Neuropsychologia 40 (2002) 327– 334
www.elsevier.com/locate/neuropsychologia
Dissociated long lasting improvements of straight-ahead pointing
and line bisection tasks in two hemineglect patients
Laure Pisella a,*, Gilles Rode a,b, Alessandro Farnè c, Dominique Boisson a,b,
Yves Rossetti a,b
a
Institut National de la Santé et de la Recherche Médicale, Unité 534: Espace et Action, 16 a6enue Lépine, Case 13, 69676 Bron, France
b
Hôpital Henry Gabrielle-B.P. 57 -F-69565 Saint Genis La6al Cedex, France
c
Dipartimento di Psicologia, Uni6ersità di Bologna, Bologna, Italy
Received 12 May 2000; received in revised form 31 January 2001; accepted 3 May 2001
Abstract
In this experiment, we evaluated over a longer time period the previously demonstrated effects of a short prism adaptation on
hemispatial neglect. We followed two patients (PE and SA), during a period of 5 days (1 day before and 4 days after the prism
adaptation procedure), repeatedly measuring their performances on a straight-ahead pointing task and a line bisection task. We
also assessed the comparative temporal evolution of the rightward biased egocentric reference frame (as measured by the
straight-ahead demonstration) and a classical neuropsychological symptom of neglect, namely the rightward bias observed on line
bisection. Firstly, the results showed that prismatic effect could be maintained for 4 days, on the two tasks (separately
straight-ahead for PE, line bisection for SA). This long-term effect implies a very profound action of prism adaptation based on
active processes and opens large possibilities for clinical applications. Secondly, no correlation was found between the evolution
of the performances on the two tasks, neither for patient PE, nor for patient SA (within-subject double-dissociation). Moreover,
a double-dissociation between subjects was demonstrated on long-term effects. A new conception has thus to be found to explain
the various symptoms manifested in neglect and more investigations have to be performed in order to establish to what extent they
can be considered independent. It can be concluded that elucidating the mechanism through which prism adaptation affects
neglect could lead to a better understanding of the neglect syndrome. © 2001 Elsevier Science Ltd. All rights reserved.
Keywords: Double-dissociation; Egocentric reference; Hemispatial neglect; Plasticity; Prism adaptation; Space representation
1. Introduction
The syndrome of unilateral neglect is frequently observed in right-handed patients following right hemisphere brain damage. This condition can be defined as
a loss of visual awareness for contralesional stimuli
despite residual implicit processing [10,24]. Typically,
the patient fails to report, respond to or orient toward
left-sided stimuli [15,18], or tends to underestimate it
[28]. Neglect symptoms have been described to range
from sensori –motor levels [17,26] to mental representations of space [4,31]. In addition, neglect is responsible
for poor functional recovery and is resistant to treatment [12].
* Corresponding author. Fax: + 61-3-9347-6618.
E-mail address: pisella@psych.unimelb.edu.au (L. Pisella).
Orienting in space requires an integration of retinal,
eye-position and head-position signals, together with
vestibular information. These signals are classically
considered to be further transformed to build a unitary
egocentric reference, aligned with the sagittal body axis
(review in [21]). This hypothesis draws on the notion
that spatially-directed behaviour from perception to
action has to be coded in a supramodal coordinate
system. One of the classical manifestations of hemispatial neglect is an alteration of the egocentric reference,
which can be tested by requiring the subject to point
straight-ahead in the dark [20,44]. Patients often produce subjective mid-line demonstrations deviated to the
right [7,16].
Along this line, a reference-shift hypothesis of neglect
has been proposed, according to which all the orienting
biases observed in neglect patients [1,13,17,26,27] are
0028-3932/01/$ - see front matter © 2001 Elsevier Science Ltd. All rights reserved.
PII: S 0 0 2 8 - 3 9 3 2 ( 0 1 ) 0 0 1 0 7 - 5
328
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
due to ‘‘an illusory rotation of the egocentric reference,
somewhat as if the subject felt being constantly rotated
toward the lesion side’’ [19]. Postulating that the rightward shift of the egocentric reference constitutes the
anchor of the neglect syndrom [23], this hypothesis
predicts that a restoration of the centred straight-ahead
demonstration should produce an improvement in performance on other neglect tests. Support for this hypothesis was found in the temporary improvement of
neglect patients after different types of physiological
manipulation [5,22,30– 32,37,41] that compensate for
the pathological shift of the egocentric reference, and
hence afford an improvement of the patient’s behaviour
in the left hemispace [23].
