Relationships Between Exterior Views and Nurse Stress
advertisement

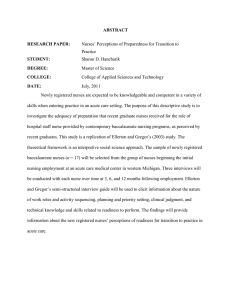
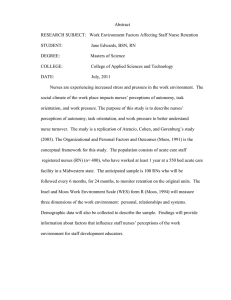
P PA AP PE ER RS S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC Relationships Between Exterior Views and Nurse Stress: An Exploratory Examination Debajyoti Pati, PhD, MASA, AIIA; Tom E. Harvey Jr., AIA, FACHA, MPH; and Paul Barach, MD, MPH Abstract Objective: Examine the relationships between acute stress and alertness of nurse, and duration and content of exterior views from nurse work areas. Background: Nursing is a stressful job, and the impacts of stress on performance are well documented. Nursing stress, however, has been typically addressed through operational interventions, although the ability of the physical environment to modulate stress in humans is well known. This study explores the outcomes of exposure to exterior views from nurse work areas. Methods: A survey-based method was used to collect data on acute stress, chronic stress, and alertness of nurses before and after 12-hour shifts. Control measures included physical environment stressors (that is, lighting, noise, thermal, and ergonomic), organizational stressors, workload, and personal characteristics (that is, age, experience, and income). Data were collected from 32 nurses on 19 different units at two hospitals (part of Children’s Healthcare of Atlanta) in November 2006. Results: Among the variables considered in the study view duration is the second most influential factor affecting alertness and acute stress. The association between view duration and alertness and stress is conditional on the exterior view content (that is, nature view, non-nature view). Of all the nurses whose alertness level remained the same or improved, almost 60% had exposure to exterior and nature view. In contrast, of all nurses whose alertness levels deteriorated, 67% were exposed to no view or to only non-nature view. Similarly, of all nurses whose acute stress condition remained the same or reduced, 64% had exposure to views (71% of that 64% were exposed to Author Affiliations: Dr. Pati is Director of Research at HKS, Inc., in Dallas, TX. Mr. Harvey is Senior Vice President at HKS. Dr. Barach is Chair of the Research Council at the Center for Health Design and a visiting professor of anesthesia and emergency medicine in the Center for Patient Safety at Utrecht University Medical Center in the Netherlands. Corresponding Author: Debajyoti Pati, HKS, Inc., 1919 McKinney Avenue, Dallas, TX 75201 (dpati@hksinc.com). Acknowledgments: This study would not have been feasible without the valuable contributions of D. J. Feather, Pam Black, Taylor Sommers, and Elena Morales at Children’s Healthcare of Atlanta. We acknowledge the assistance provided to us by Dr. Craig Zimring at the Georgia Institute of Technology, College of Architecture. Finally, our appreciation goes to Dr. Gary Evans at Cornell University, College of Human Ecology, for his advice on theoretical issues and recommendations on paper-based measures for perceived stress and arousal. a nature view). Of nurses whose acute stress levels increased, 56% had no view or only a non-nature view. Conclusions: Although long working hours, overtime, and sleep deprivation are problems in healthcare operations, the physical design of units is only now beginning to be considered seriously in evaluating patient outcomes. Access to a nature view and natural light for care-giving staff could bear direct as well as indirect effects on patient outcomes. Key Words: Nursing, acute stress, alertness, natural light, nature view, patient safety, evidence-based design, healthcare architecture Background It could be argued that patient well-being is a function of caregiver well-being. While considerable attention in healthcare architecture and research has focused on improving patient conditions, architectural research focus on the direct caregivers has been limited. This is despite numerous studies demonstrating that nurses are frequently stressed and fatigued, with possible detrimental implications on patient care. The high-stress work environment in which nurses provide care is not new, with scientific publications as far back as the 1980s addressing the issue (Hinshaw & Atwood, 1984). More recent studies focused on nursing empowerment, nurse burnout, and nurse satisfaction (Greco, Laschinger, & Wong, 2006, including several of Laschinger’s previous works) underscore the prevalence and acuteness of the problem. The results of a 2001 nationwide survey of 4,826 nurses revealed that over 70% of the respondents reported stress as one of their top three concerns (Houle, 2001), a finding that has been replicated several times (Tabone, 2004a). Though a severe problem in itself, the high stress level of direct caregivers raises serious concerns pertaining to patient well-being. Although it has not been empirically investigated in healthcare settings in a rigorous manner, studies from other settings suggest that serious implications for performance could result from high levels of stress and fatigue. Stress and fatigue could impact such criti- HERD Vol. 1, No. 2 WINTER 2008 • HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 27 PA P E R S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC cal aspects of performance as reaction time or alertness, irritability, attention to detail, problem solving ability, energy level, and decision-making ability, and thus they could contribute to errors (Barach & Weinger, 2007; Page, 2004; Tabone, 2004b). Moreover, reduced motivation and work performance are typical of tired workers in workplaces, which could equally apply to stressed and tired caregivers in healthcare settings (Tabone, 2004a). While the Institute of Medicine report (Page, 2004) firmly established that patient safety and well-being is heavily dependent on nurses, robust studies linking nurse stress and fatigue with work performance and patient safety had not been widely available. Recent studies in healthcare settings are beginning to identify the relationship among stress, fatigue, and medication errors, especially regarding sleep deprivation and the scheduling of nursing care (Agency for Healthcare Research and Quality, 2001). In a 2005 study that tracked the work patterns of 393 nurses (for example, shift, overtime, hours worked) along with errors and near misses (Oklahoma Nurses Association, 2005-6), it was found that caregiver errors and lapses were correlated with their work patterns. It was further identified that overtime aggravated the situation, especially when it followed a 12-hour shift. This assumes greater seriousness because nurses working more than 12 hours regularly, and as long as 22.5 hours at a stretch in some instances, have been reported in the literature (Page, 2004). The Harvard Work Hours Health and Safety Group has systematically demonstrated an association among work hours, patient safety, and schedules among interns. (Although these studies did not focus on nurses, they provide hard evidence in healthcare settings.) In a randomized study involving an intervention in interns’ work schedules that compared a traditional schedule that included extended