Clinical Nutrition 29 (2010) 347–351
Contents lists available at ScienceDirect
Clinical Nutrition
journal homepage: http://www.elsevier.com/locate/clnu
Original Article
Validity of predictive equations for resting energy expenditure in Belgian
normal weight to morbid obese women
Peter J.M. Weijs a, b, c, d, *, Greet A.A.M. Vansant e, f, g
a
Department of Nutrition and Dietetics, Hogeschool van Amsterdam, University of Applied Sciences, Amsterdam, The Netherlands
Department of Nutrition and Dietetics, Internal Medicine, VU University Medical Center, Amsterdam, The Netherlands
c
EMGO Institute for Health and Care Research, Amsterdam, The Netherlands
d
Department of Intensive Care Medicine, VU University Medical Center, Amsterdam, The Netherlands
e
Department of Nutrition, Public Health Medicine, Catholic University, Leuven, Belgium
f
University Hospital Gasthuisberg, Leuven, Belgium
g
LFoRCe (Leuven Food Science and Nutrition Research Centre), Catholic University, Leuven, Belgium
b
a r t i c l e i n f o
s u m m a r y
Article history:
Received 14 July 2009
Accepted 30 September 2009
Background & aims: Individual energy requirements of overweight and obese adults can often not be
measured by indirect calorimetry, mainly due to the time-consuming procedure and the high costs. To
analyze which resting energy expenditure (REE) predictive equation is the best alternative for indirect
calorimetry in Belgian normal weight to morbid obese women.
Methods: Predictive equations were included when based on weight, height, gender, age, fat free mass
and fat mass. REE was measured with indirect calorimetry. Accuracy of equations was evaluated by the
percentage of subjects predicted within 10% of REE measured, the root mean squared prediction error
(RMSE) and the mean percentage difference (bias) between predicted and measured REE.
Results: Twenty-seven predictive equations (of which 9 based on FFM) were included. Validation was
based on 536 F (18–71 year). Most accurate and precise for the Belgian women were the Huang, Siervo,
Muller (FFM), Harris–Benedict (HB), and the Mifflin equation with 71%, 71%, 70%, 69%, and 68% accurate
predictions, respectively; bias 1.7, 0.5, þ1.1, þ2.2, and 1.8%, RMSE 168, 170, 163, 167, and 173 kcal/d.
The equations of HB and Mifflin are most widely used in clinical practice and both provide accurate
predictions across a wide range of BMI groups. In an already overweight group the underpredicting
Mifflin equation might be preferred. Above BMI 45 kg/m2, the Siervo equation performed best, while the
FAO/WHO/UNU or Schofield equation should not be used in this extremely obese group.
Conclusions: In Belgian women, the original Harris–Benedict or the Mifflin equation is a reliable tool to
predict REE across a wide variety of body weight (BMI 18.5–50). Estimations for the BMI range between
30 and 40 kg/m2, however, should be improved.
Ó 2009 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved.
Keywords:
Resting energy expenditure
Predictive equation
Overweight
Obesity
Indirect calorimetry
Validation
1. Introduction
Prevalence of overweight and obesity is high and increasing.1,2
Any weight reduction program will try to establish a reachable goal
for weight loss and a reachable goal for dietary intake. This requires
knowledge of individual energy requirements, and relies on accurate methods of assessment. Since the golden standard, indirect
* Corresponding author. Department of Nutrition and Dietetics, School of Sports
and Nutrition, Hogeschool van Amsterdam, University of Applied Sciences,
Dr. Meurerlaan 8, 1067 SM Amsterdam, The Netherlands. Tel.: þ31205953534; fax:
þ31205953400.