More recently, however, Chokron and Bartolomeo
[6], Farnè et al. [11] and Bartolomeo and Chokron [2]
studied two, 23 and 18 neglect patients respectively and
challenged this reference shift theory of hemispatial
neglect by showing that not all patients exhibited a
rightward shift of the egocentric reference. In those
three studies, a total of 43 patients were examined, and
only 27 of them exhibited a deviation of the manual
straight-ahead to the right. In addition, Farnè et al. [11]
showed that the same proportion of right brain-damaged patients without neglect exhibited a similar trend.
In a previous investigation, we studied 16 neglect
patients with the aim of testing the effects of the
adaptation to an optical deviation towards the ipsilesional side on their spatial deficit through two experiments [34]. In the first experiment, the effect of prism
adaptation was tested on manual straight-ahead
demonstration with eyes closed. After adaptation, all
patients exposed to the optical shift of the visual field
(n= 8) showed an improvement on this task. In the
second experiment, the effect of prism adaptation on
clinical manifestations of neglect was tested on six
patients, as assessed by classical neuropsychological
tests. The battery included the line bisection task, line
cancellation task, drawing from memory, copying and
reading. Upon removal of the prisms, each of the six
patients (four with hemianopia and two without hemianopia) showed an improvement in performance on
each of these five tests, showing that prism adaptation
improves symptoms of spatial neglect [34]. A control
group of six neglect patients performing the pointing
procedure with neutral goggles exhibited no significant
improvement. By contrast with the other physiological
manipulations [5,22,30– 32,37,41], this improvement
was maintained 2 h after the prism exposure [34].
The first question raised by these former results
involved the potential duration of the benefits induced
by prism adaptation. We therefore followed the performances of two neglect patients over a testing period of
1 week on two continuous and sensitive tests adapted to
repeated measures: straight-ahead demonstration and
line bisection.
This longitudinal study allowed us to assess a secondary question about the reference shift hypothesis of
neglect. In our previous study [34], the three neglect
patients who took part in the two experiments were
improved on both the straight-ahead demonstration
(Exp. 1) and the classical neuropsychological tests (Exp.
2). This conjunction may support the view that the core
of neglect is indeed a deviation of the internally represented midsagittal plane of the body [23]. If this view is
correct, a covariation should be expected for the two
types of performance. Alternatively, if the deviation of
the egocentric reference and the visual neglect symptoms rely on separate mechanisms, it should be possible
to selectively alter one of them without affecting the
other (simple dissociation) and vice versa (double-dissociation). If no correlation is observed between the two
tested variables, then at least two different and independent mechanisms have to be advocated, each being
responsible for a particular neglect symptom. Hence,
we also compared the effects of prism adaptation on
straight-ahead demonstrations (evaluating the egocentric reference) and on line bisection (one of the most
sensitive tests of neglect) in these two neglect patients.
A lack of correlation between the egocentric reference
and a cancellation task has been obtained recently with
a group analysis [11]. It should be emphasised here that
the lack of an inter-individual correlation (as obtained
by [11] or [2]) does not rule out the possibility for an
intra-individual link between the two variables explored. Only longitudinal studies can distinguish
changes over time within individuals from differences
among people in their baseline levels (cohort effect);
Cross-sectional studies cannot [9]. Repeated observations of individuals enable a direct study of change in
parameters A and B. These changes can be used to
assess the link between A and B in a more sensitive
manner. The advantages of using prism adaptation is
that it allowed us to compare the temporal evolution of
the two parameters within-subject (as well as between
subjects), assuming that prism adaptation will trigger
alterations in at least one of the tested parameters. If
the two parameters were to show the same evolution
over time, it would be compatible with the hypothesis
that the prismatic effect on cognitive symptoms is mediated by an alteration of the egocentric reference.
