Tenascin-C expression relates to clinicopathological features
advertisement

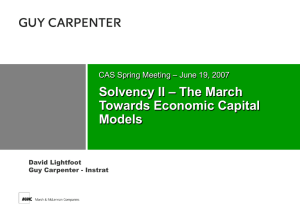
Neuropathology and Applied Neurobiology (2008), 34, 316–329 doi: 10.1111/j.1365-2990.2007.00898.x Tenascin-C expression relates to clinicopathological features in pilocytic and diffuse astrocytomas C. Maris*, S. Rorive*, F. Sandras*, N. D’Haene*, N. Sadeghi†, I. Bièche‡, M. Vidaud‡, C. Decaestecker§¶ and I. Salmon* Departments of *Pathology and †Radiology, Erasme University Hospital, and §Laboratory of Toxicology, Institute of Pharmacy, Université Libre de Bruxelles, Brussels, Belgium, ‡Laboratoire de Génétique Moléculaire, Faculté des Sciences Pharmaceutiques et Biologiques, Université Paris V, Paris, France, and ¶Fonds National de la Recherche Scientifique, Brussels, Belgium. C. Maris, S. Rorive, F. Sandras, N. D’Haene, N. Sadeghi, I. Bièche, M. Vidaud, C. Decaestecker and I. Salmon (2008) Neuropathology and Applied Neurobiology 34, 316–329 Tenascin-C expression relates to clinicopathological features in pilocytic and diffuse astrocytomas Aims: Tenascin-C (TN-C) is an extracellular matrix brain glycoprotein for which conflicting in vitro and in vivo results are reported in the literature dealing with its involvement in astrocytoma aggressiveness, in particular astrocytoma invasion. In view of these conflicting results and the lack of data available on low-grade astrocytomas, the present study focuses on pilocytic World Health Organization (WHO) grade I, and diffuse WHO grade II astrocytomas, that is, two histological entities associated with very different invasive abilities. Methods: Using real-time reverse transcription polymerase chain reaction and immunohistochemistry, we analysed the TN-C expression in normal brain tissue as well as in a series of 54 pilocytic and 53 grade II astrocytomas. Conclusions: Our data on normal brain showed that while TN-C is largely expressed in supratentorial white matter, it was largely absent in infratentorial white matter. Paralleling these observations, we showed that TN-C expression in low-grade astrocytomas similarly varies according to tumour site. Cox regression analysis evidenced that TN-C provided an independent prognostic value which is enhanced in the case of grade II astrocytomas for which positive TN-C expression is associated with a higher risk of recurrence. We also analysed TN-C expression specifically in vascular areas of low-grade astrocytomas without demonstrating any prognostic value for this additional feature. Results: Similarly to normal brain, low-grade astrocytomas exhibit variations in TN-C expression with site, and this expression is associated with an independent prognostic value in terms of recurrence. Keywords: extracellular matrix, low-grade astrocytoma, multivariate analysis, prognosis, tenascin-C Introduction Astrocytomas can be grouped into histological entities associated with very different clinical behaviour patterns and pathological findings, and are classified into four categories (grade I–IV) according to the World Health Organization’s (WHO) grading system [1,2]. Grade IV astrocytomas (glioblastomas) constitute the most aggresCorrespondence: Isabelle Salmon, Departments of Pathology, Erasme University Hospital, Université Libre de Bruxelles, Brussels, Belgium. Tel: +322 553115; Fax: +322 554790; E-mail: isalmon@ulb.ac.be 316 sive type, and their biological characteristics are widely studied. While grade II diffuse astrocytomas constitute the first step in the malignancy development continuum within the so-called group of diffuse astrocytic tumours (that is, WHO grade II–IV), grade I pilocytic astrocytomas are generally well delineated and do not progress to higher grades. However, aggressive progression may be observed in a number of pilocytic astrocytomas with an infiltration pattern often leading to tumour recurrence, even though these tumours do not necessarily share the biological features of diffuse high-grade astrocytomas [2–4]. © 2007 Blackwell Publishing Ltd Tenascin-C expression in astrocytomas Aggressiveness and poor prognosis in the case of patients suffering from astrocytomas are mainly associated with the ability of astrocytoma cells to invade the surrounding parenchyma; this ability is modulated by the tumour environment, especially the extracellular matrix (ECM) [5]. In addition, the ECM plays a number of central roles in other biological processes, such as proliferation and angiogenesis, which are involved in astrocytoma development [5–8]. While the composition and the roles of the ECM in the central nervous system (CNS) are not well defined, various authors agree that the ECM of the brain is different from that of the other organs. While collagen, fibronectin and laminin are the predominant ECM components in non-CNS tissue, hyaluronan, proteoglycans, tenascin-C (TN-C) and thrombospondin are the principal elements in the CNS ECM [8,9]. TN-C is a glycoprotein characterized by a hexameric structure. Its aminoterminus includes a series of cysteines and heptad repeats, both of which are involved in multimerization. This terminal part is followed by 14.5 epidermal growthfactor-like and 17 fibronectin type III-like repeats. Finally, the carboxy-terminus consists of a COOH-terminal knob made up of a sequence homology with the globular domain of the b and g chains of human fibrinogen [10,11]. While TN-C is encoded by a single gene under the control of a single promoter, a number of structurally and functionally different human TN-C isoforms are generated by the alternative splicing of the TN-C transcript at the fibronectin type III repeat level [10,11]. By regulating the adhesive and signalling properties of cells, TN-C is able to play a number of morphoregulatory roles during the processes of development and tissue remodelling as well as in disease [10–13]. However, conflicting in vitro and in vivo results are reported in the literature concerning the role that TN-C plays in the different processes such as cell adhesion, motility and invasion that lead to astrocytoma cell migration – see the Discussion [14–21]. It should be emphasized that most TN-C-related studies concern high-grade astrocytomas. In fact, very limited data are available on low-grade astrocytic tumours, and in particular on pilocytic (WHO grade I) astrocytomas, which display very different behavioural patterns as compared with the diffuse (WHO grade II–IV) group. This motivated us to analyse the TN-C expression in normal brain tissue as well as in a series of 107 low-grade astrocytomas [by means of real-time reverse transcription polymerase