E-mail address: p.j.m.weijs@hva.nl (P.J.M. Weijs).
calorimetry is hardly feasible in most clinical settings, it remains
important to use the most accurate predictive equation for resting
energy expenditure (REE) in overweight and obese persons.3
Predictive equations have usually been developed in healthy
subjects, based on regression analysis of body weight, height,
gender and age as independent variables and measured REE by
indirect calorimetry as dependent variable. Based on a comparison
of published evidence for Harris and Benedict,4 FAO/WHO/UNU
weight or weight and height equations,5 Mifflin6 and Owen7,8
equation, Frankenfield et al.,9 an expert panel has advised to use the
Mifflin equation for overweight and obese subjects. However, this
expert panel also acknowledges that there are limited data to
support the use of Mifflin equation in overweight and obese
subjects.9
0261-5614/$ – see front matter Ó 2009 Elsevier Ltd and European Society for Clinical Nutrition and Metabolism. All rights reserved.
doi:10.1016/j.clnu.2009.09.009
348
P.J.M. Weijs, G.A.A.M. Vansant / Clinical Nutrition 29 (2010) 347–351
The level of overweight might be an important factor for accuracy of the predictive equation, but the level of overweight varies
among studies. For most equations overweight and obese subjects
were included, but their relative contribution to the final equation
often remains unclear. Therefore validation of predictive equations
should be performed in specific overweight and obese groups of
subjects. Recent evaluations of validity of REE predictive equations
have been published for overweight and obese subjects3,10–13 and
for extremely obese subjects with BMI over 40 kg/m2.14–18 Only
a few studies have validated equations for a clearly defined overweight group (BMI 25–30)3,12 or obese group (BMI 30–40).3,10
The range of published REE predictive equations was recently
validated for US and Dutch adults,3 including equations based on
body composition (fat free mass and fat mass). As part of evidence
based practice, the literature was systematically searched for REE
predictive equations, and subsequently included REE equations
were validated with indirect calorimetry data of Belgian women
with BMI ranging from 18.5 to above 50 kg/m2 in order to find the
most accurate and precise REE predictive equation for Belgian
women.
not been physically active before the measurement and the evening
before. Oxygen consumption and carbon dioxide production were
measured and energy expenditure was calculated by the Weir
formula.20 The measurements took place for at least 30 min and
only steady state periods of measurement (20 min) were selected.
The first 10 min of the measurement was always discarded.
Acceptable coefficient of variation was 10%. Body weight, fat free
mass (FFM) and fat mass (FM) were assessed y BIA (Bodystat 1500,
Euromedix, Leuven, Belgium) immediately after calorimetry when
subjects were lying down for at least 30 min, and were still in the
fasting state. None of the subjects was using any diuretics or other
medication which may give a shift intra/extracellular water
compartments.
2.2. REE predictive equations
The inclusion of REE predictive equations has been described
elsewhere.3 Only the Siervo equation has been reintroduced, since
this was based on obese women.11 Based on 136 Dutch overweight
and obese (BMI 25–40) subjects (95F, 41M) the following Weijs
predictive equation was generated: REE (kcal/d) ¼ weight(kg)
2. Subjects and methods
14:038 þ heightðcmÞ 4:498 þ sexð0 ¼ female; 1 ¼ maleÞ
Subjects were recruited at the department of Nutrition, Public
Health Medicine (normal weight) and at the Obesity Clinic
(University Hospital Gasthuisberg) Leuven over the past years.
Inclusion criteria for the original weight loss studies were being
female above the age of 18 and a BMI above 28 kg/m2 without any
major metabolic complications. Control subjects were healthy
women within the same age category but with a BMI <28. Both
weight and height were measured under standardized conditions;
body composition was determined using the single-frequency bioelectrical impedance method using a validated equation.19 All
participants gave informed consent. All procedures were in accordance with ethical standards of the institution.
2.1. Indirect calorimetry and antropometry
The indirect calorimetry measurements were performed with
a ventilated hood system (Acertys Healthcare NV, Aartselaar,
Belgium) which was calibrated with a standard gas every day
before use. Measurements were standardized by internal guidelines. The subjects were in supine position and awake. All subjects
were fasted overnight and measured in the morning. Subjects had
137.566 age(y) 0.977 221.631.(R2 ¼ 0.69, SEE ¼ 204). This
equation has been added based on the assumption that Belgian and
Dutch subjects might be similar. Additionally, the Harris–Benedict
equation was tested based on ideal body weight (Hamwi equation),
ideal body weight plus 25% of overweight ( ¼ adjusted body weight,
ABW25), and ideal body weight plus 50% of overweight
( ¼ adjusted body weight, ABW50).