work hours with an intervention schedule that eliminated extended work shifts and reduced weekly work hours, Landrigan et al. (2004) demonstrated that the traditional schedule was associated with 35.9% more serious medical errors and 56.6% more nonintercepted serious errors. In a similar interventional study that focused on sleep and attentional failure and that involved 20 interns over a 3-week period, Lockley et al. (2004) found that the rate of attentional failure for interns in the intervention schedule was half that of those on the traditional schedule during on-call nights. Typically, however, the stress problem has been treated as a healthcare operational and management issue, less relevant to the physical environment in which nurses work, where changes to the physical environment occur as a result of operational interventions. Examples include hand-washing stations for infection control and technology integration, which demand novel design solutions. While workflow issues do contribute to stress, the stress-modulating potential of physical design is rarely incorporated in stress research. Instead, long work hours, frequent overtime, sleep deprivation, and similar issues have been the focus of addressing stress and fatigue among care-giving staff. Organizational characteristics as potential 28 WWW.HERDJOURNAL.COM ISSN: 1937-5867 stressors are also frequently addressed. These factors might include the type of relationship with physicians, career development opportunities, recognition for work, and the competence of support staff, among others (Aiken & Patrician, 2000). The predominant focus on operational and managerial issues constitutes a missed opportunity, because the physical environment itself could be an additional source of stress, or it could interact with facility operations to modulate the stress of the work environment. As elaborated below, the physical environment as a stressor has been well documented in previous literature. Noise in the environment has been shown to be a significant environmental stressor, with potentially unsafe consequences for patients and staff. Noise has been shown to affect patients physiologically (blood pressure, heart rate) as well as psychologically (sleep deprivation, pain, intensive care unit (ICU) psychosis, self-reported stress, and annoyance) (Baker, 1984; Morrison et al., 2003; Topf & Thompson, 2001), and it constitutes one of the most important environmental stressors (Moore et al., 1998). Noise has a substantial effect on staff, too. The detrimental impacts of noise on communication, concentration, and cognitive performance, leading to stress and fatigue, have been reported by the World Health Organization (Agency for Healthcare Research and Quality, 2005). Occupational stress originating from high noise levels (that is, telephones, alarms, and beepers) has been shown to be positively related to nurse burnout (Topf & Dillon, 1988). Conversely, the auditory environment also has been shown to have a beneficial influence on patients. For instance, music in waiting rooms has been shown to reduce stress levels in patients (Routhieaux & Tansik, 1997). Beside the auditory environment (the most studied aspect of healthcare physical settings) the impact of other environmental factors is also supported in available literature. Studies in other settings suggest that inappropriate lighting and thermal environments could induce stress in users (Boff & Lincoln, 1988a; Boff & Lincoln, 1988b). Improper ergonomics in the work environment can also result in physical strain in healthcare settings (Bashir, 2002; Benyon & Reilly, 2002; Davis, Badii, & Yassi, 2004; Smedley, Egger, Cooper, & Coggon, 1995; Smedley et al., 2003; Trinkoff, Lipscomb, Geiger-Brown, & Brady, 2002; Waters, Collins, Galinsky, & Caruso, 2006). The negative impacts of hospital wayfinding issues are widely known, and studies report their negative consequences on stress in patients and visitors (Carpman, Grant, & Simmons, 1984). Studies on visual environments have focused on diverse issues, ranging from style to positive distractions. In one study the style (traditional versus nouveau) of interiors was shown to have an influence on mood and reported satisfaction (Leather, Beale, Santos, Watts, & Lee, 2003). Artwork in interiors might reduce stress and improve tolerance to pain (Ulrich & Gilpin, 2003), specifically art representing nature themes (e.g., water, flowers, a garden). The influence of nature is not restricted to artwork alone. Actual views of nature have a similarly favorable influence. In a study comparing natural and urban environments, stress recovery during exposure to nature was shown to be faster and more complete (Ulrich et al., 1991). Typically, however, studies on the positive impact of a view of nature have focused on the patient population. For instance, Wilson (1972) studied the effects of windowless intensive care environments by comparing 100 patients in two ICUs. Results indicated that patients in windowless ICU settings were twice as likely to experience delirium. In a similar study patients in windowless intensive therapy units in two U.K. hospitals were found to have a less accurate memory of their length of stay, were less oriented to time, and were twice as likely to have hallucinations or delusions compared to patients in a unit with windows (Keep, James, & Inman, 1980). Focusing on a separate set of patient outcomes, Ulrich (1984) demonstrated that patients exposed to views of trees through their room windows (as opposed to matched patients exposed to a brick wall) were associated with shorter post-operative stays, fewer pain medications, more favorable comments on nurses’ notes, and fewer minor complications. A subsequent study focusing on preferences (Verderber, 1986) found that nature views were preferred over monotonous views and views of architectural features, such as buildings. Indications that exterior views from healthcare settings may have an impact on nurses are suggested from one study in which staff working in windowless spaces or spaces far from windows reported lower levels of well-being compared to other staff members (Verderber & Reuman, 1987). Study Framework Based on earlier study findings related to patients, we argue that nature views could have similar positive effects on staff. If nature views or representations of nature can affect such a wide assortment of physiological and psychological parameters in patients, could they be used to reduce the stress and fatigue problems of caregivers? Figure 1 represents a framework articulating the relationship between views and stress. There are a number of other environmental and organizational factors that are obvious confounding variables. We designed the study as a preliminary examination of the relationship between view and stress/alertness, with controls for the confounding variables shown in the framework. Research Question We designed the study with the objective to examine the relationship between views and stress with preliminary controls for obvious confounding variables. We studied two outcome parameters: (1) acute stress, and (2) alertness. The study focused on the following questions: 1. What is the relationship between duration of exposure to exterior views, and stress and alertness in nurses? 