chain reaction (RT-PCR) and immunohistochemistry] and to focus on the potential involvement of 317 TN-C in the magnetic resonance imaging (MRI) aspects of low-grade astrocytomas. To this end, we used multivariate data analyses that enabled us: (i) to study the case distribution in a multivariate (clinical and anatomopathological) feature space in which the feature interactions were analysed (by means of Log-linear models); and (ii) to carry out multivariate prognosis analyses (by means of Cox regression). Materials and methods Clinical and histopathological data The investigations using normal tissue were carried out on samples from five normal human post mortem brains (without neuropathological alterations) obtained within 24 h of death. Six samples were taken from six different areas: grey and white matter from the cerebral hemispheres (frontal lobes) and grey and white matter from the cerebellar hemispheres, the brainstem and the cervical spinal cord. Three samples from each site were stored at -80°C for RT-PCR analyses and three others were embedded in paraffin. A series of 107 low-grade astrocytomas was investigated in parallel. This series consisted of archival formalin-fixed and paraffin-embedded samples obtained from the Laboratory of Pathology of the Erasme University Hospital (Brussels, Belgium) and collected between 1984 and 2005. As detailed in Table 1, all the cases were classified by two pathologists according to the WHO classification [1,2]. Frozen tumour samples from astrocytomas were also available for RT-PCR analyses (see below). These samples were used subject to the approval of the Université Libre de Bruxelles Hôpital Erasme Ethics Committee. The available clinical data included patients’ ages and genders, their tumour sites, the extent of their surgical resections and their pre- and post-surgical adjuvant treatments and follow-ups, as detailed in Table 1. The preoperative neuroimaging data (including fluid attenuated inversion recovery and enhanced T1-weighted images when available) were retrospectively reviewed and enabled 100 astrocytomas to be classified as either well- or ill-circumscribed (see MRI status in Table 1). Because of the absence of normal tissue in the available materials, histopathological infiltration could not be assessed for a large number of cases and was thus not considered in the present study. © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 318 C. Maris et al. Table 1. Clinicopathological data for 107 patients with low-grade astrocytomas Number of patients Age: child/adult* Gender: male/female Sites Cerebral hemisphere Diencephalon Cerebellum Brain stem Spinal cord Others† MRI status Ill-circumscribed Well-circumscribed Not specified Surgical resection Total Partial Biopsy Adjuvant therapy Pre-surgery Post-surgery Follow-up (months) Range Median Recurrence‡ (median delay) Death 210 kDa Pilocytic Grade II 181.8 kDa 54 29/25 29/25 53 14/39 30/23 115.5 kDa 12 7 20 10 3 2 22 2 9 4 15 1 23 24 7 46 7 0 30 22 2 8 40 5 7 7 4 17 1–335 44 14 (34) 4 1–348 39 20 (17) 8 The data present numbers of cases in the different categories except where other measurements are indicated (such as range). *Cut-off value of 18 years. †optic nerve, corpus callosum. ‡cases with total or partial surgery. MRI, magnetic resonance imaging. The recurrences concerned patients having benefited of a total or subtotal surgery, and were defined as cases presenting magnetic resonance imaging (MRI) evidence of progression that required new surgery or adjuvant treatments. Immunohistochemistry Five-micrometer-thick sections were submitted to standard immunohistochemistry as previously detailed [22,23], with the immunohistochemical expression being visualized by means of streptavidin—biotin–peroxidase complex kit reagents (BioGenex, San Ramon, CA, USA) with diaminobenzidine/H2O2 as the chromogenic substrate. Counterstaining with haematoxylin concluded the processing. The TN-C expression was evidenced by means of a murine monoclonal anti-TN-C antibody clone DB7 82.2 kDa 1 2 3 4 5 6 7 Figure 1. Western blot analysis showing negative control (lane 2); TN-C protein (lane 3); normal supratentorial grey matter (lane 4); normal supratentorial white matter (lane 5); and glioblastomas (lanes 6 and 7). TN-C, tenascin-C. (Chemicon Int, Temecula, CA, USA; dilution 1:200). Figure 1 illustrates the antibody specificity (1:750 dilution) proven by means of Western blot analysis using purified human TN-C protein (1.25 mg; Chemicon Int, Temecula, CA, USA; Figure 1 lane 3), 200 mg of proteins from the normal supratentorial grey (lane 4) and white (lane 5) matter, and 50 mg of proteins from two glioblastomas (lanes 6 and 7). For immunohistochemistry purposes, a negative control was carried out by replacing the primary TN-C antibody with non-immune serum (Dako, Glostrup, Denmark). Evaluation of the immunohistochemical TN-C expression The TN-C immunostaining intensity was assessed by two independent observers (CM, SR) using standard lightmicroscopy. Where discrepancies were encountered, the cases were settled by consensus with a third observer (IS). In view of the staining patterns observed (see Results), TN-C immunostaining in astrocytomas was systematically evaluated in the ECM, distinguishing between a negative to low expression level (labelled as ‘negative’) and a moderate to high one (labelled as ‘positive’). Additional investigations were carried out in vascular areas. This enabled us to identify in a number of cases presenting a particular pattern of TN-C expression (illustrated in Results). This particular pattern is defined by a major enhancement of TN-C expression in the vessel walls and/or perivascular ECM as compared with neighbouring tumour ECM, and was mentioned as vascular enhancement (VE) in the following. As detailed in the results, this latter evaluation was possible with certainty in 50 pilocytic and 44 grade II astrocytomas only. The two TN-C-related features were labelled ECM TN-C and VE TN-C respectively. © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Tenascin-C expression in astrocytomas Real-time RT-PCR Real-time RT-PCR analyses were carried out on a series of tissue samples in order to evaluate the TN-C mRNA expression. RNA extraction, cDNA synthesis and PCR reaction conditions have been described previously [23]. After samples that did not satisfy the quality controls had been excluded, the remaining series consisted of 40 normal brain tissue samples (10 cerebral grey and 12 white matter, 10 cerebellar grey and eight white matter samples), nine pilocytic astrocytomas (four supratentorial and