2. Methods
2.1. Cases description
Two right-handed females [SA (56) and PE (47)]
showing left unilateral neglect consecutive to a damage
of the right hemisphere participated in the study. Both
had been admitted to a neurological rehabilitation unit
for severe left hemiplegia. Clinical features are de-
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
Table 1
Delay post onset
Left hemiparesis
Left hemianesthesia
Left hemianopia
Head and gaze
deviation
Anosognosiaa
Left auditory
extinction
Aethiology
Site lesions (C.T.
scan data)
SA
PE
3 weeks
Present
Present
Present
Present
8 weeks
Absentb
Absent
Present
Present
1
Present
0
Present
Haemorrhagic
Basal ganglia,
caudate
Paraventricular
white matter
Internal capsule
Ischemic
Frontal, temporal
Paraventricular white
matter
Internal capsule
a
Assessed by the four point scale of Bisiach et al., 1986 [3]: score
0, the deficit was spontaneously reported or mentioned by the patient
following a general discussion about his complaints; score 1, the
disorder was reported only following a specific question about the
strength of the patient’s left limbs; score 2, the disorder was acknowledged only after its demonstration through routine techniques of
neurological examination and score 3, no acknowledgement of the
disorder could be obtained from the patient.
b
The left hemiparesis of patient PE resolved during her stay and
was not present at the time of testing.
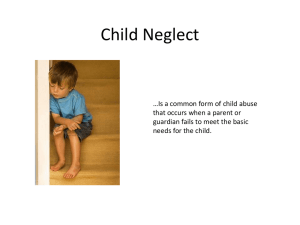
scribed in Table 1. The two patients showed a rather
extensive unilateral brain lesion, which was documented
by CT-scan (Fig. 1). Patients had no past history of
stroke and did not suffer from impaired vigilance,
confusion, general mental deterioration or psychiatric
disorders. The two patients showed severe neglect affecting extrapersonal and personal space. They were
included in the study following a neurospychological
screening based on a routine protocol [32]. PE scored
329
10 left on the Albert cancellation test, 3+ 1 on the
Gainotti copying test (following the scoring procedure
described in [34]) and drew nine petals on the right
versus one on the left on the daisy drawing test. SA
scored 10 left on the Albert cancellation test, 3+ 2 on
the Gainotti copying test and drew nine petals on the
right versus 1on the left on the daisy drawing from
memory.
2.2. Experimental set up and procedure
The two patients were tested during five consecutive
days. The effect of prism adaptation on the straightahead pointing and line bisection test was repeatedly
evaluated over ten sessions within this time period.
These two tests were administered 1 day before (−24
h), just before (− 1 h), just after (0 h) and every 2 h
after a short prism-adaptation session during Day 1
(+2, + 4 and + 6 h), then again over the next 3 days
[Day 2 (+ 24 h, +30 h), Day 3 (+ 48 h) and Day 4
(+72 h)].
2.2.1. Straight-ahead pointing test
Patients were blindfolded and seated in front of a
box that allowed pointing location to be recorded with
an accuracy of 0.1°. They were required to make free
pointings straight-ahead from a starting position near
their sternum, with their eyes closed. After every trial,
subjects returned their hand to the starting position.
Throughout the task, their head was kept aligned with
the body sagittal axis using a chin-rest. Ten trials were
performed in order to obtain a reliable average value.
The pointing error was measured as the angle between
the pointing position and the objective body midline
and carried a minus sign for leftward pointing and a
plus sign for rightward pointing.
2.2.2. Line bisection test
Patients were asked to mark the midline of 20 horizontal lines presented in the right, centre and left part
of the same testing sheet [38]. This sensitive test allowed
us to compute a score reflecting the bias in line bisection. This score was calculated as proposed by
Schenkenberg et al. [38]. It expresses the mean percentage of horizontal deviation in line bisections, towards
the right (signed positive) or towards the left (signed
negative).
Fig. 1. Reconstruction of the lesions of patients PE and SA, based on
cranial MRI scans. Horizontal sections show large right-sided subcortical (SA) and cortico-subcortical (PE) lesions (depicted in black).
2.2.3. Prism-adaptation procedure
The exposure period consisted of 50 pointing trials
made by right hand towards visual targets presented at
10° to the right and to the left of the body midline in a
80× 80 cm box (as in [34]). During this pointing session
patients were asked to point at a normal speed. They
could see the target and only the second half of their
pointing trajectory, as well as their terminal error. The
330
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
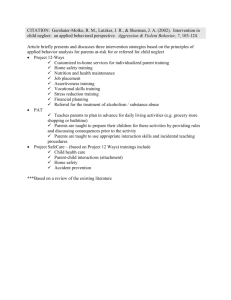
Fig. 2. Temporal evolution of the performance of the two patients in the straight-ahead pointing task. Positive values correspond to right
deviations, and negative ones to left deviations. The shadowed area represents the Pretesting period gathering the two sessions realised by the
patients before the single prism adaptation procedure. The X-axis zero corresponds to the experimental testing performed just after adaptation
(upon prism removal).