2.3. Statistics
Subject characteristics have been analysed across BMI
subgroups by ANOVA with post-hoc Bonferroni test. A prediction
between 90 and 110% of REE measured was considered an accurate
prediction, a prediction below 90% of REE measured was classified
as underprediction and a prediction above 110% of REE measured
was classified as overprediction. The percentage of patients that
had REE predicted within 10% of REE measured was considered
a measure of accuracy on the individual level.3,9 The mean
percentage difference between REE predicted and measured (bias)
was considered a measure of accuracy on a group level. The root
mean squared prediction error (RMSE) was used to indicate how
Table 1
Subject characteristics per BMI group.
BMI-group
Age, y
Height, cm
Weight, kg
BMI, kg/m2
REEb, kcal/d
REE, kcal/kg
FMg, %
FM, kg
FFMd, kg
REE, kcal/
kg FFM
RQ
a
18.5–25 N ¼ 67
a
25–30 N ¼ 45
30–35 N ¼ 145
35–40 N ¼ 147
40–45 N ¼ 80
45–50 N ¼ 35
> 50 N ¼ 17
Total N ¼ 536
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
Mean
SD
39.5
166.2
60.1
21.7
1331
22.2
27.2
16.4
44.3
30.2
10.8a
6.9a
6.5a
1.6a
150a
2.0a
5.8a
4.1a
5.6a
2.6a
43.1
163.7
75.1
28.0
1452
19.3
37.5
28.2
46.9
31.3
14.1a
5.7a
5.8b
1.5b
184b
2.1b
6.4b
5.0b
6.2a
4.6ab
41.2
165.5
89.9
32.8
1614
18.0
43.0
38.7
51.2
31.6
11.3a
6.4a
8.0c
1.4c
184c
1.8c
3.0c
4.7c
4.8b
3.4ab
42.1
163,4
100,1
37,4
1675
16,7
46,9
47,0
53,2
31,6
12.9a
6.8a
8.4d
1.5d
208c
1.7d
3.3d
5.1d
5.7b
3.3ab
41.8
164.1
113.5
42.1
1828
16.1
50.1
56.8
56.5
32.5
11.6a
7.0a
9.8e
1.3e
226d
1.7d
2.6e
5.7e
6.0c
3.2bc
40.3
164,2
127.4
47.1
2049
16.1
52.6
67.1
60.3
34.1
10.9a
7.7a
13.6f
1.5f
278e
1.4d
3.4f
8.3f
8.2d
3.4cd
37.8
162.3
139.8
53.0
2157
15.5
55.6
77.7
61.4
35.4
12.3a
7.4a
15.2g
2.4g
279e
1.5d
2.8f
8,4g
9.2d
3.9cd
41.3
164.5
95.3
35.2
1659
17.8
43.7
43.1
52.2
31.8
12.0
6.8
21.5
7.7
285
2.6
8.4
15.8
7.4
3.5
0.8
0.1
0.8
0.0a
0.8
0.1a
0.8
0.1a
0,8
0.1a
0.8
0.1a
0.8
0.1a
0.8
0.1a
ANOVA with post-hoc Bonferroni, means þ SD sharing the same character are not significantly different between these BMI groups (age and RQ, NS; height, p ¼ 0.036;
other variables p < 0.001).
b
REE, resting energy expenditure.
g
FM, fat mass.
d
FFM, fat free mass.
P.J.M. Weijs, G.A.A.M. Vansant / Clinical Nutrition 29 (2010) 347–351
160
349
3. Results
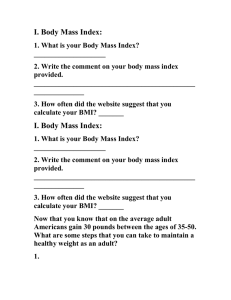
FFM and FM (kg)
140
120
100
FM
80
FFM
60
40
20
0
18.5-25 25-30
30-35
35-40
40-45
45-50
>50
BMI group
Fig. 1. Body composition of women per BMI group.
well the model predicted in our dataset.21–23 Data were analyzed
using SPSS 14.0. In earlier studies the Concordance Correlation
Coefficient and Bland–Altman were presented, however, they had
no function in the selection process and therefore they are not
presented in the present study.
