C. Effects of microwave irradiation on blood flow in the dog hindlimb. Exp Physiol. 1990;75: 367-374. Michlovitz S. Thermal Agents in Rehabilitation. Philadelphia: F.A. Davis Company; 1996. Millard JB. Effect of high frequency currents and infra-red rays on the circulation of the lower limb in man [abstract]. Ann Phys Med. 1961;6:45. Reid DC. Sports Injury Assessment and Rehabilitation. New York: Churchill Livingstone; 1992. Reid DC, Cummings GE. Factors in selecting the dosage of ultrasound with particular reference to the use of various coupling agents. Physiother Can. 1973;25:5-9. Robinson SE, Buono MJ. Effect of continuous-wave ultrasound on blood flow in skeletal muscle. Phys Ther. 1995;75:145-150. 17 30. Rose S, Draper DO, Schulthies SS, Durrant E. The stretching window. Part two: Rate of thermal decay in deep muscle following 1 MHz ultrasound. J Athl Train. 1996;31: 139-1 43. 31. Starkey C. Therapeutic Modalities for Athletic Trainers. Philadelphia: FA Davis; 1993. 32. Warren CG. Heat and stretch procedures: An evaluation using rat tail tendon. Arch Phys Med Rehabil. 1976;57: 122-1 26. 33. Warren CG, Lehmann JF, Koblanski JN. Elongation of rat tail tendon: Effect of load and temperature. Arch Phys Med Rehabil. 1971;52:465474. 34. Wilson DH. Treatment of soft tissue injuries by pulsed electrical energy. Br Med 1. 1972;2:269-270. J Orthop Sports Phys Ther.Volume 29.Number 1 .January 1999 Invited Commentary Draper, Knight, Fujiwara, and Castel need to be commended for bringing the topic of short-wave diathermy back into current conversation among physical therapists. These investigators provide evidence of significant muscle heating after 30 minutes of treatment with pulsed short-wave diathermy (average increase of 3.49 to 3.78"C). It is of note that the temperature increase reached a plateau after 15 minutes of treatment, the temperature did not increase into the rigorous heating range, and the temperature elevation was not even maintained 5 minutes after the treatment (returning to approximately 1°C of normal body temperature 10 min after treatment). The findings of this study were somewhat surprising given the use of a "pulsed" rather than "continuous" short-wave diathermy. The historical rationale for the development of the interrupted mode of short-wave diathermy was to maximize the mechanical and piezoelectric effects while minimizing tissue heating."." This mode of diathermy has been compared to the pulsating mode of ultrasound, where acute injuries can be treated without delivering heat. BENEFITS OF DEEP HEAT Short-wave diathermy, along with ultrasound, is classified as a deep heating modality. Both ultrasound and diathermy elevate tissue temperature by conversion of energy to heat. Both are thought to penetrate to a depth of 2.54 cm (1 inch) or more and are beneficial in terms of increasing tissue temperature, blood flow, vasodilation, metabolism, and tissue extensibility. Heating can increase the rate of healing by enhancing the transfer of metabolites across cell membranes, providing for greater concentration of white cells and antibodies, increasing the transport rate of toxins, engulfing bacteria and debris away from the treated area, and enriching the environment with o ~ y g e n . " ~ The J ~ ~heat ~ can promote relaxation of muscles and provide relief of muscle Heat can also change tissue tolerances, modify the firing of sensory nerves, and contribute to a decrease in pain.I"oth ultrasound and diathermy have a piezoelectric effect, which has been shown to increase hydroxyproline and collagen dep~sition.~.'~ Although ultrasound and diathermy have similarities, they have significant differences. First, ultrasound is one of the most common modalities used J Orthop Sports Phys Ther-Volume 29-Number 1 .Janilaly 1999 by physical therapists in clinical practice, whereas diathermy is one of the least commonly used modalities.I4-l5Although both are considered deep heaters, ultrasound is a high-frequency acoustic wave (greater than 20,000 Hz) and diathermy is an electromagnetic wave. Ultrasound causes deep local heating effects confined to an area approximately twice the size of the sound head. The energy is applied with a trans ducer or sound head that is kept moving to avoid the creation of damaging standing waves and burning. The tissue receives the energy from the high frc quency acoustic wave, but the patient is not an active part of an acoustic circuit. A media (gel or water) must be used to transmit ultrasound to the tissue because the acoustic waves are not conducted through air.14J5In contrast, diathermy has broad systemic heating effects that extend beyond the area under the electrodes. The electrodes used to delivery shortwave diathermy are stationary and the energy can be conducted through air. Diathermy is said to increase body temperature, respiratory rate, and pulse rate, and even to decrease blood pre~sure.