five infratentorial including three cerebellar) and nine grade II astrocytomas (five supratentorial and four infratentorial including one cerebellar). Quantitative values were obtained from the threshold cycle number (Ct value), at which the increase in the fluorescent signal associated with an exponential growth of PCR products began to be detected by the laser detector of the ABI Prism 7700 Sequence Detection System (Perkin-Elmer Applied Biosystems, Foster City, CA, USA) using the PE Biosystems analysis software according to the manufacturer’s manuals. The precise amount of total RNA added to each reaction mix (based on optical density) and its quality were both difficult to assess. Because of this, we also quantified the transcripts of RPLP0, an endogenous RNA control gene [24]. As previously detailed [23], the results were termed ‘Ntarget’ and expressed as N-fold differences in target gene expression relative to the RPLP0 gene. Primers for the RPLP0 and TN-C were chosen with the assistance of the Oligo 5.0 computer program (National Biosciences, Plymouth, MN, USA). We carried out searches in the dbEST and nr databases to confirm the absence of single nucleotide polymorphisms and the total gene specificity of the nucleotide sequences chosen as primers. To avoid the amplification of contaminating genomic DNA, one of the two primers was placed at the junction between two exons. The nucleotide sequences of the primers used were as follows: RPLP0-U (5′-GGC GAC CTG GAA GTC CAA CT-3′) and RPLP0-L (5′-CCA TCA GCA CCA CAG CCT TC-3′) for RPLP0 trancripts (PCR product of 149 bp), TNCtot-U (5′-GAG GGT GAC CAC CAC ACG CTT-3′) and TNCtot-L (5′-CAA GGC AGT GGT GTC TGT GAC ATC-3′) for total TNC transcripts (PCR product of 73 bp). Gel electrophoresis was used to verify the specificity of the PCR amplicons. For each primer pair, we performed no-template control and no-reverse-transcriptase control assays, which produced negligible signals (usually >40 in 319 Ct value), suggesting that the effects of the primer–dimer formation and genomic DNA contamination were negligible. Data analysis All the statistical analyses were carried out using Statistica (Statsoft, Tulsa, OK, USA). The first step was to study the relationships between pairs of qualitative variables by means of contingency tables. The significance of the potential associations was evaluated by means of either the c2-tests or Fisher’s exact tests (in 2 ¥ 2 cases only). The second step involved the log-linear analysis technique, which is a multivariate extension of the c2-test of independence [25]. The major task was to establish the best possible fit for the cell frequencies of a multiway contingency table by means of a log-linear model. We identified the simplest model that fitted the data (that is, explained the multivariate data distribution) by using a methodology similar to that detailed in [26] and based on the ‘Automatic best model selection’ procedure included in the log-linear analysis module of the Statistica software. Finally, the standard Cox regression analysis was also used to fit an explanatory model to the relapse-free survival data. This method enabled the possible simultaneous influence of several variables on the survival period to be tested. In addition, the nonparametric Mann–Whitney test was used to compare independent groups of quantitative values provided by real-time RT-PCR. Results Expression of TN-C in the normal human brain As shown in Figure 2, in the cerebral white matter area, there is a highly heterogeneous level of TN-C expression with a high level of immunopositivity, whereas the cortex displayed a low level of immunopositivity limited to the first layer and the external glia limitans (Figure 2A). While the leptomeningeal vessels (smooth muscle cells) showed moderate TN-C immunopositivity, the capillaries of the white and grey matter did not offer any immunopositivity at all. In contrast, in the cerebellum, we observed a completely different staining pattern consisting of the absence of any expression in the white matter (Figure 2B), whereas the ECM of the molecular layer sometimes © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 320 C. Maris et al. Figure 2. Illustrations of immunohistochemical TN-C expression in normal human brains and astrocytomas. (A) Major difference in staining for TN-C of the grey and white matter in normal frontal lobes. (B) Absence of TN-C expression in the normal human cerebellum (molecular layer and white matter). (C) Diffuse and strong TN-C expression in the ECM of a supratentorial pilocytic astrocytoma in contrast to the weak or wholly absent TN-C expression in the ECM of an infratentorial pilocytic astrocytoma (D). Same variation of staining observed between a supratentorial (E) and an infratentorial grade II astrocytoma (F). Two patterns of vascular enhancement of TN-C expression (VE TN-C) in astrocytomas showing strong TN-C expression in vessels walls with (G) or without (H) perivascular enhancement. Original magnification ¥40 (A–B); ¥100 (G); ¥200 (C–F, H). ECM, extracellular matrix; VE TN-C, vascular enhancement tenascin-C. © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Tenascin-C expression in astrocytomas 321 Figure 3. Real-time RT-PCR results of total TN-C mRNA expression in normal brain tissue (A) and low-grade astrocytoma samples (B). (A) The analyses were carried out on 40 samples of cerebral and cerebellar grey and white matter (10/12 cerebral grey/white matter, 10/8 cerebellar grey/white matter). (B) The analyses were carried out on nine supratentorial (four pilocytic and five grade II) astrocytomas and nine infratentorial (five pilocytic and four grade II) ones. The data are expressed as means ⫾ SEM. RT-PCR, reverse transcription polymerase chain reaction; TN-C, tenascin-C; SEM, standard error mean. displayed a very weak level of expression. No TN-C immunopositivity was detected in the cerebellar vessels. While the ECM of the brainstem and spinal cord specimens was negative, we did observe intracytoplasmic TN-C expression in focal neurones. These results were globally confirmed at the mRNA expression level by means of quantitative RT-PCR. As shown in Figure 3A, the TN-C mRNA levels increased in the cerebral white matter as compared with the cerebellar (P = 0.047), with very low (if any) mRNA levels in the grey matter regardless of its origin. Expression of TN-C in astrocytomas To ensure certainty in the detection of the presence or absence of VE TN-C, the evaluation was carried out twice by the same observer (IS), after excluding six cases because of the limited size of the available