Table 1 shows the subject characteristics for the 536 Belgian
women. In total, 536 women with a BMI range of 18.5–above
50 kg/m2 were included. As could be expected, REE rises with
BMI. After correction for fat free mass, the difference between the
groups largely disappears, although BMI group is still a significant
factor. No differences in respiratory quotients (RQs) were found
between the groups. Fig. 1 shows body composition of the women
for 7 different BMI groups. Table 2 shows REE in kcal/d,
percentage bias, maximum values found for negative error
(underprediction) and positive error (overprediction), the RMSE
in kcal/d, the percentage accurate predictions and the percentage
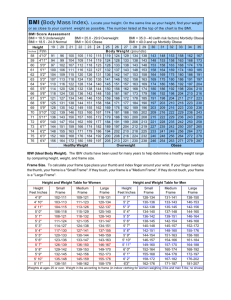
underpredictions and percentage overpredictions. Fig. 2 shows
the percentage accurate predictions for Belgian women across
BMI groups for the 5 best performing equations. Most accurate
and precise for the Belgian women were the Huang, Siervo, Muller
(FFM), original Harris–Benedict, and the Mifflin equation with
71%, 71%, 70%, 69%, and 68% accurate predictions, respectively;
bias 1.8, 0.5, þ1.1, þ2.1, and 1.9%, RMSE 168, 170, 163, 167, and
Table 2
Evaluation of REE predictive equations in 536 Belgian women based on bias, RMSE and percentage accurate predictiona.
REE predictive equation (# refers to
reference in supplementary file)
REEa
(kcal/d)
sdb
BIAS (%)c
Max. negative
error (%)d
Max. positive
error (%)e
RMSEf
Accurate
predictions (%)g
Under
predictions (%)h
Over
predic-tions (%)i
REE
HB19194
HB1984 (#1)
Bernstein (#2)
Bernstein FFMj (#2)
Owen7,8
Owen FFM7,8
Mifflin6
Mifflin FFM6
Livingston25
Schofield Wk (#3)
Schofield WHl (#3)
FAOw5
FAOwh5
Henry W (#4)
Henry WH (#4)
DeLorenzo (#5)
Siervo11
Lazzer16 (#6)
Lazzer FFM16(#6)
Muller12
Muller BMIm,12
Muller FFM12
Muller FFMBMI12
Korth (#7)
Korth FFM (#7)
Huang15
Huang FFM15
Johnstone FFM (#8)
Weijs (see Section 2)
Weijs, gender specific (#9)
HB1984IBW (see Section 2)
HB1984ABW25 (see Section 2)
HB1984ABW50 (see Section 2)
1657
1675
1687
1362
1861
1477
1361
1614
1440
1581
1672
1661
1703
1691
1651
1613
1733
1635
1737
1681
1692
1688
1659
1661
1717
1642
1614
1597
1713
1815
1800
1331
1433
1518
288
224
219
169
250
156
147
247
147
197
257
241
255
240
248
214
258
251
240
270
251
257
232
233
251
192
232
235
265
312
288
104
114
137
–
2.2
3.0
16.8
13.4
9.5
16.6
1.8
11.7
3.4
2.0
1.4
3.9
3.2
0.6
1.6
5.4
0.5
5.9
2.1
3.0
2.7
1.1
1.2
4.5
0.5
1.7
2.8
4.1
9.9
9.4
17.6
11.6
6.7
–
25.7
24.6
39.7
15.9
35.7
39.8
28.9
36.6
30.4
29.0
29.0
26.5
26.8
27.9
28.4
22.4
29.3
22.5
27.4
24.0
35.1
24.9
25.7
23.5
30.6
27.8
28.7
23.7
22.7
21.0
53.6
45.4
37.1
–
33.0
34.0
8.4
46.7
21.0
8.5
28.0
14.8
27.1
38.3
33.8
38.1
35.3
32.4
26.7
36.4
33.8
37.1
34.4
34.5
33.1
30.9
30.1
36.3
30.8
27.7
26.0
34.4
46.5
42.9
29.7
26.8
26.8
–
167
169
345
260
257
353
173
291
191
212
199
205
193
183
181
182
170
184
168
169
170
163
163
179
183
168
172
172
239
223
424
332
251
–
69
68
19
36
48
23
68
45
67
59
61
60
61
66
66
63
71
59
68
68
65
70
69
63
63
71
69
65
48
49
23
37
52
–
10
9
81
1
50
77
21
54
25
16
16
12
12
16
21
5
16
7
11
9
11
12
13
8
19
18
22
8
3
4
74
58
41
–
21
23
a
b
c
d
e
f
g
h
i
j
k
l
m
REE, resting energy expenditure (as measured).