2. Is the relationship moderated by view content (nature view as opposed to non-nature view)? Method Setting Two pediatric hospitals in the Atlanta metropolitan area that afforded a range of different views were selected for the study. Both the hospitals are under the corporate umbrella of Children’s Healthcare of Atlanta (CHOA). At one hospital the presence of a green zone within the hospital offered a classic nature view situation in some areas. In both hospitals, owing to the general character of the Atlanta metropolitan landscape, views varied from the urban (buildings, streets, and parking) to the natural (trees, greenery) across the various units. Dependent Variables and Measures View Content View Duration PA P E R S Stress Alertness Organizational Characteristics Work Load Physical Environment Characteristics Personal Factors Figure 1. A preliminary framework articulating the relationship between view duration, content, stress/alertness, and other known stressors in a nurse’s work environment. The dependent variables in the study consisted of three measures: (1) acute stress, (2) chronic stress, and (3) alertness. Acute stress was defined as stress usually for a short period of time that could result from work-related pressure, minor mishaps, and other similar factors. Chronic stress was defined as prolonged (ongoing) stress that exists for long durations, resulting from such factors as lifestyle and life events. Alertness was defined as a state of readiness to respond to a stimulus, or response readiness. Acute stress and alertness were measured using the Stress/Arousal Adjective Checklist or SACL (King, Burrows, & Stanley, 1983; Mackay, Cox, Burrows, & Lazzerini, 1978). Adequate internal reliability (Cronbach’s alpha = 0.86 for acute stress and 0.74 for arousal), construct validity of the two scales, and the independence of the two scales have been reported by King, et al. (1983). We used the arousal scale to measure alertness, because arousal and alertness have been used interchangeably in earlier studies (for instance, Paus et al., 1997). Moreover, the SACL arousal HERD Vol. 1, No. 2 WINTER 2008 • HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 29 PA P E R S Relationships between Exterior Views and Nurse Stress: An Exploratory Examination PA P E R S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC scale includes such adjectives as active, vigorous, lively, tired, sleepy, drowsy, passive, energetic, alert, and aroused, which are the ones we were interested in measuring, and they appeared to possess appropriate face validity. It is commonly believed that increased arousal levels can result in performance improvements up to a point, beyond which performance deteriorates (King, et al., 1983). The arousal state (or for our purposes, the nurses’ alertness) was important, because the efficiency of patient care and patient safety partly depends on the response readiness and alertness of nurses. The SACL uses a list of 20 adjectives to assess the current stress and arousal levels of respondents. Ten of the adjectives measure stress and the remainder measure arousal. For each item respondents are required to choose from four responses to indicate the extent to which the adjectives describe their mood at that moment. The four responses are: (1) definitely yes, (2) slightly yes, (3) not sure, and (4) definitely no. The items on stress and arousal are positively or negatively weighted, depending on the directionality of their association with the two parameters of interest. Total acute stress and arousal scores are calculated by aggregating the scores associated with each item. Chronic stress was measured using the Perceived Stress Scale, or PSS-10 (Cohen, 1986; Cohen, Kamarck, & Mermelstien, 1983). The PSS-10 is a global measure of perceived stress, and the 10 items on the scale ask the subject to respond to questions regarding the frequency of certain feelings and thoughts over the past month. The scale measures the perceived level of stressfulness. Adequate internal reliability (alpha coefficient = 0.78) and construct validity of the scale have been reported by Cohen et al. (1983), and Cohen and Williamson (1988). Each item on the scale offers five responses with corresponding numerical ratings: never (0), almost never (1), sometimes (2), fairly often (3), and very often (4). The aggregated chronic stress score is calculated by adding the ratings associated with all 10 items for each respondent. A minor modification was made to the scale by reducing the time period to the past 12 hours as opposed to the past one month. Chronic stress was not expected to change over the period of one shift as a result of the stressors one encounters in the nursing environment. The purpose of including the chronic stress scale was to confirm that the chronic stress level indeed did not change over one shift. Independent Variables and Measures The study involved two independent variables: (1) the duration of exposure to exterior view, and (2) view content (nature versus non-nature view). View duration was defined as the percentage of a work shift that subjects were exposed to exterior views as they performed their work. The measure employed was perceptual, and the data reported the perceived percentage of time that subjects were exposed to exterior views. The exact question posed to respondents was: In 30 WWW.HERDJOURNAL.COM ISSN: 1937-5867 your estimation what is the percentage of the 12-hour shift during which you have a view of the outside? View content was defined as the type of exterior environment that was predominant in the exterior view frames. Like view duration, this was also a perceptual measure (as perceived by the respondents). Two types of environments were included: (1) nature, including trees, plants, bushes, lawns, sky, and water features; and (2) non-nature, including buildings, streets, terraces, and surface parking. The exact question posed to respondents was: Of the duration when you had an exterior view during your work today, what percentage of the view was: (a) A view of nature, and (b) Non-nature (other exterior) views? Both were reported in percentages. The independent variables were measured through self-reporting by the subjects. The data were collected by means of an investigatordesigned questionnaire that included the two independent variables, and a subset of the variables that were used as control measures. Figure 2 presents sample photographs that represent predominantly nature and non-nature views through patient rooms. Figure 2. Photographs through patient room windows showing a representative sample of predominantly nature views (top) and nonnature views (bottom) at the study sites. Control Variables and Measures Environmental factors Data on a number of confounding variables were collected to serve as control measures in the data analysis. Lighting, acoustics, and thermal and ergonomic conditions are known to be potential environmental stressors. Accordingly, these four factors were included in the investigator-designed questionnaire. Respondents were asked to specify on a