~ When treated with diathermy, the patient (specifically the area of the body to be treated) is an integral part of the electrostatic and electromagnetic DIATHERMY AND CURRENT CLINICAL PRACTICE Because of increased concerns about the incidence of cancer in natural and unnatural electromagnetic environments (eg, the sun, large radio or communication antennas), the cost of the therapeutic machines (usually $10,000), the size of the equipment, and the demagnifjing effects of the electromagnetic fields on other electronic devices (eg, credit cards, key control cards, computers, radios), diathermy has lost popularity in many clinical practice settings. Thirty-five years ago when I worked in the Physical Therapy Department of the US Public Health Hospital in San Francisco, we had at least 5 diathermy machines operating at a time. Diathermy was frequently applied prior to the initiation of an exercise program for patients with musculoskeletal problems across large areas, such as chronic low-back pain, shoulder dysfunction, or knee pain. In an open treatment area, we could set up patients for diathermy, visually monitor the patient, and verbally communicate with the patient while we were in the same area using our hands to treat another patient. The patient was given the responsibility to be an active member of the team, capable of ringing a bell or turning off a switch if the temperature became more than "comfortably warm." As a faculty member who co-teaches a course on therapeutic modalities, as a researcher who has investigated the healing effects of ultrasound and other modalities, and as a clinician who prioritizes treatment in terms of education, manual procedures, sensory and motor retraining, and specific therapeutic exercise, I view therapeutic modalities as adjunctive to other physical therapeutic intervention strategies. Where possible, patients must be able to apply therapeutic modalities at home. Diathermy is difficult to apply at home because the equipment is generally too large. Now available, however, are some new, small units for home use designed for wound healing, neural stimulation, and pain control. In our academic program, we obtain diathermy machines for teaching from therapists who want to remove them from their clinics. We teach the students about the physics of diathermy, the indications and contraindications for the use of diathermy, and the procedures for the safe application of diathermy. Diathermy is included as a chapter in most textbooks on physical a g e n t ~ . ~ . However, l~.l~ the students from our institution report that they rarely see diathermy in the clinics in Northern California when they have their clinical affiliations. SPECIFIC FINDINGS OF DRAPER AND HIS COLLEAGUES The investigators in this study used pulsed shortwave diathermy as the treatment device. Although the power output was not stated, the investigators found that pulsed short-wave diathermy significantly increased muscle temperature. They implied that the primary clinical benefit of this rigorous increase in muscle temperature was to facilitate increased tissue extensibility. Two things were surprising about the authors' focus on tissue extensibility. First, continuous short-wave diathermy has generally been recommended for purposes of heating whereas pulsed diathermy has been recommended for purposes of maximizing the mechanical benefits of the diathermy (eg, healing, pain relief, scar tissue breakdown). 1.7*H~15~1%20 Thus, the benefit of diathermy applied in a pulsating mode should be the mechanical and piezoelectric effects, not the heating effects. Second, the investigators claimed that the heating effects reached a desired rigorous level. However, the mean muscle temperature achieved was less than 40°C. Increases in tissue extensibility are generally attributed to rigorous heating. Studies show that approximately a 1% increase in tendon extensibility is achieved for each 1°C increase in temperature between 40 and 45°C." Although one cannot necessarily infer that muscle extensibility will be increased similarly to tendon extensibility, one also cannot assume that muscle exten- sibility increases significantly when it is warmed from a standard body temperature of 37 to 39°C. We do know, however, that people generally feel stiffer when they are cold compared to when they