material. Of the 101 remaining cases, 94 cases (50 pilocytic and 44 grade II) were concordantly evaluated (that is, 93% of concordance), of which 33 cases exhibited VE TN-C as illustrated in Figure 2G,H. In the following, we restricted any analysis related to VE TN-C to these 94 concordant cases. It should also be noted that the distinction between the different types of VE TN-C (observed in perivascular ECM only, or vascular cells only, or both) did not add additional information (data not shown). In addition, in the case of very strong VE TN-C, the identification of the vascular cell types expressing TN-C was not possible. A first analysis showed no significant dependence between the two TN-C-related features (ECM and VE TN-C), revealing that these two features produced different information on TN-C expression in lowgrade astrocytomas. The following results detailed the difference observed between these two features in relation to the other clinicopathological features analysed. We also showed that there was no need to distinguish between the tumours of the patients submitted to presurgery adjuvant therapies (n = 11) and those of the patients who had not undergone any such therapies (see Table 1), because no difference in TN-C expression (ECM and VE TN-C) was evident across these two groups (data not shown). In relation to tumour type The data concerning the immunohistochemical TN-C expression in the low-grade astrocytomas are detailed in Tables 2 and 3 and illustrated in Figure 2C–F, while the quantitative RT-PCR assessments are shown in Figure 3B. As detailed in Table 2, the total percentages of cases with positive TN-C expression in tumour ECM slightly increased from 46% for the pilocytic to 68% for the grade II (P = 0.03). At the mRNA level, no difference was observed between pilocytic and grade II cases when their locations were not taken into account (data not shown). As explained below, this was not the case when comparing infratentorial and supratentorial tumours. Although VE TN-C seemed to be more prevalent in pilocytic (44%) than in grade II (25%) astrocytomas, this tendency was not significant (P = 0.08). © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 322 C. Maris et al. Table 2. TN-C expression in low-grade astrocytomas Pilocytic Sites Supratentorial Hemisphere Diencephalon Subtotal Infratentorial Cerebellum Brain stem Spinal cord Subtotal Others Total Grade II ECM VE ECM 83 (10/12) 57 (4/7) 74 (10/19) 64 (7/11) 50 (3/6) 59 (10/17) 91 (20/22) 100 (2/2) 92 (22/24) 20 40 67 30 33 50 33 39 (4/20) (4/10) (2/3) (10/33) (1/2) 46 (25/54) (6/18) (5/10) (1/3) (12/31) (0/2) 44 (22/50) VE 6 (1/18) 0 (0/2) 5 (1/20) 22 50 67 50 (2/9) (2/4) (10/15) (14/28) (0/1) 68 (36/53) 44 75 33 43 (4/9) (3/4) (3/10) (10/23) (0/1) 25 (11/44) The data are expressed as the percentages of cases exhibiting positive TN-C expression in ECM or VE. The exact ratios are also mentioned. TN-C, tenascin-C; extracellular matrix; VE, vascular enhancement. Table 3. MRI status of low-grade astrocytomas in relation to their sites and TN-C expression (A) Occurrence of ill-circumscribed astrocytomas in relation to tumour sites Pilocytic Supratentorial Infratentorial Cerebral hemisphere Diencephalon Cerebellum Brain stem Spinal cord 44 43 19 80 100 Others Grade II (4/9) (3/7) (3/16) (8/10) (3/3) (2/2) 95 100 56 75 93 }44% }85% (21/22) (2/2) (5/9) (3/4) (14/15) (1/1) }96% }89% (B) Positive TN-C expression in relation to MRI status Pilocytic TN-C Expression Well-circumscribed Ill-circumscribed Grade II ECM 29 (7/24) 61 (14/23) VE 27 (6/22) 62 (13/21) ECM 57 (4/7) 70 (32/46) VE 14 (1/7) 27 (10/37) The data in (A) are expressed as the percentages of ill-circumscribed tumours in each category (the exact ratios are also mentioned), while the data in (B) are expressed as the percentages of cases exhibiting positive TN-C expression in ECM or VE (the exact ratios are also mentioned). TN-C, tenascin-C; MRI, magnetic resonance imaging; ECM, extracellular matrix; VE, vascular enhancement. In relation to site Because in the normal brain TN-C was expressed differently in terms of site, we analysed the possible variations in astrocytoma TN-C expression in relation to tumour site. The results shown in Table 2 indicate that the slight increase in ECM TN-C expression from the pilocytic to the grade II astrocytomas was similarly observed in the supratentorial and infratentorial astrocytomas. As also illustrated in Figure 2C–F, ECM TN-C was expressed in a significantly larger number of supratentorial pilocytic (74%) and grade II (92%) astrocytomas than their infratentorial counterparts (30% and 50% respectively; P = 0.004 for pilocytic, P = 0.002 for grade II and P < 10-6 over the total group of low-grade tumours). The ‘Others’ group containing only three cases was not taken into account in the statistical analyses. The same tendency was observed at the mRNA level. When grouping the low-grade cases per location, a © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Tenascin-C expression in astrocytomas decrease was observed in infratentorial as compared with supratentorial cases (Figure 3B) without being significant. This decrease was probably due to the relative heterogeneity detailed in Table 2 and the small number of cases analysed. Regarding VE TN-C, the pilocytic astrocytomas did not exhibit any significant variation in terms of tumour site (Table 2). This contrasts with the significant variations (P = 0.005) evidenced in grade II astrocytomas for which VE was observed in infratentorial locations (including the cerebellum) almost exclusively (see Figure 2F). In relation to patients’ ages We also investigated whether paediatric vs. adult astrocytomas were characterized by different TN-C expression levels. We observed that grade II astrocytomas in children generally had lower levels of ECM TN-C expression than those in adults (P = 0.006). We did not observe this relation in the case of the pilocytic astrocytomas (P = 0.10). No variation in VE TN-C was evident between paediatric and adult astrocytomas. In relation to the MRI status Finally, we focused on the MRI status (well- vs. ill-circumscribed). The results detailed in Table 3A show the variations in the MRI status of the low-grade astrocytomas in relation to their sites, while bringing out the differences between the supratentorial and the infratentorial sites where the cerebellar sites must be distinguished. The ill-circumscribed pilocytic tumours were found particularly in the brainstem and the spinal cord (85%), were less frequently observed in the supratentorial locations (44%) and even less so in the cerebellum (19%) (P = 0.002). As expected, the diffuse grade II tumours were generally ill-circumscribed regardless of site (96% of supratentorial cases and 89% of brainstem and spinal cord ones), except in the cerebellum where only 56% were ill-circumscribed (P = 0.009). When the pilocytic and grade II astrocytomas were grouped, a significantly higher number of ECM TN-Cpositive cases were shown in the group of the illcircumscribed tumours (66% vs. 35% for the well-circumscribed astrocytomas, P = 0.005). As detailed in Table 3B, this relation was essentially due to the pilocytic astrocytomas (61% vs. 29% P = 0.04), for which a significant association was also evident between VE TN-C and the MRI status (62% vs. 27%, P = 0.03). In contrast, no significant relation was demonstrated between VE TN-C and the MRI status in grade II astrocytomas (or after grouping the pilocytic and grade II astrocytomas). 