five-point Likert-type scale the extent to which the four environmental conditions were stressful during that shift (from “not at all” to “very stressful” or “bothersome”). PA P E R S Workload factor Personal factors The second factor that was considered as a potential stressor was workload. Data were collected on the number of hours respondents had worked since their last day off, the number of patients assigned to them on a particular shift, and the percentage of required tasks conducted by an aide (if any). Finally, data on a number of personal and demographic variables were collected. The variables included: (1) age, (2) sex, (3) education level, (4) provider role (e.g., RN, LPN), (5) position in the clinical unit, (6) total years worked as a nurse, (7) total years worked as a nurse in the hospital, and (8) hourly pay range. Table 1 lists the variables included in the study and the corresponding measures. Organizational stress We used the Revised Nursing Work Index (NWI-R) (Aiken & Patrician, 2000) as a surrogate measure for organizational stress. The NWI-R was developed to capture or measure organizational characteristics, not as an organizational stress measure. However, the measure has been shown to be highly correlated with organizational stress outcomes, such as satisfaction, turnover, and retention (Aiken & Patrician, 2000). The NWI-R is a 57-item scale with four response options for each item with associated numerical ratings: strongly agree (1), somewhat agree (2), somewhat disagree (3), and strongly disagree (4). The NWI-R score for respondents is calculated by aggregating the individual scores of the 57 items. We considered higher aggregated scores (higher aggregated disagreement with the existence of positive attributes in the job environment) as a stressor, representing a higher degree of stress. Table 1. Study Variables and Corresponding Measures Variables Measures Dependent Variables Acute Stress Stress/Arousal Adjective Checklist: SACL Chronic Stress Perceived Stress Scale: PSS-10 Arousal State Stress/Arousal Adjective Checklist: SACL Independent Variables Duration of exterior view Questionnaire View content Questionnaire Control Variables Stress from lighting environment Questionnaire Stress from auditory environment Questionnaire Stress from thermal environment Questionnaire Stress from ergonomic factors Questionnaire Workload Questionnaire Work experience Questionnaire Personal/demographic data Questionnaire Stress from organizational characteristics Revised Nursing Work Index: NWI-R The questionnaire was piloted for reliability using a combination of field testing and cognitive pretesting methods prescribed by Krosnick (1999). Two sets of survey instruments were created for the study. The first set was created for data to be collected at the beginning of a shift (before-shift survey), and the second set was created for data to be collected at the end of a shift (after-shift survey). The before-shift survey set included (1) the PSS-10 and (2) the SACL instrument. The after-shift survey included: (1) the PSS-10, (2) the SACL, (3) an investigator-designed questionnaire, and (4) the NWI-R survey. The study protocol was approved by the institutional review board of CHOA. Study Sample We did not restrict the study to any particular unit. Rather, all nurses on all units at the two hospitals were invited to participate in the study. Only registered nurses were invited to participate. Nurse aides were excluded from the study. Before data collection, descriptions of the study and data collection dates were sent by email to all nurses in the two hospitals. In addition, posters announcing the study were placed at key locations in the two hospitals. Data were collected over a period of one 12-hour shift in each of the two hospitals during the month of November 2006. The shifts started at 7:00 a.m. and concluded at 7:00 p.m. Results All respondents were female. There was considerable variability in age and experience. The mean age was 43 years with a range of 24 to 56 years. The mean total work experience as a nurse was 17 years with a range of 1.3 to 35 years. Years worked as a nurse in the hospital had a mean of 11 years, with the range varying between fresh recruits to those having served for 34 years. A total of 55 nurses at the two hospitals volunteered to participate in the study. Volunteering nurses were instructed to complete the before-shift survey set at the beginning of their shift and the after-shift survey set at the end of their shift. A total of 32 nurses from 19 different units in the two hospitals returned their completed surveys. Similar variability was evident in view duration and content. The view duration ranged from zero to 80% of the 12-hour shift, with 43.75% of nurses reporting zero hours of exposure to an external view. Nurses with zero hours’ exposure to the exterior reported working in the pediatric intensive care unit, the emergency department, the rehabilitation unit, the neonatal intensive care unit, the cardiac catheterization lab, and the recovery room. Another 37.5% HERD Vol. 1, No. 2 WINTER 2008 • HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 31 PA P E R S Relationships between Exterior Views and Nurse Stress: An Exploratory Examination PA P E R S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC reported view durations of 10% or less. Of the nurses exposed to some view during the shift, 38% reported exposure to predominantly non-nature views, and 28.6% reported predominantly nature views. Data Analysis Data analysis was conducted using SPSS version 15 for Windows (SPSS 15.0 for Windows, SPSS, Inc., 2006). Three main categories of data analyses were conducted: (1) paired sample comparison, (2) multivariate ordinary least square (OLS) regression and a joint partial F-test, and (3) multivariate regression with interaction terms. The first set of analyses was conducted to assess the construct validity of the instruments used for the study. We expected to observe the following from the paired sample comparisons: (1) Between the beginning and the end of the shift, chronic stress levels would not change. This was not dependent on day-to-day events at one’s workplace; (2) Between the beginning and the end of the shift, arousal levels would generally decrease. This is because after a 12hour work period, one’s state of alertness is expected to decline (nurses would not be as alert as they were at the beginning of the shift); and (3) Between the beginning and the end of the shift, acute stress levels would generally go up. Stressful work in healthcare settings would raise the acute stress level in nursing staff. The results of the data analysis are reported in the subsequent sections. is logical because hospitals are stressful environments, and a rise in acute stress level could be expected for people working for 12 continuous hours in such an environment. Even exposure to a nature view (with a hypothesized positive influence) may not completely compensate for the stressors hospital nurses are exposed to. What impact does view have on nurses working in hospitals? With confidence in the construct validity of our instruments resulting from the paired-sample comparisons, we