SD, standard deviation.
BIAS, mean percentage error between preditive equation and measured value.
Max. negative error, the largest underprediction that was found with this predictive equation as percentage of measured value.
Max. positive error, the largest overprediction that was found with this predictive equation as percentage of measured value.
RMSE, root mean squared prediction error (kcal/d).
Accurate predictions, the percentage of subjects predicted by this predictive equation within 10% of measured value.
Underpredictions, the percentage of subjects predicted by this predictive equation <10% of measured value.
Overpredictions, the percentage of subjects predicted by this predictive equation >10% of measured value.
FFM, equation based on fat free mass (as opposed to based on body weight).
W, equation based on body weight (as opposed to weight and height).
WH, equation based on body weight and height (as opposed to weight only).
BMI, BMI specific equations for subgroups BMI equal to 18.5–25, 25–30, >30.
63
2
11
1
8
25
23
28
27
18
13
32
13
34
22
23
24
18
18
29
18
11
9
28
49
48
4
5
7
350
P.J.M. Weijs, G.A.A.M. Vansant / Clinical Nutrition 29 (2010) 347–351
Accurate predictions (%)
90
85
80
Huang
75
Siervo
HB1919
70
Mifflin
MullerFFM
65
60
55
50
18.525
25-30
30-35
35-40
40-45
45-50
>50
BMI groups
Fig. 2. Percentage accurate REE predictions for Belgian women per BMI category for
the 5 best scoring equations.
173 kcal/d. The widely used original HB and Mifflin equations
might be preferred over new equations, with Mifflin providing
more underpredictions and HB more overpredictions. Accurate
predictions were consistent across BMI groups except for BMI 30–
40, which had fairly low accuracy. The Weijs equation performed
well with 87% accurate predictions in the normal weight group,
however, provided no advantage over the original Harris–Benedict or Mifflin equation in the obese groups. Above BMI 45 kg/m2,
the Siervo equation performed best, while the FAO/WHO/UNU or
Schofield equations should not be used in this extremely obese
group (FAOwh 45–50, 51%; FAOwh >50, 29%; SchofieldWH 45–50,
37%; SchofieldWH >50, 29%). Using ideal or adjusted body weight
for Harris–Benedict (HB1984) did not improve the REE prediction.
4. Discussion
From this study it appears that resting energy expenditure for
Belgian normal weight to morbid obese women can safely be
predicted with the original Harris–Benedict (HB) or the Mifflin
equation. Mifflin might even be preferred in an already overweight
and obese group, since it provides more underpredictions and less
overpredictions of REE relative to HB. Although the Huang, the
Siervo and the Muller (FFM) equations also performed consistent
across BMI groups, including the BMI >50 group, the HB and Mifflin
equations are already widely used in clinical practice. It is important to notice that all REE predictive equations performed least for
the BMI range 30–40. This group is frequently seeking help for
weight loss and REE estimations should still be improved for this
very large group of people. The Siervo equation performed best at
BMI >45. While the FAO/WHO/UNU or Schofield equations should
not be used for BMI >45 kg/m2. This is also important since the
Schofield equation is most recommended in guidelines in Belgium.
Recently the validity of the same set of equations has been
assessed by Weijs3 for US and Dutch adults with BMI 25–40, which
provided clear evidence for the Mifflin equation to be the preferred
equation for the US adults. For the Dutch there was not one single
accurate equation. For the Dutch adults with BMI 25–40 kg/m2,
new Weijs equations have been developed, a general equation with
weight, height, age, and gender as variables and two gender specific
equations with weight, height, and age as variables. The gender
specific equation was cross-validated in Dutch adults and provided
80% accurate predictions, in line with the Mifflin equation for US
adults with BMI 25–40. The general equation including weight,
height, age, and gender performed less by cross-validation in the
Dutch group BMI 25–40, and performed very well in Belgian
women BMI 18.5–25. Whether the HB or Mifflin equation was also
the best choice for overweight and obese female Belgian inpatients
and outpatients remains to be established.