left-based wedge prisms used in this experiment were
wide field glasses inserted into light goggles. With these
goggles on, the visual field was uniformly shifted by 10°
to the right. In normal subjects, rapid adaption usually
occurs to resolve the visuo-motor discrepancy. By contrast to a previous study which used a leftward prismatic
shift to draw attention to the neglected field [36], our
experiment was designed to test whether the compensatory after-effects of adaptation to a rightward prismatic
shift could improve neglect [34]. Hence, subjects were
always tested without prisms, both before (pretest) and
after (post-test) the adaptation procedure.
2.2.4. Statistical analysis
A one way ANOVA was used to investigate the
effects of Subject and Period of testing.
3. Results
3.1. Straight-ahead demonstration
In the pretests, both patients exhibited a shift of the
straight-ahead pointing towards the right side (Fig. 2).
Just before the prism exposure, the mean deviations of
patients PE and SA were evaluated to 3.8 and 14.9°
respectively.
During the initial stage of the post-tests (day 1), the
mean deviation of both SA and PE was reduced. The
two patients followed a similar pattern of evolution.
Just after adaptation to the 10° rightward optical deviation, the straight-ahead demonstration was shifted
about 9° leftward in the two patients. This immediate
aftereffect gradually decreased in both patients during
the first 4 h following prism adaptation. After this
short-term effect, the evolution of the mean deviations
began to differ between the two patients. Four hours
after the adaptation, the straight-ahead demonstration
of patient PE was correct (ie close to 0°) whereas the
deviation of patient SA was back to the value of the
second pretest.
In the late-tests, the performance of patient PE
seemed to be stabilised around the normal value. By
contrast, patient SA did not show a long-term improvement with respect to the demonstration performed prior
to prism adaptation.
3.2. Line bisection test
In the pretests, both patients exhibited positive deviation scores, that is that their bisection of horizontal lines
was shifted to the right of the objective centre, independently of the location of the line in the testing sheet (Fig.
3). Just before prism adaptation, the deviation scores of
SA and PE were 50.5 and 12.4% respectively, ie both
were above the liminar value of 11% used by Schenkenberg et al. [38] to define a pathological deviation.
In the post-tests, the score of SA was dramatically
reduced, whereas the score of PE remained unchanged.
Immediately after the prism exposure, the deviation
score of SA was reduced to the value of 24%. Two hours
after, the performance of SA was further improved up
to normal values and the effect seems to be durable
throughout the late-tests. By contrast, no improvement
was observed for Patient PE, either in the short-term or
in the long-term.
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
3.3. Statistical analysis
In order to investigate more precisely the effect of
prism adaptation, an analysis of variance contrasting
the pretest and the post-test periods was performed
(one way ANOVA, two periods). For patient SA, measures made during these two periods were significantly
different for straight-ahead pointing (F(1,92) = 85.2;
PB 0.001) and for the Schenkenberg test (F(1,190)=
23.4; PB 0.001). For patient PE, a significant difference
between these two periods was only found for straightahead pointing (F(1,102) \116.9; P B 0.001) and not
for the Schenkenberg test (F(1,190) = 0.66; P \ 0.1).
In order to distinguish in more detail between transient and long-lasting improvement after prism adaptation (as described in the qualitative analysis), we
divided the post-test period into two parts: measures
performed on the 1st day of the prism exposure (day 1)
and measures performed during the following 3 days
(late-test). For each patient, an additional ANOVA was
performed with contrasts in order to compare the three
defined periods by pairs (planned comparisons between
pretests, day 1 and late-tests).
3.3.1. Straight-ahead pointing
The pretests were significantly different from day 1
(F(1,102)\111; pB 0.01) and from the Late-tests (both
Fs(1,102)\ 86; PB0.001) for patient PE. Furthermore,
day 1 and late-tests were not significantly different
(F(1,102)\3; P\0.05). These results showed a durable
effect of prisms on straight-ahead pointing task for
patient PE. A significant difference was found between
performances of patient SA measured 24 h before and
just before the prism adaptation (Post Hoc test Scheffé
PB 0.005). For the sake of carefulness, the contrast
331
analysis performed for patient SA excluded this first
measure (24 h before prism adaptation). Even the single
measure made just before prism adaptation was significantly different contrasting with all eight measures
made after it (F(1,92)= 10.4; PB 0.005). A significant
difference was found contrasting the measure made just
before prisms (preperiod) and those made in day 1
(F(1,92)= 18.9; PB 0.005), although it was not contrasting pre and late periods (F(1,92)= 3.1; P\0.05).