323 Analysis of the multivariate interactions between TN-C expression, tumour grades, sites and MRI status and patients’ ages The results reported above led us to consider that interdependencies exist between the different variables, particularly in the case of low-grade astrocytomas. We decided to perform a multivariate analysis in order to analyse these interdependencies systematically. We therefore carried out a first log-linear analysis on the five-dimensional contingency table, cross-classifying ECM TN-C expression, patients’ ages (child vs. adult), tumour grades (I vs. II), sites (distinguishing between supratentorial, cerebellar and other infratentorial tumours) and MRI status (ill- vs. well-circumscribed). For the set of 97 tumours so concerned (located in the four major sites and for which the MRI status were available), the log-linear analysis was able to test for statistical significance in the case of each possible interaction between two or more features; Table 4 describes the results obtained. To begin with, we evaluated the order of the significant feature interactions (2, 3 or 4) that have to be taken into account in a log-linear model to explain the data correctly (that is, without any significant loss of information). The results shown in Table 4A indicate that only the two-feature interactions were significant. This confirms both the presence of a degree of interdependence between pairs of features and the absence of more complex relationships. Second, the information provided by the different feature interactions was analysed by evaluating the partial and marginal associations, as detailed in Table 4B. Briefly, the partial association between two features evaluates the loss of information due to the exclusion of the feature interaction of interest from a complete log-linear model of order 2 (including all the effects due to the individual features and the two-feature interactions). In addition, the marginal association between two features evaluates the gain of information by adding this particular interaction to a loglinear model including only the effects of order 1 (due to the individual features). The results (detailed in Table 4B) showed significant (partial and/or marginal) associations for each pair of features except between tumour grade and site (interaction 24). It should be noted that of all the partial associations involving ECM TN-C expression (interactions 12–15), only one was significant, that is, interaction 14 between ECM TN-C expression and tumour site. This means that failing to take account of astrocytoma sites in the evaluation of ECM TN-C expression leads to a © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 324 C. Maris et al. Table 4. Log-linear analysis of the multivariate interactions between features (A) Fitting of all K-feature interactions K-feature interaction Degrees of freedom Max.Lik. c2 P-value 1 2 3 4 5 6 14 16 9 2 19.74 75.05 11.76 5.51 0.30 0.003 <10-6 0.76 0.79 0.86 (B) Partial and marginal association – identification of the best model Effect Degrees of freedom Partial Ass. c2 Partial Ass. P-value Mrg. Ass. c2 Mrg. Ass. P-value Initial model Order 1 1 2 3 4 5 1 1 1 2 1 1.86 0.41 4.40 2.80 10.27 0.17 0.52 0.04 0.25 0.001 1.86 0.41 4.40 2.80 10.27 0.17 0.52 0.04 0.25 0.001 X Order2 12 13 14 15 23 24 25 34 35 45 1 1 2 1 1 2 1 2 1 2 0.87 3.64 13.00 1.31 2.44 0.03 8.78 3.09 0.55 9.30 0.35 0.06 0.002 0.25 0.12 0.98 0.003 0.21 0.46 0.01 4.93 10.23 20.48 7.54 6.63 3.33 14.01 10.01 6.46 16.23 0.03 0.001 0.00004 0.006 0.01 0.19 0.0002 0.007 0.01 0.0003 Best model X X X X X X X X X X X X X X X (A) Tests on the K-factor interactions (K = 1, 2, 3 or 4). A P-value <0.05 indicates that the corresponding interaction is significant. (B) Features: 1, ECM TN-C expression; 2, tumour grade; 3, patient’s age; 4, tumour site; 5, MRI status. The different interactions are denoted by the juxtaposition of the feature numbers. The partial association between the two feature i and j (denoted by ij) is computed by comparing the fit (that is, evaluating the c2 difference) of the complete model that includes all the two-way interactions with that of the model that excludes the interaction between features i and j. The marginal association between the two features i and j is computed by comparing the fit of the model that includes all the main effects (that is, order 1) with that of the model obtained after the addition of the interaction between feature i and j only. The (marginal or partial) P-values <0.1 identify the features and interactions included in the initial log-linear model to fit the data. The best model is the simplest model that is able to explain the data efficiently (that is, without any significant loss of information). Max.Lik., maximum licelihood; Partial Ass., partial association; Mrg. Ass., marginal association; ECM, extracellular matrix; TN-C, tenascin-C; MRI, magnetic resonance imaging. highly significant loss of information (P = 0.002). The best (that is, the simplest) log-linear model identifying the main significant effects able to explain the data efficiently (without any loss of information) was then generated from an initial model (see Table 4B). This best model consisted of only the feature interactions between ECM TN-C expression and the patient’s age (interaction 13) or tumour site (interaction 14), MRI status and astrocytoma grade (interaction 25) or location (interaction 45), and astrocytoma grade and the patient’s age (interaction 23). These five interactions were thus necessary and sufficient to explain the data distribution in the five-dimensional contingency tables. Figure 4 summarizes the information provided by this log-linear