A recent review by an expert panel9 advised the Mifflin equation
for overweight and obese subjects. This expert panel acknowledges
that there are limited data to support the use of Mifflin equation in
overweight and obese subjects. This evidence has now been
provided by Weijs,3 however, only for US and Dutch adults. It seems
that the Mifflin equation would also perform well in overweight
and obese Belgian women. The Dutch women were taller and
heavier within each BMI group compared to the US group. The
mean height and weight of the Belgian women with BMI 25–30 and
BMI 30–35 are almost identical to the mean values of the US group,3
which is in line with a much better performance of the US Mifflin
equation in the Belgian overweight and obese women compared to
the Dutch group. The evidence for the Mifflin equation to be
accurate is now extended to the more obese groups, although not
reaching 80% accurate predictions.
Recent evaluations of validity of REE predictive equations have
been published for overweight and obese subjects10–13 and for
extremely obese subjects.14–18 The accuracy rate found with the
Mifflin equation in the present study came very close to the accuracy rate found by Frankenfield10 (68 vs. 70%). There is more
support for the Mifflin equation in European American females,24
males25 and in extremely obese females.17 Also the original HB has
been found acceptable in a broad weight range12 and in extremely
obese.14,16 Like in the present study, Frankenfield10 found the
original HB equation to perform better in the morbidly obese (BMI
>40) than in the next lowest class (BMI 30–40). The study by Lazzer
et al.,16 evaluated REE of women with BMI >40 and also found the
original HB equation to perform best together with Siervo, then the
FAOwh and Huang, and then the Mifflin equation. Accurate
predictions were within the 5% limit, and therefore the actual
numbers cannot be compared.
However, there seems to be no consensus for the use of one
preferred REE equation. This might be explained by differences in,
e.g. subject group composition, methodology and statistics.3
Measurement conditions in this study were very strictly standardized which is certainly a strong point of this study. Only
women were studied for the simple reason that mainly women
attend the Obesity Clinic. To create a comparable group, the normal
weight persons were also only women. In the Belgian population,
the prevalence of obesity is still rising, comparable with most
Western countries. At this moment, about 30% of the adult women
are overweight while 10% is obese (BMI > 30 kg/m2). For this study,
severely obese women could be included since a University
Hospital (third line) was involved. Most women did multiple
attempts to lose weight before, but did not succeed.
It is advisable to validate REE prediction equations for every
single specific population, since prediction equations are expected
to be valid for the original population only.26 This is especially true
for individual accuracy: the percentage of accurate predictions.
There is still, room for improvement of REE predictive equations in
overweight and obese women, especially the very large BMI 30–40
group.
In conclusion, this study again demonstrates that there is a wide
variation in accuracy for REE predictive equations. For Belgian
women, ranging from normal weight to morbidly obese, either the
original Harris–Benedict or the Mifflin equations can be used.
Further improvement of accuracy from 71% to >80% should be
strived for, since this has been possible for the Mifflin equation in
the US and the Weijs equation in the Dutch group. Whether the HB
or Mifflin equation was also the best choice for overweight and
obese female Belgian inpatients and outpatients remains to be
established.
Conflict of interest
All authors have no conflict of interest to declare.
P.J.M. Weijs, G.A.A.M. Vansant / Clinical Nutrition 29 (2010) 347–351
Acknowledgements
Thanks to Ageeth Hofsteenge for her contribution in literature
search.
PW and GV designed the study, performed literature search,
data analysis, and wrote the manuscript.
References
1. Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence
of overweight and obesity in the United States, 1999–2004. JAMA
2006;295:1549–55.
2. Schokker DF, Visscher TL, Nooyens AC, van Baak MA, Seidell JC. Prevalence of
overweight and obesity in the Netherlands. Obes Rev 2007;8:101–8.
3. Weijs PJ. Validity of predictive equations for resting energy expenditure in US
and Dutch overweight and obese class I and II adults aged 18–65 y. Am J Clin
Nutr 2008;88(4):959–70.
4. Harris JA, Benedict FG. A biometric study of basal metabolism in man. Washington, DC: Carnegie Institute of Washington; 1919.
5. FAO/WHO/UNU. Energy and protein requirements. Geneva: WHO; 1985. WHO
Technical Report Series.
6. Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive
equation for resting energy expenditure in healthy individuals. Am J Clin Nutr
1990;51:241–7.