proceeded to examine the relationship between duration of exposure to exterior views and acute stress and arousal. Relationship Between View Duration, Stress, and Arousal We developed multivariate OLS regression models to identify the impact of view duration on acute stress and arousal levels. Before finalizing the models and running the regression routines, however, we made several manipulations to the data set by combining variables to create index measures. The purpose of creating index variables was two-fold. First, some of the variables were highly correlated. Moreover, the main objective of the study was to explore the association between view content and duration, and stress and arousal. The control variables were included only to account for other factors that are known to induce stress. Thus, we were less interested in exploring the associations between each individual control variable and stress or arousal. This step also helped reduce the number of parameters being tested, considering the sample size. Mean Stress and Arousal Before and After Shift The paired sample comparisons focused on comparing the mean levels of chronic and acute stress and arousal between the beginning and the end of 12-hour shifts. In this phase of analysis no distinctions were made between the nurses based on view content and duration. Table 2 summarizes the results of the paired sample t-tests conducted for each of the dependent variables. The results of the analyses coincided with our expectations. Mean chronic stress levels remained the same. The difference in mean chronic stress levels before and after the shift was not significant. However, the differences in the mean arousal level and mean acute stress level before and after the shift were significant. As expected, the general level of arousal went down between the beginning and the end of the shift, and the mean acute stress level went up for the entire group between the beginning and the end of the shift. This Workload index The first index variable created was “workload,” which included three measures: (1) hours worked since last day off, (2) number of patients under direct care during the shift, and (3) percentage of required tasks conducted by an aide. These three factors were considered to contribute to perceived as well as actual workload, and hence were aggregated. AE index The second index variable was created using four measures: (1) age, (2) number of years worked as a nurse, (3) number of years worked as a nurse in CHOA, and (4) hourly pay bracket. The four variables were highly correlated with one another and formed a meaningful cluster. We termed the new measure “AE Index” (to stand for Age and Experience index). Table 2. Results of the Paired Sample t-Tests for Chronic Stress, Acute Stress, and Arousal, Before and After a 12-Hour Shift Dependent Measure Mean Value Before Shift Mean Value After Shift Difference Between the Means Significance Chronic stress 14.5953 13.6961 –0.89923 0.062 Acute stress –3.9250 –1.8353 2.08969 0.000*** Arousal 7.9714 4.4551 –3.51634 0.000*** *** significant at 0.001 32 WWW.HERDJOURNAL.COM ISSN: 1937-5867 NWI-R score Similarly, education was highly correlated with the NWI-R score. There was no meaningful way to combine the two. Because education level is partly reflected in the AE Index, we decided to drop the variable from the multivariate model. Environmental Stress Finally, we combined the four environmental stressors (that is, lighting, auditory, thermal, and ergonomic) into one variable termed “environmental stress.” Correlational analysis with the recomputed measures showed no major bivariate correlations among the variables. The multivariate models developed with the new set of variables follow: Arousal (after shift) = View (duration) + Arousal (before shift) + Environmental Stress + AE Index + Workload + Organizational Stress Acute Stress (after Shift) = View (duration) + Acute Stress (before shift) + Environmental Stress + AE Index + Workload + Organizational Stress Table 3 summarizes the results of the regression analyses, showing the association between arousal (after shift) and view (duration), controlling for other hypothesized stressors. The model as a whole is significant, and it explains 37.2% of the variability in arousal (after shift). Among all the hypothesized factors bearing an impact on arousal levels (other than before-shift arousal level), analysis suggests that view duration is the second most influential factor. The longer the view duration, the higher the response readiness of nurses at the end of a 12-hour shift will be. The only other measure that has a greater influence is organizational stress. PA P E R S There are other logical implications from the regression results: Organizational stress has a negative influence on alertness. The higher the organizational stress, the lower the arousal level (alertness level) will be at the end of the shift. In addition, both environmental stress and workload have a negative association with arousal, suggesting that higher environmental stress, workload, or both will result in a lower level of alertness at the end of a shift. The only other positive association is with the AE Index, implying that higher age and experience are associated with higher arousal levels (alertness) at the end of a shift, or with greater experience caregivers manage to maintain relatively higher alertness throughout the shift. Considering the relatively strong influence of view duration on arousal level after shift, we ascertained the partial effect of view duration on the latter. A joint partial F-test suggested that view duration alone contributed 4.8% additional explanatory power to the model. To understand the relationship in greater detail, we grouped the respondents into two categories based on the difference between their alertness before and after their shifts, as follows: (1) alertness remained the same or improved, and (2) alertness deteriorated. We found that of all the nurses whose alertness remained the same or improved in the 12-hour period, almost 60% had exposure to exterior views. All of these nurses had exposure to a predominantly nature view. In contrast, of all nurses whose alertness deteriorated between the beginning and the end of the shift, 67% were exposed to no view or only to non-nature views. We conducted a similar set of analyses to understand the relationship between view duration and acute stress. Table 4 summarizes the results of the regression analyses, which show an association between acute stress (after shift) and view (duration), controlling for other hypothesized stressors. As in the case of arousal (not counting before-shift acute stress level), the view was the second most influen- Table 3. Summary of Regression Analyses Showing an Association Between Arousal After Shift and View Duration R R2 R2 adjusted F Significance 0.624 0.389 0.372 22.103 0.000*** Estimate Beta T Significance 7.006 0.000*** Parameters Constant View duration 13.28 0.1 0.273 4.109 0.000*** Arousal (before shift) 0.511 0.502 7.106 0.000*** Environmental stress –0.46 –0.236 –3.693 0.000*** AE Index 0.47 0.159 2.464 0.015* Workload –0.867 –0.191 –3.119 0.002* Organizational