are warm and that the skin and the muscle tend to feel more pliable when they are slightly warmer than normal body temperature. SUMMARY Draper's study provides little information on the physics of short-wave diathermy in general, the specific power parameters of the diathermy used in this study, or the basic physiologic effects expected from electromagnetic fields in this radiofrequency range. However, the study does provide one objective piece of evidence: pulsed short-wave diathermy can significantly elevate muscle temperature. Pulsed short-wave diathermy, however, did not elevate the muscle temperature into the "rigorous" range, which is generally considered a requisite for increasing tissue extensibility. However, the investigators still claim that the study findings have important implications for physical therapists in terms of enhancing tissue mobility. The investigators also suggest that the temperature remained therapeutically elevated after the modality was removed. Practically, however, this claim is not valid because the temperature decreased 1.78"C within 10 minutes, bringing the average muscle temperature to approximately 38"C, only 1°C above the average body temperature of 37°C. Past research suggests that the application of "continuous" short-wave diathermy would have been more likely than "pulsed" short-wave diathermy to elevate the muscle temperature to the range of 40 to 45°C. Even with continuous short-wave diathermy, however, it is still difficult to maintain the temperature beyond 42 to 43°C without burning the more superficial tissues. Given the temperature elevation in muscle reported in this study, manufacturers need to rethink their marketing claims about the use of pulsating diathermy to treat acute injuries where heating is undesirable. The rate of pulsation and the power selection needed to control tissue heating should be clearly specified. Over the past few years, physical therapists have not been interested in or committed to efficacy research on short-wave diathermy. This study suggests that diathermy is useful for creating temperature elevation across a large area. Although not addressed by the authors, there has also been a recent surge of interest in the public news media about the use of electromagnetic fields for other purposes such as the treatment of cancer, the control of pain, the management of arthritis, and even the restoration of function following a cerebral infarct. More research is needed to clarify the basic physiology of electromagnetic fields in the treatment of neuromuscular and skin conditions and the unique J Orthop Sports Phys Ther .Volume 29. Number 1 *January 1999 parameters o f this alternating radiofrequency wave required t o achieve specific outcomes. Nancy Byl, PhD, PT Professor and Chair University o f California, San Francisco Graduate Program in Physical Therapy School o f Medicine Box 0736 374 Parnassus Avenue San Francisco, CA 94143 REFERENCES , , , , Behrens, BJ, Micholovitz, SL. Physical Agents: Theory and Practice for the Physical TherapistAssistant. Philadelphia: FA Davis; 1996. Byl N, McKenzie A, West JM, et al. Low-dose ultrasound effects on wound healing: A controlled study withYucatan pigs. Arch Phys Med Rehab. 1992;73:656-664. By1 N, Hoft H. The use of oxygen in wound healing. In: McCullock JM, Kloth LC, Feedar JA, eds. Wound Healing: Alternatives in Management. Philadelphia: FA Davis; 1995:365404. Day MI. Diathermy. In: Hecox B, MehreteabTA, Weisberg J, eds. Physical Agents. A ComprehensiveText for Physical Therapists. Norwalk, Conn: Appleton and Lange; 1994: 1 Aa-1 a&. ,-a-, Griffin JE, Kanelis TC. Physical Agents for Physical Therapists. Springfield, Ill: Charles C Thomas, Inc.; 1982. Guy AW. Biophysics of high frequency currents and electromagnetic radiation, In: Lehmann J, ed. Therapeutic Heat and Cold, Baltimore: Williams and Wilkins; 1982: 199-277. Hayes KW. Manual for Physical Agents. Norwalk, Conn: Appleton and Lange; 1993. Hecox B, MehreteabTA, Weisberg J, eds. Physical Agents. A Comprehensive Text for Physical Therapists. Norwalk, Conn: Appleton and Lange; 1994. 9. Kloth L, Ziskin MC. Diathermy and pulsed radiofrequency radiation. Michlovitz SI, ed. Thermal Agents in Rehabilitation. 3rd ed. Philadelphia: FA Davis; 1994:213-254. 10. Lehmann JF, Guy AW, Stonebridge JB, Warren CG. Review of evidence for indications, techniques of application, contraindications, hazards and clinical effectiveness for shortwave diathermy. Rockville Md. 1974. DHEWI FDA, FPA-500. 11. Lehmann IF. Therapeutic Heat and Cold. 4th ed. Baltimore: Williams and Wilkins; 1990. 