analysis, showing the direct and indirect links so evidenced between the features. This clarified the data reported in the previous section by indicating the presence of a direct and essential association between ECM TN-C expression and the astrocytoma sites. The influence of patient’s age also seems to be an essential factor that has © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Tenascin-C expression in astrocytomas 325 ECM TN-C expression in the series of low-grade astrocytomas, which was also enhanced in the case of grade II astrocytomas (see Table 5). We also observed that tumour site did not add any prognostic information to the models described in Table 5 (data not shown). Discussion Figure 4. Illustration of the direct links evidenced between the different features analysed in the best log-linear model fitted to the data (see Table 4 and text). Of these, the thick lines indicate the links associated with significant partial associations, that is, particularly required to explain the data. to be taken into account. This contrasts with the absence of any direct relation between MRI status and ECM TN-C expression. In a second log-linear analysis, we simply replaced the ECM TN-C feature by the VE TN-C one. As seen for the initial analysis, the best log-linear model generated on these data was of order 2 (data not shown). In contrast, this model did not retain any interaction involving VE TN-C but included it as an individual feature (that is, effect of order 1). However, it should be noted that significant and almost significant partial associations were, respectively, observed between VE TN-C and tumour grade (P = 0.03), and between VE TN-C and MRI status (P = 0.05). The actual importance of these associations has to be confirmed on a larger series. In fact, the twofeature interactions retained in the best model resulting from the second analysis involved the other features (tumour grade, patient’s age, tumour site and MRI status) and confirmed the results already reported in Figure 4. Prognostic impact of TN-C expression in low-grade astrocytomas We were not able to demonstrate any prognostic value for VE TN-C. However, for ECM TN-C ,while no correlation was observed for pilocytic astrocytomas (P = 0.33; Figure 5A), positive ECM-TN-C expression was associated with a higher risk of recurrence in grade II astrocytomas (P = 0.07; Figure 5B). In order to test the prognostic contribution of this marker in the presence of standard clinical variables, multivariate Cox regression analyses were performed. The results confirmed an independent prognostic value for Tenascin-C antibodies are presented as promising agents in the design of treatment protocols for different types of solid cancers, including gliomas [27–30]. As explained by Brack et al. [27], this approach is motivated by the fact that antigens preferentially expressed in modified tumour ECM are ideal targets for tumour-targeting applications. However, this type of application requires a detailed knowledge of the distribution of the antigen expression in normal and tumoral tissue, taking into account the high level of heterogeneity encountered in cancers. While TN-C expression in the normal brain was rarely detected in the first studies [10,31–33], most authors now describe TN-C expression as being restricted to the ECM. It should be noted that only limited information is available regarding normal brain tissues, and for a few studies peritumoral tissue was used as a point of normal reference by different authors [15, 32–34]. This approach was avoided in the present study because of the impossibility of excluding the TN-C secreted by astrocytoma cells migrating in peritumoral areas (or by normal cells, such as endothelial ones, reacting in the tumour environment). The discrepancy in the data on the TN-C expression in the normal brain could also be explained by the great complexity of the CNS. In fact, very limited data are available on the actual distribution of TN-C expression across the different structures of the normal brain. As previously shown by a few authors [18,19], the TN-C expression in the normal brain is heterogeneous and increases in the white matter as compared with the grey matter. Our study reveals that this heterogeneity is greater than supposed and is related to specific tissue sites. Indeed, we observed very few, if any, cases of TN-C expression in the cerebellar white matter, although a readily discernible amount of TN-C is present in the cerebral white matter. In the case of astrocytomas, it is clear that TN-C expression is heavily increased in glioblastomas as compared with normal tissue [15,17,18,34,35]. All the authors also agree that TN-C expression in ECM increases from low- to high-grade astrocytomas [15,17,18,34]. However, in the matter of TN-C involvement in astrocytoma aggressive- © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 326 C. Maris et al. 1.0 A Cumulative Proportion of Recurrence-free patients p = 0.33 0.8 0.6 negative ECM TN-C 0.4 0.2 positive ECM TN-C 0.0 0 50 100 150 200 250 300 350 400 Time (months) Cumulative Proportion of Recurrence-free patients 1.0 B 0.8 negative ECM TN-C 0.6 p = 0.07 0.4 positive ECM TN-C 0.2 0.0 0 50 100 150 Time (months) 200 250 300 Figure 5. Kaplan–Meier curves evidencing the relationships between the ECM expression of TN-C (positive/negative) and the recurrence-free survival periods for pilocytic astrocytomas (A) and grade II astrocytomas (B). The dots symbolize the recurrences and the crosses represent the relapse-free cases respectively. ECM, extracellular matrix; TN-C, tenascin-C. ness, conflicting data have been reported in the literature, leading different authors to come to opposing conclusions concerning the roles played by TN-C in astrocytoma cell migration, that is, a stimulating effect [14,15] vs. an inhibiting one [16]. Similarly, in vitro investigations, which performed migration assays, reported either a stimulating effect [5,11] or an inhibiting one [8,15,21,36]. In view of these conflicting results, we focused our analysis on pilocytic and grade II astrocytomas, because these two histological entities are associated with very different invasive abilities [37]. As recently shown, these two entities have different molecular profiles with respect to adhesion-, ECM- and invasion-related genes [38]. In the present series, neuroimaging evaluation revealed that while a large majority of the grade II cases seemed to be invasive, about half of the pilocytic cases displayed illcircumscribed aspects. Our monovariate analyses revealed that the ECM TN-C expression in the pilocytic