Furthermore, day 1 and late periods were found to be
significantly different (F(1,92)= 17; PB 0.001). These
results reflect only a transient effect of prisms on
straight-ahead pointing task for patient SA.
3.3.2. Schenkenberg test
No difference between the three periods was found
for patient PE [pre vs day 1 (F(1,190)= 0.05; P\0.8),
pre vs late (F(1,190)=1.6; P\0.2) and day 1 vs late
(F(1,190)= 1.6; P \0.2)), which indicated that prism
adaptation had no significant effect on line bisection
task for this patient. By contrast, performances of
patient SA were significantly different between pre and
day 1 periods (F(1,190)=17.5; PB 0.001) as well as
between pre and late (F(1,190)= 21.6; PB 0.001). No
significant decrease of the adaptation effect was found
between day 1 and late (F(1,190)= 0.3; P\ 0.5). Prism
exposure thus produced a durable effect on patient SA.
Interestingly, no significant correlation was found
between the results of the straight-ahead and the
Schenkenberg tests whether the analysis was performed
with both patients together (R 2 = 0.15; F(1,18)=0.53;
P\0.6) or for each patient separately (R 2 =0.16;
F(1,8)= 1.21; P\0.2 for patient SA and R 2 =0.89;
F(1,8)= 0.88; P\ 0.4 for patient PE) This result is
compatible with the absence of a causal link between
Fig. 3. Temporal evolution of the performance of the two patients in the line bisection task (Schenkenberg test). The deviation score (%) is
calculated as in Schenkenberg et al. (1980) [38]. Same legend as in Fig. 2.
332
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
the egocentric reference bias and the other symptoms of
neglect.
3.4. Subjecti6e manifestations
In patient SA surprisingly, the improvement of neglect, as assessed by the line bisection test, was accompanied by a negative change in mood. Whereas the
patient was anosodiaphoric in the pre-tests period, the
lack of awareness of her left motor deficit disappeared
in the late-tests period (day 2) and raised a
‘catastrophic reaction’ with deep anxiety and depression. A psychotropic treatment had to be administered
from day 3.
4. Discussion
Our previous results showed that a substantial improvement of both straight-ahead pointing and line
bisection tasks can be obtained in neglect patients
exposed to base-left wedge prisms and that this improvement is maintained for at least 2 h [34]. The main
aim of the present study was to further investigate the
effects of prism adaptation on hemispatial neglect over
a longer testing period. In addition, this longitudinal
study turned out to be appropriate to investigate the
link between the two variables explored using a withinsubject design. Our study yielded three main results.
First, both patients adapted easily to the optical deviation, as shown by the important immediate after-effects
found on straight-ahead demonstration. Second, the
effects of prism adaptation on neglect symptoms can be
maintained over 4 days. Third, a clear double-dissociation between subjects was demonstrated on long-term
effects.
Initially, both patients exhibited a rightward bias on
the two tasks (straight-ahead demonstration and line
bisection) in the pre-exposure phase, with one patient
showing a more severe neglect (SA). This different level
of severity may be in accordance with the time postonset of the two patients (see Table 1). However, this
difference was not crucial to our comparisons, because
we did not compare the performances of the two
present patients but the presence, the duration and the
evolutive pattern of the effects of prism adaptation.
After the prism adaptation, both patients showed an
immediate leftward after-effect on straight-ahead pointing. Its amplitude was about 9° (for a 10° prismatic
deviation). This important effect is comparable to the
one observed in a group of eight neglect patients, and is
about twice the effect obtained with normal subjects in
the same condition [34]. In addition, the effect of
adaptation on straight-ahead was maintained here for
at least 2 h, which again contrasts with the after-effect
observed in normal subjects which is cancelled after a
few trials performed under visual feed-back [43]. These
first results demonstrate that both patients had no
problem developing an adaptation to the optical
deviation.