12. Lehmann JF. Diathermy. In: Handbook of Physical Medicine and Rehabilitation. Krusen FH, Kottke FJ, Elwood DJ, eds. Philadelphia: W.B. Saunden; 1971:273-345. 13. Lehmann J, ed. Therapeutic Heat and Cold. Baltimore: Williams and Wilkins; 1982. 14. McDermid, Ziskin MC, Michlovitz SL. Therapeutic ultrasound. In: Michlovitz SL, ed. Thermal Agents in Rehabilitation. Philadelphia: FA Davis; 1994:169-207. 15. Michlovitz, SL, ed. Thermal Agents in Rehabilitation.Philadelphia: FA Davis; 1994. 16. Nevins RG, Darwish MA. Heat transfer through subcutaneous tissue as heat generating porous material. In: Hardy J, Gagge A, Stolwijh J, eds. Physiological and Behavioral Temperature Regulation. Springfield, Ill: Charles C Thomas; 1970:281-301. 17. Schliephake E. General principles of thermotherapy. In: Licht S, ed. Therapeutic Heat. New Haven, Conn: Licht; 1958;12&169. 18. Sharrard WJW. A double-blind trial of pulsed electromagnetic fields for delayed union of tibia1 fractures. IBone Joint Surg. 1990;72~:347-351. 19. US Dept of Health and Human Services, Food and Drug Administration, Center for Devices and Radiological Health. Everything you always wanted to know about the medical devices amendmen&...and weren't afraid to ask. 3rd ed. HHS Pub. 90-41 73, 1990. 20. Ward AR. Electricity Fields and Waves in Therapy. Marrickville, NSW, Australia: Science Press; 1986. 21. Woo S. Temperature dependent behavior of the canine medial collateral ligament. 1 Biomech Eng. 1987;109:6& 71. Author Response The purpose o f o u r paper was n o t t o present technical information regarding the physics o f shortwave diathermy. That information is n o t new, and the reader can find it in most any textbook. Our purpose was t o present new findings regarding the rate o f temperature increase in human muscle during pulsed short-wave diathermy application. Dr. By1 made several inferences t o ultrasound in her commentary. We have been performing ultrasound research for nearly a decade and tried t o include some o f these findings in this manuscript. T h e reviewers, however, insisted that we focus o n diathermy. We will now respond t o the main concerns: (1) the reason pulsed short-wave diathermy was used and (2) the therapeutic temperature range. J Onhop Sports Phys Ther-Volume 29.Number 1 .January 1999 We have found that many continuous short-wave diathermy treatments are quite uncomfortable t o the patient. These treatments often heat at such a fast rate that pain is experienced before adequate heating occurs in the tissues. We employed high-intensity pulsed short-wave diathermy in our study, because i t provides a gentle rate o f increase in muscle temperature that is n o t uncomfortable t o the patient. A t the intensity we employed (see text) pulsed short-wave diathermy heats at rates comparable t o continuous l M H z ultrasound at 1.5 W/cm2. We need t o correct Dr. By1 regarding baseline temperature. Core temperature in humans is about 37°C; however, as you move closer t o the surface the temperature drops. In o u r studies in human muscle, 21 baseline temperature has been as low as 31°C at 1 cm deep, to as high as 36°C at 5 cm deep. In none of our studies has the baseline muscle temperature been 37°C. Again, 37°C is core temperature, not muscle temperature. In this study, the baseline temperature was 35.8"C. Thus, the temperature was still 2.2"C above the baseline temperature 10 minutes after the diathermy treatment began (not to within 1°C of baseline temperature as Dr. By1 stated). Dr. Byl's other concern was that the recommended temperature range for tissue extensibility is 40 to 45°C. We have the same concerns, but for different reasons. In our 8 years of performing human in vivo thermotherapy research, the average peak temperatures that we observed were between 39 and 41°C (we just completed a similar study using identi- cal pulsed short-wave diathermy parameters and our mean peak temperature was 40.3"C). In over 200 subjects tested only 1 has reached 43°C. and he was so uncomfortable that the ultrasound treatment had to be terminated. We realize that past researchers have set the therapeutic range at 40 to 45°C for a minimum duration of 5 minutes. These temperatures might be reached in animals, but rarely in humans. The peak temperature reached in this study was 39.8"C,just 0.2"C less than 40°C. Dr. By1 is suggesting that 0.2"Cwould have made a significant difference in tissue extensibility. We think not. We feel that the magnitude of the increase over normal (baseline) is more important than an absolute temperature. David 0.Draper, EdD, ATC J Orthop Sports Phys Ther*Volume 29. Number 1 .January 1999