7. Owen OE, Kavle E, Owen RS, Polansky M, Caprio S, Mozzoli MA, et al.
A reappraisal of caloric requirements in healthy women. Am J Clin Nutr
1986;44:1–19.
8. Owen OE, Holup JL, D’Alessio DA, Craig ES, Polansky M, Smalley KJ, et al.
A reappraisal of the caloric requirements of men. Am J Clin Nutr 1987;46:875–85.
9. Frankenfield D, Roth-Yousey L, Compher C. Comparison of predictive equations
for resting metabolic rate in healthy nonobese and obese adults: a systematic
review. J Am Diet Assoc 2005;105:775–89.
10. Frankenfield DC, Rowe WA, Smith JS, Cooney RN. Validation of several established equations for resting metabolic rate in obese and nonobese people. J Am
Diet Assoc 2003;103:1152–9.
11. Siervo M, Boschi V, Falconi C. Which REE prediction equation should we use in
normal-weight, overweight and obese women? Clin Nutr 2003;22(2):193–204.
12. Müller MJ, Bosy-Westphal A, Klaus S, Kreymann G, Lührmann PM, NeuhäuserBerthold M, et al. World Health Organization equations have shortcomings for
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
351
predicting resting energy expenditure in persons from a modern, affluent
population: generation of a new reference standard from a retrospective
analysis of a German database of resting energy expenditure. Am J Clin Nutr
2004;80:1379–90.
De Luis DA, Aller R, Izaola O, Romero E. Prediction equation of resting energy
expenditure in an adult Spanish population of obese adult population. Ann Nutr
Metab 2006;50:193–6.
Das SK, Saltzman E, McCrory MA, Hsu LKG, Shikora SA, Dolnikowski G, et al.
Energy expenditure is very high in extremely obese women. J Nutr
2004;134:1412–6.
Huang KC, Kormas N, Steinbeck K, Loughnan G, Caterson ID. Resting metabolic rate
in severely obese diabetic and nondiabetic subjects. Obes Res 2004;12:840–5.
Lazzer S, Agosti F, Silvestri P, Derumeaux-Burel H, Sartorio A. Prediction of
resting energy expenditure in severely obese Italian women. J Endocrinol Invest
2007;30(1):20–7.
Dobratz JR, Sibley SD, Beckman TR, Valentine BJ, Kellogg TA, Ikramuddin S, et al.
Predicting energy expenditure in extremely obese women. J Parenter Enteral
Nutr 2007;31(3):217–27.
Boullata J, Williams J, Cottrell F, Hudson L, Compher C. Accurate determination
of energy needs in hospitalized patients. J Am Diet Assoc 2007;107(3):393–401.
Vansant G. Valiation of the bio-electrical impedance method in severely obese
women. Int J Obes 2000;24(Suppl. 1). Abstract 610.
Weir JB. New methods for calculating metabolic rate with special reference to
protein metabolism. J Physiol 1949;109:1–9.
Weijs PJM, Kruizenga HM, van Dijk AE, van der Meij B, Langius JAE, Knol DL,
et al. Validation of predictive equations for resting energy expenditure in adult
outpatients and inpatients. Clin Nutr 2008;27(1):150–7.
Kutner MH, Nachtsheim CJ, Neter J, Li W. Applied linear statistical models. 5th ed.
New York: McGraw-Hill/Irwin; 2005.
Sheiner LB, Beal SL. Some suggestions for measuring predictive performance.
J Pharmacokinet Biopharm 1981;9:503–12.
Vander Weg MW, Watson JM, Klesges RC, Eck Clemens LH, Slawson DL,
McClanahan BS. Development and cross-validation of a prediction equation for
estimating resting energy expenditure in healthy African–American and
European–American women. Eur J Clin Nutr 2004;58:474–80.
Livingston EH, Kohlstadt I. Simplified resting metabolic rate – predicting
formulas for normal-sized and obese individuals. Obes Res 2005;13:
1255–62.
Moreira da Rocha EE, Alves VGF, Silva MHN, Chiesa CA, da Fonseca RBV. Can
measured resting energy expenditure be estimated by formulae in daily clinical
nutrition practice? Curr Opin Clin Nutr Metab Care 2005;8:319–28.