The second important result is the observation of
long lasting improvement of line bisection in SA and of
straight-ahead demonstrations in PE. As in our previous study, these long-term effects contrast with the
short duration of our adaptation procedure (about 5
min). Once the effect of prisms was maintained for 4 h
after the prism adaptation procedure, we did not observe any return to the initial pathological deviations
over the 4-day follow-up period. As the benefit seems to
be durably gained, one may assume that an important
step has been made in the recovery process. This longterm effect implies a central action of prism adaptation,
that can be based on active processes triggering plastic
neuronal changes rather than a simple orthesis effect
[see 34]. Furthermore, in both cases the improvement
consisted of a sudden quasi-normalisation of the
parameter studied. In SA, the sudden remission of
visuo–spatial neglect may explain the negative modification of mood. One may hypothesise that prism adaptation restored a symmetrical conscious representation
of peripersonal and personal space, increasing the perceptive awareness of her left hemibody hence of her
hemiplegia. This supports the idea that prism adaptation can act on cognitive levels in both neglect patient
[31,33,34] and healthy subjects [8]. It is important to
note that such a reduction of deficit awareness could
not be achieved when the patient had been repeatedly
invited to look at his left paretic hemibody.
The third interesting result obtained here is that
during the late phase following prism adaptation (days
2–4) the effects on the two symptoms were double-dissociated between the two patients. No bias in line
bisection reappeared in SA, whereas after 4 h the
rightward shift of the egocentric reference was comparable with the pretests. Patient PE exhibited the
mirror dissociation: the shift of the egocentric reference
remained improved during the follow-up period,
whereas line bisection performance was not affected by
the adaptation procedure. These results confirm that
the benefit of prism adaptation on spatial cognition is
not mediated by a modification of the egocentric reference. These two symptoms probably depend on distinct
mechanisms in different, though neighbouring, brain
structures. In reference to this point a recent functional
brain imaging study by Vallar and colleagues [40] is of
great interest. These authors asked normal subjects to
make subjective judgements of their body midline by
stopping a vertical bar moving along the horizontal
plane. Results showed that the angular gyrus (area 39),
especially in the right hemisphere, was the most activated cortical area during the execution of this task. In
another study of 110 right-handed stroke patients, Val-
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
lar and Perani [42] showed that in the subgroup of 29
patients showing severe neglect, ‘the lesions surimpose in
the supramarginal gyrus of the inferior parietal lobule’.
Therefore, the focus area responsible for midline computation and estimation (area 39) may lie just adjacent to
the main focus of the composite contour maps drawn for
the lesions responsible for neglect, that is the supramarginal gyrus (fronto– temporo – parieto junction or area
40) [42]. This anatomo– functional dissociation is likely
to explain the several dissociations recently found between neglect and the rightward bias in straight-ahead
demonstration, suggesting that these two phenomena are
not causally related [2,6,11]. Our study further demonstrates on the basis of a within-subject design that these
biases rely upon two different brain mechanisms. This
result is fully compatible with the growing evidence that
hemispatial neglect cannot be understood as a unitary
disturbance [14,25,29].
Lastly, with respect to the classical use of double-dissociation in neuropsychological studies (see [35]), the
present study has provided a new type of double-dissociation. Because the positive and negative behavioural
consequences of a given restricted lesion may be partially
explained by the reorganisation of surrounding intact
brain tissue, the specificity of the effect of a single lesion
is often questionable. A more reliable indicator of the
separation between two processes is provided by a
‘double-dissociation’, where a lesion of structure X will
specifically disrupt function A while sparing function B,
and a lesion of Y will specifically affect B while A would
remain intact [[39], review in [35]]. It is particularly
interesting that the two neglect symptoms studied here
were not dissociated in the pretest between SA and PE.
It is only the longitudinal follow-up of the patients that
uncovered the double-dissociation. The induction of
variation of at least one symptom by our prism adaptation procedure has provided a useful tool to increase the
sensitivity of the correlation studied. A ‘dynamical double dissociation’ could thus be observed whereas a single
cross-section measurement did not reveal any dissociation. Such longitudinal study of several symptoms,
combined with the description of the effects of a given
manipulation on these symptoms, should provide fruitful
information about the causal ground of neuropsychological disorders.
[2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
Acknowledgements
This work was supported by Région Rhône-Alpes
(Thématiques prioritaires) and Inserm (PROGRES).
[20]
[21]
References
[1] Bartolomeo P, Inhibitory processes and spatial bias after right
333
hemisphere
damage,
Neuropsychological
Rehabilitation,
2000;10(5):511 – 526.