stress –3.664 –0.307 –4.851 0.000*** *** significant at 0.001 ** significant at 0.01 * significant at 0.05 HERD Vol. 1, No. 2 WINTER 2008 • HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 33 PA P E R S Relationships between Exterior Views and Nurse Stress: An Exploratory Examination PA P E R S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC tial factor in explaining acute stress levels after shift. Environmental stressors (that is, lighting, acoustics, thermal, and ergonomic) were the most influential factors. Furthermore, workload demonstrated a positive relationship with acute stress: A greater workload is associated with a higher level of acute stress after shift. On the other hand, greater age and experience are associated with lower levels of acute stress after shift. The association between organizational characteristics and acute stress was not significant, but positive. Additionally, a partial F-test of the model suggested that view duration alone explained 6.4% of the variance in after-shift acute stress. stress was conditional on the view content—nature or non-nature. We hypothesized a similar model for arousal. However, partitioning a relatively small sample into three subcategories and corresponding interaction terms has its own analytical pitfalls. We approached the issue by introducing a categorical variable on view content (which, incidentally, has identical problems; sample sizes of the categories were 14 with no view, 13 with predominantly nature views, and 5 with predominantly non-nature views). The results suggest that exposure to a nature view over a non-nature view, and a non-nature view over no view have a beneficial impact on both acute stress and arousal. (Given the small sample size, this conclusion should be treated as merely suggestive; full data are available upon request). Figures 3 and 4 illustrate the interaction effects. Note that we explored only the differences in group means; there is a possibility that the slopes might be different for the three groups, which we did not examine. This does suggest, however, that views (nature or non-nature) have a positive effect on acute stress (Figure 3). Specifically, although acute stress levels went up for the whole group during the shift, the nurses exposed to a nature view had a lower level of stress than those exposed to a non-nature view. The highest acute stress levels were observed in nurses working in a no-view situation. Similarly, a nature view (as opposed to a non-nature view and no view) has a positive effect on alertness (Figure 4). Specifically, although alertness levels went down for the whole group during the shift, nurses exposed to a nature view were at a higher level of alertness than those exposed to a non-nature view. The lowest levels of alertness were observed in nurses working in a no-view situation. One nonconfirming aspect of the multivariate analysis was the direction of the association between view duration and acute stress after shift. We were expecting a negative association. However, the analysis suggests a positive association: Longer view duration was associated with higher post-shift acute stress, everything else remaining the same. To understand this relationship in greater detail, we grouped the respondents into two categories based on the difference between their acute stress levels before and after shift, as follows: (1) acute stress level remained the same or was reduced, and (2) acute stress level increased. We found that of all nurses whose acute stress condition remained the same or was reduced between the beginning and the end of the shift, 64% were exposed to views (71% of the 64% were exposed to a nature view). On the other hand, of all the nurses whose acute stress levels increased between the beginning and the end of the shift, 56% had no view during the shift, or had only a non-nature view. This suggests a beneficial effect of view on acute stress. Discussion Data analysis revealed that: (1) Chronic stress did not change over the period of a 12-hour shift; (2) Acute stress for the whole group went up between the beginning and the end of the shift; and (3) Arousal levels (or alertness) for the whole group went down be- Interaction Effects The conflicting findings on the relationship between view and acute stress prompted us to look for possible interaction effects. Our hypothesis was that the relationship between view duration and acute Table 4. Summary of Regression Analyses Showing an Association between Acute Stress after Shift and View Duration R R2 R2 adjusted F Significance 0.669 0.447 0.431 28.063 0.000*** Parameters Estimate Beta t Significance –6.348 0.000*** Constant –13.223 View duration 0.117 0.266 4.956 0.000*** Acute stress (before shift) 0.499 0.5 9.616 0.000*** Environmental stress 0.847 0.362 6.453 0.000*** AE Index –0.864 –0.244 –4.174 0.000*** Workload 0.599 0.11 1.998 0.047* NWI-R 0.902 0.063 1.157 0.249 *** significant at 0.001 ** significant at 0.01 * significant at 0.05 34 WWW.HERDJOURNAL.COM ISSN: 1937-5867 PA P E R S 0 -0.5 Before Shift After Shift Acute Stress Scale -1 -1.5 No View -2 Non-Nature View -2.5 Nature View -3 -3.5 -4 -4.5 Figure 3. Figure shows the interaction effect of view types on acute stress, with nurses exposed to views at a lower level of acute stress. (Note that the possibility of slope interaction was not explored.) 9 8 Arousal Scale 7 6 5 No View 4 Non-Nature View Nature View 3 2 1 0 Before Shift After Shift Figure 4. Figure shows the interaction effect of view types on alertness, with nurses exposed to a nature view (as opposed to a non-nature or no view) at a higher level of alertness. (Note that the possibility of slope interaction was not explored.) tween the beginning and the end of the shift. These three findings contributed to the construct validity of our study instruments. Because this study was designed as a preliminary examination, our primary focus was on the directionality of the relationships rather than on absolute values. Despite the small sample, findings were consistent with our expectations. Furthermore, the multivariate OLS regression analyses suggest that exposure to view is an influential factor in explaining both arousal and acute stress after shift. In fact, view explained as much as 5% to 6% of the variance in arousal and acute stress after shift. More notable are the findings that, among the variables considered in the study, view is second only to stress associated with organizational characteristics (in the case of alertness) and environmental stress HERD Vol. 1, No. 2 WINTER 2008 • HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 35 PA P E R S Relationships between Exterior Views and Nurse Stress: An Exploratory Examination PA P E R S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC Organizational Characteristics Work Load Personal Factors Organizational Characteristics Work Load Personal Factors Staff Outcome Physical Environment Patient Outcome Organizational Outcome Figure 5. Model of the potential direct and indirect impact of care-giver view on the patient and the organization. (in the case of acute stress) in its influence. Finally, the implication that the relationship between view