and/or grade II astrocytomas © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Tenascin-C expression in astrocytomas 327 Table 5. Cox regression analysis Model/P-value Variable b P-value All pilocytic and grade II cases P = 0.00004 ECM TN-C Grade Age Surgery Adjuvant treatment 0.94 0.73 -0.04 -1.24 0.74 0.02 0.08 0.005 0.03 0.05 Grade II cases P = 0.002 ECM TN-C Age Surgery Adjuvant treatment 1.93 -0.06 -0.70 0.58 0.006 0.002 0.37 0.26 The ‘Model/P-value’ indicates the overall level of significance of the model. Except ‘Age’, which is a quantitative variable, all the others are binary. ECM TN-C distinguishes between negative and positive expression, grade between pilocytic and grade II astrocytomas, surgery between total and subtotal, and adjuvant treatment between absence and presence. The equation at the basis of the Cox Regression model is an exponential function of a linear combination of the variables considered, where b indicates the coefficient of each variable in the linear combination. The associated P-value is a measure of the level of significance of the contribution of each variable to the model (and leads to the conclusion that b is significantly different from zero). If P < 0.05, the feature is associated with a significant prognostic value independently of the other parameters taken into account. ECM, extracellular matrix; TN-C, tenascin-C. varied according to the tumours’ sites, the patients’ ages and the MRI status. Multivariate log-linear analyses were thus required to evaluate the actual interdependence between the different features and to identify which factors actually are related to the ECM TN-C expression in the astrocytomas. This approach has two main advantages. The first is that it provides a systematic approach to the analysis of complex multidimensional tables, while the second is that it enables the relative importance of the different effects (such as feature interactions) to be judged. This helped us to clarify that ECM TN-C expression in low-grade astrocytomas is indirectly related to the MRI infiltration status and directly related to the tumours’ location. It is important to note that this model characterizes low-grade astrocytomas, which are well known for their occupation of both cerebellar and cerebral sites in contrast to high-grade astrocytomas, which are more frequently located in the cerebral hemispheres. According to our hypothesis, the lack of TN-C in the normal cerebellar ECM in contrast to its strong expression in the normal cerebral ECM leads to very different tumoral ECMs. Indeed, we have shown that a greater number of both supratentorial pilocytic and grade II astrocytomas exhibit ECM TN-C expression as compared with infratentorial ones. It is known that high-grade astrocytoma cells are able to secrete TN-C and thus strongly modify the ECM composition [6]. Our data suggest that low-grade astrocytomas do not have the same ability, and this may well reflect on cell migration. While future research should confirm these results on a larger series, our data suggest that VE TN-C could be associated with the MRI status, especially in the case of pilocytic astrocytomas. We also agree completely with Zagzag et al. [15], who emphasized that pilocytic astrocytomas display an increase in perivascular TN-C enhancement, and especially around hyperplastic vessels. As reported in the literature, endothelial cells are able to secrete TN-C [39], and the detection of TN-C in the vascular areas of astrocytomas suggests a functional role played by TN-C in angiogenesis [15,17,18] and, more particularly, in the migration of endothelial cells [36]. The literature shows that both glioma angiogenesis and invasion are invasive processes sharing common mechanisms of regulation that can be simultaneously inhibited by naturally occurring factors [15,17,18]. This may (at least partly) explain the association between VE TN-C and the MRI status suggested by our data. However, we did not succeed in showing any prognostic value associated with VE TN-C for which the conflicting results reported in the literature concerned small series that did not include pilocytic astrocytomas [15,17,18]. In contrast, ECM TN-C expression was associated with an independent prognostic value, particularly in the case of grade II astrocytomas. This agrees with another result associating ECM TN-C immunopositivity with shorter survival for patients with glioblastomas (grade IV) [34]. In conclusion, similarly to normal brain, low-grade astrocytomas exhibit variations in TN-C expression with © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 328 C. Maris et al. sites, and this expression is associated with an independent prognostic value in terms of recurrence. However, additional information could be provided by the currently lacking analysis of different TN-C isoforms, especially in the case of normal brain and low-grade astrocytomas. To the best of our knowledge, only one study mentions the absence of large TN-C isoforms in these two categories of tissue as opposed to their presence in high-grade astrocytomas [34]. In fact, the scant availability of commercially available antibodies against alternatively spliced domains now limits immunohistochemical evaluation. Acknowledgements We are grateful to Ms Nathalie Watteau for secretarial support and Ms Blair Jenkins for help in preparing the manuscript. This work was carried out with the support of grants awarded by the Fonds Yvonne Boël (Brussels, Belgium). References 1 Kleihues P, Cavenee WKC (Eds). WHO Classification of Tumours. Pathology and Genetics. Tumours of the Nervous System. Lyon: IARC Press, 2000 2 Kleihues P, Louis DN, Scheithauer BW, Rorke LB, Reifenberger G, Burger PC, Cavenee WK. The WHO classification of tumors of the nervous system. J Neuropathol Exp Neurol 2002; 61: 215–25;discussion 26–9 3 Perilongo G, Garre ML, Giangaspero F. Low-grade gliomas and leptomeningeal dissemination: a poorly understood phenomenon. Childs Nerv Syst 2003; 19: 197–203 4 Buschmann U, Gers B, Hildebrandt G. Pilocytic astrocytomas with leptomeningeal dissemination: biological behavior, clinical course, and therapeutical options. Childs Nerv Syst 2003; 19: 298–304 5 Gladson CL. The extracellular matrix of gliomas: modulation of cell function. J Neuropathol Exp Neurol 1999; 58: 1029–40 6 Zamecnik J. The extracellular space and matrix of gliomas. Acta neuropathol 2005; 110: 435–42 7 Rauch U. Extracellular matrix components associated with remodeling processes in brain. Cell Mol Life Sci 2004; 61: 2031–45 8 Bellail AC, Hunter SB, Brat DJ, Tan C, Van Meir EG. Microregional