Bartolomeo P, Chokron S. Egocentric frame of reference: its
role in spatial bias after right hemisphere lesions. Neuropsychologia 1999;37:881 – 94.
Bisiach E, Vallar G, Perani D, Papagno C, Berti A. Unawareness of disease following lesions of the right hemisphere:
anosognosia for hemiplegia and anosognosia for hemianopia.
Neuropsychologia 1986;24(4):471 – 82.
Bisiach E, Luzzatti C. Unilateral neglect of representational
space. Cortex 1978;14:129 – 33.
Cappa S, Sterzi R, Vallar G, Bisiach E. Remission of hemineglect and anosognosia during vestibular stimulation. Neuropsychologia 1987;25:775 – 82.
Chokron S, Bartolomeo P. Patterns of dissociation between
left hemineglect and deviation of the egocentric reference. Neuropsychologia 1997;35:1503 – 8.
Chokron S, Imbert M. Variations of the egocentric reference
among normal subjects and a patient with unilateral neglect.
Neuropsychologia 1995;33:703 – 11.
Colent C, Pisella L, Bernier C, Rode G, Rossetti Y. Cognitive
bias induced by visuo – motor adaptation to prisms: a simulation of unilateral neglect in normals? Neuroreport 2000;11:9 in
press.
Diggle PJ, Liang KJ, Zeger SL. Analysis of longitudinal data.
In: Oxford Statistical Science Serie S, vol. 13. Oxford: Oxford
University Press, 1994:1 – 19.
Driver J, Mattingley JB. Parietal neglect and visual awareness.
Nature Neuroscience 1998;1:17 – 22.
Farnè A, Ponti F, Ladavas E. In search for biased egocentric
reference frames in neglect. Neuropsychologia 1998;36:611 – 23.
Halligan PW, Marshall JC, Wade DT. Visuospatial neglect:
underlying factors and test sensitivity. Lancet 1989;2:908 –11.
Halligan PW, Marshall JC. The bisection of horizontal and
radial lines. The International Journal of Neuroscience
1993;70:149 – 67.
Halligan PW, Marshall JC. Current issues in spatial neglect:
an editorial introduction. In: Halligan PW, Marshall JC, editors. Spatial Neglect: Position Papers on Theory and Practice.
A Special Issue of Neuropsychological Rehabilitation. Hove:
Erlbaum Associates Ltd, 1994:103 – 11.
Halligan PW, Drawing attention to neglect, The Psychologist,
1995; June, 257-265.
Heilman KM, Bowers D, Watson RT. Performance on hemispatial pointing task by patients with neglect syndrome. Neurology 1983;33:661 – 4.
Heilman KM, Bowers D, Coslett HB, Whelan H, Watson RT.
Directional Hypokinesia Neurology 1985;35:855 – 9.
Heilman KM, Watson RT, Valenstein E. Neglect and related
disorders. In: Heilman KM, Valenstein E, editors. Clinical
Neuropsychology. New-York: Oxford University Press,
1985:243 – 93.
Jeannerod M, Biguer B. The directional coding of reaching
movements. A visuomotor conception of spatial neglect. In:
Jeannerod M, editor. Neurophysiological and Neuropsychological Aspects of Spatial Neglect. Amsterdam: Elsevier Science
Publishers, 1987:87 – 113.
Jeannerod M, Biguer B. Egocentric reference and represented
space. Revue Neurologique 1989;145:635 – 9.
Jeannerod M, Rossetti Y. Visuomotor coordination as a dissociable visual function: experimental and clinical evidence. In:
Kennard CC, editor. Visual Perceptual Defect, vol. 2. London:
I.P.R. Baillere Tindall Ltd, Baillere’s Clinical Neurology,
1993:439 – 60.
334
L. Pisella et al. / Neuropsychologia 40 (2002) 327–334
[22] Karnath HO, Chris K, Hartje W. Decrease of contralateral
neglect by neck muscle vibration and spatial orientation of trunk
midline. Brain 1993;116:383 –96.
[23] Karnath HO, Schenkel P, Fischer B. Trunk orientation as the
determining factor of the ‘contralateral’ deficit in the neglect
syndrome and as the physical anchor of the internal representation of body orientation in space. Brain 1991;114:1997 –2014.
[24] Marshall JC, Halligan PW. Blindsight and insight in visuo-spatial neglect. Nature 1988;336:766 –7.