duration and stress/arousal could be conditional on view content is important to people in both healthcare design and healthcare operations planning. More specifically, the probability of the study’s findings conforming to a series of expected outcomes purely by chance is so low that it partly offsets any shortcomings related to the nonexperimental design and sample size of the study. Because long working hours, overtime, and sleep deprivation are problems in healthcare operations, the suggestion that the physical design of clinical units could potentially improve the situation significantly is of considerable importance. As mentioned earlier, stress and alertness have hypothetical associations with safety issues. Moreover, these results offer a rather simple way to create inspiring spaces that promote enthusiasm among nurses, enhance job satisfaction and retention, and promote calm in an intense dayto-day work environment. This would necessitate a rethinking of the way we approach healthcare facility design. Currently considerable emphasis is placed on nature views and natural light in patient rooms. The issue, however, is less frequently discussed in the context of the caregiver’s environment, particularly those who work in areas of the hospital that do not afford occasional views through patient rooms. Access to a nature view or natural light or both for care-giving staff could have a direct as well as an indirect effect on patient outcomes. Figure 5 demonstrates this hypothesis, which also suggests that these phenomena could impact organizational objectives such as staff retention/turnover/recruitment, variable costs, and market share. Future studies should address one major confounding factor that was not dealt with in this study. This confounding factor pertains to view as opposed to natural light. Incidentally, this shortcoming is also typical of the seminal studies mentioned in the introductory section. In other words, it is not clear whether the positive influence of exposure to the exterior on patients and staff is associated with the view, with natural light, or both. Limitations of the Study Despite the small sample in this study, the fact that a range of expected outcomes was confirmed by data analysis is notable, and it develops a good foundation and confidence for subsequent studies. 36 WWW.HERDJOURNAL.COM ISSN: 1937-5867 This is especially important considering the impact natural light bears on the neurobiological and physiological processes of human beings. Recent studies are adding considerable weight to the associations between light wavelength, circadian rhythm, and alertness, among other outcomes. Lockley et al. (2005) designed a between-subject study involving 16 healthy adults at the Intensive Physiological Monitoring Unit at Brigham and Women’s Hospital in Boston. One group was exposed to monochromatic light wavelength of 460 nm (blue light), and the other group was exposed to monochromatic light wavelength of 555 nm (green light), for a period of 6.5 hours. They found that subjects exposed to 460 nm light had fewer attentional failures, decreased auditory reaction time, and lower sleepiness ratings. The study was an extension of an earlier study (Lockley, Brainard, & Czeisler, 2003) that articulated the variable impact of light wavelength on human circadian rhythm, specifically the impact of blue light on human circadian pacemakers. These studies begin to suggest that spectral qualities of light (or natural light) may significantly impact the alertness of nurses, irrespective of the availability of exterior view, with identifiable implications on patient safety parameters. Future studies need to address this topic. Regardless of the outcome of such future studies, the findings will have a major impact on the way nursing units are designed. In addition to the perception measures employed in this study, objective measures of physiological correlates of stress and duration of view in any future studies would begin to provide information that could directly affect how hospitals are designed for safety in the future. Conclusions and Implications for Hospital Design and Operation Why is this study critical to hospital administrators, nurses, and patients and their families? The study reveals that visual relief can positively affect caregivers: It can, on a daily basis, improve alertness and sharpen focus in an intense day-to-day work environment. On a long-term basis, it might enhance job satisfaction and retention, which consequently lowers operating costs. Additionally, higher response readiness should mean improved patient safety. Quality of view—referring to visual and perhaps mental respite—is shown to be a significant, possibly critical, factor in caregivers’ focus on their subjects (patients) and their tasks (care giving). These findings warrant a change in facility planning priorities and the operational policies of healthcare facilities. The message to trustees, administrators, and their planning and design consultants might be to: 1. Embrace the importance of view and visual relief—especially for staff work areas—as capital planning and budgeting are conducted. 2. Require that the programming of space requirements include a specific description of design intent (for a generous view) along with the allocation of space to accommodate these elements of design. 3. Insist that the design of capital projects demonstrate attention to the provision of views in all areas of the workplace created for staff. This single goal, stated as a guiding principle for a project, will have an immense impact on physical design. 4. Mandate restorative breaks as an integral aspect of operational policy. This could partly address the serious issue of patient safety that healthcare organizations are struggling with today. Insist that employees take breaks that include views—away from their work environment, if necessary, if views are otherwise unavailable. References Agency for Healthcare Research and Quality. (2001). Making health care safer: A critical analysis of patient safety practices. Rockville, MD: Agency for Healthcare Research and Quality. Retrieved April 20, 2006, from http://www.ahrq.gov/ Clinic/ptsafety/index.html PA P E R S Agency for Healthcare Research and Quality. (2005). Creating a culture of patient safety through innovative hospital design. In Advances in Patient Safety, Vol. 2. Rockville, MD: Agency for Healthcare Research and Quality. Retrieved April 20, 2006, from http://www.ahrq.gov/downloads/pub/advances/vol2/Reiling.pdf Aiken, L. H., & Patrician, P. A. (2000). Measuring organizational traits of hospitals: The revised nursing work index. Nursing Research, 49(3), 146–153. Baker, C. F. (1984). Sensory overload and noise in the ICU: Sources of environmental stress. Critical Care Quarterly, 6(4), 66–80. Barach, P., & Weinger, M. (2007). Trauma team performance. In W. C. Wilson, C. M. Grande, & D. B. Hoyt (Eds.), Trauma: Emergency resuscitation and preoperative anesthesia management, Vol. 1. New York: Marcel Dekker, Inc. Bashir, M. (2002). Avoiding muscular strain in patient-care activities. Nursing Journal of India, 93(4), 80–81. Benyon, C., & Reilly, T. (2002). Epidemiology of musculoskeletal disorders in a sample of British nurses and physiotherapists. In T. Reilly (Ed.), Musculoskeletal disorder in health related occupations. Lancaster: IOS Press. Boff, K. R., & Lincoln, J. E. (1988a). Engineering data compendium: Human perception and performance, Vol. 1. Wright-Patterson A.F.B., OH: Harry G. Armstrong Aerospace Medical Research Laboratory. Boff, K. R., & Lincoln, J. E. (1988b). Engineering data compendium: Human perception and performance , Vol. 3. Wright-Patterson A.F.B., OH: Harry G. Armstrong Aerospace Medical Research Laboratory. Carpman, J., Grant, M., & Simmons, D. (1984). No more mazes: Research about design for wayfinding in hospitals. Ann Arbor, MI: The University of Michigan Hospitals. Cohen, S. (1986). Contrasting the Hassle Scale and the Perceived Stress Scale. American Psychologist, 41, 717–718. Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health. Newbury Park, CA: Sage Publications. Cohen, S., Kamarck, T., & Mermelstien, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. Davis, P. M., Badii, M., & Yassi, A. (2004). Preventing disability from occupational musculoskeletal injuries in an urban, acute and tertiary care hospital: Results from a prevention and early active return-to-work safely program. Journal of Occupational and Environmental Medicine, 46(12), 1253–1262. Greco, P., Laschinger, H. K. S., & Wong, C. (2006). Leader empowering behaviours, staff nurse empowerment and work engagement/burnout. Nursing Leadership, 19(4), 41–56. Hinshaw, A. S., & Atwood, J. R. (1984). Nursing staff turnover, stress and satisfaction: Models, measures and management. In H. H. Werley & J. J. Fitzpatrick (Eds.), Annual Review of Nursing Research: Vol 1 (pp. 133–153). New York: Springer. Houle, J. (2001). Health and safety survey. American Nurses Association. Retrieved April 2, 2006, from http://nursingworld.org/MainMenuCategories/OccupationalandEnvironmental/occupationalhealth/HealthSafetySurvey.aspx Keep, P. J., James, J., & Inman, M. (1980). Windows in the intensive therapy unit. Anaesthesia, 35(3), 257–262. King, M. G., Burrows, G. D., & Stanley, G. V. (1983). Measurement of stress and arousal: Validation of the stress/arousal adjective checklist. British Journal of Psychology, 74, 473–479. Krosnick, J. A. (1999). Survey research. Annual Review of Psychology, 50, 537– 567. Landrigan, C., Rothschild, J., Cronin, J., Kaushal, R., Burdick, E., Katz, J., et al. (2004). Effect of reducing interns’ work hours on serious medical errors in intensive care units. The New England Journal of Medicine, 351(18), 1838–1848. Leather, P., Beale, D., Santos, A., Watts, J., & Lee, L. (2003). Outcomes of environmental appraisal of different hospital waiting areas. Environment & Behavior, 35(6), 842–869. Lockley, S. W., Cronin, J., Evans, E., Cade, B., Lee, C., Landrigan, C., et al. (2004). Effect of reduced interns’ weekly work hours on sleep and attentional failures. The New England Journal of Medicine, 351(18), 1829–1837. HERD Vol. 1, No. 2 WINTER 2008 • HEALTH ENVIRONMENTS RESEARCH & DESIGN JOURNAL 37 PA P E R S Relationships between Exterior Views and Nurse Stress: An Exploratory Examination PA P E R S HERD Volume 1, Number 2, pp 27-38 Copyright ©2008 Vendome Group, LLC Lockley, S. W., Brainard, G. C., & Czeisler, C. S. (2003). High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. The Journal of Clinical Endocrinology & Metabolism, 88(9), 4502–4505. Lockley, S. W., Evans, E. E., Scheer, F., Brainard, G. C., Czeisler, C. A., & Aeschbach, D. (2005). Short-wavelength sensitivity for the direct effects of light on alertness, vigilance, and the waking electroencephalogram in humans. Sleep, 29(2), 161–168. Mackay, C., Cox, T., Burrows, G., & Lazzerini, T. (1978). An inventory of the measurement of self-reported stress and arousal. The British Journal of Social and Clinical Psychology, 17, 283–284. Moore, M., Nguyen, D., Nolan, S., Robinson, S., Ryals, B., Imbrie, J., et al. (1998). Interventions to reduce decibel levels on patient care units. American Surgeon, 64(9), 894–899. Morrison, W. E., Haas, E. C., Shaffner, D. H., Garrett, E. S., & Fackler, J. C. (2003). Noise, stress, and annoyance in a pediatric intensive care unit. Critical Care Medicine, 31(1), 113–119. Oklahoma Nurses Association. (2005-2006). Implications of fatigue on patient safety. The Oklahoma Nurse, 50(4), 7–8. Page, A. (2004). Keeping patients safe: Transforming the work environment of nurses. Washington, DC: The National Academy Press. Paus, T., Zatorre, R., Hofle, N., Caramanos, Z., Gotman, J., Petrides, M., et al. (1997). Time-related changes in neural systems underlying attention and arousal during the performance of an auditory vigilance task. The Journal of Cognitive Neuroscience, 9, 392–408. Routhieaux, R. L., & Tansik, D. A. (1997). The benefits of music in hospital waiting rooms. Health Care Supervisor, 16(2), 31–40. Smedley, J., Egger, P., Cooper, C., & Coggon, D. (1995). Manual handling activities and risk of low back pain in nurses. Occupational and Environmental Medicine, 52, 160–163. Smedley, J., Inskip, H., Trevelyan, F., Buckle, P., Cooper, C., & Coggon, D. (2003). Risk factors for incident neck and shoulder pain in hospital nurses. Occupational and Environmental Medicine, 60, 864–869. 38 WWW.HERDJOURNAL.COM ISSN: 1937-5867 Tabone, S. (2004a). Data suggest nurse fatigue threatens patient safety. Silver Spring, MD: Center for American Nurses. Tabone, S. (2004b). Nurse fatigue: The human factor. Texas Nursing, June–July, 1–3. Topf, M., & Dillon, E. (1988). Noise-induced stress as a predictor of burnout in critical care nurses. Heart Lung, 17(5), 567–574. Topf, M., & Thompson, S. (2001). Interactive relationships between hospital patients’ noise-induced stress and other stress with sleep. Heart Lung, 30(4), 237–243. Trinkoff, A. M., Lipscomb, J. A., Geiger-Brown, J., & Brady, B. (2002). Musculoskeletal problems of the neck, shoulder, and back and functional consequences in nurses. American Journal of Industrial Medicine, 41(3), 170–178. Ulrich, R. S. (1984). View through a window may influence recovery from surgery. Science, 224(4647), 420–421. Ulrich, R. S., & Gilpin, L. (2003). Healing arts: Nutrition for the soul. In S. B. Frampton, L. Gilpin, & P. Charmel (Eds.), Putting patients first: Designing and practicing patient centered care (pp. 117–146). San Francisco: Jossey-Bass. Ulrich, R. S., Simons, R. F., Losito, B. D., Fiorito, E., Miles, M. A., & Zelson, M. (1991). Stress recovery during exposure to natural and urban environments. Journal of Environmental Psychology, 11(2), 201–230. Verderber, S. (1986). Dimensions of person-window transactions in the hospital environment. Environment & Behavior, 18(4), 450–466. Verderber, S., & Reuman, D. (1987). Windows, views, and health status in hospital therapeutic environments. Journal of Architectural & Planning Research, 4(2), 120–133. Waters, T., Collins, J., Galinsky, T., & Caruso, C. (2006). NIOSH research efforts to prevent musculoskeletal disorders in the healthcare industry. Orthopaedic Nursing, 25(6), 380–389. Wilson, L. M. (1972). Intensive care delirium: The effect of outside deprivation in a windowless unit. Archives of Internal Medicine, 130(2), 225–226.