extracellular matrix heterogeneity in brain modulates glioma cell invasion. Int J Biochem Cell Biol 2004; 36: 1046–69 9 Sobel RA. The extracellular matrix in multiple sclerosis lesions. J Neuropathol Exp Neurol 1998; 57: 205–17 10 Joester A, Faissner A. The structure and function of tenascins in the nervous system. Matrix Biol 2001; 20: 13–22 11 Jones PL, Jones FS. Tenascin-C in development and disease: gene regulation and cell function. Matrix Biol 2000; 19: 581–96 12 Jones FS, Jones PL. The tenascin family of ECM glycoproteins: structure, function, and regulation during embryonic development and tissue remodeling. Dev Dyn 2000; 218: 235–59 13 Bourdon MA, Ruoslahti E. Tenascin mediates cell attachment through an RGD-dependent receptor. J Cell Biol 1989; 108: 1149–55 14 Friedlander DR, Zagzag D, Shiff B, Cohen H, Allen JC, Kelly PJ, Grumet M. Migration of brain tumor cells on extracellular matrix proteins in vitro correlates with tumor type and grade and involves alphaV and beta1 integrins. Cancer Res 1996; 56: 1939–47 15 Zagzag D, Friedlander DR, Miller DC, Dosik J, Cangiarella J, Kostianovsky M, Cohen H, Grumet M, Greco MA. Tenascin expression in astrocytomas correlates with angiogenesis. Cancer Res 1995; 55: 907–14 16 Giese A, Loo MA, Rief MD, Tran N, Berens ME. Substrates for astrocytoma invasion. Neurosurgery 1995; 37: 294– 301; discussion 301–2 17 Herold-Mende C, Mueller MM, Bonsanto MM, Schmitt HP, Kunze S, Steiner HH. Clinical impact and functional aspects of tenascin-C expression during glioma progression. Int J Cancer 2002; 98: 362–9 18 Leins A, Riva P, Lindstedt R, Davidoff MS, Mehraein P, Weis S. Expression of tenascin-C in various human brain tumors and its relevance for survival in patients with astrocytoma. Cancer 2003; 98: 2430–9 19 Tews DS. Adhesive and invasive features in gliomas. Pathol Res Pract 2000; 196: 701–11 20 Kulla A, Liigant A, Piirsoo A, Rippin G, Asser T. Tenascin expression patterns and cells of monocyte lineage: relationship in human gliomas. Mod Pathol 2000; 13: 56–67 21 Giese A, Loo MA, Norman SA, Treasurywala S, Berens ME. Contrasting migratory response of astrocytoma cells to tenascin mediated by different integrins. J Cell Sci 1996; 109: 2161–8 22 D’Haene N, Maris C, Sandras F, Dehou MF, Remmelink M, Decaestecker C, Salmon I. The differential expression of Galectin-1 and Galectin-3 in normal lymphoid tissue and non-Hodgkin’s and Hodgkin’s lymphomas. Int J Immunopathol Pharmacol 2005; 18: 431–43 23 Mathieu A, Saal I, Vuckovic A, Ransy V, Vereerstraten P, Kaltner H, Gabius HJ, Kiss R, Decaestecker C, Salmon I, Remmelink M. Nuclear galectin-3 expression is an independent predictive factor of recurrence for adenocarcinoma and squamous cell carcinoma of the lung. Mod Pathol 2005; 18: 1264–71 24 Bieche I, Parfait B, Le Doussal V, Olivi M, Rio MC, Lidereau R, Vidaud M. Identification of CGA as a novel estrogen receptor-responsive gene in breast cancer: an © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Tenascin-C expression in astrocytomas 25 26 27 28 29 30 31 32 outstanding candidate marker to predict the response to endocrine therapy. Cancer Res 2001; 61: 1652–8 Agresti A. Categorical Data Analysis. Hoboken: John Wiley, 1990 Lakhan VC, Lavalle PD. Use of loglinear models to assess factors influencing concern for the natural environment. Environ Manage 2002; 30: 77–87 Brack SS, Silacci M, Birchler M, Neri D. Tumor-targeting properties of novel antibodies specific to the large isoform of tenascin-C. Clin Cancer Res 2006; 12: 3200–8 De Santis R, Albertoni C, Petronzelli F, Campo S, D’Alessio V, Rosi A, Anastasi AM, Lindstedt R, Caroni N, Arseni B, Chiodi P, Verdoliva A, Cassani G, Chinol M, Paganelli G, Carminati P. Low and high tenascinexpressing tumors are efficiently targeted by ST2146 monoclonal antibody. Clin Cancer Res 2006; 12: 2191–6 Petronzelli F, Pelliccia A, Anastasi AM, D’Alessio V, Albertoni C, Rosi A, Leoni B, De Angelis C, Paganelli G, Palombo G, Dani M, Carminati P, De Santis R. Improved tumor targeting by combined use of two antitenascin antibodies. Clin Cancer Res 2005; 11: 7137s–45s Akabani G, Reardon DA, Coleman RE, Wong TZ, Metzler SD, Bowsher JE, Barboriak DP, Provenzale JM, Greer KL, DeLong D, Friedman HS, Friedman AH, Zhao XG, Pegram CN, McLendon RE, Bigner DD, Zalutsky MR. Dosimetry and radiographic analysis of 131I-labeled anti-tenascin 81C6 murine monoclonal antibody in newly diagnosed patients with malignant gliomas: a phase II study. J Nucl Med 2005; 46: 1042–51 Higuchi M, Ohnishi T, Arita N, Hiraga S, Hayakawa T. Expression of tenascin in human gliomas: its relation to histological malignancy, tumor dedifferentiation and angiogenesis. Acta Neuropathol 1993; 85: 481–7 Erickson HP. Tenascin-C, tenascin-R and tenascin-X: a family of talented proteins in search of functions. Curr Opin Cell Biol 1993; 5: 869–76 329 33 Bourdon MA, Wikstrand CJ, Furthmayr H, Matthews TJ, Bigner DD. Human glioma-mesenchymal extracellular matrix antigen defined by monoclonal antibody. Cancer Res 1983; 43: 2796–805 34 Carnemolla B, Castellani P, Ponassi M, Borsi L, Urbini S, Nicolo G, Dorcaratto A, Viale G, Winter G, Neri D, Zardi L. Identification of a glioblastoma-associated tenascin-C isoform by a high affinity recombinant antibody. Am J Pathol 1999; 154: 1345–52 35 Natali PG, Nicotra MR, Bigotti A, Botti C, Castellani P, Risso AM, Zardi L. Comparative analysis of the expression of the extracellular matrix protein tenascin in normal human fetal, adult and tumor tissues. Int J Cancer 1991; 47: 811–16 36 Zagzag D, Shiff B, Jallo GI, Greco MA, Blanco C, Cohen H, Hukin J, Allen JC, Friedlander DR. Tenascin-C promotes microvascular cell migration and phosphorylation of focal adhesion kinase. Cancer Res 2002; 62: 2660–8 37 Kachra Z, Beaulieu E, Delbecchi L, Mousseau N, Berthelet F, Moumdjian R, Del Maestro R, Beliveau R. Expression of matrix metalloproteinases and their inhibitors in human brain tumors. Clin Exp Metastasis 1999; 17: 555–66 38 Rorive S, Maris C, Debeir O, Sandras F, Vidaud M, Bieche I, Salmon I, Decaestecker C. Exploring the distinctive biological characteristics of pilocytic and low-grade diffuse astrocytomas using microarray gene expression profiles. J Neuropathol Exp Neurol 2006; 65: 794–807 39 Zagzag D, Friedlander DR, Dosik J, Chikramane S, Chan W, Greco MA, Allen JC, Dorovini-Zis K, Grumet M. Tenascin-C expression by angiogenic vessels in human astrocytomas and by human brain endothelial cells in vitro. Cancer Res 1996; 56: 182–9 © 2007 Blackwell Publishing Ltd, Neuropathology and Applied Neurobiology, 34, 316–329 Received 25 July 2007 Accepted 27 July 2007