[25] Mattingley JB, Bradshaw JL. How many neglects? Some considerations based on anatomy and information processing. In:
Halligan PW, Marshall JC, editors. Spatial Neglect: Position
Papers on Theory and Practice. A Special Issue of Neuropsychological Rehabilitation. Hove: Erlbaum Associates Ltd,
1994:169 – 73.
[26] Mattingley JB, Bradshaw JL, Phillips JG. Impairments of movement initiation and execution in unilateral neglect. Brain
1992;115:1849 – 74.
[27] Milner AD, Harvey M, Pritchard CL. Visual size processing in
spatial neglect. Experimental Brain Research 1998;123:192 – 200.
[28] Milner AD, Brechmann M, Pagliarini L. To halve and to halve
not: an analysis of line bisection judgements in normal subjects.
Neuropsychologia 1992;30(6):515 –26.
[29] Milner AD, Harvey M. Toward a taxonomy of spatial neglect.
In: Halligan PW, Marshall JC, editors. Spatial Neglect: Position
Papers on Theory and Practice. A Special Issue of Neuropsychological Rehabilitation. Hove: Erlbaum Associates Ltd,
1994:177 – 83.
[30] Pizzamiglio L, Frasca R, Guariglia C, Incoccia C, Antonucci G.
Effect of optokinetic stimulation in patients with visual neglect.
Cortex 1990;26:535 –40.
[31] Rode G, Rossetti Y, Li L, Boisson D. The effect of prism
adaptation on neglect for visual imagery. Behavioural Neurology
1999;11:251 – 8.
[32] Rode G, Perenin MT. Temporary remission of representational
hemineglect through vestibular stimulation. Neuroreport
1994;5:869 – 72.
[33] Rossetti Y, Rode G, Pisella L, Farnè A, Ling L, Boisson D.
Sensorimotor plasticity and cognition: prism adaptation can
[34]
[35]
[36]
[37]
[38]
[39]
[40]
[41]
[42]
[43]
[44]
affect various levels of space representation. In: Grealy M,
Thomson JA, editors. Studies in Perception and Action. New
York: Lawrence Erlbaum Associates, 1999:265 – 9.
Rossetti Y, Rode G, Pisella L, Farnè A, Ling L, Boisson D,
Perenin MT. Prism adaptation to a rightward optical deviation
rehabilitates left hemispatial neglect. Nature 1998;395:166 –9.
Rossetti Y, Revonsuo A. Beyond dissociations: recomposing the
mind-brain after all? In: Rossetti Y, Revonsuo A, editors. Beyond Dissociation: Interaction between Dissociated Implicit and
Explicit Processing. Amsterdam: Benjamins, 2000:1 – 17.
Rossi PW, Kheyfets S, Reding MJ. Fresnel prisms improve
visual perception in stroke patients with homonymous hemianopia or unilateral visual neglect. Neurology 1990;40:1597 –9.
Rubens AB. Caloric stimulation and unilateral visual neglect.
Neurology 1985;35:1019 – 24.
Schenkenberg T, Bradford DC, Ajax ET. Line bisection with
neurologic impairment. Neurology 1980;30:509 – 17.
Teuber HL. Physiological psychology. Annual Rev Psychology
1955;6:267 – 96.
Vallar G, Lobel E, Galati G, Berthoz A, Pizzamiglio L, Le
Bihan D. A fronto-parietal system for computing the egocentric
spatial frame of reference in humans. Experimental Brain Research 1999;124:281 – 6.
Vallar G, Rusconi ML, Barozzi S, Bernardini B, Ovadia D,
Papagno C, Cesarani A. Improvement of left visuo –spatial
hemineglect by left-sided transcutaneous electrical stimulation.
Neuropsychologia 1995;33:73 – 82.
Vallar G, Perani D. The anatomy of unilateral neglect after
right-hemisphere stroke lesions. A clinical/CT-scan correlation
study in man. Neuropsychologia 1986;24:609 – 22.
Welch RB, Bridgeman B, Anand S, Browman KE. Alternating
prism exposure causes dual adaptation and generalization to a
novel
displacement.
Perception
and
Psychophysics
1993;54(2):195 – 204.
Werner H, Wapner S, Bruell JH. Experiments on sensory-tonic
field theory of perception:VI. Effect of position of head, eyes and
of object on position of the apparent median plane. Journal of
Experimental Psychology 1953;46:293 – 9.